Embed Size (px)
Citation preview
Alzheimer’s Disease and Alzheimer’s Disease and Related Dementia DisordersRelated Dementia Disorders
Brian R. Ott, MDBrian R. Ott, MD
Professor, Department of NeurologyProfessor, Department of Neurology
Brown UniversityBrown University
Director, Alzheimer’s Disease and Memory Disorders Center Director, Alzheimer’s Disease and Memory Disorders Center
Rhode Island Hospital Rhode Island Hospital
Mild Cognitive ImpairmentMild Cognitive Impairment
•• Mild cognitive impairment Mild cognitive impairment (usually affecting memory)(usually affecting memory)
•• Other cognitive abilities often intactOther cognitive abilities often intact
•• No functional disabilityNo functional disability
•• Represents a preRepresents a pre--AD transitional state for manyAD transitional state for many
•• Progression to AD occurs more frequently than in Progression to AD occurs more frequently than in normal elderly (~10normal elderly (~10--15% each year)15% each year)
»» Almkvist. Almkvist. J Neural Transm SupplJ Neural Transm Suppl. 1998;54:21. 1998;54:21--29. 29. »» Petersen. Petersen. Arch NeurolArch Neurol. 1999;56:303. 1999;56:303--308.308.

Mild Cognitive ImpairmentMild Cognitive Impairment
•• “Mild cognitive impairment“Mild cognitive impairmentss predict dementia in nonpredict dementia in non--demented elders”demented elders”
•• Memory loss alone rarely (6%) progresses to Memory loss alone rarely (6%) progresses to dementia over two years.dementia over two years.
•• Memory loss Memory loss plusplus other cognitive impairments does other cognitive impairments does predict conversion to ADpredict conversion to AD
–– 48% at two years48% at two years–– 77% at four years vs 24% of memory only pts.77% at four years vs 24% of memory only pts.
»» Bozoki. Bozoki. Arch NeurolArch Neurol 2001;58:4112001;58:411--416416
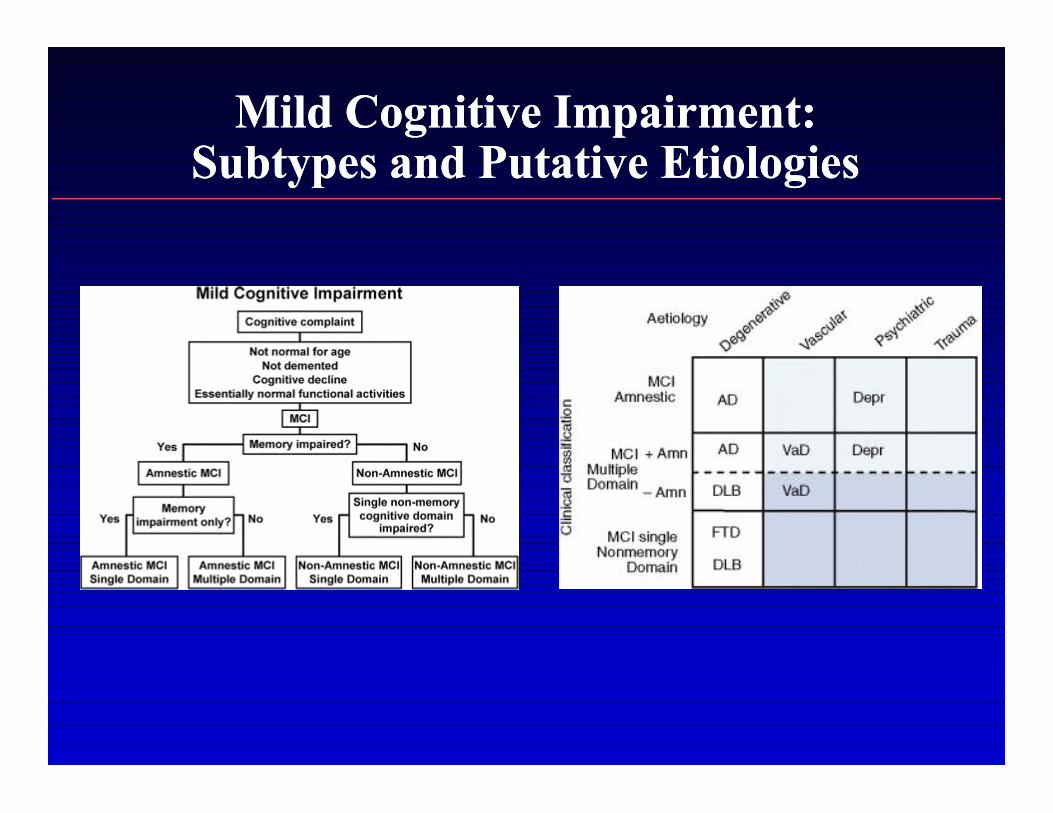
Mild Cognitive Impairment: Mild Cognitive Impairment: Subtypes and Putative EtiologiesSubtypes and Putative Etiologies

Mild Cognitive ImpairmentMild Cognitive Impairment
•• “Mild cognitive impairment represents early“Mild cognitive impairment represents early--stage stage Alzheimer’s disease”Alzheimer’s disease”
•• Prospective clinical and psychometric study of 177 Prospective clinical and psychometric study of 177 normal elders and 277 MCI followed normal elders and 277 MCI followed >> 9.5 years9.5 years
–– 100% of CDR 0.5 progressed to dementia100% of CDR 0.5 progressed to dementia–– 60% progressed to dementia by 5 years60% progressed to dementia by 5 years–– 24/25 patients with CDR 0.5 at post mortem had 24/25 patients with CDR 0.5 at post mortem had
dementia disorder dementia disorder •• 21 (84%) had AD21 (84%) had AD
»» Morris. Morris. Arch NeurolArch Neurol 2001;58:3972001;58:397
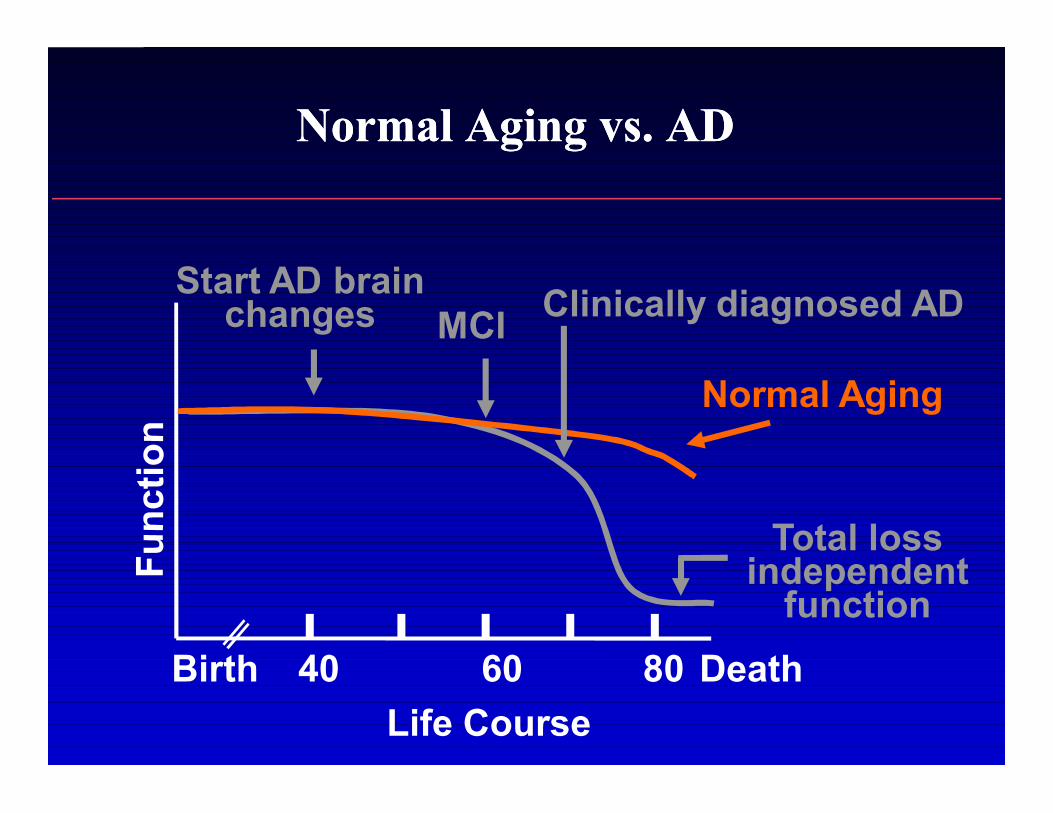
Normal Aging vs. ADNormal Aging vs. AD
Birth 60 DeathLife Course
Start AD brain changes MCI
40 80
Clinically diagnosed AD
Total loss independent
function
Normal Aging

Neuropathologic ChangesNeuropathologic ChangesCharacteristic of Alzheimer’s DiseaseCharacteristic of Alzheimer’s DiseaseNormal
AP = amyloid plaques.NFT = neurofibrillary tangles.Courtesy of Albert Enz, PhD, Novartis Pharmaceuticals Corporation.
AD
AP NFT

Pathology of ADPathology of AD
•• There are 3 consistent neuropathological There are 3 consistent neuropathological hallmarks:hallmarks:
–– AmyloidAmyloid--rich senile plaquesrich senile plaques–– Neurofibrillary tanglesNeurofibrillary tangles–– Neuronal degenerationNeuronal degeneration
•• These changes eventually lead to clinical These changes eventually lead to clinical symptoms, but they begin years before symptoms, but they begin years before the onset of symptomsthe onset of symptoms
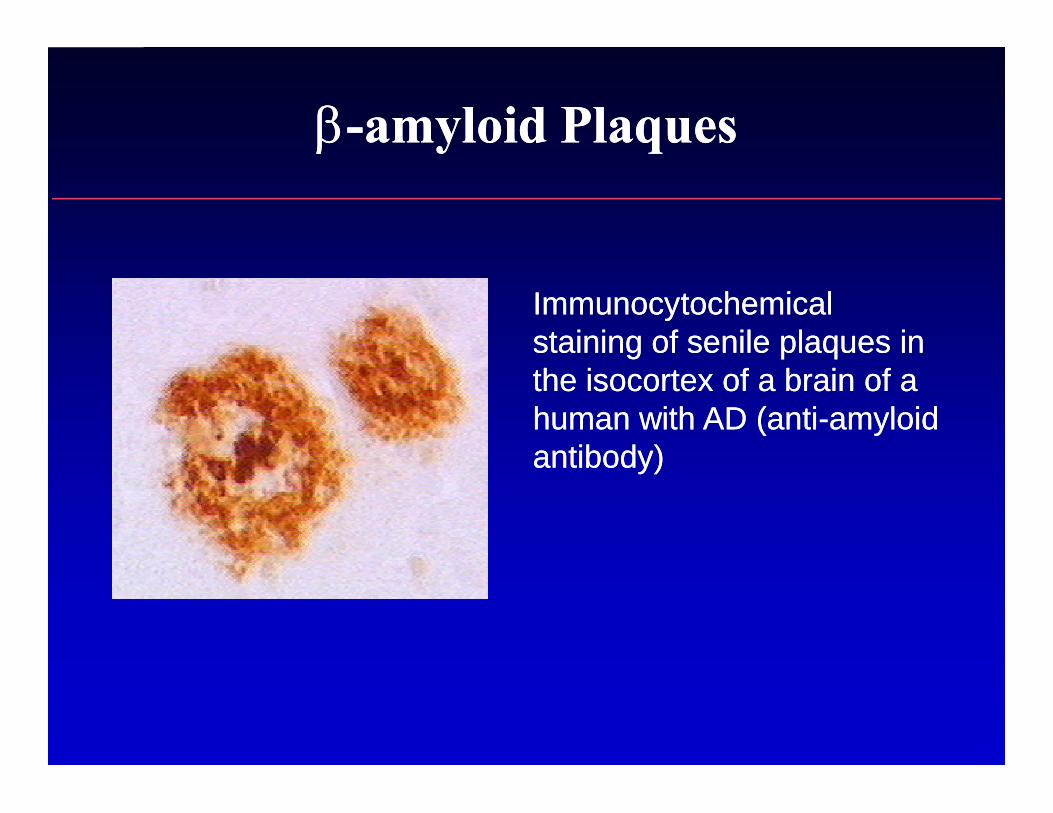
Immunocytochemical Immunocytochemical staining of senile plaques in staining of senile plaques in the isocortex of a brain of a the isocortex of a brain of a human with AD (antihuman with AD (anti--amyloid amyloid antibody)antibody)
ββ--amyloid Plaquesamyloid Plaques

Proteolytic Cleavages of Amyloid Proteolytic Cleavages of Amyloid Precursor Protein Produce APrecursor Protein Produce Aββ PeptidePeptide
β-amyloid precursor protein
β-secretase
Aβ peptide
γ-secretase
Extracellular space
TM Cytoplasm
COOHNH2
Selkoe DJ et al. JAMA. 2000;283:1615-1617.
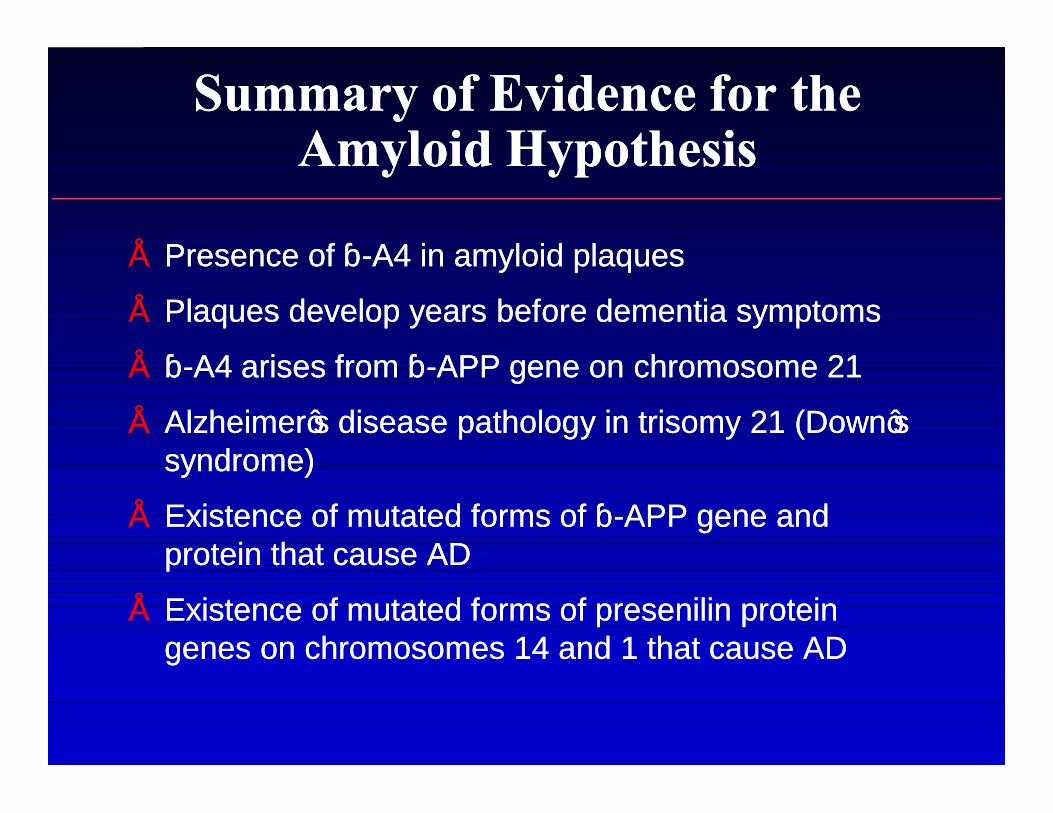
Summary of Evidence for the Summary of Evidence for the Amyloid HypothesisAmyloid Hypothesis
•• Presence of Presence of ββ--A4 in amyloid plaquesA4 in amyloid plaques
•• Plaques develop years before dementia symptomsPlaques develop years before dementia symptoms
•• ββ--A4A4 arises from βarises from β--APP gene on chromosome 21APP gene on chromosome 21
•• Alzheimer’s disease pathology in trisomy 21 (Down’s Alzheimer’s disease pathology in trisomy 21 (Down’s syndrome)syndrome)
•• Existence of mutated forms of Existence of mutated forms of ββ--APP gene and APP gene and protein that cause ADprotein that cause AD
•• Existence of mutated forms of presenilin protein Existence of mutated forms of presenilin protein genes on chromosomes 14 and 1 that cause ADgenes on chromosomes 14 and 1 that cause AD

