Embed Size (px)
Citation preview

Alzheimer disease
Developed by Dr. June Carroll, Ms. Shawna Morrison and Dr. Judith Allanson
Last updated April 2015

Disclaimer
• This presentation is for educational purposes only and should not be used as a substitute for clinical judgement. GEC-KO aims to aid the practicing clinician by providing informed opinions regarding genetic services that have been developed in a rigorous and evidence-based manner. Physicians must use their own clinical judgement in addition to published articles and the information presented herein. GEC-KO assumes no responsibility or liability resulting from the use of information contained herein.

Objectives• Following this session the learner will be able to:– Refer to their local genetics centre and/or order genetic
testing appropriately for Alzheimer disease (AD)– Discuss and address patient concerns regarding AD– Find high quality genomics educational resources
appropriate for primary care

Case 1
• Mary, 25yo female in good health
• Concerned about her risk of Alzheimer disease (AD) as her father’s condition is worsening quickly
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

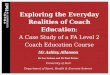
Case 2
• Mandy, 55yo female in good health
• Concerned about her risk of Alzheimer disease due to her father’s recent diagnosis
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 3
• Morgan, 55yo female in good health
• Concerned about her risk of Alzheimer disease due to her father’s recent diagnosis and family history
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W

What is Alzheimer disease?• Alzheimer disease (AD) is an adult-onset progressive
dementia that gradually reduces a person’s memory and ability to learn, reason, make judgments, communicate and carry out daily activities. Individuals may also experience changes in personality and behaviour
• General population lifetime risk of developing dementia is 10-12%
Sporadic, late onset, unknown cause
Late-onset familial AD (LOAD)has a mean age of onset of >60-65years (15-25%)
Early-onset familial AD (EOAD) hasa mean age of onset < 60-65 years(<2%)

• Early-onset AD (EOAD) has an autosomal dominant inheritance pattern
• Three genes have been associated with EOAD:– amyloid precursor protein (APP)– presenilin 1 (PSEN1)– presenilin 2 (PSEN2)
• Each of these genes is involved in production of the amyloid ß (Aß) peptide, a major component of amyloid plaques
What do I need to know about the genetics of Alzheimer disease?

What do I need to know about the genetics of Alzheimer disease?
• Late-onset familial AD (LOAD) has been associated with apolipoprotein E (APOE)
• APOE is considered a risk modifier, especially APOE 4
• Approximately 1% of the general population are APOE 4 homozygotes (carry two copies of 4)
• Approximately 42% of persons with AD do NOT have an APOE 4 allele
• APOE 4 is neither necessary nor sufficient to cause LOAD

What do I need to know about the genetics of Alzheimer disease?
• Alzheimer disease (AD) develops due to a complex interaction between genetic and environmental factors
• With one affected first-degree relative, the risk of Alzheimer disease is approximately 20-25% (approximately double the population risk)

Who should be offered referral for genetic consultation?
Consider a genetics consult for:Patients with Alzheimer disease (AD) with onset <60-
65 yearsPatients with late-onset AD and multiple affected
close relativesClose relatives of the above two types of patientsA member of a family in which there is an identified
mutation in the APP, PSEN1 or PSEN2 genes

Who will be offered genetic testing and what do the test results mean?
• Genetic testing for Alzheimer disease (AD) is only available for a small number of families with early-onset AD (EOAD)– Testing likely to be initiated in a living affected
relative• If a gene mutation is found, other family members
are eligible for testing focused on the identified family mutation– Inheriting a mutation in APP, PSEN1 or PSEN2
gene causes early-onset Alzheimer disease (EOAD)

• Clinical testing is currently not available for late-onset AD (LOAD) or sporadic cases
• When there are multiple related affected individuals, research testing may be available
• APOE 4 testing is not recommended for risk assessment because of low sensitivity and specificity
• APOE 4 is neither necessary nor sufficient for the disease
Who will be offered genetic testing and what do the test results mean?

How will genetic testing help you and your patient?
• In the case of genetic testing for early-onset Alzheimer disease (EOAD), – A positive test result for a known family gene mutation
can result in:• Relief from uncertainty• An increased feeling of control• Opportunity to plan life decisions
– A negative test result for a known family gene mutation can result in:• Relief from fear of developing EOAD• Knowledge that children are not at risk for EOAD

Are there harms or limitations of genetic testing?
• Currently no cure or effective preventive therapy is available if a gene mutation is found
• In the case of genetic testing for early-onset Alzheimer disease (EOAD), – A positive test result for a known family gene mutation
can result in:• Adverse psychological reaction, family issues/distress• Insurance/job discrimination, confidentiality issues
– A negative test result for a known family gene mutation can result in survivor guilt

Case 1
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

Case 1
• Family history is suggestive of early-onset AD (EOAD – dx<60-65y) and dominant inheritance pattern
• Offer referral for genetics consultation with option of genetic testing
ADdx 55
d.85
ADdx53
AD dx 61
25
d.65
ADdx 57
63 58 5560d.68
A&W A&W
A&W
Stroke

Case 2
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 2
• Family history is suggestive of sporadic AD
• Mandy’s AD risk is about 20-25% because of an affected FDR
• No referral to genetics indicated
MI
ADdx 80
88 8690 75
55
80
d.87d.85
arthritis IDDM
A&W

Case 3
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W

Case 3
• Family history suggestive of late-onset AD (LOAD)
• Referral to genetics can be considered for counselling and personal risk estimation
• No genetic testing is available but participation in research may be possible
ADdx78
ADdx 80
d.88 8690 75
55
80
d.87d.85
AD dx83
IDDM
A&W

Pearls
•Informative genetic testing is currently available to only a small number of families with early-onset (<60-65 years of age) Alzheimer disease (EOAD)
•Genetic testing is not possible for most cases of AD
•Apolipoprotein E gene variations alone cannot be used to predict risk of developing AD

References• Alonso Vilatela ME et al., Genetics of Alzheimer’s disease. Arch Med Res.
2012; 43(8): 622-31 and Goldman JS et al., Genetic counseling and testing for Alzheimer disease: Joint practice guidelines of the American College of Medical Genetics and the National Society of Genetic Counselors. Genet Med 2011; 13(6): 597-605
• American College of Medical Genetics/American Society of Human Genetics Working Group on APOE and Alzheimer's disease (1995) Statement on use of apolipoprotein E testing for Alzheimer's disease. JAMA 1995; 274(20): 1627-1629
• Bird TD. Alzheimer Disease Overview. 1998 Oct 23 [Updated 2014 Jan 30]. In: Pagon RA, Adam MP, Bird TD, et al., editors. GeneReviews™ [Internet]. Seattle (WA): University of Washington, Seattle; 1993-2014. Available from: http://www.ncbi.nlm.nih.gov/books/NBK1161/
• Genetics Education Project