Embed Size (px)
Citation preview

J. clin. Path., 1977, 30, 661-665
Alveolar rhabdomyosarcoma presenting as subacuteintravascular coagulationA. ELDOR, ELLA NAPARSTEK,1 J. H. BOSS,2 AND SHOSHANA BIRAN3
From the Departments of Haematology,l Pathology,2 and Oncology,3 Hadassah Medical Organization,Jerusalem, Israel
SUMMARY A patient with rhabdomyosarcoma is described in whom the presenting clinical andlaboratory features were those of disseminated intravascular coagulation. The patient's rapiddownhill course was primarily expressed by haemorrhagic tendency. An alveolar rhabdomyo-sarcoma, affecting many organs, including vascular and cardiac lumina, was found at necropsy andwas considered to be the cause of the consumption coagulopathy.
Rhabdomyosarcoma, the malignant tumour ofstriated muscle, is one of the more common softtissue tumours. Horn and Enterline (1958) sub-divided this neoplasm into the pleomorphic botryoid,embryonal, and alveolar varieties. The alveolarrhabdomyosarcoma occurs mainly in young persons(Enzinger and Shiraki, 1969). The prognosis is poorand the median survival about eight months. Thecause of death in most patients is haematogenous andlymphatic metastatic spread. To the best of ourknowledge, haemorrhagic tendency has been des-cribed in only three cases of alveolar rhabdomyo-sarcoma (Merskey et al., 1967; Lechner and Moran,1952) while it has not been observed in any of the 110cases reported by Enzinger and Shiraki (1969). Wehave recently treated a patient with alveolar rhab-domyosarcoma who presented with signs andsymptoms of a severe bleeding tendency. The labora-tory findings were compatible with the diagnosis ofsubacute disseminated intravascular coagulationleading to a consumption coagulopathy. Because ofthe rarity of this condition it seemed worthwhile toreport this patient's illness.
Case report
A 44-year-old Israeli-born Caucasian engineer wasadmitted to the Department of Haematology of theHadassah Hospital for evaluation on 16 June 1975.
Received for publication 13 December 1976
He complained of fatigue, weight loss, fever (39'C),night sweats, and chest as well as low back pain forone month. Two weeks before admission severallumps on both sides of the neck and large sub-cutaneous haematomas developed. The stools hadbeen soft and tarry black for the last few days. Thepatient had been in hospital elsewhere and treatedwith chloramphenicol and gentamicin. Since therewas no improvement he was transferred to ourhospital. His family and past histories were non-contributory. He appeared severely ill and pale, histemperature was 39°C, and blood pressure 130/80mmHg. The pulse rate was 96 per minute and regular,the respiratory rate 28 per minute. Two large sub-cutaneous haematomas were found on the chest andleft buttock respectively. Tender lumps, measuring2 x 2 cm in diameter, adherent to the adjacenttissues, were palpated on both sides of the neck.Bronchial breathing was heard over the base of theleft lung. The heart sounds were normal. Theabdomen was soft and not tender. The liver waspalpable 4 cm below the right costal margin; it wasfirm and not tender. The spleen was palpable. Rectalexamination did not disclose any abnormality. Thepatient had melaena. There were no abnormalities onneurological examination.