Immunization with AImmunization with A$$ Reduces Reduces AA$$ Deposition Deposition in Hippocampus of in Hippocampus of AβAβ4242-- Injected MiceInjected Mice
Schenk et.al, Nature, 400:173-177, 1999
hippocampal Aβ deposition (a,b)
neuritic plaque formation (c,d)
cortical astrocytosis (e,f)
Immunized young mice
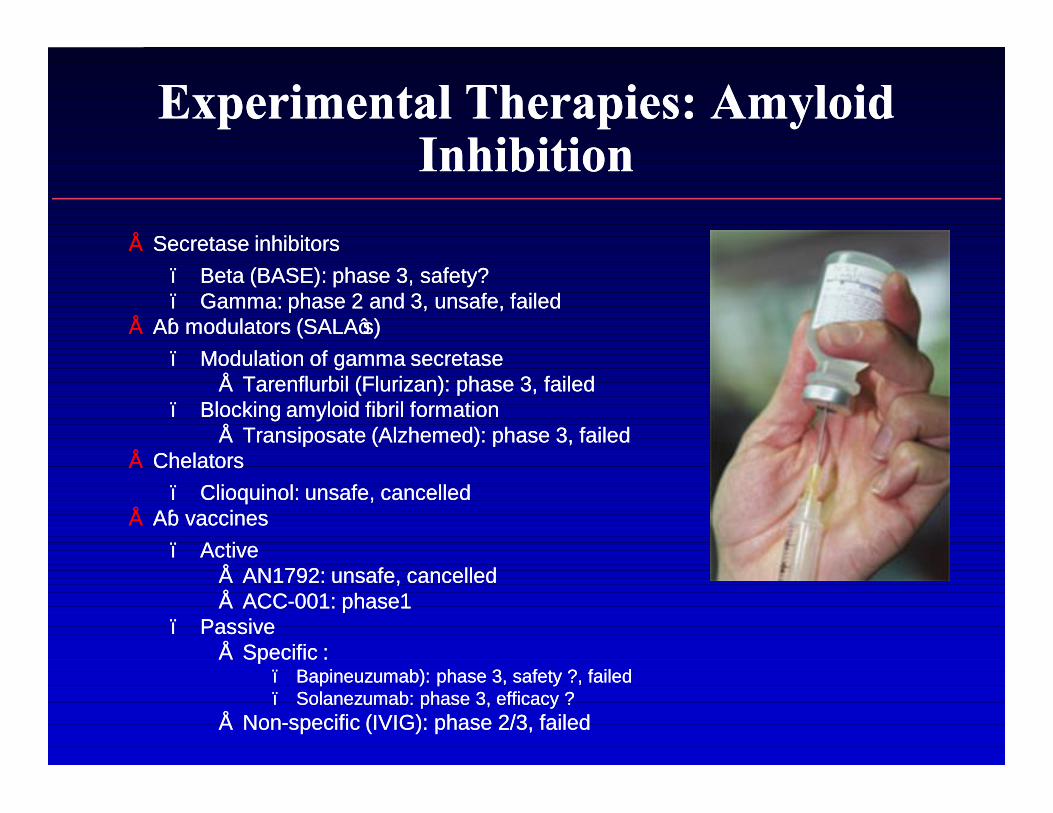
Experimental Therapies: Amyloid Experimental Therapies: Amyloid InhibitionInhibition
•• Secretase inhibitorsSecretase inhibitors–– Beta (BASE): phase 3, safety?Beta (BASE): phase 3, safety?–– Gamma: phase 2 and 3, unsafe, failedGamma: phase 2 and 3, unsafe, failed
•• AAβ modulators (SALA’s)β modulators (SALA’s)–– Modulation of gamma secretaseModulation of gamma secretase
•• Tarenflurbil (Flurizan): phase 3, failedTarenflurbil (Flurizan): phase 3, failed–– Blocking amyloid fibril formation Blocking amyloid fibril formation
•• Transiposate (Alzhemed): phase 3, failedTransiposate (Alzhemed): phase 3, failed•• ChelatorsChelators
–– Clioquinol: unsafe, cancelledClioquinol: unsafe, cancelled•• AAββ vaccinesvaccines
–– Active Active •• AN1792: unsafe, cancelledAN1792: unsafe, cancelled•• ACCACC--001: phase1001: phase1
–– PassivePassive•• Specific :Specific :
–– Bapineuzumab): phase 3, safety ?, failed Bapineuzumab): phase 3, safety ?, failed –– Solanezumab: phase 3, efficacy ?Solanezumab: phase 3, efficacy ?
•• NonNon--specific (IVIG): phase 2/3, failedspecific (IVIG): phase 2/3, failed
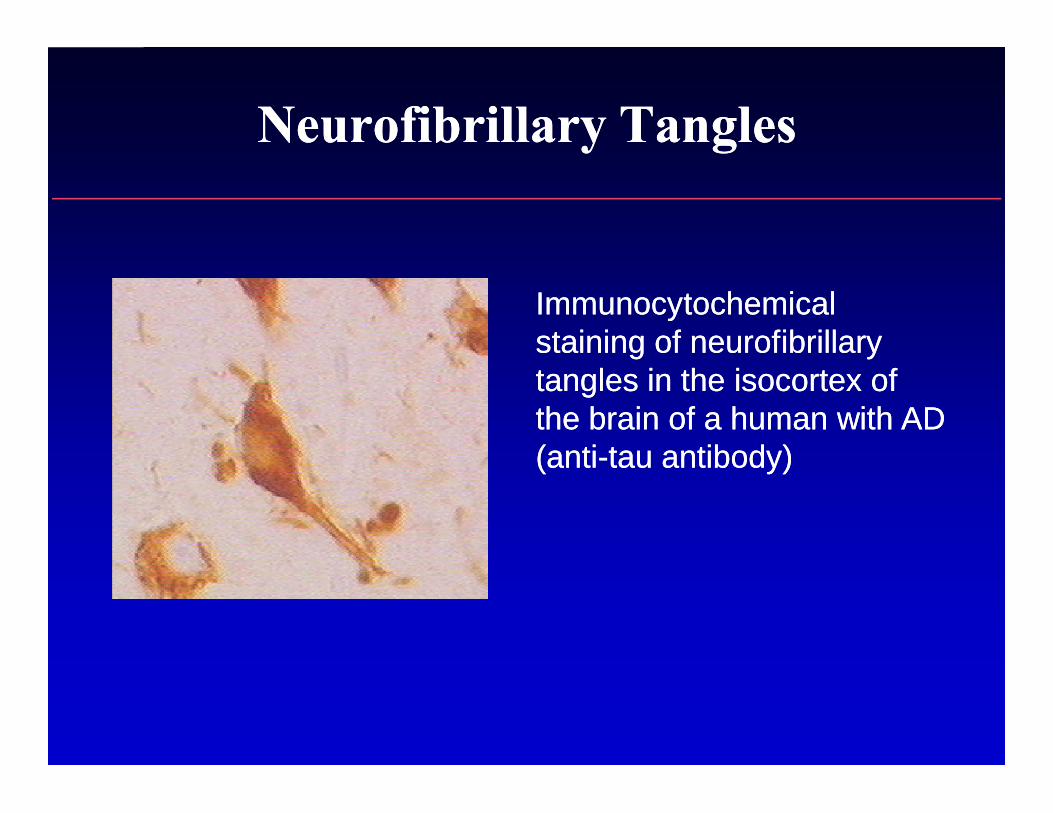
Neurofibrillary TanglesNeurofibrillary Tangles
Immunocytochemical Immunocytochemical staining of neurofibrillary staining of neurofibrillary tangles in the isocortex of tangles in the isocortex of the brain of a human with AD the brain of a human with AD (anti(anti--tau antibody) tau antibody)
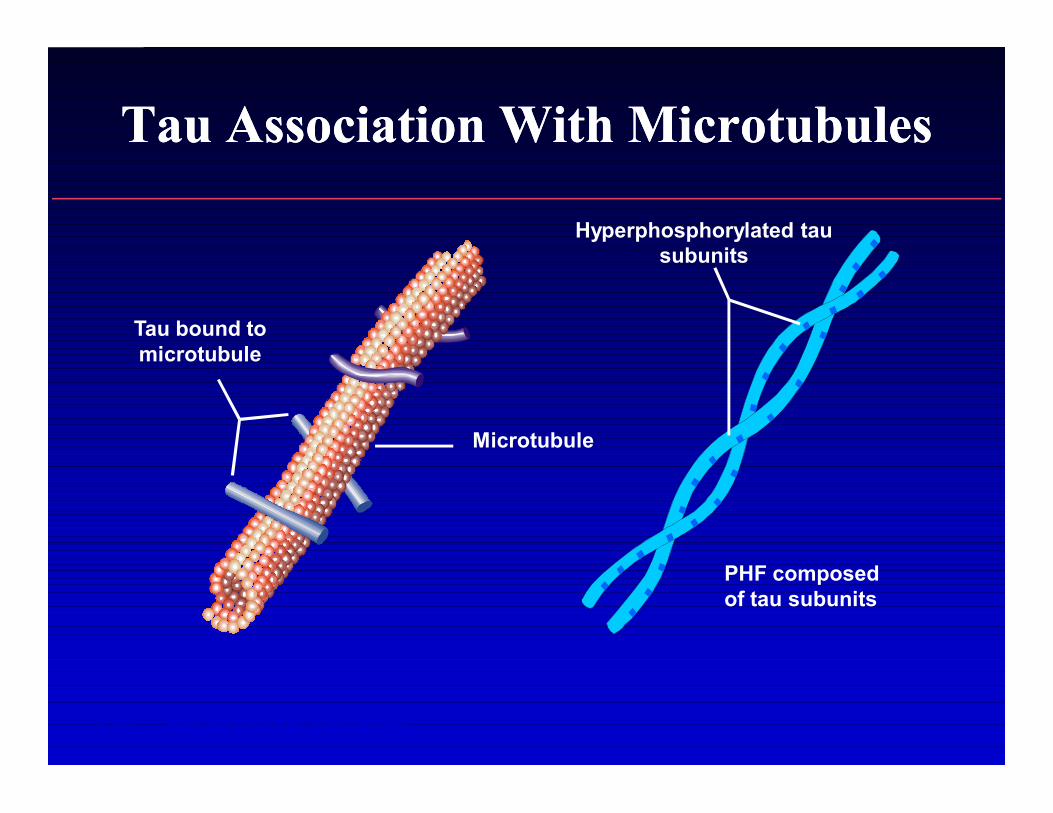
Tau Association With MicrotubulesTau Association With Microtubules
Tau bound to microtubule
Microtubule
Hyperphosphorylated tau subunits
PHF composed of tau subunits
PHF = paired helical filaments.
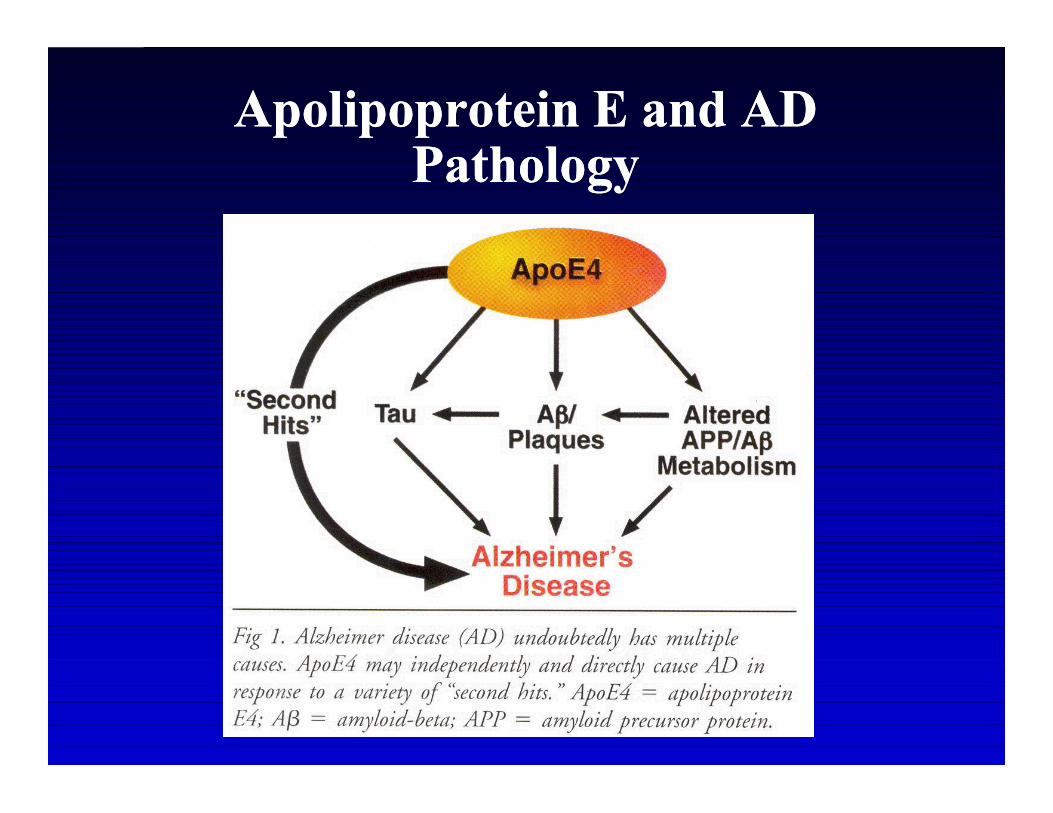
Apolipoprotein E and AD PathologyApolipoprotein E and AD Pathology
•• Apolipoprotein E (APOE) genotype is associated Apolipoprotein E (APOE) genotype is associated with AD risk with AD risk
•• APOEAPOE--epsilon2 may be protectiveepsilon2 may be protective——APOEAPOE--epsilon4 is associated with increased riskepsilon4 is associated with increased risk
•• The role of APOEThe role of APOE--epsilon2 and APOEepsilon2 and APOE--epsilon4 epsilon4 in pathogenesis is not knownin pathogenesis is not known
•• APOE is found in APOE is found in ββ--amyloid plaques and amyloid plaques and neurofibrillary tangles and may affect proteinneurofibrillary tangles and may affect protein––protein interactionsprotein interactions
Apolipoprotein E and AD Apolipoprotein E and AD PathologyPathology

