Embed Size (px)
Citation preview

PEDIATRIC DENTISTRY/Copyright © 1982 byAmerican Academy of Pedodontics
Special Issue/Radiology Conference
Radiographic considerations for specialpatients -- modifications, adjuncts, andalternatives
Paul S. Casamassimo, DDS, MS
IntroductionThe charge for this presentation is threefold: 1) To
describe radiographic techniques advocated for specialpatient populations, 2) To comment on the adequacyof the techniques, and 3) To discuss alternatives to ra-diographic surveys.Special Patient Populations
The term special, as interpreted from the literature,includes patients whose age, development, or diseaserequires modification of usual intraoral radiographictechnique or precludes its use. Special patients mayrequire extraoral techniques or may have to be treatedwithout a radiographic diagnosis. Table 1 depicts thedental literature descriptions of special patients in de-tail. Although these descriptions are somewhat vague,they represent what is available and will be the work-ing definitions used in this presentation.Criteria for Adequacy
Determination of the adequacy of usual and modi-fied techniques requires application of criteria relatedto the patient, technician/diagnostician, and tech-nique. Manson-HingI provides eight criteria for choos-ing a technique. They are:
1. Time expended by personnel,2. Effort expended by personnel,3. Radiation dosage patient subjected to,4. Accuracy of technique,5. Ability of diagnostician to use the product of the
technique,6. Skill and familiarity of the technician,7. Patient ability and needs,8. Available equipment.
Others have described criteria for determining ade-quacy of individual films, ~ Although the literatureprovides information on most of the criteria above forvarious techniques, the data using patient ability andneeds as a main variable -- 7. above -- are scanty.
This author could find only three studies thatlooked at patient ability or need in an organized fash-ion. Two of these4.~ compared the supine patient to theupright patient. Another compared intra- and extrao-ral film survey combinations for patient comfort usingchildren as subjects.6 Due to the lack of available dataon accuracy, comments about the adequacy of altema-
tives to usual techniques will be the opinion of thisauthor. Manson-Hing’s criteria will be the basis forcritique of various techniques.
Alternatives to Radiographic ExaminationsFinally, the presentation will cover alternatives to
radiographic eg~ninations in oral diagnosis. The fewavailable alternative techniques will be describedbriefly and evaluated in relation to characteristics ofspecial patient populations.
Radiographic Techniques for the SpecialPatient
The dental literature provides mtmerous tech-niques which are purported to be effective with specialpatients. For the purposes of this presentation, the in-troral film -- the periapical or bitewing -- will be con-sidered usual and customary. All of the modifications,
Table 1. Characteristics of special patient populations asdescribed in the dental literature.
448 SPECIAL PATIENT CONSIDERATIONS: Casamassimo

adjuncts, and alternatives will be considered depar-tures from the intraoral film or film survey in whichthe patient provides complete cooperation.
The alternatives to usual and customary intraoralradiography comprise four major categories:
1. Modifications of the intraoral technique,2. Adjuncts in the form of devices, personnel, or in-
duced changes in the patient,3. Alternatives to intraoral filming which include
the extraoral film techniques,4. Miscellaneous approaches.These four alternative approaches will be described
in this section.1. Modifications of the Intraoral Technique.
Table 2 (p. 450) depicts the many modifications of in-traoral radiography described in the literature. Thesemodifications can be grouped very roughly into fourcategories:
(1.1) Modifications of the film packet,(1.2) Modification of the film holder,(1.3) Supporting devices for the film holder or pa-
tient’s jaw,(1.4) Modification of the film or film holder posi-
tion.(1.1) Modifications of the film packet include
bending the corners,7 using the smallest possible film,8
or bending an occlusal film for use in either the ante-rior or posterior area.9,1° All of these techniques are rec-ommended for young children whose size, anxiety, orboth, require a minimum of discomfort. Another mod-ification for comfort is that recommended by Lewis etal." in which cotton rolls are taped to the film packetto provide comfort and to maintain the plane of thefilm. All of the above techniques are suggested as al-ternatives to usual and customary techniques. Mini-mal criteria are provided to suggest when to use theseand no data to show they are effective. The choice ofone or the other apparently is made from one’s experi-ence, or trial and error.