LABORATORY TESTSThe blood sedimentation rate (Westegren examina-tion) was 15 mm in the first hour. The haemoglobinwas 7-9 g. The white blood cell count was 7-7 x 109/lwith a normal differential count. The number of
661
on January 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.7.661 on 1 July 1977. D
ownloaded from

A. Eldor, Ella Naparstek, J. H. Boss, and Shoshana Biran
platelets was 60 x 109/1. Red cells were normocyticand normochromic. Blood urea nitrogen glucose andelectrolytes were within the normal range. The serumuric acid was 8-4 mg/dl, bilirubin 2-5 mg/dl, andalkaline phosphatase 380 u/ml (normal 30-70 u/ml).Glutamic oxaloacetic transaminase (SGOT) was480 u/ml (normal 24-50 u/ml) and lactic dehydro-genase (LDH) 2900 u/ml (normal 150-300 u/ml).Vitamin B12 was 4000 pg/ml (normal 200-900 pg/ml).Electrophoresis and immunoelectrophoresis of theserum proteins were normal. The alphafetoproteinlevel in the serum was not raised. Blood, sputum,and urine cultures were sterile. Urine analysisdisclosed a few erythrocytes in the sediment. Chestradiographs showed several small, round shadowsin both lung fields. Intravenous pyelography wasnormal, although a big mass about 6 x 15 cm indiameter, was visualised over the left psoas muscle,displacing the left kidney laterally and upwards. Aliver scan showed an enlarged liver with multiplesmall filling defects. The patient's course was rapidlydownhill. Subcutaneous haemorrhages continuedto appear and melaena was observed daily. On thefirst day in hospital, sudden paralysis of the leftrecurrent laryngeal nerve, with slight hoarseness,developed. Biopsy of one of the nuchal lumpsrevealed an organised haematoma. The results of thecoagulation studies suggested a consumption coagu-lopathy and are summarised in the Table. The lack
Table Coagulation studies
June16 20 24 26 29
Platelets x 100/1 60 70 60 50 60Clotting time (min) 8 9 7 8
(Lee and White, 1913)Prothrombin time ( Y.) 47 25 40 47 36
(Quick, 1951)Partial thromboplastin time (s) 39 38 36 41 40
(Proctor and Rapaport, 1951)Fibrinogen (mg/dl) 215 174 69
(Ratnoffand Menzie, 1951)Euglobulin lysis time-started (min) 105 70 90 45 90(Von Kaulla and Schultz, 1958)
Fibrinogen related material (Mg/ml) 160 320(Merskey et al., 1966)
of a histological diagnosis, notwithstanding, it wasassumed that the patient was suffering from a rapidlygrowing malignant tumour complicated by con-sumption coagulopathy. The patient was treated byintravenous injections of 200 mg cyclophosphamidedaily, 250 mg hydrocortisone acetate, and 10 000units heparin, the latter given in four divided doses.In addition, he received 300 mg of allopurinol daily.Blood and platelet transfusions were administeredfrequently. No response to therapy was apparent,the patient's condition deteriorated rapidly, and
deep jaundice (bilirubin 10 mg/dl) developed. Bloodydiarrhoea and haematuria were noted during thethree days before death. The patient lost conscious-ness on the 15th day in hospital and died within afew hours.
NECROPSY FINDINGSThe body was that of a well nourished man. Theperitoneal cavity contained 600 ml of serosanguinousfluid. An elongated mass, bulging anteriorly, wasfound within the left psoas muscle. Cut sectionsrevealed a spindle-shaped, soft, fleshy tumour mass,measuring 8 x 5 x 4 cm, surrounded by muscletissue on all its aspects. Although not encapsulated,the tumour was well demarcated from the adjacentmuscle tissue. There was widespread metastaticspread involving the heart, larynx, trachea, lungs,liver, spleen, lymph nodes, pancreas, omentum,mesentery, parietal peritoneum, kidneys, urinarybladder, thyroid and adrenal glands, fat tissue, andbones. The liver (4500 g) and spleen (720 g) werestudded with numerous, variously sized tumournodules, the largest being 2-5 cm in diameter. Centralsoftening and haemorrhages were found on cuttingthrough many of these nodules. The lungs (right550 g; left 720 g) contained a multitude of smallround tumour nodules, ranging up to 0 5 cm indiameter, and were the site of massive intra-alveolarhaemorrhage. There were petechial haemorrhagesin all serosal membranes.
