Embed Size (px)
Citation preview

AMERICAN ACADEMY OF PEDIATRICS
AMERICAN HEART ASSOCIATION
ENDORSED CLINICAL REPORTGuidance for the Clinician in Rendering Pediatric Care
Jane W. Newburger, MD, MPH; Masato Takahashi, MD; Michael A. Gerber, MD; Michael H. Gewitz, MD;Lloyd Y. Tani, MD; Jane C. Burns, MD; Stanford T. Shulman, MD; Ann F. Bolger, MD;
Patricia Ferrieri, MD; Robert S. Baltimore, MD; Walter R. Wilson, MD; Larry M. Baddour, MD;Matthew E. Levison, MD; Thomas J. Pallasch, DDS; Donald A. Falace, DMD; and Kathryn A. Taubert, PhD
Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease:A Statement for Health Professionals From the Committee on Rheumatic
Fever, Endocarditis, and Kawasaki Disease, Council on CardiovascularDisease in the Young, American Heart Association
ABSTRACT. Background. Kawasaki disease is anacute self-limited vasculitis of childhood that is charac-terized by fever, bilateral nonexudative conjunctivitis,erythema of the lips and oral mucosa, changes in theextremities, rash, and cervical lymphadenopathy. Coro-nary artery aneurysms or ectasia develop in �15% to 25%of untreated children and may lead to ischemic heartdisease or sudden death.
Methods and Results. A multidisciplinary committeeof experts was convened to revise the American HeartAssociation recommendations for diagnosis, treatment,and long-term management of Kawasaki disease. Thewriting group proposes a new algorithm to aid cliniciansin deciding which children with fever for >5 days and<4 classic criteria should undergo electrocardiography,receive intravenous gamma globulin (IVIG) treatment, orboth for Kawasaki disease. The writing group reviewsthe available data regarding the initial treatment for chil-dren with acute Kawasaki disease, as well for those whohave persistent or recrudescent fever despite initial ther-apy with IVIG, including IVIG retreatment and treat-ment with corticosteroids, tumor necrosis factor-� antag-onists, and abciximab. Long-term management ofpatients with Kawasaki disease is tailored to the degreeof coronary involvement; recommendations regardingantiplatelet and anticoagulant therapy, physical activity,follow-up assessment, and the appropriate diagnosticprocedures to evaluate cardiac disease are classified ac-cording to risk strata.
Conclusions. Recommendations for the initial evalu-ation, treatment in the acute phase, and long-term man-agement of patients with Kawasaki disease are intendedto assist physicians in understanding the range of accept-able approaches for caring for patients with Kawasakidisease. The ultimate decisions for case management
must be made by physicians in light of the particularconditions presented by individual patients. Pediatrics2004;114:1708–1733; AHA Scientific Statements, vasculitis,therapy, aneurysm, diagnosis.
ABBREVIATIONS. MI, myocardial infarction; CI, confidenceinterval; Ig, immunoglobulin; TNF-�, tumor necrosis actor-�; 2D,2-dimensional; 2DE, 2-dimensional echocardiography; IVIG, intra-venous immunoglobulin; ESR, erythrocyte sedimentation rate;CRP, C-reactive protein; LV, left ventricular; RCA, right coronaryartery; LAD, left anterior descending coronary artery; LMCA, leftmain coronary artery; LCX, left circumflex coronary artery; IVUS,intravascular ultrasound; MRA, magnetic resonance angiography;CT, computed tomography; MRI, magnetic resonance imaging; IL,interleukin; INR, international normalized ratio; tPA, tissue plas-minogen activator; ECG, electrocardiogram.
Kawasaki disease is an acute, self-limited vas-culitis of unknown etiology that occurs pre-dominantly in infants and young children.
First described in Japan in l967 by Tomisaku Ka-wasaki, the disease is now known to occur in bothendemic and community-wide epidemic forms in theAmericas, Europe, and Asia in children of all races.1Kawasaki disease is characterized by fever, bilateralnonexudative conjunctivitis, erythema of the lips andoral mucosa, changes in the extremities, rash, andcervical lymphadenopathy. Coronary artery aneu-rysms or ectasia develop in �15% to 25% of un-treated children with the disease and may lead tomyocardial infarction (MI), sudden death, or isch-emic heart disease.2,3 In the United States, Kawasakidisease has surpassed acute rheumatic fever as theleading cause of acquired heart disease in children.4Treatment of Kawasaki disease in the acute phase isdirected at reducing inflammation in the coronaryartery wall and preventing coronary thrombosis,whereas long-term therapy in individuals who de-velop coronary aneurysms is aimed at preventingmyocardial ischemia or infarction.
A new feature of these recommendations is an
This report was approved by the American Heart Association ScienceAdvisory and Coordinating Committee on June 16, 2004.This report was copublished in the October 26, 2004 issue of Circulation.The guidance in this report does not indicate an exclusive course of treat-ment or serve as a standard of medical care. Variations, taking into accountindividual circumstances, may be appropriate.doi:10.1542/peds.2004-2182PEDIATRICS (ISSN 0031 4005). Copyright © 2004 by the American Acad-emy of Pediatrics.
1708 PEDIATRICS Vol. 114 No. 6 December 2004 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

algorithm for the evaluation and treatment of pa-tients in whom incomplete or atypical Kawasaki dis-ease is suspected (refer to “Criteria for Treatment ofKawasaki Disease” later in this statement and Fig 1).We attempt to summarize the current state of knowl-edge of the management of patients with Kawasakidisease. The recommendations are evidence based
and derived from published data wherever possible.The levels of evidence on which recommendationsare based are classified as follows: level A (highest),multiple randomized clinical trials; level B (interme-diate), limited number of randomized trials, nonran-domized studies, and observational registries; andlevel C (lowest), primarily expert consensus.
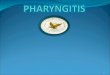
Fig 1. Evaluation of suspected incomplete Kawasaki disease. (1) In the absence of gold standard for diagnosis, this algorithm cannot beevidence based but rather represents the informed opinion of the expert committee. Consultation with an expert should be sought anytimeassistance is needed. (2) Infants �6 months old on day �7 of fever without other explanation should undergo laboratory testing and, ifevidence of systemic inflammation is found, an echocardiogram, even if the infants have no clinical criteria. (3) Patient characteristicssuggesting Kawasaki disease are listed in Table 1. Characteristics suggesting disease other than Kawasaki disease include exudativeconjunctivitis, exudative pharyngitis, discrete intraoral lesions, bullous or vesicular rash, or generalized adenopathy. Consider alternativediagnoses (see Table 2). (4) Supplemental laboratory criteria include albumin �3.0 g/dL, anemia for age, elevation of alanine amino-transferase, platelets after 7 days �450 000/mm3, white blood cell count �15 000/mm3, and urine �10 white blood cells/high-powerfield. (5) Can treat before performing echocardiogram. (6) Echocardiogram is considered positive for purposes of this algorithm if any of3 conditions are met: z score of LAD or RCA �2.5, coronary arteries meet Japanese Ministry of Health criteria for aneurysms, or �3 othersuggestive features exist, including perivascular brightness, lack of tapering, decreased LV function, mitral regurgitation, pericardialeffusion, or z scores in LAD or RCA of 2–2.5. (7) If the echocardiogram is positive, treatment should be given to children within 10 daysof fever onset and those beyond day 10 with clinical and laboratory signs (CRP, ESR) of ongoing inflammation. (8) Typical peeling beginsunder nail bed of fingers and then toes.
AMERICAN ACADEMY OF PEDIATRICS 1709 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

Recommendations for initial evaluation, treatmentin the acute phase, and long-term management ofpatients with Kawasaki disease are intended to assistphysicians in understanding the range of acceptableapproaches for caring for patients with Kawasakidisease. Where published data do not define well thebest medical practices, our report provides practicalinterim recommendations. Ultimately, managementdecisions must be individualized to a patient’s spe-cific circumstances.
EPIDEMIOLOGYIn the past, Kawasaki disease may have masquer-
aded as other illnesses, and old reports on infantilepolyarteritis nodosa describe pathological findingsthat are identical to those of fatal Kawasaki dis-ease.5–8 Kawasaki disease is markedly more preva-lent in Japan and in children of Japanese ancestry,with an annual incidence of �112 cases per 100 000children �5 years old.9 In the United States, theincidence of Kawasaki disease has been best esti-mated from hospital discharge data.10,11 An esti-mated 4248 hospitalizations associated with Ka-wasaki disease occurred in the United States in 2000,with a median age of 2 years.10 Race-specific inci-dence rates derived from administrative data indi-cate that Kawasaki disease is most common amongAmericans of Asian and Pacific Island descent (32.5/100 000 children �5 years old), intermediate in non-Hispanic African Americans (16.9/100 000 children�5 years old) and Hispanics (11.1/100 000 children�5 years old), and lowest in whites (9.1/100 000children �5 years old).10 These estimates are similarto those reported in smaller studies.12,13 Recent re-ports have emphasized the occurrence of Kawasakidisease in older children, who may have a higherprevalence of cardiovascular complications relatedto late diagnosis.14–16
Rates of recurrence and familial occurrence of Ka-wasaki disease are best documented in the literaturefrom Japan; these rates may be lower in other racesand ethnicities. In Japan, the recurrence rate of Ka-wasaki disease has been reported to be �3%.17 Theproportion of cases with a positive family history is�1%.17,18 Within 1 year after onset of the first case ina family, the rate in a sibling is 2.1%, which is arelative risk of �10-fold as compared with the unaf-fected Japanese population; �50% of the secondcases develop within 10 days of the first case.19 Therisk of occurrence in twins is �13%.19,20 Higher ratesof Kawasaki disease in the siblings of index cases andtwins suggest a possible role for genetic predisposi-tion that interacts with exposure to the etiologicagent or agents in the environment.19–22 The reportedoccurrence of Kawasaki disease in children of par-ents who themselves had the illness in childhoodalso supports the contribution of genetic factors.23–26
In the United States, Kawasaki disease is morecommon during the winter and early spring months;boys outnumber girls by �1.5 to 1.7:1; and 76% ofchildren are �5 years old.10,11 Reported associationsof Kawasaki disease with antecedent respiratory ill-ness and exposure to carpet-cleaning fluids have notbeen consistently confirmed.12,13,27–30 Other factors
that are reportedly associated with Kawasaki diseaseinclude having preexisting eczema,31 using a humid-ifier,30 and living near a standing body of water.32
The case fatality rate in Kawasaki disease in Japanis 0.08%.17 The standardized mortality ratio (the ob-served number of deaths divided by the expectednumber of deaths based on vital statistics in Japan) inpatients diagnosed between 1982 and 1992 was 1.25(95% confidence interval [CI]: 0.84–1.85) overall and2.35 (95% CI: 0.96–5.19) for boys with cardiac sequel-ae.33 In the United States, the in-hospital mortalityrate is �0.17% (the investigators used administrativedata that may include readmissions for coronary dis-ease).15 Virtually all deaths in patients with Ka-wasaki disease result from its cardiac sequelae.34 Thepeak mortality occurs 15 to 45 days after the onset offever; during this time well-established coronaryvasculitis occurs concomitantly with a marked ele-vation of the platelet count and a hypercoagulablestate.35 However, sudden death from MI may occurmany years later in individuals who as children hadcoronary artery aneurysms and stenoses. Many casesof fatal and nonfatal MI in young adults have beenattributed to “missed” Kawasaki disease in child-hood.36
ETIOLOGY AND PATHOGENESISThe etiology of Kawasaki disease remains un-
known, although clinical and epidemiological fea-tures strongly suggest an infectious cause. A self-limited, generally nonrecurring illness that manifestsitself by fever, rash, enanthem, conjunctival injection,and cervical adenopathy fits well with an infectiousetiology or trigger. The epidemiological featuresnoted above, including age distribution, winter-spring seasonality, occurrence of community out-breaks with wave-like geographic spread, and ap-parent epidemic cycles, are suggestive of atransmissible childhood disease. The laboratory fea-tures also suggest infection. However, efforts to iden-tify an infectious agent in Kawasaki disease withconventional bacterial and viral cultures and serolog-ical methods, as well as with animal inoculation,have failed to identify an infectious cause.
An attractive hypothesis is that Kawasaki diseaseis caused by a ubiquitous infectious agent that pro-duces clinically apparent disease only in certain ge-netically predisposed individuals, particularlyAsians. Its rarity in the first few months of life and inadults suggests an agent to which the latter are im-mune and from which very young infants are pro-tected by passive maternal antibodies. Because littleevidence exists of person-to-person transmission,this hypothesis assumes that most infected childrenexperience asymptomatic infection with only a smallfraction developing overt clinical features of Ka-wasaki disease. The genetic basis of susceptibility iscurrently unknown.
The hypothesis that Kawasaki disease is related toa bacterial superantigenic toxin has been suggestedbecause of the reported selective expansion of V�2and V�8 T-cell receptor families, but this theory re-mains controversial.37–40 A recent prospective multi-center study failed to show a significant difference in
1710 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

the prevalence of toxin-producing strains betweenpatients with Kawasaki disease and febrile con-trols.41 Recent investigations support an alternativehypothesis: The immune response in Kawasaki dis-ease is oligoclonal (antigen driven, ie, similar to aresponse to a conventional antigen) rather than poly-clonal (as found typically in superantigen-driven re-sponses), and immunoglobulin A (IgA) plasma cellsplay a central role.42–44
It also is possible that Kawasaki disease resultsfrom an immunologic response that is triggered byany of several different microbial agents. Support forthis hypothesis includes documented infection bydifferent microorganisms in different individualcases, failure to detect a single microbiological orenvironmental agent after almost 3 decades of study,and analogies to other syndromes caused by multi-ple agents (eg, aseptic meningitis). This hypothesis issomewhat difficult to reconcile with the distinctiveclinical/laboratory picture of Kawasaki disease andwith its epidemiological features, however.
Efforts to associate Kawasaki disease with expo-sure to drugs or to such environmental pollutants astoxins, pesticides, chemicals, and heavy metals havefailed, although clinical similarities between Ka-wasaki disease and acrodynia (mercury hypersensi-tivity) are notable.
Striking immune perturbations occur in acute Ka-wasaki disease, including marked cytokine cascadestimulation and endothelial cell activation. The keysteps leading to coronary arteritis are still being clar-ified, but endothelial cell activation, CD68� mono-cyte/macrophages, CD8� (cytotoxic) lymphocytes,and oligoclonal IgA plasma cells appear to be in-volved.43,45 The prominence of IgA plasma cells inthe respiratory tract, which is similar to findings infatal viral respiratory infections, suggests a respira-tory portal of entry of an etiologic agent or agents.44
Enzymes including matrix metalloproteinases thatare capable of damaging arterial wall integrity maybe important in the development of aneurysmal di-latation.46 Vascular endothelial growth factor(VEGF), monocyte chemotactic and activating factor(MCAF or MCP-1), tumor necrosis actor-� (TNF-�),and various interleukins also appear to play impor-tant roles in the vasculitic process.47–54
PATHOLOGYAlthough the coronary arteries virtually always
are involved in autopsy cases, Kawasaki disease is ageneralized systemic vasculitis involving blood ves-sels throughout the body. Aneurysms may occur inother extraparenchymal muscular arteries such asthe celiac, mesenteric, femoral, iliac, renal, axillary,and brachial arteries.55 The early stages in the forma-tion and development of arteritis in Kawasaki dis-ease have been well studied morphologically in rel-atively large muscular arteries.55 The media ofaffected vessels demonstrate edematous dissociationof the smooth muscle cells, which is most obvioustoward the exterior. Endothelial cell swelling andsubendothelial edema are seen, but the internal elas-tic lamina remains intact. An influx of neutrophils isfound in the early stages (7–9 days after onset), with
a rapid transition to large mononuclear cells in con-cert with lymphocytes (predominantly CD8� T cells)and IgA plasma cells.42–45 Destruction of the internalelastic lamina and eventually fibroblastic prolifera-tion occur at this stage. Matrix metalloproteinasesare prominent in the remodeling process.56 Activeinflammation is replaced over several weeks tomonths by progressive fibrosis, with scar formation.
Arterial remodeling or revascularization may oc-cur in Kawasaki disease with coronary arteritis. Pro-gressive stenosis in the disease results from activeremodeling with intimal proliferation and neoangio-genesis; the intima is markedly thickened and con-sists of linearly arranged microvessels, a layer that isrich in smooth muscle cells, and fibrous layers. Sev-eral growth factors are prominently expressed at theinlet and outlet of aneurysms, where they are acti-vated by high shear stress.57
During the clinical course of Kawasaki disease,vomiting and abdominal pain are seen often.Kurashige and colleagues58 described the intestinaltract in 31 fatal cases, but in only 3 patients wasmesenteric arteritis found. Using biopsy specimensof the jejunal mucosa, Nagata et al59 studied cellsurface phenotypes of mononuclear cells and entero-cytes. Both HLA-DR�CD3� (activated T cells) andDR�CD4� cells (activated helper T cells) were sig-nificantly increased in the lamina propria of patientswith acute Kawasaki disease as compared with con-trols. In contrast, CD8� cells (suppressor/cytotoxic Tcells) were significantly reduced in both the epithe-lium and the lamina propria of individuals withKawasaki disease as compared with controls. Duringthe convalescent phase of the disease, these cell pat-terns returned to normal.59 Hydrops of the gallblad-der may be clinically apparent in patients with Ka-wasaki disease. A study of surgically removedgallbladders revealed a nonspecific severe perivas-cular inflammatory cell infiltration60; distinct arteritisin the gallbladder wall has not been well docu-mented.
Lymphadenopathy, an early finding in patientswith Kawasaki disease, usually disappears by au-topsy. Pathological findings in lymph nodes includethrombotic arteriolitis and severe lymphadenitiswith necrosis.55 Lymph node biopsies performed inthe first week of the illness revealed abnormal hy-perplasia of the endothelium of the postcapillaryvenule and hyperplasia of reticular cells around thepostcapillary venule.1
DIAGNOSISIn the absence of a specific diagnostic test or pa-
thognomonic clinical feature, clinical criteria havebeen established to assist physicians in diagnosingKawasaki disease. Other clinical and laboratory find-ings observed in patients with this disease are fre-quently helpful in diagnosis. Table 1 describes theclinical and laboratory features of Kawasaki diseaseaccording to the epidemiological case definition.
Principal Clinical FindingsThe classic diagnosis of Kawasaki disease has been
based on the presence of �5 days of fever and �4 of
AMERICAN ACADEMY OF PEDIATRICS 1711 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

