Embed Size (px)
Citation preview

BioMed Central
Journal of Occupational Medicine and Toxicology
ss
Open AcceResearchAluminosis – Detection of an almost forgotten disease with HRCTThomas Kraus*1, Karl Heinz Schaller2, Jürgen Angerer2, Ralf-Dieter Hilgers3 and Stephan Letzel4Address: 1Institute and Outpatient-Clinic for Occupational and Social Medicine, Aachen University of Technology, Pauwelsstr. 30, D-52074 Aachen, Germany, 2Institute and Outpatient-Clinic for Occupational, Social and Environmental Medicine of the University of Erlangen-Nuremberg, Schillerstr. 25 and 29, D-91054 Erlangen, Germany, 3Institute for Medical Statistics, Aachen University of Technology, Pauwelsstr. 30, D-52074 Aachen, Germany and 4Institute for Occupational, Social and Environmental Medicine of the University Mainz, Obere Zahlbacher Str. 67, 55131 Mainz, Germany
Email: Thomas Kraus* - [email protected]; Karl Heinz Schaller - [email protected]; Jürgen Angerer - [email protected]; Ralf-Dieter Hilgers - [email protected]; Stephan Letzel - [email protected]
* Corresponding author
AbstractThe aim of this study was to investigate whether it is possible to detect high-resolution computedtomography (HRCT) findings in aluminium powder workers, which are consistent with early stagesof aluminosis.
62 male workers from 8 departments of two plants producing aluminium (Al) powder wereinvestigated using a standardized questionnaire, physical examination, lung function analysis,biological monitoring of Al in plasma and urine, chest X-ray, HRCT and immunological tests.
Chronic bronchitis was observed in 15 (24.2%) of the workers, and four workers (6.5%) reportedshortness of breath during exercise. HRCT findings in 15 workers (24.2%) were characterized byill-defined centrilobular nodular opacities. Workers with ill-defined centrilobular nodular opacitieshad a lower vital capacity than workers who had no such HRCT-findings (90.9 % pred. vs. 101.8 %pred., p = 0.01). Biological monitoring in plasma and urine revealed higher internal exposure to Alin affected workers (33.5 µg/l plasma to 15.4 µg/l plasma, p = 0.01) and (340.5 µg/g creat. to 135.1µg/g creat., p = 0.007). Years of exposure and concentration of aluminum in urine and plasmaappear to be the best predictors for HRCT findings. Age and decreased vital capacity showborderline significance.
We conclude that aluminosis is still relevant in occupational medicine. With HRCT it is possible todetect early stages of aluminosis and biological monitoring can be used to define workers at highrisk.
BackgroundThe influence of the toxicity of aluminium and its com-pounds on humans has been the cause of much contro-versy for many years. Since the 1930's an 40's it has beenknown that high-level and long term occupational expo-
sure to metallic aluminium powder and aluminium oxidecan cause lung disease. At that time emphasis was placedon the short and long term effect of toxicity on the respi-ratory tract [4-7]. Recently the main discussion has beenon the neurotoxicity and in particular on the controversial
Published: 17 February 2006
Journal of Occupational Medicine and Toxicology 2006, 1:4 doi:10.1186/1745-6673-1-4
Received: 19 December 2005Accepted: 17 February 2006
This article is available from: http://www.occup-med.com/content/1/1/4
© 2006 Kraus et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Page 1 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
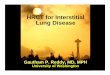
relationship between Alzheimer's disease and occupa-tional or environmental exposure to aluminium [1-3]. Itwas assumed that under today's working conditions lungfibrosis induced by aluminium dust could not occur any-more [6,7]. However, several severe cases of aluminium-induced lung fibrosis have occurred in the last 15 years inGermany [8-10] (Fig. 1).
Histological examination of lung tissue samples showedsevere subpleural and interstitial fibrosis with scar emphy-sema and spotted granulomateous pneumonitis withgiant cells. Energy dispersed X-ray analysis of this caseshowed high concentrations of aluminium in the intersti-tial zones [9]. The pathogenesis of lung diseases inducedby aluminium dust is still unclear. It has been much dis-cussed whether only non-greased aluminium powder(pyro powder) or also greased aluminium powder cancause lung changes. The question is whether diverse addi-tives, in particular stearic acids, are a pathogenetic factorin the development of lung fibrosis [4,5,8]. At first, dis-eases were detected in employees exposed only to highconcentrations of stamped, non-greased aluminium flakepowder. In the production process of aluminium powder,different amounts of stearic acid are added depending onits later use. Non-greased or barely-greased aluminiumpowder with a stearin content of less than 0.1 % (acetoneextract) is used for sintered metals in powder metallurgyand in the production of fireworks, rockets and explosivesin pyrotechnics. In other production fields (e.g. in the pro-duction of porous concrete and pigments for metallicpaints) mainly greased aluminium powders are used inpaste form or as granules with a lower exposure to dust.The threshold values for disease prevention, currentlyvalid in Germany, are a maximum concentration at theworkplace (MAK value) of 4 mg/m3 as inhalable dust, 1.5mg/m3 as respirable dust and a biological tolerance valueat the workplace (BAT value) of 200 µg/l in urine [11].
