Embed Size (px)
Citation preview

ENT
© 2005 The Medicine Publishing Company Ltd223ANAESTHESIA AND INTENSIVE CARE MEDICINE 6:7
The success rate of the Macintosh laryngoscope (particularly when combined with the gum-elastic bougie) is such that many anaesthetists cannot claim to be competent in the use of any other device. However, there has been an explosion of alternative methods of tracheal intubation. Many depend on advances in fibre-optic technology that allow better visualization of the glottis. The flexible fibre-optic laryngoscope is the best-known device, but new rigid and malleable fibre-optic endoscopes are appearing, which are more robust, cheaper, have better optics and are easier to clean. Video systems, in which a camera is mounted distally on a flexible or rigid instrument and the image displayed on a small television screen, are also available. This technology converts a familiar-looking laryngoscope into a true endoscope. However, there remains a place for ‘blind’ techniques, particularly when blood, secretions or debris obscure vision.
Blind techniquesBlind techniques are independent of electrical power and generally unaffected by blood and secretions. Therefore, they are success-ful in situations that cannot be controlled with high technology solutions. However, greater dexterity and experience are required than with visual methods. The chances of trauma to the glottis and perforation of the pharyngeal mucosa are greater, though both complications can occur when sighted methods are used. Blind nasal – skilled practitioners have achieved great success with this technique, but the opportunities for instruction are few. Combining the use of a Macintosh laryngoscope, a nasotracheal tube and Magill’s forceps to pass the tube towards an invisible glot-tic aperture remains a worthwhile low-technology technique. Digital – guiding the tube into the glottis digitally was used by Sir William MacEwan in the first report of intubation in the UK in 1874. It has been described as ‘guided tactile probing’ in a report describing success when flexible fibre-optics had failed. Intubating laryngeal mask airway (ILMA) has been used to intubate in many difficult patients and has been successful after the failure of flexible fibre-optic methods. Retrograde intubation – epidural catheters were originally used after a Tuohy needle was inserted through the cricothyroid membrane or upper tracheal ring space. Radiological guidewires with J tips and at least 110 cm in length are suitable. A dedicated kit is marketed by Cook Critical Care Ltd, which contains a wire stiffener to increase the diameter of the wire. Retrograde intubation
can be converted to a partially visual technique by the addition of a flexible fibre-optic laryngoscope. The wire is threaded up the working channel of the ’scope and the endoscope (loaded with tracheal tube) is passed into the trachea using such visual clues as are available. The wire should always be withdrawn through the mouth to avoid contamination of the cervical tissue.
Light-guided intubationLight-guided techniques can be successful in situations where vision is impossible due to bleeding. They have the advantage over blind techniques that visual clues are available. The Trachlight is the best known instrument (Figures 1 and 2).
Sighted techniques Alternative laryngoscope blades – the McCoy levering tip laryngoscope is familiar to all UK anaesthetists, but straight blade instruments are less so (Figure 3). These blades are inserted along the right side of the tongue and the tip is placed below the epiglot-tis (Figure 4). Rigid bronchoscope can be used as an alternative to a straight blade. A gum-elastic bougie is passed through the ’scope into the trachea and a pusher, such as a small uncuffed tracheal tube, used to keep it in place while the bronchoscope is withdrawn. A tracheal tube is then railroaded over the bougie. Rigid and semi-rigid fibre-optic endoscopes use fibre-optic bundles to establish a line of sight from the tip of the instrument
Alternatives to the Macintosh and flexible fibre-optic laryngoscopesIan Calder
Ian Calder is Consultant Anaesthetist at The National Hospital for
Neurology and Neurosurgery, Queen Square, London, and The Royal Free
Hospital, London.
1 The Trachlight.
Reproduced with
permission from
Dercksen B, Borg
P A J. Light-guided
intubation: the
Trachlight. In:
Calder I, Pearce A,
eds. Core topics in
airway management.
Cambridge
University Press,
2005.
2 Transillumination
with the Trachlight.
Reproduced with
permission from
Dercksen B, Borg
P A J. Light-guided
intubation: the
Trachlight. In:
Calder I, Pearce A,
eds. Core topics in
airway management.
Cambridge
University Press,
2005.
