Embed Size (px)
Citation preview

COMMENT
ALTERNATIVE DISPUTE RESOLUTIONSTRATEGIES IN MEDICAL
MALPRACTICE
THOMAS B. METZLOFF*
I. INTRODUCTION
Perhaps no other litigation area has been the subject of as much interestin reform as has medical malpractice. A distinct element of this interesthas centered on efforts to change the process by which malpractice casesare handled. Since the mid-1970's, virtually every state has attemptedsome type of "tort reform" intended to impact the manner in which medicalmalpractice suits are handled.' In light of the incredible growth in the use
Copyright © 1992 by Alaska Law Review
* Professor of Law, Duke University School of Law, and Director, The MedicalMalpractice Program for the Private Adjudication Center. The Center is a non-profitaffiliate of the Duke University School of Law involved in teaching, researching, andproviding services relating to ADR. In 1987, the Center received a grant from the RobertWood Johnson Foundation to study existing litigation procedures and to develop ADRmethods for malpractice cases. Under the auspices of that program, the Center has advisedlitigants in numerous medical malpractice cases on ADR options.
This article developed from a presentation that the author made to the Alaska HealthResources & Access Task Force in Anchorage on October 22, 1992. The author appreciatesthe insights about the Alaskan situation shared with him by members of the Alaska TrialLawyers' Association, the Alaska Medical Society and Dr. Rodman Wilson, a long-timeadvocate for health care and malpractice reform in Alaska. The author would also like toacknowledge the assistance provided by Nancy Cornwell, Project Director, Health Resources& Access Task Force. Finally, the author wishes to thank Jon Aronie, Debbie Munsen, andJenny Bogdes, staff members with the Alaska Law Review, for their assistance in thepreparation of this comment.
1. For discussions of malpractice reform efforts including descriptions of proceduralchanges, see U.S. GEm. Accr. OFF., MEDICAL MALPRACrICE: A FRAMEWORK FOR ACrION(1987) [hereinafter FRAMEWORK FOR ACTION]; PAUL C. WEILER, MEDICAL MALPRACTICEON TRIAL (1991); Glen 0. Robinson, The Medical Malpractice Crisis of the 1970's: ARetrospective, 49 LAW & CONTEMP. PROBS., Spring 1986, at 5; Walter J. Wadlington, LegalResponses to Patient Injury: A Future Agenda for Research and Reform, 54 LAW &CONMrEP. PROBS., Spring 1991, at 199.

ALASKA LAW REVIEW
of alternative dispute resolution ("ADR") methods in the past decade,2 itis inevitable that policy-makers will become interested in exploring howthe myriad ADR techniques might be best employed in the malpracticecontext. This comment will examine actual and potential applications ofADR approaches for handling medical malpractice disputes, focusingparticularly on ADR strategies for Alaska.
IL CONCEPTUALIZING THE POTENTIAL BENEFITS OF ADR:UNDERSTANDING THE CURRENT SYSTEM
An initial task is to describe ADR's potential benefits in themalpractice context. This requires an understanding of the currentlitigation frameworlk. Ilustration 1 (Appendix A) depicts a simplified timeline showing how a typical malpractice claim is processed through thecurrent system. The "X" indicates the point of the alleged malpractice.Malpractice suits are typically not filed until at least one or two years afterthe alleged negligence. Relatively little is known about why some potentialplaintiffs decide to assert a malpractice claim while others elect to donothing? No doubt the decision involves several factors, such as thesophistication of the patient, the patient's access to legal information, andthe seriousness of the patient's injury.4
Malpractice claimants usually must resort to filing a formal lawsuit ifthey are to obtain compensation. While there is some pre-itigationsettlement of malpractice claims, it is rare; most claimants who obtain anycompensation do so only after filing a lawsuit.5 Once a lawsuit is filed,the litigation system has three primary phases, each of which is shown inIllustration 1: (1) the pleading stage, which defines the parties' claims anddefenses; (2) the discovery stage, during which the litigants investigate thefacts surrounding their dispute; 6 and (3) the trial stage, in which the
2. For a general overview of ADR techniques and discussion of issues relating to theirdevelopment, set STEPEN B. GOLDBERG ET AL., DISPUTE RESOLUrION (2d ed. 1992).
3. Recent evidence shows that most patients with potential malpractice claims - thosepatients who have suffered an iatrogenic injury attributable to a physician's negligence -do not assert any claim. See HARVARD MEDICAL PRACTICE STUDY, PATIENTS, DOCTORS,AND LAWYERS: MEDICAL INJURY, MALPRACTICE LiTIGATION, AND PATIENT COMPENSATIONIN NEW YORK (1990).
4. See generally Marlynn L. May & Daniel B. Stengel, Who Sues their Doctors? HowPatients Haidle Medical Grievances, 24 LAW & Soc'Y REv. 105 (1990).
5. See JAMES S. KAKAiK & NICHoLAS M. PACE, CoSTS AND COMPENSATION PAIDIN TORT LITIGATION 31 (1986) (noting that approximately 90% of the dollars paid toclaimants occurred after a lawsuit was filed). In comparison, only about 33% of the dollarsawarded to automobile accident claimants required a lawsuit; the balance was paid insettlements reached without the need to resort to a lawsuit. Id.
6. Rules of procedure permit both parties full access to all relevant information
430 [Vol. 9:2