Aluminium lung is characterized as diffuse interstitialfibrosis which is mainly located in the upper and middlelobes of the lung. In advanced stages it is characterized bysubpleural bullous emphysema with an increased risk ofspontaneous pneumothorax [5]. The prognosis for severeforms of lung fibrosis is poor because the disease can con-tinue to progress after the end of exposure. Therefore earlydetection of aluminium induced fibrotic changes is inval-uable to the timely introduction of preventative measures.Early stage lung changes, induced by aluminium dust,could not be diagnosed to date using conventional X-raysin several cross-sectional studies in the aluminium pow-der industry [9] or during general occupational medicalsurveillance.
The aim of this study is to check whether sensitive toolsfor the detection of interstitial lung diseases, such as high
resolution computed tomography (HR-CT), allow for theearly detection of aluminium induced lung disease.
Study group and MethodsStudy designIn a cross-sectional study, male workers were examined intwo plants producing aluminium powder in Germany.The examination was offered to all workers from 8 depart-ments, who had a high exposure to aluminium powder. Inplant A, 34 of 76 high-exposed workers (44.7%) took partin the study. In plant B, 28 of 44 high-exposed workers(63.6%) from the production units gave their informedconsent. None of the workers refused due to medical rea-sons to take part in the study. The age of the workersranged between 22 and 64 years with a median of 41 years(mean 41.4, SD 9.9 yrs). The smoking history of the work-ers (20 non-smokers, 32 current smokers, 10 formersmokers) was quantified by the cumulative cigarette con-sumption expressed in pack-years (PY).
The study design included a standardized history withspecial attention to occupational history including formerexposures to fibrotic agents, a physical examination of thecardiopulmonary system, biological monitoring of alu-minium in urine and in plasma, lung function analysisand conventional X-rays (first 28 consecutively examinedworkers only) and high resolution computed tomographywith standardized technical parameters [12]. Sufficientdata on ambient monitoring results from the two plantswere not available retrospectively.
MethodsAluminium concentrations in plasma and urine weredetermined by graphite furnace atomic absorption spec-
HRCT-scan of severe aluminosis with subpleural bullaeFigure 1HRCT-scan of severe aluminosis with subpleural bullae.
Page 2 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
trometry (GF-AAS) under the conditions of internal andexternal quality assurance [13,14]. Bodyplethysmographyand spirometry were performed with a Jaeger-Masterlab(Jaeger-Toennies GmbH, Germany) according to ATS cri-teria [15]. It included measurements of the vital capacity(VC), forced expiratory volume (FEV1), total resistance(Rtot), and total lung capacity (TLC). Lung function meas-urements relative to the corresponding reference valuesproposed by the European Community for Coal and Steel[16] were used in the analysis. Evaluation of the conven-tional X-rays was performed using the ILO-classificationfor pneumoconiosis [17], by an experienced blinded (noknowledge of the quantitative exposure or clinical data)radiologist. After the first 28 consecutive chest X-ray exam-inations, this method was discontinued due to the lack ofaluminium-related findings in the chest X-rays. The HRCT
was performed during breath-holding at full inspirationwith a Somatom plus4 scanner from Siemens, Erlangen.Slice thickness was 1 mm with a slice interval of 10 mm.The evaluation of the CT scans was performed with asemi-quantitative score system for CT [12]. Similar to theILO-Classification for pneumoconioses small roundedopacities, irregular and linear opacities, emphysema, hon-eycombing and ground glass pattern as well as pleuralplaques and diffuse pleura thickening were quantified asprofusion grade (parenchyma) and thickness and extent(pleura).
In the case of suspected aluminium-related findings, fur-ther diagnostic tests were performed to exclude otherinterstitial lung diseases. These tests included ergometry,diffusion capacity (DLCO single breath method), bloodgas analysis, and immunological parameters (Table 5).These parameters were C-reactive protein, anti-ribonucle-ase, rheumatoid factor, Rose-Waaler test, antinucleic anti-bodies (ANA) fluorescence test, ribonucleoprotein /Smantibodies, U1-ribonucleoprotein antibodies, sm anti-bodies, Sjoegren-syndrome-A-antibodies (Ro and La),sclerodermia-70-antibodies, CENP-B-antibodies, anti-Jo-antibodies, antimitochondrial antibodies and neu-trophile cytoplasmatic antibodies (AK/C and AK/P). Spe-cific IgG antibodies were analyzed for Penicilliumnotatum, Cladosporium herbarum and Aspergillus fumi-gatus. Specific IgE antibodies were analyzed for grasses,tree pollen (beech, alder, birch, hazel), flakes of cat skin,mold (Penicillium notatum, Cladosporium herbarum,Aspergillus fumigatus), household dust and dust mites.
