Embed Size (px)
Citation preview

Alvin D. Dubin, DO Legacy LectureAOCOO‐HNS 100th Annual Clinical Assembly‐May 5, 2016The Phoenician Scottsdale Arizona
The Changing Face of Medicine –Population Health Management
Fixing Health Care’s Broken System
Richard F. Multack DO, FOCOO, MBA



Welcome to “The “Burning Platform” of Physician Autonomy


Dispelling FantasyWho is the real villain here?

Many of you are thinkingNot my circus !
DenialAnger
Not my Monkeys !

BargainingDepressionAcceptance

Please don’t worry
9

Still‐ we are not going to be practicing our old fashioned brand of medicine anymore

The Way We Were

Entitlement Programs
• Social Security Act 1935‐Monthly benefits started 1940• Average life expectancy
• Male 59.9• Female 63.9
• Medicare and Medicaid ‐1965• Average life expectancy 69.5
• Male 66.8• Female 73.71
• 1965: 8% Medicaid Enrollment –Today >20%
• Average life expectancy today – 79.0• 10,000+ “Baby Boomers” join Medicare every day

The Process was clearly brokenThings were just not aligned


How did we get here?•1. Unsustainable growth of health cost

2. Growing lack of access to healthcare
Is the Physician Shortage a Demand-Capacity
Mismatch? .

3. Disparities in careVariation in the cost, quality, and intensity of clinical services remains a challenge for health system performance in the United States.

Who’s driving up U.S. healthcare costs? “cowboy doctors”—physicians who provide intensive, unnecessary, and often ineffective patient care, resulting in wasteful spending of hundreds of billions of dollars annually.

We were Confused

We lacked direction

Sometimes… you need to pick a different road

“The best way to deal with the future is to create it”
Abraham Lincoln

What have we done?• 1. HITECH ACT (American Recovery and Reinvestment Act of 2009)
• 2. Patient Protection and Affordable Care Act of 2010• Pay 4 Performance• Patient Centered Medical Home• Payment Bundling• Shared Savings / ACO• Value Based Purchasing• Hospital penalty for Readmissions, and other quality issues such as HACs

PQRS• Tax Relief and Health Care Act of 2006•Medicare Improvement for Patient and Providers Act of 2008
• Created PQRS• Bonus 1.5 % for successful participation• Penalties begin in 2015 based on 2013 data
• 1.5% decrease all Medicare reimbursement for not reporting• Escalates to 2% in 2016 based on 2014 data

Further Government Programs and Policies
• Hospital Acquired Conditions Policy of 2008
• Value‐ Based Purchasing and Readmissions Program of 2012
• Improving Medicare Post‐Acute Care Transformation Act 2014
• 2015 Physician Value‐Based Payment Modifier Policies• The Affordable Care Act mandates that by 2017, CMS adjust provider payments based on cost and quality through the VBM modifier. tied to the Physician Quality Reporting System,. All physicians’ performance in 2015 will impact their payment in 2017.
• However, successful participation in PQRS in 2015 will exempt solo practitioners and physician practices with fewer than 10 providers, from any negative payment adjustments.
• Failure to participate in PQRS in 2015 will result in a “double whammy,” including a 2 percent penalty from the PQRS program in addition to a 4% penalty from the VBM program, for a total penalty of up to 6 percent for practices with 10 or more providers

Before we go any further I want to be absolutely sure I am communicating the correct message

Reimbursement Model Shift
1%
12%
32%
55%
0.30%2014
• Payers demanding value (high quality, low cost) by incorporating either capitation or quality indicators in contracts
• Providers shifting focus from maximizing patient volume toward balancing volumes with cost and quality performance

Medicare Physician PaymentMACRA
• Medicare Access and CHIP Reauthorization Act of 2015• Replaces the “dreaded” Sustainable Growth Rate
• Halted elimination of 10 and 90 –day global procedure payments in 2017 and 2018• CMS was authorized to request actual post op data and to punish physicianswho do not provide requested datawith a penalty as high as 5 percent. The law mandated the review and revisions be finalized by 2019.
• Beginning in 2019 establishes two payment tracks for physicians
• Those in Alternative Payment Models (APM)
• All others in MERIT‐BASED INCENTIVE PAYMENT SYSTEMS (MIPS)