ADR STRATEGIES
dispute is resolved by the jury. In addition, for those cases that run thecourse of the procedural gauntlet, the system provides an appeal process.
While one can articulate the goals of the procedural system in variousways, the following seem paramount, at least in the context of medicalmalpractice disputes: (1) to identify and dismiss non-meritorious litigation;(2) to provide a framework in which voluntary settlement negotiations canoperate; and (3) to provide a dispute resolution process (the jury) forresolving non-settled claims.7
A. Identifying Non-Meritorious LitigationIt is well known that the vast majority of malpractice cases (upwards
of ninety percent) are resolved prior to trial. In fact, this high percentageof settlements combines two very different phenomena: (1) plaintiffsdismissing their suits without receipt of any payment; and (2) settlementsin which the plaintiff receives a monetary indemnity. The former categorypotentially includes a large number of non-meritorious claims that arguablyshould not have been filed in the first place. One of the major criticismsof malpractice litigation is that it permits, or even fosters, such claims.
Existing empirical evidence suggests that a significant percentage offiled malpractice claims are eventually dismissed or dropped withoutpayment to the plaintiff.8 To some observers, this suggests that thoseclaims were lacking in merit and should never have been filed. While thisis not necessarily true, it does raise serious concerns as to whether there aretoo many "frivolous" malpractice cases. The procedural device known assummary judgment is intended to discourage non-meritorious litigation bygiving the courts the opportunity to dismiss such claims. Although there
relating to a claim. This investigatory process includes several different methods ofobtaining information, including requests for relevant documents (such as medical records);interrogatories (written questions of the opposing party); and depositions (in which theparties, relevant witnesses, and experts respond to oral questions asked by the attorneys).
7. See Thomas B. Metzloff, Researching Litigation: The Medical MalpracticeExample, 51 LAW & CONTEMP. PROBS., Autumn 1988, at 199, 202 [hereinafter Metzloff,Researching Litigation].
8. The extent of "frivolous" malpractice litigation is a sharply contested point. Thebest current empirical evidence suggests that the percentage of non-meritorious malpracticeclaims is substantial, probably near the 40% level. See Frederick W. Cheney et a].,Standard of Care and Anesthesia Liability, 261 JAMA 1599 (1989). Cheney's studyinvolved expert review of over 1,000 case files to determine whether inadequate medicalcare was in fact rendered. The study found that 46% of the claims involved appropriatecare (and thus were technically "non-meritorious" claims). The majority of the plaintiffsin those cases received no compensation, although about 40% did receive some amount.However, the amount received was usually far less than for those plaintiffs with similarinjuries who were victims of inadequate care. Id.; see generally Henry S. Farber &Michelle I White, Medical Malpractice: An Empirical Examination of the LitigationProcess, 22 RAND . ECON. 199 (1991) (finding that 95 of 252 claims against a hospitalinvolved "appropriate" care).
19921
ALASKA LAW REVIEW
has been no empirical study directed towards the use of summary judgmentin malpractice cases, the conventional wisdom is that summary judgmentis ineffective.9 Medical professionals concerned with plaintiffs bringingseemingly non-meritorious malpractice claims also have made repeatedefforts to seek sanctions or damages against plaintiffs' attorneys. 0 Theseefforts, however, also have proven largely unsuccessful.
B. Settlement of Malpractice LitigationTo date, there has been no comprehensive analysis of the settlement
process in malpractice cases either with respect to when settlementstypically occur in the course of the litigation or with respect to the exactfactors which determine whether a settlement will occur at all." It isclear, however, that settlements are common in malpractice cases. Onaverage, about fifty percent of all malpractice lawsuits are settled with theplaintiff receiving a payment.12 Critics of the system suggest that the highcost of malpractice litigation and the unpredictability of the results (1) forcepatients to settle claims for significantly less than the true value of theirclaims, 3 and (2) force physicians to settle claims in which they havemeritorious defenses. 4
In the past, most malpractice insurance contracts provided that thephysician had to consent to settlement prior to the insurer agreeing to acompromise of the claim.' s Now, however, the majority of malpracticeinsurers probably have the right to settle without the physician's consent.As a practical matter, insurers remain interested in complying with aphysician's preference with respect to settlement. The prevailing view is
9. See generally Edward Brunet, The Use and Misuse of Expert Testimony in SummaryJudgment, 22 U.C. DAviS L. REV. 93 (1988).
10. See generally Sheila L. Birnbaum, Physicians Counterattack: Liability of LawyersforInstituting UnjustifiedMedicalMalpractice Actions, 45 FoRDHAML. RE V. 1003 (1977).
11. Cf. Metloff, Researching Litigation, supra note 7, at 199. Among the factors thatmalpractice insurers likely consider in deciding whether to settle are (1) the merits of thecase; (2) the risk of a large damages award should the jury find in favor of the plaintiff; (3)the wishes of the defendant physician as to whether or not to settle; (4) the costs ofproceeding to trial; (5) the quality of the plaintiffs' attorney; (5) the sympathetic qualitiesof the plaintiff; and (6) any unusual facts in the case (such as missing medical records) thatmight influence a jury. Some malpractice insurers may give some of these factors relativelymore weight than other insurers. Id.
12. See generally U.S. GEN. Accr. OFF., MEDIcAL MALPRACIE: CHARACTERISTIcsOF CLAIMS CLOSED IN 1984 (1987) [hereinafter CLAIMS CLOSED IN 1984].
13. WEILER, supra note 1, at 53-54.14. See, e.g., WALTER K. OLSON, THE LTIGAnON EXPxSION: WHAT HAPPENED WHEN
AMERICA UNLEASHED THE LAwsurr 267-68 (1991) (arguing that the merits of the caseconstitute but a minor ingredient in explaining malpractice case results).
15. See Samuel R. Gross & Kent D. Syverud, Getting to No: A Study of SettlementNegotiations and the Selection of Cases for Trial, 90 MICH. L. REv. 319, 361 (1991).
432 [Vol. 9:2

ADR STRATEGIES
that most physicians prefer to litigate to protect their reputation (and toavoid any adverse consequences with disciplinary authorities). 6
Illustration 1 depicts the existing settlement system as a parallel processco-existing with the ongoing formal court procedures. Under the currentregime, litigants are free to consider settlement whenever they so choose.Despite this autonomy, there are a number of predictable "settlementpoints" (shown by the arrows on the settlement line in Illustration 1).These common settlement points include: (1) the pre-litigation period, (asnoted above, settlements are rare during this period in the malpracticecontext); (2) the summary judgment stage; (3) the period immediatelypreceding trial ("on the courthouse steps'); (4) the trial itself; and (5) theappeal stage. The largest number of settlements appear to occurimmediately before trial, often after the parties have incurred sizablelitigation expenses.' 7 Under traditional rules of civil procedure, there areno formal procedural events that require the parties to assess settlement oftheir claim immediately preceding trial. However, many courts have thepower to raise the settlement issue during a pre-trial conference.'
C. The Role of the Jury in Malpractice CasesOne of the most frequent complaints about malpractice litigation is that
the jury is an untrustworthy decision-maker.In fact, the jury resolves only a small percentage (about ten percent) ofmalpractice cases, with the balance either being dropped by the plaintiff orsettled.'
16. See Kent D. Syverud, The Duty to Settle, 76 VA. L. REv. 1113, 1172-73 (1990).It is now widely speculated that settlement of malpractice cases will become more
difficult. In 1990, the federal government began requiring all malpractice insurers to reportany malpractice judgment or settlement to a data bank. Hospitals and other interestedparties will have the right to search the data bank to determine a physician's history withrespect to successful malpractice claims. This process raises serious concerns on the partof physicians as to the possibility that even a single malpractice settlement might impacttheir future ability to obtain hospital privileges and the like. See Ilene D. Johnson, Reportsto the National Practitioner Data Bank, 265 JAMA 407 (1991).
17. For some quantification of the timing of settlements in malpractice cases, seeThomas B. Metzloff, Resolving Malpractice Disputes: Imaging the Jury s Shadow, 54 LAW& Co NrEMP. PROBS., Winter 1991, at 43,59 n.54 [hereinafter Metzloff, Resolving Disputes](noting that about 25% of all malpractice suits in a three-year survey of North Carolinacases were settled immediately preceding a scheduled trial).
18. See FED. R. Crv. P. 16 (noting that one purpose of pre-trial conferences is toconsider prospects for settlement). There is an abundant literature on judicial involvementin the settlement process. See, e.g., Judith Resnik, Managerial Judges, 96 HARV. L. REV.376 (1982); American Law Institute Study on Paths to a "Better Way": Litigation,Alternatives, and Accommodation, 1989 DUKE L.. 811, 819-20. For a criticism of judicialcoercion of settlements, see Owen M. Fiss, Against Settlement, 93 YALE LJ. 1073 (1984).
19. See generally Stephen Daniels & Lori Andrews, The Shadow of the Law: JuryDecisions in Obstetrics and Gynecology Cases, in 2 MEDICAL PROFSSIONAL LIAB=1TY ANDTHE DELIVERY OF OBSTETRICAL CARE 161 (Victoria P. Rostow & Roger J. Bulger eds.,
1992]