Informed written consent was obtained from each partic-ipant. The protocol was approved by the Ethics Commit-tee of the Medical School of the University Erlangen-Nuremberg, Germany.
Statistical analysisThe data were described by means, standard deviationsand proportions.
Table 1: Mean, median and standard deviation (SD) of aluminium concentrations in plasma and urine at different workplaces
Al-plasma (µg/l) Al-urine (µg/g creat)
No. % mean median S.D. mean median S.D.
polisher 7 11.3 16.3 5.7 21.5 189.5 76.6 232.3dryer 6 9.7 8.4 8.9 3.8 60.9 62.8 40.2stamper 11 17.7 40.7 40.1 25.9 382.2 415.7 273.1packing 4 6.5 14.0 12.0 10.8 192.2 193.7 124.2mixing 10 16.1 23.1 12.3 24.3 195.8 132.9 215.2ball mills 11 17.7 9.9 7.4 5.8 80.2 27.0 86.5sieving 6 9.7 21.9 15.0 18.3 227.7 175.1 198.4others (controller, metalworker) 7 11.3 12.1 12.8 10.0 83.4 44.7 92.9
Correlation of Al concentrations in plasma and urine (marked dots are workers with early aluminosis)Figure 2Correlation of Al concentrations in plasma and urine (marked dots are workers with early aluminosis).
Page 3 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
We used Pearson correlation to investigate the correlationbetween aluminium concentrations in plasma and urine.
Unpaired t-test were used to find univariate distributionaldifferencies between the cases (occupational disease =yes) and non cases (occupational disease = no) withrespect to age (years), weight (kg), height (cm), time ofexposure (months), Al -plasma (µg/l), Al -urine (µg/gcreat), FEV1/VC (%), TLC (% pred.), VC (% pred.), Rtot(kPa*s/l) and body mass index. Moreover differenciesbetween cases and non-cases in the distribution of smok-ing habits was analysed using χ2 test. The next step of theanalysis is addressed to the question of the multivariatedependency between several independent factors and theoccurrence of an occupational disease (aluminosis). If the
univariate p-value of distributional differencies was below0.40 the corresponding independent factors was includedin the multivariate model. The margin p ≤ 0.4 is chosen tobe rather conservative, because of the limited sample size.Thus the multivariate associations between the occurrenceof an aluminosis and age, sex, smoking habits, lung func-tion parameters (vital capacity, total resistance, forcedexpiratory volume) and biological monitoring were stud-ied using a logistic regression model. Differences with a p-value smaller or equal to 0.05 were regarded as significant.
HRCT-scansFigure 5HRCT-scans. In the whole lung area there are small, ill-defined, diffuse opacities, in the upper right-hand field subp-leural curvilinear lines. Figure 3 upper field, figure 4 middle field, Figures 5 and 6 lower field (case 10, table 5 and 6) [18]
HRCT-scansFigure 4HRCT-scans. In the whole lung area there are small, ill-defined, diffuse opacities, in the upper right-hand field subp-leural curvilinear lines. Figure 3 upper field, figure 4 middle field, Figures 5 and 6 lower field (case 10, table 5 and 6) [18]
HRCT-scansFigure 3HRCT-scans. In the whole lung area there are small, ill-defined, diffuse opacities, in the upper right-hand field subp-leural curvilinear lines. Figure 3 upper field, figure 4 middle field, Figures 5 and 6 lower field (case 10, table 5 and 6) [18]
HRCT-scansFigure 6HRCT-scans. In the whole lung area there are small, ill-defined, diffuse opacities, in the upper right-hand field subp-leural curvilinear lines. Figure 3 upper field, figure 4 middle field, Figures 5 and 6 lower field (case 10, table 5 and 6) [18]
Page 4 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
Statistical analysis were performed using proc ttest, freqand logist with SAS® software.
ResultsOccupational and disease historyThe 62 male workers (plant A: 28; plant B: 34) wereexposed to aluminium powder for a median of 123months (range 13 – 360 months) as stampers (n = 11),polishers (n = 7), dryers (n = 6), packers (n = 4), mixers (n= 10), ball mill operators (n = 11) and others as control-lers, metalworkers etc. (n = 7). Former exposure to fibroticagents was reported by 14 workers. 11 were exposed toasbestos as construction workers (n = 3), metalworkers (n= 6) and car mechanics (n = 2), and 3 to silica dusts. Expo-sure to other fibrotic agents at the current workplace (e.g.other metals including cobalt, beryllium etc.) can beexcluded. 15 workers reported a chronic cough andphlegm, 11 of them were smokers. 9 had a positive historyof pneumonia, pleuritis or tuberculosis. Four workersreported shortness of breath during exercise.
