Embed Size (px)
Citation preview

AmblyopiaAmblyopiaNew knowledge and practical approachesNew knowledge and practical approaches
ESA 2007ESA 2007
Early morning courseEarly morning course
May 21, 2007May 21, 2007
Daisy Godts CO, Ilse De Veuster MDUniversity Hospital Antwerp

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
AmblyopiaAmblyopia
• Pubmed:
– 5829 amblyopia
– 3051 amblyopia treatment
– 2860 amblyopia therapy
– 490 amblyopia occlusion
– 149 amblyopia patching
– 122 amblyopia atropine
– 70 amblyopia penalization
– 5 amblyopia inverse occlusion

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Definition of amblyopiaDefinition of amblyopia
Amblyopia is a diagnosis of exclusion
Because the basis is defective central visual processing,
careful assessment of the retina and optic nerve is
essential
The diagnosis is established by a unilateral or bilateral
reduction of BCVA not entirely attributable to structural
abnormalities of the visual pathways
PPP AAO 2002: Amblyopia

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Definition of amblyopiaDefinition of amblyopia
• VA 2 / 3 lines ( < 20/50 3 years of age / <
20/40 5 years of age) / fixation behaviour
• No differences with corrective lenses
• Amblyopia inducing factor present
• Onset : immature visual system
• Prevalence : 2-4% general population
PPP AAO 2002: Amblyopia

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Definition of amblyopiaDefinition of amblyopia
• Pattern deprivation
• Strabismus :
– Synchronous stimulus of visual cortex of non corresponding images of two foveas
– Binocular rivalry => suppression
• Optical defocus
– Refractive error removes fine details from the retinal image
– Anisometropia : 100% amblyopia risk : +4D/-6D vs 50% +2,5D/-4D

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Pathofysiological mechanismsPathofysiological mechanismsType of amblyopia
Abnormal binocular
interaction
Visual image distortion
Strabismic +
Refractive: Ametropia Anisometropia +
++
Deprivation: Unilateral Bilateral
+ ++
Organic: Unilateral Bilateral
+ ++
Focal Points AAO volume XVIII nr 2, March 2000 : Practical management of amblyopia

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
ManagementManagement
Two principles
• Optimise clarity of retinal image in the amblyopic
eye: clear visual axis + correction of refractive
errors
• Increase cortical processing of visual input of
amblyopic eye = enhance the neural stimulus to
the visual cortex

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
ManagementManagement
• Parent’s explanation !!!!
• Surgery if necessary
• Optical correction : spectacles, contact lenses
• Patching/occlusion
• Atropine/penalization/optical
penalisation/defocus

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
ManagementManagement
Response is related to:
• Type of amblyopia
• Initial VA
• Age
• Duration of amblyopia
• Method of treatment
• Compliance

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Robbe 8 yearsRobbe 8 years
During screening low VA RE, consulted ophthalmologist:
too late, no treatment anymore. Second opinion
VA RE: 0.1 sc 0.25 +4.25 Logmar
VA LE: 1.0 sc
Cycloplegic refraction RE: +6.75 –0.75 x 150
LE: +4.00 -0.75 x 130
Straight eyes with fusion and moderate stereopsis
Central fixation BE
Anterior and posterior segment: normal
Therapy: +4.75/ +2.00

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Robbe 8 yearsRobbe 8 years
2 months control
VA RE: 0.3 cc Logmar
VA LE: 1.0 cc
BV: normal
8 hours occlusion LE
2 months control: good compliance
VA RE: 0.5 cc Logmar
VA LE: 1.0 cc
BV: normal
6 hours occlusion LE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Robbe 8 yearsRobbe 8 years
2 months control: good compliance
VA RE: 0.7 cc LogmarVA LE: 1.0 ccBV: normal4 hours occlusion LE
2 months control: good compliance
VA RE: 0.8- cc LogmarVA LE: 1.0 ccBV: normal2 hours occlusion LE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Steele A L, Bradfield Y S, Kushner B J, France T D, Struck M C, Gangnon R G . Successful Treatment of Anisometropic Amblyopia with Spectacles Alone. J AAPOS 2006;10:37-43
The mean time to resolution in this study was 5.8 + - 3.9 months with a range of 2 to 15 months
Age at presentation ranged from 0.8 to 7.9 years (mean 4.8, SD 1.7)
We analyzed age, best corrected initial visual acuity in the amblyopic eye, initial stereoacuity, type, and amount of anisometropia to assess which of these presenting characteristics are significantly associated with time to cure.
Worse initial visual acuity was significantly associated with longer time to resolution (P 0.05)
Anisometropia amblyopia : Anisometropia amblyopia : GlassesGlasses

