Embed Size (px)
Citation preview

Biol Blood Marrow Transplant 20 (2014) 816e822
American Society for BloodASBMTand Marrow Transplantation
Alternative Donor Transplantation for OlderPatients with Acute Myeloid Leukemia inFirst Complete Remission: A Center forInternational Blood and Marrow TransplantResearch-Eurocord Analysis
Daniel Weisdorf 1,2,*, Mary Eapen 2, Annalisa Ruggeri 3,4,Mei-Jie Zhang 2,3,5, Xiaobo Zhong 5, Claudio Brunstein 1,Celalettin Ustun 1, Vanderson Rocha 3,6, Eliane Gluckman 3,7
1Department of Medicine, Blood and Marrow Transplant Program, University of Minnesota,Minneapolis, Minnesota2Center for International Blood and Marrow Transplant Research,Department of Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin3 Eurocord, Hopital Saint Louis, Paris, France4 Service d Hematologie et Therapie Cellulaire, Hopital Saint Antoine, Paris, France5Division of Biostatistics, Medical College of Wisconsin, Milwaukee, Wisconsin6Oxford University Hospitals NHS Trust, Department of Clinical Haematology, Churchill Hospital,Oxford, United Kingdom7Université Paris Diderot, Paris, France
Article history:
Received 23 January 2014Accepted 22 February 2014Key Words:Allogeneic transplantationAcute myeloid leukemiaUmbilical cord bloodUnrelated donors
Financial disclosure: See Acknowl* Correspondence and reprint re
Marrow Transplant Program, DiTransplantation, University of MinSE, Minneapolis, MN 55455.
E-mail address: weisd001@umn
1083-8791/$ e see front matter �http://dx.doi.org/10.1016/j.bbmt.20
a b s t r a c tWe studied patients with acute myeloid leukemia (AML) over age 50 and in first complete remission (CR1)after adult unrelated donor (URD) (n ¼ 441, 8/8 HLA matched; n ¼ 94, 7/8 HLA matched) or umbilical cordblood (UCB; n ¼ 205) transplantations. UCB recipients achieved CR1 within 8 weeks less often, and receivedreduced-intensity conditioning and cyclosporine-based graft-versus-host disease (GVHD) prophylaxis moreoften. Neutrophil recovery was slower in UCB (69% by day 28) compared with 8/8 HLA-matched URD (97%)and 7/8 HLA-matched (91%) (P < .001) recipients. Three-year transplantation-related mortality (TRM) washigher and leukemia-free survival (LFS) lower with UCB (35% and 28%, respectively) versus 8/8 HLA-matched URD (27% and 39%, respectively). TRM was higher in 7/8 HLA-matched URD (41%, P ¼ .01), butLFS was similar at 34% (P ¼ .39). Three-year chronic GVHD was the lowest in UCB (28%) versus 53% and 59%in 8/8 and 7/8 HLA-matched URD recipients, respectively. Three-year survival was 43% in 8/8 HLA-matchedURD (95% confidence interval [CI], 38% to 48%), 30% in UCB (95% CI, 23% to 37%) (P ¼ .002) and 37% in 7/8URD (95% CI, 27 to 46). Allotransplantation for AML in CR1 with any of these grafts extends LFS for over onethird of older patients. In the absence of an 8/8 HLA-matched URD or when transplantation is neededurgently, UCB can provide extended survival. Less frequent chronic GVHD with UCB transplantation may beof particular value for older patients.
� 2014 American Society for Blood and Marrow Transplantation.
INTRODUCTIONPostremission allogeneic transplantation is increasingly
used for treatment of the high-risk acute myeloid leukemia(AML) affecting older adults [1-14]. Although previousreports have validated the utility of several alternative donorsources, little data exist to carefully examine differences intoxicities, outcome, and potency of leukemia controlamongst the available donor choices in these patients.Reports that have compared fully HLA-matched bonemarrow and peripheral blood progenitor cell trans-plantations to mismatched umbilical cord blood (UCB)transplantations confirm comparable leukemia-free survivalbetween the 3 graft sources [15,16]. Transplantation-relatedmortality (TRM) rates are higher and hematopoietic recov-ery and chronic graft-versus-host disease (GVHD) are lower
edgments on page 821.quests: Daniel Weisdorf, MD, Blood andvision of Hematology, Oncology andnesota, MMC 480, 420 Delaware Street
.edu (D. Weisdorf).
2014 American Society for Blood and Marrow14.02.020
after UCB compared with matched bone marrow andperipheral blood progenitor cell transplantation. A limitationof published reports is the inclusion of patients with bothacute myeloid and lymphoblastic leukemia and inclusion ofadults of all ages, with the median ages of study cohortsranging from 30 to 40 years. Data from the Center for Inter-national Blood and Marrow Transplant Research (CIBMTR)show 60% of allogeneic transplant recipients with hemato-logic malignancies in the United States are now over the ageof 50. Because older adults (aged 50 years or older) havehealthy siblings available to be donors less frequently,volunteer adult unrelated donors (URD) or umbilical cordblood (UCB) grafts can facilitate the curative potential ofallotransplantation and to date, haploidentical trans-plantations are rarely performed in this age group. Althoughphysicians may have little hesitation in recommendingHLA-matched sibling donor transplantation, higher GVHDand mortality risks associated with unrelated donor (URD)transplantation might limit others from offering this treat-ment option for older adults [17-20]. As GVHD risks are highafter mismatched URD transplantation, there is further
Transplantation.
D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822 817
hesitation in proceeding to transplantation when anHLA-matched adult unrelated donor is not available. There-fore, in the current analyses, we examined outcomes in 742adults over the age of 50 years with AML in first completeremission (CR1) to compare the effectiveness of trans-plantation of grafts from HLA-matched and mismatchedadult donors to that after HLA-mismatched UCB.