Comprehensive Payment Model• Payment Change is necessary and it must include a Cultural change• Must shift more payment to primary care. (5% to 10%)• Critical to risk adjust primary care payment‐ You get paid more not for doing more but for sicker patients
• Need to change how providers are paid• Risk‐Adjusted Fixed Fee per Patient , possibly modified by;
• Experience• Quality• Utilization targets• Shared savings• (Number of Patients) X (Established Rate) = Expected Reimbursement• No codes or explanation of benefits or prior approval
• Pay a simple fair salary• Not productivity driven• Need intrinsically motivated doctors who want to work
• Needs to be implemented “Cold Turkey”

MACRA Reform: APM TrackAlternative Payment Model (APM) Track• 5% annual lump sum bonus payment
from 2019 to 2024 and earn any shared savings/capitation surplus
• Must participate in an APM that meets the following criteria‒ Bears financial risk‒ Authorized quality measures‒ Meaningful Use ‒ OR participate in a Patient Centered
Medical Home• Risk allocation timeline
‒ 2019: At least 25% of a provider’s payments must come from services provided under an APM model
‒ 2021-2022: 50%‒ 2023 and After: 75%

Merit‐Based Incentive Payment System (MIPS)
• Sunsets existing payment programs: PQRS, VBM, EHR Meaningful Use
• CMS will incorporate these measures and develop methodology for assessing performance
• Physician performance will determine annual payment adjustor

MIPS
• There will be a Composite Threshold Performance Scale (0‐100)• The system will award bonuses and impose penalties based on whether physicians score above or below a certain threshold on quality measures, including meeting the requirements for the meaningful use of health IT.
• Reimbursement will actually be based on;• Four (4) performance categories
• 25Pts MU of CHERT• 15Pts Clinical Practice Improvement• 30Pts VBM‐measured quality• 10Pts VBM‐measured resource use
• First Performance Measure Year ‐2017• First likely payment adjustments 2019

CPICredit will be available for participating in an established quality improvement program (such as through a hospital or medical group) that meets ABPMR standards.


MIPS
•Physician Composite Core• Mean or median scores of all clinicians subject to MIPS• Zero Sum Process
• Bonus is paid from penalties• Bonus capped
• 4% 2019• 5% 2020• 7% 2021• 9% 2022
• In 2018‐2023 $500 million per year will be paid out to exceptionally performing physicians

How will the Centers for Medicare & Medicaid Services (CMS) determine physician scores under MIPS, which requires a zero to 100 composite score?

MACRA Reform: Physician Choice
MIPSUp to 9%
Adjustment Factor based upon performance
Top performers may get
additional bonus
After 2026: 0.25% annual
payment update
APMLump sum
quality bonus
Shared savings or capitation
surplus
After 2026: 0.75% annual
payment update
Financial Comparisons
Physicians have greater revenue opportunity under the APM track, but must be able to demonstrate they meet criteria of bearing significant risk
Participation in CI program prepares providers to succeed in new Medicare payment and value‐based care

What about Sequestration???

The federal budget sequestration cuts impacting Medicare claims went into effect on April 1, 2013 any Medicare service or procedure performed on or after this date is subject to a two percent (2%)reduction in payment. This also includes Medicare Fee For Service (FFS) program,

MIPS
•Current Reimbursement is in a holding pattern • Annualized payment rates will be increased by 0.05% from 2014‐2018‐ Based on a fee that was decreased 2% by Sequestration
• The current 3 incentive programs will end in 2017• Includes 3% penalty for not meeting meaningful use criteria
• Includes 2% penalty for not reporting data to PQRS

MIPS Payment Adjustment Percentages

Bundled Payment
• The bundled payment rationale establishes one all inclusive price, focusing on a patients total episode of care.
• The payment combines all of a patient’s services from the date of admission to a set number of days (usually 30‐120) after discharge from that hospital.