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Anisometropic amblyopia : GlassesAnisometropic amblyopia : Glasses
• 3 - 7 years
• Anisometropia : 0,5D SE or 1,5 D astigmatism
• Prescription: hyperopia > 3D full or max –1,5D
• hyperopia < 3 D ( investigator )
• VA 20/40 – 20/250
• VA change : 2,9 lines +- 1,8
• 77% patients improvement of 2 lines
• Resolution of amblyopia ( VA 1 line) = 27%
• Amblyopia resolution ~ base line VA
~ magnitude of anisometropia
PEDIG Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmoly 2006; 113:895.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Aaron 4 yearsAaron 4 years
19/09/06 During screening low VA BE, consulted ophthalmologist: no treatment possible. Second opinion
VA RE: 0.10 sc LEA symbols VA LE: 0.20 sc
Cycloplegic refraction RE: +6.50 –1.75 x 0LE: -1.50 –1.50 x 0
Straight eyesAnterior segment: normalPosterior segment: RE normal, LE myelin vessels
Therapy: contact lenses +6.00 –1.75 x 0-1.50 –1.25 x 0

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
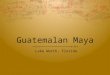
Aaron 4 yearsAaron 4 years
Posterior segment: RE normal, LE myelin vessels

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Aaron 4 yearsAaron 4 years
1 month control:
VA RE: 0.16 ccl LEA symbolsVA LE: 0.40 cclBV: normal
2 months control:
VA RE: 0.25 ccl LEA symbolsVA LE: 0.50 cclNear VA RE: 0.4/1.6 ccl
LE: 0.4/ 0.8 ccl6 hours occlusion LE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Aaron 4 yearsAaron 4 years
1 month control: good compliance to occlusion
VA RE: 0.40 ccl LEA symbols
VA LE: 0.50 ccl
Near VA RE: 0.4/1.0 ccl LE: 0.4/ 0.8 ccl
BV: normal
6 hours occlusion LE
2 months control: good compliance
VA RE: 0.60 ccl LEA symbols
VA LE: 0.60 ccl
Near VA RE: 0.4/1.0 ccl LE: 0.4/ 0.8 ccl
3 hours occlusion LE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Patching regimensPatching regimens
• 3 - 7 years
• Moderate amblyopia : 20/40 –20/80
• Anisometropic, strabismic and mixed amblyopia
• 2 hours + 1 hour near activity vs 6 hours + 1hr
• Age/base line acuity/ cause of amblyopia : no difference
• Results:
– 5 weeks: 2 hrs 1,84 lines improvement vs 1,92 line
– 4 months : 2,4 lines improvement in both groups
PEDIG A randomized trial of patching regimens for treatment of moderate amblyopia in children. Arch Ophthalmol 2003; 121: 603

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Patching regimensPatching regimens
• 3 - 7 years
• Severe amblyopia : 20/100 –20/400
• Anisometropic, strabismic and mixed amblyopia
• Full-time vs 6 hours + 1 hour near activity each
• Age/base line acuity/ cause of amblyopia : no difference
• Results:
– 5 weeks: 6 hrs 3.5 lines improvement vs 3.7 lines in FTO
– 4 months : 6 hrs 4.8 lines improvement vs 4.7 lines in FTO
PEDIG A randomized trial of prescribed patching regimens for treatment of severe amblyopia. Ophthalmology 2003; 110: 2075

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Argita 9 yearsArgita 9 years
10/11/06 first ophthalmological examination because poor VA during school examination, Roma gypsies
VA RE: 0.2 sc Logmar VA LE: 0.1 sc Cycloplegic refraction RE: +9.00 –2.00 x 170
LE: +10.00 –2.75 x 10
Straight eyesAnterior and posterior segment: normal
Therapy: +8.00 –2.00 x 170+9.00 –2.75 x 10

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Argita 9 yearsArgita 9 years
09/02/07 3 months of full-time spectacle wear
VA RE: 0.6 cc Logmar VA LE: 0.2 cc Micro-esotropia LE central fixation Therapy: 6 hours occlusion RE, control 2 months
17/04/07 good compliance to occlusionVA RE: 0.6 cc Logmar VA LE: 0.25 cc Micro-esotropia LE central fixation
Therapy: more/idem occlusion RE ? Stop occlusion?