FC = Frontal cortexPC = Parietal cortexOC = Occipital cortexH = HippocampusB = Nucleus basalisS = Medial septal nucleus
Adapted from Coyle JT, et al. Science. 1983;219:1184-1190.
Cholinergic System Innervates Cholinergic System Innervates Areas Associated With MemoryAreas Associated With Memory
FC
PC
B H
OCS
Cholinergic Changes in ADCholinergic Changes in AD
•• The most prominent neurotransmitter The most prominent neurotransmitter abnormalities are cholinergicabnormalities are cholinergic
–– Reduced activity of choline acetyltransferaseReduced activity of choline acetyltransferase(synthesis of acetylcholine)(synthesis of acetylcholine)11
•• Reduced number of cholinergic neurons in Reduced number of cholinergic neurons in late AD (particularly in basal forebrain)late AD (particularly in basal forebrain)22
1. Bartus RT et al. Science. 1982;217:408-414. 2. Whitehouse PJ et al. Science. 1982;215:1237-1239.
Cholinergic HypothesisCholinergic Hypothesis
•• Acetylcholine (ACh) is an important Acetylcholine (ACh) is an important neurotransmitter in areas of the brain neurotransmitter in areas of the brain involved in memory formationinvolved in memory formation
•• Loss of ACh activity correlates with the Loss of ACh activity correlates with the severity of AD severity of AD
Bartus RT et al. Science. 1982;217:408-414.
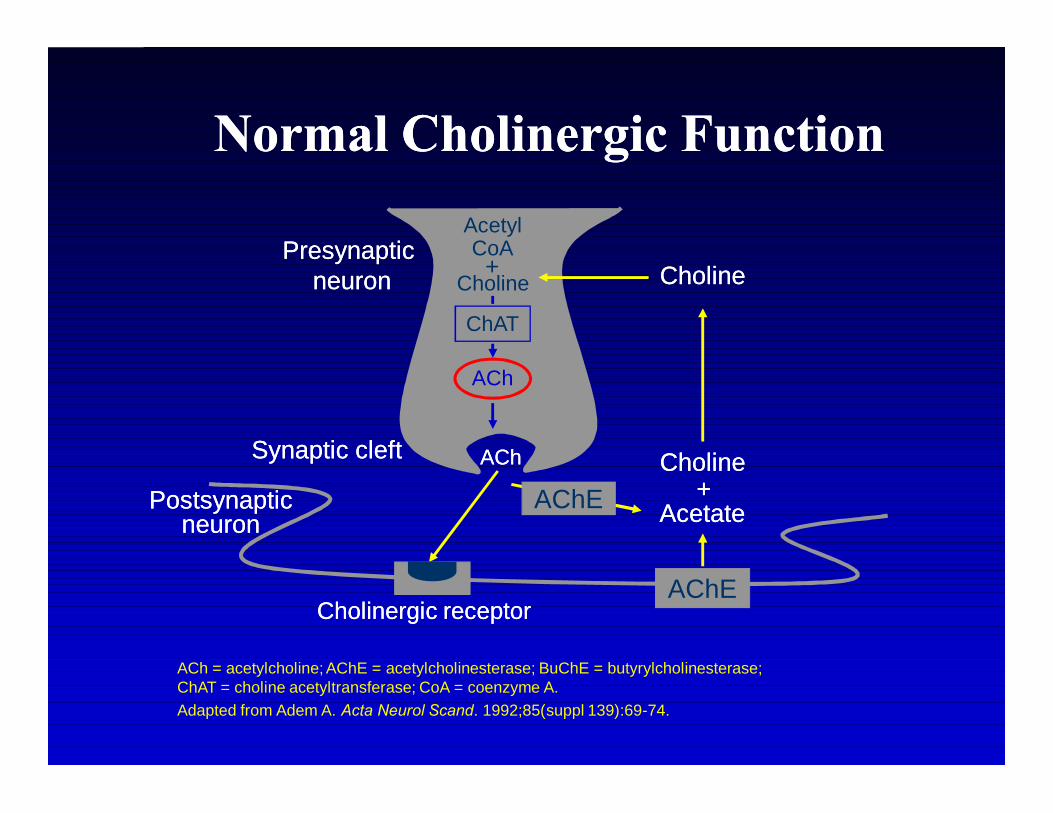
ACh = acetylcholine; AChE = acetylcholinesterase; BuChE = butyrylcholinesterase; ChAT = choline acetyltransferase; CoA = coenzyme A.Adapted from Adem A. Acta Neurol Scand. 1992;85(suppl 139):69-74.
AChE
AcetylCoA
CholineCholineAChACh
Presynaptic Presynaptic neuronneuron
Synaptic cleftSynaptic cleft
PostsynapticPostsynapticneuronneuron
Cholinergic receptorCholinergic receptor
AcetateAcetate
CholineCholineCholine+
++
ACh
AChE
ChAT
Normal Cholinergic FunctionNormal Cholinergic Function

Cholinesterase Inhibitors:Cholinesterase Inhibitors:General OverviewGeneral Overview
AChE = acetylcholinesterase; BuChE = butyrylcholinesterase.Physicians’ Desk Reference®. 2000; Nordberg A, Svensson AL. Drug Safety. 1998;19:465-480. Weinstock M. CNS Drugs. 1999;12:307-323; Enz A, et al. Prog Brain Res. 1993;98:431-438.
Tacrine Donepezil Rivastigmine GalantamineYear Available 1993 1996 2000 2001Brain No Yes Yes YesSelectivity (brain-region
selective)Reversibility Reversible Reversible Reversible ReversibleChemical Acridine Piperidine Carbamate PhenanthreneClass alkaloidEnzymesInhibited
AChE Yes Yes Yes YesBuChE Yes Negligible Yes Negligible
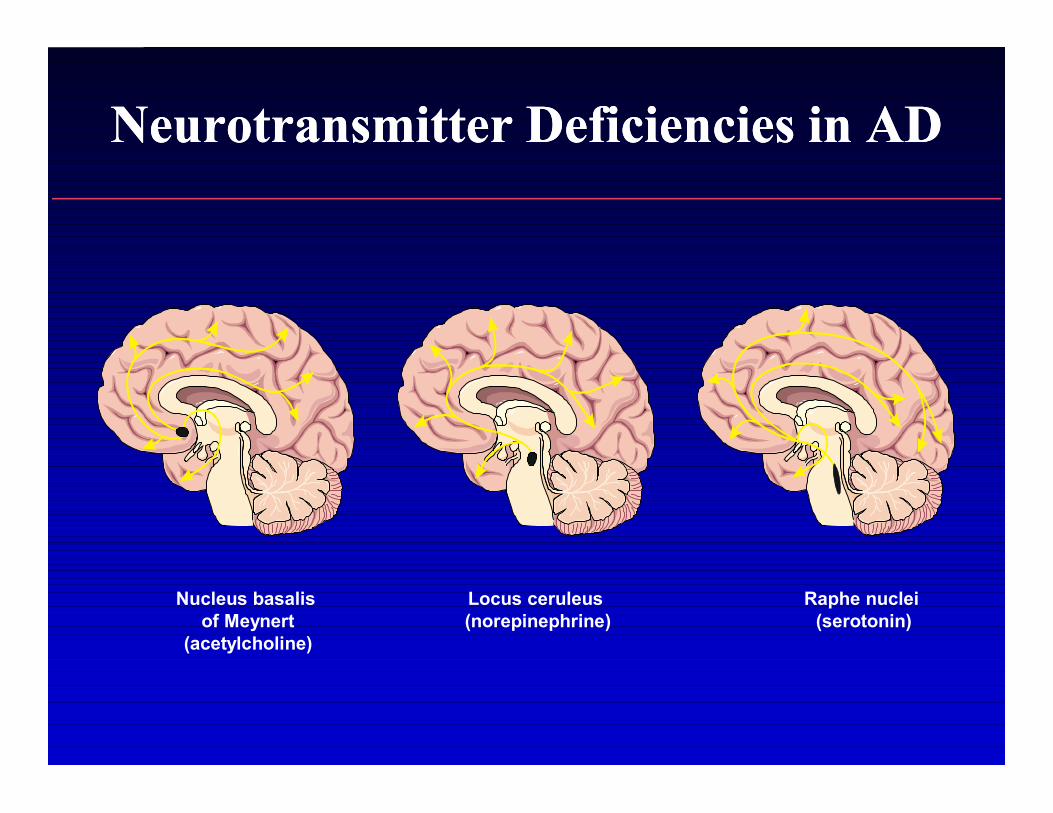
Neurotransmitter Deficiencies in ADNeurotransmitter Deficiencies in AD
Nucleus basalisof Meynert
(acetylcholine)
Raphe nuclei(serotonin)
Locus ceruleus(norepinephrine)
Mild Cognitive ImpairmentMild Cognitive Impairment
•• Upregulation of ChAT activity could be important factor Upregulation of ChAT activity could be important factor preventing the transition of MCI persons to AD.preventing the transition of MCI persons to AD.
•• ChAT levels in MCI and ADChAT levels in MCI and AD–– parietal cortex: reduced only in severe ADparietal cortex: reduced only in severe AD–– superior frontal cortexsuperior frontal cortex
•• increased in MCIincreased in MCI•• unchanged in normals and mild ADunchanged in normals and mild AD
–– hippocampushippocampus•• also increased in MCI compared to normals and mild ADalso increased in MCI compared to normals and mild AD
»» DeKosky. DeKosky. Ann NeurolAnn Neurol 2002;51:1452002;51:145
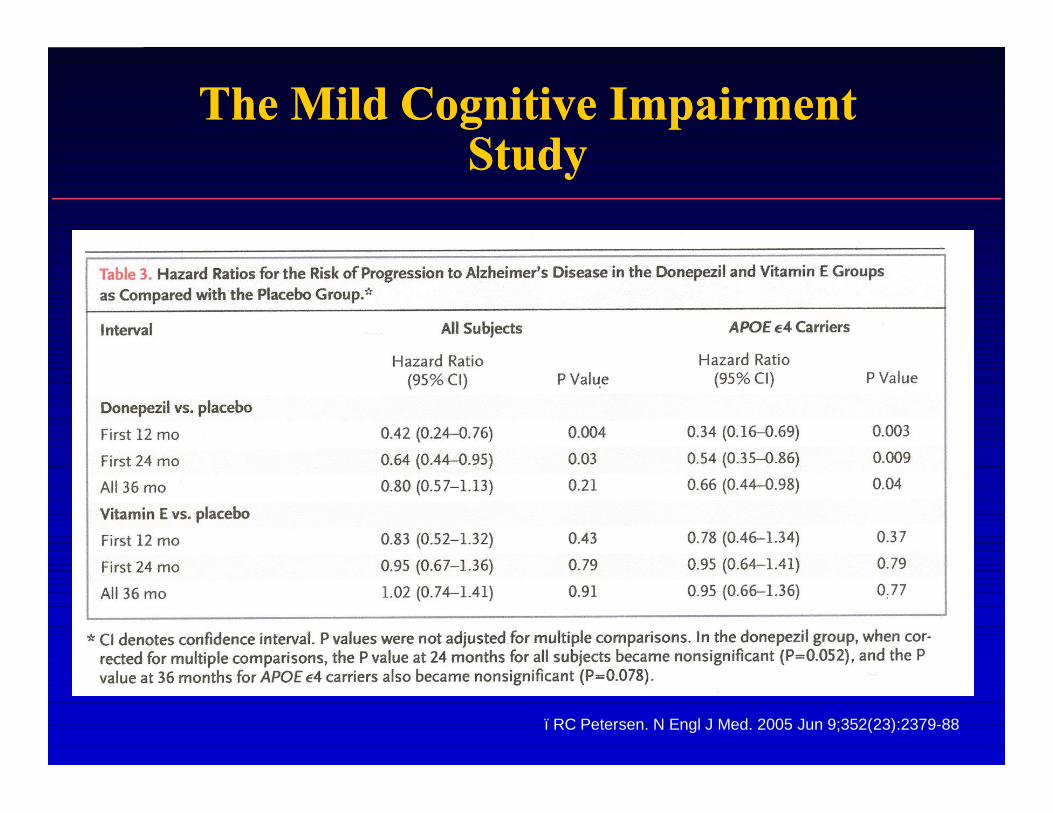
The Mild Cognitive Impairment The Mild Cognitive Impairment StudyStudy
–RC Petersen. N Engl J Med. 2005 Jun 9;352(23):2379-88
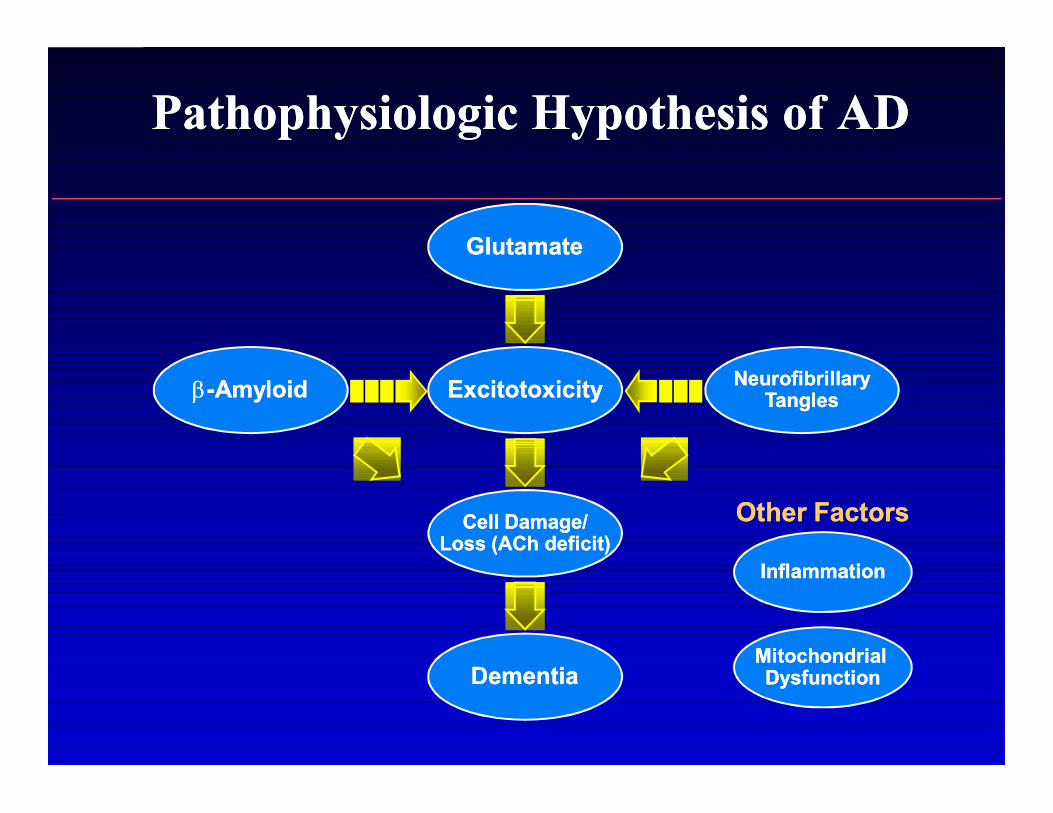
Pathophysiologic Hypothesis of ADPathophysiologic Hypothesis of AD
Mitochondrial Mitochondrial DysfunctionDysfunction
InflammationInflammation
Other FactorsOther Factors
ββ--AmyloidAmyloid
GlutamateGlutamate
ExcitotoxicityExcitotoxicity
Cell Damage/Cell Damage/Loss (ACh deficit)Loss (ACh deficit)
DementiaDementia
NeurofibrillaryNeurofibrillaryTanglesTangles

Memantine Pivotal Trials in Memantine Pivotal Trials in Moderate to Severe ADModerate to Severe AD
Study DesignStudy Design
FirstFirst--Line Therapy Line Therapy in Moderate in Moderate to Severe ADto Severe AD11
Combination Combination Memantine and Memantine and DDonepezilonepezil22
Nursing Home Nursing Home Patients With Patients With DementiaDementia33
Memantine doseMemantine dose 10 mg bid10 mg bid 10 mg bid10 mg bid(plus donepezil)(plus donepezil) 10 mg qd10 mg qd
Duration in weeksDuration in weeks 2828 2424 1212
MMSE rangeMMSE range 33--1414 55--1414 <10<10
Principal Efficacy MeasuresPrincipal Efficacy Measures
Global changeGlobal change CIBICCIBIC--PlusPlus CIBICCIBIC--PlusPlus CGICGI--CC
CognitionCognition SIBSIB SIBSIB
FunctionFunction ADCSADCS--ADLADL1919 ADCSADCS--ADLADL1919 BGPBGP--CareCare
Sources: Reisberg B, et al. N Engl J Med. 2003;348:1333-1341. Tariot P, et al. JAMA. 2004;291:317-324.Winblad B, Poritis N. Int J Geriatr Psychiatry. 1999;14:135-146.
–– In academic referral centers the accuracy of the In academic referral centers the accuracy of the diagnosis of “probable AD” is 81diagnosis of “probable AD” is 81--100%.100%.
•• Galasko et al, 1994Galasko et al, 1994•• Morris et al, 1988Morris et al, 1988•• Tierney, 1988Tierney, 1988
–– In one post mortem series, 77% of cases of In one post mortem series, 77% of cases of “possible” AD had AD.“possible” AD had AD.
•• Galasko et al, 1994Galasko et al, 1994
–– In a community based post mortem series, the In a community based post mortem series, the accuracy of the diagnosis of “probable” AD was accuracy of the diagnosis of “probable” AD was 75%75%
•• Lim et al, 1999Lim et al, 1999
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:NINCDS/ADRDA CriteriaNINCDS/ADRDA Criteria

AD Is Often MisdiagnosedAD Is Often MisdiagnosedPatient initially diagnosed with AD
Patient’s first diagnosis other than AD
Yes28%
NoNo72%72%
21%
7%
9%
14%
14%
35%
Normal agingDepression No diagnosisDementia (not AD) Stroke
OtherSource: Consumer Health Sciences,LLC. Alzheimer’s Caregiver Project. 1999.