Biological monitoringThe median aluminium concentration in plasma was 12.5µg/l (range 2.5 – 84.4 µg/l) and in urine 83.3 µg/l (range
3.7 – 630.0 µg/l) or 104.3 µg/g creat. (range 7.9 – 821.2µg/g creat.). The BAT value of 200 µg/l urine was exceededin 20 cases (32.3 %). The aluminium concentrations inplasma and urine showed a significant correlation (r =0.83) related to the urinary Al concentration in µg/l and r= 0.93 related to µg/gcreat. (Figure 2).
The intensity of exposure depended on the workplacearea. A detailed description of the internal aluminiumexposure at the different workplaces is shown in Table 1.The highest aluminium concentrations in biologicalmaterials were found in stampers.
Chest X-raysChest X-rays were performed with the first 28 workersinvestigated. In 3 patients small rounded and irregularopacities with a profusion of 1/0 (n = 2) and 1/2 (n = 1)according to the ILO-classification were found. The find-ings were described by the radiologist as non-specific.
HRCT-findingsHRCT revealed in 15 of 62 workers (24.2%) parenchymalchanges of the same pattern. This was characterized bysmall rounded opacities predominantly in the upper lung
Table 3: Anamnestic, lung function data and biological monitoring in workers with and without HRCT findings (t-test)
Parameter Al-induced findings
no yes
Mean Std.Err. Mean Std.Err. Pr>|t|
Age (years) 40.9 1.6 42.9 1.8 0. 3855Weight (kg) 82.9 2.0 82.0 3.7 0. 8221Height (cm) 172.9 1.1 173.5 1.7 0. 7726Time of exposure (months) 142.7 15.2 180.0 21.7 0.1700Al -plasma (µg/l) 15.4 2.5 33.5 6.1 0.0124Al -urine (µg/gcreat) 135.1 24.5 340.5 62.4 0. 0065FEV1/VC (%) 83.9 0.8 86.0 0.7 0.0660TLC (% pred.) 104.6 1.9 95.4 5.1 0.1070VC (% pred.) 101.8 2.1 90.9 3.5 0.0133Rtot (kPa*s/l) 0.2 0.0 0.2 0.0 0.1363Body mass index 27.8 0.6 27.3 1.1 0.6951
Table 2: Smoking habits in workers with and without aluminium-induced findings (% in brackets)
Smoking habits
Non-smokers Current smokers Former smokers total
no aluminosis 17 (27.4) 23 (37.1) 7 (11.3) 47 (75.8)aluminosis 3 (4.8) 9 (14.5) 3 (4.8) 15 (24.2)Total 20 (32.6) 32 (51.6) 10 (16.1) 62 (100)
Page 5 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
regions. Moreover there were signs of a beginning thicken-ing of the interlobular septae in three cases. In four casesthese opacities were located additionally in the middleand lower lobes. The rounded opacities had a maximumdiameter of 3 mm. 9 of the 15 workers with roundedopacities had worked as stampers and were exposed tobarely greased or non-greased aluminium-flake powder.
10 of 15 workers with HRCT findings were found to havealuminium concentrations in urine above the thresholdlimit value of 200 µg/l (Fig. 2).
Examples of the parenchymal changes are shown in Fig-ures 3, 4, 5 and 6. This example has been published as acase report with detailed informations on the diagnosticprocedures and results [18].
Workers with aluminium-induced CT-findingsWorkers with HRCT changes had worked as stampers (n =9), polishers (n = 2), ball mill operators (n = 2), mixers (n= 1) and sievers (n = 1). Affected workers had higher con-centrations of aluminium in plasma (AI-plasma, p = 0.01)and urine (AI-urine, p = 0.003) and a lower vital capacity(p = 0.01) (table 3). The age, time of exposure, total lungcapacity (TLC), resistance (Rtot), and the results of theTiffeneau-test (FEV1/VC) did not differ between workerswith and without lung changes induced by aluminiumdust in the univariate comparison between the groups(table 3). Smoking habits, including number of pack-years, had no influence on the prevalence of HRCTchanges (χ2 test, p = 0.5028) (table 2). Parenchymalchanges did not correlate with the existance of respiratorysymptoms. Higher (200 and more) aluminium concentra-tions in urine (with relation to creatinine) and higher(120 days and more) duration of exposure were signifi-cantly associated with aluminosis. Vital capacity andFEV1/VC were factors of borderline significance (table 4).Including aluminium concentration in urine without cor-rection for creatinine and aluminium concentration inplasma into the regression model yielded to similar
results. With these variations the model fit was slightlyworse.