(1.2) Modifications of film holder include usingthe Rinn Snap-A-Raya in place of another intraoralholder, or making a film holder from tongue depres-sors and tape.~2 The benefit of these modifications ap-pears to be the ease with which the handicapped oryoung patient can hold the film. The method forchoosing these techniques, as well as their advantages,is reported empirically. Starkey’3 also reported abitewing technique using a rubber band held by thechild, but did not suggest indications for the techniqueother than its use with children.
(1.3) Supporting devices for the film holder orpatient’s jaw include mouth props, helmets with chinstraps, or straps with Velcro strips. TM Jaw control ap-pears to be the criterion for choosing any one of thesetechniques. The handicapped patient with poor jaw
"Rinn Company, Elgin, Illinois
control, either for opening or closing, would be helpedby this technique. The Velcro strap and the helmetchin strap are used to keep the jaw closed after thefilm or film holder has been placed. A similar tech-nique is used for unconscious patients being treatedunder general anesthesia.~4 The mouth props are usedto hold film holders against the teeth.
(1.4) Modifications of the film or film holderposition have been advocated for gagging, handicap-ping conditions, and the young or recalcitrant child.’5,~s
One technique, the "reverse" bitewing, involves place-ment of the film in the buccal vestibule and directingthe beam through the jaws from the opposite side ofthe patient’s head. The buccal placement minimizesgagging yet provides a radiograph that looks muchlike a usual and customary periapical or bitewing, ex-cept for superimposition of the intervening structures.This technique does require an immobile patient, andwith even minimal movement the already compro-mised quality is jeopardized. The technique may notwork unless gagging is the sole problem.
The occlusal film is often advocated as a substitutefor periapical views in the young child ~7,~,~° and thetechnique is described in several pediatric dentistrytextbooks2~~ The patient who has suspected trau-matic injury to the teeth and jaws can also be consid-ered "special" and the occlusal film is indicated foremergency surveys.
A final modification of film position is that de-scribed by Beaver~ in which a pedodontic film is insert-ed lengthwise in a Rinn Snaparay to provide the smal-lest mesial-distal length possible while still permittingrepresentation of contacting tooth surfaces.
2. Adjuncts in the Form of Devices, Personnel,or Induced Changes in the Patient. Table 3 depictsthe behavioral, pharmacological, and physical ad-juncts which can be used with usual and customarytechniques, or with the modifications suggested earlierin this presentation.
Behavior techniques used as adjuncts include fami-liarization with technique and machine (also known topediatric dentists as tell-show-do),~ distraction of theyoung patient, ~ postponement of radiographic exami-nation for two or three appointments,~ and hypnos-is. ~,~ The young child may require familiarization, dis-traction, or postponement while the gagging adultmay need help with hypnosis. All of these are usualand customary techniques or modifications. Familiari-zation may take time, but the raport established maycarry over to continuing treatment. Postponementpresents the risk of having to begin treatment withoutradiographs or asking parents to return for visits usedmainly to condition the child. Hypnosis requires askill many dentists do not have; many patients cannotbe hypnotized.
Pharmacological agents have been advocated to se-
PEDIATRIC DENTISTRY: Volume 3, Special Issue 2 449
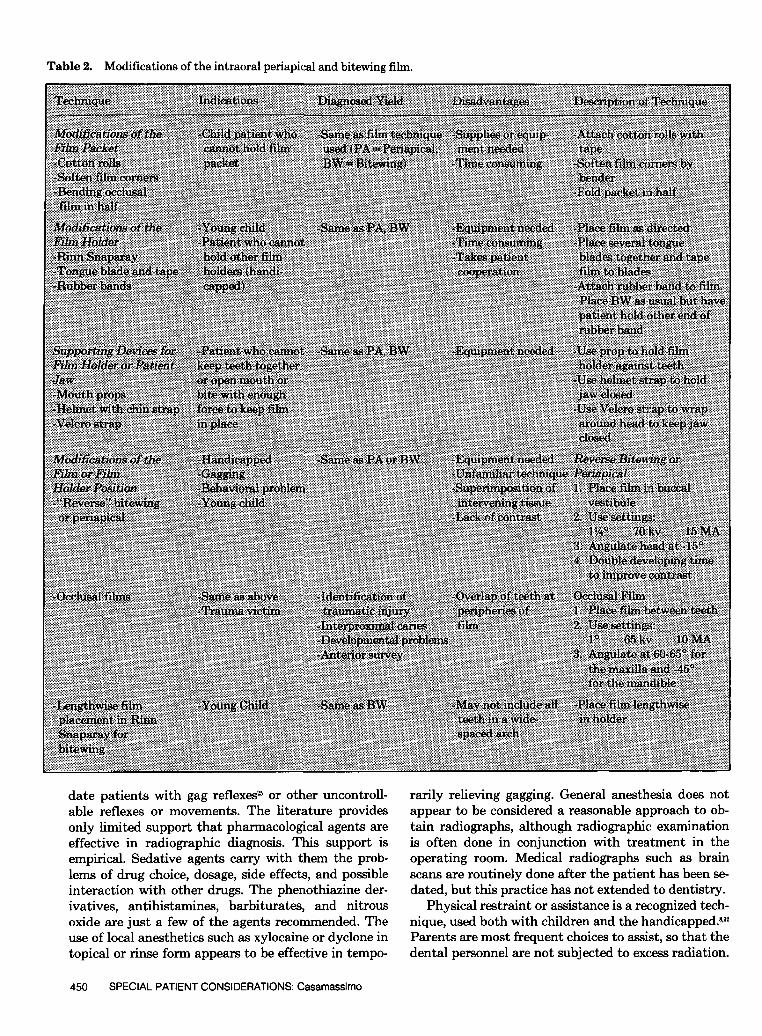
Table 2. Modifications of the intraoral periapical and bitewing film.