AD Is UnderdiagnosedAD Is Underdiagnosed
•• Early AD is subtleEarly AD is subtle——the initial signs and the initial signs and symptoms are easily missedsymptoms are easily missed
•• Less than half of AD patients are diagnosedLess than half of AD patients are diagnosed
•• Undiagnosed AD patients face unnecessary Undiagnosed AD patients face unnecessary added social, financial, and medical added social, financial, and medical problemsproblems
•• Early diagnosis and appropriate intervention Early diagnosis and appropriate intervention may lessen disease burdenmay lessen disease burden
Sano M et al. N Engl J Med. 1997:336:1216-1222.

Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:MRI VolumetryMRI Volumetry
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:MRI VolumetryMRI Volumetry
• Hippocampal volume is a sensitive and specific indicator of neuropathology, regardless of the presence or absence of cognitive impairment (Nun Study)*
– predicted AD neuropathologic criteria for all cases•• 24 demented sisters24 demented sisters•• 32 non32 non--demented sistersdemented sisters
–– 8 sisters with mild memory impairment8 sisters with mild memory impairment–– 24 sisters with intact memory24 sisters with intact memory
»» Gosche et al. Neurology 58:1476Gosche et al. Neurology 58:1476--1482,20021482,2002
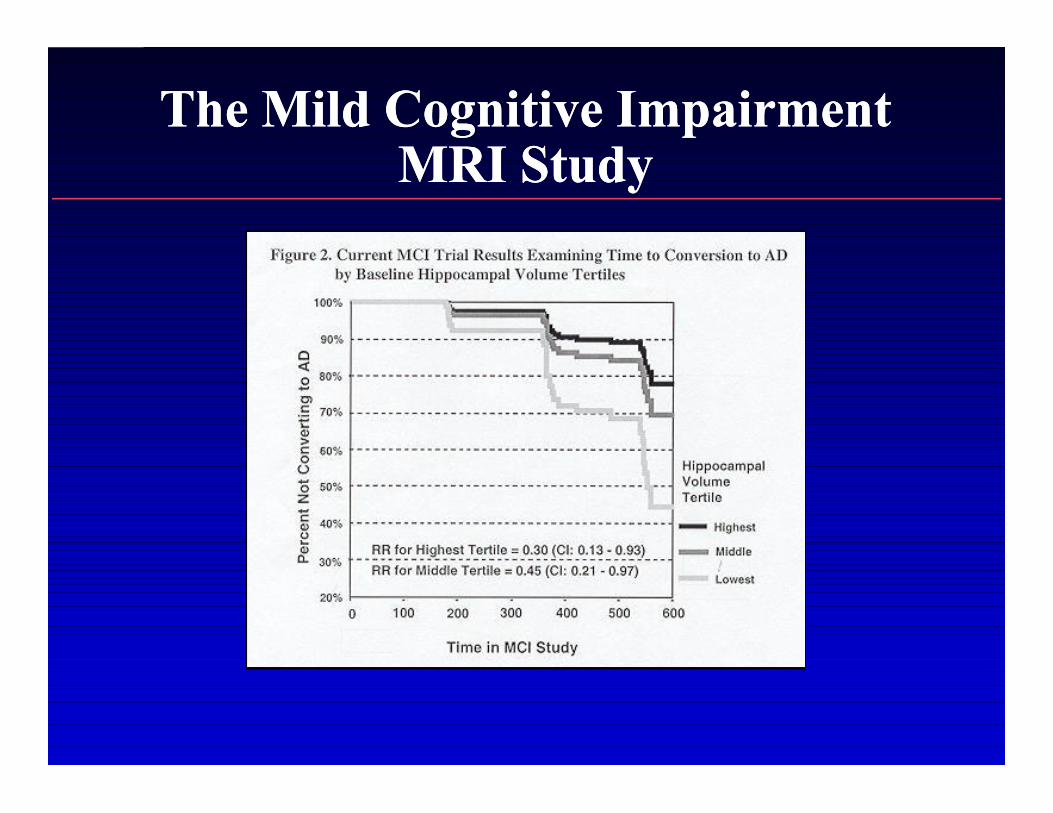
The Mild Cognitive Impairment The Mild Cognitive Impairment MRI StudyMRI Study

Typical AD PET ScanTypical AD PET Scan
Provided courtesy of M. Mega, MD, PhD, Department ofNeurology, UCLA School of Medicine.
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:PET and SPECTPET and SPECT

•• Therapeutics and Technology Assessment Therapeutics and Technology Assessment Subcommittee of the AANSubcommittee of the AAN
–– “SPECT can be considered an established “SPECT can be considered an established technique to support the clinical diagnosis of technique to support the clinical diagnosis of AD.”AD.”
–– PPV = 87PPV = 87--100% in post100% in post--mortem seriesmortem series•• Read et al, 1995Read et al, 1995•• Bonte et al, 1997Bonte et al, 1997•• Risberg et al, 1997Risberg et al, 1997
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:SPECTSPECT
•• Diagnostic pattern is bilateral reduction of Diagnostic pattern is bilateral reduction of temporoparietal cortical perfusiontemporoparietal cortical perfusion
•• Most common cause of false positives is Most common cause of false positives is Parkinson’s disease and related syndromesParkinson’s disease and related syndromes
•• Sensitivity in clinical series relatively lowSensitivity in clinical series relatively low–– average = 79% (range 29average = 79% (range 29--100%) 100%) –– true positives higher in more advanced diseasetrue positives higher in more advanced disease
•• mild = 40mild = 40--70% vs severe = 8070% vs severe = 80--90%90%
–– 20% of AD patients show unilateral defects20% of AD patients show unilateral defects
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:SPECTSPECT

Human Amyloid PET ImagingHuman Amyloid PET ImagingAVAV--45 (45 (florbetapir F18)florbetapir F18)
Clark C. JAMA 305:275-283, 2011
Human Amyloid PET ImagingHuman Amyloid PET ImagingAVAV--45 (45 (florbetapir F18)florbetapir F18)
•• Phase 3 histopathology studyPhase 3 histopathology study11
–– 35 subjects expected to die < 6 months35 subjects expected to die < 6 months•• 18/19 (97%) of AD subjects positive scan18/19 (97%) of AD subjects positive scan•• 0/16 normal subjects positive scan0/16 normal subjects positive scan
–– 74 young (1874 young (18--50) normal subjects50) normal subjects•• All 74 amyloid negativeAll 74 amyloid negative
•• Phase 2 studiesPhase 2 studies2,32,3
–– Positive scan predicts conversion from MCI to AD over 2Positive scan predicts conversion from MCI to AD over 2--4 years4 years•• FDA approval to estimate amyloid plaque density: April 10, 2012FDA approval to estimate amyloid plaque density: April 10, 2012
–– Not covered by insuranceNot covered by insurance–– Centers for Medicare & Medicaid Services (CMS) meeting Centers for Medicare & Medicaid Services (CMS) meeting
1/30/13 concluded low to intermediate confidence that amyloid 1/30/13 concluded low to intermediate confidence that amyloid PET results affect health outcomes…recommended only PET results affect health outcomes…recommended only “coverage with evidence development” on July 3rd“coverage with evidence development” on July 3rd
1. Clark C. JAMA 305:275-283, 20112. Forsberg. Neurobiol Aging 29:456, 20083. Okello. Neurology 73:744, 2009

A Randomized, Multicenter, Multicountry Study to Evaluate the A Randomized, Multicenter, Multicountry Study to Evaluate the Effectiveness of Florbetapir (18F) PET Imaging in Changing Patient Effectiveness of Florbetapir (18F) PET Imaging in Changing Patient Management and to Evaluate the Relationship Between Florbetapir Management and to Evaluate the Relationship Between Florbetapir
PET Scan Status and Cognitive DeclinePET Scan Status and Cognitive Decline
•• This study is designed to determine the effectiveness This study is designed to determine the effectiveness of florbetapir (18F) in changing patient management of florbetapir (18F) in changing patient management and to evaluate the association between scan status and to evaluate the association between scan status and cognitive decline. and cognitive decline.
•• N=600N=600•• Timeline: October 2012 to December 2014Timeline: October 2012 to December 2014•• Primary Outcome Measures: Primary Outcome Measures:
–– Patient Management Patient Management •• Comparison of the proportion of patients who have a change Comparison of the proportion of patients who have a change
in management from baseline to 3 months for patients who in management from baseline to 3 months for patients who receive scan results immediately (intervention arm) and receive scan results immediately (intervention arm) and those who receive scan results 12 months later (control those who receive scan results 12 months later (control arm).arm).
–– Patient Prognosis Patient Prognosis •• Association between scan status and cognitive decline.Association between scan status and cognitive decline.
•• Genetic mutations account for 45Genetic mutations account for 45--90% of early onset 90% of early onset familial AD cases, i.e. age <65familial AD cases, i.e. age <65
–– PSPS--1 mutations in 301 mutations in 30--70% of patients70% of patients–– PSPS--2 account for another 5%2 account for another 5%–– APP account for another 10APP account for another 10--15%15%
•• High PPV, assumed to be 100% for eventual High PPV, assumed to be 100% for eventual development of ADdevelopment of AD
•• Pre and post test genetic counseling, education, and Pre and post test genetic counseling, education, and support necessary for asymptomatic positivessupport necessary for asymptomatic positives
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:Gene Mutation AnalysisGene Mutation Analysis
•• AthenaAthena–– + in 44+ in 44--64% of AD cases64% of AD cases–– an e4 allele indicates a 97% PPV in persons with an e4 allele indicates a 97% PPV in persons with
dementia that AD is a contributing cause. dementia that AD is a contributing cause. Therefore, “the presence of the e4 allele usually Therefore, “the presence of the e4 allele usually rules out other causes of dementia.”rules out other causes of dementia.”
–– absence of an e4 allele does not rule out ADabsence of an e4 allele does not rule out AD–– results cannot be interpreted for asymptomatic results cannot be interpreted for asymptomatic
persons, therefore, “our policy is not to test persons, therefore, “our policy is not to test asymptomatic individuals”asymptomatic individuals”
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:Apolipoprotein E GenotypeApolipoprotein E Genotype