External Pressure on PhysiciansMD and Hospital Quality Reports
Care Coordination
Team Medical Necessity
Value Base
Purchasing
PSIs
Core Measures
ComplianceFraud Abuse
RAC
2 MIDNIGHTRULE
E&M Pro feesDenial related
claims
ICD-9-CMICD-10
POAHACs
PreventableReadmission
Complications

On top of all that then they gave us ICD‐10

I know you all feel like someone else is pulling the strings… and they are

We were complacent‐We did not realize the dangers awaitng us


$661 M community benefit
M community

Key Market Dynamics•Provider consolidation•Dominant health plans•Narrow networks emerging
•Revenue - utilization and price
•Cost pressures•

How about “BIG PHARMA” • “There’s sort of this mad rush,” one investor says of the $221 billion surge in pharmaceutical deals in the first half of this year.
• Teva Pharmaceutical Industries said it would buy Allergan’s generics business for $40.5 billion and drop its hostile bid for Mylan, while Allergan said it would buy biopharma firm Naurex for $560 million.
• Pharma companies believe acquisitions are the only way to keep their revenues growing as fast as investors expect
• It’s often cheaper for a company to acquire the next blockbuster drug than to develop it in‐house.
•Huge increase in cost of generic medication

Population Health Management


What is it?
• Population Health management is defined as, controlling the health outcomes of a group of individuals.
• This includes,• Public health intervention• Social environment• Aspects of the physical environment• Genetics• Behavioral Health

Changing Business ModelProviders traditionally generate revenue by:
• Maximizing rates• Maximizing volumes (churning)
• Which is changing to a new model• Taking financial risk for managing the
health of a population, lowering costs and serve a greater number of unique patients

Strong Alignment• Values• Top decile safety and quality• Strong brands • Highly integrated• Large employed medical groups • Strong management and governance • Excellent teaching and research • Double A ratings

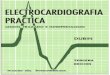
Managed Care Community Network• Provides or arranges primary, secondary and tertiary
managed health care services under contract with the Department of Healthcare and Family Services exclusively to Medicaid clients
• Full-risk health plan responsible for the total cost of care and quality
• Requires a comprehensive provider network (i.e. PCPs, Home Health, SNFs, chiropractic, Dental, Behavioral Health, Waiver Providers, additional Pediatric Specialists, Pharmacies) to meet network adequacy
56

Skilled Nursing Facility
Hospital -Outpatient
Urgent Care Ctr
Retail Clinic
Employer Clinic
• Day Surgeries• Emergency• Clinic visits• Observation• Hospital‐Based ancillary services
OutpatientAmbulatory
Free-standing Diagnosis Center
End Stage Renal Disease
OP Facility/ Comprehensive OP Rehab Fac.
HospitalPre Hospital Post Acute Care
Home Hospice
Indian Health Services
Community Mental Health Clinic
Inpatient
Hospital –Inpatient
Psych
Inpatient Rehab
Home Healthcare
Home Health Agency
Physician Practices Ambulatory
Surgery Ctr
Fed Qualified HC
Critical Access Hospital
Outpatient
Rural Health Clinic
Hospice
Critical Access Hospital Inpatient
Population at Risk
The Continuum of Care
PhysicianOfficeClinic
Physician Evaluation and Management

Changing Paradigms….From TO ...Silo care management Enterprise care managementEpisodes of care Coordination of careDischarges Transitions
Caring for the sick Keeping people wellProduction (volume) Performance (value)Acute Care Management
Population Health Management
Utilization Of Resources Right care, right place, right time
4

ECM Inpatient CM
ECMOutpatient CM
Post‐Acute‐Post acute SNF Network/Model‐Transition coaches‐Advocate At Home‐Palliative Care
Primary Care Access‐Primary Care Access, Team Model of Care
Strong Relationship and Communication
ECMOutpatient CM
Care Management Supports the Patient Continuum…

Methodology
•EMR‐ Provides Data•Statisticians‐ Analyze Data•Measuring outcomes‐ Provides Direction•Team based intervention‐Provide Efficiency•Patient engagement‐Makes Patients Responsible