the 5 principal clinical features (see Table 1).3 Typi-cally, all of the clinical features are not present at asingle point in time, and watchful waiting is some-times necessary before a diagnosis can be made.Patients with fever for �5 days and �4 principalfeatures can be diagnosed as having Kawasaki dis-ease when coronary artery disease is detected by2-dimensional (2D) echocardiography (2DE) or cor-
onary angiography. In the presence of �4 principalcriteria, the diagnosis of Kawasaki disease can bemade on day 4 of illness. Kawasaki disease should beconsidered in the differential diagnosis of a youngchild with unexplained fever for �5 days that isassociated with any of the principal clinical featuresof this disease.
The fever typically is high-spiking and remittent,with peak temperatures generally �39°C (102°F) andin many cases �40°C (104°F). In the absence of ap-propriate therapy, fever persists for a mean of 11days, but it may continue for 3 to 4 weeks and, rarely,even longer. With appropriate therapy, the feverusually resolves within 2 days.
Changes in the extremities are distinctive. Ery-thema of the palms and soles or firm, sometimespainful induration of the hands or feet, or both ery-thema and induration often occur in the acute phaseof the disease. Desquamation of the fingers and toesusually begins in the periungual region within 2 to 3weeks after the onset of fever and may extend toinclude the palms and soles. Approximately 1 to 2months after the onset of fever, deep transversegrooves across the nails (Beau’s lines) may appear.
An erythematous rash usually appears within 5days of the onset of fever. The rash may take variousforms; the most common is a nonspecific, diffusemaculopapular eruption. Occasionally seen are anurticarial exanthem, a scarlatiniform rash, an eryth-roderma, an erythema-multiforme-like rash, or,rarely, a fine micropustular eruption. Bullous andvesicular eruptions have not been described. Therash usually is extensive, with involvement of thetrunk and extremities and accentuation in the peri-neal region, where early desquamation may occur.
Bilateral conjunctival injection usually beginsshortly after the onset of fever. It typically involvesthe bulbar conjunctivae (sparing the limbus, an avas-cular zone around the iris) much more often than thepalpebral or tarsal conjunctivae; is not associatedwith an exudate, conjunctival edema or corneal ul-ceration; and usually is painless. Mild acute iridocy-clitis or anterior uveitis may be noted by slit lamp; itresolves rapidly and rarely is associated with photo-phobia or eye pain.
Changes of the lips and oral cavity include (1)erythema, dryness, fissuring, peeling, cracking, andbleeding of the lips; (2) a “strawberry tongue” that isindistinguishable from that associated with strepto-coccal scarlet fever, with erythema and prominentfungiform papillae; and (3) diffuse erythema of theoropharyngeal mucosae. Oral ulcerations and pha-ryngeal exudates are not seen.
Cervical lymphadenopathy is the least common ofthe principal clinical features. It is usually unilateraland confined to the anterior cervical triangle, and itsclassic criteria include �1 lymph node that is �1.5cm in diameter. Imaging studies frequently demon-strate multiple enlarged nodes without suppura-tion.61 The lymph nodes often are firm and nonfluc-tuant, are not associated with marked erythema ofthe overlying skin, and are nontender or only slightlytender. Occasionally, the lymph node swelling of
TABLE 1. Clinical and Laboratory Features of Kawasaki Dis-ease
Epidemiological case definition (classic clinical criteria)*Fever persisting at least 5 days†Presence of at least 4 principal features:
Changes in extremitiesAcute: Erythema of palms, soles; edema of hands, feetSubacute: Periungual peeling of fingers, toes in weeks 2
and 3Polymorphous exanthemBilateral bulbar conjunctival injection without exudateChanges in lips and oral cavity: Erythema, lips cracking,
strawberry tongue, diffuse injection of oral andpharyngeal mucosae
Cervical lymphadenopathy (�1.5-cm diameter), usuallyunilateral
Exclusion of other diseases with similar findings‡Other clinical and laboratory findings
Cardiovascular findingsCongestive heart failure, myocarditis, pericarditis, valvular
regurgitationCoronary artery abnormalitiesAneurysms of medium-size noncoronary arteriesRaynaud’s phenomenonPeripheral gangrene
Musculoskeletal systemArthritis, arthralgia
Gastrointestinal tractDiarrhea, vomiting, abdominal painHepatic dysfunctionHydrops of gallbladder
Central nervous systemExtreme irritabilityAseptic meningitisSensorineural hearing loss
Genitourinary systemUrethritis/meatitis
Other findingsErythema, induration at BCG inoculation siteAnterior uveitis (mild)Desquamating rash in groin
Laboratory findings in acute Kawasaki diseaseLeukocytosis with neutrophilia and immature formsElevated ESRElevated CRPAnemiaAbnormal plasma lipidsHypoalbuminemiaHyponatremiaThrombocytosis after week 1§Sterile pyuriaElevated serum transaminasesElevated serum gamma glutamyl transpeptidasePleocytosis of cerebrospinal fluidLeukocytosis in synovial fluid
Patients with fever at least 5 days and �4 principal criteria can bediagnosed with Kawasaki disease when coronary artery abnor-malities are detected by 2DE or angiography.† In the presence of �4 principal criteria, Kawasaki disease diag-nosis can be made on day 4 of illness. Experienced clinicians whohave treated many Kawasaki disease patients may establish diag-nosis before day 4.‡ See Table 2.§ Some infants present with thrombocytopenia and disseminatedintravascular coagulation.
1712 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

Kawasaki disease can be confused with bacterial ad-enitis.
Because the principal clinical findings that fulfillthe diagnostic criteria are not specific, other diseaseswith similar clinical features should be excluded (Ta-ble 2).
Other Clinical and Laboratory Findings
Cardiac FindingsCardiovascular manifestations can be prominent
in the acute phase of Kawasaki disease and are theleading cause of long-term morbidity and mortality.During this phase, the pericardium, myocardium,endocardium, valves, and coronary arteries all maybe involved. Cardiac auscultation of the infant orchild with Kawasaki disease in the acute phase oftenreveals a hyperdynamic precordium, tachycardia, agallop rhythm, and an innocent flow murmur in thesetting of anemia, fever, and depressed myocardialcontractility secondary to myocarditis. Children withsignificant mitral regurgitation may have a pansys-tolic regurgitant murmur that is typical of this con-dition. Occasionally, patients with Kawasaki diseaseand poor myocardial function may present with lowcardiac output syndrome or shock. Electrocardiogra-phy may show arrhythmia, prolonged PR interval, ornonspecific ST and T wave changes.
Noncardiac FindingsMultiple noncardiac clinical findings may be ob-
served in patients with Kawasaki disease. Arthritisor arthralgia can occur in the first week of the illnessand tends to involve multiple joints, including thesmall interphalangeal joints as well as large weight-bearing joints. Arthritis or arthralgia developing af-ter the 10th day of illness favors large weight-bearingjoints, especially the knees and ankles.
Children with Kawasaki disease often are moreirritable than are children with other febrile illnesses.Transient unilateral peripheral facial nerve palsy oc-curs rarely. Transient high-frequency sensorineuralhearing loss (20–35 dB) can occur during acute Ka-wasaki disease,62,63 but persistent sensorineuralhearing loss is rare.64 Gastrointestinal complaints,including diarrhea, vomiting, and abdominal pain,occur in approximately one third of patients. Rarely,Kawasaki disease can present as an acute surgicalabdomen.65 Hepatic enlargement and jaundice canoccur. Acute acalculous distention of the gallbladder(hydrops) occurs in �15% of patients during the first
2 weeks of the illness and can be identified by ab-dominal ultrasound.60 Erythema and induration atthe site of a previous vaccination with BacilleCalmette-Guerin (BCG) is common in Japan, whereBCG is used widely.66 Rare findings include testicu-lar swelling, pulmonary nodules50 and infiltrates,67
pleural effusions, and hemophagocytic syndrome.68
Laboratory FindingsLeukocytosis is typical during the acute stage of
Kawasaki disease, with a predominance of immatureand mature granulocytes. Approximately 50% of pa-tients have white blood cell counts �15 000/mm3.Leukopenia is rare. Anemia may develop, usuallywith normal red blood cell indexes, particularly withmore prolonged duration of active inflammation. Se-vere hemolytic anemia requiring transfusions is rareand may be related to intravenous immunoglobulin(IVIG) infusion.69–72 Elevation of acute phase reac-tants, such as erythrocyte sedimentation rate (ESR)and C-reactive protein (CRP), is nearly universal inKawasaki disease, usually returning to normal by 6to 10 weeks after onset of the illness. Because thedegree of elevation of ESR and CRP may show adiscrepancy in some patients at the time of presen-tation, both should be measured.73 Furthermore, el-evation of ESR (but not of CRP) can be caused byIVIG therapy per se; therefore, ESR should not beused as the sole determinant of the degree of inflam-matory activity in IVIG-treated patients.
A characteristic feature of the later phases of theillness is thrombocytosis, with platelet counts rang-ing from 500 000 to �1 million/mm3. Thrombocyto-sis rarely is present in the first week of the illness,usually appears in the second week, and peaks in thethird week with a gradual return to normal by 4 to 8weeks after onset in uncomplicated cases. The meanpeak platelet count is �700 000/mm3. Thrombocyto-penia is seen rarely in the acute stage and may be asign of disseminated intravascular coagulation. Alow platelet count at illness presentation is a riskfactor for coronary aneurysms (see “Risk Scores forPredicting Aneurysms”). In patients with arthritis,arthrocentesis typically yields purulent-appearingfluid with a white blood cell count of 125 000 to300 000/mm3, a normal glucose level, and negativeGram stain and cultures.74 Plasma lipids are mark-edly altered in acute Kawasaki disease, with de-pressed plasma cholesterol, high-density lipoprotein(HDL), and apolipoprotein AI.75–78
Mild to moderate elevations in serum transami-nases occur in �40% of patients and mild hyperbil-irubinemia in �10%.79 Plasma gammaglutamyltranspeptidase is elevated in �67% of patients.80 Hy-poalbuminemia is common and is associated withmore severe and more prolonged acute disease. Uri-nalysis reveals intermittent mild to moderate sterilepyuria in �33% of patients, although suprapubicurine generally does not show pyuria, which sug-gests urethritis. In children who undergo lumbarpuncture, �50% demonstrate evidence of asepticmeningitis with a predominance of mononuclearcells, as well as normal glucose and protein levels.81
Elevation of serum cardiac troponin I, a marker
TABLE 2. Differential Diagnosis of Kawasaki Disease: Dis-eases and Disorders With Similar Clinical Findings
Viral infections (eg, measles, adenovirus, enterovirus, Epstein-Barr virus)
Scarlet feverStaphylococcal scalded skin syndromeToxic shock syndromeBacterial cervical lymphadenitisDrug hypersensitivity reactionsStevens-Johnson syndromeJuvenile rheumatoid arthritisRocky Mountain spotted feverLeptospirosisMercury hypersensitivity reaction (acrodynia)
AMERICAN ACADEMY OF PEDIATRICS 1713 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

that is specific for myocardial damage, has been re-ported in acute Kawasaki disease, which is consistentwith myocardial cell injury in the early phase of thedisease.82,83 Such elevation was not confirmed in an-other study.84 Troponin assays do not play a role inthe routine management of children with Kawasakidisease.
Laboratory tests, even though they are nonspecific,can provide diagnostic support in patients with clin-ical features that are suggestive but not diagnostic ofKawasaki disease. A moderately to markedly ele-vated CRP or ESR, which is almost universally seenin children with Kawasaki disease, is uncommonin viral infections. Platelet counts usually are�450 000/mm3 in patients evaluated after day 7 ofillness. Clinical experience suggests that Kawasakidisease is unlikely if platelet counts and acute-phaseinflammatory reactants (ie, ESR and CRP) are normalafter day 7 of illness. In addition, low white bloodcell count, lymphocyte predominance, and low plate-let count in the absence of disseminated intravascu-lar coagulation suggest a viral etiology.
Incomplete (Atypical) Kawasaki DiseaseSome patients who do not fulfill the criteria out-
lined in Table 1 have been diagnosed as having“incomplete” or “atypical” Kawasaki disease, a di-agnosis that often is based on echocardiographicfindings of coronary artery abnormalities. The term“incomplete” may be preferable to “atypical,” be-cause these patients lack sufficient clinical signs ofthe disease to fulfill the classic criteria; they do notdemonstrate atypical clinical features. The phrase“atypical Kawasaki disease” should be reserved forpatients who have a problem, such as renal impair-ment, that generally is not seen in Kawasaki disease.The conventional diagnostic criteria should beviewed as guidelines that are particularly useful inpreventing overdiagnosis but may result in failure torecognize incomplete forms of illness. IncompleteKawasaki disease is more common in young infantsthan in older children, making accurate diagnosisand timely treatment especially important in theseyoung patients who are at substantial risk of devel-oping coronary abnormalities.85 The laboratory find-ings of incomplete cases appear to be similar to thoseof classic cases. Therefore, although laboratory find-ings in Kawasaki disease are nondiagnostic, theymay prove useful in heightening or reducing thesuspicion of incomplete Kawasaki disease.
Echocardiography also may be useful in evaluat-ing children with protracted fever and some featuresof Kawasaki disease. Although aneurysms rarelyform before day 10 of illness, perivascular bright-ness, ectasia, and lack of tapering of the coronaryarteries in the acute stage of Kawasaki disease mayrepresent coronary arteritis before the formation ofaneurysms. Decreased left ventricular (LV) contrac-tility, mild valvular regurgitation (most commonlymitral regurgitation), and pericardial effusion alsomay be seen in an echocardiogram of a person withacute Kawasaki disease.
Incomplete Kawasaki disease should be consid-ered in all children with unexplained fever for �5
days associated with 2 or 3 of the principal clinicalfeatures of Kawasaki disease (see “Criteria for Treat-ment of Kawasaki Disease” and Fig 1). Becauseyoung infants may present with fever and few, ifany, principal clinical features, echocardiographyshould be considered in any infant aged �6 monthswith fever of �7 days’ duration, laboratory evidenceof systemic inflammation, and no other explanationfor the febrile illness.
Common Pitfalls in DiagnosisCertain common pitfalls in the diagnosis of Ka-
wasaki disease should be noted. Children maypresent with only fever and a unilateral enlargedcervical lymph node. The rash and mucosal changesthat follow often are mistaken for a reaction to anti-biotics that are administered for presumed bacteriallymphadenitis. Sterile pyuria may be mistaken for apartially treated urinary tract infection with sterileurine cultures. The young infant may present withfever, rash, and cerebrospinal fluid pleocytosis andbe misdiagnosed with viral meningitis. Occasionally,a child may present with an acute abdomen and beadmitted to a surgical service. Kawasaki diseaseshould be considered in the differential diagnosis ofevery child with fever of at least several days’ dura-tion, rash, and nonpurulent conjunctivitis, especiallyin children �1 year old and in adolescents, in whomthe diagnosis is frequently missed.
Risk Scores for Predicting AneurysmsSeveral scoring systems have been developed to
identify children at highest risk for coronary arteryabnormalities.86–89 Duration of fever, presumably re-flecting the severity of ongoing vasculitis, has beenconfirmed as a powerful predictor of coronary arteryaneurysms in various studies.87–89 Harada et al90,91
developed a risk score to use at the time a childpresents with Kawasaki disease to determine the riskof future coronary aneurysms. At some centers inJapan, the Harada score is used to determinewhether IVIG treatment will be used. Intravenousgamma globulin is given to children who fulfill 4 ofthe following criteria, assessed within 9 days of onsetof illness: (1) white blood cell count �12 000/mm3;(2) platelet count �350 000/mm3; (3) CRP �3�; (4)hematocrit �35%; (5) albumin �3.5 g/dL; (6) age�12 months; and (7) male sex. For children with �4risk factors but continuing acute symptoms, the riskscore is reassessed daily. In North America, whereIVIG is recommended for all children with Kawasakidisease, Beiser et al92 constructed a predictive instru-ment for the development of coronary artery lesionsamong patients treated with high-dose IVIG withinthe first 10 days of the onset of illness using datafrom a US multicenter database of patients withacute Kawasaki disease. The risk factors that Beiserand associates used in the sequential classificationinstrument included baseline neutrophil and bandcounts, hemoglobin concentration, platelet count,and temperature on the day after IVIG infusion. Thisinstrument allowed the clinician to identify within 1day of treatment the low-risk children in whom ex-tensive and frequent cardiac testing may be unnec-
1714 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

essary. Its positive predictive value was less satisfac-tory, however; the frequencies of the development ofcoronary artery abnormalities in boys and girls whowere classified as high risk were only 13.8% and5.5%, respectively. Because of the imperfect perfor-mance of scoring systems, all patients who are diag-nosed with Kawasaki disease should be treated withIVIG.
Criteria for Treatment of Kawasaki DiseaseThe original guidelines for the diagnosis of Ka-
wasaki disease were created by a committee that wasappointed by the Japanese Ministry of Health in1970. At that time, the coronary artery complicationsof Kawasaki disease were not yet appreciated. Inaddition, neither effective treatment nor a noninva-sive method of assessing coronary artery abnormal-ities existed. The case definition was created, there-fore, for epidemiological surveillance and toestablish the extent of the clinical syndrome nowknown as Kawasaki disease in Japan. The case defi-nition intentionally was made restrictive to excludepatients with rheumatic fever and Stevens-Johnsonsyndrome.
More than 3 decades later, the clinical landscapehas changed dramatically. Echocardiographicscreening for coronary enlargement has shown that asubstantial number of children with Kawasaki dis-ease and coronary artery abnormalities are not iden-tified by the classic case definition.93–95 Thus, al-though the present case definition provides a specifictool for epidemiological surveillance, it may not bethe optimal method for aiding clinicians in the rec-ognition of children with a systemic vasculitis thatrequires prompt treatment. Given the potential seri-ousness of the complications, together with the effi-cacy and safety of early treatment, high sensitivity ofthe treatment criteria is more important than is highspecificity. We have therefore devised an algorithmto aid clinicians in deciding whether a child withsigns and symptoms suggestive of Kawasaki diseaseshould be treated with IVIG. To strive for the great-est sensitivity while maintaining sufficient specificityto prevent widescale overuse of IVIG, we have at-tempted to base our recommendations on laboratoryand echocardiographic data derived from the popu-lation of patients with Kawasaki disease who meetthe classic epidemiological case definition.
The 1993 American Heart Association guidelineson Kawasaki disease suggested that the diagnosiscould be made on day 4 of fever, with day 1 byconvention being the first day of fever.3 In the pres-ence of 4 of 5 classic criteria (Table 1), US and Japa-nese experts agree that only 4 days of fever arenecessary before initiating treatment.
It is also broadly agreed that Kawasaki disease canbe diagnosed in the absence of full criteria whencoronary abnormalities are present. The definition ofcoronary artery abnormalities has changed since theoriginal Japanese Ministry of Health criteria weredevised. In particular, coronary artery dimensions,adjusted for body surface area, provide a more accu-rate assessment of the size of the proximal rightcoronary artery (RCA) or left anterior descending
coronary artery (LAD) as compared with expectedpopulation norms.96,97 A z score �2.5 (ie, a coronarydimension that is �2.5 SDs above the mean for bodysurface area) in 1 of these arterial segments would beexpected to occur in �0.6% of the population with-out Kawasaki disease, and a z score �3.0 in 1 of thesesegments would be expected to occur in �0.1% of thepopulation without Kawasaki disease. Having a cor-onary artery z score �2.5 in both the proximal RCAand LAD would be uncommon in the general pop-ulation. Because of anatomic variation in the leftmain coronary artery (LMCA), its z score must beinterpreted with caution. Occasional cases of coro-nary prominence in patients with other disordershave been noted. Clinical experience, however, sug-gests that coronary enlargement in other febrile ill-nesses is rare, whereas coronary enlargement in Ka-wasaki disease is relatively common. Thus, coronaryartery z scores should be incorporated into the rec-ommendations for the evaluation and treatment ofKawasaki disease.
The present writing group proposes a scheme toaid the clinician in deciding which patients withfever and �4 classic criteria should undergo echo-cardiography or receive IVIG treatment or both forKawasaki disease (Fig 1). In the absence of a goldstandard for diagnosis, this algorithm cannot be ev-idence based but rather represents the informedopinion of a committee of experts (evidence level C).We offer this opinion as guidance to clinicians untilan evidence-based algorithm or a specific diagnostictest for Kawasaki disease becomes available.
CARDIAC FINDINGS
Coronary Aneurysms
EchocardiographyThe major sequelae of Kawasaki disease are re-
lated to the cardiovascular and, more specifically, thecoronary arterial system, so cardiac imaging is acritical part of the evaluation of all patients withsuspected Kawasaki disease. Because it is noninva-sive and has a high sensitivity and specificity for thedetection of abnormalities of the proximal LMCAand RCA, echocardiography is the ideal imagingmodality for cardiac assessment (evidence level C).Evaluation of the cardiovascular sequelae of Ka-wasaki disease requires serial cardiac ultrasoundstudies and should be performed using equipmentwith appropriate transducers and supervised by anexperienced echocardiographer. The initial echocar-diogram should be performed as soon as the diag-nosis is suspected, but initiation of treatment shouldnot be delayed by the timing of the study (ie, waitingfor sedation). This initial study establishes a baselinefor longitudinal follow-up of coronary artery mor-phology, LV and left valvular function, and the evo-lution and resolution of pericardial effusion whenpresent. Because detailed echocardiographic imag-ing is compromised if a child is uncooperative, seda-tion often is required for younger children (eg, chlo-ral hydrate 65–100 mg/kg, maximum 1000 mg, orother short-acting sedative or hypnotic agents).
The 2D imaging should be performed with the
AMERICAN ACADEMY OF PEDIATRICS 1715 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