•• With appropriate cutoffs, low AWith appropriate cutoffs, low Aββ42 and high tau levels in CSF support 42 and high tau levels in CSF support diagnosis of AD vs. normal elders with a sensitivity of 77% and diagnosis of AD vs. normal elders with a sensitivity of 77% and specificity of 90% specificity of 90%
–– many cases in nonmany cases in non--diagnostic rangediagnostic range–– positives may be useful in distinguishing early AD from normal agingpositives may be useful in distinguishing early AD from normal aging–– 26/74 (35%) of cases with other neurological disorders classified as AD26/74 (35%) of cases with other neurological disorders classified as AD
•• ?high risk of false + in clinical practice?high risk of false + in clinical practice•• awaiting post mortem information awaiting post mortem information
•• When AT index in AD range, phosphoWhen AT index in AD range, phospho--tau discriminates AD from FTD tau discriminates AD from FTD and DLBand DLB
–– Sensitivity 72Sensitivity 72--85%; specificity 7485%; specificity 74--85%85%
Galasko et al. Arch Neurol. 55:937Galasko et al. Arch Neurol. 55:937--945,1998945,1998
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:CSF Aβ42 and TauCSF Aβ42 and Tau
•• Consensus Report of the Working Group on: Consensus Report of the Working Group on: “Molecular and Biochemical Markers of Alzheimer’s “Molecular and Biochemical Markers of Alzheimer’s Disease”Disease”
–– Regan Research Institute of the Alzheimer AssociationRegan Research Institute of the Alzheimer Association–– National Institute on Aging Working GroupNational Institute on Aging Working Group
•• For suspected earlyFor suspected early--onset familial AD it is appropriate onset familial AD it is appropriate to search for mutations e.g. presenilin 1to search for mutations e.g. presenilin 1
•• For lateFor late--onset and sporadic ADonset and sporadic AD–– ApoE e4 “can add confidence to the clinical diagnosis”ApoE e4 “can add confidence to the clinical diagnosis”–– Among other proposed markers, CSF AβAmong other proposed markers, CSF Aβ4242 and tau come and tau come
closest to fulfilling criteria for a useful biomarkerclosest to fulfilling criteria for a useful biomarker
Neurobiol of Aging. 19:109Neurobiol of Aging. 19:109--116,1998116,1998
Diagnosis of Alzheimer’s Disease:Diagnosis of Alzheimer’s Disease:Consensus on BiomarkersConsensus on Biomarkers
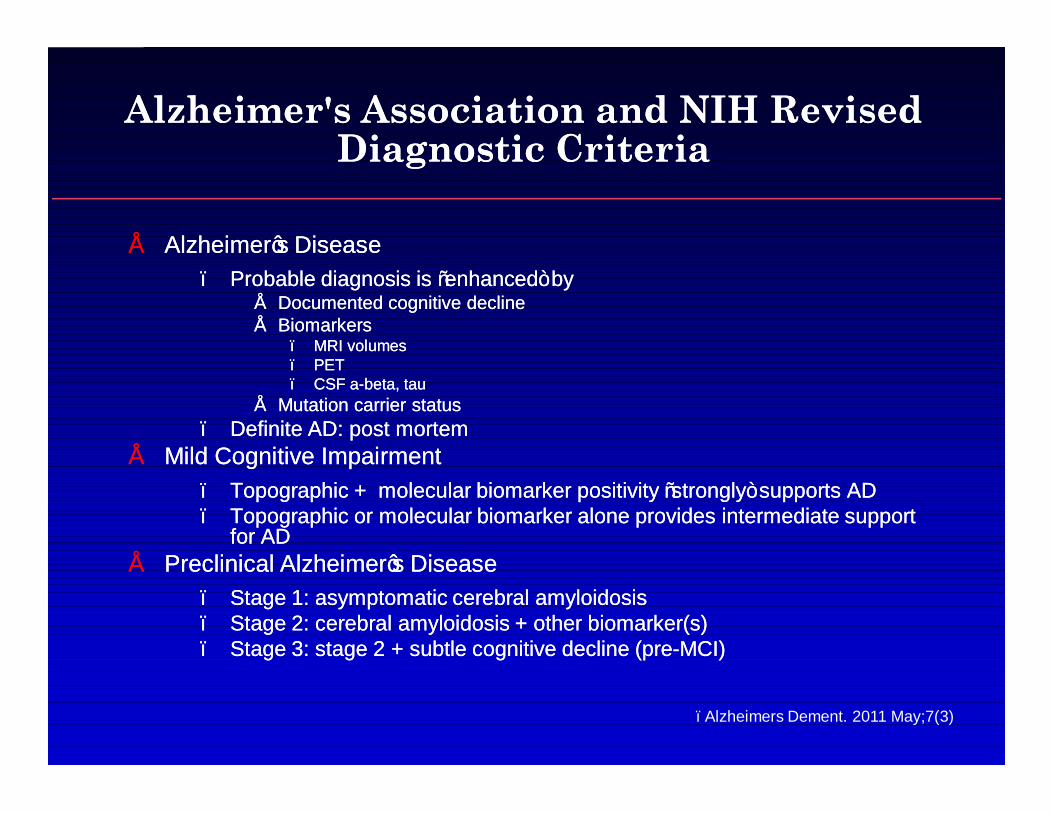
Alzheimer's Association and NIH Revised Alzheimer's Association and NIH Revised Diagnostic CriteriaDiagnostic Criteria
•• Alzheimer’s DiseaseAlzheimer’s Disease–– Probable diagnosis is “enhanced” byProbable diagnosis is “enhanced” by
•• Documented cognitive declineDocumented cognitive decline•• BiomarkersBiomarkers
–– MRI volumesMRI volumes–– PETPET–– CSF aCSF a--beta, taubeta, tau
•• Mutation carrier statusMutation carrier status–– Definite AD: post mortemDefinite AD: post mortem
•• Mild Cognitive ImpairmentMild Cognitive Impairment–– Topographic + molecular biomarker positivity “strongly” supports ADTopographic + molecular biomarker positivity “strongly” supports AD–– Topographic or molecular biomarker alone provides intermediate support Topographic or molecular biomarker alone provides intermediate support
for ADfor AD•• Preclinical Alzheimer’s DiseasePreclinical Alzheimer’s Disease
–– Stage 1: asymptomatic cerebral amyloidosisStage 1: asymptomatic cerebral amyloidosis–– Stage 2: cerebral amyloidosis + other biomarker(s)Stage 2: cerebral amyloidosis + other biomarker(s)–– Stage 3: stage 2 + subtle cognitive decline (preStage 3: stage 2 + subtle cognitive decline (pre--MCI)MCI)
–Alzheimers Dement. 2011 May;7(3)
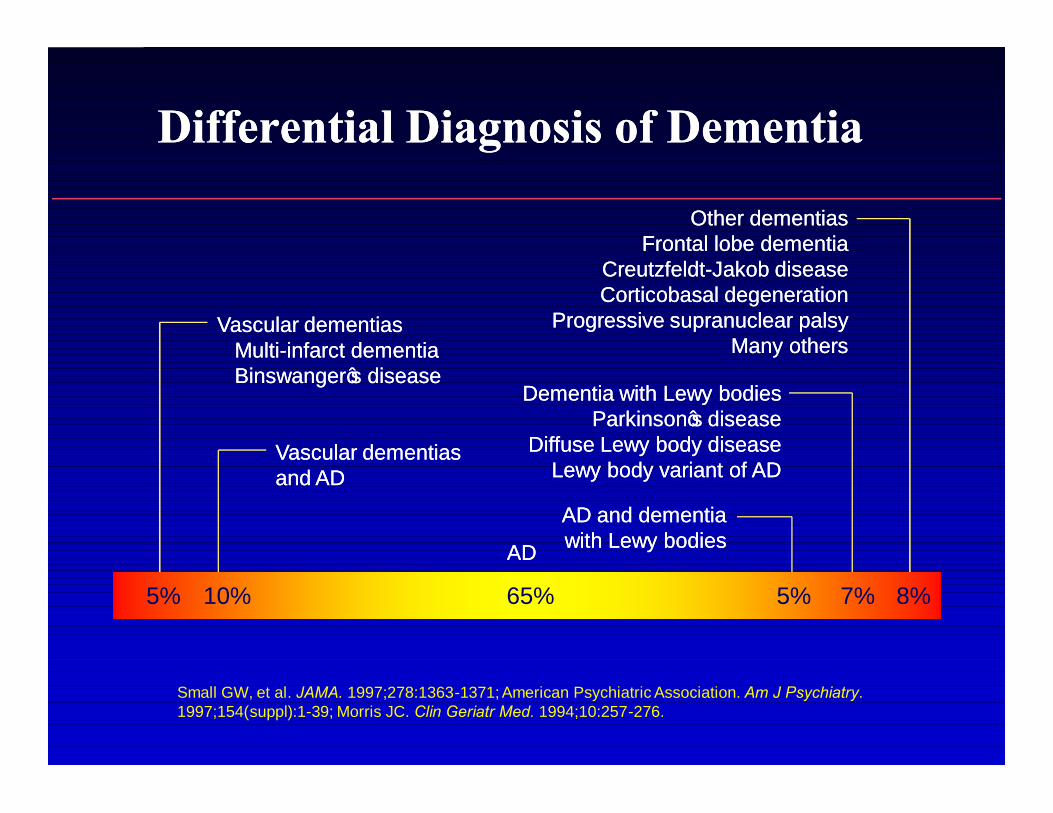
Differential Diagnosis of DementiaDifferential Diagnosis of Dementia
5% 10% 65% 5% 7% 8%
Dementia with Lewy bodiesDementia with Lewy bodiesParkinson’s diseaseParkinson’s disease
Diffuse Lewy body diseaseDiffuse Lewy body diseaseLewy body variant of ADLewy body variant of AD
Vascular dementias Vascular dementias and ADand AD
Other dementiasOther dementiasFrontal lobe dementiaFrontal lobe dementia
CreutzfeldtCreutzfeldt--Jakob diseaseJakob diseaseCorticobasal degenerationCorticobasal degeneration
Progressive supranuclear palsyProgressive supranuclear palsyMany othersMany others
AD and dementia AD and dementia with Lewy bodieswith Lewy bodies
Vascular dementiasVascular dementiasMultiMulti--infarct dementiainfarct dementiaBinswanger’s diseaseBinswanger’s disease
ADAD
Small GW, et al. JAMA. 1997;278:1363-1371; American Psychiatric Association. Am J Psychiatry. 1997;154(suppl):1-39; Morris JC. Clin Geriatr Med. 1994;10:257-276.
Vascular DementiaVascular Dementia
•• Second or third most common cause of dementiaSecond or third most common cause of dementia
•• Affects 5.2% of the population over 90 years of ageAffects 5.2% of the population over 90 years of age
•• Associated with:Associated with:–– StrokeStroke–– Cerebrovascular diseaseCerebrovascular disease
•• Often coexists with AD and may share common Often coexists with AD and may share common pathologypathology
•• Causes decline in cognition, function, and behaviorCauses decline in cognition, function, and behavior
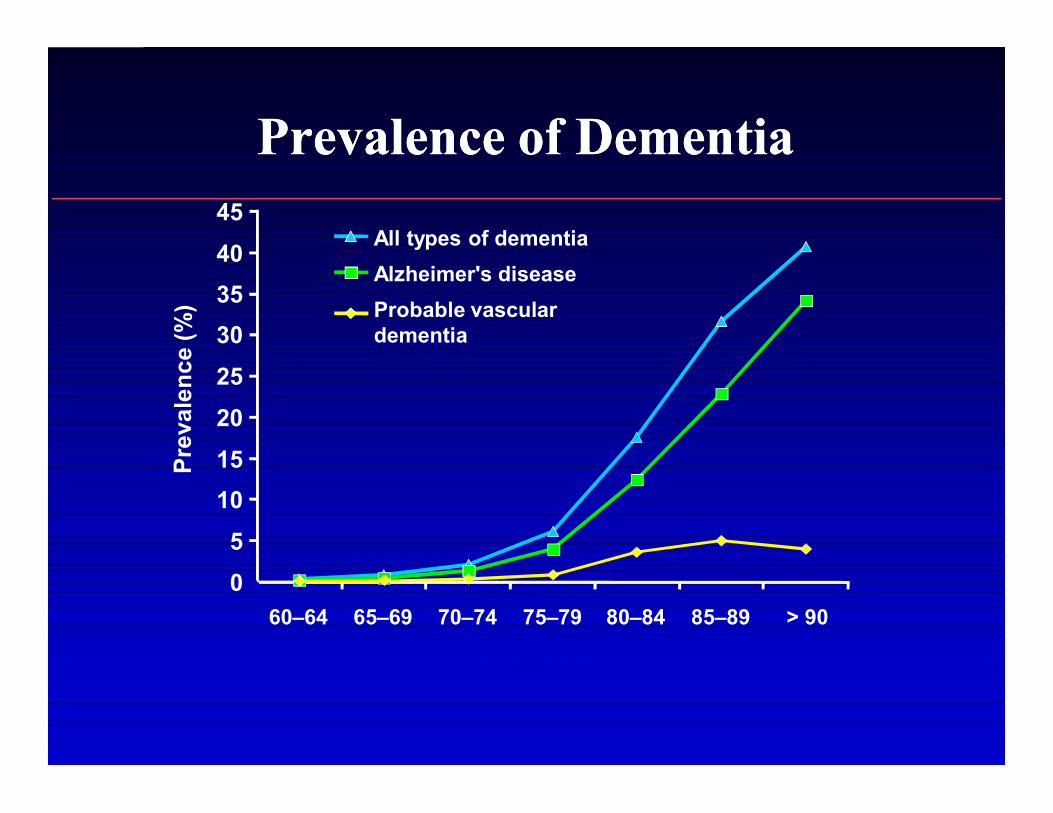
Prevalence of DementiaPrevalence of Dementia
05
1015202530354045
60–64 65–69 70–74 75–79 80–84 85–89 > 90
All types of dementiaAlzheimer's diseaseProbable vasculardementia
Age (years)