Reimbursement Today

2020 Outlook

From Fill the Hospital to Empty the Hospital

POPULATION MANAGEMENT

So how are we going to actually manage the population?• Access
• 24/7 Access to office or ambulatory acute care setting• Same day appointments
• Management• Medical Home• Narrow networks• Integrated care – keep it in the system
• Clinical Effectiveness‐carve out waste• Decreasing unnecessary pre‐op testing• Stopping unnecessary and obsolete lab testing• Stopping unnecessary imaging and procedures• Appropriate use of blood transfusions• Standardization of equipment and procedures such as total hips leveraging economies of scale for better vendor pricing

So how are we going to actually manage the population?
• Extensive social support• Care management• Social work• Integrated home health• Integrated PAN network• Behavioral health• Patient family engagement

High-spending doctors less likely to be suedReuters HealthProviding more care than necessary may workto lower a doctor's risk of being accused of malpractice, suggests a new U.S. study. The researchers found thatdoctors in Florida who provided the most costly carebetween 2000 and 2009 were alsoleast likely to be sued between 2001 and 2010.

One percent of U.S. docsresponsible for a third of malpractice paymentsReutersJust one out of every 100 U.S. doctors is responsible for 32 percent of the malpractice claims that result in payments to patients,

SummaryConclusions
Better life stylePreventive careAppropriate careIntegrated careHome CareSkilled nursing careAppropriate end of life care

Top 10 Challenges Facing Physicians in 2016
• Preparing for the Merit Based Incentive Payment System and P4P• Independent practice versus employment• Consolidation of major healthcare payers• Meaningful use Stage 2 / Stage 3• The battle over maintenance of certification• Overcoming barriers to team – based care• Wondering if the Affordable Care Act will survive a Presidential Election or another recession
• Preventing data breaches• Challenges of Chronic Care• Remote Medicine

I want to leave you with some happy thoughts

The “train” of change has left the station there is no turning back‐Please jump on board
Because……clearly great things lie ahead

When it comes to Population Health Management, Documentation and Physician ReimbursementDon’t do things half way

Remember,You will always have a supportive friend at Advocate Health Care

References• Advocate Health Care, MPAK‐ “ Health Care’s Perfect Storm’ Leadership Development Institute Quarter 1 2015
• Advocate Health Care, Physician Leadership Development Day 2015, June 19, 2015, “Strategies to Whether The Storm” , Lee Sack, MD CMO Advocate Health Care
• “The Changing Face of Medicine‐“What’s In It For Me” Richard F. Multack, DO, VPMM, ASSH (2013)
• “The Changing Face of Medicine‐2014 and Beyond” Richard F. Multack, DO, VPMM ASSH (2014)
• Kindig D, Stoddart G. What is population health? (http://www.ajph.org/cgi/reprint/93/3/380.pdf) American Journal of Public Health 2003 Mar;93(3):380‐3 Retrieved 2015‐5‐7
• Howe, Rufus, and Christopher Spence. Population health management: Healthways’ Pop Works (http://www.healthways.com/assets/0/98/E4CDDEDB‐5004‐4E74‐A5C9‐E1973F5ABC05.pdf). HCT Project 2004‐07‐17, volume 2, chapter 5, pages 291‐297. Retrieved 2015‐5‐7
• Coughlin JF, Pope J, Leedle BR. Old age, new technology, and future innovations in disease management and home health care (http://web.mit.edu/agelab/news_events/pdfs/home.health.care.pdf) Home Health Care Management & Practice 2006 Apr; 18 (3):196‐207. Retrieved 2015‐5‐7
• DMAA: The Care Continuum Alliance. Publications. Population Health management (http://www.dmaa.org/pubs_dm_journal.asp) Retrieved 2015‐5‐7
• Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ (May 27, 2006) “Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data” (http://www.fic.nih.gov/news/fogarty/2006/depp_lancet_367.pdf) (PDF). The Lancet 367 (9524): 1747‐1757. Doi:10.1016/SO140‐6736(06)68770‐9
• (http://dx.doi.org/10.1016%2FS0140‐6736%2806%2968770‐9). PMID 167321270 (http://www.ncbi.nlm.nih.gov/pubmed/16731270).
• Congressional Budget Office, May 2013” Estimates of the Effects of the Affordable Care Act on Health Insurance Coverage
• CDC/NCHS “ National Ambulatory Medical Care Survey 20009‐2010 Primary Care Shortages could be Eliminated Through Use of Teams, Nonphysicians and Electronic Communication‐ Health Affairs 32 1 Jan 2013
• Michael E. Porter and Thomas H. Lee, “The Strategy That Will Fix Health Care,” HBR October 2013
• Kaiser Family Foundation, “2012 Employer Health Benefits Survey”
• Chicago Tribune‐2015‐”how health care will look with a physician shortage”
• The New Yorker‐ 2015‐”Why is the US perpetually short of nurses”
• The New York Times ‐2015‐”Who’s driving up US healthcare costs”
• HITEC ACT‐ American Recovery and Reinvestment Act of 2009
• Patient Protection Act and Affordable Care Act of 2010