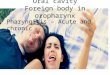
highest-frequency transducer possible. Imaging withhigh-frequency transducers should be attemptedeven in older children, because these probes allowfor higher-resolution, detailed evaluation of the cor-onary arteries. Studies should be recorded in a dy-namic video or digital cine format, because the nor-mal translational movement of the heart facilitatesthe display of the coronary artery anatomy. Suchrecordings will allow future review and comparisonwith subsequent studies. In addition to standard im-aging from parasternal, apical, subcostal, and su-prasternal notch windows, 2DE evaluation of pa-tients with suspected Kawasaki disease should focuson imaging the LMCA, LAD, left circumflex coro-nary artery (LCX), RCA (proximal, middle, and dis-tal segments), and posterior descending coronary ar-teries. Multiple imaging planes and transducerpositions are required for the optimal visualizationof all major coronary segments (Table 3, Fig 2). Max-imal efforts should be made to visualize all majorcoronary segments. In order of highest to lowestfrequency, common sites of coronary aneurysms in-clude the proximal LAD and proximal RCA, fol-lowed by the LMCA, then LCX, and finally the distalRCA and the junction between the RCA and poste-rior descending coronary artery.
Evaluation of the coronary arteries should includequantitative assessment of the internal vessel diam-eters. Measurements should be made from inneredge to inner edge and should exclude points ofbranching, which may have normal focal dilation.The number and location of aneurysms and the pres-ence or absence of intraluminal thrombi also shouldbe assessed. Aneurysms are classified as saccular ifaxial and lateral diameters are nearly equal or asfusiform if symmetric dilatation with gradual proxi-mal and distal tapering is seen. When a coronaryartery is larger than normal (dilated) without a seg-mental aneurysm, the vessel is considered ectatic.Care must be taken in making the diagnosis of ecta-sia because of considerable normal variation in cor-onary artery distribution and dominance. In the last
American Heart Association statement,3,98 aneu-rysms were classified as small (�5-mm internal di-ameter), medium (5- to 8-mm internal diameter), orgiant (�8-mm internal diameter). The Japanese Min-istry of Health criteria classify coronary arteries asabnormal if the internal lumen diameter is �3 mm inchildren �5 years old or �4 mm in children �5 yearsold; if the internal diameter of a segment measures�1.5 times that of an adjacent segment; or if thecoronary lumen is clearly irregular.99 Current statis-tics on the prevalence of coronary artery abnormali-ties secondary to Kawasaki disease are based onthese criteria. Although the Japanese Ministry ofHealth criteria are not based on an individual pa-tient’s body size, coronary artery dimensions in chil-dren without Kawasaki disease have been shown toincrease with indexes of body size, such as bodysurface area or body length.
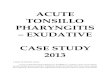
More recently, de Zorzi and colleagues96 showedthat the body surface area–adjusted coronary dimen-sions of some people with Kawasaki disease whosecoronary arteries were considered “normal” arelarger than expected in the acute, convalescent, andlate phases when compared with references estab-lished for body size. Figure 3 shows coronary inter-nal diameters according to body surface area in thepopulation without Kawasaki disease. Because useof the Japanese Ministry of Health criteria may resultin both underdiagnosis and underestimation of thetrue prevalence of coronary dilation, coronary vesselmeasurements adjusted for body surface area shouldbe compared with those of the population withoutKawasaki disease. Of note, z scores are available foronly the LMCA, proximal LAD, and proximal RCA,so that the Japanese Ministry of Health criterion of“size 1.5 times that of the surrounding segment” isstill useful for diagnosing aneurysms in peripheralsites. Enlargement of the LMCA caused by Kawasakidisease does not involve the orifice and rarely occurswithout associated ectasia of the LAD, LCX, or botharteries. In addition to measuring coronary arterydimensions, imaging the coronary arteries also mayreveal the lack of normal tapering and perivascularechogenicity or “brightness.”23
Although the echocardiographic examination ofpatients with Kawasaki disease is focused on thecoronary arteries, other information can and shouldbe obtained. Histological evidence suggests thatmyocarditis is universal in acute Kawasaki disease,and other studies have shown depressed ventricularcontractility to be common early in the course ofKawasaki disease. Therefore, assessment of LV func-tion should be a part of the echocardiographic eval-uation of all patients with suspected Kawasaki dis-ease. LV end-diastolic and end-systolic dimensionsand a shortening fraction should be measured fromstandard M-mode tracings. Apical imaging allowsthe estimation of LV end-diastolic and end-systolicvolumes and an ejection fraction. Although loadingconditions influence these measurements, they aremore readily measured than are complex indexes ofcontractility and are adequate for routine clinicalfollow-up. Evaluating regional wall motion may beuseful, especially in children with coronary artery
TABLE 3. Echocardiographic Views of Coronary Arteries inPatients With Kawasaki Disease
LMCA: Precordial short axis at level of aortic valve; precordiallong axis of left ventricle (superior tangential); subcostal LVlong axis
LAD: Precordial short axis at level of aortic valve; precordialsuperior tangential long axis of left ventricle; precordial shortaxis of left ventricle
Left circumflex: Precordial short axis at level of aortic valve;apical 4-chamber
RCA, proximal segment: Precordial short axis at level of aorticvalve; precordial long axis (inferior tangential) of leftventricle; subcostal coronal projection of right ventricularoutflow tract; subcostal short axis at level of atrioventriculargroove
RCA, middle segment: Precordial long axis of left ventricle(inferior tangential); apical 4-chamber; subcostal LV long axis;subcostal short axis at level of atrioventricular groove
RCA, distal segment: Apical 4-chamber (inferior); subcostalatrial long axis (inferior)
Posterior descending coronary artery: Apical 4-chamber(inferior); subcostal atrial long axis (inferior); precordial longaxis (inferior tangential) imaging posterior interventriculargroove
1716 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

abnormalities. The aortic root also should be imaged,measured, and compared with references for bodysurface area because evidence exists that mild aorticroot dilation is common among patients with Ka-wasaki disease.100 Because pericarditis may be asso-ciated with the vasculitis and myocarditis seen inpatients with Kawasaki disease, the presence or ab-sence of a pericardial effusion should be noted.
Standard pulsed and color flow Doppler interro-gation should be performed to assess the presenceand degree of valvular regurgitation (in particularfor mitral and aortic valves). Color flow Dopplerwith a low Nyquist limit setting from a favorableangle of view may allow coronary flow to be dem-onstrated and may be useful in positively identifyingcoronary artery lumens.
It is important to recognize the limitations of echo-cardiography in the evaluation and follow-up of pa-tients with Kawasaki disease. Although echocardio-graphic detection of thrombi and coronary arterystenosis has been reported, the sensitivity and spec-ificity of echocardiography for identifying these ab-normalities is unclear. In addition, the visualizationof coronary arteries becomes progressively more dif-ficult as a child grows and body size increases. An-giography, intravascular ultrasound (IVUS), trans-esophageal echocardiography, and other modalitiesincluding magnetic resonance angiography (MRA)and ultrafast computed tomography (CT) may be ofvalue in the assessment of selected patients (see be-low).
For uncomplicated cases, echocardiographic eval-uation should be performed at the time of diagnosis,at 2 weeks, and at 6 to 8 weeks after onset of thedisease. More frequent echocardiographic evaluationis needed to guide management in children at higherrisk (eg, those who are persistently febrile or who
exhibit coronary abnormalities, ventricular dysfunc-tion, pericardial effusion, or valvular regurgitation).Recent studies have shown that repeat echocardiog-raphy performed 1 year after the onset of the illnessis unlikely to reveal coronary artery enlargement inpatients whose echocardiographic findings werenormal at 4 to 8 weeks.101,102 Because abnormalitiesin coronary artery function,103–105 coronary flow re-serve,106 and aortic root dilation100 remain potentialconcerns even among patients in whom coronarydilatation was never detected, repeat echocardiogra-phy beyond 8 weeks in patients with previouslynormal findings should be considered optional. Fol-low-up echocardiograms should identify the pro-gression or regression of coronary abnormalities,evaluate ventricular and valvular function, and as-sess the presence or evolution of pericardial effu-sions.
Other Noninvasive TestsMagnetic resonance imaging (MRI) and MRA may
delineate coronary artery aneurysms in the proximalcoronary artery segments and provide data regard-ing flow profile (evidence level C).107–109 A recentsmall series in patients with Kawasaki disease dem-onstrated that coronary MRA accurately diagnosedall coronary artery aneurysms, coronary occlusions,and coronary stenoses present on x-ray angiogra-phy.110 MRI and MRA may be used to image periph-eral artery aneurysms. Ultrafast CT also has beenused to assess coronary aneurysms.111,112 Furtherlarger studies in patients with Kawasaki disease areneeded to establish the reliability of MRA and ultra-fast CT for the detection of coronary artery aneu-rysms and stenoses in distal segments, as well as forthe presence of collateral circulation.
Cardiac stress testing for reversible ischemia is
Fig 2. 2D echocardiogram. AO indicates aorta; PA, pulmonary artery; CX, circumflex coronary artery; L MAIN, left main coronaryartery.
AMERICAN ACADEMY OF PEDIATRICS 1717 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

indicated to assess the existence and functional con-sequences of coronary artery abnormalities in chil-dren with Kawasaki disease and coronary aneu-rysms (evidence level A). The types of stress testsreported in children with Kawasaki disease includenuclear perfusion scans with exercise,113,114 exerciseechocardiography,115,116 and stress echocardiogra-phy with pharmacological agents such as dobut-amine,117,118 dipyridamole, or adenosine.119 More re-cently, MRI stress imaging with quantification ofregional perfusion has detected significant coronarystenoses.120 Myocardial perfusion also can be as-sessed by myocardial contrast echocardiography,taking gas-filled microbubbles to measure the micro-
circulatory flow and hence capillary density in dif-ferent myocardial regions.121 With stress, the myo-cardial blood volume fraction decreases distal to astenosis, causing a perfusion defect on myocardialcontrast echocardiography.122,123
The predictive value of stress tests for coronaryartery disease requiring intervention is a function ofthe probability of significant disease in the popula-tion tested (Bayes’ theorem). For example, false-pos-itive tests are more likely in patients with a previ-ously low probability of coronary disease. Usedappropriately, stress test results may guide a clini-cian’s decision to refer a patient for invasive evalu-ation (ie, cardiac catheterization), as well as for cath-eter or surgical intervention. The choice of stressmodality should be guided by institutional expertisewith particular techniques, as well as by the age ofthe child (eg, pharmacological stress should be usedin young children in whom traditional exercise pro-tocols are not feasible).
Cardiac Catheterization and AngiographyCoronary angiography offers a more detailed def-
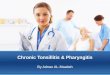
inition of coronary artery anatomy than does cardiacultrasound, making it possible to detect coronaryartery stenosis or thrombotic occlusion and to deter-mine the extent of collateral artery formation in pa-tients with Kawasaki disease (Fig 4). Before recom-mending coronary angiography to a patient, aphysician must compare the potential benefits of theprocedure with its risks and cost. In patients withmild ectasia or small fusiform aneurysms demon-strated by echocardiography, coronary angiographyis unlikely to provide any further useful informationand is not recommended (evidence level C). Patientswith more complex coronary artery lesions may ben-efit from coronary angiography after the acute in-flammatory process has resolved. Practices regard-ing the timing of cardiac catheterization for suchpatients vary greatly from center to center; coronaryangiography is generally recommended 6 to 12months after the onset of illness or sooner if indi-cated clinically (evidence level C). In long-term fol-low-up, the decision to perform angiography may beguided by echocardiographic imaging of coronaryarteries, ventricular regional wall motion abnormal-ities, and clinical signs or noninvasive studies indi-cating myocardial ischemia. The failure to image dis-tal coronary arteries in a patient in whom largeproximal aneurysms have regressed may be an indi-cation for another imaging modality, including car-diac angiography, to guide the appropriate use ofantithrombotic agents (evidence level C). Patientswho have undergone surgical revascularization orcatheter intervention may have a repeat cardiac cath-eterization so that the efficacy of the treatment can beevaluated (evidence level C).
Additional techniques used during cardiac cathe-terization may detect structural or functionalchanges in the coronary artery wall. Patients withangiographically documented regression of coronaryartery aneurysms have shown abnormal thickeningof the intima-media complex by IVUS124 and abnor-mal vasoreactivity in response to various vasodila-
Fig 3. Mean and prediction limits for 2 and 3 SDs for size of LAD(A), proximal RCA (B), and LMCA (C) according to body surfacearea for children �18 years old. LMCA z scores should not bebased on dimension at orifice and immediate vicinity; enlarge-ment of LMCA secondary to Kawasaki disease usually is associ-ated with ectasia of LAD, LCX, or both.
1718 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

tors.125,126 The long-term clinical implications ofthese anatomical and functional changes are un-known at this time.
Aneurysms can occur in arteries outside the coro-nary system, most commonly the subclavian, bra-chial, axillary, iliac, or femoral vessels, and occasion-ally in the abdominal aorta and renal arteries.127 Forthis reason, abdominal aortography and subclavianarteriography are recommended in patients with Ka-wasaki disease undergoing coronary arteriographyfor the first time (evidence level C).
MyocarditisMyocarditis has been demonstrated in autopsy
and myocardial biopsy studies to be a common fea-ture of early Kawasaki disease.34,128 Myocardial in-flammation has been documented in 50% to 70% ofpatients using 67Ga citrate scans (planar or single-photon emission CT)129 and 99mTc-labeled whiteblood cell scans.130–132 The severity of myocarditisdoes not appear to be associated with the risk ofcoronary artery aneurysms, however.133,134
Although the majority of patients with Kawasakidisease has abnormal myocardial contractility byechocardiographic assessment at presentation, myo-cardial mechanics improve rapidly after IVIG ther-apy, with a high concordance between the clinicaland myocardial responses to therapy.135 The speedof recovery suggests that depressed contractility inpatients with Kawasaki disease is caused by rapidlyreversible mechanisms such as those involving cir-culating toxins or activated cytokines. It is also pos-sible that the inflammatory infiltrate found betweenthe muscle fibers on postmortem examination inearly Kawasaki disease may resolve quickly.
The occurrence of myocarditis during the acutephase of Kawasaki disease has fostered concern
about the potential long-term effects of the diseaseon myocardial function. Biopsy of the right ventric-ular myocardium was performed in 201 patientswith Kawasaki disease to assess the evolution andcourse of myocardial change.136 The interval be-tween onset of the disease and myocardial biopsyranged from 2 months to 11 years. Myocardial ab-normalities, including fibrosis and cellular disar-rangement, as well as abnormal branching and hy-pertrophy of myocytes, were detected at all timeperiods after onset of the disease; their severity wasunrelated to the presence of coronary artery abnor-malities. In addition, electron microscopic examina-tion of endomyocardial biopsies has demonstratedultrastructural abnormalities late after Kawasaki dis-ease.137
Despite the concerns raised about histopathologicabnormalities on myocardial biopsy, long-term myo-cardial contractility and function measured by echo-cardiography appear to be normal, except amongpatients with ischemic heart disease.135 Assessmentof the full impact of Kawasaki disease on heart func-tion must await follow-up studies of these childreninto adulthood.
Valvular RegurgitationMitral regurgitation may result from transient
papillary muscle dysfunction, MI, or valvulitis. Theappearance of mitral regurgitation after the acutestage usually is secondary to myocardial ischemia,although late-onset valvulitis unrelated to ischemiahas been documented.138 Kato et al2 reported 6 pa-tients (1.0% of their series) with mitral regurgitationin the acute or subacute stage of Kawasaki disease,with resolution in 3 patients, death from MI in 2, andpersistence from papillary muscle dysfunction in 1.
Aortic regurgitation has been documented angio-
Fig 4. Coronary angiogram demonstrating giant aneurysm of the LAD with obstruction and giant aneurysm of the RCA with area ofsevere narrowing in 6-year-old boy.
AMERICAN ACADEMY OF PEDIATRICS 1719 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