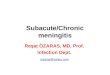
Histologically, the tumour of the psoas muscleand the metastatic nodules showed variously sized,round, oval or polygonal nests and islands, sharplyseparated from each other by delicate, vascularised,connective tissue septa. In some areas, sheets andanastomosing cords were evident. These featuresimparted on the neoplasm an epithelial-like appear-ance, which was emphasised in silver-impregnatedsections. While one, two, and, rarely, more layers ofcells were closely attached to the septa, the vastmajority of the cells were separated and unattached(Fig. 1). The cells were oval, elongated, spindle-shaped or strap-like; a few tennis racket-like cellswere also found (Fig. 2). Cells abutting on thesepta were cuboidal or polyhedral. Binucleated orbizarre, multinucleated giant cells were abundant.The cytoplasm was deeply eosinophilic, and crossstriations were not seen in sections stained withhaematoxylin and eosin or phosphotungstic acidhaematoxylin. The nuclei varied in size and shape,most being round or ovoid and eccentrically placed;eosinophilic intranuclear inclusions were frequent.The thyroid gland was the site of several smallmetastases. One round whitish nodule, 4 x 6 mm indimension, was a highly differentiated papillarycystadenocarcinoma (Fig. 3).
662
on January 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.7.661 on 1 July 1977. D
ownloaded from

Alveolar rhabdomyosarcoma presenting as subacute intravascular coagulation
Fig. 1 General view oftumour. Mosttumour cells arefreelyfloating, thesepta being linedby a layer ofone tothree cells thick. Haematoxylin andeosin x 100.
Fig. 2 Higher magnification showingthe variously shapedfreefloatingtumour cells. Other cells are attachedto the septa. Note tennis racket cells.Haematoxylin and eosin x 420
In addition to many pericardial and myocardialtumour nodules, there were several metastases inthe endocardium, in the shape of small, round oroval foci, replacing adjacent myocardium presentingas intracavitary bosselations, some ofwhich appearedas polypoid structures. Other pertinent findingswere extramedullary haematopoiesis in the liver,spleen, and adrenal glands, jaundice and intrahepaticcholestasis, recent jejunal and ileal haemorrhages,pulmonary oedema, acute passive congestion of theinternal organs, and terminal pancreatitis. Patchy
intra-alveolar haemorrhages were found in bothlungs. The small and medium-sized blood vesselswere meticulously searched for fibrin plateletthrombi. None was found except for recent thrombiin the small veins of the tumour septa. There weretumour cell emboli in a few glomerular capillaries.A single vein contained a mural organising thrombus,in which several tumour cells were lodged. Anosteoma was found in the frontal bone. The brainwas oedoematous, and cut sections revealed recentintracerebellar and subarachnoid haemorrhage.
663
on January 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.7.661 on 1 July 1977. D
ownloaded from

A. Eldor, Ella Naparstek, J. H. Boss, and Shoshana Biran
Fig. 3 Highly differentiatedpapillarycystadenocarcinoma of the thyroidgland containing metastatic rhabdo-myosarcoma cells. Haematoxylinandeosin x 90.
Discussion
The patient presented with an unusual symptomcomplex comprising a widely spread alveolar rhab-domyosarcoma and subacute disseminated intra-vascular coagulation manifested by a generalisedhaemorrhagic tendency. The histological features ofthe neoplasm are characteristic of alveolar rhabdo-myosarcoma as described by Horn and Enterline(1958). This is a particularly malignant neoplasm,most affected patients dying within a short time fromthe onset of clinical signs.At necropsy of our patient, tumour dissemination
was found to be extensive and widespread. Ofspecial interest are the metastases of the rhabdo-myosarcoma into a low-grade papillary cystadeno-carcinoma of the thyroid gland. This phenomenon,referred to as metastasis of tumour to tumour, is of
extreme rarity, the more so as the host tumour wasalso malignant. Furthermore, dissemination to theendocardium and intracavitary growth pattern in theform of polypoid structures are also unusual.
In the last month of his life the patient sufferedfrom a haemorrhagic tendency, associated withprogressive changes of the clotting mechanism. Thethrombocytopenia, decline in fibrinogen, and thehigh titres of fibrinogen-related material (fibrinogendegradation products) support the diagnosis ofsubacute disseminated intravascular coagulation(DIC). The latter was presumably triggered by thewidely spread tumour metastases, which invadedblood vessels and the interior of the heart. It is notsurprising that no fibrin-platelet thrombi were found
on histological examination, in view of the subacutecourse of the DIC, since it is likely that activationof the fibrinolytic system was responsible for dis-solution of any thrombi formed during the terminalperiod. DIC in patients with metastatic cancer isconsidered to result from activation of the coagula-tion system by thromboplastic material releasedfrom the tumour tissue and/or destruction of endo-thelium caused by tumour invasion (Merskey et al.,1967; Peck and Reiquam, 1973; Sun et al., 1974;Al-Mondhiry, 1975). The clinical presentation ofDIC in the majority of cancer patients is a haemorr-hagic tendency,while thrombotic events are evidencedin a minority only (Al-Mondhiry, 1975). Some casesof DIC complicating cancer are asymptomatic, theprocess being detected by impaired coagulationtests only (Al-Mondhiry, 1975; Peck and Reiquam,1973).
