Embed Size (px)
DESCRIPTION
ALTEs , SIDS, and Prems. Russell Lam September 1, 2011 Special thanks to Bela Sztukowski for her help on this presentation. Objectives. Discuss the history of ALTEs , diagnostic work-up, and follow-up Review risk factors for SIDS - PowerPoint PPT Presentation
Citation preview

ALTEs, SIDS, and Prems
Russell LamSeptember 1, 2011
Special thanks to Bela Sztukowski for her help on this presentation

ObjectivesDiscuss the history of ALTEs, diagnostic work-up,
and follow-upReview risk factors for SIDSReview some conditions commonly encountered in
the ED relevant to prematurely born patients

Case 12 mo male brought in after a
choking episode Grandmother picked up baby
after a nap, 2 hours post feed Baby made choking noise
and turned off-colour. Back blows given
Vitals in ED: P120 R45 T 37 BP 95/60 Sp02 100% room air
Exam unremarkable

What investigations do you want (if any)?How long will you monitor in the ED?What do you tell this grandmother?

A historical perspective

“The hypothesis implicating prolonged apnea during sleep is causally related to SIDS underscores the need for further research directed toward a greater understanding of the variables influencing the occurrence of sleep apnea…”
2 decades later – evidence of infanticide for all 5 infants became known

DefinitionsApparent Life Threatening Event
Frightening to the observerCombination of
Apnea Color change Tone change Cough or gagging
Infantile Apnea and Home Monitoring. NIH Consensus Statement 1986 Sep 29-Oct 1;6(6):1-10.

DefinitionsSudden infant death syndrome
Death of infant or child unexplained by historyPost mortem fails to demonstrate adequate
explanation
Less than 1 yearCase investigation and death scene examination fail
to demonstrate adequate explanation
Infantile Apnea and Home Monitoring. NIH Consensus Statement 1986 Sep 29-Oct 1;6(6):1-10.
Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development. Pediatr Pathol. 1991;11:677–684

DefinitionsApnea of infancy
Unexplained cessation in breathing > 20s or < 20s if Bradycardia Cyanosis Pallor Hypotonia
Apnea of prematuritySame as above but < 37 weeks GA
Infantile Apnea and Home Monitoring. NIH Consensus Statement 1986 Sep 29-Oct 1;6(6):1-10.

Who gets ALTEs?0.5-6% of all infantsDifficult to estimate true incidence as:
Subjective nature of definitionNot all ALTEs will visit the EDRetrospective data
Brooks JG. Apparent life-threatening events and apnea of infancy. Clin Perinatol 1992;4:809 – 838.

Who gets ALTEs?
Prospective study (1993-2001)2.46/1000 live birthsAverage age of ALTE = 8 weeks55% of ALTEs had diagnoses
Respiratory (RSV/pneumonia) (29%) GI (GERD/Feeding aspiration) (22%) Congenital cardiac (2%) Metabolic/Neuro (2%)

ALTE Risk Factors
Family history of infant death, single parenthood, profuse night sweating, smoking, repeated cyanotic episodes, pallor, apnea, feeding difficulties

Typical History

Breathing Apnea 70%
Difficulty breathing 62%
Colour Cyanosis 71%
Red face 29%
Pallor 51%
Tone Stiffness 46%
Floppiness 43%
Limb Jerking 22%
GI Choking 35%
Vomiting 18%

Typical physical
Stratton SJ, Taves A, Lewis RJ, et al. Ann Emerg Med 2004; 43:711–717
General physical appearance, work of breathing, circulatory signs, respiratory rate, pulse rate not clinically abnormal

Differential of the cause of an ALTE?


Causes of ALTEs?
N = 643 pts (1991-2002)Most common diagnoses
GERD (31%)Seizure (11%)LRTI (8%)Unknown (23%)

Serious Bacterial Infection?Altman (2008) – Retrospective chart review N=243
5% had occult bacterial infection26% had obvious bacterial infection
Mittal (2009) – Prospective cohort N=19822.2% had cultures0% had serious bacterial infection
Zuckerbraun (2009) – Retrospective chart review N=18261.5% had cultures2.7% had serious bacterial infectionPremature patients more likely to have SBI (6.7 v 0.8%)

A reasonable work-up?