ALASKA LAW REVIEW
The key issue is whether juries tend, as some observers suggest, to findin favor of sympathetic plaintiffs regardless of the merits of the case.Contrary to popular perception, most studies of malpractice trials haveshown that, more often than not, physicians prevail and juries arereasonably competent decision-makers, at least with respect to the liabilityissue. Despite the fact that physicians usually win, there is growingconcern with the number of large verdicts in favor of some plaintiffs.
There is a growing consensus, however, that one of the most seriousproblems with malpractice juries is their lack of consistency in awardingdamages.' This raises several questions. First, do malpractice juriesaward amounts comparable to awards for similar injuries in other litigationcontexts, such as automobile accident cases?' Second, are existing juryawards sufficiently predictable to provide a "going rate" for settling othermalpractice disputes?'
1989).The length of malpractice trials varies considerably; recent evidence suggests that the
median trial length is five days, but a significant number of much longer trials exist. SeeMetzloff, Resolving Disputes, supra note 17, at 49-50.
20. Metzloff, Resolving Disputes, supra note 17, at 82-83. This fact by itself is notdeterminative, however, as it is first necessary to know more about why some cases are triedand others dropped or settled. Existing evidence strongly suggests that the trial selectionprocess is far from random. Instead, it is possible that due to insurer unwillingness to settlenon-meritorious malpractice cases, many weak plaintiffs' cases are tried, resulting innumerous pro-defendant results.
21. See generally David J. Nye et al., The Causes of the Medical Malpractice Crisis:An Analysis of Claims Data and Insurance Company Finances, 76 GEO. U. 1495 (1988).
With respect to large jury verdicts, one must also consider the impact of possible post-trial adjustments through various mechanisms such as appeal. Recent evidence suggests thatparticularly large malpractice awards are often reduced, although the specific dynamics ofhow these awards are challenged is not well understood. See Ivy E. Broder, Characteristicsof Million Dollar Awards: Jury Verdicts and Final Disbursements, 11 JUST. SYS. 1. 349(1986); MICHAEL G. SHANLEY & MARK A. PTERSON, POST-TRIAL ADJUSTmN TO JURYAWARDS 27 (1987). While post-trial reductions provide some solace, the evidence does notindicate that the post-trial adjustment process serves as an efficient or reliable "qualitycontrol" check on jury awards. Metzloff, Resolving Disputes, supra note 17, at 87-88;WEMLER, supra note 1, at 48.
22. This criticism is not necessarily directed to juries per so, but can also be targetedat the substantive law of damages which allows substantial discretion by the decision-maker- be it judge or jury - on the appropriate amount to award.
23. See Randall R. Bovbjerg et al., Juries and Justice: Are Malpractice and OtherPersonal Injuries Created Equal?, 54 LAW & CONTEMP. PROBS., Winter 1991, at 5.
24. See, e.g., Randall R. Bovbjerg et al., Valuing Life and Limb in Tort: Scheduling"Pain and Suffering," 83 NW. U. L. REV. 908 (1989). Recent empirical studies demonstrateserious problems in predicting the amount of damages a jury may award, and that this factordoes indeed negatively impact the settlement process. See Metzloff, Resolving Disputes,supra note 17, at 88-93.
A related concern involves the issue of punitive damages. While the evidence suggeststhat punitive damages are rarely awarded in malpractice cases, this fact alone does not meanthat these concerns are insubstantial. Punitive damages are occasionally awarded againsthospitals, often in large amounts. Also, many malpractice plaintiffs, whether they prevailon the claim or not, allege punitive damages, which contributes to the high level of concern
[Vol. 9:2

ADR STRATEGIES
III. THE POTENTIAL BENEFITS OF MALPRACTICE ADR
Numerous commentators have advocated the use of ADR in mal-practice cases. 5 In general, the arguments favoring the use of ADR inthe malpractice context have been based on the six goals briefly outlinedbelow.
A. Use of a More Qualified Decision-MakerMany ADR advocates have questioned the legitimacy of lay juries
deciding complex malpractice disputes and have looked to ADR to providea more qualified decision-maker. Often, specific methods -- such as thescreening panel procedures discussed below -- directly involve medicalprofessionals in the decision-making process. Other approaches rely onusing skilled lawyers with experience in resolving complex claims.
B. Reduction in Litigation CostMalpractice litigation is undoubtedly expensive. The best available
evidence indicates that the costs of litigating malpractice disputes exceedthe amount paid in compensation to injured plaintiffs. ADR is oftenseen as a means to reduce those expenses.
C. Reducing the Trauma of Malpractice LitigationTraditional malpractice litigation takes an emotional toll on the parties,
particularly the doctor accused of malpractice. Physicians perceive the suitas an allegation of almost criminal misconduct; doctors often speak interms of innocence or guilt, despite the fact that a malpractice trial is nota criminal proceedingY ADR methods mitigate this problem by being
exhibited by physician defendants. See Stephen Daniels & Joanne Martin, Myth andRealityin Punitive Damages, 75 MINN. L. REV. 1 (1990).
25. See, e.g., FRAMEWORK FOR ACION, supra note 1, at 30-31 (noting desirability ofevaluating ADR mechanisms for malpractice); Neil D. Schor, Note, Health Care Providersand Alternative Dispute Resolution: Needed Medicine to Combat Medical MalpracticeClaims, 4 OIO ST. J. oN DiSP. RESOL. 65 (1988); Rhoda M. Powsner & FrancesHamermesh, Medical Malpractice Crisis the Second Time Around: Why Not Arbitrate?, 8I. LEGAL MEE). 283 (1987).
26. See Kakalik & Pace, supra note 5, at 41, 54 (noting that costs and expensesincurred by malpractice plaintiffs constituted approximately 36% of the amount recovered,while aggregate defense costs were approximately 30% of the amount awarded incompensation). Certainly, the high costs are a partial function of the use of the jury asdecision-maker. See Metzloff, ResolvingDisputes, supra note 17, at 53-59 (discussing costsassociated with jury trials and noting that more than half of defense expenditures weredirectly related to the trial stage of the case).
27. See F. Patrick Hubbard, The Physicians' Point of View Concerning MedicalMalpractice: A Sociological Perspective on the Symbolic Importance of "Tort Reform," 23
1992]

ALASKA LAW REVIEW
more private and less lengthy, thus diminishing the time the physician mustspend away from her practice 28
D. Improving the Quality of Expert WitnessesThe medical profession and commentators frequently complain about
the low quality of experts who testify on behalf of plaintiffs.?9 In turn,plaintiffs' attorneys note the difficulty in obtaining skilled experts who arewilling to testify against colleagues. Certainly, expert evidence plays acrucial role hi malpractice litigation; in virtually every malpractice case,both parties must have experts to testify as to the applicable standard ofcare. A potential benefit of ADR is altering the method by which expertsare obtained, such as by requiring the use of court-appointed neutralexperts.
E. Handling the Small CaseGiven the expense inherent in litigating a malpractice claim through to
trial, it is commonly perceived that experienced malpractice plaintiffs'attorneys will only consider those claims involving serious injuries andpotentially large damage awards. Certainly, it is more difficult formodestly injured patients to assert a malpractice claim. Accordingly, someview ADR as a less onerous process that will facilitate the assertion ofthese currently excluded claims.
F. Dealing with Frivolous LitigationAs noted above, many commentators are concerned with the apparently
high incidenoe of non-meritorious malpractice suits.3 One possible causeof this problem is inadequate screening of potential malpractice claims.Given the complexity of proving a malpractice case, very few plaintiffs canpursue a claim successfully without the assistance of counsel. It is thuswidely recognized that plaintiffs' attorneys serve a critical gatekeeping
GA. L. REV. 295, 320-23 (1989); WELER, supra note 1, at 6-7.28. The interest in privacy is by no means limited to malpractice defendants. Seriously
injured plaintiffs may prefer the less public setting of aR. For example, the PrivateAdjudication Center at Duke University recently administered a malpractice arbitration ina case in which the plaintiff was a five-year old child suffering from the after-effects of adrug overdose. His parents did not want him to sit through a lengthy trial listening toexperts discuss the nature of his disabilities. The parties agreed that he need not be presentduring the two-day arbitration and that no transcript of the proceedings be made.
29. See PETR W. HUBER, GALILEO'S REVENGT: JUNK SCmNCE IN THE COURTROOM75-91 (1991) (discussing the inconsistent quality of expert testimony in obstetricalmalpractice cases).
30. See supra part lIA.
[Vol. 9:2

