Embed Size (px)
Citation preview

Volume 33. Number 2. June 2016
AMERICAN ACADEMYOF COSMETIC SURGERY
The American Journalof Cosmetic Surgery
Carbon Dioxide-Assisted Pneumodissection in Fat Grafting
A Personal Approach for Abdominoplasty
Internet Access to Advanced 3-Dimensional Software for the Prototypingand Design of Complex and Precise Custom Mandibular Implants
Comparison of Permanent Versus Absorbable Suture in the Tongue-in-Groove Technique in Endonasal Rhinoplasty
Vision Loss in a Young. Healthy Woman Following Liposuction
ADVANCING THE MULTI-SPECIALTY, GLOBAL DISCIPLINE
OF COSMETIC SURGERY AND MEDICINE FOR THE
"•&£NEFIT OF PATIENTS AND PRACTITIONERS
ajcs.sagepub.com • ajcsonline.org
==== .̂.. ISSN: 0748-8068

Article
Internet Access to Advanced3-Dimensional Software for thePrototyping and Design of Complex andPrecise Custom Mandibular Implants
(The American Journal ofCosmetic Surgery2016, Vol. 33(2)83-90©The Author(s)20l6Reprints and permissions:sagepub.com/journalsPermissions.navDOI: I O.I 177/0748806816648677acs.sagepub.com
®SAGE
William J. Binder, MD1 and Karan Dhir, MD1
AbstractA large percentage of patients with microgenia requesting chin augmentation also exhibit an associated component ofmicrognathia with either narrow or acutely angled mandibular bodies and/or hypoplasia of the gonial angles. Augmentationof the face and mandible should optimally address all regions of deficiency and can now be customized with a high degreeof accuracy using software that can be accessed over the Internet. We discuss the advanced capabilities of merging asophisticated software system (Geometric Freeform® software; Morrisville, North Carolina) and computed tomography(CT) imaging to design precise, total custom mandibular implants over the Internet without the need for physical modeling.In revision cases, this process also allowed for the implant to be removed and replaced within a single-stage procedure.We retrospectively reviewed 34 cases in an outpatient surgical center and described the preoperative evaluation, imagingprotocol, customization process, and surgical procedure for custom mandibular and custom total mandibular augmentation.Between January 2004 and June 2015, 25 patients underwent total mandibular augmentation and 9 had custom extendedmandibular angle and body augmentation. All patients received solid silicone rubber implants that were customized usingvirtual or acrylic prototypes digitally designed via real-time video conferencing. This custom process achieved an enhancedlevel of satisfaction with an improved ability to achieve symmetry based on quantitative measurements during the interactivedesign process, alloplastic facial implants can be customized with a high degree of accuracy, precision, and fit by combiningthe capabilities of 3-dimensional CT and advanced computer design software accessed via the Internet.
Keywordscustom mandibular implant, facial implants, chin augmentation, gonial angle implants, revision facial implants, facial plasticsurgery, silastic facial implants
Introduction
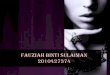
The use of alloplastic materials in facial augmentation has beenwell established and is increasingly recognized as a key compo-nent in the correction and restoration of skeletal contour defects.In particular, implants play a prominent role in aesthetic facialcontouring and the remediation of soft tissue volume loss inrejuvenating the aging face.'"3 Early designs of prefabricatedimplants attempted to solve various challenges faced by recon-structive and aesthetic surgeons; however, the ability to improvethe design of complex anatomical shapes was limited to thetechnology of the day (Figure 1 A). Preliminary efforts to cus-tomize implants for complex cases were extrapolated from afacial moulage created over soft tissue topography (Figure IB).This approach attempted to approximate topographical volume
and variation but resulted in an implant that was poorly adaptedto the underlying facial skeleton. Over the past decade, innova-tive advancements in computer technology have vastly
improved the customization process to adapt the facial prosthe-ses to the underlying bony topography with a greater degree ofprecision, fit, and reliability. Tn the mid-1980s, computedtomography (CT) imaging replaced standard radiographic tech-niques, resulting in the evolution of computer-aided design and
'University of California, Los Angeles, USA
Corresponding Author:William J. Binder, 120 S. Spalding Drive, Suite 340, Beverly Hills,CA 90212, USA.Email: [email protected]

84 The American Journal of Cosmetic Surgery 33(2)
Figure I. (A) Early prefabricated implants were limited by the technology of the day that hindered the production of complex,anatomically correct allografts. The resulting facial contour and projection were not aesthetically pleasing secondary to inaccuraciesin volume and anatomic skeletal enhancement. (B) Early customized implants borne from facial moulage and designed over soft tissuetopography did not adapt to the underlying skeletal surface, were unstable, and increased the risk of displacement. (C) Improvementsin radiographic imaging and medical modeling allowed for molding of wax elastomer over an anatomically correct skeletal surfacefor improved customization and fit. Major asymmetry, inaccuracies in the degree of augmentation, and revision cases pose ongoingchallenges in customizing implants.
