Embed Size (px)
Citation preview

Please Mute Your Computer to Prevent Background Noise
Participants will be placed in the waiting room until the meeting begins at 6:00 PM CT
AMA Guides® Editorial PanelVirtual Panel Meeting
Thursday, November 18th, 2021
1

© 2021 American Medical Association. All rights reserved.2
Topics
• October Meeting Summary • Proposals to update the AMA Guides:
• ENT• fPROMs
• Closing of Public Meeting• Executive Session

© 2021 American Medical Association. All rights reserved.
Attendance• Attendance will be taken to establish a quorum.Panel Members
Panel Advisors
Helene Fearon, PTSteven Feinberg, MDDavid Gloss, MDRobert Goldberg, DORita Livingston, MD, MPH
Doug Martin, MDKano Mayer, MDMark Melhorn, MDLylas Mogk, MDMarilyn Price, MD
Noah Raizman, MDMichael Saffir, MDJan Towers, PhD
Chris Brigham, MDHon. Shannon Bruno Bishop, JDBarry Gelinas, MD, DC
Abbie Hudgens, MPAHon. David Langham, JD

© 2021 American Medical Association. All rights reserved.
Confidentiality/COI Reminders
• Confidentiality• It is at the discretion of the AMA, the publisher and convener, which topics, news items, or policy
decisions resulting from this or any Editorial Panel meeting will be announced publicly at the appropriate time. Until and unless the AMA makes such a public announcement, all discussion and decisions made during AMA Guides® Editorial Panel Meetings are confidential.
• Please refrain from tweeting or participating in podcasts, interviews, or news articles about Panel meetings, discussions, or deliberations. Recording devices by Panel members and co-chairs is strictly prohibited. The AMA will record all Panel meetings for reference materials and will be the only recording of Panel meetings allowed.
• Conflict of Interest (COI)• You are here because of your interest and/or experience with the AMA Guides®, but your affiliations
could pose a potential conflict of interest. Please mention all of your disclosures if they are relevant to the topic being discussed or the opinions you hold and express.
• While you were nominated by a society, remember that your Editorial Panel duty is to the AMA Guides®. You are not here to represent the interests of any society, profession, or employer.

© 2020 American Medical Association. All rights reserved.
The AMA GME Competency Education Program
5
• Updated policy in early 2019.
• This is what we expect of our members and guests at AMA-sponsored events.
• We take harassment and conflicts of interest seriously. Read our policy or file a claim at ama-assn.org/codeofconductor call (800) 398-1496.

© 2021 American Medical Association. All rights reserved.
Meeting Mechanics
• Webcams are optional but may be used if Panel Members and Advisors wish to do so
• Panel members and advisors are open-line participants and may speak at any time throughout the duration of the event.
• Please consider muting your phone to prevent background noise and raising your hand to pose a question or comment.
• All other attendees are open line participants but have been auto-muted to prevent background noise.
• Hand raise or chat feature encouraged to indicate desire to speak. Please unmute yourself prior to speaking.

© 2021 American Medical Association. All rights reserved.7
Meeting Mechanics (con’t)
• Co-chairs will introduce proposals and presenters.• Presenters will provide an overview of the proposal. • Primary and secondary reviewers will be called upon first to lead
discussion and recommend action. • Editorial panel members and advisors are encouraged to contribute to
discussion. • Oral disclosures are not required of panel members and advisors during the
meeting but might be helpful when expressing a strong opinion.• Public participants are invited to participate towards the end of discussion
and are asked to disclose any conflicts of interest when introducing themselves.

© 2021 American Medical Association. All rights reserved.8
October 14 Meeting Highlights
• Three Newsletter articles were approved by the Panel as authoritative. Authoritative articles reflect an official AMA interpretation, application or clarification. Revisions to the AMA Guides are not made via the Newsletter. These designated articles are in the process of being earmarked AMA Guides Digital.
• Grade Modifiers: Discussions of the Spine 3-Grade modifier system is based on current best science and will move the 3-Grade to the other musculoskeletal chapter when appropriate. Further discussion on this topic within the spine proposal is anticipated at the upcoming December 16th meeting.
• Discussion on Editorial Priorities to determine new topics to prioritize for advancement. Topics under consideration include telemedicine, long-haul COVID, pain and more. Further discussion and finalization of new topics to occur at the upcoming December 16th meeting.
• AMA Guides Sixth 2022 is now available on AMA Guides Digital! Education Module will be available on December 9th on the AMA Ed Hub™.