METHODSPatients
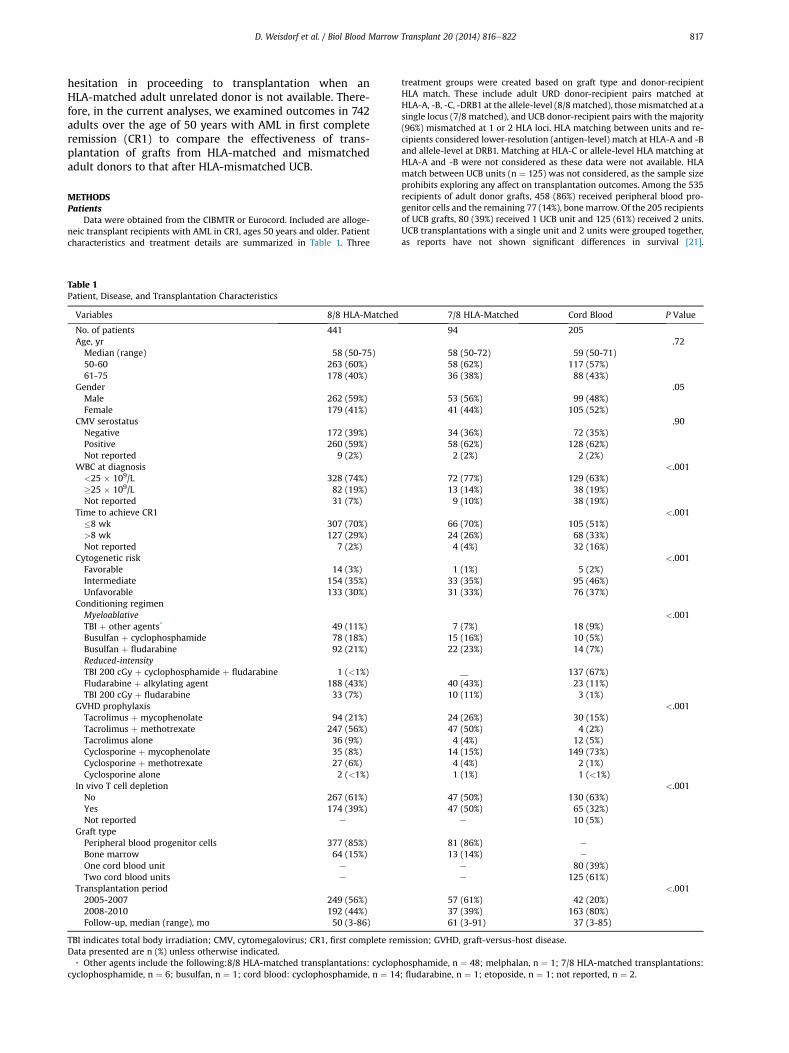
Data were obtained from the CIBMTR or Eurocord. Included are alloge-neic transplant recipients with AML in CR1, ages 50 years and older. Patientcharacteristics and treatment details are summarized in Table 1. Three
Table 1Patient, Disease, and Transplantation Characteristics
Variables 8/8 HLA-Matched
No. of patients 441Age, yrMedian (range) 58 (50-75)50-60 263 (60%)61-75 178 (40%)
GenderMale 262 (59%)Female 179 (41%)
CMV serostatusNegative 172 (39%)Positive 260 (59%)Not reported 9 (2%)
WBC at diagnosis<25 � 109/L 328 (74%)�25 � 109/L 82 (19%)Not reported 31 (7%)
Time to achieve CR1�8 wk 307 (70%)>8 wk 127 (29%)Not reported 7 (2%)
Cytogenetic riskFavorable 14 (3%)Intermediate 154 (35%)Unfavorable 133 (30%)
Conditioning regimenMyeloablativeTBI þ other agents* 49 (11%)Busulfan þ cyclophosphamide 78 (18%)Busulfan þ fludarabine 92 (21%)Reduced-intensityTBI 200 cGy þ cyclophosphamide þ fludarabine 1 (<1%)Fludarabine þ alkylating agent 188 (43%)TBI 200 cGy þ fludarabine 33 (7%)
GVHD prophylaxisTacrolimus þ mycophenolate 94 (21%)Tacrolimus þ methotrexate 247 (56%)Tacrolimus alone 36 (9%)Cyclosporine þ mycophenolate 35 (8%)Cyclosporine þ methotrexate 27 (6%)Cyclosporine alone 2 (<1%)
In vivo T cell depletionNo 267 (61%)Yes 174 (39%)Not reported e
Graft typePeripheral blood progenitor cells 377 (85%)Bone marrow 64 (15%)One cord blood unit e
Two cord blood units e
Transplantation period2005-2007 249 (56%)2008-2010 192 (44%)Follow-up, median (range), mo 50 (3-86)
TBI indicates total body irradiation; CMV, cytomegalovirus; CR1, first complete remData presented are n (%) unless otherwise indicated.
* Other agents include the following:8/8 HLA-matched transplantations: cyclopcyclophosphamide, n ¼ 6; busulfan, n ¼ 1; cord blood: cyclophosphamide, n ¼ 14
treatment groups were created based on graft type and donor-recipientHLA match. These include adult URD donor-recipient pairs matched atHLA-A, -B, -C, -DRB1 at the allele-level (8/8matched), thosemismatched at asingle locus (7/8 matched), and UCB donor-recipient pairs with the majority(96%) mismatched at 1 or 2 HLA loci. HLA matching between units and re-cipients considered lower-resolution (antigen-level) match at HLA-A and -Band allele-level at DRB1. Matching at HLA-C or allele-level HLA matching atHLA-A and -B were not considered as these data were not available. HLAmatch between UCB units (n ¼ 125) was not considered, as the sample sizeprohibits exploring any affect on transplantation outcomes. Among the 535recipients of adult donor grafts, 458 (86%) received peripheral blood pro-genitor cells and the remaining 77 (14%), bonemarrow. Of the 205 recipientsof UCB grafts, 80 (39%) received 1 UCB unit and 125 (61%) received 2 units.UCB transplantations with a single unit and 2 units were grouped together,as reports have not shown significant differences in survival [21].