manufacturing methods that use CT topographical data to pro-duce anatomically correct 3-dimensional (3D) resin stereolitho-graphic medical models (Figure 1C).4 This not only enhancedthe ability for surgical planning and execution in orthognathicsurgery but also vastly improved the dependability of restor-ative onlay modalities.
In correcting contour skeletal deficiencies, the implantcustomization process has traditionally relied upon the useof wax and silicone clay to form and fit onlay implants overskeletal models. The wax and silicone clay molds were thenconverted to silastic implants that were better adapted to theunderlying skeletal surface and produced favorable out-comes (Figure 1C).1"3 This traditional approach to custom-izing implants, however, had several shortcomings. First, itdid not achieve the optimal, aesthetically correct degree ofaugmentation due to the limited ability to precisely quantifyvolume, dimension, and asymmetry. Second, determiningthe method and approach to aesthetic augmentation wassubject to the surgeon's sole discretion based on the patient'sdesires and input during the initial consultation. Althoughthe design process primarily relies upon the experience ofthe surgeon and his ability to visualize and align the amountof augmentation and contour, the implant must ultimatelycoincide with both the patient's and surgeon's ideal of theend result. The ability to accurately predict and quantify theamount of augmentation remains an ongoing inherent limi-tation in all common chin or malar augmentation proce-dures. Therefore, adopting a method to assist in quantifying
the degree of augmentation can be extremely useful to theaesthetic surgeon.
Facial asymmetry, particularly in revision cases with exist-ing implants, poses a major impediment to fabricating newimplants by obscuring the ability to accurately estimate sizeand dimension. This in turn hinders the ability to replace facialimplants in a single-stage procedure. As such, past technologyto customize implants was limited in the ability to subtract pre-viously inserted implants and accurately address the complexi-ties of revision cases without necessitating multiple surgicalprocedures. Prefabricated implants are difficult to customizeintraoperatively around areas of significant topographical vari-ability and abrupt surface changes. Moreover, attempts to opti-mize symmetry and the degree of augmentation may be furtherchallenged by areas of osteoresorption and/or osteoneogenesispresenting from the region of the pre-existing implant.
The merging of capabilities offered by 3D CT imaging, 3Dcomputer-aided modeling software, and the Internet repre-sents a major contemporary advancement that enables the cus-tomization of facial implants while overcoming manylimitations of prior methods. In this approach, the reconstruc-tive and aesthetic surgeon can customize facial prostheses ona virtual platform by combining video conferencing protocolsand collaboration with live technical support to design 3Donlay prostheses. This combined approach is performed digi-tally, thereby forgoing the absolute need for the physical modelitself (Figure 2 A). Digital measuring tools and techniques cannow optimize the degree of 3D augmentation, quantify facial

Binder and Dhir 85
Figure 2. (A) With the advent of improvements in 3D digital software and CT resolution, the surgeon can now customize facialprostheses on a virtual stage by combining video conferencing protocols and collaboration with a live technical support staff. Theenhanced design process can measure and account for inherent asymmetries and variations in skeletal topography, which results ina highly accurate onlay customized implant. (B) The improved ability to measure, subtract, or overlap previously inserted implantedmaterials allows customized implants to be designed to the specifications of the topography of the underlying mandible and alleviates theneed for multistage (removal and replacement) procedures.Note. 3D = 3-dimensional; CT = computed tomography.