© 2021 American Medical Association. All rights reserved.
Lase Ajayi, MDMember since 2013
9
ENT ProposalDr. Robert Sataloff, MD, DMA, FACSAmerican Academy of Otolaryngology - Head and Neck Surgery

© 2021 American Medical Association. All rights reserved.10
ENT Proposal - Summary
• Rotary Chair Testing (slide 11) • Dysphagia
• New Example (slide 12)• Proposed additional Added to condition description: Dysphagia may be
caused by structural, neuromuscular, neoplastic and other maladies. Oropharyngeal tumors must be ruled out and may occur even in young people, especially in association with human papilloma virus (HPV) infection.
• Addition of videonystagmography (VNG) to subtitle and to accompany electronystagmography (ENG)

© 2021 American Medical Association. All rights reserved.11
Proposed Lanugage: Rotary Chair Testing Rotary chair testing helps identify whether dizziness is due to dysfunction in the inner ear or brain. Caloric testing (ENG/VNG) generally is considered the gold standard for identifying unilateral vestibular dysfunction. Rotary chair testing is the gold standard for detection of bilateral vestibular dysfunction. ENG/VNG is performed to evaluate most people with suspected labyrinthine dysfunction. Rotary chair testing is obtained when bilateral disease is suspected, or when more sophisticated information is required. Rotational chair testing has no contraindications such as neck trauma, which is not the case with ENG/VNG. In rotary chair testing, rotation is computer controlled and extremely accurate. It is well-tolerated and even can be performed in children. Rotary chair testing has been used for decades, and there is extensive literature on the technique. In addition to bilateral semicircular canal paresis, common indications include equivocal or inconclusive ENG/VNG results, evaluation of vestibular compensation, ototoxicity management, and testing of special populations includes children and handicapped individuals. Rotary chair testing assesses the integrity of vestibuloocular reflex (VOR), and suppression of that reflex. The tests are complementary. Unlike caloric testing, rotary chair testing stimulates both ears simultaneously. Caloric testing assesses the vestibular system at a frequency of only 0.03 Hz; but rotary chair testing assesses from 0.01 Hz through 0.64 Hz. Common rotary chair tests include sinusoidal harmonic acceleration (SHA), VOR suppression, and the velocity step test. Other subtests may include slow harmonic (sinusoidal) testing in darkness, high-velocity or high-frequency sinusoidal rotation, rotation with fixation on head-fixed targets to evaluate suppression, optokinetic after-nystagmus, tilted-axis rotation (OVAR), rotation with fixation on earth-fixed targets, optokinetic testing, and others. Rotary chair testing allows monitoring of the VOR over time, which is important because the phase abnormality and symmetry in VOR recover in some patients following vestibular injury.

© 2021 American Medical Association. All rights reserved.12
Proposed Example: 15% WPI; Subject 70-year-old man
• History: This 70-year-old male worked for approximately four decades in an industry in which he was exposed to carcinogens. He had no history of smoking cigarettes or consuming alcohol. At age 60, he was treated with surgery and radiation therapy for squamous cell carcinoma of the right side of the tongue and floor of mouth. Since that time, he had had dysphagia. He had to eatslowly, was unable to swallow food of some textures; and sometimes he coughed after drinking liquids, although he did not sense aspiration. He also had difficulty maintaining his body weight.
• Current symptoms: Dysphagia as described above.• Physical examination: Partial restriction of tongue motion on the right. Dry, mildly erythematous mucosa of the oral cavity, pharynx
and larynx consistent with radiation change. On strobovideolaryngoscopy, he had diffuse laryngeal edema and severe right vocal fold paresis.
• Clinical studies: Barium swallow showed silent aspiration. Modified barium swallow with a speech-language pathologist present revealed the following abnormalities:
• Oral stage: Mastication was effective. Lingual transfers were segmented. There was posterior bolus leakage prior to the initial swallow to the distal pharynx with thin liquids and to the proximal pharynx with all other textures.
• Pharyngal stage: Delay of swallow initiation. Sluggish epiglottic displacement. Pharyngeal dysmotility with resultant bolus hold up in valleculae in pyriform sinuses. The residuals increased with thicker textures. Spontaneous second swallow cleared residuals only partially. A cued liquid chaser cleared most of the remaining residuals from the valleculae, but pyriform sinus residuals increased with thin liquid trials. Osteophytic spurs at C5-6 and C6-7 may have contributed to pyriform sinus residuals. There was transient laryngeal penetration of thin liquids to the level of the vocal folds. Sensation of the penetration was inconsistent. No aspiration was seen during the study, but the patient was felt to be at high risk for intermittent aspiration as had been identified on the previous barium swallow.