Perusal of the literature for further instances ofrhabdomyosarcoma complicated by DIC revealedthree cases. In their report on DIC, Merskey andJohnson (1966) mentioned two such examples. Thethird case, reported by Lechner and Moran (1952),when the concept of DIC was not yet recognised, isthat of a rhabdomyosarcoma in a patient who died ofmassive gastrointestinal haemorrhage. In the patientdescribed here the causal connection between thetumour and the DIC is suggested by the lack of otherpossible causes such as septicaemia or shock.
References
Al-Mondhiry, H. (1975). Disseminated intravascularcoagulation. Experience in a major cancer center.
664
on January 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.7.661 on 1 July 1977. D
ownloaded from

Alveolar rhabdomyosarcoma presenting as subacute intravascular coagulation
Thrombosis et Diasthesis Haemorrhagica, 34, 181-193.Enzinger, F. M. and Shiraki, M. (1969). Alveolarrhabdomyosarcoma, an analysis of 110 cases. Cancer,24, 18-31.
Horn, R. C., Jr. and Enterline, H. T. (1958). Rhabdo-myosarcoma: a clinicopathological study and classi-fication of 39 cases. Cancer, 11, 181-199.
Lechner, F. C., Jr. and Moran, T. J. (1952). Rhabdo-myosarcoma with fatal haemorrhage from intestinalmetastases: case report with autopsy. AmericanJournal of Clinical Pathology, 22, 461-465.
Lee, R. I. and White, P. D. (1913). A clinical study ofthe coagulation time of blood. American Journal ofMedical Science, 145, 495-503.
Merskey, C. and Johnson, A. J. (1966). Diagnosis andtreatment of intravascular coagulation. Pathogenesisand treatment of thromboembolic diseases. Throm-bosis et Diasthesis Haemorrhagica, Supplement 21,555-563.
Merskey, C., Johnson, A. J., Kleiner, G. J., and Wohl,H. (1967). The defibrination syndrome: clinicalfeatures and laboratory diagnosis. British Journal ofHaematology, 13, 528-549.
Merskey, C., Kleiner, G. J., and Johnson, A. J. (1966).
Quantitative estimation of split products of fibrinogenin human serum, relation to diagnosis and treatment.Blood, 28, 1-18.
Peck, S. D. and Reiquam, C. W. (1973). Disseminatedintravascular coagulation in cancer patients: sup-portive evidence. Cancer, 31, 1114-1119.
Proctor, R. R. and Rapaport, S. I. (1961). The partialthromboplastin time with kaolin: a simple screeningtest for first stage plasma clotting factor deficiencies.American Journal of Clinical Pathology, 36, 212-219.
Quick, A. J. (1951). The Physiology and Pathology ofHaemostasis, p. 125. Lea and Febiger, Philadelphia.
Ratnoff, 0. D. and Menzie, C. (1951). A new methodfor the determination of fibrinogen in small samplesof plasma. Journal ofLaboratory and Clinical Medicine,37, 316-320.
Sun, N. C. J., Bowie, E. J. W., Kazmier, F. J., Elveback,L. R., and Owen, C. A., Jr. (1974). Blood coagulationstudies in patients with cancer. Mayo Clinic Proceed-ings, 49, 636-641.
Von Kaulla, K. N. and Schultz, R. L. (1958). Methodsfor evaluation ofhuman fibrinolysis. American Journalof Clinical Pathology, 29, 104-112.
665
on January 10, 2020 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.30.7.661 on 1 July 1977. D
ownloaded from