asymmetry, and measure, subtract, or overlap previouslyimplanted materials without the need for multistage removaland replacement procedures (Figure 2B). The software tech-nology also enhances the assessment of spatial orientation andrefines the implant design by accurately measuring asymmet-rical differences. This improves precision in quantitativelypredicting the amount of augmentation required (Figure 3A).Ultimately, the surgeon can become intimately familiar withthe process of designing custom implants, particularly in refin-ing the inherent differences and variations in skeletal anatomyand improving the ability to appreciate all 3D discrepancies.
The capacity for virtual mirroring, a primary benefit of thecomputer design, allows for precise matching of shape andcontour while measuring the actual amount of augmentationrequired for the implant to match the contralateral side.4 Thisdesign process has been utilized in customizing implants formandibular reconstruction as well as enhancing skeletal defi-ciencies in the midface and forehead.5
In this article, we retrospectively reviewed 34 cases anddescribed the design process, surgical procedure, manage-ment, outcomes, and complications of 3D customized implantsfor the augmentation of the entire mandibular complex.
Materials and Methods
Design and Fabrication of the Custom Implant
The preoperative evaluation includes a review of the patient'sprevious surgical and medical history and CT radiographicimaging reformatted into a 3D image. A radiographic evaluation
of the region to be augmented is performed whereby the targetarea is scanned with a slice thickness of 0.625 to 1.2 mm, andthe surrounding areas are scanned using low-dose techniques ofgreater thickness.6 This method ensures minimal radiationexposure with complete CT assessment of the proposed area ofaugmentation. Once the scan is completed, DICOM (DigitalImaging and Communications in Medicine) images are trans-ferred to the commercial manufacturer where the design processis initiated. Commercially available software is utilized to refor-mat the DICOM images into 3D skeletal and soft tissue images.Careful examination, analysis, and measurement of the virtualimage are extremely useful in planning the implant design. Thedata are then uploaded to a commercial platform (3D Systems,Inc., Golden, Colorado). Using the Geometric Freeform© soft-ware, the technician manipulates a tactile joystick to emulate thephysical process of sculpting clay to mold the implant to theunderlying bony topography in 3 dimensions.
The surgeon is able to view the process over a peer-to-peernetworking Internet protocol that allows him or her to com-municate with the technician in real time. The technician canvisually demonstrate 3D quantitative and qualitative digitaldata while utilizing virtual mirroring techniques to improvesymmetry along a measurable midsagittal plane. As preexist-ing silicone or expanded polytetrafluoroethylene (ePTFE)implants can be visualized on CT and measured, new implantscan be designed around these types of implants. In contrast,polyethylene (MEDPOR®; Stryker, Kalamazoo, Michigan)implants appear radiolucent or transparent on CT imagingand cannot be visualized. However, the density of theMEDPOR implant differs from that of bone and can be

86 The American journal of Cosmetic Surgery 33(2)
Figure 3. (A) Early attempts to customize implants were limited by variations due to asymmetry as well as difficulty in quantifyingthe degree of augmentation necessary for precise correction and contour. Currently, the merging of 3D CT imaging capabilities and3D computer-aided modeling software represents a major advancement in the method for measuring asymmetrical differences andimproving accuracy in quantitatively predicting the amount of augmentation required. (B) Detaching the anterior mental ligament at itsinsertion bilaterally allows for subperiosteal dissection to progress along the inferior border of the mandible and reduces the tendencyfor the dissection vector to be directed superiorly. This maneuver decreases risk of injury to the mental nerve intraoperatively anddeters implant displacement superiorly during fibrosis postoperatively (left). Anterior mandibular ligament detachment at lateral incisionborder corresponding to radiographic imaging (right). (C) When inserting a single, whole implant, the gonial angle must be relativelysmall to limit injury to the mental nerve at the mental foramen. Alternatively, the implant may be cut in the midline and each hemi-implant is passed retrograde via the intraoral incisions and then reapproximated in the midline.Note. 3D = 3-dimensional; CT = computed tomography.