© 2021 American Medical Association. All rights reserved.
Kyle Edmonds, MDMember since 2005
13
1. Primary / Secondary Reviewers2. Panel Members3. Public Participants

Update on fPROM* Review for Guides 6th Edition
*Patient-reported outcome measures of function
Stephen Gillaspy, PhDKathryn Mueller, MD, MPH, FACOEMRobert Glueckauf, PhDDaniel Bruns, PsyD, FAPA

Kathryn L Mueller, MD, MPH, FACOEM
• Professor, University of Colorado, School of Public Health and School of Medicine – Department of Physical Medicine and Rehabilitation
• Prior Medical Director, Colorado Division of Workers Compensation –Currently a consultant
• Past President American College of Occupational Medicine
• Serves on Academic and International Advisory Boards for MedRisk and Workers Compensation Research Institute
• No relevant disclosures

Stephen R. Gillaspy, PhD- Senior Director, Health Care Financing and the
Center for Psychology & Health, American Psychological Association
- Licensed clinical psychologist, clinical scientist and senior administrator with extensive experience integrating psychological services into larger healthcare systems.
- Serves as the APA advisor to the American Medical Association's Relative Value Update Committee (RUC).
- Former professor and director of pediatric psychology in the department of pediatrics at the University of Oklahoma, College of Medicine
- Former President of the Oklahoma Psychological Association (OPA) in 2013 and chaired OPA’s Division for Research, Academics, and Training from 2009 to 2011.
- No relevant disclosure
16

IHCInterdivisional Healthcare Committee
An APA Affiliated Think Tank
■ APA Division 17 – Society of Counseling Psychology■ APA Division 22 – Rehabilitation Psychology■ APA Division 31 – State, Provincial and Territorial Affairs■ APA Division 38 – Society for Health Psychology■ APA Division 40 – Society for Clinical Neuropsychology■ APA Division 42 – Psychologists in Independent Practice■ APA Division 43 – Society for Couple & Family Psychology■ APA Division 54 – Society of Pediatric Psychology■ Also attended by APA leadership and ACOEM
Rob Glueckauf, PhDFlorida State University
IHC Chair

Toni Vincent, MPH, PMP-Director of Operations, Office of Health and Health Care Financing, American Psychological Association -Master of Public Health, George Washington University -Certified Project Management Professional (PMP) ® -Member American Public Health Association, Project Management Institute
18

• American Psychological Association
• Member of Interdivisional Healthcare Committee (IHC)
• American College of Occupational and Environmental Medicine
• Current chair of mental health treatment guidelines
• State of Colorado
• Past chair of chronic pain treatment guidelines
• Senior clinical instructor at University of Colorado Medical School
• Principle investigator in 15-year longitudinal study of 29 million patients assessing the impact of biopsychosocial treatment guidelines
• Served as CMS Technical Expert for Medical Incentive Payment System
• 2011 National Cancer Institute / Society for Behavioral Medicine Award: Data Harmonizing Pioneer
• Independent Pain Psychology Group Practice
• Disclosure
• Co-author of two standardized psychological tests designed for the assessment of patient risk for poor response to medical treatment
Daniel Bruns, PsyD FAPAChair: Functional Outcome Assessment Task Force

fPROM Project Organization
ACOEM APA
Interdivisional Healthcare Committee
Review By Functional Assessment Task
Force
Stephen Gillaspy, PhDAPA Senior Director
Kathryn Mueller, MDPast ACOEM President
Robert Glueckauf, PhDIHC Chair
Daniel Bruns, PsyDTask Force Chair
University of Colorado Medical Research
Librarians
18 Task Force-Appointed Reviewers


