Embed Size (px)
Citation preview

nature reviews | neurology volume 5 | auGust 2009 | 411
news & views
AlZHeIMer DISeASe
Alzheimer disease neuropathology in the oldest oldJillian J. Kril
As the human lifespan increases, the number of people living beyond their nineties is rising rapidly. This changing population demographic will have an effect on many aspects of health and society, including the number of people living with dementia. To accurately diagnose dementia, we must understand the relationship between the observed neuropathology and age.
the pathological hallmarks of alzheimer disease (aD), neurofibrillary tangles (nFts) and neuritic plaques (nPs), are found with increasing frequency in advancing age (Figure 1).1 these findings, together with the sharp rise in the prevalence of demen-tia with age, have led to the prevailing view that the accumulation of aD-type pathol-ogy parallels the emergence of dementia. a burgeoning body of literature, however, sug-gests that the association between aD-type pathology and dementia does not hold in the oldest old (≥95 years of age), question-ing many of our assumptions about the pathophysiology of aD and our ability to accurately make a diagnosis of aD at post-mortem. a study by savva, wharton and colleagues,2 investigating the effect of age on the relationship between aD-type pathol-ogy and dementia, has provided evidence that the precision with which nFt and nP densities predict dementia decreases with increasing age among individuals >70 years of age.
the current pathological criteria for the assessment of aD pathology evaluate the distribution and density of nFts and nPs to yield a probability statement with respect to dementia.3 these criteria require a greater density of nPs for a diagnosis of aD in older patients (>75 years of age) than in younger individuals (50–75 years of age); however, the criteria do consider that aD-type pathology might not correlate uni-formly with dementia in patients aged over 75 years. the report by savva, wharton and colleagues2 drew on a population-based sample of the elderly (aged 69–103 years), which included both community-dwelling and institution-dwelling patients. the researchers conducted neuro pathological examinat ions on the brains of 426 in dividuals for whom the dementia status
was known from assessments conducted, on average, 1.5 years before death. the density of aD-type pathology (nFts and nPs) and the severity of other patholo-gies (atrophy, lewy body density and cerebro vascular disease) were scored in the cerebral cortex and hippocampus of these brains. Data were then divided into five age groups for analysis (≤80, 80–84, 85–89, 90–94 and ≥95 years of age). the researchers found that the prevalence of moderate or severe aD-type pathology pro-gressively increased with age in both brain regions of individuals without dementia. By contrast, in the brains from people with dementia, the prevalence of such pathol-ogy remained constant or decreased with increasing age. the findings from the study indicated that in the younger old (<80 years of age) the presence of moderate or severe aD-type pathology was strongly associ-ated with dementia, but the strength of the associations progressively declined with age and was at its weakest in the oldest old (≥95 years of age).
the overlap in prevalence of moderate or severe pathology in patients with and without dementia has obvious implications for the usefulness of the current patho-logical criteria for the diagnosis of aD. the attenuation of the relationship between aD-type pathology and dementia in the oldest old will result in errors in diagnosis and have consequences for many aspects of health care, such as health resource and care management planning, as well as influenc-ing our understanding of the biology of aD. the growing number of people living to their tenth or eleventh decade will provide the opportunity to refine these criteria, by taking into account the variable relation-ships between pathology and cognitive function across the lifespan.
the study by savva, wharton and col-leagues also highlights the importance of neuronal loss over the accumulation of abnormal protein deposits, such as nFts or nPs, in causing cognitive impairment and dementia. in most brain regions that have been examined, including the hippo-campus,4 atrophy has been found to be an accurate indicator of neuron number that was independent of diagnosis. savva, wharton, et al. found that moderate or severe atrophy in either the cortex or the hippocampus correlated with dementia across all age groups.2 this finding is sup-ported by in vivo5,6 and postmortem7 mri studies, which confirm the value of medial
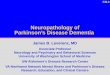
Figure 1 | Alzheimer disease pathology in the hippocampus of an elderly individual. The observed neuritic plaque (red arrowhead) and neurofibrillary tangles (black arrows) were revealed by modified Bielschowsky silver stain.
nrneurol_N&V_AUG09.indd 411 21/7/09 14:50:22
© 2009 Macmillan Publishers Limited. All rights reserved

412 | AUGUST 2009 | volUme 5 www.nature.com/nrneurol
news & views
temporal lobe volume, and atrophy over time, in predicting dementia. Hippocampal and cortical atrophy, however, are not spe-cific to aD and cannot be used to reliably identify patients with this disease, although measuring such atrophy is a useful adjunct to the clinical diagnosis, and consideration should be given to incorporating measures of neuron loss into pathological criteria.