discerned by the freeform software for digital subtraction.7The final customized implant design file is then transmitted,and a negative mold is produced through 3D printing. Thefinal custom implant is then commercially produced from thecomputer mold into a solid silicone rubber implant (Figures2A and 3A) Implantech Associates, Inc., Ventura, CA).
Surgical Technique for the Insertion of theCustom Total Mandibular Implant
The surgical placement of a total (angle-to-angle) mandibu-lar implant is performed under general endotracheal orlaryngotracheal mask anesthesia. The approach involves a
1- to 1.5-cm external submental incision and 2 intraoralangle or gonial incisions. A subperiosteal plane is dissectedover the anterior surface of the mandible while limiting thesuperior extent of dissection to the vertical height of the chincomponent of the implant. Further surgical dissection iscontinued posteriorly with a 4-mm periosteal elevator alongthe parasymphyseal area and below the mental foramenbilaterally.'"3 Surgical dissection along the inferior border ofthe mandible is aided by detaching the anterior mental liga-ments lateral to the submental incision (Figure 3B). Thisallows the dissection to progress along the inferior border ofthe mandible and reduces the tendency for the dissectionvector to be directed superiorly, thereby minimizing

Binder and Dhir 87
potential injury to the mental nerve. This is the standardprocedure for inserting an extended chin implant.
The posterior gonial incisions arc made slightly lateral tothe gingivobuccal sulcus to maintain a cuff of mucosa forample primary closure. Wide (1-1.2 cm) periosteal elevatorsare utilized for subperiosteal dissection along with elevationof the overlying masseter muscle to reduce the risk of pene-trating injury to the surrounding soft tissue and overlyingmuscle fibers. The posterior dissection is additionally con-trolled by placing the opposite hand held firmly against theborder of the mandibular angle and ramus, preventing slip-page of the elevator in a posterior direction. The massetermuscle is carefully dissected from the inferior ramus and thedissection pockets are joined to the anterior mandibularpocket previously dissected.
There are 2 approaches used for the placement of a totalmandibular implant. Large implants can be inserted in 1piece via the submental incision if the gonion component isrelatively small (Figure 3C). Alternatively, if the gonioncomponent is thick or has excess bulk, the silicone implant isthen cut in the midline prior to implantation, inserted via aretrograde to antegrade direction, and passed through thegonial incisions. As the implant is advanced under the mentalnerve, the risk of injury is avoided by expanding adequatedissection along the inferior border of the mandible whileretracting the soft tissues interiorly through the submentalincision. With age or in the edentulous patient, the surgeonshould be aware of a decrease in the vertical height of themandibular body due to bone resorption; however, the dis-tance between die inferior border of the mandible and mentalforamen remains relatively constant.8'9 Any large degree ofresorption is found to occur in patients beyond the seventhdecade of life and is observed mostly along the alveolarridge, mandibular angle, ramus, and prejowl region.9'10
Intraoperatively, a 2.0 silk suture assists with passing of theimplant along the mandibular pocket. The suture is placedthrough the anterior or mental portion of the hemi-implant. Along clamp is carefully inserted into the submental incisionand passed below the mental foramen and extended laterallyuntil the head of the clamp is directly visible within the intra-oral goniat pocket. The suture loop is threaded between thetines of the clamp, and the implant is advanced toward themidline. Once both sides are seated correctly, the anterior endsof the implant appose each other in the midline. The bilateralimplants are adjoined in the midline with permanent 4-0 clearnylon or polydioxanone suture (PDS) interrupted sutures.