ENT
© 2005 The Medicine Publishing Company Ltd224ANAESTHESIA AND INTENSIVE CARE MEDICINE 6:7
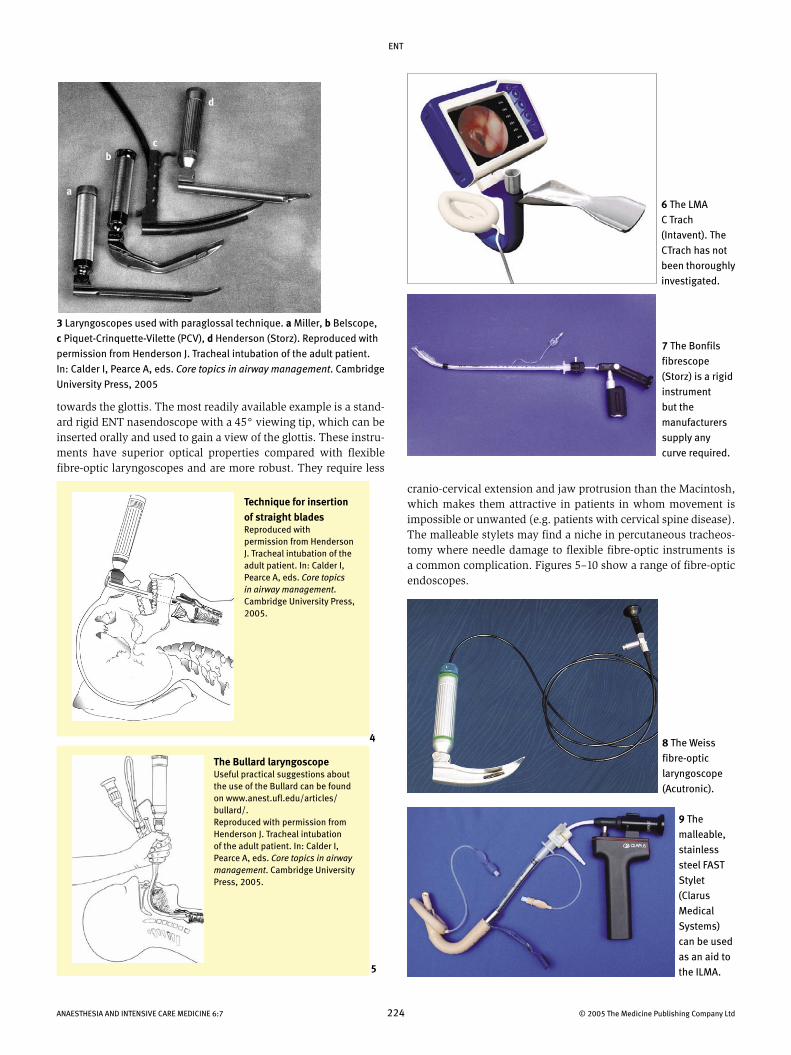
towards the glottis. The most readily available example is a stand-ard rigid ENT nasendoscope with a 45° viewing tip, which can be inserted orally and used to gain a view of the glottis. These instru-ments have superior optical properties compared with flexible fibre-optic laryngoscopes and are more robust. They require less
3 Laryngoscopes used with paraglossal technique. a Miller, b Belscope,
c Piquet-Crinquette-Vilette (PCV), d Henderson (Storz). Reproduced with
permission from Henderson J. Tracheal intubation of the adult patient.
In: Calder I, Pearce A, eds. Core topics in airway management. Cambridge
University Press, 2005
4
5
6 The LMA
C Trach
(Intavent). The
CTrach has not
been thoroughly
investigated.
7 The Bonfils
fibrescope
(Storz) is a rigid
instrument
but the
manufacturers
supply any
curve required.
8 The Weiss
fibre-optic
laryngoscope
(Acutronic).
cranio-cervical extension and jaw protrusion than the Macintosh, which makes them attractive in patients in whom movement is impossible or unwanted (e.g. patients with cervical spine disease). The malleable stylets may find a niche in percutaneous tracheos-tomy where needle damage to flexible fibre-optic instruments is a common complication. Figures 5–10 show a range of fibre-optic endoscopes.
9 The
malleable,
stainless
steel FAST
Stylet
(Clarus
Medical
Systems)
can be used
as an aid to
the ILMA.
Technique for insertion of straight bladesReproduced with permission from Henderson J. Tracheal intubation of the adult patient. In: Calder I, Pearce A, eds. Core topics in airway management. Cambridge University Press, 2005.
The Bullard laryngoscope Useful practical suggestions about the use of the Bullard can be found on www.anest.ufl.edu/articles/bullard/.Reproduced with permission from Henderson J. Tracheal intubation of the adult patient. In: Calder I, Pearce A, eds. Core topics in airway management. Cambridge University Press, 2005.
a
bc
d
ENT
© 2005 The Medicine Publishing Company Ltd225ANAESTHESIA AND INTENSIVE CARE MEDICINE 6:7
10 The Levitan stylet (Clarus Medical Systems) is malleable and
has excellent optics.