7/8 HLA-Matched Cord Blood P Value
94 205.72
58 (50-72) 59 (50-71)58 (62%) 117 (57%)36 (38%) 88 (43%)
.0553 (56%) 99 (48%)41 (44%) 105 (52%)
.9034 (36%) 72 (35%)58 (62%) 128 (62%)2 (2%) 2 (2%)
<.00172 (77%) 129 (63%)13 (14%) 38 (19%)9 (10%) 38 (19%)
<.00166 (70%) 105 (51%)24 (26%) 68 (33%)4 (4%) 32 (16%)
<.0011 (1%) 5 (2%)
33 (35%) 95 (46%)31 (33%) 76 (37%)
<.0017 (7%) 18 (9%)
15 (16%) 10 (5%)22 (23%) 14 (7%)
__ 137 (67%)40 (43%) 23 (11%)10 (11%) 3 (1%)
<.00124 (26%) 30 (15%)47 (50%) 4 (2%)4 (4%) 12 (5%)
14 (15%) 149 (73%)4 (4%) 2 (1%)1 (1%) 1 (<1%)
<.00147 (50%) 130 (63%)47 (50%) 65 (32%)
e 10 (5%)
81 (86%) e
13 (14%) e
e 80 (39%)e 125 (61%)
<.00157 (61%) 42 (20%)37 (39%) 163 (80%)61 (3-91) 37 (3-85)
ission; GVHD, graft-versus-host disease.
hosphamide, n ¼ 48; melphalan, n ¼ 1; 7/8 HLA-matched transplantations:; fludarabine, n ¼ 1; etoposide, n ¼ 1; not reported, n ¼ 2.

D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822818
Transplantations were performed between 2005 and 2010. The institutionalreview boards of the Medical College of Wisconsin and the National MarrowDonor Program approved this study.
OutcomesNeutrophil recovery was defined as achieving an absolute neutrophil
count � .5 �109/L for 3 consecutive days and platelet recovery to 20 � 109/Lby day 90. Grade II to IV acute GVHD and chronic GVHDwere assigned usingstandard criteria [22,23], as data to determine National Institutes of Healthchronic GVHD classifications were not available for most patients. TRM wasdefined as death occurring in the absence of leukemia relapse. Leukemiarelapse was defined as molecular, cytogenetic, or morphologic evidence ofrecurrence. Treatment failure was defined as relapse or death from anycause; the inverse of leukemia-free survival. Overall mortality was definedas death from any cause.
Statistical AnalysisWe compared demographics, treatment characteristics, and outcomes
among the 3 treatment groups: 8/8 HLA-matched URD, 7/8 HLA-matchedURD, and mismatched UCB transplantations. Chi-square or the Wilcoxonstatistic was used to compare patient, disease, and transplantation charac-teristics between the 3 treatment groups for categorical or continuousvariables, respectively. The probabilities of neutrophil recovery, acute andchronic GVHD, TRM, and leukemia relapse were calculated using thecumulative incidence estimator [24], and leukemia-free and overall survivalwere calculated using the Kaplan and Meier estimator [25]. To study theassociation between treatment groups and outcomes, multivariate Coxregression models were built [26]. Results are expressed as hazard ratios(HR). All P values are 2-sided and values � .05 were considered significant.
Multivariate models were built using the forward step-wise selectionprocess considering variables shown in Table 1. The treatment group (8/8HLA-matched URD, 7/8 HLA-matched URD, or UCB transplantation), as themain study question, was included in all steps of model building, regardlessof level of significance. The other variables tested were retained in the finalmultivariate model if the variable attained the level of significance set forthese analyses. All models met the assumptions of proportionality, exceptfor TRM. Therefore, a time-dependent model was created for TRM and theeffects are shown as within 3 months after transplantation and beyond thisperiod. There were no first order interactions. Analyses were done using SAS(version 9.3, Cary, NC).
RESULTSPatients, Disease, and Transplantation Characteristics
Among the 441 8/8 HLA-matched URD, 94 7/8 HLA-matched URD, and 205 UCB transplantations, the ages ofthe patients at transplantationwere similar. Themedian agesat transplantation were 58 years for URD recipients and59 years for UCB. However, slightly more UCB recipientswere female and a smaller fraction had a lower white bloodcount at diagnosis. Performance score at transplantationwasnot available for 89 (43%) UCB recipients. However, amongthose for whom performance score was available, there wereno differences across the 3 treatment groups; 274 of 441(62%) recipients of 8/8 HLA-matched URD, 60 of 94 (64%)recipients of 7/8 HLA-matched URD, and 87 of 116 recipientsof UCB transplants reported scores of 90 or 100 (P ¼ .15). UCBrecipients were less likely to achieve CR1 within 8 weeksfrom diagnosis. Recipients of 7/8 HLA-matched (22 of 94;23%) transplants were more likely to have had myelodys-plastic syndrome preceding AML compared with recipients
Table 2Univariate Analysis
Outcomes 8/8 HLA-Matched,Probability(95% CI)
7/8 HLA-MProbability(95% CI)
Neutrophil recovery at day 28 97% (96-99) 91% (85-9Platelet recovery to 20 � 109/L at day 90 91% (88-93) 89% (83-9Acute GVHD grade II-IV at day100 36% (32-41) 44% (34-5Chronic GVHD at 3 years 53% (48-58) 59% (49-6
GVHD indicates graft-versus-host disease.