ADR STRATEGIES
role. ' While in most states there is a small cadre of highly competentmalpractice attorneys who, as a practical matter, specialize, there are alsonumerous attorneys with little or no malpractice experience whooccasionally accept malpractice cases. This may result in the filing ofmarginal claims by inexperienced attorneys. Accordingly, some suggestthat ADR can provide an early review of the merits of the claim, thusserving as an additional gatekeeping tool.
IV. ANALYZING SPECIFIC ADR OPTIONS FOR MALPRACTICE CASES
As discussed above, there are numerous litigation concerns in themalpractice context which ADR is thought to address. Illustration 2(Appendix B) presents the malpractice time line revised to indicate howvarious ADR techniques would operate within the malpractice context.Although the diagram is not exhaustive of all of the possible ADR methodsthat might be applied to malpractice cases, it does identify those methodsthat have already been applied to malpractice cases or those that areconceptually well suited to such disputes.2 In general, each of the ADRmethods depicted in Illustration 2 establishes a new settlement point basedupon an additional type of input that the parties are to consider.
31. For a useful discussion of the role of plaintiffs' attorneys see Melvin W. Reder,Contingent Fees in Litigation with Special Reference to Medical Malpractice, in THEECONOMICS OF MEDICAL MALPRACTCE 211 (Simon Rottenberg ed., 1978).
32. An important ADR alternative not directly discussed in text is the AmericanMedical Association's ("AMA") bold and controversial administrative plan to transfer allmalpractice disputes from the courts to a specialized administrative tribunal. See AM. MED.ASS'N/SpECIALTY SOCITY MEDICAL LAmBrY PROJECr, A PROPOSED ALTERNATIVE TOTHE CIVIL JUSTICE SYSTEM FOR RESOLVING MEDICAL LIABILrTY DisPurEs: A FAULT-BASED, ADMINISTRATIVE SYSTEM (1988).
While retaining the general tort rules on negligence, the AMA proposal would employan elaborate procedural system involving an initial review and investigation by a claimsprocessor, referral to a neutral expert; assignment of a "court-appointed" attorney;mandatory settlement offers; submission of the dispute to a hearing examiner, and reviewof substantive decisions by an overseeing board. For a more complete description, see KirkB. Johnson et al., A Fault-Based Administrative Alternative for Resolving MedicalMalpractice Claims, 42 VAND. L. REV. 1365 (1989).
While some commentators have expressed interest in the AMA's proposal, others havebeen decidedly negative. Compare WEILER, supra note 1, at 117 (expressing support forthe "AMA's ingeniously designed proposal" which in his view "would likely fare quite wellin any open-minded comparison" with traditional litigation) with J. Douglas Peters, Critiqueof the American Medical Association's Model Medical Liability and Practices Reform Act,1 CTs., HEALTH Sa. & LAW 51 (1990). For an insightful examination of the proposal, seeRandall R. Bovbjerg, Reforming a Proposed Tort Reform: Improving on the AmericanMedical Association's Proposed Administrative Tribunal for Medical Malpractice, 1 Crs.,HEALTH SCi. & LAW 19 (1990). The AMA had hoped that at least a few states wouldadopt the model as an experiment; to date, none have done so.
1992]

ALASKA LAW REVIEW[V.9:
What follows is a brief description of each ADR process depicted inIlustration 2 and an overview of any experiences or empirical studiesrelating to each method in the malpractice context.
A. Risk ManagementHospitals routinely employ risk management programs designed to
monitor and improve the quality of care. This is done primarily in aneffort to minimize iatrogenic injuries suffered by patients by identifyingparticularly risky procedures.?3 Another aspect of risk managementactivity is the prompt identification of any negligently inflicted injuries thatmay occur. To date, however, most hospitals have not aggressivelypursued early identification and resolution of potential malpracticeclaims.34 Accordingly, one available ADR strategy is for hospitals andother health care professionals to become more directly involved in theearly recognition of disputes, before the patient decides to file amalpractice claim. A more active stance could result in early resolution ofdisputes, by placating angry patients before these disputes are transformedinto formal suits.3
B. ArbitrationIn arbitration, the parties agree to use an arbitrator, usually a privately
retained individual, to render the decision in place of a judge or jury.Thus, arbitration is both (1) a voluntary process, in that the parties haveagreed at some point to its use, and (2) a binding process that willconclusively resolve the dispute. In addition, the parties have substantialpower to determine for themselves the particular details of the arbitrationprocedure." As depicted in Illustration 2, parties can agree to arbitrationat several points. Thus, litigants in a malpractice case can voluntarily agreeto submit their claim to binding arbitration in lieu of a jury even after thesuit is filed.37
33. See generally Laura L. Morlock & Faye E. Malitz, Do HospitalRisk ManagementPrograms Make aDifference?:RelationshipsBetweenRiskManagementProgram Activitiesand Hospital Malpractice Claims Experience, 54 LAw & CoNTmMP. PRoBS., Spring 1991,at 1; AM. MED. Ass'N/S ECIALTY SOCiETY MEDICAL LAmBrY PRojEcr, RISKMANAGEMENT PRNCmE & CoMMENrARIEs FOR THE MEDICAL OFFICE (1990).
34. For a discussion of the role of risk management in minimizing potential malpracticeclaims or in improving the handling of such claims, see Orley H. Lindgren et al., MedicalMalpractice Risk Management Early Warning Systems, 54 LAW & CONTEMP. PROBS.,Spring 1991, at 23.
35. Id. at 41.36. Procedural variables relating to the conduct of an arbitration hearing include, among
others: (1) the length of the arbitration hearing; (2) the number of arbitrators; (3) therequired qualification of arbitrators; (4) the process for selecting arbitrators; (5) the amountof discovery permitted to be conducted.
37. Far more problematic, however, is whether the physician and patient can enter into
[Vol. 9:2

ADR STRATEGIES
Currently, the use of arbitration varies widely among litigationcontexts, with some areas, such as securities litigation, dominated byarbitration.3" Legislative action to facilitate the use of arbitration inmalpractice cases was an early tort reform agenda item. Approximatelyfourteen states enacted specific legislation designed to promote malpracticearbitration3 9 Arbitration does not yet play a critical role, however, inresolving medical malpractice cases4° although its potential applicationhas been widely advocated.4'
Empirical research on arbitration's impact on malpractice cases issparse, primarily because so few malpractice cases have been submitted toarbitration. The scant evidence that does exist suggests that the process isnot inherently pro-physician.42 For example, a recent study found thatplaintiffs prevailed slightly more often in arbitration than in traditionallitigation and that the process was less time-consuming.4 3
It is not clear why the use of arbitration has not been more prevalentdespite efforts to facilitate its use. Several explanations deserveconsideration. First, early judicial hostility to the use of arbitration in
a binding arbitration agreement prior to the rendition of the medical services.38. See ShearsonAmerican Express, Inc. v. McMahon, 482 U.S. 220 (1987)
(announcing public policy in favor of arbitration, including consumer disputes againstsecurities dealers); Cf. Gilmer v. InterstateJohnson Lane Corp., 111 S. Ct. 1647 (1991)(upholding arbitration agreement in age discrimination suit).
39. For a useful review of state legislative efforts, see Irving Ladimer & Joel Solomon,Medical Malpractice Arbitration: Laws, Programs, Cases, 653 INS. L. J. 335 (1977). Thefailure of a state to enact a specific malpractice arbitration statute does not preclude the useof arbitration; most states have enacted the Model Arbitration Act, which provides a basisfor claiming a right to enter into an arbitration agreement.
40. According to a 1984 study of malpractice claims closed in that year, only 0.2% ofmalpractice claims were decided following arbitration. CLAIMS CLOSED IN 1984, supra note12, table 2.20, at 37. See generally U.S. GEN. ACCT. OFF., MEDICAL MALmACTICE: FEWCLAIMS RESOLVED THROUGH MtICHIGAN'S VOLUNTARY ARBITRATION PROGRAM 7 (1990)[hereinafter MICHIGAN PROGRAM] (noting that legislation to encourage voluntary bindingarbitration produced only 247 actual arbitrations out of approximately 20,000 malpracticeclaims in a 13 year period).
41. On the use of private contractual approaches such as arbitration to the malpracticeproblem, see Symposium, Medical Malpractice: Can the Private Sector Find Relief?, 49LAW & CONTEMP. PROBS., Spring 1986, at 1.
42. See Irving Ladimer et al., Experience in Medical Malpractice Arbitration, 2 LLEGAL MED. 433 (1981) (finding that arbitration tends to skew results in favor of plaintiffswith severe permanent disabilities as compared to those claimants with minor injuries); seegenerally Stephen Zuckerman et al., Information on Malpractice: A Review of EmpiricalResearch on Major Policy Issues, 49 LAW & CoNTEMP. PROBS., Spring 1986, at 85, 103-06(summarizing available empirical information on arbitration results); Kevin M. Clermont &Theodore Eisenberg, Trial by Jury or Judge: Transcending Empiricism, 77 CORNELL L.REV. 1124, table 3, at 1137 (1992) (finding that malpractice plaintiffs prevailed more oftenin federal court cases tried by the judge than in cases tried to a jury).
43. See MICIRGAN PROGRAM, supra note 40, at 8 (noting that plaintiffs prevailed in22,o of arbitrated cases as compared to 18% in traditional litigation). Surprisingly,however, the GAO study found that the average cost to the litigants of resolving the caseswere comparable, not cheaper as had been expected. Id.
19921