The anterior inferior portion of the implant is furthersecured by suturing it to the periosteum along the inferiorborder of the mandible through the submental incision. Iffurther fixation of the gonial portion of the implant is desired,a self-drilling screw may be secured either through the gonialincision or via a direct percutaneous approach. A small screwis used to engage the cortex for approximately 1 to 1.5 mmthereby avoiding the inferior alveolar canal. If excessivebleeding occurs, drains are inserted into the intraoral pockets
and usually removed the next day. All incisions are closedprimarily. A compressivc contour dressing is applied by plac-ing Elastoplast over the entire mandible for tamponade. Thepatient may be discharged either to home with supervision orto an aftercare facility (Figure 4A-D).
Results
During the period from January 2004 to June 2015,25patientsunderwent custom total mandibular implantation and 9underwent extended custom gonial angle and body augmen-tation utilizing the virtual custom design process. Patientswere followed postoperative for at least 1 year to up to 6years. All implant surgeries were performed in an outpatientambulatory surgical care center. Of the 25 patients whoreceived a total mandibular implant, 12 were revision casesfrom previously inserted chin implants and/or mandibularangle implants of various biomaterials. Each revision casewas completed in a single-stage procedure. The preexistingimplants in 5 of the 12 revision cases were silicone, 5 wereMEDPOR, 1 was ePTFE, and 1 was Proplast; all revisioncases were reimplanted with silicone elastomer implantsdesigned from the digitally produced molds. Patients weredischarged subsequently to either an aftercare facility or tohome care. The custom process produced an enhanced levelof satisfaction with an improved ability to achieve symmetrybased on quantitative measurements. (Figures 4-6).
Complications included 2 (5%) cases of incision sitegranulomas, 3 (8%) cases of seroma/hematoma that wereacutely drained, and 2 (5%) cases of local, unresolved infec-tion that necessitated implant removal. Of the 2 patientsrequiring implant removal, one patient had a second implantreinserted without incident, and the second patient electednot to have the implant reinserted.
Discussion
The customization process can assist the aesthetic and recon-structive surgeon in accurately designing implants to solve amultitude of problems arising from the use of prefabricatedor custom implants previously designed using physical mod-eling techniques. The senior author has over 20 years ofexperience utilizing clay modeling for customized implantsand these patients have not been included herein.
In patients with facial asymmetry, the most notable asym-metry is found in the lower third of the face.11 A large percent-age of patients with microgenia have a relative component ofassociated micrognathia with either narrow or acutely angledmandibular bodies and/or hypoplasia of the gonial angles.Minor or major degrees of asymmetry in the ramus, angle,symphysis, or body can also accompany the relative deficien-cies that are associated with the entire mandible." Utilizing thecustom process, implants can now be designed and fabricatedto encompass all areas of the mandible while compensating forits asymmetrical contour, shape, and the inherent variability.

88 The American Journal of Cosmetic Surgery 33(2)
Figure 4. (A and C) Preoperative photographs of a patient demonstrating microgenia with a poorly defined jawline and gonial angle.(B and D) Postoperative photographs of the same patient (in A and C) after the custom total mandibular implant resulting in a boldmandibular contour.
Figure 5. (A) Preoperative lateral view of a chin implant previously placed in an incorrect location about 1.0 cm above the inferiormandibular border. In addition, there is neck skin laxity in conjunction with an overall weak mandibular skeletal framework including adecrease in mandibular length, height, and chin projection. (B) One-year postoperative lateral view. Total custom mandibular implantaugmentation of all 3 regions of the mandible including the gonial angle, parasymphysis, and symphysis was performed without any softtissue or rhytidectomy (face or neck) procedures. A robust facial skeletal structure redistributes the soft tissue over a well-definedjawline, rendering an improved cervicomental angle and more youthful appearance.