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Treatment of amblyopia > 7 Treatment of amblyopia > 7 yearsyears
• 7 - 10,3 years (36 patients)
• Anisometropic, strabismic and mixed amblyopia
• Spectacles + full time occlusion/ total penalisation
• Follow up : 1 year after no further improvement in VA
• VA 20/50- 20/400 start ~ end 20/20 –20/30 for all patients
• Duration : 0,6 yrs aniso / 1,0 yrs strab / 0,8 yrs mix
• BV improved or maintained in 61% of cases
Mintz-Hittner H et al .Succesfull amblyopia therapy initiated after age 7 years. Arch Ophthalmology 2000;118: 1535

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Nikki 10 yearsNikki 10 years
Foster child since 1 year, abandoned by her parents
because of drug problems. Had glassed and occlusion long ago
VA RE: 1.0 sc Logmar
VA LE: 0.05 sc0.1 +5.OO –4.00 x 0°
Cycloplegic refraction RE: +2.50
LE: +6.25 –4.00 x 0°
CT: 12^esotropia LE
Central fixation BE
Anterior and posterior segment: normal
Therapy: Glasses?
Occlusion?

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Nikki 10 yearsNikki 10 years
Glasses RE + 1.25 LE + 5.00 –4.00 x 0°Full time occlusion RE
1.5 months: VA RE: 1.0 cc LogmarVA LE: 0.5 cc12^ETFull time occlusion RE
3 months: VA RE: 1.0 cc LogmarVA LE: 0.6 cc12^ETFull time occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Nikki 10 yearsNikki 10 years
5 months: Occlusion done 7- 8 hours
VA RE: 1.0 cc Logmar
VA LE: 0.6 cc
12^ET
4 hours occlusion RE
7 months: VA RE: 1.0 cc Logmar
VA LE: 0.7 cc
10^ET
Titmus: 4/9
2 hours occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Nikki 11 yearsNikki 11 years
9 months: VA RE: 1.0 cc Logmar
VA LE: 0.7 cc
10^ET’
Titmus 5/9, Lang I: positive
1 hour occlusion RE
12 months: VA RE: 1.0 cc Logmar
VA LE: 0.7 cc
10^ET’
Titmus: 5/9, Lang I & II: positive
1 hour occlusion RE once a week

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Nikki 12 yearsNikki 12 years
18 months: VA RE: 1.0 cc Logmar
VA LE: 0.7 cc
8^ET
Titmus 6/9, Lang I & II: positive
Stop occlusion RE
24 months: VA RE: 1.0 cc Logmar
VA LE: 0.7 cc
8^ET
Titmus: 5/9, Lang I & II: positive, TNO 240”

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Treatment of amblyopia > 10 Treatment of amblyopia > 10 yearsyears
• 10 - 18 years, 66 patients
• VA 20/40 –20/160
• Optimal optical correction > 4 wks
• Anisometropic, strabismic and mixed amblyopia
• Daily patching 2 hrs/day ( 1 hour of near visual
activity)
• 2 month follow up
• 18/66 (27%) VA improvement with 2 or more lines
• 10-14 years vs 14–18 years: no difference
PEDIG A prospective, pilot study of treatment of amblyopia in children 10 to < 18 years old. Am J Ophthalmol 2004;137: 581-583.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Treatment of amblyopia > 7 Treatment of amblyopia > 7 yearsyears
• 7 - 17 years, 507 patients
• 2 groups: younger group 7-12 years, older group 13-17 years
• VA 20/40 – 20/400
• Anisometropic, strabismic and mixed amblyopia
• Optimal optical correction alone or + 2-6h patching+atropine
• 24 weeks follow-up (6 weeks controls)
• Younger group: 53% improvement (patching+atropine)
25% improvement (optical correction)
• Older group: 25% improvement (patching)
23% improvement (optical correction)
• No diplopia
PEDIG Randomized trial of treatment of amblyopia in children aged 7 to 17 years. Arch Ophthalmol 2005; 123: 437-447