date patients with gag reflexes= or other uncontroll-able reflexes or movements. The literature providesonly limited support that pharmacological agents areeffective in radiographic diagnosis. This support isempirical. Sedative agents carry with them the prob-lems of drug choice, dosage, side effects, and possibleinteraction with other drugs. The phenothiazine der-ivatives, antihistamines, barbiturates, and nitrousoxide are just a few of the agents recommended. Theuse of local anesthetics such as xylocaine or dyclone intopical or rinse form appears to be effective in tempo-
rarily relieving gagging. General anesthesia does notappear to be considered a reasonable approach to ob-tain radiographs, although radiographic’, examinationis often done in conjunction with treatment in theoperating room. Medical radiographs such as brainscans are routinely done after the patient has been se-dated, but this practice has not extended to dentistry.
Physical restraint or assistance is a re~ognized tech-nique, used both with children and the handicapped.~
Parents are most frequent choices to assist, so that thedental personnel are not subjected to excess radiation.
450 SPECIAL PATIENT CONSIDERATIONS: Casamassimo

Lead gloves and aprons are standard equipment toprotect those assisting. One difficulty with parentalassistance is their lack of familiarity with technique.This lack of skill often necessitates repeated filming.
The use of restraining devices such as the Papooseboardb or Pediwrapc is poorly documented. These devi-ces restrain the body, but may not adequately controlhead or mouth movements.
3. Alternatives to Intraoral Filming -- Extrao-ral Techniques. When intraoral filming is not possi-ble or practical due to a child’s age or a patient’shandicap, extraoral techniques may be the only alter-native. The lateral jaw or lateral oblique and the pan-oramic films are the most common substitues for in-traoral surveys. Table 4 shows three alternatives to in-traoral techniques.
The lateral jaw exposure provides a unilateral viewof the posterior dentition and jaws2,~~ Traumatic in-juries, periapical pathosis, and dental developmentalstatus can be seen on the lateral jaw film. The tech-nique involves an occlusal film or lateral film cassetteon the side to be filmed. The X-ray head is placed onthe opposite side and the beam directed through theface to the cassette or film packet. The patient or par-ent can hold the film, or it can be taped to the face. A
bOlympic Medical Corporation, Seattle, Wash.cClark Associates, Inc., Worchester, Mass.
child or handicapped patient may be filmed lying onhis or her side with the film between face and dentalchair. A lead shield can be placed on half the film orcassette and the same cassette used to display bothsides of the patient.
The panoramic film~ (Panorex ~, Orthopantom-ographe) is another extraoral technique used for theyoung child, the trauma victim, or the handicappedpatient. The technique yields a general survey cover-ing a large proportion of the face, but in detail toopoor for early caries detection or identification ofminor periodontal problems,sl Oral structures are alsodistorted, but with a head positioner the distortionmay be predictable. ~ The dose administered is lessthan that for a full mouth survey,~ although in chil-dren, the thyroid receives a dose higher than that re-ceived by an adult, u The technique also allows filmingof the handicapped patient without transfer.Valachovic and Lurie~ feel that the indications forpanoramic radiography are limited from the stand-point of decreased radiation exposure since, in manycases, additional intraoral films are taken whenpathosis is identified.