Criteria Considered in fPROM Review• Standardization
• Validity (content and construct)• Reliability (internal and stability over time)• Norms (community and patient)• Fairness (no gender, race, ethnicity bias)• Harmonization (measures useful across groups
and diagnoses)
General psychometric
standards
• Consistent with ICF• Forensic defensibility
• Rules of evidence (Frye, Daubert)• Regional regulations
• Practicality• Guides internal consistency
AMA Guides standards

Measures Should Be Consistent With the ICFand the Biopsychosocial Model
BiologicalThe Guides' impairment evaluation focuses
primarily on the effects of disorders or disease on bodily functions and structures
Psychosocial/Behavioral
Activities play a central role in the ICF.We found that most fPROMs
use ADL-type items to assess function

Dx Specific MeasuresFocus: Symptoms or Effect
of the Condition
e.g. Lower Limb QuestionnaireRoland-Morris Low Back Pain and Disability
Questionnaire
Used only for a specific diagnosis. Use of these would create gaps in the Guides:
Diagnoses with no recommended measure
Global/General Measures Focus: Activities
of the Patient
Rand MOS, SF-36 & PROMIS-29 MeasuresICF also focuses on patient activity
Applicable to any medical Dx or to a healthy individual
fPROMs and the “Swiss Cheese” Problem
Reviews of literature have not shown that specific measures are superior to general measures for outcome assessment (Chiarotto, 2018)

One-Dimensional Measures
Physical FunctioningPROMIS 10 Physical Functioning
Mental FunctioningBeck Depression Inventory
Social FunctioningPROMIS 8 Social Ability
Pain InterferencePDQ, Oswestry
Multidimensional Measures
Rand/SF 36(8 Scales and Measures)
PROMIS-29(10 Scales and Measures)
Evaluating Different Types of fPROMs
Too Specific: One-dimensional measures assess only one aspect of functioning
Too Complex: Measures with 8-10 Scales are too complicated to interpret. [Use composite scores to simplify]

• PROMIS Function on ambulating– Are you able to go for a walk for at least 15 minutes ?
• Oswestry uses 4.8 times more words to ask the same question– Pain does not prevent me from walking any distance – Pain prevents me from walking more than one mile– Pain prevents me from walking more than a quarter of a mile– Pain prevents me from walking more than 100 yards– I can only walk using a cane or crutches – I'm in bed most of the time and have to crawl to the toilet
Measure Efficiency and Patient Burden
Some measures are much more efficient at gathering information.We felt this was an advantage

What constitutes unusually high [or low] levels of functional impairment?
• We found that most medical outcome measures are unable to make this determination– They were developed for pre-post assessment – “Ipsative” measures
• Standardized measures compare one score to a norm group– Establishing what is high requires that the test be extensively studied with
healthy persons in the community– “Normative” measures
We concluded that norm-based measures were superior for identifying high and low scores

Norm-Based T Score Output from PROMIS Physical Function Scale Offers More Information
Your T-score on the physical function measure is 37. The average T-score is 50.
Your score indicates that your level of physical function is higher (better) than:
– 14% of people in the general population– 10% of people age 35 to 45– 11% of males
All PROMIS T-Scores of 50 = that of average community memberAll PROMIS scales have a standard deviation of 10
Pre-post type measures do not provide this kind of information


NIH Patient Reported Outcome Measure System (PROMIS) Was Designed to Promote Data Harmonization
• There are a “cacophony” of fPROMs of varying quality, complexity, and response burden– The goal was a system that could allow comparisons across studies or
across conditions using a single metric – Cella, 2010
• Data harmonization: The process of combining data from different sources to assemble a larger picture– PROMIS measures were designed to be used with individuals with any
diagnosis, or no diagnosis