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Thomas 4 yearsThomas 4 years
Second opinion: glasses +4.00/+5.75 since age 2 year
occlusion 4h RE/day poor compliance
AV RE: 0.7 cc Snellen E
AV LE: 0.2 cc
Cycloplegic refraction RE: +4.50 –0.50 x 40
LE: +6.50 –1.00 x 150
Partial accommodative esotropia LE
Therapy: LE +6.00 –1.00 x 150
Occlusion RE at school

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Thomas 4 yearsThomas 4 years
3 months: Very poor compliance to occlusion
AV RE: 0.9 cc Snellen E
AV LE: 0.2 cc
= partial accommodative ET LE
Therapy: Atropine 0.50 % RE, plano glass RE
6 months: AV RE: 0.2 sc/atropine Snellen E
AV LE: 0.8 cc
Therapy: RE + 4.00 Stop atropine RE, 1 h alternate occlusion

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Thomas 5 yearsThomas 5 years
8 months: Good compliance to occlusion
AV RE: 0.8 cc Snellen E
AV LE: 0.8 cc
= partial accommodative ET LE
Therapy: 1 h alternate occlusion
14 months: Good compliance to occlusion
AV RE: 1.0 cc Snellen E
AV LE: 0.8 cc
Therapy: 2h occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Thomas 6 yearsThomas 6 years
20 months: Good compliance to occlusion
AV RE: 1.0 cc Snellen E
AV LE: 0.8 cc
near VA RE: 1.0 cc LEA
VA LE: 0.8 cc
= partial accommodative ET LE
Therapy: 2 h occlusion RE
26 months: Poor compliance to occlusion
AV RE: 1.0 cc Logmar
AV LE: 0.6 cc
Therapy: Atropine 0.5 % RE 2X week

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Thomas 7 yearsThomas 7 years
32 months: No atropine used, occlusion 2 h RE
AV RE: 1.0 cc Logmar
AV LE: 1.0 = cc
near VA RE: 1.0 cc LEA numbers
VA LE: 0.8+ cc
= partial accommodative ET LE
Therapy: 2 h occlusion RE 2-3 times a week

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Atropine vs patchingAtropine vs patching
• 3-7 years, 419 patients
• VA 20/40 – 20/100
• Anisometropic, strabismic and mixed amblyopia
• Occlusion > 6 hours vs atropine daily
• Results:
– 5 wks : 2,22 lines improvement occlusion vs 1,37
atropine
– 16 wks: 2,94 vs 2,42
– 6 months: 3,16 vs 2,84
• Patching = more rapid and possible slightly better VA
• Atropine easier administration and lower cost PEDIG. A randomized trial of atropine vs patching for treatment of moderate amblyopia in children. Arch 2002; 120: 268

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Atropine vs patchingAtropine vs patching
• 3-7 years, 419 children
• VA 20/40 - 20/100
• Anisometropic, strabismic and mixed amblyopia
• VA 6 months: 0,25 ( 20/30-2) atropine daily vs 0,21 (20/30)
occlusion (6h - FTO)
Age, depth of amblyopia, cause of amblyopia: no difference
Atropine as effective in VA 20/100 as when 20/40
Occlusion faster improvement especially when VA 20/80-
20/100 and when FTO or nearly FTO
PEDIG. A comparison of atropine and patching treatments for moderate amblyopia by patient age, cause of amblyopia, depth of amblyopia and other factors. Ophthalmology 2003; 110: 1632-1638.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Atropine vs patching : Atropine vs patching : 2 y follow-2 y follow-upup
• Follow-up 18 months after 6-months randomised trial
• 419 children age < 7 years
• Initial VA 20/40 to 20/100
• After 2 years: VA increased from baseline 3.7 lines
(occlusion 6h-FTO) and 3.6 lines (atropine daily)
• In both groups mean amblyopic VA was 20/32, 1.8 lines
worse than the sound eye (20/20)
Atropine or patching produced similar improvement of
moderate amblyopia in children age 3-7 yearsPEDIG Two-year follow-up of a 6 month randomized tral of atropine versus patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2005: 123: 149-157.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Glen 4 yearsGlen 4 years
10/11/04 first ophthalmological examination because poor VA during school examination
VA RE: 0.2 sc Snellen E VA LE: 1.0 sc Cycloplegic refraction RE: +1.75
LE: +1.75 –0.50 x 100
Esotropia RE, poor fixation possible eccentricAnterior and posterior segment: normal
Therapy: orthoptic consult