ALASKA LAW REVIEW[.
malpractice cases created an obstacle.0 Second, many of the statutoryprovisions ostensibly designed as consumer protection measures actuallyserve to limit the use of arbitration agreements.45 Third, malpracticeattorneys, both on the plaintiff and defense side, generally are averse toroutine use of arbitration.4 6 The jury is often viewed by both plaintiff anddefense attorneys (and many insurers) as an appropriate "dispute resolver"in many types of malpractice cases, such as those in which there is acritical factual dispute. Fourth, some attorneys believe that arbitrators tendto make compromise decisions that do not fully vindicate their clients'interests. Particularly in the malpractice context, where physicians possessa strong interest in vindicating their conduct, this perception of arbitrators"splitting the baby" represents a potentially significant problem 7 Finally,the lack of interest in arbitration on the part of malpractice insurers mayrepresent a concern that if a truly expedited process for assertingmalpractice claims were established, the number of malpractice claimsasserted would skyrocket.
C. MediationMediation is one of the most overused but misunderstood terms in the
ADR lexicon. Although not susceptible to strict definition, mediation isgenerally a dispute resolution process in which the litigants themselves(and usually their attorneys) meet with an impartial, disinterested mediatorin an attempt to settle the case.48 The mediator's role is primarily tofacilitate the parties' understanding of the nature of the dispute and toexplore practical solutions, even if those solutions are not necessarilyrequired by applicable substantive law principles. Mediation is thought tobe particularly well suited to disputants with a longstanding past
44. See, e.g., Obstetrics & Gynecologists Ltd. v. Pepper, 693 P.2d 1259 (Nev. 1985);Roberts v. McNivnara-Warren Community Hosp., 360 N.W.2d 279 (Mich. Ct. A pp. 1984).See generally Mary Bedikian, Medical Malpractice Arbitration Act: Michigan's Experiencewith Arbitration, 10 AM. LL. & MED. 287 (1984) (reviewing early case law under Michiganarbitration statute).
45. See, e.g., GA. CODE ANN. § 9-9-61 (Supp. 1992) (permitting patient to agree toarbitration only after alleged act of physician negligence has occurred and after consultingwith an attorney).
46. See Nicolas P. Terry, The Technical and Conceptual Flaws of Medical MalpracticeArbitration, 30 ST. Louis U. LJ. 571, 574-75 (1986) (suggesting that "for conceptual andtechnical reasons, malpractice arbitration as currently envisaged is a dangerouslyinappropriate solution to the real or perceived malpractice crisis").
47. See PHYSICIAN INSURERS ASSOCIATION OF AMERICA, A COMPREmNSIVE REVIEWOF ALTERNATIVES TO TBE PRESENr SYSTEM OF RESOLVING MEDICAL LIABILrrY CLAIMS49 (1989) (discussing possible disadvantages to arbitration, including the concern withcompromise results).
48. See generally Lon L. Fuller, Mediation - Its Forms and Functions, 44 S. CAL. L.REV. 305 (1971).
440 [Vol. 9:2

ADR STRATEGIES
relationship who desire or otherwise need to maintain a working, if notnecessarily cordial, future relationship.
Experience with the use of traditional mediation in malpractice casesis very limited.4 9 For several years, Wisconsin has unsuccessfullyemployed a hybrid procedure that is ostensibly labelled as a mediationprocess.50 More recently, a few states have enacted legislationempowering trial court judges to mandate the use of mediation in any civildispute, including malpractice cases!' While these programs were notspecifically designed for malpractice cases, judges have routinely referredmalpractice cases to mediation under these programs. To date, however,there are no empirical evaluations of the results of these hybrid ADRprocesses in the malpractice context.
D. Screening PanelsIn the mid-1970's, a number of states adopted special litigation
procedures for malpractice cases. Commonly called "pre-trial screeningpanels," these early ADR examples usually required plaintiffs to submittheir claims to a special panel (often composed of a physician, attorney,and lay member). The panel would consider the parties' respectivepositions and issue a non-binding decision. In theory, a panel finding ofno liability would induce the plaintiff to drop the claim; a finding ofliability would provide an impetus to defendants to settle. In any event,either party could insist upon trial by jury, although some states made thepanel's finding admissible at the subsequent trial5 2 Recently, severalstates have abolished their screening panel procedures.5 3
49. Professor Leonard L. Riskin at the University of Missouri-Columbia has attemptedto apply traditional mediation techniques to malpractice cases, but the project has beenlimited by the paucity of cases voluntarily referred to this process. See LEONARD L. RISIN,CENTER FOR THE STUDY OF DisPurE RESOLUTION, FINAL REPORT TO THE NATIONALINSTIIUTE FOR DISPUTE RESOLUTION ON INNOVATION FUND GRANT FOR MEDICALMALPRACTICE MEDIATION 7-8 (1992) (on file with author). There are sporadic reports ofsuccessful mediations in individual malpractice cases. See, e.g., Hank De Zutter,Proponents Say ADR Spells Relief, ILL. LEGAL TIMES, Jan. 1988, at 1 (describing successfulmediation of a malpractice case).
50. See Catherine S. Meschievitz, Mediation and Medical Malpractice: Problems withDefinition and Implementation, 54 LAW & CONTEMP. PROBS., Winter 1991, at 195 (notingseveral problems relating to a hybrid mediation process in Wisconsin). In fact, theWisconsin process is probably more aptly described as a variant on the screening-panelmodel rather than a mediation procedure given the lack of mediation training among thepanel members and the lack of discussion among the disputants. Id. at 211-12; see infrapart IV.D.
51. See, e.g., FLA. STAT. ANN. § 44.1011-106 (West Supp. 1992).52. For a comprehensive overview of the screening panel procedures, see Jean A.
Macchiaroli, Medical Malpractice Screening Panels: Proposed Model Legislation to CureJudicial Ills, 58 GEO. WASH. L. REv. 181 (1990).
53. See, e.g., Debra L. Fortenberry, Note, Screening Panels: Corrective Surgery or
1992]

ALASKA LAW REVIEW
The most common criticism of the panels is that they areadministratively cumbersome and that they sometimes lead to longdelays. "' Other concerns are that the process may come too early in theevolution of the claim before the parties have conducted sufficientinvestigation. Other commentators continue to express support for thisADR approach.-1 Existing empirical studies are generally mixed, withsome indications that screening panels do indeed screen out low-meritcases, but perhaps only because more claimants elect to assert a claimbefore the panels.5 6
E. Early Neutral Evaluation and Court-Ordered ArbitrationOne rapidly growing area in the ADR field is the development of
court-sponsored ADR programs. Concerned with burgeoning dockets,numerous state and federal courts have initiated mandatory, but non-binding, ADR processes. Two of these initiatives are potentially wellsuited to malpractice.
Early neutral evaluation (Number 5 in Illustration 2) calls for the earlyassessment of the case by an experienced neutral attorney on the basis ofbrief presentations by the parties.7 Ordinarily, the evaluator is a skilledlitigator with experience in the particular type of case in dispute. Thetheory is that the parties will benefit by the evaluator's neutral assessmentof the value of the case and therefore reconsider their positions. If the casedoes not settle, the evaluation is usually kept confidential5 8 As shown,this ADR intervention occurs relatively early in the dispute, after theparties have had some time to conduct discovery on key issues, but before
Amputation, 4 J. Dis,. RES. 255,259-62 (1989) (discussing repeal of Ohio screening panel);Jona Goldschmidt, Where Have All the Panels Gone?: A History of the Arizona MedicalLiability Review Panel, 23 ARIZ. ST. LJ. 1013 (1992).
54. See, e.g., WEILER, supra note 1, at 42 (suggesting that screening panels are "fraughtwith difficulty" and describing several practical problems with screening panels includingdelay and imposition of additional expense).
55. See Macchiaroli, supra note 52, at 239-49.56. Useful empirical studies include J. MARDFMN, MEDICAL MALPRACTICE IN THE STATE
OF HAWAII (1986) (discussing experiences with Hawaii screening panel system); StephenShmanske & Tina Stevens, The Performance of Medical Malpractice Review Panels, 11 J.HEALTH POL., POL'Y & L. 525 (1986).
For an in-depth discussion of Alaska's medical malpractice advisory panel, see supraJonathan S. Aronae, Note, Alaska's Medical Malpractice Expert advisory Panel: Assessingthe Prognosis, 9 ALASKA L. REV. 401 (1992).
57. See Wayne D. Brazil, A Close Look at Three Court Sponsored ADR Programs: WhyThey Exist, How They Operate, What They Deliver, and Whether They Threaten ImportantValues, 1990 U. CH. LEGAL F. 303, 334-35. Brazil explains that a typical case presentationis perhaps 15 minutes in length and entails an explanation of the parties' legal theories aswell as short description of the evidence that supports each theory. Id. at 335.
58. A secondary goal is for the evaluator to assist the parties in focusing discoveryshould the case not settle. Id. at 336-37.
[Vol. 9:2