AMA Guides and Data Harmonization Current Guides fPROMs Preclude Comparisons Across Chapters
Measure
Percent of items on measure referring to:
Example items from these measuresillustrate their nonequivalencePain Basic
ADLs
Instru-mental ADLs
Advanced ADLs
Lower Limb Questionnaire 43% 71% 0% 0% How difficult is it for you to put on or take off socks?
QuickDASH 18% 27% 27% 27% Has your arm, shoulder or hand problem interfered with your normal social activities with family, friends, neighbors…
PDQ 100% 33% 7% 40% Has your income declined since since your pain began?[Note: No impairments are rated unless due to pain]
Basic ADL: Ability to feed self, wash & dress self, walk, bowel and bladder controlInstrumental ADLs: Ability to use phone, travel to store, shop, use money, prepare food, clean upAdvanced ADLs: Ability to be productive at home or work, engage in recreation, and family/community activities(Dinken, 1951; Katz 1983; Reuban, 1989)


• The PROMIS 29 measure generates:• 7 scales• 2 summary scores
• Physical Health• Mental Health
• We concluded that the P29 Physical Health Summary Score is:
– Supported by the strongest science
– Offers the best answer to the AMA Guides questions
– Would allow for data harmonization across chapters
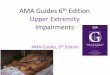
PROMIS 29’s Physical Health Summary Score

PROMIS 29’s “Physical Health Summary Score”
Physical Functioning
FatigueAbility to Perform
Social Roles
Physical Health Summary Scores
Pain Intensity &
Interference
Pain Interference
0-10 Pain Intensity
Each of these is a standardized 4 item-long scale, plus the
0-10 pain rating
P29’s Interpretation is Simplified by Using a “Global” Type “Summary Score.”
It is Calculated by an Equation That Uses Four PROMIS 29 Scale Scores
(17 Items)
17 items, but 65% fewer words than the Oswestry.
More info, less burden.

Physical Functioning Is One of Four Components Of The PROMIS Physical Health Summary Score
• Development of Physical Functioning Scale• Literature review identified 1728 items from 165 measures of physical functioning • Expert review categorized and edited items • Patient focus groups
– What outcomes do patients value?– Sought patient feedback on item clarity
and relevance
• (Rose, 2014; Dewalt 2007; Reeve, 2007)

• Data: 149 remaining items administered to 21,133 subjects– Both patients and community members
• Analysis: Extensive analysis of items– Biased items were eliminated
• Results: A four-item measure of Physical Functioning was developed and is used in the PROMIS 29
• To avoid bias, this scale was normed on a sample of community members matched to US census data
• (Rose, 2014; Dewalt 2007; Reeve, 2007)
• Each scale on PROMIS 29 went through a similar process
Development of Physical Functioning Scale

PROMIS 29 Physical Function: Items and Conversion Table
T-scores Based on Community Norms
T50 = Average in communityStandard Deviation = 10

• PROMIS 29 was tested on a diverse patient population– Patient diagnoses included
• Migraine, cancer, cardiac, pulmonary, neurological, injury, depression, drug abuse, etc.
– Development research subjects in this phase n=5000• 51% female, • 60% non-Hispanic White, • 17% Hispanic, • 14% non-Hispanic Black, • 9% Asian • Hays, 2018
• P29 interpretation was simplified by developing two summary scores– Physical Health Summary Score (recommended score)– Mental Health Summary Score
Following development of the 7 PROMIS 29 scales:

• PHSS is a “global” measure that summarizes multiple aspects
of physical health
– This score can be accepted as a “black box” for determining the
patient reported level of function
– For additional information, you can “unpack the box” and look at the
scores of the four component scales, the way you might look at the
item responses on a scale
PROMIS 29’s “Physical Health Summary Score”