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Glen 4 yearsGlen 4 years
07/06/05 second opinion, low VA RE, no therapy done, consulted ophthalmologist did not know what to do
VA RE: 0.01 sc Snellen E VA LE: 1.0 sc
Cycloplegic refraction RE: +1.75 –0.50 x 105LE: +1.25 –0.25 x 100
Esotropia RE, no central fixation Anterior and posterior segment: normal
Therapy: 4 hours occlusion LE, control 4-5 weeks

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Glen 4 yearsGlen 4 years
15/11/05 Poor compliance to occlusion, max 1 hour
VA RE: 0.05 sc Snellen E
VA LE: 1.0 sc
Cycloplegic refraction RE: +1.75 –0.50 x 105
LE: +1.21 –0.25 x 100
Esotropia RE, poor fixation
Unstable fixation RE
Therapy: Atropine 0.5% LE + occlusion LE
Control 4 weeks

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Glen 5 yearsGlen 5 years
19/10/06 atropine used beginning last year, sometimes
occlusion done
VA RE: 0.1 sc Snellen E
VA LE: 1.0 sc
Esotropia RE, poor fixation
Central unstable fixation RE
Therapy: Full time occlusion (day and night)
6 weeks control

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Glen 5 yearsGlen 5 years
07/12/06 Good compliance
VA RE: 0.5 sc Snellen E VA LE: 1.0 sc Therapy: Full time occlusion, 6 weeks control
11/01/07 good compliance
VA RE: 0.8 sc Snellen EVA LE: 1.0 scTherapy: 6 hours occlusion, 8 weeks control
22/03/07 Good compliance
VA RE: 0.8 sc Snellen E VA LE: 1.0 sc
Therapy: 3 hours occlusion, 2 months control

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Compliance : occlusionCompliance : occlusion
• Poor parental fluency in the national language
• Low level of education
• Poor acuity at the start of treatment
An educational program primarily aimed at the child
improved compliance and reduced the number of
children who did not comply with occlusion at all
SE Loudon, M Fronius, CWN Looman, M Awan, B Simonsz, PJ van der Maas, HJ Simonsz: Predictors and a remedy for noncompliance with amblyopia therapy in children measured with the occlusion dose monitor.Invest Ophthalmol Vis Sci. 2006 Oct;47(10):4393-400.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Dixon Woods M et al. Why is compliance with occlusion therapy for amblyopia so hard? A qualitative study. Arch Dis Child 2006; 91: 491
Compliance : occlusionCompliance : occlusion
• Semi structured interviews ( n = 28 ) of parents of a child prescribed
patching ( 2 to 8 years : mean duration of patching: 3 months to 5
years)
• Problems with patching
– Begin of treatment/ extreme emotional reactions of child/ low VA ~ struggle with everyday life activities
– Social impact : risk of teasing
– Strain relationship child – parent
– Time consuming

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Compliance : occlusionCompliance : occlusion
• Strategies to support patching
– Explanation : need for patching
– Rewarding the effort with VA increase at follow
up/ attention and praise/ game / no big deal
– Normalisation strategies : toy with patch /other
children with patch
– Customising the patch :figures on the patch etc
– Establishing routine :structure and routine
– Support of others : teachers, day care workers
Dixon Woods M et al. Why is compliance with occlusion therapy for amblyopia so hard? A qualitative study. Arch Dis Child 2006; 91: 491

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Jef 4.5 yearsJef 4.5 years
Since 1.5 years glasses + occlusion RE during school
hours, no VA improvement, good compliance
VA RE: 1.0 sc 1.0 cc (+1.00) E linear
VA LE: 0.1 sc 0.1 cc (+3.00)
Cycloplegic refraction RE: +2.50
LE: +4.50
Partial accommodative esotropia LE
Parafoveal fixation LE
Anterior and posterior segment: normal

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Jef 4.5 yearsJef 4.5 years
Therapy: Inverse occlusion?