Frequency of VaDFrequency of VaDin Dementia Autopsy Seriesin Dementia Autopsy Series
Study (n)Study (n) VaDVaD±± (Pure)(Pure) PopulationPopulation
Brun 1994 (175)Brun 1994 (175) 70% (34%)70% (34%) Dem StudyDem Study
Galasko 1994(170)Galasko 1994(170) 9% (2%)9% (2%) AD Res CtrsAD Res Ctrs
Drach 1997 (59)Drach 1997 (59) 27% (12%)27% (12%) Nursing HomeNursing Home
Nolan 1998 (87)Nolan 1998 (87) 37% (0%)37% (0%) Dem ClinicDem Clinic
Lim 1999 (134)Lim 1999 (134) 34%+ (3%)34%+ (3%) Dem RegisterDem Register
Duara 2000 (307)Duara 2000 (307) 16% (4%)16% (4%) Brain BankBrain Bank
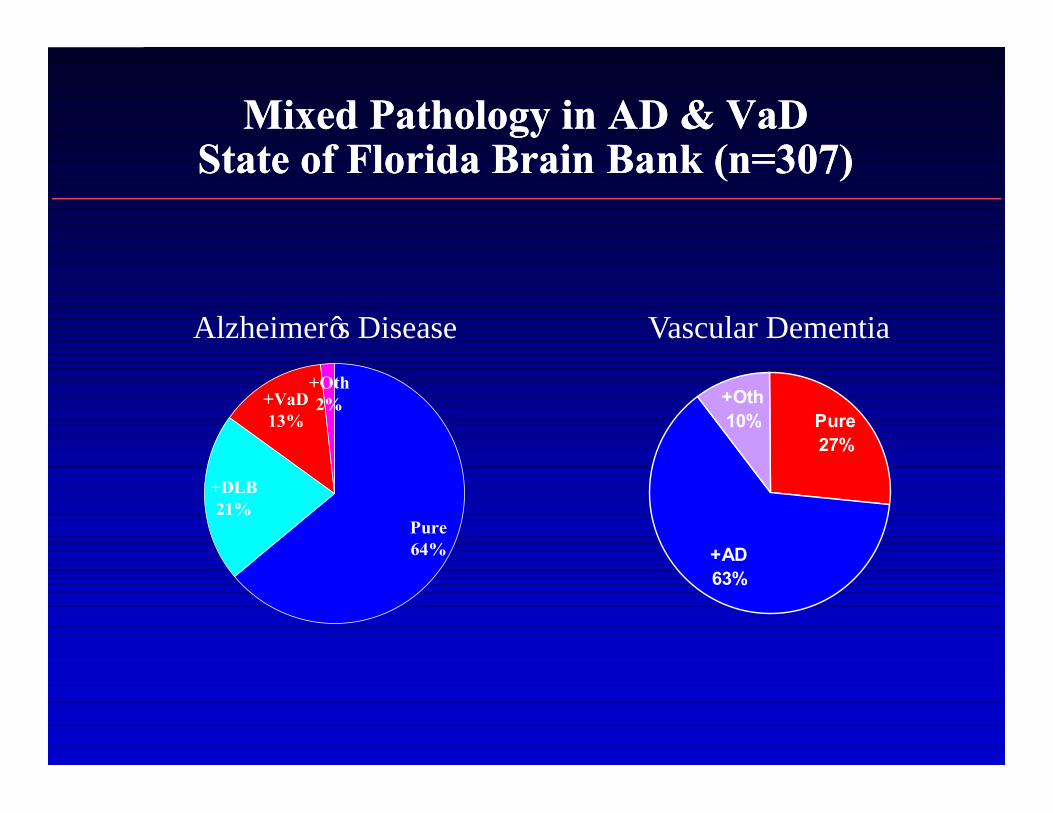
Mixed Pathology in AD & VaDMixed Pathology in AD & VaDState of Florida Brain Bank (n=307)State of Florida Brain Bank (n=307)
Pure27%
+AD63%
+Oth10%
Pure64%
+DLB21%
+VaD13%
+Oth2%
Alzheimer’s Disease Vascular Dementia
Campbell, Stephens, Ballard, 2001.
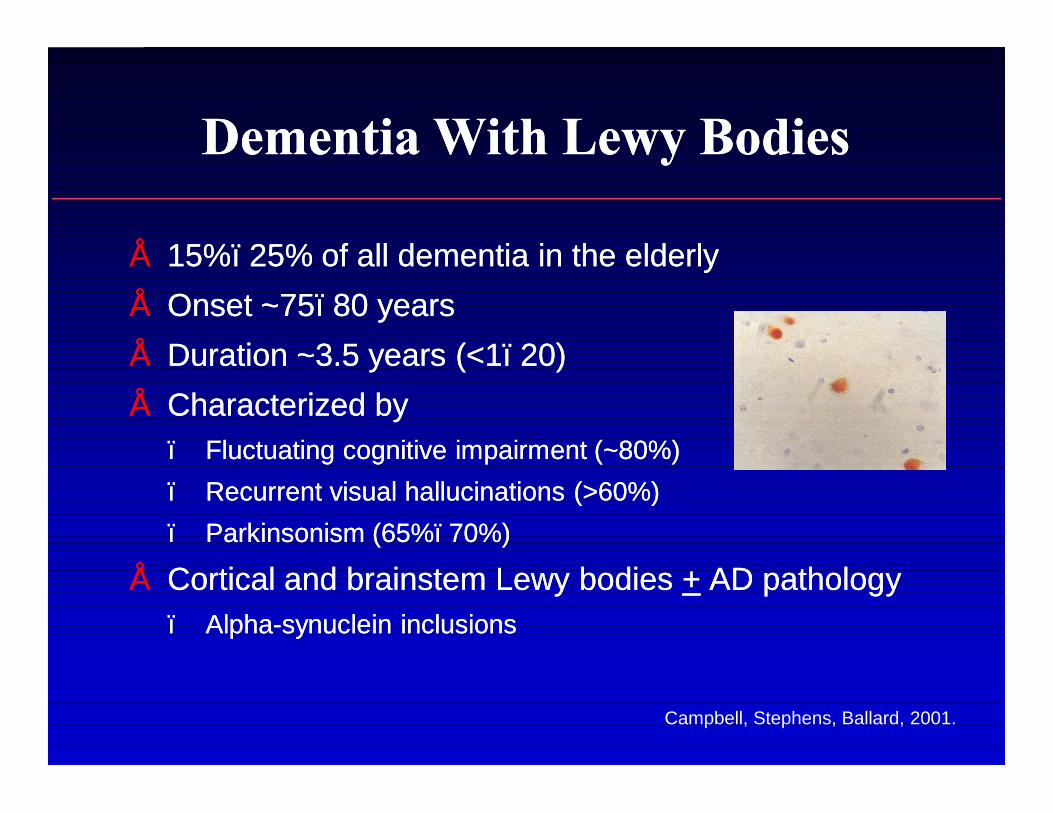
Dementia With Lewy BodiesDementia With Lewy Bodies
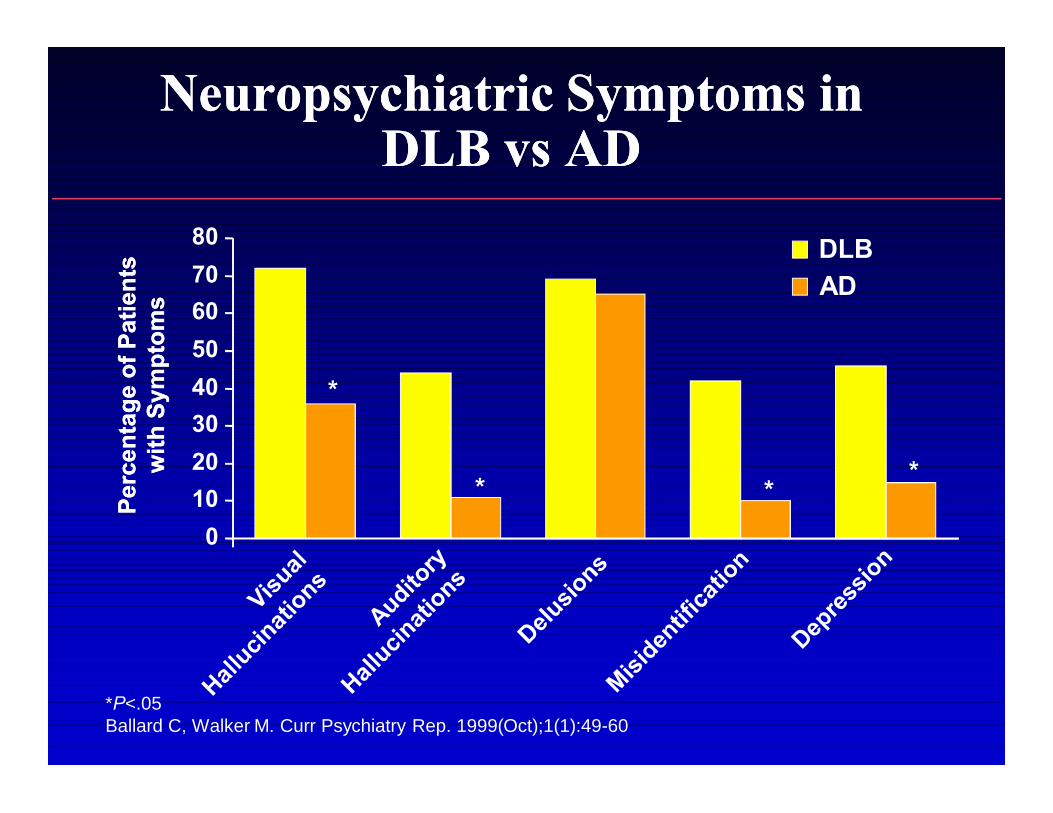
•• 15%15%––25% of all dementia in the elderly25% of all dementia in the elderly•• Onset ~75Onset ~75––80 years80 years•• Duration ~3.5 years (<1Duration ~3.5 years (<1––20)20)•• Characterized by Characterized by
–– Fluctuating cognitive impairment (~80%)Fluctuating cognitive impairment (~80%)–– Recurrent visual hallucinations (>60%)Recurrent visual hallucinations (>60%)–– Parkinsonism (65%Parkinsonism (65%––70%)70%)
•• Cortical and brainstem Lewy bodies Cortical and brainstem Lewy bodies ++ AD pathologyAD pathology–– AlphaAlpha--synuclein inclusionssynuclein inclusions
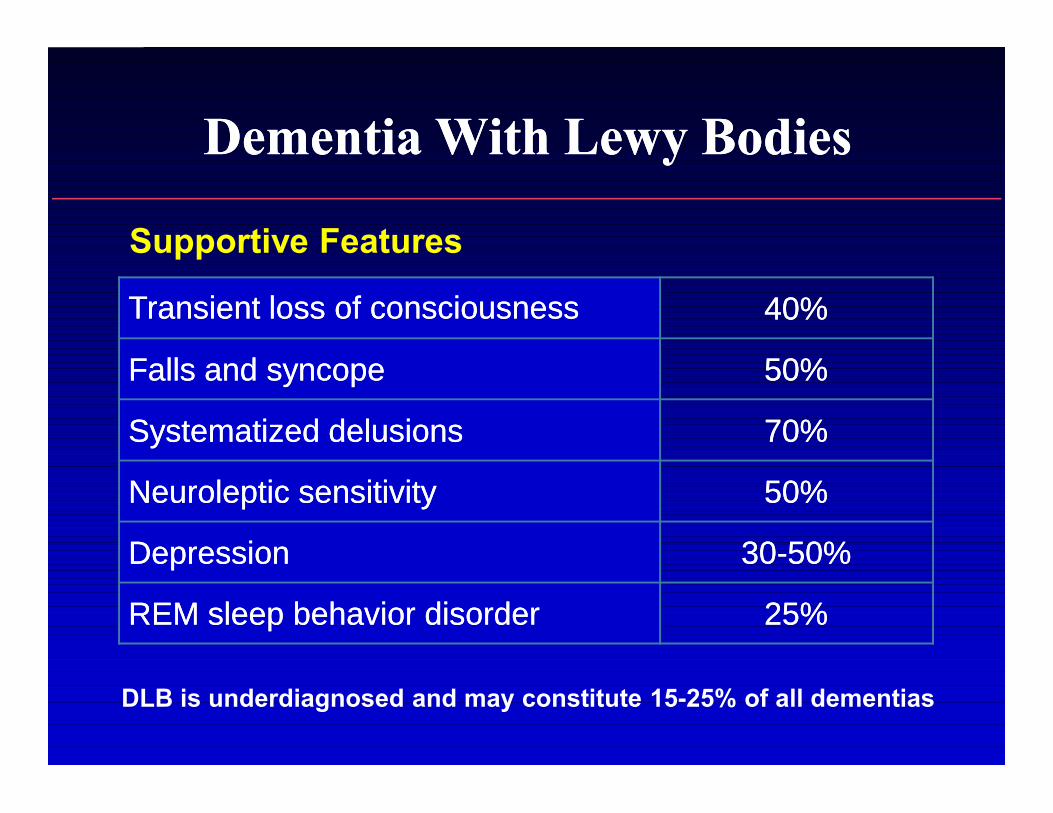
Dementia With Lewy BodiesDementia With Lewy Bodies
DLB is underdiagnosed and may constitute 15-25% of all dementias
Supportive Features
Transient loss of consciousnessTransient loss of consciousness 40%40%
Falls and syncopeFalls and syncope 50%50%
Systematized delusionsSystematized delusions 70%70%
Neuroleptic sensitivityNeuroleptic sensitivity 50%50%
DepressionDepression 3030--50%50%
REM sleep behavior disorderREM sleep behavior disorder 25%25%
Dementia With Lewy BodiesDementia With Lewy Bodies
•• Presence of dementia, gait/balance disorder, Presence of dementia, gait/balance disorder, prominent hallucinations and delusions, sensitivity to prominent hallucinations and delusions, sensitivity to traditional antipsychotics, and fluctuations in alertnesstraditional antipsychotics, and fluctuations in alertness
•• Neuropsychologic tests do not reliably differentiate Neuropsychologic tests do not reliably differentiate DLB from either AD or VaD DLB from either AD or VaD
•• Patients with DLB show less temporal lobe atrophy on Patients with DLB show less temporal lobe atrophy on MRI and more hypoperfusion on SPECT and PET in MRI and more hypoperfusion on SPECT and PET in the occipital lobes than do patients with ADthe occipital lobes than do patients with AD
•• Neuroimaging, however, has not proven successful in Neuroimaging, however, has not proven successful in differentiating DLB from ADdifferentiating DLB from AD
Heyman A et al. Neurology. 1999;52:1839-1844. Ballard CG et al. Dement Geriatr Cogn Disord. 1999;10:104-108.
Barber R et al. Neurology. 1999;52:1153-1158.
*
* **
*P<.05Ballard C, Walker M. Curr Psychiatry Rep. 1999(Oct);1(1):49-60
01020304050607080 DLB
AD
Perc
enta
ge o
f Pat
ient
sPe
rcen
tage
of P
atie
nts
with
Sym
ptom
sw
ith S
ympt
oms
Neuropsychiatric Symptoms in Neuropsychiatric Symptoms in DLB vs ADDLB vs AD
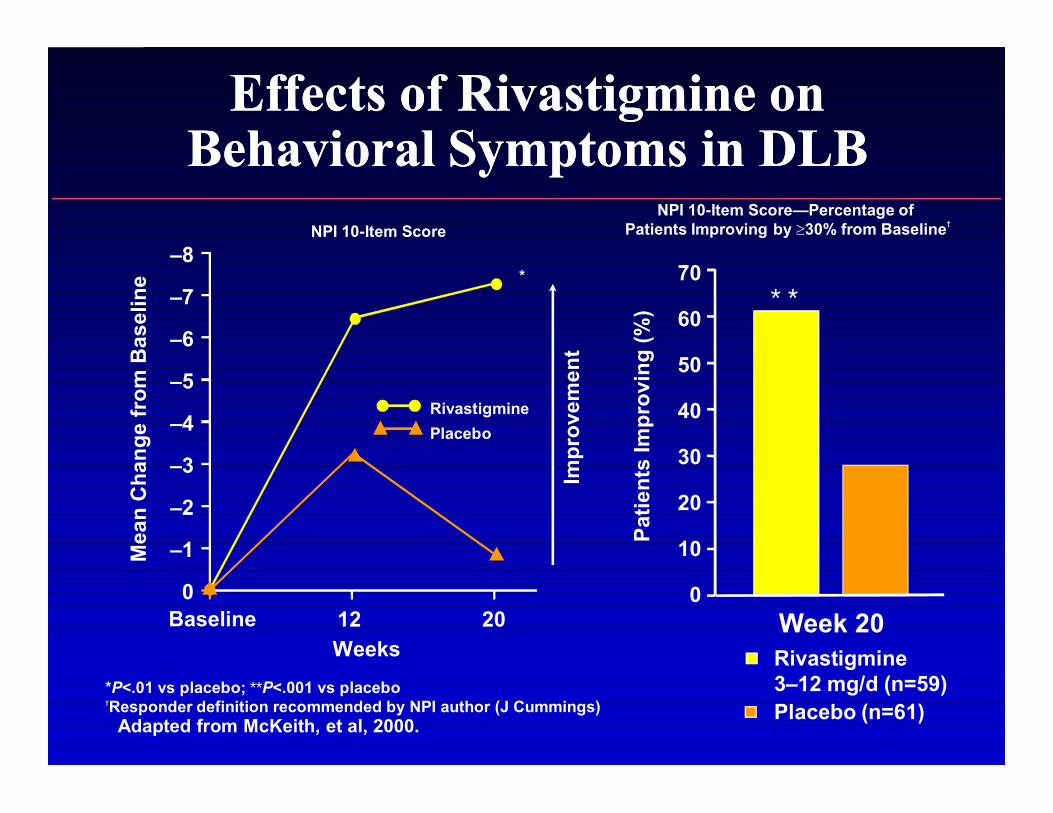
*P<.01 vs placebo; **P<.001 vs placebo†Responder definition recommended by NPI author (J Cummings)
Adapted from McKeith, et al, 2000.
Baseline
Impr
ovem
ent
NPI 10-Item Score
*
Mea
n C
hang
e fr
om B
asel
ine
–8
–7
–6
–5
–4
–3
–2
–1
0
RivastigminePlacebo
12 20Weeks Rivastigmine
3–12 mg/d (n=59)Placebo (n=61)
NPI 10-Item Score—Percentage of Patients Improving by ≥30% from Baseline†
* *70
60
50
40
30
20
10
0
Patie
nts
Impr
ovin
g (%
)Week 20
Effects of Rivastigmine on Effects of Rivastigmine on Behavioral Symptoms in DLBBehavioral Symptoms in DLB

Perry, et al, 1985; Korczyn, 2001.
PD and DementiaPD and Dementia
•• At least oneAt least one--third of PD patients develop third of PD patients develop dementia dementia
•• Patients with PD have degeneration of the Patients with PD have degeneration of the nucleus basalis of Meynert and low brain nucleus basalis of Meynert and low brain ChAT levelsChAT levels
•• The dementia of PD is not improved by The dementia of PD is not improved by dopaminomimetic drugsdopaminomimetic drugs
•• ChE inhibitor therapy in PD may be beneficialChE inhibitor therapy in PD may be beneficial

Frontotemporal DementiaFrontotemporal Dementia
•• FTD is the most common of the FTD is the most common of the neurodegenerative syndromes produced by neurodegenerative syndromes produced by frontotemporal lobar degeneration, and is frontotemporal lobar degeneration, and is less common than AD, VaD, and DLBless common than AD, VaD, and DLB
•• FTD is characterized more by the pattern of FTD is characterized more by the pattern of behavioral deficits than by behavioral deficits than by neuropsychological impairmentneuropsychological impairment
Perry RJ. Neurology. 2001;56(11):46-51.Perry RJ. Neurology. 2000;54(12):2277-84. Morris JC. Neurology. 2001;57(2):173-174.