• The Physical Health Summary Score
– Is calculated by an equation using the component scales• PHSS=[(Physical Health * 0.872) + (Pain * -0.094) + (Social * 0.113) + (Fatigue* -0.009)] *10 + 50
• PROMIS measures are increasingly available in EHR
• AMA Spreadsheet or App?
• Other societies have already created web scoring for other
PROMIS tests. See: https://orthotoolkit.com/promis-10/
Scoring the Physical Health Summary Score

• If the rater does not have access to this software, physical
and social scales account for majority of variance
– Physical Function scale assesses basic level of function
– Social Function scale assesses more complex levels of function
• These are the two biggest contributors to Physical Health
Summary Score, and could be used as a substitute
There Is Also a Hand scoring Workaround


• Univ Colorado Med School research librarians assisted lit review
– Identified both well-known & unfamiliar tests as candidates for review
• There are easily over 1000 fPROM outcome measures
• 38K studies on these measures:
– Rand/SF-36, PROMIS, Oswestry, Roland Morris
• Developed a review system to rate measures for Guides
– 18 reviewers trained in the system were provided with articles and support line
• Inter-rater reliability (agreement%) was calculated
– Final overall inter-rater reliability was 82%
Methods of Literature Review

• Developed a review system to rate measures for Guides– The Guides has unique needs – both clinical and forensic– A system tailored to the needs of the Guides was developed to rate measures– APA created a web-based system for gathering data from raters
• Reviewers Were Recruited by IHC– 18 reviewers (9 senior, 9 early career/fellowship training)– Reviewers trained in the system were provided with articles and support line
• Inter-rater reliability (agreement%) was calculated– Reliabilities calculated for each fPROM and for each item in the rating– Final overall inter-rater reliability was 82%
• Rater reliability across measures: Std Dev = 10.15; Std Error = 3.4
• These psychometric findings provided the empirical justification for further analyses
Rating Process For Candidate fPROMs


ACME Strength Test v6How much weight can you lift from floor to waist?
– 1 pound
– 2 pounds
– 3 pounds
– 4 pounds
– 5 pounds
– 6 pounds
– 7 pounds
– 8 pounds
… 200 pounds
Hypothetical Test of Strength: Precision vs Length
This test is precise but very long!
How can you have a test that is short
and precise?

IRT: Computerized Adaptive Testing
Can you lift 50 pounds?
100?
150?200?
250?175?
125?135?110?
75?85?
90?80?
65?70?60?
25?
35?40?
45?35?
30?32?28?
12?20?
25?15?
6?9?3?
NoNoYes Yes
CAT tests can be short and precise


PROMIS 29 Overview
Physical Functioning
FatigueAbility to Perform
Social Roles
Physical Health Summary Scores
Pain Intensity &
Interference
Pain Interference
Pain Intensity
PROMIS 29 is like a “Russian Doll” system of tests where a “summary score” is calculated
from several component scales. All component scales are independently valid
and reliable, and are mathematically combined to create the overall score.

PROMIS 29 Overview
Physical Functioning
FatigueSocial Roles & Activities
Emotional Distress
Sleep Disturbance
Global Physical Health
Pain Intensity &
Interference
Global Mental Health
AnxietyDepressionPain
InterferencePain
Intensity
FCE
PDQ PHQ9 GAD7PDQ
Sleep Study

You can treat the Physical Summary Score as a
closed box without consideration for its inner workings
Both PROMIS 29 and SF 36 Use Summary Scores
Alternately, you can unpack the box and find more
information inside

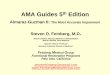
PROMIS 29 Groups Functioning Into Two Broad Factors Based On Their Mathematical Relationships
Method: Confirmatory Factor Analysis
Scales previously developed using IRT
Principle components analysis of scales
Two factors extracted
Promax oblique rotation
Variance explained: Not reported
Correlation of physical and mental factors: 0.69

PROMIS Uses Standardized T-Scores Based on Community Norms A High Score = A high Level of what the scale measures
Mean = 50; Std Dev = 10
From HealthMeasures.net

PHSS=(Physical Health * 0.872) + (Pain * -0.094) + (Social * 0.113) + (Fatigue* -0.009) + (Sleep * 0.002) + (Emotion* 0.003)
PHSS

© 2020 American Medical Association. All rights reserved.
Theresa Phan, MDMember since 2013
55
1. Primary / Secondary Reviewers2. Panel Members3. Public Participants

© 2021 American Medical Association. All rights reserved.56
Closing
• Thank you to today’s presenters. This now concludes the public meeting.• Summary of Panel Actions will be posted on the AMA Guides website. • The next public Editorial Panel Meeting will be held virtually on December
16th at 6:00 pm CT. • Panel members and advisors will convene in Executive Session
momentarily. Panel members please standby.