References continued• Chicago Tribune‐2015‐”how health care will look with a physician shortage”
• The New Yorker‐ 2015‐”Why is the US perpetually short of nurses”
• The New York Times ‐2015‐”Who’s driving up US healthcare costs”
• HITEC ACT‐ American Recovery and Reinvestment Act of 2009
• Patient Protection Act and Affordable Care Act of 2010
• Tax Relief and Health Care Act of 2006
• Medicare Improvement for Patient Providers Act of 2008
• The Far side Cartoon 1985
• Medicare Access and CHIP reauthorization Act of 2015
• Physician News‐ “Medicaid vies for Attention in Physician Payment Reform 2015
• Balanced Budget and Emergency Deficit Control Act of 1985
• Budget Control Act of 2011
• The Hill‐ 2015‐ “Clinton has ‘serious concerns’ about health insurance mergers”
• Crain Chicago Business‐”Advocate Health Care and Aetna team up to offer plan on Illinois Exchange”
• Survey‐ “Physician Leaders Strongly Support Value Based Care”
• Kaiser Health News
• Reuters Health‐ “High Spending Doctors Less Likely to be sued
• BJM‐2014‐ “Defensive Medicine Works”‐ http://bit.ly//pbpZ2w
• Advocate Strategic Operations Meeting/ Margin Management December 2015

References continued
• http://go.cms.gov/ijkyhoF
• https://www.cms.gov/Medicare/Quality‐Initiatives‐Patient‐Assessment‐Instruments/Value‐Based‐Programs/MACRA‐MIPS‐and‐APMs/MACRA‐MIPS‐and‐APMs.html
• HR2‐Medicare Access and CHIP Reauthorization Act of 2015> http://www.govtrack.us/congress/bill/114/hr2
• Congressional Research Services Review of HR2 > https://www.fas.org/sgp/crs/misc/R43962.pdf


Is the ACA working? Advocate Strategic Operations / Margin Management Meeting December 2015

Health Care Costs Increasing…

U.S. Health Spending Tops $3 TrillionFox NewsSo much for controlling medical costs. According to the Department of Health and Human Services report on trends in spending that was recently published in Health Affairs, health‐related spending in the U.S. topped the $3 trillion mark in 2014. This equates to $9,500 for every man, woman and child in America. To put the spending into further perspective, total government spending in 2014 was $3.5 trillion.

There Has Been Little Reform of Health Care�Health care delivery has not structurally changed and won’t until incentives change�Pharma utilization/costs ballooning�The industry is fragmented and is inefficient relative to other industries�We have stunning levels of over capacity –beds, imaging equipment, surgery suites, lab svcs, etc.�Health care pricing remains an enigma

Top Ten List for Survival of a Transformative Event1.Size is critical and consolidation synergies a must2.Pursue ruthless standardization3.Fly full airplanes4.Measure and improve productivity at every level5.Aggressively protect and leverage intellectual capital

Top Ten List for Survival of a Transformative Event6. Develop robust analytic platform7. Unlock waste in clinical process8. Own or partner with every part of patient continuum9. Own (not partner) with primary care funnel and enlarge it through acquisition, growth and capacity10.Build the organization around the principle that you are in the relationship business