Frontotemporal DementiaFrontotemporal Dementia
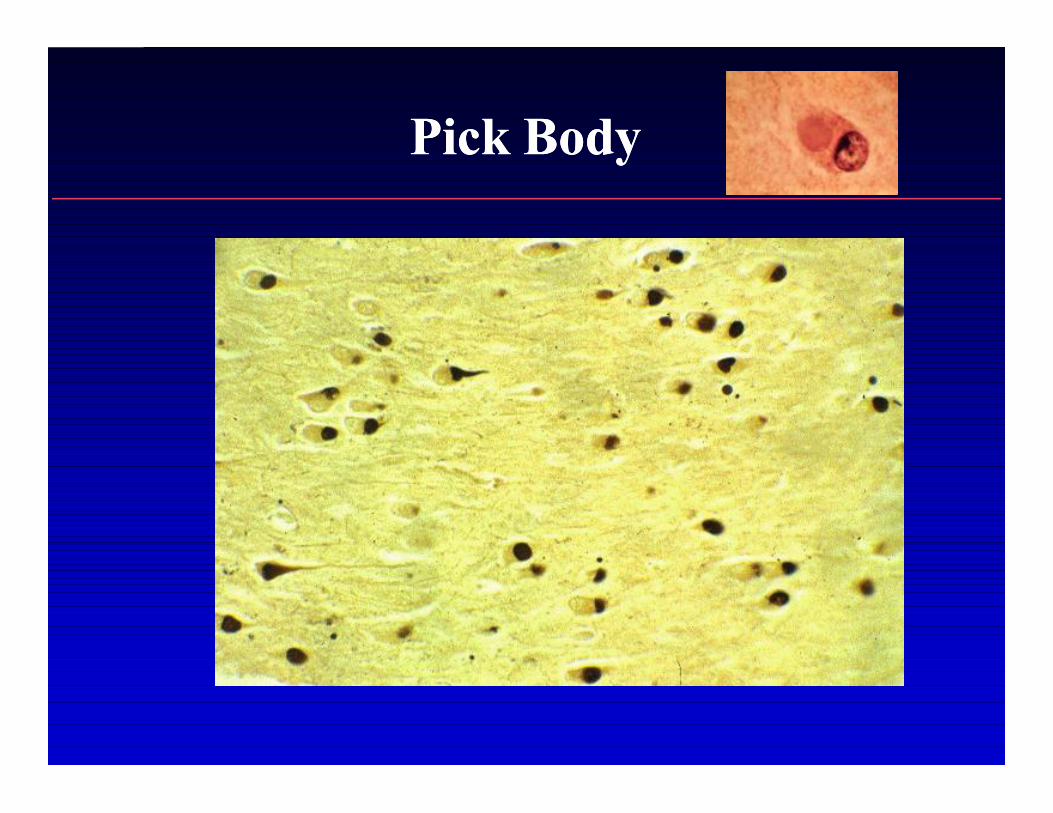
Pick BodyPick Body
•• Clinical features of FTD include decline in personal Clinical features of FTD include decline in personal hygiene and grooming, mental rigidity and inflexibility, hygiene and grooming, mental rigidity and inflexibility, distractibility and impersistence, hyperorality and distractibility and impersistence, hyperorality and dietary changes, perseverative and stereotyped dietary changes, perseverative and stereotyped behavior, and wanderingbehavior, and wandering
•• Current treatment options only address symptomatic Current treatment options only address symptomatic management, and there is no evidence for the use of management, and there is no evidence for the use of AChEIs in this conditionAChEIs in this condition
–– Serotonin deficit may relate to behaviorSerotonin deficit may relate to behavior
•• Supportive role of neuroimagingSupportive role of neuroimaging
Frontotemporal DementiaFrontotemporal Dementia
Perry RJ. Neurology. 2001;56(11):46-51.Perry RJ. Neurology. 2000;54(12):2277-84. Morris JC. Neurology. 2001;57(2):173-174.
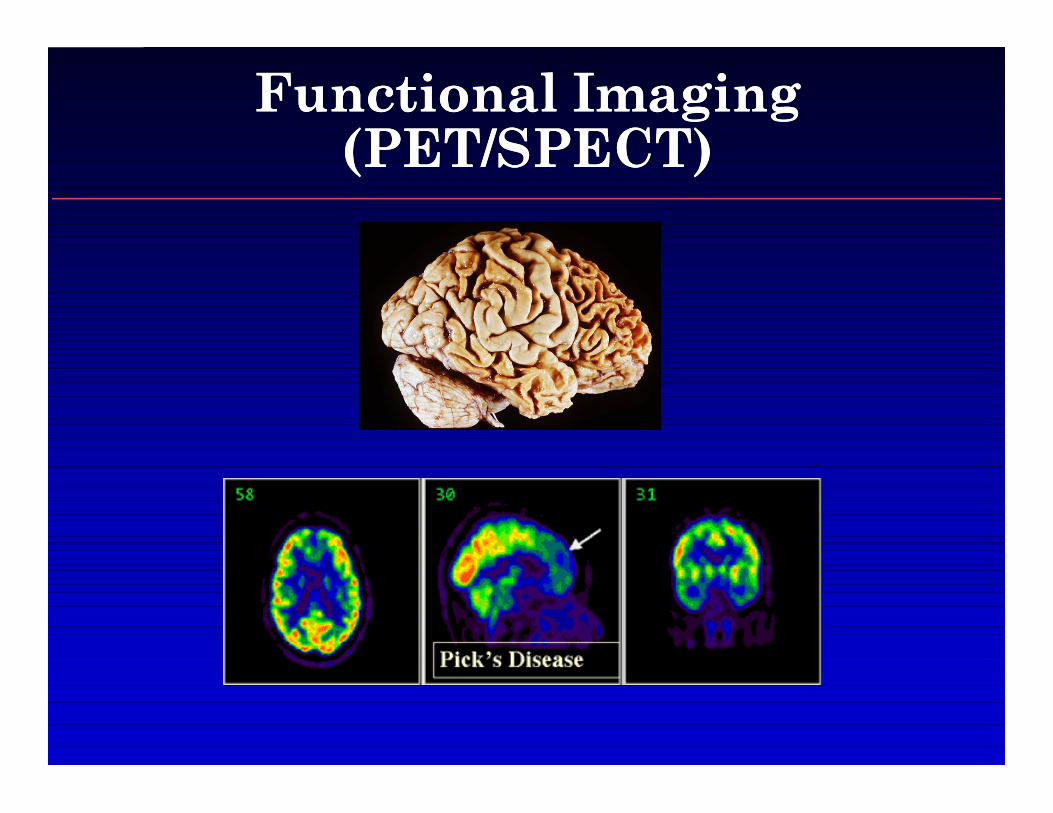
Functional Imaging Functional Imaging (PET/SPECT)(PET/SPECT)

MRI: Frontotemporal DementiaMRI: Frontotemporal Dementia
3
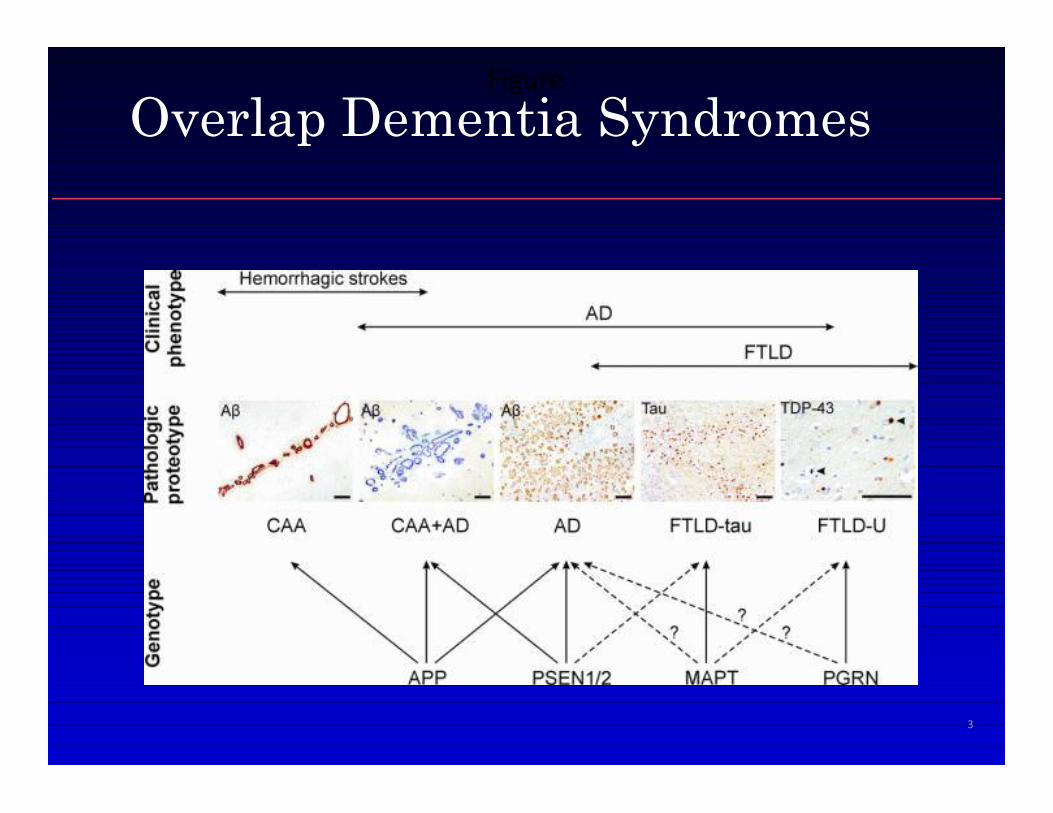
FigureOverlap Dementia Syndromes
Evolving Nosology of “Dementia” Evolving Nosology of “Dementia” DisordersDisorders
•• “Dementia: A word to be forgotten” “Dementia: A word to be forgotten”
•• Molecular, imaging, and behavioral observations will Molecular, imaging, and behavioral observations will define disease in the futuredefine disease in the future
Genetic/Environmental factors: testsGenetic/Environmental factors: testsVV
Pathologic changes in brain: brain imaging/CSFPathologic changes in brain: brain imaging/CSFVV
Change over time: preclinical diagnosisChange over time: preclinical diagnosisVV
Topographic variations: brain imagingTopographic variations: brain imagingVV
Behavioral and cognitive syndromes: History & examBehavioral and cognitive syndromes: History & exam
Trachtenberg. Arch Neurol 65:593-595, 2008
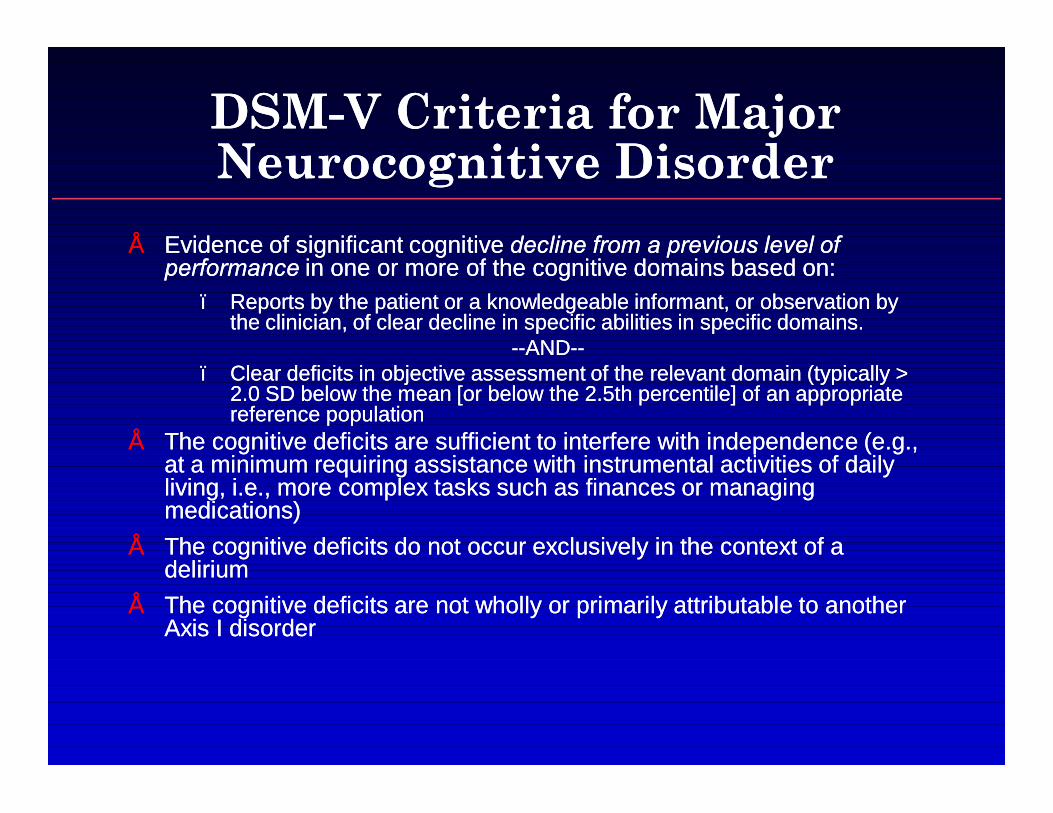
DSMDSM--V Criteria for Major V Criteria for Major Neurocognitive DisorderNeurocognitive Disorder
•• Evidence of significant cognitive Evidence of significant cognitive decline from a previous level of decline from a previous level of performance performance in one or more of the cognitive domains based on:in one or more of the cognitive domains based on:
–– Reports by the patient or a knowledgeable informant, or observation by Reports by the patient or a knowledgeable informant, or observation by the clinician, of clear decline in specific abilities in specific domains.the clinician, of clear decline in specific abilities in specific domains.
----ANDAND----–– Clear deficits in objective assessment of the relevant domain (typically > Clear deficits in objective assessment of the relevant domain (typically >
2.0 SD below the mean [or below the 2.5th percentile] of an appropriate 2.0 SD below the mean [or below the 2.5th percentile] of an appropriate reference populationreference population
•• The cognitive deficits are sufficient to interfere with independence (e.g., The cognitive deficits are sufficient to interfere with independence (e.g., at a minimum requiring assistance with instrumental activities of daily at a minimum requiring assistance with instrumental activities of daily living, i.e., more complex tasks such as finances or managing living, i.e., more complex tasks such as finances or managing medications)medications)
•• The cognitive deficits do not occur exclusively in the context of a The cognitive deficits do not occur exclusively in the context of a deliriumdelirium
•• The cognitive deficits are not wholly or primarily attributable to another The cognitive deficits are not wholly or primarily attributable to another Axis I disorderAxis I disorder

DSMDSM--V Criteria for Minor V Criteria for Minor Neurocognitive DisorderNeurocognitive Disorder
•• Evidence of minor cognitive Evidence of minor cognitive decline from a previous level of decline from a previous level of performance performance in one or more cognitive domains based on:in one or more cognitive domains based on:
–– Reports by the patient or a knowledgeable informant, or observation by the clinician, Reports by the patient or a knowledgeable informant, or observation by the clinician, of minor levels of decline in specific abilities as outlined for the specific domains of minor levels of decline in specific abilities as outlined for the specific domains above. Typically these will involve greater difficulty performing these tasks, or the above. Typically these will involve greater difficulty performing these tasks, or the use of compensatory strategies.use of compensatory strategies.
----ANDAND——---- Mild deficits on objective cognitive assessment (typically 1 to 2.0 SD below the Mild deficits on objective cognitive assessment (typically 1 to 2.0 SD below the
mean [or in the 2.5th to 16mean [or in the 2.5th to 16thth percentile] of an appropriate reference population (i.e., percentile] of an appropriate reference population (i.e., age, gender, education, premorbid intellect, and culturally adjusted).age, gender, education, premorbid intellect, and culturally adjusted).
–– When serial measurements are available, a significant (e.g., 0.5 SD) decline from When serial measurements are available, a significant (e.g., 0.5 SD) decline from the patients' own baseline would serve as more definitive evidence of declinethe patients' own baseline would serve as more definitive evidence of decline
•• The cognitive deficits are not sufficient to interfere with independence The cognitive deficits are not sufficient to interfere with independence (Instrumental Activities of Daily Living are preserved), but greater effort (Instrumental Activities of Daily Living are preserved), but greater effort and compensatory strategies may be required to maintain and compensatory strategies may be required to maintain independence.independence.
•• The cognitive deficits do not occur exclusively in the context of a The cognitive deficits do not occur exclusively in the context of a deliriumdelirium
•• The cognitive deficits are not wholly or primarily attributable to another The cognitive deficits are not wholly or primarily attributable to another Axis I disorderAxis I disorder

What about treatment?