graphically by Nakano and colleagues139 in �5% ofchildren with Kawasaki disease and was attributedto valvulitis. Other investigators have observed amuch lower incidence of aortic regurgitation in theacute phase,2 but late-onset aortic regurgitation hasbeen reported as an exceedingly rare finding afterKawasaki disease and may be associated with theneed for aortic valve replacement.2,138,140 Approxi-mately 4% of a consecutive series with Kawasakidisease had mild aortic regurgitation as seen byechocardiogram.100
TREATMENT
Initial Treatment
AspirinAspirin has been used in the treatment of Ka-
wasaki disease for many years. Although aspirin hasimportant anti-inflammatory (at high doses) and an-tiplatelet (at low doses) activity, it does not appear tolower the frequency of the development of coronaryabnormalities.141 During the acute phase of illness,aspirin is administered at 80 to 100 mg/kg per day in4 doses with IVIG (see next section). High-dose as-pirin and IVIG appear to possess an additive anti-inflammatory effect. Practices regarding the durationof high-dose aspirin administration vary across insti-tutions, and many centers reduce the aspirin doseafter the child has been afebrile for 48 to 72 hours.Other clinicians continue high-dose aspirin until day14 of illness and �48 to 72 hours after fever cessation.When high-dose aspirin is discontinued, cliniciansbegin low-dose aspirin (3–5 mg/kg per day) andmaintain it until the patient shows no evidence ofcoronary changes by 6 to 8 weeks after the onset ofillness (evidence level C). For children who developcoronary abnormalities, aspirin may be continuedindefinitely (evidence level B). Of note, the concom-itant use of ibuprofen antagonizes the irreversibleplatelet inhibition that is induced by aspirin142; thus,in general, ibuprofen should be avoided in childrenwith coronary aneurysms taking aspirin for its anti-platelet effects (evidence level B).
Reye syndrome is a risk in children who takesalicylates while they are experiencing active infec-tion with varicella or influenza and has been re-ported in patients taking high-dose aspirin for a pro-longed period after Kawasaki disease.143,144 It isunclear whether the low-dose therapy used for anti-platelet effect increases the risk of Reye syndrome.Children who are taking salicylates long-term shouldreceive an annual influenza vaccine.145 Althoughvaccine manufacturers recommend that salicylatesbe avoided for 6 weeks after the administration ofvaricella vaccine, physicians need to weigh the the-oretical risks associated with varicella vaccineagainst the known risks of wild-type varicella inchildren receiving long-term salicylate therapy.145
Some physicians substitute another antiplatelet med-ication for aspirin during the 6-week period. Parentsof the children receiving salicylates should be in-structed to contact their child’s physician promptly ifthe child develops symptoms of or is exposed toeither influenza or varicella.
IVIGThe efficacy of IVIG administered in the acute
phase of Kawasaki disease in reducing the preva-lence of coronary artery abnormalities is well estab-lished.141,146–148 The mechanism of action of IVIG intreating Kawasaki disease is unknown. IVIG appearsto have a generalized anti-inflammatory effect. Thepossible mechanisms of action include modulation ofcytokine production, neutralization of bacterial su-perantigens or other etiologic agents, augmentationof T-cell suppressor activity, suppression of antibodysynthesis, and provision of anti-idiotypic antibodies.
A variety of dose regimens have been used inJapan and the United States. Two meta-analyseshave demonstrated a dose-response effect, withhigher doses given in a single infusion having thegreatest efficacy.141,148 Furthermore, peak adjustedserum IgG levels are lower among patients whosubsequently develop coronary artery abnormalitiesand are inversely related to fever duration and lab-oratory indexes of acute inflammation.147,149 The as-sociation of lower peak IgG levels with worse out-comes lends further support to the concept of arelationship between serum IgG concentration andtherapeutic effectiveness.
Patients should be treated with IVIG, 2 g/kg in asingle infusion (evidence level A), together with as-pirin (see previous section).3 This therapy should beinstituted within the first 10 days of illness and, ifpossible, within 7 days of illness. Treatment of Ka-wasaki disease before day 5 of illness appears nomore likely to prevent cardiac sequelae than doestreatment on days 5 to 7, but it may be associatedwith an increased need for IVIG retreatment.150,151
IVIG also should be administered to children pre-senting after the 10th day of illness (ie, children inwhom the diagnosis was missed earlier) if they haveeither persistent fever without other explanation152
or aneurysms and ongoing systemic inflammation,as manifested by elevated ESR or CRP (evidencelevel C).
Gamma globulin is a biological product madefrom pooled donor plasma, and potentially impor-tant product-manufacturing differences exist. Per-haps for this reason, adverse effects appear to varyconsiderably among products.153–155 The results ofclinical studies comparing the efficacy of immuneglobulin products have conflicted,156,157 with moststudies failing to find a significant difference be-tween brands. Within the US health care system, theuse of high-dose IVIG is cost-effective.130 In Japan,however, some centers treat only children who arepredicted to be at high risk for developing coronaryartery disease,90 although practices have been chang-ing since 1996 with the approval by the JapaneseMinistry of Health of the 2 g/kg regimen.
Measles and varicella immunizations should bedeferred for 11 months after a child receives high-dose IVIG.145 A child in whom the risk of exposure tomeasles is high, however, may be vaccinated earlierand then be reimmunized �11 months after IVIGadministration if the child has an inadequate sero-logical response. Even when treated with high-dose
1720 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

IVIG regimens within the first 10 days of illness,�5% of children with Kawasaki disease develop atthe least transient coronary artery dilation and 1%develop giant aneurysms.98,141,148 Additional poten-tially beneficial treatments are discussed below, butthe optimal treatment awaits delineation of the spe-cific agent or agents and pathogenetic mechanisms ofKawasaki disease.
SteroidsAlthough corticosteroids are the treatment of
choice in other forms of vasculitis, their use has beenlimited in children with Kawasaki disease.158 Corti-costeroids were used as the initial therapy for Ka-wasaki disease long before the first report of IVIGefficacy by Furusho et al146 in 1984. Although anearly study by Kato et al159 suggested that steroidsexert a detrimental effect when used as the initialtherapy for Kawasaki disease, subsequent studieshave shown either no ill effects or possible benefit. Ina randomized trial of high-dose intravenous methyl-prednisolone plus heparin as compared with heparinalone, Kijima et al160 found that steroid therapy wasassociated with a greater rate of improvement incoronary abnormalities. In a randomized trial in 100children treated with intravenous prednisolone fol-lowed by an oral taper versus low-dose IVIG (300mg/kg per day for 3 consecutive days), Nonaka andcolleagues161 reported shorter fever duration in thesteroid group but no significant difference in theprevalence of coronary aneurysms. In a retrospectivereview, Shinohara et al162 found that treatment reg-imens that included prednisolone were associatedwith significantly shorter fever duration and a lowerprevalence of coronary artery aneurysms. Most re-cently, a small randomized trial examined whetherthe addition of 30 mg/kg of intravenous methyl-prednisolone to conventional therapy with IVIG (2g/kg) and aspirin improved outcomes.163 Patientswho received steroids had a shorter duration of feverand shorter hospital stays, as well as a lower meanESR and median CRP 6 weeks after the onset ofillness. No differences between treatment groups incoronary outcomes were noted, with limited statisti-cal power. Children to whom corticosteroids andIVIG were administered, compared with those whoreceived IVIG alone, had reduced levels of cytokines,including interleukin-2 (IL-2), IL-6, IL-8, and IL-10within 24 hours of IVIG administration.164 Atpresent, the usefulness of steroids in the initial treat-ment of Kawasaki disease is not well established(evidence level C). A National Heart, Lung, andBlood Institute–funded, multicenter randomized,placebo-blind trial that is in progress will providemore information on the effectiveness of such treat-ment.
PentoxifyllinePentoxifylline is a methyl xanthine compound that
specifically inhibits TNF-� messenger RNA tran-scription. Because TNF-� appears to be important inthe inflammatory cascade in Kawasaki disease, pen-toxifylline has been assessed as a therapeutic adjunctto standard therapy. In a small clinical trial in which
all patients were treated with a low-dose regimen ofIVIG plus aspirin, the individuals who receivedhigh-dose pentoxifylline appeared to have fewer an-eurysms and therapy was well tolerated.165 A recentstudy reported the pharmacokinetics of an oral pe-diatric suspension of pentoxifylline in children withacute Kawasaki disease.166 The drug was well toler-ated, and no toxicities were noted. The role of pen-toxifylline in the initial treatment of Kawasaki dis-ease is uncertain (evidence level C).
Treatment of Patients Who Failed to Respond to InitialTherapy
IVIGApproximately �10% of patients with Kawasaki
disease fail to defervesce with initial IVIG thera-py.156,167,168 Failure to respond usually is defined aspersistent or recrudescent fever �36 hours after com-pletion of the initial IVIG infusion. Most expertsrecommend retreatment with IVIG, 2 g/kg (evidencelevel C). The putative dose-response effect of IVIGforms the theoretical basis for this approach.
SteroidsCorticosteroids also have been used to treat pa-
tients who have failed to respond to initial therapyfor Kawasaki disease.158 Several small case serieshave described children with Kawasaki disease withrecrudescent or persistent fever despite IVIG treat-ment in whom the administration of steroid therapywas associated with an improvement in symptomsand the absence of a significant progression in coro-nary artery abnormalities or adverse effects.168–170 Ina recent small randomized trial, Hashino et al171
compared the efficacy and safety of additional IVIGtherapy with pulse steroid therapy in patients withIVIG-resistant Kawasaki disease. Seventeen patientswho did not respond to an initial infusion of 2 g/kgIVIG plus aspirin followed by an additional IVIGinfusion of 1 g/kg were randomized to receive eithera single additional dose of IVIG (1 g/kg) or pulsesteroid therapy. Patients in the steroid group had ashorter duration of fever and lower medical costs.No significant difference in the incidence of coronaryartery aneurysms was noted between the 2 groups,but power to detect a difference was limited.
Studies of steroids in the initial therapy for Ka-wasaki disease, as well as in therapy for patientswith persistent or recrudescent fever despite treat-ment with IVIG and aspirin, have shown that corti-costeroids reduce fever. The effects of steroids oncoronary artery abnormalities are still uncertain,however. Until multicenter controlled trials areavailable, the present writing group recommendsthat steroid treatment be restricted to children inwhom �2 infusions of IVIG have been ineffective inalleviating fever and acute inflammation (evidencelevel C). The most commonly used steroid regimen isintravenous pulse methylprednisolone, 30 mg/kgfor 2 to 3 hours, administered once daily for 1 to 3days.
AMERICAN ACADEMY OF PEDIATRICS 1721 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

Other TreatmentsPlasma exchange has been reported in an uncon-
trolled clinical trial to be an effective therapy inpatients who are refractory to IVIG and to lower theincidence of coronary artery aneurysms.172 Of note,treatment assignment was not randomized, and fewdetails about the comparability of treatment groupswere provided in this short report. Earlier reports ofdramatic response to this mode of treatment consistof small case series.173,174 Because of its risks, plasmaexchange is not in general recommended (evidencelevel C).
Ulinastatin is a human trypsin inhibitor purifiedfrom human urine that has been used in Japan as anadjunctive therapy for acute Kawasaki disease. This67 000-Dalton glycoprotein inhibits neutrophil elas-tase as well as prostaglandin H2 synthase at themessenger RNA level.175 Ulinastatin has been pro-posed as useful in IVIG-refractory patients,175 but itseffectiveness is unproven, and additional experiencewith this agent is necessary before it can be recom-mended (evidence level C).
Abciximab, a platelet glycoprotein IIb/IIIa receptorinhibitor, has been used to treat patients in the acuteor subacute phase of Kawasaki disease who havelarge coronary aneurysms.176 Patients who receivedabciximab plus standard therapy as compared withhistorical controls treated with standard therapyalone showed a greater regression in maximum an-eurysm diameter, suggesting that treatment with ab-ciximab might promote vascular remodeling. Pro-spective controlled trials are needed, but abciximabtherapy may be considered in patients with largeaneurysms in the acute or subacute phase (evidencelevel C).
A new class of agents that may play a role in thetreatment of patients with refractory Kawasaki dis-ease is monoclonal antibodies to various proinflamma-tory cytokines.177 A humanized monoclonal anti-body against TNF-�, infliximab, is being studied in aclinical trial of treatment for children who fail tobecome afebrile after initial IVIG treatment. Al-though its effectiveness in reducing the prevalence ofcoronary artery aneurysms is unproven, therapywith infliximab or other agents directed at TNF-�might be considered in patients who are resistant toIVIG and steroids (evidence level C).
Cytotoxic agents such as cyclophosphamide, in con-junction with oral steroids, have been suggested asuseful for the treatment of exceptional patients withparticularly refractory acute Kawasaki disease.168
This therapy is used widely to treat other severevasculitides. Cyclosporin A was reported to be inef-fective in halting the progression of obliterative pan-arteritis in a single case report of fatal Kawasakidisease.178 Of note, the risks of cytotoxic agents ex-ceed the benefits for the vast majority of patientswith Kawasaki disease (evidence level C).
In summary, because controlled data are lacking,the relative roles of repeated doses of IVIG, cortico-steroids, TNF-� antagonists, plasma exchange, abcix-imab, and agents such as cyclophosphamide for pa-
tients with refractory Kawasaki disease remainuncertain.
Prevention of Thrombosis in Patients With CoronaryDisease
The management of coronary disease in patientswith Kawasaki disease depends on the severity andextent of coronary involvement. No prospective dataexist to guide clinicians in choosing an optimal reg-imen, so recommendations are based on knownpathophysiology, retrospective case series in chil-dren with Kawasaki disease, and extrapolation fromexperience in adults with coronary disease. Thera-peutic regimens used in patients with Kawasaki dis-ease depend on the severity of coronary involvementand include antiplatelet therapy with aspirin, with orwithout dipyridamole or clopidogrel; anticoagulanttherapy with warfarin or low-molecular-weight hep-arin; or a combination of anticoagulant and antiplate-let therapy, usually warfarin plus aspirin.
Platelet activation is a profound component of theacute illness and persists throughout the convales-cent and chronic phases. As a result, antiplateletagents play a critical role in managing patients atevery stage. Low-dose aspirin may be appropriatefor asymptomatic patients with mild and stable dis-ease. As the extent and severity of the coronaryartery enlargement increase, the combination of as-pirin with other antiplatelet agents (eg, clopidogrel,dipyridamole) aimed at antagonizing adenosine-5�diphosphate may be more effective in suppressingplatelet activation. Clopidogrel in combination withaspirin has been shown to be more effective thaneither agent alone in preventing vascular events inboth coronary and cerebral territories in adults (theClopidogrel in Unstable Angina to Prevent RecurrentEvents study).179–182 Most experts believe that a pre-dominantly platelet-directed approach is appropri-ate in the setting of stable, mild-to-moderate disease(evidence level C).
When a coronary aneurysm expands rapidly, therisk of thrombosis is particularly high. For this rea-son, the use of heparin with aspirin has been advo-cated (evidence level C). The goals for treatment inthis group include prevention of thrombosis, as wellas modification of the evolution of the derangementof the coronary shape and size, which may relate tothe remodeling effects of endothelial damage andthrombosis.
The coronary aneurysm presents increasingly ab-normal flow conditions, which are unlike other com-mon clinical conditions such as atherosclerosis.183
Within the aneurysm itself, the vessel dilatation re-sults in low blood flow velocities and relative stasisof flow, which predispose the aneurysm to chronicthrombus formation. Additional severe abnormali-ties of coronary flow may arise over time secondaryto incremental stenoses at the proximal or distal orproximal and distal ends of the aneurysm. This com-bination of stenosis at the aneurysm inlet, in imme-diate proximity to a dilated, low-velocity region, is apowerful stimulus to thrombus formation. Plateletsare activated by the high shear stress that occurs atthe stenosis and then are stimulated further as they
1722 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

decelerate and linger within the turbulent, low-ve-locity regions distal to the stenosis. The poststenoticturbulence also is responsible for endothelial activa-tion that results from gradients in the region of shearstress. Thus, progressive stenosis of these chronicallyhypercoagulable segments augments both the plate-let and endothelial mechanisms for thrombosis. Fi-nally, the presence of chronic thrombus in the aneu-rysm presents fibrin and clotting precursors that canamplify the thrombotic cascade. Patients with giantaneurysms, with or without stenosis, are at the high-est risk for coronary thrombosis.
The most common antithrombotic regimen for pa-tients with giant aneurysms is low-dose aspirin to-gether with warfarin, maintaining an internationalnormalized ratio (INR) of 2.0 to 2.5 (evidence levelC). Some physicians substitute a therapeutic dose oflow-molecular-weight heparin for warfarin, al-though this therapy requires twice-daily subcutane-ous injections.
Treatment of Coronary ThrombosisOnce thrombosis is initiated in proximity to a seg-
ment at risk, it may progress rapidly and create athrombus burden unlike that which occurs in adultatherosclerotic coronary occlusion. Coronary occlu-sion in adults with atherosclerosis involves plaquerupture or inflammation that exposes lipids and theextracellular matrix to the coagulation system. Ka-wasaki disease-associated acute thrombosis is notrelated to this form of plaque instability or rupture.Therefore, established thrombolytic protocols foradults with atherosclerotic coronary disease may not
necessarily be optimal for the Kawasaki disease pop-ulation.
The treatment of acute coronary occlusion in pa-tients with Kawasaki disease should target multiplesteps in the coagulation cascade (Table 4). In casereports, streptokinase,184,185 urokinase,186–188 and tis-sue plasminogen activator (tPA)189,190 each has beenadministered to infants and children with coronarythrombosis with varying success rates (evidencelevel C). Because no randomized, controlled trialshave been performed in children, the treatment ofinfants and children with coronary thrombosis isderived from studies in adults with acute coronarysyndromes. The goals of therapy include reestablish-ing coronary patency, salvaging the myocardium,and improving survival.191 In adult trials, treatmentwith streptokinase has demonstrated a lower inci-dence of bleeding than have other agents (eg,Gruppo Italiano per lo Studio della Sopravvivenzanell’Infarto [GISSI-1], Second International Study ofInfarct Survival [ISIS-2]),192,193 but potential allergiccomplications limit its use in patients with a historyof streptococcal pharyngitis within the past 6months. Better coronary patency rates are achievedwith tPA than with streptokinase in adults (GlobalUtilization of Streptokinase and Tissue PlasminogenActivator for Occluded Coronary Arteries [GUSTO-1]).194–196 Tenecteplase-tPA is 14 times more fibrinspecific than is tPA and may be more fibrinolytic atthe site of the thrombus. Its longer association withthe fibrin-rich clot and higher fibrin specificity maylead to the enhanced dissolution of older clots (�4hours), with fewer bleeding complications as com-
TABLE 4. Antiplatelet, Anticoagulant, and Thrombolytic Medications
Medication Route Dosage
Aspirin Oral Antiplatelet dose: 3–5 mg/kg every dayClopidogrel Oral 1 mg/kg per day* to max (adult dose) of 75 mg/dayDipyridamole Oral 2–6 mg/kg per day in 3 divided doses†Unfractionated heparin Intravenous Load: 50 U/kg
Infusion: 20 U/kg/hAdjust dosage to achieve desired therapeutic level, usually
plasma heparin level�0.35–0.7 in antifactor Xa activityor aPTT 60–85 s
Low-molecular-weight heparin Subcutaneous Infants �12 monthsTreatment: 3 mg/kg per day, divided every 12 hProphylaxis: 1.5 mg/kg per day, divided every 12 h
Children/adolescentsTreatment: 2 mg/kg per day, divided every 12 h
Prophylaxis: 1.5 mg/kg per day, divided every 12 hProphylaxis: 1 mg/kg per day, divided every 12 hProphylaxis: 1.5 mg/kg per day, divided every 12 h
Adjust dose to achieve desired therapeutic level, usuallyantifactor Xa � 0.5–1.0 U/mL
Abciximab Intravenous Bolus: 0.25 mg/kgInfusion: 0.125 �g/kg per min for 12 h
Streptokinase Intravenous Bolus: 1000–4000 U/kg over 30 minInfusion: 1000–1500 U/kg per h
tPA Intravenous Bolus: 1.25 mg/kgInfusion: 0.1–0.5 mg/kg per h for 6 h, then reassess
Urokinase Intravenous Bolus: 4400 U/kg over 10 minInfusion: 4400 U/kg per h
Warfarin Oral 0.1 mg/kg per day, given every day (0.05–0.34 mg/kg perday; adjust dose to achieve desired INR, usually 2.0–2.5)
No published studies in children.† Clopidogrel is preferred to dipyridamole, based on adult studies.
AMERICAN ACADEMY OF PEDIATRICS 1723 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