The Siemens Status-xf provides still another optionfor extraoral filming. This machine is not common in
dS. S. White Penwalt Corporation, X-ray DivisioneSiernens Electric Ltd., Medical Systems~Siemens Electric Ltd., Medical Systems
Table 3. Adjuncts to the intraoral or modified intraoral film.
i~::~::~!~i::~:~:~i~::iii~ ~ ii~i~i~i~:: .............................
~::~?::~::~::::~ :::::::::::::::::::::::::::::::::::::::::::::::::::::::: ~::~::~::~::~
:::::::::::::::::::::::::::::: .................~ ..................
::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::::: ::::::::::::::::::::::::::::
~ ....................
PEDIATRIC DENTISTRY: Volume 3, Special Issue 2 451
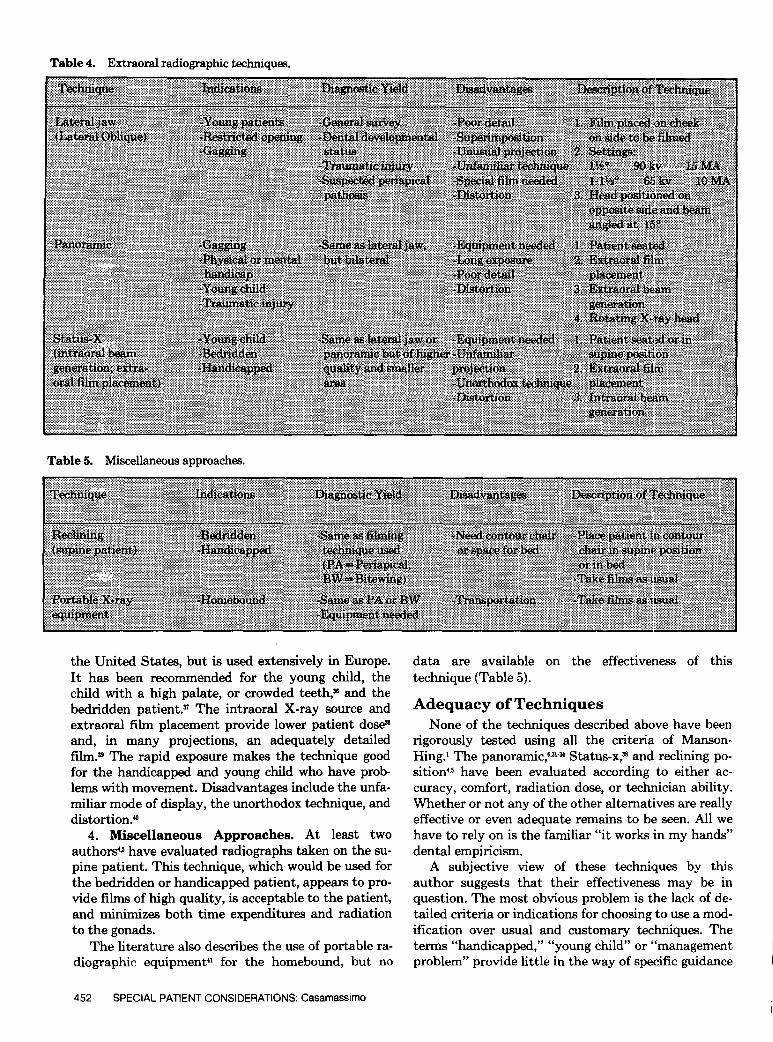
Table 4.
Table 5.
Extraoral radiographic techniques.
Miscellaneous approaches.
the United States, but is used extensively in Europe.It has been recommended for the young child, thechild with a high palate, or crowded teeth, s and thebedridden patient. ~ The intraoral X-ray source andextraoral film placement provide lower patient dose~
and, in many projections, an adequately detailedfilm. ~ The rapid exposure makes the technique goodfor the handicapped and young child who have prob-lems with movement. Disadvantages include the unfa-miliar mode of display, the unorthodox technique, anddistortion.~
4. Miscellaneous Approaches. At least twoauthors~ have evaluated radiographs taken on the su-pine patient. This technique, which would be used forthe bedridden or handicapped patient, appears to pro-vide films of high quality, is acceptable to the patient,and minimizes both time expenditures and radiationto the gonads.