ADR STRATEGIES
the bulk of expenditures have been made. To date, formal early-neutralevaluation programs have been limited to the federal courts. Becausemalpractice cases most often arise in state courts, there is no evidence asto how well this model would work in the malpractice context 9
Court-ordered arbitration (Number 6 in Illustration 2) is a process inwhich certain disputes are channelled to a non-binding arbitration processfollowing the completion of designated period of discovery. As with theother ADR methods, the details of how specific programs operate variessubstantially?6 This particular ADR method originated in the state courtsin the mid-1950's and was targeted at minor disputes. After a period ofslow or no growth in the use of this process, a wave of states adoptedcourt-ordered arbitration programs during the 1980'S.61 The federal courtfollowed suit with the initiation of experimental arbitration programs.62
While programs vary, the following example presents a typicalapproach, based upon the program in effect in the Middle District of NorthCarolina.6 3 After suit is filed and the case is determined eligible for theADR program, the parties are given three months to conduct discovery.The parties are urged to agree upon the selection of a single arbitrator froma list of experienced attorneys prepared by the court.6 If they are unableto agree, one is appointed for them. The arbitrator is paid by the court atthe maximum rate of $500 per case. The rules anticipate a pre-hearingexchange of information relating to such factors as the identity of witnesseswho will testify at the hearing and the documents that will be produced.The rules do not establish a maximum length for the hearing, but onaverage the hearings last approximately seven hours.65 The arbitratormust issue an award within fifteen days of the hearing. Following thedecision, either party may request a trial de novo; however, before
59. Early neutral evaluation was pioneered in the United States District Court for theNorthern District of California. For a brief history of the development of the early neutralevaluation model in that court, see David J. Levine, Northern District of California AdoptsEarly Neutral Evaluation to Expedite Dispute Resolution, 72 JUDICATURE 235 (1989).
60. For an excellent overview of characteristics and performance in federal court-ordered arbitration programs, see BARBARA S. MEMRHOEFER, FED. JUD. CENTER, COURT-ANNEXED ARBrrRATION IN TEN DISTRICT COURTS (1990).
61. On the history of the growth in state court programs, see Susan Keilitz et al., StateAdoption of Alternative Dispute Resolution, 12 STATE CT. J., Spring 1988, at 4.
62. See Paul Nejelski & Andrew S. Zeldin, Court Annexed Arbitration in the FederalCourts: The Philadelphia Story, 42 MD. L. REV. 787 (1983).
63. E. ALLAN LIND, ARBITRATING HIGH-STAiEs CASES: AN EVALUATION OF COURT-ANNEXED ARBrRATION IN A UNITED STATES DismTR COURT (1990) (containing copy ofthe local rules controlling the North Carolina federal court's court-ordered arbitrationprogram).
64. The rules require that the arbitrator have been a member of the state bar for at leasteight years and be determined by the court to be competent to perform the duties of anarbitrator. Id. at 77.
65. Id. at 30-31.
19921

ALASKA LAW REVIEW
proceeding with a conventional trial, the parties must confer with thearbitrator to discuss his or her assessments of the case in an effort toachieve a settlement.66 If the case proceeds to trial, no evidence relatingto the court-ordered arbitration results is admissible.'
To date, few malpractice cases have been subjected to court-orderedarbitration. In state courts, programs typically have a jurisdictional capproviding that only cases involving less than a certain amount incontroversy (such as $25,000) go through the process. At thejurisdictionalamount levels commonly in effect, virtually no malpractice cases areeligible. The federal court programs, however, target higher value cases(up to $150,000 in the Middle District of North Carolina) and, as a result,some malpractice cases have been covered. 68
In contrast to many of the other ADR programs described in thiscomment, court-ordered arbitration programs have been subjected tointensive empirical scrutiny. The results of the studies vary in theiranalysis of the programs' effectiveness. In general, the evidence supportsthe view that litigants are well satisfied with court-ordered arbitration andthat the process does result in more expeditious resolution of claims.69 Ofcourse, a key element in determining the success of a program is how wellthe program is administered at the state level.70
F. The Summary Jury Trial and Its VariationsThe summary jury trial ("SJT') is a relatively new ADR process, first
used in 1980 by a federal judge in Ohio.7' To date, it has been usedregularly only in scattered federal district courts, although several state
66. Id. at 84.67. Id.68. Metzloff, Researching Litigation, supra note 7, at 225 n.82.69. See, e.g., Stevens H. Clarke et al., Court-Ordered Arbitration in North Carolina:
Case Outcomes and Litigant Satisfaction, 14 JUST. SYs. . 154 (1991) (discussing resultsof study using random assignment of cases which indicated high levels of party satisfactionand reduced case disposition times for North Carolina state court program); E. ALLAN LMET AL., THE PERCEPTION OF JusICu: TORT LrIGANrS' ViEws OF TRIAL, CouRT-ANNExEDARBITRATION, mrD JUDICIAL SETILEMENr CONFERENCES (1989); Lind, supra note 63,(evaluating performance of court-ordered arbitration program for the federal district courtfor the Middle District of North Carolina); see generally Deborah R. Hensler, What WeKnow and Don't Know About Court-Administered Arbitration, 69 JUDICAlURE 270 (1986).
70. Clarke, supra note 69, at 181-82 (noting that the North Carolina state court programwas planned and managed with great care" and that a different program "lacking this kind
of planning and management might not work as well").71. See, e.g., Thomas D. Lambros, The Federal Rules of Civil Procedure: A New
Adversarial Model for a New Era, 50 U. PIT. L. REv. 789, 798-804 (1989); D. MARIMPROVIE, Fn. JuD. CENTER, SETrLEMENr STRATEGIES FOR FEDERAL Disrucr JUDGES 68-76 (1986). For an interesting critique of the SJT process, see Joan K. Archer Rowland,Comment, Communication and Psychology Variables: Reasons to Reject the Summary JuryTrial as an Alternate Dispute Resolution Technique, 39 KAN. L. REV. 1071 (1991).
444 [Vol. 9:2