of 8/8 HLA-matched (70 of 441; 16%) and UCB (31 of 205;15%) transplants (P ¼ .05). In a subset of patients (n ¼ 352;transplantations between 2008 and 2010), data on chemo-therapy delivered before transplantation were available. Inthese patients, 119 of 192 (61%) recipients of 8/8 HLA-matched, 25 of 37 (68%) recipients of 7/8 HLA-matched,and 67 of 96 (70%) recipients of UCB transplants proceededto transplantation after induction therapy (P ¼ .12).Approximately 45% of recipients of 8/8 HLA-matched andUCB transplants received a single cycle of induction therapycompared with 50% of recipients of 7/8 HLA-matchedtransplants (P ¼ .94). Recipients of 8/8 HLA-matched(175 of 441, 40%) and UCB (90 of 205, 44%) transplantswere more likely to proceed to transplantation within3 months of achieving CR1, compared with recipients of 7/8HLA-matched URD transplants (with 24 of 94, 26%)(P< .001). Data on cytogenetic risk were not available for onethird of adult donor transplantations and 14% of UCB trans-plantations. Among those for whom data were available,unfavorable risk cytogenetics was equally likely across the 3treatment groups: 37% among UCB recipients compared with30% and 33% among matched and mismatched URD re-cipients, respectively. There were differences between UCBand URD transplantations with respect to transplantationconditioning and GVHD prophylaxis. UCB recipients weremore likely to receive reduced-intensity conditioning (RIC),whereas URD recipients were just as likely to receive mye-loablative or RIC. The combination of low-dose (200 cGy)total body irradiation with cyclophosphamide and fludar-abine was used exclusively for recipients of UCB grafts. Onthe other hand, fewer than 10% of URD recipients receivedtotal body irradiation 200 cGy and fludarabine. Nearly onehalf of all RIC URD transplantation patients received analkylating agent with fludarabine. Tacrolimus-based GVHDprophylaxis was used most often in the URD recipients, andcyclosporine combinations were used more often for UCB.In vivo T cell depletion using antithymocyte globulin oralemtuzumab was used for a smaller fraction of the UCBtransplantations (32%) compared with the URD groups (39%and 50%, after 8/8 and 7/8 HLA-matched transplantations,respectively). Most URD transplant recipients receivedfilgrastim-mobilized peripheral blood progenitor cells (85%and 86% for 8/8 and 7/8 HLA-matched transplants, respec-tively). URD transplantations were initiated in the earlierstudy years for this older age population and accounted for56% of 8/8 URD and 61% of 7/8 URD transplantations between2005 and 2007, whereas 80% of UCB transplantations wereperformed between 2008 and 2010.
Hematopoietic Recovery, GVHD, and TRMAfter amedian follow-up of 50, 61, and 37months after 8/8
HLA-matched, 7/8 HLA-matched URD, and UCB trans-plantations, respectively, univariate cumulative incidence
atched, Cord Blood,Probability(95% CI)
8/8 HLA-Matchedversus Cord Blood,P Value
7/8 HLA-Matchedversus Cord Blood,P Value
6) 69% (63-75) <.0001 <.00014) 69% (62-75) <.0001 <.00014) 35% (28-41) .69 .149) 28% (22-34) <.0001 <.0001

Table 3Multivariate Analysis
Outcome Hazard Ratio(95% confidence interval)
P Value
Transplantation-related mortalityEarly effect (0-3 months)8/8 HLA-matched BM or PBPC 1.007/8 HLA-matched BM or PBPC 1.19 (.52-2.72) .68Umbilical cord blood 2.83 (1.73-4.62) <.0001
Effect beyond 3 months8/8 HLA-matched BM or PBPC 1.007/8 HLA-matched BM or PBPC 1.73 (1.18-2.54) .005Umbilical cord blood 1.00 (.68-1.47) .99
Relapse*
8/8 HLA-matched BM or PBPC 1.007/8 HLA-matched BM or PBPC .86 (.57-1.29) .47Umbilical cord blood 1.15 (.85-1.54) .36
Treatment failure*
8/8 HLA-matched BM or PBPC 1.007/8 HLA-matched BM or PBPC 1.18 (.91-1.53) .22Umbilical cord blood 1.35 (1.09-1.65) .005
Overall mortalityy
8/8 HLA-matched BM or PBPC 1.007/8 HLA-matched BM or PBPC 1.24 (.95-1.62) .12Umbilical cord blood 1.43 (1.16-1.76) .0008
BM indicates bone marrow; PBPC, peripheral blood progenitor cells.* Adjusted for cytogenetic risk.y Adjusted for cytogenetic risk and patient age.
D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822 819
analyses of hematopoietic recovery and acute and chronicGVHDare shown inTable 2. Theprobabilities of hematopoieticrecovery were lower after UCB compared with 8/8 and 7/8HLA-matched transplants (P < .0001). The probability of day-100 grade II to IV acute GVHD, however, was similar in all 3groups, but the 3-year probability of chronic GVHD wassignificantly lower after UCB transplantations compared with8/8 and 7/8 HLA-matched transplantations (P < .0001).Compared with that of 8/8 HLA-matched transplantations,TRM was higher after 7/8 HLA-matched and UCB trans-plantations (P ¼ .01 and P ¼ .05, respectively), but rateswere similar after UCB and 7/8HLA-matched transplantations(P ¼ .42).
Results of multivariate analyses, adjusting for othersignificant factors showed that grade II to IV acute GVHD risks
Figure 1. Treatment related mortality (*compared with 8/8 URD P < .0001 within 3 mfree survival, relapse, and survival after allogeneic HCT. Adjusted P values reflect the mHLA-matched URD.
were similar after UCB compared with 8/8 HLA-matchedtransplantations (HR, .96; 95% confidence interval [CI], .73 to1.26; P ¼ .75). Acute GVHD risks were higher after 7/8compared with 8/8 HLA-matched transplantation (HR, 1.46;95% CI, 1.06 to 2.03; P ¼ .01). In vivo T cell depletion wasassociated with significantly lower risks of acute GVHD, in-dependent of graft type (HR, .56; 95% CI, .43 to .72; P< .0001).Compared with that of 8/8 HLA-matched transplantations,chronic GVHD risks, analyzed with death as a competinghazard, were significantly lower after UCB transplantations(HR, .49; 95% CI, .37 to .66; P < .0001), but risks were higherafter 7/8 HLA-matched transplantations (HR,1.38; 95% CI, 1.03to 1.85; P ¼ .03). As with acute GVHD, in vivo T cell depletionwas associated with lower chronic GVHD risks (HR, .52; 95%CI, .42 to .66; P < .0001).