The literature also describes the use of portable ra-diographic equipment4’ for the homebound, but no
data are available on the effectiveness of thistechnique (Table 5).
Adequacy of Techniques
None of the techniques described above have beenrigorously tested using all the criteria of Manson-Hing.~ The panoramic,~3~u Status-x,s and reclining po-sition 4.s have been evaluated according to either ac-curacy, comfort, radiation dose, or technician ability.Whether or not any of the other alternatives are reallyeffective or even adequate remains to be seen. All wehave to rely on is the familiar "it works in my hands"dental empiricism.
A subjective view of these techniques by thisauthor suggests that their effectiveness may be inquestion. The most obvious problem is the lack of de-tailed criteria or indications for choosing to use a mod-ification over usual and customary techniques. Theterms "handicapped," "young child" or "managementproblem" provide little in the way of specific guidance
452 SPECIAL PATIENT CONSIDERATIONS: Casamassimo

for the clinician. Gagging is probably the clearest cri-terion for modification of technique, but no authorprovides a suitable method for identifying this prob-lem or measuring its severity other than trial anderror.
Manson-Hing~ considers time and effort of person-nel a prime consideration in choosing a technique. Itshould be obvious that both additional time and effortwill be expended if adequate criteria are not availablefor choosing a technique suitable for a special patient.In addition, the rarity with which these techniquesare used in general dental practice make one suspectthat additional time and effort will be expanded to ob-tain a suitable product. The technical process is notrote and may require repetition to obtain even a com-promised product.
This lack of familiarity leads to several other short-comings related to radiation dose and quality or ac-curacy of films. Both the panoramic film and the lat-eral jaw deliver less radiation than a full-mouth seriesof intraoral films, but if patient selection is poor or ifthe technician is not familiar with the technique, filmswill have to be retaken because of a nondiagnosticproduct. The low dosage advantages may be lost inorder to obtain diagnostic quality.
Another major shortcoming of these techniques isthe need for additional equipment or supplies. Manypractitioners do not have the option of a panoramicfilm. Parental assistance requires both a lead apronand lead gloves which accounts for an expenditure ofabout $200 and parental willingness.
A factor mentioned by Manson-Hing which mightgo unnoticed is the ability of the diagnostician to readfilms of varying quality and format. The lateral jawand panorex present views which are less familiar tothe general dentist. Their detail is limited and struc-tures are not only in strange relationships to one an-other, but distorted in size and form. Whether or notevery clinician can sort out these variations frompathosis has not been clearly demonstrated in theliterature.
To determine whether a technique is adequate onemust also consider the patient’s needs. The panoramicfilm has been shown to be inadequate for diagnosis offine detail such as early or incipient dental caries.~1
The lateral jaw provides even less information in lessdetail, and in a more distorted and unusual view.These are not diagnostically equivalent to a full-mouth intraoral survey.
The young child appears to have need for only themost simple of surveys, and postponement is often ad-vocated except for clarification of obvious problemsfirst observed clinically ’; Most authors who advocateddeferring radiographic examination did so prior toHeadstart program data which indicate that abouthalf of two-year-old children have dental decay. One
also has to ask if an occasional occlusal film will suf-fice, since studies comparing a 3-film survey to an 8-film survey show that the former missed a large pro-portion of congenital anomalies.4~
The handicapped patient presents dental needstoday which are vastly different from even a decadeago. The panoramic film or lateral jaw that wouldhave been sufficient for the extractions that were therule in the handicapped population before will not suf-fice today for the handicapped person whose oralhealth has improved with increased awareness. To-day’s handicapped person tends to have fewer cariouslesions than in the past, but is still plagued with perio-dontal disease. Bitewing films or the panoramic film,which would be the minimum of a "survey" for thehandicapped patient, do not show either occlusal car-ies, or early interproximal lesions respectively,a This isthe disease state being seen more and more often withthe handicapped, especially those who have benefitedfrom fluoride.
Periodontal disease, which is the more critical prob-lem for the handicapped person today, is resistant toradiographic examination in its early stages.~ Evenlongstanding periodontal defects can be missed on ra-diographic examination, depending on location.~
Based on the above discussion, this author con-cludes that the available techniques are a last resortwhen all other possibilities have been tried. Theyshould be considered 1) adjunctive and 2) most effec-tive when used only as indicated.