Treating a single area with prefabricated gonion angleimplants in conjunction with chin augmentation does notaddress mandibular parasymphyseal and body deficiencies.However, by utilizing the customization process, the sur-geon can now create custom total mandibular implants that
address all regions of mandibular deficiency, which in turnmay confer a higher degree of surgeon confidence, predict-ability, and patient satisfaction. This is a novel approach forfacial contouring of the lower third of the face by ameliorat-ing the gap, or indentation, that occurs at the junction of

Binder and Dhir 89
Figure 6. (A) The custom design process allows for novel approaches to facial contouring in areas including the cranium, midface, andentire mandible. The aesthetic objectives are achieved through improved quantification of volume, dimension, and asymmetry on a virtualstage. (B-D) Preoperative and postoperative photographs of a patient who underwent rhinoplasty facial implantation of the cranium,midface, and total mandible utilizing the 3D virtual custom design process. Postoperative photographs demonstrate improved symmetry,dimension, and aesthetic contour matching the patient's preoperative objectives.
anterior mandibular with gonial angle implants in the para-symphyseal region, thus providing a straight mandibularline that is sought in facial aesthetic surgery.
During the initial consultation, the patient's facial contourgoals are discussed and the augmentation options continue toinclude standard prefabricated implants in addition to cus-tomized implants. For patients with extreme facial skeletaldeformities and/or malocclusion, orthognathic surgical con-sultation is warranted. The safety and technical ease to insertcustom total mandibular implants has evolved to be in linewith a standard chin augmentation surgical approach utiliz-ing a single external incision. Conversely, the custom pro-cess utilizes an outside technician and facility(3D Systems,Inc.; Golden, CO) that results in an increased cost for thedesign time. The additive cost to the customization processmust be weighed and considered based on the goals of thepatient, and the surgeon's need for technology to provide animproved fit for primary cases with gross asymmetry revi-sion cases, and when dealing with the parasymphyseal
deficiency that often occurs with prefabricated implants. Forpatients with microgenia and appropriate gonial angle pro-jection, a standard prefabricated chin implant remains thestandard and can be modified intraoperatively by shaving theimplant for symmetry and proper sizing.
In aesthetic surgery, it is well established diat a robustskeletal framework can provide a better foundation enablingimproved and longer lasting effects of facial soft tissue pro-cedures.1"3'9'12 Similarly, it is well known that utilizing allo-plastic augmentation to address skeletal volume deficiencies,particularly those resulting from the aging process, can dra-matically enhance the results of rhytidectomy.3 Extending oraugmenting any of the key areas of deficiencies in the facialskeleton such as the chin, midface, and gonion angleimproves the skeletal framework and facilitates more appro-priate soft tissue draping (Figure 5). In many cases, the for-mation and recurrence or accentuation of the jowl particularlyafter rhytidectomy can result from an unrecognized skeletaldeficiency of the gonial angle posterior to the soft tissue

90 The American journal of Cosmetic Surgery 33(2)
component. We refer to these cases as the reformation of the"pseudo-jowl" where post-face-lift patients present with arelatively tight soft tissue envelope, but with a persistence ofthe jowl that appears to be aggregated at the mid-portion ofthe mandible posterior to the mandibulocutaneous ligamentand anterior to a deficient skeletal gonial angle (Figure 6Aand B). In addition, the virtual custom design process allowsfor the application of novel facial contouring tactics to allregions of the face, including the midface and cranium, tomeet the expectations of both the patient and surgeon. Wepresent a 35-year-old male with a prior history of foreheadimplantation who had requested consultation for facial con-touring utilizing the custom design process. The patientarrived with specific aesthetic requests based on his ideals offacial contour. During the consultation, he desired a well-defined, lowered superior orbital rim with a well-projectedforehead, malar implantation, and improved mandibular con-tour along all 3 segments of the mandible.