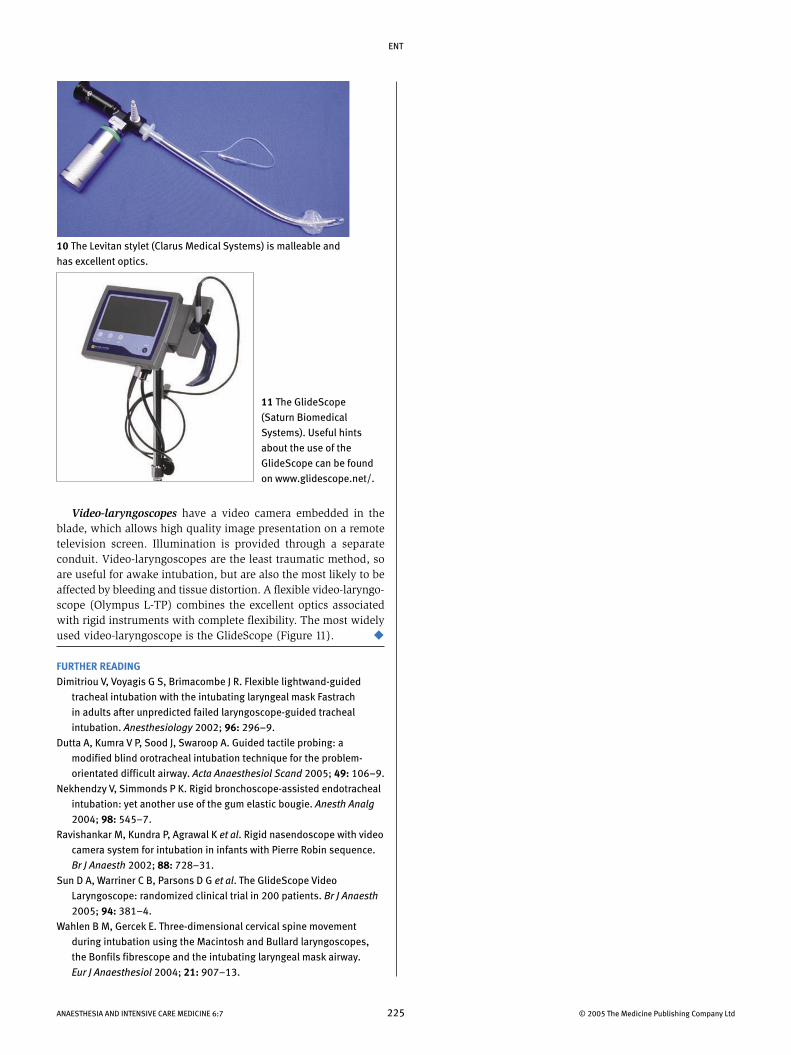
11 The GlideScope
(Saturn Biomedical
Systems). Useful hints
about the use of the
GlideScope can be found
on www.glidescope.net/.
Video-laryngoscopes have a video camera embedded in the blade, which allows high quality image presentation on a remote television screen. Illumination is provided through a separate conduit. Video-laryngoscopes are the least traumatic method, so are useful for awake intubation, but are also the most likely to be affected by bleeding and tissue distortion. A flexible video-laryngo-scope (Olympus L-TP) combines the excellent optics associated with rigid instruments with complete flexibility. The most widely used video-laryngoscope is the GlideScope (Figure 11).
FURTHER READINGDimitriou V, Voyagis G S, Brimacombe J R. Flexible lightwand-guided
tracheal intubation with the intubating laryngeal mask Fastrach
in adults after unpredicted failed laryngoscope-guided tracheal
intubation. Anesthesiology 2002; 96: 296–9.
Dutta A, Kumra V P, Sood J, Swaroop A. Guided tactile probing: a
modified blind orotracheal intubation technique for the problem-
orientated difficult airway. Acta Anaesthesiol Scand 2005; 49: 106–9.
Nekhendzy V, Simmonds P K. Rigid bronchoscope-assisted endotracheal
intubation: yet another use of the gum elastic bougie. Anesth Analg
2004; 98: 545–7.
Ravishankar M, Kundra P, Agrawal K et al. Rigid nasendoscope with video
camera system for intubation in infants with Pierre Robin sequence.
Br J Anaesth 2002; 88: 728–31.
Sun D A, Warriner C B, Parsons D G et al. The GlideScope Video
Laryngoscope: randomized clinical trial in 200 patients. Br J Anaesth
2005; 94: 381–4.
Wahlen B M, Gercek E. Three-dimensional cervical spine movement
during intubation using the Macintosh and Bullard laryngoscopes,
the Bonfils fibrescope and the intubating laryngeal mask airway.
Eur J Anaesthesiol 2004; 21: 907–13.




![HEINE Classic+ Macintosh Fiber Optic Bladesmedicalshop.ro/col_docs/doc_108_ro.pdf · [ 064 ] 10 SECTION LARYNGOSCOPES For information on HEINE battery and rechargeable handles and](https://img.pdfslide.us/doc/110x75/6010f6b2a0582316614e73a5/heine-classic-macintosh-fiber-optic-064-10-section-laryngoscopes-for-information.jpg)
