pared with tPA (Assessment of the Safety and Effi-cacy of a New Thrombolytic [ASSENT-2]).197 Allthrombolytic regimens include aspirin and eitherheparin or low-molecular-weight heparin.
The platelet glycoprotein IIb/IIIa receptor partici-pates in the final common pathway for platelet ag-gregation. Inhibition of this receptor has shown greatpromise for improving outcomes when administeredwith aspirin and heparin, both with and without theuse of thrombolytics in adults with acute coronarysyndromes.198–200 Reduced-dose thrombolytic ther-apy in combination with the administration of a gly-coprotein IIb/IIIa inhibitor, such as abciximab, re-stores antegrade flow as effectively as does full-dosethrombolytic therapy, but it is associated with lowerrates of reocclusion and reinfarction (evidence levelC). Mechanical restoration of coronary blood flow(ie, the use of immediate coronary angioplasty orstent placement) is effective in adults and has beenused in a small number of children (evidence levelC).23 The choice of method to reestablish perfusion inchildren with Kawasaki disease and coronary throm-bosis should be based on that which can be admin-istered with the greatest expertise in a timely fashion.
Surgical and Catheter Coronary InterventionsThe current recommendations for surgical and
catheter interventions summarize the current opin-ions of experts based on limited data. The presentwriting group recommends that decisions about in-tervention in individual patients be made in concertwith experienced adult interventional cardiologistsand cardiac surgeons.
Surgical ManagementAttempts at excision or plication of the coronary
artery aneurysm have not been successful and havecaused deaths. Surgical management in Kawasakidisease comprises primarily coronary artery bypassgrafts for obstructive lesions.201–203 The diameter andlength of internal mammary grafts increase with thesomatic growth of children as compared with thetendency of saphenous vein grafts to shorten some-what over time. In a recently published series, thepatency rates of arterial grafts (primarily the left andright internal mammary arteries) were 94%, 82%,and 78% at 1, 5, and 10 years, respectively, whereaspatency rates for venous grafts were 82%, 63%, and36%, respectively.202 No early deaths occurred, andonly 2 patients died at late follow-up of mean 6.7 �4.5 years, 1 with sudden death and the other in atraffic accident. Freedom from cardiac events afterbypass was �70% at 10 years. Although the resultsduring the first decade after coronary artery bypasssurgery in childhood are encouraging, the arterialgraft patency rate in later adult life is still unknown.
The indications for coronary bypass graft proce-dures in children have not been established in clini-cal trials, but such surgery should be consideredwhen reversible ischemia is present on stress-imag-ing test results, the myocardium to be perfusedthrough the graft is still viable, and no appreciablelesions are present in the artery distal to the plannedgraft site (evidence level C). One panel of experts
stated that surgical revascularization may be consid-ered under the following conditions: severe occlu-sion of the main trunk of the LMCA, severe occlusionof �1 major coronary artery, severe occlusion in theproximal segment of the LAD, collateral coronaryarteries in jeopardy, or all of the above.204 Mostexperts agree that surgery is indicated after recurrentMI because the prognosis is so unfavorable.205,206
Interventional Cardiac Catheterization TechniquesCatheter interventions including balloon angio-
plasty, rotational ablation, and stent placement havebeen performed in a relatively small number of chil-dren with Kawasaki disease. Most of the experiencehas been accumulated in Japan. In general, balloonangioplasty has not been successful even with high-pressure balloons when it is done �2 years after theacute illness because of dense fibrosis and calcifica-tion in the arterial wall.207,208 The relatively highballoon pressures that are necessary under these cir-cumstances can lead to late neoaneurysm forma-tion.208 For this reason, if percutaneous transluminalcoronary angioplasty cannot be performed with aballoon pressure of �10 atm, then rotational ablationor bypass surgery is advisable as an alternative pro-cedure.209 IVUS imaging has been found to be auseful tool for evaluating internal vessel morphologybefore and after percutaneous transluminal coronaryangioplasty.207 Stent placement has been useful inolder children with mild calcification and in childrenwith giant aneurysms. Rotational ablation and stentplacement have met with a success rate �80% ac-cording to a collective experience in Japan.210
The recommendations for catheter intervention forpatients with Kawasaki disease recently formulatedby the Research Committee of the Japanese Ministryof Health, Labor, and Welfare209 state that catheterintervention should be considered in patients pre-senting with ischemic symptoms, patients withoutischemic symptoms but with reversible ischemia onstress test, and patients without ischemia but with�75% stenosis in the LAD (evidence level C). Bypasssurgery is preferred in patients with severe LV dys-function. Catheter intervention is contraindicated forindividuals who have vessels with multiple, ostial, orlong-segment lesions (evidence level C).
Cardiac TransplantationA small number of patients with Kawasaki disease
have undergone cardiac transplantation for severemyocardial dysfunction, severe ventricular arrhyth-mias, and severe coronary arterial lesions for whichinterventional catheterization or coronary artery by-pass procedures were not feasible.211 The timing oftransplant has ranged from a few weeks or months toas long as 12 years after acute Kawasaki disease.Almost half of the transplant patients had undergoneprevious bypass grafting procedures without expe-riencing improvement in myocardial function. Thisprocedure should be considered only for individualswith severe, irreversible myocardial dysfunction andcoronary lesions for which interventional catheter-ization procedures or coronary artery bypass are notfeasible (evidence level C).
1724 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

LONG-TERM FOLLOW-UP
Natural History
Regression and Evolution of Coronary LesionsCoronary artery lesions resulting from Kawasaki
disease change dynamically with time. Angiographicresolution 1 to 2 years after onset of the disease hasbeen observed in �50% to 67% of vessels with cor-onary aneurysms.2,212 The likelihood that an aneu-rysm will resolve appears to be determined in largemeasure by its initial size, with smaller aneurysmshaving a greater likelihood of regression.213,214 Otherfactors that are positively associated with the regres-sion of aneurysms include age at onset of Kawasakidisease �1 year, fusiform rather than saccular aneu-rysm morphology, and aneurysm location in a distalcoronary segment.212 Vessels that do not undergoapparent resolution of abnormalities may demon-strate persistence of aneurysmal morphology, devel-opment of stenosis or occlusion, or abnormal tortu-osity. Rupture of a coronary aneurysm can occurwithin the first few months after Kawasaki disease,but this is an exceedingly rare occurrence.
Course of Patients With Persistent Coronary ArteryAbnormalities
Whereas aneurysm size tends to diminish withtime, stenotic lesions that are secondary to markedmyointimal proliferation are frequently progres-sive.2,127,215 The prevalence of stenosis continues torise almost linearly over time.2,215 The highest rate ofprogression to stenosis occurs among patients whoseaneurysms are large.215 The worst prognosis occursin children with so-called giant aneurysms (ie, thosewith a maximum diameter �8 mm).215–219 In theseaneurysms, thrombosis is promoted by the combina-tion of sluggish blood flow within the massivelydilated vascular space and the frequent occurrence ofstenotic lesions at the proximal or distal end of theaneurysms.
MI caused by thrombotic occlusion in an aneurys-mal, a stenotic, or both types of coronary artery is theprincipal cause of death from Kawasaki disease.206
The highest risk of MI occurs in the first year afteronset of the disease, and most fatal attacks are asso-ciated with obstruction in either the LMCA or boththe RCA and LAD.206 Serial stress tests and myocar-dial imaging are mandatory in the management ofpatients with Kawasaki disease and significant cor-onary artery disease so that the need for coronaryangiography and for surgical or transcatheter inter-vention can be determined.
The carotid artery wall in patients with coronaryartery lesions 6 to 20 years after the onset of Ka-wasaki disease has been found to be less distensibleand thicker than that in control patients.220 Thesechanges of arterial properties in patients with Ka-wasaki disease are not associated with major alter-ations of the lipid profile and are postulated to besecondary to the changes in arterial walls after adiffuse vasculitis. Extrapolation from these findingsin carotid arteries suggests that the coronary arteriesmay be predisposed to accelerated atherosclerosis inpatients with Kawasaki disease and coronary artery
lesions. A similar study has not yet been performedin children with Kawasaki disease who did not de-velop coronary abnormalities.
Late cardiac sequelae of Kawasaki disease mayfirst manifest in adulthood.221,222 A history of a Ka-wasaki disease-like illness in childhood should besought in patients who present with coronary aneu-rysms in the absence of generalized atheroscleroticdisease. Some adult patients may be unable to recallan illness that occurred so early in life, however.
Course of Patients With Spontaneous Regression ofAneurysms
Approximately 50% of the vascular segments withcoronary artery aneurysms in Kawasaki diseaseshow angiographic regression of aneurysms. Thisregression usually occurs by myointimal prolifera-tion, although more rarely the mechanism of regres-sion can be organization and recanalization of athrombus.34,223,224 Pathological examination revealsfibrous intimal thickening despite a normal coronaryartery lumen diameter. Similarly, transluminal (in-travascular) ultrasound of regressed coronary aneu-rysms shows marked symmetrical or asymmetricalmyointimal thickening.124,225,226 Regressed coronaryartery aneurysms are not only histopathologicallyabnormal, but they also show reduced vascular re-activity to isosorbide dinitrate and constriction withacetylcholine, indicating endothelial dysfunc-tion.104,125,126,226 A recent follow-up study with IVUSsuggested a significant correlation between the initialdiameters of the coronary arteries and intima-medialthickness �10 years later.225
Course After Kawasaki Disease Without DetectableCoronary Lesions
Although coronary artery aneurysms produce themost serious sequelae of Kawasaki disease, vascularinflammation during the acute stage of the illness isdiffuse. Generalized endothelial dysfunction hasbeen suggested by the observation that plasma 6-ke-to-prostaglandin F1 remains generally undetectableduring the 8 weeks after the onset of Kawasaki dis-ease.227 In addition, Kawasaki disease produces al-tered lipid metabolism that persists beyond clinicalresolution of the disease.75,77,228 Children with Ka-wasaki disease with normal coronary arteries alsohave been reported to have higher brachial-radialartery mean pulse wave velocity than do childrenwithout Kawasaki disease, suggesting increased ar-terial stiffness.228 Histological data concerning thelong-term status of the coronary arteries in childrenwho never had demonstrable abnormalities are fewand difficult to interpret.223,229
Some investigators in Japan have studied coronaryphysiology in the population without aneurysms.Among children with a history of Kawasaki diseasebut with normal epicardial coronary arteries, lowermyocardial flow reserve and higher total coronaryresistance compared with normal controls werefound by Muzik et al.106 Children without a historyof coronary aneurysms after Kawasaki disease alsohave been reported to have abnormal endothelium-dependent brachial artery reactivity.103 The data con-
AMERICAN ACADEMY OF PEDIATRICS 1725 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

flict regarding the impairment of long-term endothe-lium-dependent relaxation of the epicardial coronaryarteries among children in whom coronary arterydilation was never detected.105,230
From a purely clinical perspective, children with-out known cardiac sequelae during the first month ofKawasaki disease appear to return to their previous(usually excellent) state of health, without signs orsymptoms of cardiac impairment.2 Meaningfulknowledge about long-term myocardial function,late-onset valvar regurgitation, and coronary arterystatus in this population must await their carefulsurveillance in future decades.
Risk StratificationClinical experience with Kawasaki disease permits
the stratification of patients according to their rela-tive risk of myocardial ischemia. Risk-level catego-ries are listed below and are summarized in Table 5.This stratification allows for patient management tobe individualized with respect to medical therapy toreduce the risk of thrombosis, physical activity, fre-quency of clinical follow-up and diagnostic testing,and indications for cardiac catheterization and coro-nary angiography. With careful clinical follow-up 10to 20 years after the onset of Kawasaki disease, pa-tients with no coronary artery changes on echocar-diography at any stage of the illness seem to dem-onstrate a risk for clinical cardiac events that issimilar to that in the population without Kawasakidisease,2 but research studies suggest subclinical ab-normalities of endothelial function and myocardialflow reserve.103,231–233 Furthermore, patients withKawasaki disease seem to have a more adverse car-diovascular risk profile, with higher blood pressureand greater adiposity, as compared with control chil-dren.234 The risk level for a given patient with coro-nary artery involvement may change over time be-cause of the changes in coronary artery morphology.For example, the development of thrombosis or ste-nosis associated with an aneurysm increases therisk for myocardial ischemia. Aneurysms also mayregress to normal internal lumen diameter overtime; optimal management of patients with re-gressed aneurysms is controversial because struc-tural and functional coronary artery abnormalitiespersist.57,126,226,235,236 The following suggestions forlong-term management are based on a consensus ofexperts and serve as a guide to clinicians until long-term studies and prospective trials facilitate evi-dence-based practice (evidence level C).
Risk LevelsRisk Level I—Patients with no coronary artery changes on
echocardiography at any stage of the illness
• No antiplatelet therapy is needed beyond the ini-tial 6 to 8 weeks after the onset of illness.
• No restriction of physical activity is necessary after6 to 8 weeks.
• Because the degree of future risk for ischemicheart disease in this category of patients is stillundetermined, periodic assessment and counsel-
ing about known cardiovascular risk factors every5 years is suggested.
• Coronary angiography is not recommended.Risk Level II—Patients with transient coronary artery
ectasia or dilatation (disappearing within the initial 6 to 8weeks after the onset of illness)
• No antiplatelet therapy is needed beyond the ini-tial 6 to 8 weeks after the onset of illness.
• No restriction of physical activity is necessary after6 to 8 weeks.
• Risk assessment and counseling is recommendedat 3- to 5-year intervals.
• Coronary angiography is not recommended.Risk Level III—Patients with isolated (solitary) small to
medium (�3-mm but �6-mm, or z score between 3 and 7)coronary artery aneurysm in �1 coronary arteries onechocardiography or angiography
• Long-term antiplatelet therapy with aspirinshould be administered, at least until the aneu-rysms regress.
• Physical activity without restriction in infants andchildren in the first decade of life is permitted afterthe initial 6 to 8 weeks. Stress tests with myocar-dial perfusion evaluation may be useful in thesecond decade to guide recommendations forphysical activity. Participation in competitive col-lision or high-impact sports is discouraged in chil-dren receiving antiplatelet therapy.
• Annual follow-up by a pediatric cardiologist withechocardiogram and electrocardiogram (ECG) isrecommended. Stress tests with myocardial perfu-sion imaging is recommended every 2 years inpatients �10 years old.
• Coronary angiography is indicated if myocardialischemia is demonstrated by stress tests withimaging.Risk Level IV—Patients with �1 large coronary artery
aneurysm (�6 mm), including giant aneurysms, and patientsin whom a coronary artery contains multiple (segmented) orcomplex aneurysms without obstruction
• Long-term antiplatelet therapy is recommended.Adjunctive therapy with warfarin with a targetINR of 2.0:2.5 is recommended for patients withgiant aneurysms. Daily subcutaneous injections oflow-molecular-weight heparin merits consider-ation as an alternative to warfarin for infants andtoddlers, in whom blood drawing for INR testingis difficult. Low-molecular-weight heparin alsomay be used as a bridge during the initial phase ofwarfarin therapy or during the reintroduction ofwarfarin after the interruption of therapy for thepurpose of elective surgery; therapeutic levels areassessed by measuring antifactor Xa levels. Someexperts recommend a combination of aspirin andclopidogrel for patients with multiple or complexaneurysms.
• Recommendations about physical activity shouldbe guided by annual stress tests with myocardialperfusion evaluation. Collision or high-impactsports should be discouraged because of the risk ofbleeding. Participation in noncontact dynamic or
1726 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

TA
BL
E5.
Ris
kSt
rati
fica
tion
Ris
kL
evel
Phar
mac
olog
ical
The
rapy
Phys
ical
Act
ivit
yFo
llow
-Up
and
Dia
gnos
tic
Tes
ting
Inva
sive
Tes
ting
I(n
oco
rona
ryar
tery
chan
ges
atan
yst
age
ofill
ness
)
Non
ebe
yond
1st
6–8
wee
ksN
ore
stri
ctio
nsbe
yond
1st
6–8
wee
ksC
ard
iova
scul
arri
skas
sess
men
t,co
unse
ling
at5-
yin
terv
als
Non
ere
com
men
ded
II(t
rans
ient
coro
nary
arte
ryec
tasi
ad
isap
pear
sw
ithi
n1s
t6–
8w
eeks
)
Non
ebe
yond
1st
6–8
wee
ksN
ore
stri
ctio
nsbe
yond
1st
6–8
wee
ksC
ard
iova
scul
arri
skas
sess
men
t,co
unse
ling
at3-
to5-
yin
terv
als
Non
ere
com
men
ded
III
(1sm
all-
med
ium
coro
nary
arte
ryan
eury
sm/
maj
orco
rona
ryar
tery
)
Low
-dos
eas
piri
n(3
–5m
g/kg
aspi
rin
per
day
),at
leas
tun
til
aneu
rysm
regr
essi
ond
ocum
ente
d
For
pati
ents
�11
yol
d,n
ore
stri
ctio
nbe
yond
1st
6–8
wee
ks;p
atie
nts
11–
20y
old
,phy
sica
lac
tivi
tygu
ided
bybi
enni
alst
ress
test
,eva
luat
ion
ofm
yoca
rdia
lpe
rfus
ion
scan
;co
ntac
tor
high
-im
pact
spor
tsd
isco
urag
edfo
rpa
tien
tsta
king
anti
plat
elet
agen
ts
Ann
ual
card
iolo
gyfo
llow
-up
wit
hec
hoca
rdio
gram
�E
CG
,co
mbi
ned
wit
hca
rdio
vasc
ular
risk
asse
ssm
ent,
coun
selin
g;bi
enni
alst
ress
test
/ev
alua
tion
ofm
yoca
rdia
lpe
rfus
ion
scan
Ang
iogr
aphy
,if
noni
nvas
ive
test
sugg
ests
isch
emia
IV(�
1la
rge
orgi
ant
coro
nary
arte
ryan
eury
sm,o
rmul
tipl
eor
com
plex
aneu
rysm
sin
sam
eco
rona
ryar
tery
,w
itho
utob
stru
ctio
n)
Lon
g-te
rman
tipl
atel
etth
erap
yan
dw
arfa
rin
(tar
get
INR
2.0–
2.5)
orlo
w-
mol
ecul
ar-w
eigh
the
pari
n(t
arge
t:an
tifa
ctor
Xa
leve
l0.
5–1.
0U
/m
L)
shou
ldbe
com
bine
din
gian
tan
eury
sms
Con
tact
orhi
gh-i
mpa
ctsp
orts
shou
ldbe
avoi
ded
beca
use
ofri
skof
blee
din
g;ot
her
phys
ical
acti
vity
reco
mm
end
atio
nsgu
ided
byst
ress
test
/ev
alua
tion
ofm
yoca
rdia
lpe
rfus
ion
scan
outc
ome
Bia
nnua
lfo
llow
-up
wit
hec
hoca
rdio
gram
�E
CG
;an
nual
stre
sste
st/
eval
uati
onof
myo
card
ial
perf
usio
nsc
an
1st
angi
ogra
phy
at6–
12m
oor
soon
erif
clin
ical
lyin
dic
ated
;re
peat
edan
giog
raph
yif
noni
nvas
ive
test
,clin
ical
,or
labo
rato
ryfi
ndin
gssu
gges
tis
chem
ia;e
lect
ive
repe
atan
giog
raph
yun
der
som
eci
rcum
stan
ces
(see
text
)V
(cor
onar
yar
tery
obst
ruct
ion)
Lon
g-te
rmlo
w-d
ose
aspi
rin;
war
fari
nor
low
-mol
ecul
ar-
wei
ght
hepa
rin
ifgi
ant
aneu
rysm
pers
ists
;con
sid
erus
eof
�-b
lock
ers
tore
duc
em
yoca
rdia
lO
2co
nsum
ptio
n
Con
tact
orhi
gh-i
mpa
ctsp
orts
shou
ldbe
avoi
ded
beca
use
ofri
skof
blee
din
g;ot
her
phys
ical
acti
vity
reco
mm
end
atio
nsgu
ided
byst
ress
test
/m
yoca
rdia
lpe
rfus
ion
scan
outc
ome
Bia
nnua
lfo
llow
-up
wit
hec
hoca
rdio
gram
and
EC
G;
annu
alst
ress
test
/ev
alua
tion
ofm
yoca
rdia
lpe
rfus
ion
scan
Ang
iogr
aphy
reco
mm
end
edto
add
ress
ther
apeu
tic
opti
ons
AMERICAN ACADEMY OF PEDIATRICS 1727 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