Name FDA approved indication for dementia severity of each drug
• Aricept (Donepezil)– Mild, moderate, severe
• Razadyne (Galantamine)– Mild, moderate
• Exelon (Rivastigmine)– Mild, moderate
• Namenda (Memantine)– Moderate, severe
Combination Rx with cholinesterase inhibitor and
memantine
• Shown effective in mild to moderate AD
• Shown effective in moderate to severe AD
• Shown effective for all stages of AD
• Not any more effective than monotherapy for AD
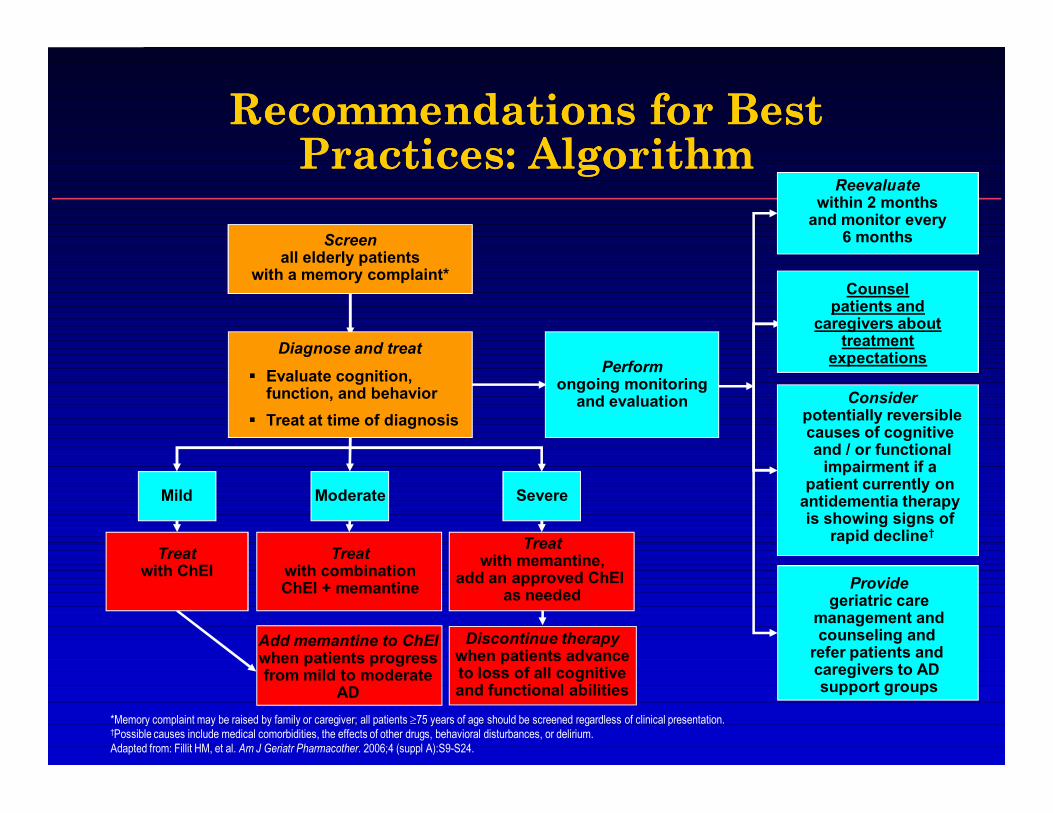
Recommendations for Best Recommendations for Best Practices: AlgorithmPractices: Algorithm
Screenall elderly patients
with a memory complaint*
*Memory complaint may be raised by family or caregiver; all patients ≥75 years of age should be screened regardless of clinical presentation.†Possible causes include medical comorbidities, the effects of other drugs, behavioral disturbances, or delirium.Adapted from: Fillit HM, et al. Am J Geriatr Pharmacother. 2006;4 (suppl A):S9-S24.
Performongoing monitoring
and evaluation
Reevaluatewithin 2 months
and monitor every6 months
Counselpatients and
caregivers about treatment
expectations
Considerpotentially reversiblecauses of cognitive and / or functional
impairment if a patient currently on
antidementia therapy is showing signs of
rapid decline†
Providegeriatric care
management andcounseling and
refer patients and caregivers to AD support groups
Diagnose and treat§ Evaluate cognition,
function, and behavior§ Treat at time of diagnosis
SevereModerate
Discontinue therapywhen patients advance to loss of all cognitive and functional abilities
Mild
Treatwith memantine,
add an approved ChEI as needed
Treatwith combinationChEI + memantine
Treatwith ChEI
Add memantine to ChEIwhen patients progressfrom mild to moderate
AD
Which drug is approved for treatment of Parkinson’s disease
related dementia?
• Donepezil
• Galantamine
• Rivastigmine
• Memantine

Which drug(s) shown effective in in clinical trials for the treatment of Dementia with Lewy bodiees?
• Rivastigmine
• Galantamine
• Donepezil
• Memantine

*P<.01 vs placebo; **P<.001 vs placebo†Responder definition recommended by NPI author (J Cummings)
Adapted from McKeith, et al, 2000.
Baseline
Impr
ovem
ent
NPI 10-Item Score
*
Mea
n C
hang
e fr
om B
asel
ine
–8
–7
–6
–5
–4
–3
–2
–1
0
RivastigminePlacebo
12 20Weeks Rivastigmine
3–12 mg/d (n=59)Placebo (n=61)
NPI 10-Item Score—Percentage of Patients Improving by ≥30% from Baseline
†
* *70
60
50
40
30
20
10
0
Patie
nts
Impr
ovin
g (%
)Week 20
Effects of Effects of RivastigmineRivastigmine on on BehavioralBehavioral Symptoms in DLBSymptoms in DLB

Clinical Trial: Donepezil for Dementia with Lewy Bodies
• 142 subjects, randomized, placebo controlled, 12 weeks
• Efficacy for – MMSE– Global function: CIBIC+– Behavior: NPI
• Delusions• Hallucinations• Fluctuating cognition
– Caregiver burden
Mori, E. et al. Ann Neurol: 72:41-52,2012
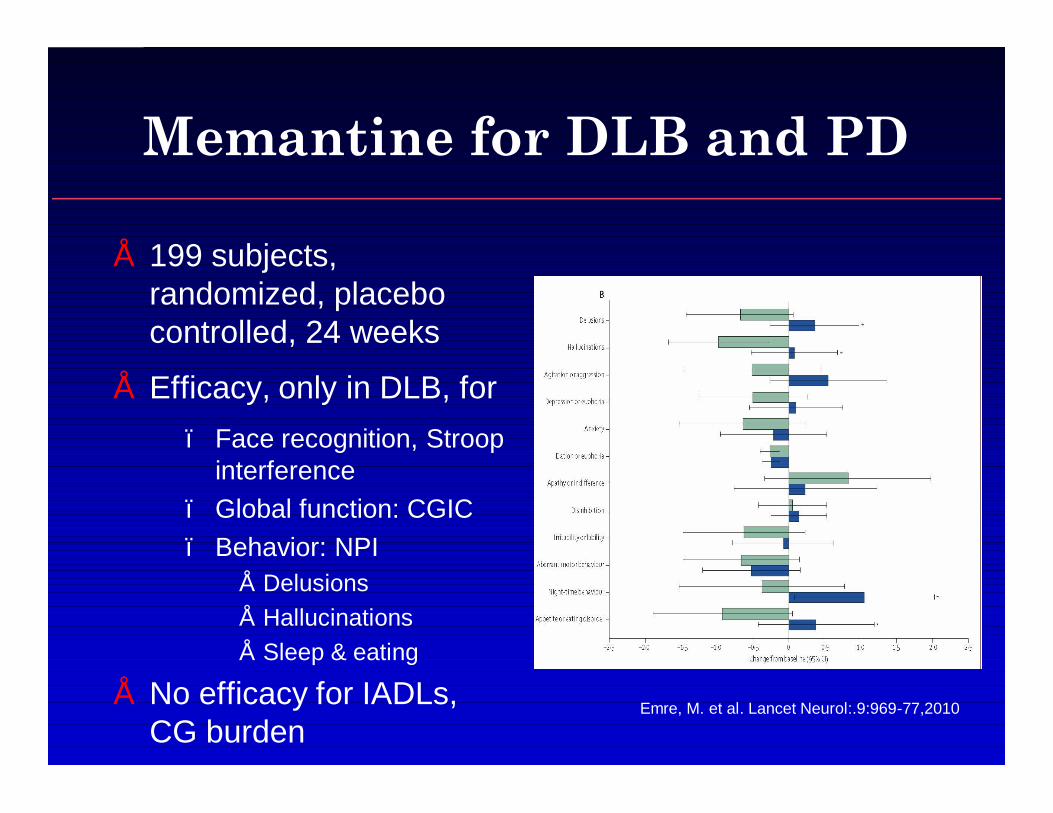
Memantine for DLB and PD
• 199 subjects, randomized, placebo controlled, 24 weeks
• Efficacy, only in DLB, for – Face recognition, Stroop
interference– Global function: CGIC– Behavior: NPI
• Delusions• Hallucinations• Sleep & eating
• No efficacy for IADLs, CG burden
Emre, M. et al. Lancet Neurol:.9:969-77,2010
What statement is true regarding treatment of mild cognitive
impairment?
• Cholinesterase inhibitors are effective in treating cognitive deficits of MCI
• Donepezil was shown to reduce progression to dementia over 3 years in ApoE-E4 positive subjects
• Vitamin E was shown to reduce progression to dementia over 3 years in ApoE-E4 positive subjects
• All of the above
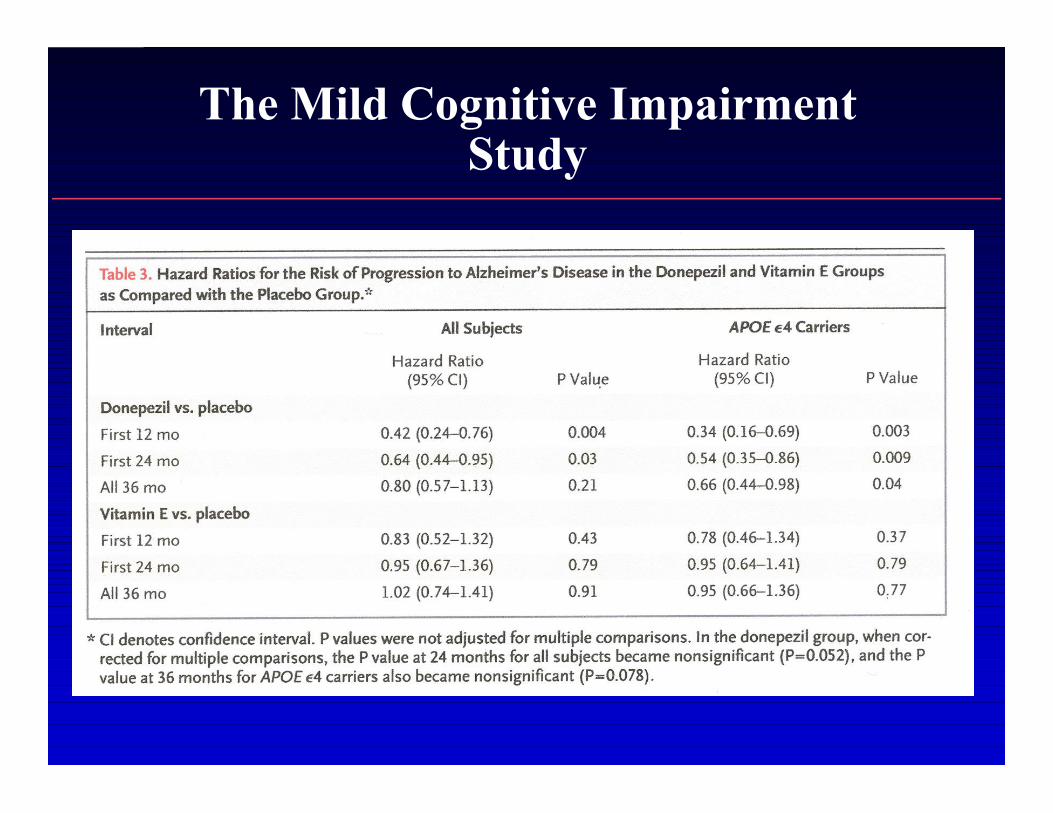
The Mild Cognitive Impairment Study
Medical food approved for treatment of AD?
• Medium chain triglyceride shake
• Folic acid
• Vitamin E in high dosage
• Gingko Biloba
• Omega 3 fatty acids

Axona®
• Medium chain triglycerides converted to ketones
• Alternative energy source for neurons not adequately utilizing glucose
– AD is “type 3 diabetes”
• Symptomatic benefit seen only in ApoE4- subjects in one 3-month trial
Black box warning re: mortality risk of antipsychotics in elderly
dementia patients
• Applies only to newer “atypical” drugs
• Applies only to older drugs
• Includes risk due to neuroleptic malignant syndrome
• Includes risk due to diabetes
• Includes risk due to cardiovascular problems, including sudden death

Black Box WarningConventional Antipsychotics: Chlorpromazine, Fluphenazine, Haloperidol, Loxapine,
Molindone, Perphenazine, Pimozide, Prochlorperazine, Thioridazine, Thiothixene, Trifluoperazine
Increased Mortality in Elderly Patients with Dementia Related Psychosis
–Elderly patients with dementia related psychosis treated with atypical antipsychotic drugs are at an increased risk of death compared to placebo. –Analyses of seventeen placebo controlled trials (modal duration of 10 weeks, largely in patients taking atypical antipyschotic drugs, revealed a risk of death in the drug treated patients of between 1.6 to 1.7 times that seen in placebo treated patients. Over the course of a typical 10-week controlled trial, the rate of death in drug treated patients was about 4.5% compared to a rate of about 2.6% in the placebo group. –Although the causes of death were varied, most of the deaths appeared to be either cardiovascular (e.g., heart failure, sudden death) or infectious (e.g., pneumonia) in nature. –Observational studies suggest that, similar to atypical antipsychotic drugs, treatment with conventional antipsychotic drugs may increase mortality. –The extent to which the findings of increased mortality in observational studies may be attributed to the antipsychotic drug as opposed to some characteristic(s) of the patients is not clear. –This drug is not approved for the treatment of patients with dementia-related psychosis (See WARNINGS in package insert).
Which antidepressant was shown possibly effective in treating FTD?
• Sertraline
• Citalopram
• Imipramine
• Venlafaxine
• Trazodone
DB, PC Randomized Trials DB, PC Randomized Trials in in bvFTDbvFTD
•• ParoxiteneParoxitene–– Potent SSRI with mild Potent SSRI with mild anticholinergicanticholinergic effectseffects–– DB, PCC, 40 mg, 6 weeksDB, PCC, 40 mg, 6 weeks
•• Worse cognition and no effect on behaviorWorse cognition and no effect on behavior•• Non significant trend toward increase in behavioral problems on NPINon significant trend toward increase in behavioral problems on NPI
•• TrazodoneTrazodone–– Weak serotonin agonist, adrenergic and histaminic blockerWeak serotonin agonist, adrenergic and histaminic blocker–– DB, PC, crossover trial, 26 patients, 300 mg dailyDB, PC, crossover trial, 26 patients, 300 mg daily
•• Significant decrease in NPI score, by >50%Significant decrease in NPI score, by >50%–– Improvement in irritability, agitation, depressive symptoms and eating Improvement in irritability, agitation, depressive symptoms and eating
disordersdisorders•• No adverse effect on MMSENo adverse effect on MMSE•• Half experienced fatigue, dizziness, hypotension or cold extremitiesHalf experienced fatigue, dizziness, hypotension or cold extremities
–1. Deakin JB. Psychopharmacol10:10,2003.–2. Lebert F. Dement Geriatr Cogn Disord. 2004;17(4):355-9.
Questions?