TRM was high after both UCB and 7/8 HLA-matchedtransplantations compared with 8/8 HLA-matched trans-plantations, but the timing of mortality differed. As shown,compared with TRM risks of 8/8 HLA-matched trans-plantations, TRM risks were significantly higher after UCBtransplantations within the first 3 months after trans-plantation (Table 3) and, after 7/8 HLA-matched trans-plantations, beyond 3 months after transplantation (Table 3).The 3-year probabilities of TRM after 8/8 HLA-matched andUCB transplantations were 27% (95% CI, 23% to 31%) and 35%(95% CI, 28% to 42%), respectively, P ¼ .05 (Figure 1). Thecorresponding probability after 7/8 HLA-matched trans-plantation was 41% (95% CI, 31% to 51%), P ¼ .01. There wereno significant differences in TRM rates after 7/8 HLA-matched and UCB transplantations (P ¼ .30). The time toCR1 and time from diagnosis or from CR1 to hematopoieticcell transplantation (HCT) were not significantly associatedwith TRM or other outcomes. To examine these influencesmore fully, we reassessed the demographic and trans-plantation characteristics of those patients surviving free ofleukemia at 3 months after transplantation. At that timepoint, the surviving UCB recipients were slightly younger(median age, 58 versus 60 years; P ¼ .01), but other clinicaland demographic characteristics were similar between thosewho died of transplantation-related complications withinthe first 3 months and those who survived into the latter
onths of HCT; compared with 7/8 URD P < .001 beyond 3 months), leukemia-ultivariate analyses shown in Table 3. * indicates P < .0005 compared with 8/8

D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822820
follow-up period (data not shown). Similarly, there were notime period differences in clinical characteristics of 8/8 and7/8 HLA-matched transplant recipients. Thus, the excesstoxicities of UCB grafting apparent in these first 3 post-transplantation months were associated, in part, withslower engraftment and greater risks of graft failure. Thehigher TRM after 7/8 HLA-matched transplantations isattributable to higher risks of GVHD and its associatedmorbidity and mortality. In addition, we tested for the effectof performance score on the subset of patients for whomthese datawere available; TRM risks were higher for patientswho reported performance scores of 80 or lower (HR, 1.45;95% CI, 1.08 to 1.94; P ¼ .01).
Relapse, Leukemia-free, and Overall SurvivalRelapse risks were not significantly different between
the 3 treatment groups (Table 3). Cytogenetic risk groupand intensity of transplantation conditioning regimenwere the only 2 factors that influenced relapse risks andthese effects were independent of donor graft type.Relapse risks were higher in patients with unfavorablecytogenetic risk compared with intermediate cytogeneticrisk (HR, 1.89; 95% CI, 1.41 to 2.50; P < .0001) and goodcytogenetic risk (HR, 3.85; 95% CI, 1.25 to 12.5; P ¼ .02).Relapse risks were higher after RIC compared with mye-loablative regimens (HR, 1.36; 95% CI, 1.04 to 1.77; P ¼ .02).White blood cell count at diagnosis was not associatedwith leukemia relapse. The 3-year probabilities of relapse,adjusted for cytogenetic risk and intensity of trans-plantation conditioning regimens, were 35% (95% CI, 30%to 40%) and 35% (95% CI, 28% to 41%) after 8/8 HLA-matched and UCB transplantations, respectively (P ¼ .95),(Figure 1). The corresponding probability after 7/8 HLA-matched transplantations was 26% (95% CI, 18 to 35) andnot different from that after 8/8 HLA-matched (P¼ .09) andUCB transplantations (P ¼ .13).
Treatment failure (relapse or death; inverse of leukemia-free survival) and overall mortality were higher after UCBtransplantations compared with after 8/8 HLA-matchedtransplantations (Table 3). Treatment failure and mortalityrisks after UCB transplantations and 7/8 HLA-matchedtransplantations were not significantly different. Cytoge-netic risk group and patient age influenced treatment failureand mortality. Mortality risks were also associated withperformance score. These effects were independent of donorgraft type. Treatment failure was higher in patients withunfavorable cytogenetic risk compared with those withintermediate cytogenetic risk (HR, 1.49; 95% CI, 1.06 to 1.85;P¼ .0001) and good cytogenetic risk (HR, 2.04; 95% CI, 1.06 to3.85; P ¼ .03), and was also higher in patients ages 61 to 75,(P ¼ .046) without a significant interaction with graft source.The 3-year probabilities of leukemia-free survival, adjustedfor cytogenetic risk and age, were 39% (95% CI, 34% to 43%)and 28% (95% CI, 22% to 35%) after 8/8 HLA-matched and UCBtransplantations, respectively (P ¼ .01) (Figure 1). The cor-responding probability after 7/8 HLA-matched trans-plantations was 34% (95% CI, 24% to 43%) and not differentfrom that after 8/8 HLA-matched (P ¼ .32) or UCB trans-plantations (P ¼ .39). Similarly, overall mortality was higherin patients with unfavorable cytogenetic risk compared withthose with intermediate cytogenetic risk (HR, 1.47; 95% CI,1.19 to 1.82; P ¼ .0001) and those with good cytogenetic risk(HR, 2.04; 95% CI, 1.04 to 4.00; P ¼ .04). Mortality risks werealso higher in patients ages 61 to 75 years comparedwith those ages 50 to 60 years (HR, 1.21; 95% CI, 1.01 to 1.45;
P ¼ .038) with no interaction between age and graft source.Poor performance score (�80) was associated with higheroverall mortality (HR, 1.27; 95% CI, 1.03 to 1.57; P ¼ .026) andwas independent of graft source. The 3-year probabilities ofoverall survival adjusted for cytogenetic risk and agewere 43% (95% CI, 38% to 48%) and 30% (95% CI, 23% to 37%)after 8/8 HLA-matched and UCB transplantations, respec-tively (P ¼ .002) (Figure 1). The corresponding probabilityafter 7/8 HLA-matched transplantations was 37% (95% CI, 27%to 46%) and not different from that after 8/8 HLA-matched orUCB transplantations (P ¼ .25).