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Jef 4.5 yearsJef 4.5 years
1 month full time inverse occlusion LE
VA RE: 0.9 cc Linear EVA LE: <0.05 cc
Total fixation loss LE
R/ Full time occlusion RE, no bilateral fixation
1 month: VA RE: 0.6 cc Linear E
VA LE: 0.2+ cc
Central unsteady fixation LE
R/ Full time occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
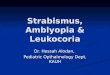
Jef 4.5 yearsJef 4.5 years
Central fixation RE Central unsteady fixation LE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Jef 5 yearsJef 5 years
3 months: Full time occlusion done
VA RE: 0.5 cc E linear
VA LE: 0.4 cc
Central fixation LE
ET RE
R/ Alternate occlusion
4 months: Alternate occlusion done
VA RE: 0.8- cc E linear
VA LE: 0.6- cc
ET LE
Central fixation
R/ 6 hours occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Jef 5 yearsJef 5 years
6 months: 6 hours occlusion done
VA RE: 1.0 cc E linear
VA LE: 0.6 cc
Central fixation LE
ET LE
R/ 6 hours occlusion RE
8 months: 6 hours occlusion done
VA RE: 1.0 cc E linear
VA LE: 0.8 cc
ET LE
Central fixation
R/ 4 hours occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Inverse occlusionInverse occlusion1. Pigassou-Albouy R. Treatment of eccentric fixation. Inverse
prism and occlusion. J Fr Ophtalmol. 1988;11(8-9):597-600. Review. French. No abstract available.
2. Koskela PU, Hyvarinen L. Contrast sensitivity in amblyopia. III. Effect of occlusion. Acta Ophthalmol (Copenh). 1986 Aug;64(4):386-90.
3. Blassmann K, Neuhann T. Treatment of amblyopia with soft occlusion lenses (author's transl). Klin Monatsbl Augenheilkd. 1978 May;172(5):766-70. German.
4. Andree G. The influence of inverse occlusion on fixation and function of amblyopic eyes. Albrecht Von Graefes Arch Klin Exp Ophthalmol. 1966 Aug 15;170(3):257-64. German. No abstract available.
5. Postic G. Influence of inverse and direct occlusion on the amblyopic eye with excentric fixation. Bull Mem Soc Fr Ophtalmol. 1966;79:305-66. French. No abstract available.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Celine 8 yearsCeline 8 years
During screening at school 1 year ago low VA LE, glasses
(-1.00 –0.50 x 110/-5.00 –3.00 x 145), no occlusion,
second opinion
VA RE: 0.8 cc Logmar VA LE: 0.3 cc
Cycloplegic refraction RE: -1.50LE: -4.75 –2.75 x 150
Straight eyes with peripheral fusion and central suppression
LE, poor stereopsis
Central fixation BE
Anterior and posterior segment: normal

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Celine 8 yearsCeline 8 years
6 weeks 4 hours occlusion RE
Good compliance
VA RE: 0.8 cc LogmarVA LE: 0.6=/0.7= cc
Near VA RE: 1.0 cc LEA numbers LE: 0.8 cc
BV: normal2 hours occlusion RE

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Celine 8 yearsCeline 8 years
3 months 1-2 hours occlusion RE
VA RE: 0.9 cc LogmarVA LE: 08= cc
Near VA RE: 1.0 cc LEA numbers LE: 0.8 cc
CT: straight eyesCentral and peripheral fusionGood stereopsisStop occlusion

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Celine 9 yearsCeline 9 years
Control 1 year
VA RE: 0.9 –2.50 LogmarVA LE: 08= –5.50 –2.75 x 150
Near VA RE: 1.0 cc LEA numbers LE: 0.8 cc
CT: straight eyesCentral and peripheral fusion
Good stereopsis

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Cessation of treatmentCessation of treatment
Bhola et al. Recurrence of Amblyopia After Occlusion Therapy. Ophthalmology 2006;Vol 113, 11: 2097-2100
• < 10 years (retrospective)
• Anisometropic, strabismic and mixed amblyopia
• > 8 hours patching daily
• 27% recurrence of amblyopia after 1 year ( 179 / 653)
by 2 logMAR levels
• Recurrence inversely correlated with patient age
• Important risk of recurrence when amblyopia therapy
is decreased before the age of 10 years

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Cessation of treatmentCessation of treatment
PEDIG. Risk of Amblyopia Recurrence After Cessation of Treatment J AAPOS 2004;8: 420-428.
• < 8 years
• Anisometropic, strabismic and mixed amblyopia
• >2 hours patching daily or > 1 drop atropine weekly
• VA <20/40 at enrollment, improvement of 3 logMAR
levels
• 24% recurrence of amblyopia after 52 weeks ( 35 /
145) by 2 logMAR levels
• Occlusion (n = 112) : 25 % recurrence
• Atropine (n = 33) : 21% recurrence