ADR STRATEGIES
courts have recently begun experimenting with the process. Because of itsfederal court origins, only a few malpractice cases (which are usually filedin state courts) have been subjected to SJTsZ The process is usuallyvoluntary, although a few judges have attempted to require partyparticipation.!
3
The theory of the SJT is that in cases headed for a lengthy trial, theparties would benefit by having a summary or preview of the casepresented to a jury for an advisory verdict. The presentation would begreatly expedited compared to a normal trial; cases that might take severalweeks to try in a traditional fashion would be presented in the SJT settingin a day. This efficiency is achieved by taking various shortcuts, mostnotably having the lawyers summarize the evidence in lieu of witnesstestimony. In theory, the summary jury's verdict will aid the parties inreaching a voluntary settlement.
Evidence of the SJT's efficacy is mixed! 4 Researchers have haddifficulty designing empirically sound studies of the process primarilybecause its voluntary nature precludes the use of random assignment ofcases to control groups to create valid comparative studies.75
While proponents of the SyT generally claim that the process is wellsuited to personal injury suits such as medical malpractice, there are, infact, serious reasons to question its application.76 Some malpractice casesturn on factual issues that are better resolved after the jury has had a fullopportunity to assess witness credibility. Other cases turn on complexexpert evidence that is not easily or fairly summarized in so brief a fashion.Other malpractice cases are tried conventionally in only a few days and arethus not good candidates for the SJT process, which is usually targeted atcases that require a week or more to litigate. While on a case-by-case basisthe SJT might be suitable for particular malpractice disputes, it is unlikelythat it represents a plausible alternative in the majority of malpracticeactions.
72. For one of the few malpractice cases that is reported to have used the process, seeLockhart v. Patel, 115 F.R.D. 44 (E.D. Ky. 1987).
73. The Seventh Circuit has held that federal district courts cannot mandate the use ofsummary jury trials. Strandell v. Jackson County, 838 F.2d 884 (7th Cir. 1988). Numerousdistrict courts in other circuits, however, have held that they have such power. See, e.g.,McKay v. Ashland Oil, Inc., 120 F.R.D. 43 (E.D. Ky. 1988).
74. For existing studies, see M. DANIEL JAcouBovrrCH & CARL M. MOORE, FED. JUD.CENTER, SUMMARY JURY TRIALS IN TH-E NORTHERN DISTcr OF OHIO (1982); James J.Alfini, Summary Jury Trials in State and Federal Courts: A Comparative Analysis of thePerceptions of Participating Lawyers, 4 OHIO ST. I. ON DISP. RESOL 213 (1989)(describing research study of state and federal court SIT programs in Florida).
75. See Richard A. Posner, The Summary Jury Trial and Other Methods of AlternativeDispute Resolution: Some Cautionary Observations, 53 U. CQ. L. REv. 366,374-75 (1986).
76. See Thomas B. Metzloff, Reconfiguring the Summary Jury Trial, 41 DUKE LJ. 806,841-50 (1992) [hereinafter Metzloff, Summary Jury Trial].
1992] 445

ALASKA LAW REVIEW
There also exists a-potentially important variation on the SJT, whichutilizes some of its techniques in a binding procedure, which is referred toin Illustration 2 as a "jury-determined settlement"77 In this process, thelitigants agree to a shortened trial usually after negotiating an agreementthat specifies the range within which the parties are willing to settle. Thesummary jury's decision determines the precise amount of the settlementwithin the confines of the parties' "high/low" agreement. To date, severallarge malpractice cases have utilized this hybrid process in North Carolinawhere the state court rules are expressly designed to facilitate bindingSJTs. 8 Because the parties must agree on the settlement parameters, thisprocess is necessarily voluntary and cannot be mandated by a court. It isessentially an ADR process to limit the parties' litigation risk both bysetting appropriate limits on the result (in lieu of the unpredictable juryprocess) and by lowering litigation expenses.
V. DETERMINING A MALPRACTICE ADR STRATEGY FOR ALASKA
Having canvassed several potential ADR choices, the final matter is todevelop a strategy as to which specific ADR initiatives should be pursuedand in what fashion. For several reasons, this is not a simple task. First,it is clear that ADR program performance is a function not just of the typeof process used but of how it is administered. Accordingly, the manner inwhich a program is implemented may be as important as which process ischosen; certainly, administration issues must be carefully attended to duringthe planning process. Also, many ADR methods have not been directlyapplied to complex litigation such as malpractice disputes, and thus thereis little or no empirical evidence as to how those processes will workwithin that context. 9
In developing an informed ADR strategy for a particular litigationcontext, it is necessary to establish desired criteria. This comment offersfive goals for a malpractice ADR system, as well as four ADR strategiesthat achieve such goals."
77. Id. at 850-65.78. Id. at 852-53. For a description of some of the North Carolina cases, see THOMAS
B. METZLOFF ET AL., SUMMARY JURIES IN THE NORTH CAROLNA STATE COURT SYSTEM19-28 (1991).
79. See generally Edward Brunet Questioning the Quality of Alternate DisputeResolution, 62 TOL. L. REv. 1 (1987).
80. Even a cursory examination of attributes of some of the existing ADR optionssuggests that they are not appropriate ADR solutions for the bulk of malpractice disputes.For example, the summary jury trial does not appear well suited to accomplishing thesegoals. By continuing to employ a jury, the SJT does not address the concern of having askilled decision-maker or the problem of inconsistency in awarding damages. Second, byoccurring so late in the process (usually in the period immediately preceding trial), it does
[Vol. 9:2

ADR STRATEGIES
A. The Goals of a Malpractice ADR System1. A Malpractice ADR System Should Be Designed to Produce
Decisions on the Merits, Not to Promote Compromise Settlements.Because of state and federal requirements to report all malpracticesettlements for disciplinary and reporting purposes, no system that tries tocoerce nuisance value settlements is likely to achieve general acceptanceamong malpractice insurers or physicians.
2. A Malpractice ADR System Should Be Focused in Part upon EarlyIdentification of Non-Meritorious Claims. There is substantial evidenceregarding the high frequency of weak or non-meritorious claims in themalpractice context. Accordingly, an ADR system must be cognizant ofthe medical profession's interest in minimizing the expense and disruptiveimpact caused by the assertion of marginal claims.
3. A Malpractice ADR System Should Utilize Decision-Makers Skilledin Understanding Complex Medical Evidence Within the Existing LegalFramework for Assessing Liability and Awarding Damages. Malpracticecases regularly involve complex medical issues relating to both thestandard of care and causation. Accordingly, an ADR system shouldprovide decision-makers who are knowledgeable in the types of medicalissues that may arise. This does not necessarily mean that the system mustemploy physicians in the role of decision-makers. The negligence standardto be applied involves the application of both legal and medical elements.Thus, experienced attorneys may be well suited for this role.
4. A Malpractice ADR System Should Be Designed to PromoteConsistency in the Award of Damages. Strong evidence demonstrates theinconsistency in malpractice damage awards."' Absent substantive lawchanges to address the problems noted, an ADR system must make aconcerted effort to apply the existing law of damages in as rational amanner as possible. This would serve the goals of both equity andpredictability.
not offer significant cost reductions. See Metzloff, Summary Jury Trial, supra note 76, at843-44 (discussing the lack of potential for meaningful cost savings associated with the useof summary jury trials in malpractice cases). This does not mean that the ST is necessarilyinappropriate for all cases; rather, it suggests that it should not be put forward as a routineor mandatory ADR process for handling malpractice disputes generally.
81. See supra note 24 and accompanying text.
19921