As 60% of UCB transplantations infused 2 UCB units and,in 40%, a single UCB unit, we examined whether trans-plantation outcomes were comparable between the 2groups. With the exception of higher TRM at 3-years aftertransplantation of 2 UCB units (41%; 95% CI, 32% to 50%)compared with 1 UCB unit (27%; 95% CI, 18% to 37%), P ¼ .04,there were no significant differences in relapse or overallsurvival. The 3-year probabilities of relapse after trans-plantation of 2 UCB units compared with 1 unit were 35%(95% CI, 26% to 44%) and 48% (95% CI, 35% to 62%), respec-tively, P ¼ .09. The corresponding probabilities of overallsurvival were 28% (95% CI, 20% to 37%) and 25% (95% CI, 14%to 38%), P ¼ .70.
We also tested for other factors that may potentially in-fluence survival after transplantation, including patientcytomegalovirus seropositivity (HR, 1.01; 95% CI, .83 to 1.22;P¼ .96), conditioning regimen intensity (HR, 1.04; 95% CI, .84to 1.27; P ¼ .74), and transplantation of grafts from femaledonors to male recipients compared with other gendercombinations (HR, .99; 95% CI, .77 to 1.28; P ¼ .97) and foundnone. Mortality risks were lower, but not significantly forpatients for whom the interval between achieving CR1 andtransplantation was longer than 3 months compared withthose who underwent transplantation within 3 months (HR,.83; 95% CI, .68 to 1.01; P ¼ .06). The interval between CR1and transplantation was forced into the final model and theresults were consistent with that reported above (data notshown).
DISCUSSIONThese data examining a large group of alternative donor
transplantations in older patients reported to 2 large inter-national observational registries demonstrate better out-comes after 8/8 HLA-matched transplantations comparedwith those after 7/8 HLA-matched URD or UCB trans-plantations. These observations differ somewhat from thosepreviously reported from our groups as well as others [15-20].The current analysis includes a homogenous group with AMLand all were in CR1 at transplantation, whereas other reportsincluded other leukemias and all disease stages at trans-plantation. Our observations confirm that, for the older pop-ulation with AML, allotransplantation in CR1 can provideextended leukemia-free survival for 30% to 43% of patientsusing any of the donor graft sources available to them.Although an 8/8 HLA-matched adult URD is preferred forpatients who can promptly obtain such a donor, there areknown limitations in timely donor availability. For thoseethnic or racial minorities, or mixed race populations wheresuitably HLA-matched adult unrelated donors are uncom-monly identified, banked unrelated UCB or adult URD mis-matched at a single HLA-locus provide ameaningful chance ofextended leukemia-free survival [27-29]. The higher TRMafter mismatched transplantations with UCB and adultURD must be considered when opting for a mismatched

D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822 821
transplantation. Additionally, the rapid availability of UCBunits provides effective therapy for older patients with ex-pected short initial remissions; settings where ongoingconsolidation therapy has not been effective in limiting risksof relapse [28-36]. Another option of recent interest is ahaploidentical family donor, but as yet, it is uncommonlychosen for this age group. During the study period (2005 to2010), only 29 haploidentical HCTs for patients over age 50with AML in CR1 were reported to the CIBMTR, precludingmeaningful analysis of this approach. Other factors, includingpolymorphisms for immunologically or pharmacologicallyrelevant genetic elements, might also differentially influenceoutcomes, but such data were not available for our analysis[37-41].
Other factors may influence the choices of HCT usingdifferent donors and grafts, particularly with broader andextended experience in this older population; or affect thechoicewhether to proceed to HCTat all [42,43]. The generallydisappointing outcomes for older patients with AML treatedmore conventionally cannot be compared directly in thisobservational HCT dataset, though other reports have sug-gested value for this allografting approach [3,5,7,17,27-29,31-33]. Nonetheless, when considering HCT for older patients,the significantly lower risks of chronic GVHD, occurringwithout apparent compromise in antileukemic protection,might be associated with less morbidity and late mortality inrecipients of UCB transplants [9]. Avoiding the need for long-term immunosuppression and its associated morbiditiesmay be of added importance for these older patients. Anadditional study, directed towards the functional recoveryand quality of life of survivors after allotransplantation at 1, 2,or more years beyond transplantation, may provide neededinsights in assessing these differential late morbidities of anotherwise successful allograft [1]. Studies addressing func-tional recovery and health-related quality of life are outsidethe scope of registry-based studies such as ours.
Limited other data have described outcomes of alterna-tive donor transplantation for this older population. In-vestigators from the University of Minnesota in the UnitedStates, Hôpital Saint-Louis, and Nantes in France recentlydescribed similar overall and leukemia-free survival in amodest-sized population of patients with AML in the sameage group [42]. These somewhat better, or at least compa-rable outcomes, in these 3 experienced centers when judgedagainst this multicenter observational registry data mayreflect center experience in donor selection and specificmanagement practices for this older population and suggeststhat specialized techniques may further improve the re-ported outcomes for this older population. Earlier, McCluneet al. reported similar outcomes for a cohort of sibling andURD recipients overlapping this age group, emphasizing thatallotransplantation is an appropriate and valuable alterna-tive for patients with AML in early remission [44].