Back to the case…Would you admit this 2 month old patient?
History = consistent with ALTE definitionPhysical = normalRisk Factors
None (no smoke at home, usually feeds well, married parents)

3 year prospective study N = 598 patients met “hospital required” outcome
criteriaMultiple ALTEs and prematurity (<37 weeks) SD from
“hospital not required patients”Most common demographic features were age <
1mos and multiple ALTEsFrom this study, 2 criterion features developed:
age < 1mos and/or multiple ALTEs yields 100% NPV 100% Sens for need for hospital admission

Mortality? Recurrence?
9 year prospective study N = 5633 deaths (0.5%)
2 SIDS and 1 from child abuse
Recurrence37.9% had recurrent episodes8.9% would return visit for ALTE

How is ALTE different from SIDS?

Take home points on ALTEScary+ Apnea/Colour Change/Tone/ChokingBroad differential but mostly GER/LRTI/CNSLikely need admission + broad work-upLow mortality rate (0.5%)ALTE ≠ SIDS


Case 26 mo male brought in because of cough x 3 daysYou diagnose URTI and discharge the patientOn the way out, mother asks: “By the way, a
mother from book club just got an apnea monitor. Should I get one too?”

A little about SIDSMost common cause of death in 1mos-1y (20-25%
of all deaths < 1 year)2006 = 0.54 per 1000 live births in the USMost will occurs age 2-4 months, almost all by 6
months

SIDS versus SUDISudden Unexpected Death of Infancy (SUDI)
Umbrella term which includes SIDS but also other causes of sudden infant death (CVS, Abuse, Metabolics)
SIDS requires autopsy and death scene examination

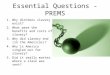
Pathophysiology of SIDS
Filiano and Kinney. Biol Neonate 1994;65(3-4): 194-7

Long QT?
Schwartz et al. 1998. New Eng J Med. 338 (24):1709-1714

Risk factors?

Risk factors?Sleeping proneMaternal smoking during and after pregnancyBed-sharing, especially if EtOH or very tired
parentSoft bedding, pillow, covers over the headPrematurity (<37 weeks)Low birth weight (<2500g)

A safe sleeping environmentCPS 2004 Guidelines
1st six months babies should sleep in own crib in parent’s room
Sleep on back in an approved cribNo quilts/comforters, pillowsRoom-sharing is protective, bed-sharing is notNo sleeping on couch, water bed, air mattress, car
seats



Pacifiers?
Huack et al. Pediatrics (2005). 116 (5):716-722

CPS (2004)Does not recommend pacifier use to reduce risk of
SIDSCaution before routinely advising against pacifier use
AAP (2005)Pacifier for 1st year of life when putting down to sleepDelay until 1 month of age if exclusive breastfeeding

Apnea Monitors?CHIME study (1994-1998)
1079 infants in 4 groups Healthy Term, Idiopathic ALTE, SIDS-Sibling, Preterm All given plethysmography
All groups had similar numbers of apnea/bradycardia on monitors Extreme apneas in 10% of all infants Significantly more AsBs in Preterm infants
But all resolved by 43 weeks post conceptual age 6 deaths, none on monitors

Apnea Monitors?AAP 2005
Many infants get Apneas/Bradycardia and do not dieApnea resolves prior to when most SIDS deaths
occurDoes not prevent SUDIPossible groups who need apnea monitors
Preterm infants CPAP/Trach’d patients

Twins?Malloy (1995)
N = 23464 single SIDS deaths and 1056 twin SIDS deaths
RR 1.13 (95%CI 0.97-1.31) for twins when adjusted for birth weight
RR 8.17 (90%CI 1.18-56.67) if 1 twin died of SIDSGetahun (2004)
N = 501 SIDS deaths overallRR 1.9 (95%CI 1.68-2.01) but not matched for birth
weightRR 4.7 (95%CI not reported) if 1 twin died of SIDS

Take home points on SIDSDifferent from ALTETwo most important risk factors are prone sleeping
and maternal smokingBack to sleep in their own cribDon’t discourage pacifiersApnea monitors don’t helpIf a twin already died of SIDS, other twin at way
higher risk. Admission debatable…


Case 32 month old ex 24 week male comes in with wheeze
and coughMom hands you a summary from the NICU that she
was givenELBW and SGARDS/BPDNECGrade III IVHROP Zone 2 Stage 1GERD with FundoG-Tube Fed

The LingoPrematurity = <37 weeks gestational ageBirth weight
Low birth weight = < 2500gVery low birth weight = < 1500gExtremely low birth weight = < 1000g