recreational sports is encouraged if no evidenceexists of stress-induced myocardial ischemia.
• Cardiology evaluation with echocardiogram andECG should be done at 6-month intervals. Stresstests with myocardial perfusion evaluation shouldbe performed annually. The patient should bemonitored for known risk factors of atherosclero-sis and his or her family should be counseledaccordingly.
• Cardiac catheterization with selective coronary an-giography should be performed 6 to 12 monthsafter recovery from the acute illness, or sooner ifclinically indicated, to delineate the complex cor-onary artery anatomy. Follow-up angiographymay be indicated if noninvasive studies suggestmyocardial ischemia. In addition, elective cardiaccatheterization in the absence of noninvasive evi-dence of myocardial ischemia may be useful torule out subclinical major coronary artery obstruc-tions in some situations, such as when the patientexperiences atypical chest pain, the ability to per-form dynamic stress testing is limited by age,unique activity restrictions or insurability recom-mendations are needed, or the anatomy or size ofthe aneurysm cannot be clearly defined by echo-cardiography for decisions regarding anticoagula-tion.
• For females of childbearing age, reproductivecounseling is strongly recommended.Risk Level V—Patients with coronary artery obstruction
confirmed by angiography
• Long-term antiplatelet therapy with or withoutadjunctive therapy with warfarin anticoagulationis recommended (see “Risk Level IV”).
• �-Adrenergic-blocking drugs should be consid-ered to reduce myocardial oxygen consumption.
• Recommendations about dynamic physical activi-ties should be based on the patient’s responseto stress testing. Collision or high-impact sportsshould be discouraged because of the risk of bleed-ing. Patients should avoid a sedentary lifestyle.
• Cardiology evaluation with an echocardiogramand ECG should be obtained at 6-month intervals.Stress tests with myocardial perfusion evaluationshould be performed annually. The patient shouldbe monitored for known risk factors of atheroscle-rosis and his or her family should be counseledaccordingly.
• Cardiac catheterization with selective coronary an-giography is recommended to address the thera-peutic options of bypass grafting or catheter inter-vention and to identify the extent of collateralperfusion. Repeat cardiac catheterization may beindicated when new onset or worsening myocar-dial ischemia is suggested by noninvasive diag-nostic testing or clinical presentation. If the patienthas undergone surgical revascularization or acatheter intervention, then repeat cardiac catheter-ization may be indicated to evaluate the efficacy ofthe treatment.
• For females of childbearing age, reproductivecounseling is strongly recommended.
SUMMARYKawasaki disease is the leading cause of acquired
heart disease in children in the United States. Coro-nary artery aneurysms or ectasia develop in �15% to25% of untreated children; treatment with IVIG inthe acute phase of the disease reduces this risk to�5%. Treatment with high-dose IVIG is recom-mended for children with fever of 4 days’ durationand 4 of 5 classic clinical criteria, as well as for thosewith fewer clinical criteria in whom coronary abnor-malities are noted by echocardiogram. This scientificstatement proposes a new algorithm to aid cliniciansin deciding which children with fever for �5 daysand �4 classic criteria should undergo echocardiog-raphy, receive IVIG treatment, or both for Kawasakidisease. For patients with persistent or recurrent fe-ver after initial IVIG infusion, IVIG retreatment maybe useful. We reviewed the available data regardingother therapies for children with IVIG-resistant Ka-wasaki disease, including treatment with corticoste-roids, TNF-� antagonists, and abciximab. Angio-graphic resolution occurs in �50% of aneurysmalarterial segments, but these segments show persis-tent histological and functional abnormalities. Theremainder may continue to be aneurysmal, oftenwith the development of progressive stenosis or oc-clusion. The long-term management of patients withKawasaki disease should be tailored to the degree ofcoronary involvement. The present writing groupmade recommendations for each risk level regardingantiplatelet and anticoagulant therapies, physical ac-tivity, follow-up assessment, and the appropriate di-agnostic procedures that may be performed to eval-uate cardiac disease. The risk level for a given patientwith coronary arterial involvement may change overtime because of the changes in coronary artery mor-phology. Our statement on the initial evaluation,treatment in the acute phase, and long-term manage-ment of patients with Kawasaki disease is intendedto provide practical interim recommendations untilevidence-based data are available to define best med-ical practices.
DISCLOSUREThe American Heart Association makes every effort to avoid
any actual or potential conflicts of interest that may arise as aresult of an outside relationship or a personal, professional, orbusiness interest of a member of the writing panel. Specifically, allmembers of the writing group are required to complete and sub-mit a Disclosure Questionnaire showing all such relationships thatmight be perceived as real or potential conflicts of interest.
Dr Jane W. Newburger has received research grants from Phil-ips Medical and Pfizer and is a National Heart, Lung, and BloodInstitute Advisory Council member; Dr Masato Takahashi hasreceived a research grant from Sonofi-Synthelabo; and Dr Jane C.Burns has received a research grant from Centocor. No disclosureswere made by the remaining authors of this report: Dr Michael A.Gerber, Dr Michael H. Gewitz, Dr Lloyd Y. Tani, Dr Stanford T.Shulman, Dr Ann F. Bolger, Dr Patricia Ferrieri, Dr Robert S.Baltimore, Dr Walter R. Wilson, Dr Larry M. Baddour, Dr Mat-thew E. Levison, Dr Thomas J. Pallasch, Dr Donald A. Falace, andDr Kathryn A. Taubert.
REFERENCES1. Kawasaki T. Acute febrile mucocutaneous syndrome with lymphoid
involvement with specific desquamation of the fingers and toes inchildren [in Japanese]. Arerugi. 1967;16:178
1728 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

2. Kato H, Sugimura T, Akagi T, et al. Long-term consequences of Ka-wasaki disease. A 10- to 21-year follow-up study of 594 patients.Circulation. 1996;94:1379–1385
3. Dajani AS, Taubert KA, Gerber MA, et al. Diagnosis and therapy ofKawasaki disease in children. Circulation. 1993;87:1776–1780
4. Taubert KA, Rowley AH, Shulman ST. Nationwide survey of Ka-wasaki disease and acute rheumatic fever. J Pediatr. 1991;119:279–282
5. Landing BH, Larson EJ. Are infantile periarteritis nodosa with coro-nary artery involvement and fatal mucocutaneous lymph node syn-drome the same? Comparison of 20 patients from North America withpatients from Hawaii and Japan. Pediatrics. 1977;59:651–662
6. Gee SJ. Cases of morbid anatomy: aneurysms of coronary arteries in aboy. St Bartholomew’s Hosp Rep. 1871;7
7. Yanagawa H, Yashiro M, Nakamura Y, Kawasaki T, Kato H. Results of12 nationwide epidemiological incidence surveys of Kawasaki diseasein Japan. Arch Pediatr Adolesc Med. 1995;149:779–783
8. Burns JC, Kushner HI, Bastian JF, et al. Kawasaki disease: a briefhistory. Pediatrics. 2000;106(2). Available at: www.pediatrics.org/cgi/content/full/106/2/e27
9. Yanagawa H, Nakamura Y, Yashiro M, et al. Incidence survey ofKawasaki disease in 1997 and 1998 in Japan. Pediatrics. 2001;107(3).Available at: www.pediatrics.org/cgi/content/full/107/3/e33
10. Holman RC, Curns AT, Belay ED, Steiner CA, Schonberger LB. Ka-wasaki syndrome hospitalizations in the United States, 1997 and 2000.Pediatrics. 2003;112:495–501
11. Chang RK. The incidence of Kawasaki disease in the United States didnot increase between 1988 and 1997. Pediatrics. 2003;111:1124–1125
12. Davis RL, Waller PL, Mueller BA, Dykewicz CA, Schonberger LB.Kawasaki syndrome in Washington State. Race-specific incidence ratesand residential proximity to water. Arch Pediatr Adolesc Med.1995;149:66–69
13. Bronstein DE, Dille AN, Austin JP, Williams CM, Palinkas LA, BurnsJC. Relationship of climate, ethnicity and socioeconomic status toKawasaki disease in San Diego County, 1994 through 1998. PediatrInfect Dis J. 2000;19:1087–1091
14. Stockheim JA, Innocentini N, Shulman ST. Kawasaki disease in olderchildren and adolescents. J Pediatr. 2000;137:250–252
15. Chang RK. Hospitalizations for Kawasaki disease among children inthe United States, 1988–1997. Pediatrics. 2002;109(6). Available at:www.pediatrics.org/cgi/content/full/109/6/e87
16. Momenah T, Sanatani S, Potts J, Sandor GG, Human DG, PattersonMW. Kawasaki disease in the older child. Pediatrics. 1998;102(1). Avail-able at: www.pediatrics.org/cgi/content/full/102/1/e7
17. Yanagawa H, Nakamura Y, Yashiro M, Ojima T, Tanihara S, Oki I,Zhang T. Results of the nationwide epidemiologic survey of Kawasakidisease in 1995 and 1996 in Japan. Pediatrics. 1998;102(6). Available at:www.pediatrics.org/cgi/content/full/102/6/e65
18. Hirata S, Nakamura Y, Yanagawa H. Incidence rate of recurrent Ka-wasaki disease and related risk factors: from the results of nationwidesurveys of Kawasaki disease in Japan. Acta Paediatr. 2001;90:40–44
19. Fujita Y, Nakamura Y, Sakata K, et al. Kawasaki disease in families.Pediatrics. 1989;84:666–669
20. Harada F, Sada M, Kamiya T, Yanase Y, Kawasaki T, Sasazuki T.Genetic analysis of Kawasaki syndrome. Am J Hum Genet.1986;39:537–539
21. Yanagawa H, Yashiro M, Nakamura Y, Kawasaki T, Kato H. Epide-miologic pictures of Kawasaki disease in Japan: from the nationwideincidence survey in 1991 and 1992. Pediatrics. 1995;95:475–479
22. Quasney MW, Bronstein DE, Cantor RM, et al. Increased frequency ofalleles associated with elevated tumor necrosis factor-alpha levels inchildren with Kawasaki disease. Pediatr Res. 2001;49:686–690
23. Newburger JW, Taubert KA, Shulman ST, et al. Summary and ab-stracts of the Seventh International Kawasaki Disease Symposium:December 4–7, 2001, Hakone, Japan. Pediatr Res. 2003;53:153–157
24. Kaneko K, Obinata K, Katsumata K, Tawa T, Hosaka A, Yamashiro Y.Kawasaki disease in a father and daughter. Acta Paediatr.1999;88:791–792
25. Bruckheimer E, Bulbul Z, McCarthy P, Madri JA, Friedman AH, Hel-lenbrand WE. Images in cardiovascular medicine: Kawasaki disease:coronary aneurysms in mother and son. Circulation. 1998;97:410–411
26. Uehara R, Yashiro M, Nakamura Y, Yanagawa H. Kawasaki disease inparents and children. Acta Paediatr. 2003;92:694–697
27. Bell DM, Brink EW, Nitzkin JL, et al. Kawasaki syndrome: descriptionof two outbreaks in the United States. N Engl J Med.1981;304:1568–1575
28. Rauch AM. Kawasaki syndrome: review of new epidemiologic andlaboratory developments. Pediatr Infect Dis J. 1987;6:1016–1021
29. Rauch AM, Glode MP, Wiggins JW Jr, et al. Outbreak of Kawasakisyndrome in Denver, Colorado: association with rug and carpet clean-ing. Pediatrics. 1991;87:663–669
30. Treadwell TA, Maddox RA, Holman RC, et al. Investigation of Ka-wasaki syndrome risk factors in Colorado. Pediatr Infect Dis J.2002;21:976–978
31. Brosius CL, Newburger JW, Burns JC, Hojnowski-Diaz P, Zierler S,Leung DY. Increased prevalence of atopic dermatitis in Kawasakidisease. Pediatr Infect Dis J. 1988;7:863–866
32. Rauch AM, Kaplan SL, Nihill MR, Pappas PG, Hurwitz ES, Schon-berger LB. Kawasaki syndrome clusters in Harris County, Texas, andeastern North Carolina. A high endemic rate and a new environmentalrisk factor. Am J Dis Child. 1988;142:441–444
33. Nakamura Y, Yanagawa H, Harada K, Kato H, Kawasaki T. Mortalityamong persons with a history of Kawasaki disease in Japan: the fifthlook. Arch Pediatr Adolesc Med. 2002;156:162–165
34. Fujiwara H, Hamashima Y. Pathology of the heart in Kawasaki dis-ease. Pediatrics. 1978;61:100–107
35. Burns JC, Glode MP, Clarke SH, Wiggins J Jr, Hathaway WE. Coagu-lopathy and platelet activation in Kawasaki syndrome: identificationof patients at high risk for development of artery aneurysms. J Pediatr.1984;105:206–211
36. Burns JC, Shike H, Gordon JB, Malhotra A, Schoenwetter M, KawasakiT. Sequelae of Kawasaki disease in adolescents and young adults. J AmColl Cardiol. 1996;28:253–257
37. Abe J, Kotzin BL, Jujo K, Melish ME, Glode MP, Kohsaka T, Leung DY.Selective expansion of T cells expressing T-cell receptor variable re-gions V beta 2 and V beta 8 in Kawasaki disease. Proc Natl Acad SciUSA. 1992;89:4066–4070
38. Yamashiro Y, Nagata S, Oguchi S, Shimizu T. Selective increase ofV�2� T cells in the small intestinal mucosa in Kawasaki disease. PediatrRes. 1996;39:264–266
39. Leung DY, Giorno RC, Kazemi LV, Flynn PA, Busse JB. Evidence forsuperantigen involvement in cardiovascular injury due to Kawasakisyndrome. J Immunol. 1995;155:5018–5021
40. Leung DY. Superantigens related to Kawasaki syndrome. SpringerSemin Immunopathol. 1996;17:385–396
41. Leung DY, Meissner HC, Shulman ST, et al. Prevalence of superanti-gen-secreting bacteria in patients with Kawasaki disease. J Pediatr.2002;140:742–746
42. Rowley AH, Eckerley CA, Jack HM, Shulman ST, Baker SC. IgAplasma cells in vascular tissue of patients with Kawasaki syndrome.J Immunol. 1997;159:5946–5955
43. Rowley AH, Shulman ST, Spike BT, Mask CA, Baker SC. OligoclonalIgA response in the vascular wall in acute Kawasaki disease. J Immu-nol. 2001;166:1334–1343
44. Rowley AH, Shulman ST, Mask CA, et al. IgA plasma cell infiltrationof proximal respiratory tract, pancreas, kidney, and coronary artery inacute Kawasaki disease. J Infect Dis. 2000;182:1183–1191
45. Brown TJ, Crawford SE, Cornwall ML, Garcia F, Shulman ST, RowleyAH. CD8 T lymphocytes and macrophages infiltrate coronary arteryaneurysms in acute Kawasaki disease. J Infect Dis. 2001;184:940–943
46. Takeshita S, Tokutomi T, Kawase H, et al. Elevated serum levels ofmatrix metalloproteinase-9 (MMP-9) in Kawasaki disease. Clin ExpImmunol. 2001;125:340–344
47. Yasukawa K, Terai M, Shulman ST, et al. Systemic production ofvascular endothelial growth factor and fms-like tyrosine kinase-1 re-ceptor in acute Kawasaki disease. Circulation. 2002;105:766–769
48. Maeno N, Takei S, Masuda K, et al. Increased serum levels of vascularendothelial growth factor in Kawasaki disease. Pediatr Res.1998;44:596–599
49. Asano T, Ogawa S. Expression of monocyte chemoattractant protein-1in Kawasaki disease: the anti-inflammatory effect of gamma globulintherapy. Scand J Immunol. 2000;51:98–103
50. Freeman AF, Crawford SE, Finn LS, et al. Inflammatory pulmonarynodules in Kawasaki disease. Pediatr Pulmonol. 2003;36:102–106
51. Eberhard BA, Andersson U, Laxer RM, Rose V, Silverman ED. Evalu-ation of the cytokine response in Kawasaki disease. Pediatr Infect Dis J.1995;14:199–203
52. Furukawa S, Matsubara T, Umezawa Y, Okumura K, Yabuta K. Serumlevels of p60 soluble tumor necrosis factor receptor during acuteKawasaki disease. J Pediatr. 1994;124:721–725
53. Lin CY, Lin CC, Hwang B, Chiang B. Serial changes of serum inter-leukin-6, interleukin-8, and tumor necrosis factor alpha among pa-tients with Kawasaki disease. J Pediatr. 1992;121:924–926
54. Ohno T, Yuge T, Kariyazono H, et al. Serum hepatocyte growth factorcombined with vascular endothelial growth factor as a predictive
AMERICAN ACADEMY OF PEDIATRICS 1729 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