4 of 15 affected workers (26.7%) and 10 of 42 (23.8%)non-affected workers were exposed to fibrotic agents informer occupations. 5 affected workers reported symp-toms of chronic bronchitis, 4 reported shortness of breathinduced by exercise. During further medical work-up ofthe 15 affected workers, exercise induced decrease in pO2occured in 4 cases (table 5, Nos. 2,10,12,14). 8 patientspresented positive results in immunological tests for spe-cific IgE, indicating sensitization to environmental anti-gens. None of them had any symptoms which suggested aclinical relevance of these findings. Auto-antibodies wereslightly positive in three cases (n = 2 ANA, ANA normalvalue < 1:10; sjoegren syndrome antigen La normal value< 1) without clinical signs of a corresponding disease(table 6). In 11 of 15 cases results from biological moni-toring of Al in plasma were available from former years.The Al-concentrations ranged between 9.8 µg/l and 183µg/l (median 85 µg/l, arithmetic mean 84.6 µg/l) (table6).
DiscussionLung diseases induced by aluminium dust are very rare inoccupational medicine. Between 1960 and 1989 only afew individual cases were identified, mainly in the alu-minium powder industry. It was assumed that undertoday's working conditions lung fibrosis induced by alu-minium dust was virtually non-existant [6,7]. In formertimes, it was even proposed that workers exposed to silicainhale aluminium lactate to suppress the development ofsilicosis [19,20]. Since the beginning of the 90s, however,several cases of severe fibrosis have been recognized by theemployers'liability insurance and financially compen-sated in Germany [8]. Young men with only short periodsof exposure were also affected and the prognosis was poor[10]. In other aluminium industries the existence of alu-minium-induced lung diseases is the subject of much con-troversy [21,22]. In most studies, especially in cross-
Table 4: Logistic regression analysis of factors predicting the occurrence of HRCT changes
Analysis of Maximum Likelihood Estimates Odds Ratio Estimates
Parameter DF Estimate Standard Error Wald Chi-Square Pr>ChiSq Point Estimate 95% Wald Confidence Limits
Intercept 1 -14.5072 10.9830 1.7447 0.1865Age 1 -0.0571 0.0630 0.8217 0.3647 0.944 0.835 1.069Time of exposure 1 0.0152 0.00681 4.9905 0.0255 1.015 1.002 1.029Smoking habits 1 0.4164 1.1040 0.1423 0.7060 1.516 0.174 13.200Vital capacity 1 -0.0664 0.0371 3.2085 0.0733 0.936 0.870 1.006FEV1/VC 1 0.2206 0.1231 3.2149 0.0730 1.247 0.980 1.587Resistance 1 -4.9536 5.8181 0.7249 0.3945 0.007 <0.001 632.518Al (urine(creat.) 1 0.00768 0.00278 7.6541 0.0057 1.008 1.002 1.013
Page 6 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
sectional studies of workers exposed to aluminium, noincrease in the prevalence of pneumoconiotic changeswas found using conventional chest X-rays [9,23]. In onestudy, Townsend et al [24] classified an increase in smallirregular opacities in aluminium smelters as non-specificchanges. De Vuyst et al [25] reported severe lung fibrosisin an aluminium polisher. Early stages of aluminosis havenot yet been described.
In recent years the use of high resolution computed tom-ography (HRCT) has proved very reliable for the detectionof occupationally induced pneumoconiosis [26]. In sev-eral studies HRCT could be shown to have higher sensitiv-ity and specificity compared to conventional chest X-rays,in particular for asbestos-related diseases [26-28]. So farthere are only case reports available on the use of HRCTwith workers exposed to aluminium dust [10,29]. Theydescribed advanced stages of aluminosis. The predomi-nant CT findings consist of subpleural bullae, and paren-chymal changes with distortion of intrathoracalstructures. Early stages of aluminosis have not been speci-fied using either conventional X-rays or CT.
In 15 of 62 high exposed workers we were able to detectearly stages of aluminosis for the first time using HRCT.The CT findings are specified by small rounded and ill-defined centrilobular opacities mainly in the upper lobeswhich cannot be assessed using chest X-rays. The CT find-ings suggest beginning alveolitis, without fibrotic activity.Severe cases from the same plants show that there is a con-siderable risk of these early stages progressing to severefibrosis [9] (Fig. 1). Unfortunately the 15 affected workersin this study refused to undergo bronchoscopy so that nobiopsy results are available. Immediate intervention tookplace to reduce aluminium exposure in both plants.
Affected workers were removed from workplaces withhigh exposures.
Fig 2 shows that not all highly exposed workers werefound to have parenchymal changes. This suggests thatindividual susceptibility plays an important role in thedevelopment of aluminosis. Neither the smoking habitsnor cumulative cigarette consumption in pack-years differbetween affected and non-affected workers (Tables 2 and3). As stampers and subjects with increased and longerexposure were over-represented in the affected group,type, duration and intensity of exposure seem to be themost important risk factors besides unknown individualones. Stampers are exposed to a very fine flake powderwith a high proportion of flakes with a diameter below 5µm. Lung function analysis has a low sensitivity for detect-ing affected workers and is therefore not an appropriatetool for screening exposed workers. Affected workers,however, had a 10 % lower vital capacity than non-affected workers on a group basis (Table 3).