Role of APP:
What is APP classified as in regard to the APM issues and will APP be submitting the data needed for the member physicians ?ANSWER: APP is not currently eligible to enter into an alternative payment model in 2016. We are evaluating our options for participating in an APM for 2017.
Since Continuous Process Improvement is one of the 4 categories that will determine the score for MIPS, Does participation in APP registries cover this base?ANSWER: No, a third‐party has to prepare the quality data in a different registry for CMS.
What is the role of specialist members of APP in regard to meeting the CMS data needs?ANSWER: A key issue may be that specialists outside of AMG and
Dreyer are not officially in our MSSP ACO (we don’t submit their TINs) so I’m not sure if they get credit for being in an alternative payment model through APP membership.To avoid penalties, specialists need to independently submit their quality data by 3/31 via a CMS‐qualified registry. It is recommended that if a specialist has not done so already, that they contact a registry as soon as possible. On top of the PQRS payment adjustments, the Value Modifier payment adjusts reimbursement down, depending on practice size.

Why did they do it?
•The overarching purpose of these changes is to move away from fee‐ for‐ service , which is regarded as a major driver of the nations health cost
•To a model of greater responsibility and accountability. This approach is called Population Health management

Outpatient Care Management
•Dedicated Outpatient CMs
•Multi‐condition centers
Emergency / Acute Care
Management• Inpatient CMs• ED CMs• Hospitalists
Post‐Acute Network•SNF Post Acute Network
•Advocate At Home•Palliative Care
Transitions
Patient/PCP
Patient/Family Education and
Support
Community Agencies/Programs
ACO Value Structure: Wrap‐Around Care ContinuumAligned Goals, Strong Relationship and Communication = Patient/PCP Value

The EHR and ICD‐10‐CMThe Diagnosis Codes
• ICD‐10‐CM codes have the potential to reveal moreabout quality of care, so that data can be used in a more meaningful way to
• better understand complications, • better design clinically robust algorithms, and • better track the outcomes of care.

Role of PHOs in avoiding Penalties
Primary Care physicians earn PQRS dollars and avoid future penalties for non‐participation through inclusion in PHO participation in such thing as the Medicare Shared Savings Program (MSSP) or other ACOs‐ also includes specialists who are in a practice group (share tax ID) with primary care physicians included in MSSP

Methodology
•Population health management requires healthcare providers to develop new skill sets and new infrastructure for delivering care

Goal of Population Health Management
• Keep a patient population as healthy as possible,• Minimizing the need for expensive interventions such as emergency room visits, hospitalizations, imaging , testing and unnecessary procedures.
• Address the preventive and chronic care needs of the population.
• Modify the factors that make people sick or exacerbate their illness.

Enterprise Care Management
ECM
Growth
Home Physician Office
Emergency Department Hospital Post Acute
Enterprise Care Management
AccessData + Analytics Communication
3

MedicaidManaged Care Entity Types:
o Managed Care Organization (MCO): Traditional insurance companies offering HMO products. MCOs agree to provide most Medicaid benefits to patients in exchange for monthly full-risk capitated payments from the state. e.g. BCBS, HealthSpring, Aetna Better Health, Meridian, Harmony
o Accountable Care Entity (ACE): ACO-like model that is provider-sponsored. Starts out as share-savings and prepares organizations to later become either an MCO or MCCN. e.g. APP ACE, Community Care Partners NorthShore, Loyola Family Care
o Managed Care Community Network (MCCN): Provider-organized entities accepting full-risk capitation payments serving Medicaid clients. MCCNs must meet similar financial and regulatory requirements as an MCO.
e.g. CountyCare, Community Care Alliance of Illinois [CCAI] a subsidiary of Family Health Network
o Care Coordination Entities (CCE): Provider-organized networks offering coordinate care for specific populations - children with complex medical needs, seniors, and persons with disabilities. Providers are paid fee-for- service with additional risk and performance-based reimbursement.
e.g. Be Well Partners in Health, Together4Health, Entire