indicator for the occurrence of coronary artery lesions in Kawasakidisease. Eur J Pediatr. 2002;161:105–111
55. Naoe S, Takahashi K, Masuda H, Tanaka N. Kawasaki disease. Withparticular emphasis on arterial lesions. Acta Pathol Jpn. 1991;41:785–797
56. Gavin PJ, Crawford SE, Shulman ST, Garcia FL, Rowley AH. Systemicarterial expression of matrix metalloproteinases 2 and 9 in acute Ka-wasaki disease. Arterioscler Thromb Vasc Biol. 2003;23:576–581
57. Suzuki A, Miyagawa-Tomita S, Komatsu K, et al. Active remodeling ofthe coronary arterial lesions in the late phase of Kawasaki disease:immunohistochemical study. Circulation. 2000;101:2935–2941
58. Kurashige M, Naoe S, Masuda H, Tanaka N. A morphological study ofthe digestive tract in Kawasaki disease: 31 autopsies [in Japanese].Myakkangaku. 1984;24:407–418
59. Nagata S, Yamashiro Y, Maeda M, Ohtsuka Y, Yabuta K. Immunohis-tochemical studies on small intestinal mucosa in Kawasaki disease.Pediatr Res. 1993;33:557–563
60. Suddleson EA, Reid B, Woolley MM, Takahashi M. Hydrops of thegallbladder associated with Kawasaki syndrome. J Pediatr Surg.1987;22:956–959
61. Tashiro N, Matsubara T, Uchida M, Katayama K, Ichiyama T, Fu-rukawa S. Ultrasonographic evaluation of cervical lymph nodes inKawasaki disease. Pediatrics. 2002;109(5). Available at:www.pediatrics.org/cgi/content/full/109/5/e77
62. Sundel RP, Cleveland SS, Beiser AS, et al. Audiologic profiles ofchildren with Kawasaki disease. Am J Otol. 1992;13:512–515
63. Knott PD, Orloff LA, Harris JP, Novak RE, Burns JC; Kawasaki DiseaseMulticenter Hearing Loss Study Group. Sensorineural hearing lossand Kawasaki disease: a prospective study. Am J Otolaryngol.2001;22:343–348
64. Sundel RP, Newburger JW, McGill T, et al. Sensorineural hearing lossassociated with Kawasaki disease. J Pediatr. 1990;117:371–377
65. Zulian F, Falcini F, Zancan L, et al. Acute surgical abdomen as pre-senting manifestation of Kawasaki disease. J Pediatr. 2003;142:731–735
66. Kuniyuki S, Asada M. An ulcerated lesion at the BCG vaccination siteduring the course of Kawasaki disease. J Am Acad Dermatol.1997;37:303–304
67. Uziel Y, Hashkes PJ, Kassem E, Gottesman G, Wolach B. “Unresolvingpneumonia” as the main manifestation of atypical Kawasaki disease.Arch Dis Child. 2003;88:940–942
68. Palazzi DL, McClain KL, Kaplan SL. Hemophagocytic syndrome afterKawasaki disease. Pediatr Infect Dis J. 2003;22:663–666
69. Comenzo RL, Malachowski ME, Meissner HC, Fulton DR, BerkmanEM. Immune hemolysis, disseminated intravascular coagulation, andserum sickness after large doses of immune globulin given intrave-nously for Kawasaki disease. J Pediatr. 1992;120:926–928
70. Shulman ST. Hemolysis in Kawasaki disease. Transfusion. 1991;31:57271. Bunin NJ, Carey JL, Sullivan DB. Autoimmune hemolytic anemia in
association with Kawasaki disease. Am J Pediatr Hematol Oncol.1986;8:351–353
72. Hillyer CD, Schwenn MR, Fulton DR, Meissner HC, Berkman EM.Autoimmune hemolytic anemia in Kawasaki disease: a case report.Transfusion. 1990;30:738–740
73. Andersson MS, Burns J, Treadwell TA, Pietra BA, Glode MP. Eryth-rocyte sedimentation rate and C-reactive protein discrepancy and highprevalence of coronary artery abnormalities in Kawasaki disease. Pe-diatr Infect Dis J. 2001;20:698–702
74. Hicks RV, Melish ME. Kawasaki syndrome. Pediatr Clin North Am.1986;33:1151–1175
75. Newburger JW, Burns JC, Beiser AS, Loscalzo J. Altered lipid profileafter Kawasaki syndrome. Circulation. 1991;84:625–631
76. Salo E, Pesonen E, Viikari J. Serum cholesterol levels during and afterKawasaki disease. J Pediatr. 1991;119:557–561
77. Cabana VG, Gidding SS, Getz GS, Chapman J, Shulman ST. Serumamyloid A and high density lipoprotein participate in the acute phaseresponse of Kawasaki disease. Pediatr Res. 1997;42:651–655
78. Okada T, Harada K, Okuni M. Serum HDL-cholesterol and lipoproteinfraction in Kawasaki disease (acute mucocutaneous lymph node syn-drome). Jpn Circ J. 1982;46:1039–1044
79. Burns JC, Mason WH, Glode MP, et al. Clinical and epidemiologiccharacteristics of patients referred for evaluation of possible Kawasakidisease. United States Multicenter Kawasaki Disease Study Group.J Pediatr. 1991;118:680–686
80. Ting EC, Capparelli EV, Billman GF, Lavine JE, Matsubara T, Burns JC.Elevated gamma-glutamyltransferase concentrations in patients withacute Kawasaki disease. Pediatr Infect Dis J. 1998;17:431–432
81. Dengler LD, Capparelli EV, Bastian JF, et al. Cerebrospinal fluid profilein patients with acute Kawasaki disease. Pediatr Infect Dis J.1998;17:478–481
82. Kim M, Kim K. Changes in cardiac troponin I in Kawasaki diseasebefore and after treatment with intravenous gammaglobulin. Jpn CircJ. 1998;62:479–482
83. Kim M, Kim K. Elevation of cardiac troponin I in the acute stage ofKawasaki disease. Pediatr Cardiol. 1999;20:184–188
84. Checchia PA, Borensztajn J, Shulman ST. Circulating cardiac troponinI levels in Kawasaki disease. Pediatr Cardiol. 2001;22:102–106
85. Burns JC, Wiggins JW Jr, Toews WH, et al. Clinical spectrum ofKawasaki disease in infants younger than 6 months of age. J Pediatr.1986;109:759–763
86. Asai T. Diagnosis and prognosis of coronary artery lesions in Ka-wasaki disease. Coronary angiography and the conditions for itsapplication (a score chart) [in Japanese]. Nippon Rinsho. 1983;41:2080–2085
87. Koren G, Lavi S, Rose V, Rowe R. Kawasaki disease: review of riskfactors for coronary aneurysms. J Pediatr. 1986;108:388–392
88. Ichida F, Fatica NS, Engle MA, et al. Coronary artery involvement inKawasaki syndrome in Manhattan, New York: risk factors and role ofaspirin. Pediatrics. 1987;80:828–835
89. Daniels SR, Specker B, Capannari TE, Schwartz DC, Burke MJ, KaplanS. Correlates of coronary artery aneurysm formation in patients withKawasaki disease. Am J Dis Child. 1987;141:205–207
90. Harada K, Yamaguchi H, Kato H, et al. Indication for intravenousgamma globulin treatment for Kawasaki disease. In: Takahashi M,Taubert K, eds. Proceedings of the Fourth International Symposium onKawasaki Disease. Dallas, TX: American Heart Association; 1993:459–462
91. Harada K. Intravenous gamma-globulin treatment in Kawasaki dis-ease. Acta Paediatr Jpn. 1991;33:805–810
92. Beiser AS, Takahasha M, Baker AL, Sundel RP, Newburger JW. Apredictive instrument for coronary artery aneurysms in Kawasakidisease. United States Multicenter Kawasaki Disease Study Group.Am J Cardiol. 1998;81:1116–1120
93. Witt MT, Minich LL, Bohnsack JF, Young PC. Kawasaki disease: morepatients are being diagnosed who do not meet American Heart Asso-ciation criteria. Pediatrics. 1999;104(1). Available at: www.pediatrics.org/cgi/content/full/104/1/e10
94. Joffe A, Kabani A, Jadavji T. Atypical and complicated Kawasakidisease in infants. Do we need criteria? West J Med. 1995;162:322–327
95. Tseng CF, Fu YC, Fu LS, Betau H, Chi CS. Clinical spectrum ofKawasaki disease in infants. Zhonghua Yi Xue Za Zhi. 2001;64:168–173
96. de Zorzi A, Colan SD, Gauvreau K, Baker AL, Sundel RP, NewburgerJW. Coronary artery dimensions may be misclassified as normal inKawasaki disease. J Pediatr. 1998;133:254–258
97. Kurotobi S, Nagai T, Kawakami N, Sano T. Coronary diameter innormal infants, children and patients with Kawasaki disease. PediatrInt. 2002;44:1–4
98. Dajani AS, Taubert KA, Takahashi M, et al. Guidelines for long-termmanagement of patients with Kawasaki disease. Report from the Com-mittee on Rheumatic Fever, Endocarditis, and Kawasaki Disease,Council on Cardiovascular Disease in the Young, American HeartAssociation. Circulation. 1994;89:916–922
99. Research Committee on Kawasaki Disease. Report of Subcommittee onStandardization of Diagnostic Criteria and Reporting of Coronary ArteryLesions in Kawasaki Disease. Tokyo, Japan: Ministry of Health andWelfare; 1984
100. Ravekes WJ, Colan SD, Gauvreau K, et al. Aortic root dilation inKawasaki disease. Am J Cardiol. 2001;87:919–922
101. Scott JS, Ettedgui JA, Neches WH. Cost-effective use of echocardiog-raphy in children with Kawasaki disease. Pediatrics. 1999;104(5). Avail-able at: www.pediatrics.org/cgi/content/full/104/5/e57
102. McMorrow Tuohy AM, Tani LY, Cetta F, et al. How many echocar-diograms are necessary for follow-up evaluation of patients with Ka-wasaki disease? Am J Cardiol. 2001;88:328–330
103. Dhillon R, Clarkson P, Donald AE, et al. Endothelial dysfunction lateafter Kawasaki disease. Circulation. 1996;94:2103–2106
104. Kurisu Y, Azumi T, Sugahara T, Igarashi Y, Takamiya M, Kozuka T.Variation in coronary arterial dimension (distensible abnormality) af-ter disappearing aneurysm in Kawasaki disease. Am Heart J.1987;114:532–538
105. Mitani Y, Okuda Y, Shimpo H, et al. Impaired endothelial function inepicardial coronary arteries after Kawasaki disease. Circulation.1997;96:454–461
106. Muzik O, Paridon SM, Singh TP, Morrow WR, Dayanikli F, DiCarliMF. Quantification of myocardial blood flow and flow reserve inchildren with a history of Kawasaki disease and normal coronaryarteries using positron emission tomography. J Am Coll Cardiol.1996;28:757–762
1730 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

107. Duerinckx A, Troutman B, Allada V, Kim D. Coronary MR angiogra-phy in Kawasaki disease. AJR Am J Roentgenol. 1997;168:114–116
108. Sakuma H, Goto M, Nomura Y, Kato N, Takeda K, Higgins CB.Three-dimensional coronary magnetic resonance angiography withinjection of extracellular contrast medium. Invest Radiol. 1999;34:503–508
109. Danias PG, Stuber M, Botnar RM, et al. Coronary MR angiographyclinical applications and potential for imaging coronary artery disease.Magn Reson Imaging Clin N Am. 2003;11:81–99
110. Greil GF, Stuber M, Botnar RM, et al. Coronary magnetic resonanceangiography in adolescents and young adults with Kawasaki disease.Circulation. 2002;105:908–911
111. Frey EE, Matherne GP, Mahoney LT, Sato Y, Stanford W, Smith WL.Coronary artery aneurysms due to Kawasaki disease: diagnosis withultrafast CT. Radiology. 1988;167:725–726
112. Sato Y, Kato M, Inoue F, et al. Detection of coronary artery aneurysms,stenoses and occlusions by multislice spiral computed tomography inadolescents with kawasaki disease. Circ J. 2003;67:427–430
113. Kondo C, Hiroe M, Nakanishi T, Takao A. Detection of coronary arterystenosis in children with Kawasaki disease. Circulation.1989;80:615–624
114. Jan SL, Hwang B, Fu YC, et al. Usefulness of pharmacologic stress201Tl myocardial tomography. Comparison of 201Tl SPET and tread-mill exercise testing in patients with Kawasaki disease. Nucl MedCommun. 2000;21:431–435
115. Pahl E, Sehgal R, Chrystof D, et al. Feasibility of exercise stress echo-cardiography for the follow-up of children with coronary involvementsecondary to Kawasaki disease. Circulation. 1995;91:122–128
116. Henein MY, Dinarevic S, O’Sullivan CA, Gibson DG, Shinebourne EA.Exercise echocardiography in children with Kawasaki disease: ventric-ular long axis is selectively abnormal. Am J Cardiol. 1998;81:1356–1359
117. Noto N, Ayusawa M, Karasawa K, et al. Dobutamine stress echocar-diography for detection of coronary artery stenosis in children withKawasaki disease. J Am Coll Cardiol. 1996;27:1251–1256
118. Kimball TR, Witt SA, Daniels SR. Dobutamine stress echocardiographyin the assessment of suspected myocardial ischemia in children andyoung adults. Am J Cardiol. 1997;79:380–384
119. Bezold LI, Lewin MB, Vick GW III, Pignatelli R. Update on newtechnologies in pediatric echocardiography. Tex Heart Inst J.1997;24:278–286
120. Muhling O, Jerosch-Herold M, Nabauer M, Wilke N. Assessment ofischemic heart disease using magnetic resonance first-pass perfusionimaging. Herz. 2003;28:82–89
121. Kaul S, Ito H. Microvasculature in acute myocardial ischemia: part I:evolving concepts in pathophysiology, diagnosis, and treatment. Cir-culation. 2004;109:146–149
122. Zilberman MV, Witt SA, Kimball TR. Is there a role for intravenoustranspulmonary contrast imaging in pediatric stress echocardiogra-phy? J Am Soc Echocardiogr. 2003;16:9–14
123. Ishii M, Himeno W, Sawa M, et al. Assessment of the ability ofmyocardial contrast echocardiography with harmonic power Dopplerimaging to identify perfusion abnormalities in patients with Kawasakidisease at rest and during dipyridamole stress. Pediatr Cardiol.2002;23:192–199
124. Sugimura T, Kato H, Inoue O, et al. Intravascular ultrasound of coro-nary arteries in children. Assessment of the wall morphology and thelumen after Kawasaki disease. Circulation. 1994;89:258–265
125. Matsumura K, Okuda Y, Ito T, Hirano T, Takeda K, Yamaguchi M.Coronary angiography of Kawasaki disease with the coronary vaso-dilator dipyridamole: assessment of distensibility of affected coronaryarterial wall. Angiology. 1988;39:141–147
126. Sugimura T, Kato H, Inoue O, Takagi J, Fukuda T, Sato N. Vasodila-tory response of the coronary arteries after Kawasaki disease: evalua-tion by intracoronary injection of isosorbide dinitrate. J Pediatr.1992;121:684–688
127. Suzuki A, Kamiya T, Kuwahara N, et al. Coronary arterial lesions ofKawasaki disease: cardiac catheterization findings of 1100 cases. Pedi-atr Cardiol. 1986;7:3–9
128. Yutani C, Okano K, Kamiya T, et al. Histopathological study on rightendomyocardial biopsy of Kawasaki disease. Br Heart J.1980;43:589–592
129. Matsuura H, Ishikita T, Yamamoto S, et al. Gallium-67 myocardialimaging for the detection of myocarditis in the acute phase of Ka-wasaki disease (mucocutaneous lymph node syndrome): the useful-ness of single photon emission computed tomography. Br Heart J.1987;58:385–392
130. Klassen TP, Rowe PC, Gafni A. Economic evaluation of intravenousimmune globulin therapy for Kawasaki syndrome. J Pediatr.1993;122:538–542
131. Kao CH, Hsieh KS, Wang YL, et al. Tc-99m HMPAO labeled WBC scanfor the detection of myocarditis in different phases of Kawasaki dis-ease. Clin Nucl Med. 1992;17:185–190
132. Rinder CS, Bohnert J, Rinder HM, Mitchell J, Ault K, Hillman R.Platelet activation and aggregation during cardiopulmonary bypass.Anesthesiology. 1991;75:388–393
133. Anderson TM, Meyer RA, Kaplan S. Long-term echocardiographicevaluation of cardiac size and function in patients with Kawasakidisease. Am Heart J. 1985;110:107–115
134. Hiraishi S, Yashiro K, Oguchi K, Kusano S, Ishii K, Nakazawa K.Clinical course of cardiovascular involvement in the mucocutaneouslymph node syndrome. Relation between clinical signs of carditis anddevelopment of coronary arterial aneurysm. Am J Cardiol. 1981;47:323–330
135. Moran AM, Newburger JW, Sanders SP, et al. Abnormal myocardialmechanics in Kawasaki disease: rapid response to gamma-globulin.Am Heart J. 2000;139:217–223
136. Yutani C, Go S, Kamiya T, et al. Cardiac biopsy of Kawasaki disease.Arch Pathol Lab Med. 1981;105:470–473
137. Takahashi M, Shimada H, Billingham ME, Mason W, Miller JH. Elec-tron microscopic findings of myocardial biopsy correlated with perfu-sion scan and coronary angiography in chronic Kawasaki syndrome:myocellular ischemia possibly due to microvasculopathy. In: Kato H,ed. Kawasaki Disease. Proceedings of the 5th International KawasakiDisease Symposium, Fukuoka, Japan, May 22–25, 1995. New York, NY:Elsevier Science; 1995:401–410
138. Gidding SS. Late onset valvular dysfunction in Kawasaki disease. ProgClin Biol Res. 1987;250:305–309
139. Nakano H, Nojima K, Saito A, Ueda K. High incidence of aorticregurgitation following Kawasaki disease. J Pediatr. 1985;107:59–63
140. Gidding SS, Shulman ST, Ilbawi M, Crussi F, Duffy CE. Mucocutane-ous lymph node syndrome (Kawasaki disease): delayed aortic andmitral insufficiency secondary to active valvulitis. J Am Coll Cardiol.1986;7:894–897
141. Durongpisitkul K, Gururaj VJ, Park JM, Martin CF. The prevention ofcoronary artery aneurysm in Kawasaki disease: a meta-analysis on theefficacy of aspirin and immunoglobulin treatment. Pediatrics.1995;96:1057–1061
142. Catella-Lawson F, Reilly MP, Kapoor SC, et al. Cyclooxygenase inhib-itors and the antiplatelet effects of aspirin. N Engl J Med.2001;345:1809–1817
143. Takahashi M, Mason W, Thomas D, Sinatra F. Reye syndrome follow-ing Kawasaki syndrome confirmed by liver histopathology. In: Kato H,ed. Kawasaki Diseas. Proceedings of the 5th International KawasakiDisease Symposium, Fukuoka, Japan, May 22–25, 1995. New York, NY:Elsevier Science; 1995:436–444
144. Lee JH, Hung HY, Huang FY. Kawasaki disease with Reye syndrome:report of one case. Zhonghua Min Guo Xiao Er Ke Yi Xue Hui Za Zhi.1992;33:67–71
145. Pickering LK, ed. Red Book. 2003 Report of the Committee on InfectiousDiseases. Chicago, IL: American Academy of Pediatrics; 2003
146. Furusho K, Kamiya T, Nakano H, et al. High-dose intravenous gam-maglobulin for Kawasaki disease. Lancet. 1984;2:1055–1058
147. Newburger JW, Takahashi M, Burns JC, et al. The treatment of Ka-wasaki syndrome with intravenous gamma globulin. N Engl J Med.1986;315:341–347
148. Terai M, Shulman ST. Prevalence of coronary artery abnormalities inKawasaki disease is highly dependent on gamma globulin dose butindependent of salicylate dose. J Pediatr. 1997;131:888–893
149. Sawaji Y, Haneda N, Yamaguchi S, et al. Coronary risk factors in acuteKawasaki disease: correlation of serum immunoglobulin levels withcoronary complications. Acta Paediatr Jpn. 1998;40:218–225
150. Muta H, Ishii M, Egami K, et al. Early intravenous gamma-globulintreatment for Kawasaki disease: the nationwide surveys in Japan.J Pediatr. 2004;144:496–499
151. Fong NC, Hui YW, Li CK, Chiu MC. Evaluation of the efficacy oftreatment of Kawasaki disease before day 5 of illness. Pediatr Cardiol.2004;25:31–34
152. Marasini M, Pongiglione G, Gazzolo D, Campelli A, Ribaldone D,Caponnetto S. Late intravenous gamma globulin treatment in infantsand children with Kawasaki disease and coronary artery abnormali-ties. Am J Cardiol. 1991;68:796–797
153. Rosenfeld EA, Shulman ST, Corydon KE, Mason W, Takahashi M,Kuroda C. Comparative safety and efficacy of two immune globulinproducts in Kawasaki disease. J Pediatr. 1995;126:1000–1003
AMERICAN ACADEMY OF PEDIATRICS 1731 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