As a ’final comment on adequacy, it should be notedthat we are currently investigating several of thesetechniques in an organized fashion at the Universityof Colorado. We hope to be able to determine specificindications as well as effectiveness according to thecriteria of Manson-Hing1
Alternatives to Radiographic
ExaminationVery few alternatives to radiographic examination
exist in the special patient population. The reasons forthis are that most other adjuncts to a clinical exami-nation require a subjective evaluation by the patientas well as the clinician. The radiograph obtains objec-tive data from the patient which the clinician looks atsubjectively. Pulp testing and percussion, for example,require patient input which is difficult to obtain fromthe handicapped or young child patient.
Transillumination is one objective technique, but italso has limitations in terms of its diagnostic yield. In-terproximal caries of anterior teeth can be noted, ascan be crown fractures and some forms of soft tissuepathosis. Transillumination does not provide informa-tion about deep structures, nor details about existingpathosis.
In summary, short of a thorough clinical examina-
PEDIATRIC DENTISTRY: Volume 3, Special Issue 2 453

tion, no suitable alternatives exist. It would appearthat the ready availability of radiographic examina-tion may have deterred development of other usefultechniques. Perhaps in the future, we may have tech-niques comparable to ultrasound or automated serumtesting which are used widely in medicine.
Summary
A large number of alternatives to usual and cus-tomary radiographic techniques exist, yet indicationsare vague and efficacy is largely unproven. These tech-niques range from modifications of intraoral techni-ques to extraoral techniques. The varied nature of thespecial patient population and the lack of significantstudy data on the alternative techniques make theselittle better than last resorts. All modifications, ad-juncts, and alternatives should be viewed as sub-stitutes rather than equivalents to the usual and cus-tomary intraoral film.
Dr. Casamassimo is ~ciate professor and chief of dentistry, JohnF. Kennedy Child Development Center and School of Dentistry,University of Colorado Health Sciences Center, 4200 East NinthAvenue, Denver, Colorado 80262. Reprint requests should be sent tohim.
References1. Manson-Hing, L. R. On the evaluation of radiographic tech-
niques. Oral Surg 27:631-34, 1969.2. Wuehrmann, A. H. Evaluation criteria for intraoral radiographic
film quality. JADA 89:345-52, 1974.3. Crandell, C. E. The American Academy of Dental Radiology
training requirements in radiology for the dental assistant. JAmer Dent Hyg Aasn 45:49, 1970.
4. Park, J. K. Radiographic technic in the contour dental chiar. JAmer Dent Hyg Assn 46:351-58, 1972.
5. Shawkat, A. H., Nolting, F. W., Phillips, J. D., and Banks, T. E.Evaluation of the utilization of the supine position for intraoralradiology. Oral Surg 43:963-70, 1977.
6. Khanna, S. L. and Harrop, T. J. A five-film oral radiographicsurvey for children. J Dent Child 40:42-48, 1973.
7. Bean, L. R. and Isaac, H. K. X-ray and the child patient. DentClin NAmer 17:13-24, 1973.
8. Smith, N. J. D. Radiography in children’s dentistry, periodontaltreatment and minor oral surgery. Brit Dent J 135:221-4, 1973.
9. Beaver, H. A. Radiographic technics for the young child in yourpractice. J Mich State Dent Assoc 54:282-7, 1972.
10.Silha, R. E. The versatile occlusal dental X-ray film. Dent Ra-diol Photo 39(2):40-43, 1966.
11.Lewis, T. M., Tidswell, B. A., and McQuillan, K. A. Pedodonticroentgenology -- a practical technique. Aust Dent J 8:97-100,1963.
12.Braff, M. E. X-raying the handicapped patient. J Amer DentHyg Aasn 51:449-52, 1977.
13.Starkey, P. Bitewing radiographic technique for the young child.Dent Dig 73:488-91, 1967.
14.Coke, J. M. Personal communication. March, 1981.15.Steinberg, A. D. and Bramer, M. L. A new concept in extra- and
intraoral radiographs. J Dent Child 31:34-37, 1964.16.Groper, J. N., Nishimine, K., and O’Grady, C. A simplified ra-
diographic technique for the difficult patient. J Dent Child 32:269-70, 1965.
17.Blackman, S. Radiology in child and adolescent stomatology.Dent Pract Dent Rec 12:77-85, 1961.
18.Williamson, G. F. Alternatives to full-mouth radiographs. JAmer Dent Hyg Assn 53:118-120, 1979.