Utilizing the customization process described here, wesubtracted the existing forehead implant virtually anddespite an irregular skeletal topography, designed a smoothcontoured prototype. A total mandibular implant was alsodesigned to address areas of micrognathia and microgeniawith the aesthetic goal of achieving a "square chin" andbold jawline (Figure 6A). The forehead implant was surgi-cally implanted via a bicoronal approach in a single-stageremoval and replacement procedure. The malar implantsand mandibular implants were later implanted as describedearlier (Figure 6B-D).
Conclusions
We described a process that utilizes contemporary technol-ogy to converge digital imaging and computer-aided designmodalities into a practical, reproducible method for implantcustomization. This method yields highly predictable resultsin areas of the face that are particularly difficult to accuratelyand symmetrically augment when using off-the-shelf, pre-fabricated alloplastic implants. Customizing alloplasticimplantation of the facial skeleton can be accomplished witha high degree of accuracy, precision, and fit by leveraging thecombined capabilities of 3D CT imaging and Internet videoconferencing protocols offered by the sophisticated designsoftware. As such, at the preference of the surgeon, custom-izing implants can now also be performed without the abso-lute need for obtaining the physical model. Moreover, thisprocess facilitates a collaborative approach to fulfilling the
patient's aesthetic goals by availing input from a highly pro-ficient software technician who can assist the surgeon inachieving the anatomical objectives of the procedure.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interestwith respect to the research, authorship, and/or publication of thisarticle: Dr. Binder is a shareholder and consultant of ImplantechAssociates, Inc.
Funding
The author(s) received no financial support for the research, author-ship, and/or publication of this article.
References
1. Binder W, Kaye A. Utilizing 3-D computer modeling to cre-ate custom-designed implants to reconstruct posttraumatic andcongenital facial contour deformities. Plast and Reconstr Surg.1994;4^(6):775-785.
2. Binder WJ. Submalar augmentation: an alternative to face-liftsurgery. Arch Otol Head Neck Surg. 1989;//5(7):797-801.
3. Binder WJ. Facial rejuvenation and volumization usingimplants. Facial Plast Surg. 2011 ;27:86-97.
4. Goldsmith D, Horowitz A, Orentlicher G. Facial skeletal aug-mentation using custom facial implants. Atlas Oral MaxillofacSurg Clin North Am. 2012;20(1):119-134.
5. Rotaru H, Stan H, Florian IS, et al. Cranioplasty with custom-made implants: analyzing the cases of 10 patients. J OralMaxillofac Surg. 2012;70(2):el69-el76.
6. Benazzi S, Senck S. Comparing 3-dimensional virtual meth-ods for reconstruction in craniomaxillofacial surgery. J OralMaxillofac Surg. 2011;69(4):1184-1194.
7. Schatz CJ, Ginat DT. Imaging of cosmetic facial implantsand grafts. AJNR Am JNeuroradiol. 2013;34(9):1674-1681.
8. Mittelman H, Spencer JR, Chrzanowski DS. Chin region: man-agement of grooves and mandibular hypoplasia with alloplas-tic implants. Facial Plast Surg Clin North Am. 2007;7J(4):445-460.
9. Shaw RB, Katzel EB, Koltz PF, ct al. Aging of the facial skel-eton: aesthetic implications and rejuvenation strategies. PlastReconstr Surg. 2010;/27(l):374-383.
10. Kahn DM, Shaw RB. Overview of current thoughts onfacial volume and aging. Facial Plast Surg. 2010;26:350-355.
11. Kim SJ, Lee KJ, Lee SH, Baik HS. Morphologic relationshipbetween the cranial base and the mandible in patients withfacial asymmetry and mandibular prognathism. Am J OrthodDentofacial Orthop. 2013;W(3):330-340.
12. Binder W. Custom Designed Facial Implants. Facial PlastSurg Clin North Am. 2008; 16: 133-146.