why the relationship between aD-type pathology and dementia fails in the oldest old is unclear. one possibility is that in older individuals the importance of aD-type pathology in the causation of dementia is overshadowed by the coexistence of other pathologies, notably cerebro vascular disease. the prevalence of dual or multiple patholo-gies increases with age, and the cumulative effects of aD-type pathology and cerebro-vascular disease on cognitive function have been demonstrated in a number of studies.8,9 this premise, however, is not borne out in the data of savva, wharton and colleagues, who found that cerebrovascular pathologies, such as small-vessel disease and/or infarcts, were more strongly associated with dementia in the younger old. Further studies are urgently needed to more clearly define the relation-ship between cerebro vascular pathology and dementia in the elderly, and, more impor-tantly, to establish validated and operational-ized criteria for the pathological assessment of vascular pathology.
the study by savva, wharton, et al. con-tributes to the growing body of literature that exists showing marked differences in the pathology of dementia, in particular aD, between people under and over the age of 75 years. the research highlights the need to modify current diagnostic prac-tice to account for the age-dependent vari-ability in pathology and provides support for broadening the diagnostic criteria to include measures of neuron loss.
Disciplines of Medicine and Pathology, The University of Sydney, Sydney, Australia.
Correspondence: Discipline of Pathology, DO6, The University of Sydney, Sydney 2006, Australia [email protected]
doi:10.1038/nrneurol.2009.105
Competing interestsThe author declares no competing interests.
1. Braak, H. & Braak, e. Frequency of stages of Alzheimer-related lesions in different age categories. Neurobiol. Aging 18, 351–357 (1997).
2. savva, G. M. et al. Age, neuropathology, and dementia. N. Engl. J. Med. 360, 2302–2309 (2009).
3. [no authors listed] national institute on Aging and Reagan institute working Group on diagnostic criteria for the neuropathological diagnosis of Alzheimer’s disease. Consensus recommendations for the postmortem diagnosis of Alzheimer’s disease. Neurobiol. Aging 18 (Suppl. 4), s1–s2 (1997).
4. Kril, J. J., Hodges, J. R. & Halliday, G. M. Relationship between hippocampal volume and CA1 neuron loss in brains of humans with and without Alzheimer’s disease. Neurosci. Lett. 361, 9–12 (2004).
5. Henneman, w. J. et al. Hippocampal atrophy rates in Alzheimer disease: added value over
whole brain volume measures. Neurology 72, 999–1007 (2009).
6. Morra, J. H. et al. Automated mapping of hippocampal atrophy in 1-year repeat MRi data from 490 subjects with Alzheimer’s disease, mild cognitive impairment, and elderly controls. Neuroimage 45 (Suppl. 1), s3–s15 (2009).
7. Barkhof, F. et al. The significance of medial temporal lobe atrophy: a postmortem MRi study in the very old. Neurology 69, 1521–1527 (2007).
8. nagy, Z. et al. The effects of additional pathology on the cognitive deficit in Alzheimer disease. J. Neuropathol. Exp. Neurol. 56, 165–170 (1997).
9. snowdon, D. A. et al. Brain infarction and the clinical expression of Alzheimer’s disease. The nun study. JAMA 277, 813–817 (1997).
CereBrAl AneurySMS
To clip or to coil? That is no longer the questionE. Sander Connolly Jr and Philip M. Meyers
The relative merits of clipping and endovascular coiling to treat ruptured intracranial aneurysms are the subject of an ongoing debate. The latest results from the International Subarachnoid Aneurysm Trial offer reassurance regarding the long-term outcomes of coiling and provide support for an individualized approach.
since the initial development of detachable platinum coils for the treatment of cerebral aneurysms in the early 1990s, investi gators have been attempting to iden-tify the most appropriate candidates for treatment with this technology, as opposed to the alterna-tive approach, micro-surgical clipping. the results of a long-term follow-up study con-ducted as part of the international subarachnoid aneurysm trial (isat) should help to clarify what factors need to be taken into account when selecting an appropriate treatment for a given individual.1
isat, which recruited 2,143 patients between 1994 and 2002, has been the most ambitious effort to date to compare clip-ping and coiling. Patients with ruptured brain aneurysms that caused sub arachnoid hemor rhage were randomly assigned to either clipping or coiling treatment if the cerebrovascular surgeon and the
en dovascular surgeon agreed that the aneu-rysm could potentially be treated by either
te chnique.2 early results in this select subgroup, who tended to present in good clinical condi-tion with small ante-rior circula tion lesions, suggested a benefit for coiling, with only 24% of indivi duals being depen-dent or having died 1 year after coiling, compared with 31% after clipping
(P = 0.0001). the risk of epilepsy was also lower in patients allocated to endo vascular treatment, but middle cerebral artery aneurysms in elderly patients (>65 years) seemed to respond better to treatment with clipping, and the risk of rebleeding was also lower following clipping.2,3 in addi-tion, re-treatment of the index aneurysm was neces sary in 17% of those that were initially coiled compared with only 4% of those that were clipped. re-treatment was particularly common in young patients, those with larger aneurysms, those with
…the question is no longer ‘to clip or to coil?’ but, rather, ‘who to clip and who to coil?’
nrneurol_N&V_AUG09.indd 412 21/7/09 14:50:23
© 2009 Macmillan Publishers Limited. All rights reserved