© 2021 American Medical Association. All rights reserved.
Siobhan Wescott, MDMember since 2013
57
Executive Session

© 2021 American Medical Association. All rights reserved.
Quorum
• Attendance will be taken.Panel Members
Panel Advisors
Helene Fearon, PTSteven Feinberg, MDDavid Gloss, MDRobert Goldberg, DORita Livingston, MD, MPH
Doug Martin, MDKano Mayer, MDMark Melhorn, MDLylas Mogk, MDMarilyn Price, MD
Noah Raizman, MDMichael Saffir, MDJan Towers, PhD
Chris Brigham, MDHon. Shannon Bruno Bishop, JDBarry Gelinas, MD, DC
Abbie Hudgens, MPAHon. David Langham, JD

© 2021 American Medical Association. All rights reserved.59
Meeting Mechanics: Executive Session
• Executive Session will resume for discussion and vote on the Editorial Change Proposal
• Staff sent voting instructions via email.• Co-chairs may call for a vote or panel members may motion to
Approve, Reject, Revise or Table an Editorial Change Proposal.• Qualtrics will be used to collect votes. • Voting results shared in aggregate to inform the panel if the motion
has passed. Only AMA staff will have a record of how each panel member voted.
• Disclose conflicts of interest as appropriate and maintain confidentiality

© 2021 American Medical Association. All rights reserved.60
Potential MotionsAction Description Outcome
Approve
Proposed change is approved; Panel recommends AMA action to implement ECP.
Applicant(s) notified of Panel’s decision, after AMA staff has determined early next steps toward deployment or implementation.
Reject
Proposed change is rejected; ECP might be out of scope, lacking evidence, premature, or not suitable for AMA Guides.
Applicant(s) notified and provided rationale for the decision (i.e., application criteria not met).
Revise
Revisions are requested in effort to make ECP more acceptable; application will be reconsidered at later Panel meeting following revisions.
Applicant(s) notified regarding decision, summary of suggested revisions, and provided rationale for the decision.
Table
Decision is postponed or suspended until further notice.
Applicant(s) notified and provided rationale for the decision.

© 2021 American Medical Association. All rights reserved.
ENT Proposal – Is there a Motion?
Motion to Accept (Seconded) – Approved.
Directive: Information on example to be embedded into the text of the Guides. (for review in December to approve)

© 2021 American Medical Association. All rights reserved.
fPROMs PROMIS 29 – Is there a motion?
Motion- Request applicants provide copies of the PROMIS 29 questions for review, andprovide the crosswalk between the computer and paper scoring prior to making a decisionon moving forward to incorporate the fPROM in the Guides. Acknowledge the effort of the proposing group. Express support for the PROMIS-29 as the best available, evidence-based science. – Approved.
Discussion:Concerns w/ implementation and using a website PROMIS-29 is open source; will look into licensingComputer vs. Paper (paper application could lead to consistency issues); look at disclaimers as to why we are recommended PROMIS and rationale. Suggested method; but can use another to get functional historyMore defensible than other tools; look at our future outlook in terms of digital access. How to apply the tool to each chapter and when; discuss implementation later. Move towards incorporating PROMIS-29 into the Guides

© 2021 American Medical Association. All rights reserved.PM -6
Next Steps
• AMA staff will recap the Executive Session decisions and rationale and share a summary with the Panel.
• AMA Guides leadership will inform Applicants of the Panel’s decision in writing.
• Notice of the Panel’s decision on the applications will be posted on the AMA Guides website.

© 2021 American Medical Association. All rights reserved.
Saby Karuppiah, MDMember since 2008
Executive Session Closing
64