154. Outbreak of hepatitis C associated with intravenous immunoglobulinadministration–United States. October 1993-June 1994. MMWR MorbMortal Wkly Rep. 1994;43:505–509
155. Venglarcik JS III, Ayas M, Woods T. Severe thrombocytopenia as apresenting manifestation of Kawasaki disease. Arch Pediatr AdolescMed. 1995;149:215–217
156. Burns JC, Capparelli EV, Brown JA, Newburger JW, Glode MP. Intra-venous gamma-globulin treatment and retreatment in Kawasaki dis-ease. US/Canadian Kawasaki Syndrome Study Group. Pediatr InfectDis J. 1998;17:1144–1148
157. Silverman ED, Huang C, Rose V, et al. IVGG treatment of Kawasakidisease: are all brands equal? In: Kato H, ed. Kawasaki Disease. Pro-ceedings of the 5th International Kawasaki Disease Symposium,Fukuoka, Japan, May 22–25, 1995. New York, NY: Elsevier Science;1995:301–304
158. Shulman ST. Is there a role for corticosteroids in Kawasaki disease?J Pediatr. 2003;142:601–603
159. Kato H, Koike S, Yokoyama T. Kawasaki disease: effect of treatment oncoronary artery involvement. Pediatrics. 1979;63:175–179
160. Kijima Y, Kamiya T, Suzuki A, Hirose O, Manabe H. A trial procedureto prevent aneurysm formation of the coronary arteries by steroidpulse therapy in Kawasaki disease. Jpn Circ J. 1982;46:1239–1242
161. Nonaka Z, Maekawa K, Okabe T, Eto Y, Kubo M. Randomized con-trolled study of intravenous prednisolone and gamma globulin treat-ment in 100 cases with Kawasaki disease. In: Kato H, ed. KawasakiDisease. Proceedings of the 5th International Kawasaki Disease Sym-posium, Fukuoka, Japan, May 22–25, 1995. New York, NY: ElsevierScience; 1995:328–331
162. Shinohara M, Sone K, Tomomasa T, Morikawa A. Corticosteroids inthe treatment of the acute phase of Kawasaki disease. J Pediatr.1999;135:465–469
163. Sundel RP, Baker AL, Fulton DR, Newburger JW. Corticosteroids inthe initial treatment of Kawasaki disease: report of a randomized trial.J Pediatr. 2003;142:611–616
164. Okada Y, Shinohara M, Kobayashi T, et al. Effect of corticosteroids inaddition to intravenous gamma globulin therapy on serum cytokinelevels in the acute phase of Kawasaki disease in children. J Pediatr.2003;143:363–367
165. Furukawa S, Matsubara T, Umezawa Y, Motohashi T, Ino T, Yabuta K.Pentoxifylline and intravenous gamma globulin combination therapyfor acute Kawasaki disease. Eur J Pediatr. 1994;153:663–667
166. Best BM, Burns JC, DeVincenzo J, et al. Pharmacokinetic and tolera-bility assessment of a pediatric oral formulation of pentoxifylline inKawasaki disease. Curr Ther Res Clin Exp. 2003;64:96–115
167. Durongpisitkul K, Soongswang J, Laohaprasitiporn D, Nana A, Pra-chuabmoh C, Kangkagate C. Immunoglobulin failure and retreatmentin Kawasaki disease. Pediatr Cardiol. 2003;24:145–148
168. Wallace CA, French JW, Kahn SJ, Sherry DD. Initial intravenous gam-maglobulin treatment failure in Kawasaki disease. Pediatrics.2000;105(6). Available at: www.pediatrics.org/cgi/content/full/105/6/e78
169. Wright DA, Newburger JW, Baker A, Sundel RP. Treatment of im-mune globulin-resistant Kawasaki disease with pulsed doses of corti-costeroids. J Pediatr. 1996;128:146–149
170. Dale RC, Saleem MA, Daw S, Dillon MJ. Treatment of severe compli-cated Kawasaki disease with oral prednisolone and aspirin. J Pediatr.2000;137:723–726
171. Hashino K, Ishii M, Iemura M, Akagi T, Kato H. Re-treatment forimmune globulin-resistant Kawasaki disease: a comparative study ofadditional immune globulin and steroid pulse therapy. Pediatr Int.2001;43:211–217
172. Imagawa T, Mori M, Miyamae T, et al. Plasma exchange for refractoryKawasaki disease. Eur J Pediatr. 2004;163:263–264
173. Takagi N, Kihara M, Yamaguchi S, et al. Plasma exchange in Kawasakidisease. Lancet. 1995;346:1307
174. Villain E, Kachaner J, Sidi D, Blaysat G, Piechaud JF, Pedroni E. Trialof prevention of coronary aneurysm in Kawasaki’s disease usingplasma exchange or infusion of immunoglobulins [in French]. Arch FrPediatr. 1987;44:79–83
175. Zaitsu M, Hamasaki Y, Tashiro K, Matsuo M, Ichimaru T, Fujita I,Tasaki H, Miyazaki S. Ulinastatin, an elastase inhibitor, inhibits theincreased mRNA expression of prostaglandin H2 synthase-type 2 inKawasaki disease. J Infect Dis. 2000;181:1101–1109
176. Williams RV, Wilke VM, Tani LY, Minich LL. Does abciximab enhanceregression of coronary aneurysms resulting from Kawasaki disease?Pediatrics. 2002;109(1). Available at: www.pediatrics.org/cgi/content/full/109/1/e4
177. Weiss JE, Eberhard BA, Chowdhury D, Gottlieb BS. Infliximab as anovel therapy for refractory Kawasaki disease. J Rheumatol.2004;31:808–810
178. Kuijpers TW, Biezeveld M, Achterhuis A, et al. Longstanding obliter-ative panarteritis in Kawasaki disease: lack of cyclosporin A effect.Pediatrics. 2003;112:986–992
179. Gerschutz GP, Bhatt DL. The Clopidogrel in Unstable Angina to Pre-vent Recurrent Events (CURE) study: to what extent should the resultsbe generalizable? Am Heart J. 2003;145:595–601
180. Peters RJ, Mehta SR, Fox KA, et al. Effects of aspirin dose when usedalone or in combination with clopidogrel in patients with acute coro-nary syndromes: observations from the Clopidogrel in Unstable an-gina to prevent Recurrent Events (CURE) study. Circulation.2003;108:1682–1687
181. Albers GW, Amarenco P. Combination therapy with clopidogrel andaspirin: can the CURE results be extrapolated to cerebrovascular pa-tients? Stroke. 2001;32:2948–2949
182. Mehta SR, Yusuf S. The Clopidogrel in Unstable angina to preventRecurrent Events (CURE) trial programme; rationale, design and base-line characteristics including a meta-analysis of the effects of thienopy-ridines in vascular disease. Eur Heart J. 2000;21:2033–2041
183. Kuramochi Y, Ohkubo T, Takechi N, Fukumi D, Uchikoba Y, Ogawa S.Hemodynamic factors of thrombus formation in coronary aneurysmsassociated with Kawasaki disease. Pediatr Int. 2000;42:470–475
184. Burtt DM, Pollack P, Bianco JA. Intravenous streptokinase in an infantwith Kawasaki’s disease complicated by acute myocardial infarction.Pediatr Cardiol. 1986;6:307–311
185. Cheatham JP, Kugler JD, Gumbiner CH, Latson LA, Hofschire PJ. In-tracoronary streptokinase in Kawasaki disease: acute and thromboly-sis. Prog Clin Biol Res. 1987;250:517–518
186. Katayama F, Hiraishi S, Takeda N, Misawa H. Intracoronary urokinaseand post-thrombolytic regimen in an infant with Kawasaki disease andacute myocardial infarction. Heart. 1997;78:621–622
187. Kato H, Ichinose E, Inoue O, Akagi T. Intracoronary thrombolytictherapy in Kawasaki disease: treatment and prevention of acute myo-cardial infarction. Prog Clin Biol Res. 1987;250:445–454
188. Terai M, Ogata M, Sugimoto K, et al. Coronary arterial thrombi inKawasaki disease. J Pediatr. 1985;106:76–78
189. Horigome H, Sekijima T, Miyamoto T. Successful thrombolysis withintracoronary administration of tissue plasminogen activator in aninfant with Kawasaki disease. Heart. 1997;78:517–518
190. Levy M, Benson LN, Burrows PE, et al. Tissue plasminogen activatorfor the treatment of thromboembolism in infants and children. J Pedi-atr. 1991;118:467–472
191. Lange RA, Hillis LD. Reperfusion therapy in acute myocardial infarc-tion. N Engl J Med. 2002;346:954–955
192. Maggioni AP, Franzosi MG, Fresco C, Turazza F, Tognoni G. GISSItrials in acute myocardial infarction. Rationale, design, and results.Chest. 1990; 97:146S–150S
193. Randomised trial of intravenous streptokinase, oral aspirin, both, orneither among 17,187 cases of suspected acute myocardial infarction:ISIS-2. ISIS-2 (Second International Study of Infarct Survival) Collab-orative Group. Lancet. 1988;2:349–360
194. Ridker PM, O’Donnell C, Marder VJ, Hennekens CH. Large-scale trialsof thrombolytic therapy for acute myocardial infarction: GISSI-2,ISIS-3, and GUSTO-1. Ann Intern Med. 1993;119:530–532
195. Hennekens CH. Thrombolytic therapy: pre- and post-GISSI-2, ISIS-3,and GUSTO-1. Clin Cardiol. 1994;17:I15–I17
196. Newby LK, Rutsch WR, Califf RM, et al. Time from symptom onset totreatment and outcomes after thrombolytic therapy. GUSTO-1 Inves-tigators. J Am Coll Cardiol. 1996;27:1646–1655
197. Wang-Clow F, Fox NL, Cannon CP, et al. Determination of a weight-adjusted dose of TNK-tissue plasminogen activator. Am Heart J.2001;141:33–40
198. Westerhout CM, Boersma E. Risk-benefit analysis of platelet glycop-rotein IIb/IIIa inhibitors in acute coronary syndromes. Expert OpinDrug Saf. 2003;2:49–58
199. Ibbotson T, McGavin JK, Goa KL. Abciximab: an updated review of itstherapeutic use in patients with ischaemic heart disease undergoingpercutaneous coronary revascularisation. Drugs. 2003;63:1121–1163
200. Hellstrom HR. Platelet glycoprotein IIb/IIIa inhibitors. Circulation.2003;107:E39
201. Kitamura S, Kameda Y, Seki T, et al. Long-term outcome of myocardialrevascularization in patients with Kawasaki coronary artery disease. Amulticenter cooperative study. J Thorac Cardiovasc Surg. 1994;107:663–674
1732 KAWASAKI DISEASE: DIAGNOSIS, TREATMENT, LONG-TERM MANAGEMENT by guest on April 10, 2019www.aappublications.org/newsDownloaded from

202. Tsuda E, Kitamura S; Cooperative Study Group of Japan. Nationalsurvey of coronary artery bypass grafting for coronary stenosis causedby Kawasaki disease in Japan. Circulation. 2004;110:II61–II66
203. Yoshikawa Y, Yagihara T, Kameda Y, et al. Result of surgical treat-ments in patients with coronary-arterial obstructive disease after Ka-wasaki disease. Eur J Cardiothorac Surg. 2000;17:515–519
204. Guidelines for treatment and management of cardiovascular sequelaein Kawasaki disease. Subcommittee of Cardiovascular Sequelae, Sub-committee of Surgical Treatment, Kawasaki Disease Research Com-mittee. Heart Vessels. 1987;3:50–54
205. Kitamura S. The role of coronary bypass operation on children withKawasaki disease. Coron Artery Dis. 2002;13:437–447
206. Kato H, Ichinose E, Kawasaki T. Myocardial infarction in Kawasakidisease: clinical analyses in 195 cases. J Pediatr. 1986;108:923–927
207. Ino T, Akimoto K, Ohkubo M, et al. Application of percutaneoustransluminal coronary angioplasty to coronary arterial stenosis in Ka-wasaki disease. Circulation. 1996;93:1709–1715
208. Sugimura T, Yokoi H, Sato N, et al. Interventional treatment forchildren with severe coronary artery stenosis with calcification afterlong-term Kawasaki disease. Circulation. 1997;96:3928–3933
209. Ishii M, Ueno T, Akagi T, et al. Guidelines for catheter intervention incoronary artery lesion in Kawasaki disease. Pediatr Int. 2001;43:558–562
210. Ishii M, Ueno T, Ikeda H, et al. Sequential follow-up results of catheterintervention for coronary artery lesions after Kawasaki disease: quan-titative coronary artery angiography and intravascular ultrasound im-aging study. Circulation. 2002;105:3004–3010
211. Checchia PA, Pahl E, Shaddy RE, Shulman ST. Cardiac transplantationfor Kawasaki disease. Pediatrics. 1997;100:695–699
212. Takahashi M, Mason W, Lewis AB. Regression of coronary aneurysmsin patients with Kawasaki syndrome. Circulation. 1987;75:387–394
213. Fujiwara T, Fujiwara H, Hamashima Y. Size of coronary aneurysm asa determinant factor of the prognosis in Kawasaki disease: clinicopath-ologic study of coronary aneurysms. Prog Clin Biol Res.1987;250:519–520
214. Nakano H, Ueda K, Saito A, Nojima K. Repeated quantitative angio-grams in coronary arterial aneurysm in Kawasaki disease. Am J Cardiol.1985;56:846–851
215. Kamiya T, Suzuki A, Ono Y, et al. Angiographic follow-up study ofcoronary artery lesion in the cases with a history of Kawasakidisease–with a focus on the follow-up more than ten years after theonset of the disease. In: Kato H, ed. Kawasaki Disease. Proceedings ofthe 5th International Kawasaki Disease Symposium, Fukuoka, Japan,May 22–25, 1995. New York, NY: Elsevier Science; 1995:569–573
216. Fujiwara T, Fujiwara H, Hamashima Y. Frequency and size of coronaryarterial aneurysm at necropsy in Kawasaki disease. Am J Cardiol.1987;59:808–811
217. Nakano H, Saito A, Ueda K, Nojima K. Clinical characteristics ofmyocardial infarction following Kawasaki disease: report of 11 cases.J Pediatr. 1986;108:198–203
218. Tatara K, Kusakawa S. Long-term prognosis of giant coronary aneu-rysm in Kawasaki disease: an angiographic study. J Pediatr.1987;111:705–710
219. Matsui S, Matsumori A, Matoba Y, Uchida A, Sasayama S. Treatmentof virus-induced myocardial injury with a novel immunomodulatingagent, vesnarinone. Suppression of natural killer cell activity andtumor necrosis factor-alpha production. J Clin Invest. 1994;94:1212–1217
220. Noto N, Okada T, Yamasuge M, et al. Noninvasive assessment of theearly progression of atherosclerosis in adolescents with Kawasakidisease and coronary artery lesions. Pediatrics. 2001;107:1095–1099
221. Burns JC, Shike H, Gordon JB, Malhotra A, Schoenwetter M, KawasakiT. Sequelae of Kawasaki disease in adolescents and young adults. J AmColl Cardiol. 1996;28:253–257
222. Kato H, Inoue O, Kawasaki T, Fujiwara H, Watanabe T, Toshima H.Adult coronary artery disease probably due to childhood Kawasakidisease. Lancet. 1992;340:1127–1129
223. Tanaka N, Naoe S, Masuda H, Ueno T. Pathological study of sequelaeof Kawasaki disease (MCLS). With special reference to the heart andcoronary arterial lesions. Acta Pathol Jpn. 1986;36:1513–1527
224. Sasaguri Y, Kato H. Regression of aneurysms in Kawasaki disease: apathological study? J Pediatr. 1982;100:225–231
225. Tsuda E, Kamiya T, Kimura K, Ono Y, Echigo S. Coronary arterydilatation exceeding 4.0 mm during acute Kawasaki disease predicts ahigh probability of subsequent late intima-medial thickening. PediatrCardiol. 2002;23:9–14
226. Iemura M, Ishii M, Sugimura T, Akagi T, Kato H. Long term conse-quences of regressed coronary aneurysms after Kawasaki disease:vascular wall morphology and function. Heart. 2000;83:307–311
227. Fulton DR, Meissner C, Peterson MB. Effects of current therapy ofKawasaki disease on eicosanoid metabolism. Am J Cardiol.1988;61:1323–1327
228. Cheung YF, Yung TC, Tam SC, Ho MH, Chau AK. Novel and tradi-tional cardiovascular risk factors in children after Kawasaki disease:implications for premature atherosclerosis. J Am Coll Cardiol.2004;43:120–124
229. Fujiwara T, Fujiwara H, Nakano H. Pathological features of coronaryarteries in children with Kawasaki Disease in which coronary arterialaneurysm was absent at autopsy. Quantitative analysis. Circulation.1988;78:345–350
230. Yamakawa R, Ishii M, Sugimura T, et al. Coronary endothelial dys-function after Kawasaki disease: evaluation by intracoronary injectionof acetylcholine. J Am Coll Cardiol. 1998;31:1074–1080
231. Albisetti M, Chan AK, McCrindle BW, et al. Fibrinolytic response tovenous occlusion is decreased in patients after Kawasaki disease. BloodCoagul Fibrinolysis. 2003;14:181–186
232. Deng YB, Li TL, Xiang HJ, Chang Q, Li CL. Impaired endothelialfunction in the brachial artery after Kawasaki disease and the effects ofintravenous administration of vitamin C. Pediatr Infect Dis J. 2003;22:34–39
233. Furuyama H, Odagawa Y, Katoh C, et al. Altered myocardial flowreserve and endothelial function late after Kawasaki disease. J Pediatr.2003;142:149–154
234. Silva AA, Maeno Y, Hashmi A, Smallhorn JF, Silverman ED, Mc-Crindle BW. Cardiovascular risk factors after Kawasaki disease: acase-control study. J Pediatr. 2001;138:400–405
235. Furuyama H, Odagawa Y, Katoh C, et al. Assessment of coronaryfunction in children with a history of Kawasaki disease using (15)O-water positron emission tomography. Circulation. 2002;105:2878–2884
236. Suzuki A, Yamagishi M, Kimura K, et al. Functional behavior andmorphology of the coronary artery wall in patients with Kawasakidisease assessed by intravascular ultrasound. J Am Coll Cardiol.1996;27:291–296
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unlessreaffirmed, revised, or retired at or before that time.
AMERICAN ACADEMY OF PEDIATRICS 1733 by guest on April 10, 2019www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2004-21822004;114;1708Pediatrics
Thomas J. Pallasch, Donald A. Falace and Kathryn A. TaubertRobert S. Baltimore, Walter R. Wilson, Larry M. Baddour, Matthew E. Levison,
Lloyd Y. Tani, Jane C. Burns, Stanford T. Shulman, Ann F. Bolger, Patricia Ferrieri, Jane W. Newburger, Masato Takahashi, Michael A. Gerber, Michael H. Gewitz,
Young, American Heart AssociationEndocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in theStatement for Health Professionals From the Committee on Rheumatic Fever, Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/114/6/1708including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/114/6/1708#BIBLThis article cites 217 articles, 46 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/cardiology_subCardiologybhttp://www.aappublications.org/cgi/collection/infectious_diseases_suInfectious Diseasefollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on April 10, 2019www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2004-21822004;114;1708Pediatrics
Thomas J. Pallasch, Donald A. Falace and Kathryn A. TaubertRobert S. Baltimore, Walter R. Wilson, Larry M. Baddour, Matthew E. Levison,
Lloyd Y. Tani, Jane C. Burns, Stanford T. Shulman, Ann F. Bolger, Patricia Ferrieri, Jane W. Newburger, Masato Takahashi, Michael A. Gerber, Michael H. Gewitz,
Young, American Heart AssociationEndocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in theStatement for Health Professionals From the Committee on Rheumatic Fever, Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A
http://pediatrics.aappublications.org/content/114/6/1708located on the World Wide Web at:
The online version of this article, along with updated information and services, is
1073-0397. ISSN:60007. Copyright © 2004 by the American Academy of Pediatrics. All rights reserved. Print
the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on April 10, 2019www.aappublications.org/newsDownloaded from