19.Davis, J. M., Law, D. B., and Lewis T. An Atlas of Pedodontics,2rid Edition. Philadelphia, W. B. Saunders Company, 1981.
20.McDonald, R. E. and Avery, D. R. Dentistry for the Child andAdolescent, 3rd Edition. St. Louis, C. V. Mosby Company, 1978.
21. Braham, R. L. and Morris, M. E. Textbook of Pediatric Den-tistry. Baltimore, Williams and Wilkins Company, 1980.
22.Koppelman, E. S. The philosophy of radiographic examinationof the child. J New Jersey St Dent Soc 36:200, 1965.
23.Darzenta, N. C. and Tsamtsouris, A. Radiography in pedodon-tics. J Pedo 2:228-36, 1978.
24.Bachman, L. H. Pedodontic radiograph. Dent Radiol Photo 44:51-56, 1971.
25.Kramer, R. B. and Braham, R. L. The management of thechronic or hysterical gagger. J Dent Child 44:111-116, 1977.
26.Weyandt, J. A. Three case reports in dental hypnotherapy.Amer J Clin Hyp 15:49-55, 1972.
27.Moskowitz, E. M. and Moskowitz, H. Simplified extraoral ra-diography. Brit Jour Orthodontics 3(3):139-141, 1976.
28. Poyton, H. G. and Fireman, S. M. The oblique lateral ra-diographic projection in dental practice. J Canad Dent Assn 11:727-31, 1974.
29.Delahanty, J. L. and Goldberg, I. L. An extraoral radiographictechnique: use of the lateral oblique jaw radiograph. GeneralDent 28:20-21, 1980.
30.Choukas, N. C. and Ireland, J. F. Panoramic survey of the hos-pitalized patient. Ill Dent Jour 36:719-22, 1967.
31.Hulburt, C. E. and Wuehrman, A. H. Compa~on of interproxi-mal carious lesion detection in panoramic and standard intraoralradiography. JADA 93:1154-58, 1976.
32.Ryan, J. B., Rosonberg, H. M. and Law, D. B. Evaluation of ahead poeitioner for panoramic radiography. J Dent Child 40:97-102, 1973.
33.Wall, B. F., Fisher, E. S., Paynter, R., Hudson, A., and Bi~d, P.D. Doses to patients from pantomographic and conventionaldental radiography. Brit J Radio152:727-34, 1979.
34.Myers, D. R., Shoal, H. K., Wege, W. R., Carlton, W. H., andGilbert, M. A. Radiation exposure during panoramic radiogra-phy in children. Oral Surg 48:588-93, 1978.Valachovic, R. W. and Lurie, A. G. Risk-benefit considerationsin pedodontic radiology. Pediatr Dent 2:128-148, 1980.
Stapff, K. H. Radiographic procedures for children using thestatus-X equipment. Quintessence Int 7:67-74, 1972.Rottke, B. Application of the Status-X in oral medicine.Erlangen, West Germany, Siemens Company, 1971.Lieberman, J. E. and Webber, R. L. Clinical evaluation of a pro-totype intraoral source X-ray system. Oral Surg 46:318-27, 1978.Hielscher, W. Indications, production and interpretation of pan-oramic radiographs with the status-X Urdt. Erlangen, West Ger-many, Siemens Company, 1968.
40.Webber, R. L., Schuette, W. H., and Whitehouse, W. C. An alter-native approach to dose reduction in dental radiography. OralSurg 40:553-63, 1975.
41.Waldman, H. B. Dental radiography for the homebound. J PubHeal Dent 28:32-34, 1968.
42.Macrae, P. D., Bodnarchuk, A., Castaldi, C. R., and Zacherl, W.A. Detection of congenital dental anomalies, how many films? JDent Child 35:107-114, 1968.King, N. M. and Shaw, L. Value of bitewing radiographs in de-tection of occlusal caries. Comm Dent Oral Epi 7(4):218-221,1979.Alnamo, J. and Tammisalo, E. H. Comparison of radiographicand clinical s~gns of early periodontal dise~. Scand J Dent Res81:548-52, 1973.Lang, N. P. and Hill, R. W. Radiography in periodontics. J ClinPerio 4(1):16-28, 1977.
36.
37.
38.
39.
44.
45.
454 SPECIAL PATIENT CONSIDERATIONS: Casamassimo