All workers have had regular medical check-ups involvinganamnesis, lung function tests and chest X-rays not exhib-iting early stages of aluminosis. When interpreting the sig-nificant correlations between Al-concentrations in plasmaand urine and the presence of aluminosis, it has to be con-sidered that the results of biological monitoring representacute exposure while the development of aluminosis islikely to be a chronic effect. In 11 of 15 affected workers,results from biological monitoring of Al in plasma wereavailable (table 5b). These show that Al exposure hasbeen, at least during the last 10 years, very high. For diag-nostic purposes HRCT proved to be more sensitive andspecific than chest X-rays for identifying lung diseaseinduced by aluminium dust. However, it is not possible to
Table 5: Anamnestic data and biological monitoring results in 15 affected workers with HRCT findings
Case No. age workplace duration ofexposure (months)
Al-plasma (µg/l)
Al-urine (µg/gcreat)
smoking habits/packyears
other fibrotic agents
cough phlegm shortness of breath
1 39 polisher 122 62.3 665.6 current 9.60 asbestos - - +2 35 stamper 113 42.9 467.8 former 8.00 asbestos + - -3 39 stamper 150 28.1 172.6 current 24.00 silica - - -4 42 ball mill 120 16.6 91.1 current 13.20 asbestos + + -5 48 stamper 78 73.0 545.9 non - no - - -6 41 stamper 124 52.8 446.8 non - no - - -7 31 mixing 156 14.0 207.4 non - no - - -8 48 polisher 312 5.7 72.2 current 22.00 no + + +9 50 stamper 360 8.9 17.3 current 51.00 no + + +10 39 stamper 174 41.0 415.7 former 3.30 no + + +11 53 stamper 258 12.2 210.8 current 11.40 no + + -12 55 stamper 198 77.0 821.2 current 29.25 no - - -13 35 ball mill 276 16.0 142.3 current 29.00 no - - -14 45 sieving 96 26.4 577.5 current 15.50 no - - -15 44 stamper 163 256.0 253.0 former 16.00 no - - -
Page 7 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
use HRCT as a screening tool in an undifferentiated waybecause of the high costs and considerably higher radia-tion exposure compared to chest X-rays. For the selectiveuse of HRCT, high-risk groups must be defined on thebasis of risk factors [26]. Our study showed that job clas-sification, e.g. working as a stamper for many years and,high aluminium concentrations in plasma and urine arethe best markers of workers at risk.
Pathogenetic considerationsRadiomorphological patterns suggest that aluminosisdevelops from alveolitis, as has been shown for otherpneumoconiotic diseases [31]. Long-term follow-up ofthe affected workers will show whether and to what extentregression of the disease is possible. Etiologic agents andpathogenetic considerations other than aluminium can-not be supported.
Arguments for aluminium-induced changes are supportedby (1) the consistent pattern in all affected workers, (2)the fact that there is a dose-dependency in the findings (3)that the changes were found in two different plants and(4) the lack of results that would support another hypoth-esis.
The exposure of 3 workers to asbestos and of 1 worker tocrystalline silica cannot be responsible for the radiologicalfindings in those cases. The sensitization of 8 affectedworkers to environmental antigens is without clinical rel-evance because none of them reported characteristicsymptoms. Moreover, type-I sensitization does not lead toalveolitic changes in the lungs. Specific IgG antibodies orsymptoms that are typical of hypersensitivity pneumoni-tis due to environmental antigens could not be found. Thethree slightly positive antibodies (two ANA, one SS-AG-La) are without clinical relevance because there were noother findings suggesting an auto-immune disease of anykind.
In the scientific literature it has been discussed for manyyears whether only non-greased aluminium powder orspecial additives such as stearic acid are responsible forthe development of fibrosis induced by aluminium dust[4,5,8]. In our group all participants were exposed to amixture of non-greased and at least barely greased alu-minium powder. Parenchymal changes induced by alu-minium dust were present mainly in workers that wereexposed to barely or non-greased aluminium powder atthe stamping workplaces. The highest exposures to alu-
Table 6: Lung function data and results of the immunological tests in 15 affected workers with HRCT findings.
Case No. VC %pred
FEV1/VC (%)
TLC %pred.