The current analysis was conducted using data collectedby 2 large international registries and subject to severallimitations. There were differences in patient and diseasecharacteristics, as well as in transplantation strategies, be-tween the comparison groups, which were in part overcomeby performing carefully controlled regression analyses.Further improvements in donor and graft selection to in-crease the fraction with HLA-allele better-matched grafts,improved HLA matching and cell dose for UCB unit selection,plus elements of supportive care using in vivoTcell depletionand optimal GVHD prophylaxis, could further improve sur-vival for this older population. Although older patients with
AML are often presumed to be too old or too sick for trans-plantation and infrequently have available matched siblingdonors, these encouraging results suggest that allo-transplantation need not be withheld, and for the right AMLpatients, can produce extended and even curative long-termsurvival.
ACKNOWLEDGMENTSConflict of interest statement: There are no conflicts of
interest to report.Financial disclosure: Supported in part by grants from the
NIH and the National Institute for Health Research (NIHR),Oxford Biomedical Research Centre at Oxford UniversityHospitals NHS Trust and University of Oxford.
REFERENCES1. Deschler B, Binek K, Ihorst G, et al. Prognostic factor and quality of life
analysis in 160 patients aged > or ¼60 years with hematologic neo-plasias treated with allogeneic hematopoietic cell transplantation. BiolBlood Marrow Transplant. 2010;16:967-975.
2. Devine S, Owzar K, Blum W, et al. A phase II study of allogeneictransplantation for older patients with AML in first complete remissionusing a reduced intensity conditioning regimen: results from CALGB100103/BMT CTN 0502. Blood. 2012;120 [Abstract 230].
3. Estey E. Acute myeloid leukemia and myelodysplastic syndromes inolder patients. J Clin Oncol. 2007;25:1908-1915.
4. Wong R, Giralt SA, Martin T, et al. Reduced-intensity conditioning forunrelated donor hematopoietic stem cell transplantation as treatmentfor myeloid malignancies in patients older than 55 years. Blood. 2003;102:3052-3059.
5. Farag SS, Maharry K, Zhang MJ, et al. Comparison of reduced-intensityhematopoietic cell transplantation with chemotherapy in patients age60-70 years with acute myelogenous leukemia in first remission. BiolBlood Marrow Transplant. 2011;17:1796-1803.
6. Koreth J, Aldridge J, Kim HT, et al. Reduced-intensity conditioninghematopoietic stem cell transplantation in patients over 60 years:hematologic malignancy outcomes are not impaired in advanced age.Biol Blood Marrow Transplant. 2010;16:792-800.
7. Kurosawa S, Yamaguchi T, Uchida N, et al. Comparison of allogeneichematopoietic cell transplantation and chemotherapy in elderly pa-tients with non-M3 acute myelogenous leukemia in first completeremission. Biol Blood Marrow Transplant. 2011;17:401-411.
8. Majhail NS, Brunstein CG, Shanley R, et al. Reduced-intensity he-matopoietic cell transplantation in older patients with AML/MDS:umbilical cord blood is a feasible option for patients without HLA-matched sibling donors. Bone Marrow Transplant. 2012;47:494-498.
9. Uchida N, Wake A, Takagi S, et al. Umbilical cord blood transplantationafter reduced-intensity conditioning for elderly patients with hema-tologic diseases. Biol Blood Marrow Transplant. 2008;14:583-590.
10. Appelbaum FR. Dose intensity and the toxicity and efficacy of alloge-neic hematopoietic cell transplantation. Leukemia. 2005;19:171-175.
11. Barrett AJ, Savani BN. Stem cell transplantation with reduced-intensityconditioning regimens: a review of ten years experience with newtransplant concepts and new therapeutic agents. Leukemia. 2006;20:1661-1672.
12. Finke J, Nagler A. Viewpoint: what is the role of allogeneic haemato-poietic cell transplantation in the era of reduced-intensity conditioninge is there still an upper age limit? A focus on myeloid neoplasia.Leukemia. 2007;21:1357-1362.
13. Lazarus HM, Rowe JM. Reduced-intensity conditioning for acutemyeloid leukemia: is this strategy correct. Leukemia. 2006;20:1673-1682.
14. Aoudjhane M, Labopin M, Gorin NC, et al. Comparative outcome ofreduced intensity and myeloablative conditioning regimen in HLAidentical sibling allogeneic haematopoietic stem cell transplantationfor patients older than 50 years of age with acute myeloblasticleukaemia: a retrospective survey from the Acute Leukemia WorkingParty (ALWP) of the European group for Blood and Marrow Trans-plantation (EBMT). Leukemia. 2005;19:2304-2312.
15. Eapen M, Rocha V, Sanz G, et al. Effect of graft source on unrelateddonor haematopoietic stem-cell transplantation in adults with acuteleukemia: a retrospective analysis. Lancet Oncol. 2010;11:653-660.
16. Brunstein CG, Eapen M, Ahn KW, et al. Reduced-intensity conditioningtransplantation in acute leukemia: the effect of source of unrelateddonor stem cells on outcomes. Blood. 2012;119:5591-5598.
17. Mohty M, de Lavallade H, Padaique P, et al. The role of reduced in-tensity conditioning allogeneic stem cell transplantation in patientswith acute myeloid leukemia: a donor versus no donor comparison.Leukemia. 2005;19:916-920.

D. Weisdorf et al. / Biol Blood Marrow Transplant 20 (2014) 816e822822
18. Shimoni A, Hardan I, Shem-Tov N, et al. Allogeneic hematopoieticstem-cell transplantation in AML and MDS using myeloablative versusreduced-intensity conditioning: the role of dose intensity. Leukemia.2006;20:322-328.
19. Shimoni A, Kroger N, Zabelina T, et al. Hematopoietic stem-cell trans-plantation fromunrelateddonors inelderlypatients (age>55years)withhematologic malignancies: older age is no longer a contraindicationwhen using reduced intensity conditioning. Leukemia. 2005;19:7-12.