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Cessation of treatmentCessation of treatment
PEDIG. Risk of Amblyopia Recurrence After Cessation of Treatment J AAPOS 2004;8: 420-428.
• 2 h daily stop: low recurrence risk (14%)
• 6-8 h patching stop: high recurrence risk (42%)
• Patching hours should be weaned before treatment is
stopped

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Cessation of treatmentCessation of treatment
PEDIG. Factors Associated with Recurrence of Amblyopia on Cessation of Patching. Ophthalmology 2007
• < 8 years (prospective)
• Anisometropic, strabismic and mixed amblyopia
• 6-8 hours patching daily, stopped abruptly/weaned
• Risk of recurrence higher when:
• Better VA at the time of cessation
• More lines of improvement
• History of recurrence
• Orthotropia or good stereoacuity no protective effect

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
• 3-7 years
• Anisometropic, strabismic and mixed amblyopia
• VA 20/40 – 20/100
• Atropine, 6h patching or both
• Follow-up 2 years
• 14% new strabismus, 3% > 8 (atropine = occlusion)
• Microtropia (1-8 ): 36% resolution, 14% increase > 8
• Heterotropia > 8 : 20% resolution, 64% increase > 8
Adverse effects of treatment : Adverse effects of treatment : risk of strabismusrisk of strabismus
PEDIG. The Effect of Amblyopia Therapy on Ocular Alignment. J AAPOS 2005, Vol 9, 6: 542-545.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
• 3-7 years (419 patients)
• Anisometropic, strabismic and mixed amblyopia
• VA 20/40 – 20/100
• Atropine daily versus 6h-FTO occlusion
• 6 months : VA decrease 2 lines 17 patients in atropine
group, 3 patients in patching group
• 2 years: all patients normal VA (20/20) in both groups
Adverse effects of treatment : Adverse effects of treatment : VA sound eye decreaseVA sound eye decrease
PEDIG. Two-year follow-up of a 6 month randomized tral of atropine versus patching for treatment of moderate amblyopia in children. Arch Ophthalmol. 2005: 123: 149-157.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
• Mean age : 4 years
• Follow up : 54 weeks
• No difference between no treatment / only spectacles/ glasses + occlusion
• VA 6/9 – 6/36 no strabismus
Adverse effects of treatment : Adverse effects of treatment : stereo acuitystereo acuity
.Richardson SR et al. Stereoacuity in Unilateral Visual Impairment Detected at Preschool Screening: Outcomes from a Randomized Controlled Trial Invest Ophthalmol Vis Sci. 2005;46:150–154

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Adverse effects of treatment : Adverse effects of treatment : no successno success anisometropic amblyopiaanisometropic amblyopia
Hussein M AW et al. Risk Factors for Treatment Failure of Anisometropic Amblyopia . J AAPOS 2004; 8:429-434.
• 3-8 years
• 104 children with anisometropic amblyopia
• VA < 20/50, 3 lines interocular difference
• Anisometropia 1D
• Relative failure = failure of VA to improve 3
lines
• Functional failure = final VA < 20/40

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Adverse effects of treatment : Adverse effects of treatment : no successno success anisometropic amblyopiaanisometropic amblyopia
Hussein M AW et al. Risk Factors for Treatment Failure of Anisometropic Amblyopia . J AAPOS 2004; 8:429-434.
• Risk of functional failure
• Age above 6 years
• An initial visual acuity of 20/200 or worse
• Risk of relative failure
• Poor treatment compliance
• Astigmatism of 1,5D
• No risk
• Degree of anisometropia
• Type of refractive error
• Concurrent strabismus

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Do we change our habbitsDo we change our habbits
Questionaire to 380 pediatric ophthalmologists
• 39% no modification
• 33% rare adjustments
• 12% adapted amount of patching hours
Wygnanski-Jaffe T. The Effect on Pediatric Ophthalmologists of the Randomized Trial of Patching Regimens for Treatment of Moderate Amblyopia. J AAPOS 2005;9:208-211.

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts

UZ Antwerp ESA 2007 Daisy UZ Antwerp ESA 2007 Daisy GodtsGodts
Hope to see you in Antwerp !