The Lingo
Age Terminology During Perinatal Period. Pediatrics. 114 (5):1362-1364

Bronchopulmonary DysplasiaDefined by oxygen needs beyond 28 days of lifeInitial respiratory disease (RDS/Meconium
Aspiration) then chronic lung disease that develops afterwards
3 big risk factorsOxygen toxicityMechanical ventilationExaggerated inflammatory response
Lacy Gomella. Neonatology. 2004


BPD pearls for the EDExamines like asthma
Increased RR, wheeze, cracklesTreat like asthma
SABA, Inhaled Corticosteroids, Oxygen
Consider diureticsSpecial consideration: RSV
If RSV and BPD, more likely to develop apnea and a more severe course = admit!
Passive RSV immunoglobulin upon NICU discharge?
Fleisher et al. Textbook of Pediatric Emergency Medicine. 2010

Necrotizing EnterocolitisSpectrum of acquired neonatal disease with end
expression of serious intestinal injuryEtiology is multifactorial
Infectious/Ischemic/Feeds
Mostly in preterms in first few weeks of life but can present in term babies in first 10 days of life
Presents asSeptic infantLower GI BleedingAbdominal distension and feed intolerence/vomiting
Hackam. Necrotizing Enterocolitis: A leading cause of death and disability. 2008. http://knol.google.com/k/dr-david-hackam/necrotizing-enterocolitis/Mpv6w2_G/t5RhXw.

Hackam. Necrotizing Enterocolitis: A leading cause of death and disability. 2008. http://knol.google.com/k/dr-david-hackam/necrotizing-enterocolitis/Mpv6w2_G/t5RhXw.

Hackam. Necrotizing Enterocolitis: A leading cause of death and disability. 2008. http://knol.google.com/k/dr-david-hackam/necrotizing-enterocolitis/Mpv6w2_G/t5RhXw.


Hackam. Necrotizing Enterocolitis: A leading cause of death and disability. 2008. http://knol.google.com/k/dr-david-hackam/necrotizing-enterocolitis/Mpv6w2_G/t5RhXw.

NEC pearls for the EDTreatment
Broad spectrum antibiotics (Amp/Gent ± Flagyl)NPONG decompressionSerial X-rays Consult surgery
Lacy Gomella. Neonatology. 2004

Apnea of prematurityApnea of infancy
Unexplained cessation in breathing > 20s or < 20s if Bradycardia Cyanosis Pallor Hypotonia
Apnea of prematuritySame as above but < 37 weeks GA
Infantile Apnea and Home Monitoring. NIH Consensus Statement 1986 Sep 29-Oct 1;6(6):1-10.

Apnea of prematurityMore common with younger GAEtiology is multifactorial
Combination of central/obstructive apnea
Treatment in NICUCaffeine, though should be discontinued by
dischargeCPAP

AOP pearls in the EDTypically, NICUs keep babies 8 days after last
apnea episodeIf truly AOP, should resolve by 43 weeks PCASIDS is not prolongation of apnea of prematurityApnea in someone who was previously discharged
from the NICU a few days ago requires careful considerationAOP or not?ALTE?

Post-hemorrhagic HydrocephalusResults from intraventricular hemorrhageRisk of IVH goes up with lower GA
Screening protocols
Secondary to bleeding from germinal matrix in lateral ventricles

Agamanolis. Neuropathology. 2010. http://neuropathology-web.org/chapter3/chapter3dGmh.html

Agamanolis. Neuropathology. 2010. http://neuropathology-web.org/chapter3/chapter3dGmh.html

Agamanolis. Neuropathology. 2010. http://neuropathology-web.org/chapter3/chapter3dGmh.html

Agamanolis. Neuropathology. 2010. http://neuropathology-web.org/chapter3/chapter3dGmh.html

http://www.chop.edu/export/system/galleries/images/hospital/conditions/brain-tumors-161397.gif

VP Shunt Dysfunction/InfectionSymptoms = non specific but may include
headache/vomiting/mental status/feverDiagnosis =
Push the valve (operation varies on the valve)CT/MRI head to rule out worsening ventriculomegalyShunt Series (Skull x-ray, CXR, AXR)Shunt Tap
TreatmentNeurosurgery consult for ± shunt revision


Take home points about premsThey come with lots of comorbid diseasesBPD, NEC, Apnea of Prematurity, VP Shunt
Dysfunction are just a fewParents often know more about their child’s
conditions than you do

ObjectivesDiscuss the history of ALTEs, diagnostic work-up,
and follow-upReview risk factors for SIDSReview conditions commonly encountered in the
ED relevant to prematurely born patients