20. Alousi AM, Le-Rademacher J, Saliba RM, et al. Who is the better donorfor older hematopoietic transplant recipients: an older-aged sibling ora young, matched unrelated volunteer? Blood. 2013;121:2567-2573.
21. Scaradavou A, Brunstein CG, Eapen M, et al. Double unit grafts suc-cessfully extend the application of umbilical cord blood transplantationin adults with acute leukemia. Blood. 2013;121:752-758.
22. Przepiorka D, Weisdorf D, Martin P, et al. 1994 Consensus conferenceon acute GVHD grading. Bone Marrow Transplant. 1995;15:825-828.
23. Flowers ME, Kansu E, Sullivan KM. Pathophysiology and treatment ofgraft-versus-host disease. Hematol Oncol Clin North Am. 1999;13:1091-1112.
24. Gooley TA, Leisenring W, Crowley J, Storer BE. Estimation of failureprobabilities in the presence of competing risks: new representationsof old estimators. Stat Med. 1999;18:695-706.
25. Klein JP, Moeschberger ML. Survival Analysis: Statistical methods forcensored and truncated data, Second ed. New York, NY: Springer-Ver-lag; 2003.
26. CoxDR. Regressionmodel and life tables. J R Stat Soc B. 1972;34:187-200.27. Ustun C, Lazarus HM, Weisdorf D. To transplant or not: a dilemma for
treatment of elderly AML patients in the twenty-first century. BoneMarrow Transplant. 2013;48:1497-1505.
28. Oran B, Weisdorf DJ. Survival for older patients with acute myeloid leu-kemia: a population-based study. Haematologica. 2012;97:1916-1924.
29. Appelbaum FR, Gundacker H, Head DR, et al. Age and acute myeloidleukemia. Blood. 2006;107:3481-3485.
30. Becker H, Marcucci G, Maharry K, et al. Favorable prognostic impact ofNPM1 mutations in older patients with cytogenetically normal de novoacute myeloid leukemia and associated gene- and microRNA-expression signatures: a Cancer and Leukemia Group B study. J ClinOncol. 2010;28:596-604.
31. Frohling S, Schlenk RF, Kayser S, et al. Cytogenetics and age are majordeterminants of outcome in intensively treated acute myeloid leuke-mia patients older than 60 years: results from AMLSG trial AML HD98-B. Blood. 2006;108:3280-3288.
32. Gardin C, Turlure P, Fagot T, et al. Postremission treatment of elderlypatients with acute myeloid leukemia in first complete remission afterintensive induction chemotherapy: results of the multicenter ran-domized Acute Leukemia French Association (ALFA) 9803 trial. Blood.2007;109:5129-5135.
33. Giles FJ, Borthakur G, Ravandi F, et al. The haematopoietic cell trans-plantation comorbidity index score is predictive of early death andsurvival in patients over 60 years of age receiving induction therapy foracute myeloid leukaemia. Br J Haematol. 2007;136:624-627.
34. Itzykson R, Gardin C, Pautas C, et al. Impact of post-remission therapyin patients aged 65-70 years with de novo acute myeloid leukemia: acomparison of two concomitant randomized ALFA trials with over-lapping age inclusion criteria. Haematologica. 2011;96:837-844.
35. Leith CP, Kopecky KJ, Godwin J, et al. Acute myeloid leukemia in theelderly: assessment of multidrug resistance (MDR1) and cytogeneticsdistinguishes biologic subgroups with remarkably distinct responses tostandard chemotherapy. A Southwest Oncology Group study. Blood.1997;89:3323-3329.
36. Kantarjian H, O’Brien S, Cortes J, et al. Results of intensive chemo-therapy in 998 patients age 65 years or older with acute myeloidleukemia or high-risk myelodysplastic syndrome: predictive prog-nostic models for outcome. Cancer. 2006;106:1090-1098.
37. Middleton PG, Taylor PRA, Jackson G, et al. Cytokine gene poly-morphisms associated with severe acute-graft-versus-host disease inHLA-identical sibling transplants. Blood. 1998;92:3943-3948.
38. Lin M-T, Storer B, Martin PJ, et al. Relation of an interleukin-10 pro-moter polymorphism to graft-versus-host disease and survival afterhematopoietic-cell transplantation. N Engl J Med. 2003;349:2201-2210.
39. Dickinson AM, Harrold JL, Cullup H. Haematopoietic stem cell trans-plantation: can our genes predict clinical outcome? Expert Rev MolMed. 2007;9:1-19.
40. Newell LF, Gooley T, Hansen JA, et al. Tumor necrosis factor poly-morphism affects transplantation outcome in patients with myelo-dysplastic syndrome but not in those with chronic myelogenousleukemia, independent of the presence of HLA-DR15. Biol BloodMarrow Transplant. 2010;16:1700-1706.
41. Xiao H, Cao W, Lai X, et al. Immunosuppressive cytokine gene poly-morphisms and outcome after related and unrelated hematopoieticcell transplantation in a Chinese population. Biol Blood Marrow Trans-plant. 2011;17:542-549.
42. Peffault de Latour R, Brunstein CG, Porhcer R, et al. Similar overallsurvival using sibling, unrelated donor, and cord blood grafts afterreduced-intensity conditioning for older patients with acute myelog-enous leukemia. Biol Blood Marrow Transplant. 2013;19:1355-1360.
43. Eapen M, Klein JP, Sanz GF, et al. Effect of donor-recipient HLAmatching at HLA A, B, C, and DRB1 on outcomes after umbilical-cordblood transplantation for leukaemia and myelodysplastic syndrome:a retrospective analysis. Lancet Oncol. 2011;12:1214-1221.
44. McClune BL, Weisdorf DJ, Pedersen TL, et al. Effect of age on outcome ofreduced-intensity hematopoietic cell transplantation for older patientswith acute myeloid leukemia in first complete remission or withmyelodysplastic syndrome. J Clin Oncol. 2010;28:1878-1887.