Rtot (kPa*l/s) Diff.Cap. (%)
pO2 pCO2 spec. IgE spec. IgG Autoanti- bodies Maximum Al-conc. in
plasma (µg/l) since 1980
1 83.0 85.4 65.10 0.24 119 → → neg neg neg 62.32 82.8 80.7 98.70 0.14 89 ↓ → pos*5 neg neg 112.73 99.8 82.9 82.80 0.30 116 ↑ → pos*6 neg neg 29.54 96.4 89.2 69.00 0.27 105 ↑ → pos*1 neg ANA pos 1:20 9.85 87.0 88.6 66.90 0.24 99 ↑ → pos*7 neg neg 106.26 95.3 86.1 97.80 0.03 95 → → neg neg neg 85.07 84.3 86.5 139.00 0.12 97 ↑ → neg neg neg 28.18 100.0 90.9 85.70 0.15 88 ↑ → pos*2 neg ANA pos.1:20 -9 83.6 86.6 121.00 0.31 64 ↑ → neg neg neg -10 57.5 88.6 68.20 0.12 71 ↓ → pos*4 neg neg 170.111 105.0 83.9 142.00 0.09 117 ↑ → pos*3 neg neg 45.012 86.7 84.5 72.70 0.39 102 ↓ → neg neg neg 183.013 120.0 88.3 125.00 0.14 - ↑ → pos*8 neg neg -14 90.8 83.4 111.00 0.21 100 ↓ ↑ neg neg SS-B-AG La 1.9 -15 91.2 83.9 99.10 0.23 110 ↑ → neg neg neg 100.5
Antigens Class*1 Ragweed, birch, dust mites 2Alder, hazel 1*2 Penicillium notatum, dust mites 3Houshold dust, Aspergillus fumigatus 2Ragweed, Cladosporium herbarum 1*3 Asp. fumigatus 1*4 Dust mites 2*5 Dust mites 1*6 Grasses 2Dust mites, flakes of cat skin, household dust 3*7 Penicillium notatum 3*8 Dust mites 3
Page 8 of 9(page number not for citation purposes)

Journal of Occupational Medicine and Toxicology 2006, 1:4 http://www.occup-med.com/content/1/1/4
minium dust exist at these workplaces and most of thisaluminium dust is respirable with a diameter smaller than5 µm. Lung changes induced by aluminium dust in work-ers that were exposed to only greased aluminium powdercould not be detected in our study. Barely greased or non-greased aluminium powder is therefore thought to be themain pathogenetic risk factor for the development of lungfibrosis induced by aluminium dust, although it is stillnot clear whether greased aluminium powder alone cancause aluminium-induced lung diseases.
ConclusionAluminium is of growing importance in industry and ade-quate substitutes will not be available in the near future.Our findings show that aluminosis is still relevant in occu-pational medicine. Probably the detection of early stagesof aluminosis is not due to a recurrence of a historical dis-ease but to the use of more sensitive diagnostic tools.However, it is important that in addition to a reduction inexposure also specific and efficient measures of secondaryprevention are implemented. Biological monitoring is themost easily available and suitable tool for the identifica-tion and screening of high risk groups [30]. Our findingsalso show that in high-risk groups, HRCT can be animportant complementary tool for the early detection ofaluminosis.
AcknowledgementsThe study was supported by a grant from the Koelsch-Stiftung e.V.
We thank the occupational health physicians and the technical staff from the participating companies. Special thanks to Kathy Bischof for her edito-rial assistance.
References1. Sjögren B, Iregren A, Frech W, et al.: Effects on the nervous sys-
tem among welders exposed to aluminium and manganese.Occ Environ Med 1996, 53:32-40.
2. Strong MJ, Garruto RM, Joshi JG, et al.: Can the mechanisms ofAluminium neurotoxicity be integrated into a unifiedscheme? J Toxicol Environ Health 1996, 48:599-613.
3. Savory J, Exley C, Forbes WF, et al.: Can the controversy of therole of aluminium in Alzheimer's disease be resolved? Whatare the suggested approaches to this controversy and meth-odological issues to be considered? J Toxicol Environ Hlth 1996,48:615-635.
4. Dinman D: Aluminium in the Lung: The Pyropowder Conun-drum. J Occup Med 1987, 29:869-876.
5. Koelsch F: Das Aluminium in der Arbeits- und Versicherungs-medizin. Darmstadt, Dr. Dietrich Steinkopff Verlag; 1964.
6. Morgan W, Dinman B: Pulmonary effects of aluminum. In Alumi-num and health Edited by: Gitelman HJ. New York, Basel, MarcelDekker, Inc; 1989:209-234.
7. Reichel G: Aluminiumstaubpneumokoniose. In PneumokoniosenEdited by: Ulmer WT, Reichel G. Berlin, Heidelberg, New York,Springer Verlag; 1976:484-487.
8. Hartung M, Manke HG, Schmid K, Letzel S: Lungenfibrosen durchAluminiumpulver. In Verh Dtsch Ges Arbeitsmed Umweltmed Editedby: Schuckmann F, Schopper-Jochum S. Stuttgart, Gentner Verlag;1990:263-268.
9. Letzel S: Arbeitsmedizinische Untersuchungen zur Belastungund Beanspruchung in der aluminiumpulverherstellendenIndustrie. In Sonderschrift 8 Edited by: Schriftenreihe der Bundesan-
stalt für Arbeitsmedizin. Berlin, Bremerhaven, Wirtschaftsverlag NW,Verlag für neue Wissenschaft GmbH; 1994.
10. Dehm B, Letzel S, Raithel HJ, et al.: Lungenfibrose nach berufli-cher Aluminiumstaubexposition. Arbeitsmed Sozialmed Umwelt-med 1996, 31:161-164.
11. Deutsche Forschungsgemeinschaft: List of MAK and BAT Values.In Report No. 35 Edited by: Greim H. Weinheim, Wiley-VCH; 2000.
12. Kraus T, Raithel HJ, Hering KG: Evaluation and Classification ofhigh resolution computed tomography findings in patientswith pneumoconiosis. Int Arch Occ Environ Health 1996,68:249-254.
13. Schaller KH, Letzel S, Angerer J: Aluminium. In Handbook on Metalsin Clinical Chemistry Edited by: Seiler H, Sigel A, Sigel H. New York,Basel, Marcel Dekker; 1994:217-226.
14. Lehnert G, Schaller KH, Angerer J: Report on the status of theexternal quality-control programs for occupational-medicaland environmental-medical toxicological analyses in biologi-cal materials in Germany. Int Arch Occup Environ Health 1999,72:60-64.
15. American Thoracic Society: Standardization of Spirometry,1994 Update. Am J Respir Crit Care Med 1995, 152:1107-1136.
16. Quanjer PH, Tammeling GJ, Cotes JE, Pedersen OF, Peslin R, YernaultJC: Lung volumes and forced expiratory flows. Eur Respir J1993, 6:5-40.
17. International Labour Office: International classification of radio-graphs of pneumoconiosis. Occupational safety and healthseries. No. 22 (rev 80). Geneva, International Labour Office; 1980.
18. Kraus T, Schaller KH, Angerer J, Letzel S: Aluminium dust-induced lung disease in the pyro-powder-producing industry:detection by high-resolution computed tomography. Int ArchOccup Environ Health 2000, 73:61-64.
19. Dubois F, Begin R, Cantin A, et al.: Aluminium inhalation reducessilicosis in a sheep model. Am Rev Respir Dis 1988, 137:1172-1179.
20. Begin R, Masse S, Rola-Pleszczynski M, et al.: Aluminum lactatetreatment alters the lungs biological activity of quartz. ExpLung Research 1986, 10:385-399.
21. Abramson MJ, Wlodarczyk JH, Saunders NA, Hensley MJ: Does alu-minum smelting cause lung disease? Am Rev Respir Dis 1989,139:1042-1057.
22. Jederlinic PJ, Abraham JL, Churg A, Himmelstein JS, Epler GR,Gaensler EA: Pulmonary fibrosis in aluminum oxide workers –Investigation of nine workers with pathologic examinationand microanalysis in three of them. Am Rev Respir Dis 1990,142:1179-1184.
23. Saia B, Cortese S, Piazza G, et al.: Chest x-ray findings among alu-minium production plant workers. Med Lavoro 1981, 4:323-329.
24. Townsend MC, Sussman NB, Enterline PE, et al.: Radiographicabnormalities in relation to total dust exposure at a bauxiterefinery and alumina-based chemical products plant. Am RevRespir Dis 1988, 138:90-95.
25. DeVuyst P, Dumortier P, Rickaert F, VanDeWeyer R, Lenglud C, Yer-nault JC: Occupational lung fibrosis in an aluminium polisher.Eur J Respir Dis 1986, 68:131-140.
26. Kraus T, Raithel HJ: Frühdiagnostik Asbest-verursachterErkrankungen. Schriftenreihe des Hauptverbands der gew-erblichen Berufsgenossenschaften. DCM, Druck Center Meck-elheim; 1998.
27. Friedman AC, Fiel SB, Fisher MS, et al.: Asbestos-related pleuraldisease and asbestosis: a comparison of CT and chest radiog-raphy. AJR 1988, 150:269-275.
28. Aberle DR, Gamsu R, Ray CS, Feuerstein IM: Asbestos-relatedpleural and parenchymal fibrosis: Detection with High-Reso-lution CT. Radiology 1988, 166:729-734.
29. Akira M: Uncommon Pneumoconioses: CT and PathologicFindings. Radiology 1995, 197:403-409.
30. Letzel S, Schaller KH, Angerer J, et al.: Biological Monitoring ofoccupational Aluminium Powder Exposure. Occ Hyg 1996,3:271-280.
31. Akira M, Yokoyama K, Yamamoto S, et al.: Early asbestosis: evalu-ation with high-resolution CT. Radiology 1991, 178:409-416.
Page 9 of 9(page number not for citation purposes)