ALASKA LAW REVIEW
5. A Malpractice ADR System Should Be Designed to Reduce the Costof Litigation Significantly Through an Efficiently Administered System.The overall transaction costs associated with malpractice litigation areextraordinarily high. As a result, any ADR system must be designed toreduce litigation expenses, at least for the majority of cases to which it willbe applied.
B. ADR Strategies for the Malpractice Context1. Use of Voluntary ADR. One approach would be to rely primarily on
the voluntary efforts of litigants and malpractice insurers to use particularADR methods in appropriate cases. For the past four years, the PrivateAdjudication Center, a non-profit affiliate of the Duke University Schoolof Law, has been providing ADR consulting services to malpracticelitigants on a case-by-case basis with some success.' The largestmalpractice insurer in North Carolina has commented favorably on this useof ADR, noting that even the consideration of litigation alternatives hasassisted it in settling several cases.'
A major advantage of a voluntary approach is its ability to utilize anyof the different ADR methods discussed in part mH. Clearly, each of thedifferent procedures may be better suited to certain types of malpracticedisputes. Thus, realizing the full benefits of ADR requires a carefulmatching of specific malpractice disputes with the particular ADR processbest suited to that case.84 Also, it may be that there are some malpracticecases best suited to traditional litigation, and that any mandatory referralto a particular ADR process will result in increased litigation expenses.The importance of carefully matching ADR procedures with particulardisputes might work best under the case-by-case assessment inherent in avoluntary approach. If a state were to enact some form of mandatoryADR, policy-makers should be cognizant of the litigants' legitimate interestin agreeing to alternative ADR methods in appropriate cases. Thus, any
82. As part of the duties as the Director of the Private Adjudication Center's MedicalMalpractice ADR program, this author regularly consults with malpractice insurers,hospitals, plaintiffs attorneys, and defense attorneys about the use of various ADR methodsin specific malpractice cases. Since its inception in 1988, the program has used or observedthe use of several of the different ADR methods discussed in this comment, includingvoluntary mediation, several forms of binding arbitrations, court-ordered mediation, court-ordered arbitration and binding summary jury trials.
83. See MEDICAL MutruAL INSURANCE COMPANY OF NORTH CAROLINA, 1990 ANNuALREPORT 7 (1990) ('We have found that simply proposing alternative dispute resolution oftengets the discussion going again, which leads to settlements in cases that might otherwise goto court.").
84. Cf. Maurice Rosenberg, Resolving Disputes Differently: Adieu to AdversaryJustice?, 21 CREIGHTON L. REv. 801, 809 (1988) ("[Tlhe ideal system will requiredeploying a whole battery of dispute-resolving mechanisms, various directed, variouslydriven and variously employed.).
448 [Vol. 9:2

ADR STRATEGIES
mandatory program should offer litigants the opportunity to select adifferent ADR method.
Nonetheless, there are several drawbacks to avoluntary ADR approach.The main problem is the fact that in a voluntary system, one party mayblock the use of ADR regardless of how well suited the case. 5 Obtainingan agreement to use ADR in even a simple malpractice case requires theconsent of five different parties: (1) the plaintiff- (2) plaintiffs' counsel;(3) the defendant; (4) defense counsel; and (5) the malpractice insurer.These actors may have divergent interests that impact their views on theutility of ADR either in general or for their specific case. Reachingagreement becomes even more difficult if the case involves multipledefendants. Likewise, if different malpractice insurers are involved, avoluntary consensus agreement on a particular ADR approach could benearly impossible to obtain.
Second, even if all the parties agree that ADR should be used,substantial negotiations are often required as to what specific form shouldbe used. Spending time negotiating the alternative ground rules defeats oneof the principle benefits of ADR, that of efficiency. Third, certain ADRoptions, such as court-ordered arbitration, depend upon the courtestablishing the procedural rules to govern the process and administrate theprogram. A court is less likely to establish a program without assurancesthat it will be used.
2. Facilitating Private Arbitration. A second approach would be tofoster the development of private arbitration agreements between healthcare providers and patients. A well designed and administered arbitrationprocess provides several advantages over traditional litigation. The primarybenefits include the quality of the decision-maker and the speed ofresolution (with its attendant potential reduction in litigation expenses).These benefits accrue both to physicians and potential claimants whocurrently are often unable to access the system because of its exceptionallyhigh administrative costs. An arbitration program with appropriateselection criteria for arbitrators would be as likely to generate reliable andconsistent results.
The malpractice arbitration statutes enacted during the 1970's wereostensibly designed to facilitate the use of arbitration, but in retrospect,
85. Existing empirical studies have regularly shown low levels of utilization forvoluntary ADR programs, which is probably attributable either to attorney or litigantunfamiliarity with the processes involved, the economic motivation of attorneys to maintainthe status quo, or the adversarial nature of litigation. See Sally E. Merry & Susan S. Silbey,What Do Plaintiffs Want? Reexamining the Concept ofDispute, 9 JUST. SYS. J. 151, 151-53(1984); Dwight Golann, Making Alternative Dispute Resolution Mandatory: TheConstitutional Issues, 68 OR. L. REv. 487, 488 (1989).
19921 449
ALASKA LAW REVIEW
their encouragement is minimal. By requiring extensive disclosure topatients, by prohibiting physicians from conditioning the provision ofmedical services on the signing of an agreement and by mandatingprocedurally cumbersome arbitration rules, these statutes - especially inlight of strict judicial scrutiny of any agreements that were employed --have virtually insured that few physicians would even attempt to enter intoarbitration contracts with their patients.
If binding arbitration is desirable (this author believes it is) there is aneed for a new generation of malpractice arbitration statutes that moredirectly promote the use of arbitration. Such new statutes would: (1)reduce the disclosures that a physician has to make to a patient; (2) permitphysicians to make acceptance of arbitration a condition for renderingservices; and (3) allow greater flexibility to the parties to design lesscumbersome arbitration procedures.
At first blush, such a statute would seem contrary to the patient'sinterests, and as a result politically unfeasible. This view is myopic. Thekey issue in terms of protecting patient interest is not pre-agreementdisclosures and warnings, but providing statutory safeguards to ensure thequality and neutrality of the arbitration procedure itself. On this point, themost important factors are the neutrality and qualifications of thearbitrator.86 Assuming an arbitration process that is fair to both patientand physician, there is no reason to restrict its use in malpractice simplybecause it is the physician who takes the initiative in seeing that anarbitration agreement is in place.
If a new statute were enacted, it remains unclear how many physicianswould take advantage of such a provision. Especially for individualphysicians, it is uncomfortable to discuss the prospects for a potentialmalpractice claim with a patient. Moreover, plaintiffs' attorneys, at leastin some cases, would be likely to attempt to challenge arbitrationagreements on a case-by-case basis.
86. Some of the issues relating to the development of a fair and comprehensivearbitration scheme have been addressed in recent federal legislative proposals. One of themost innovative was a proposal by Senator Peter Domenici (R. New Mexico) that wouldrequire the use of arbitration in most malpractice cases. Under the proposed legislation, allmedical malpractice cases would have been resolved through arbitration (or another ADRprocess voluntarily agreed to by the parties) administered by one of several certifled ADRproviders. The bill set forth specific qualifications for what attributes a certified ADRprovider must possess. A summary of the proposed statute and a discussion of itsimplications for ADR providers is provided in Clark C. Havighurst & Thomas B. Metzloff,S. 1232 - A Late Entry in the Race for Malpractice Reform, 54 LAW & CONTEMP. PROBS.,Spring 1991, at 179. A major difference between the mid-1970's and the current situationis the growth in private ADR providers. Numerous entities have either entered or expandedtheir operations in providing ADR services to disputants. Unquestionably, many of theseorganizations would be interested in establishing a malpractice arbitration program ifsufficient demand existed.
[Vol. 9:2

ADR STRATEGIES
3. Development ofMediation-Based Programs. Another approach wouldbe to require malpractice litigants to submit their claims to mediation. Inthis author's opinion, a mediation-based approach is inappropriate for themajority of malpractice cases. A mediation approach makes sense,however, if one assumes that malpractice litigants commonly havelitigation goals other than to obtain compensation for their injuries. Indeed,in some percentage of malpractice cases, the plaintiff has filed the lawsuitout of anger at the physician or hospital. In those cases, a mediationsession designed to explore the plaintiff's anger and aimed at elicitingappropriate recognition of that emotion by the defendants could well beproductive. To be sure, there are malpractice cases that do involve thisdynamic; s7 on a limited case-by-case basis, mediation should beconsidered as an ADR option.88
4. Applying the Court-Ordered Arbitration Model to Malpractice.This author believes that the optimal ADR strategy would be to apply thecourt-ordered arbitration model. As an initial matter, court-orderedarbitration has the advantage of being well established in other litigationcontexts and constitutional.89
The court-ordered arbitration model meets the established criteria inevery respect. First, among all ADR options, an arbitration process (be itbinding or non-binding) is least "settlement' oriented and more focusedupon making decisions on the merits of the case according to controlling
87. For example, the Private Adjudication Center has conducted a few mediations inmedical malpractice cases, one of which involved a classic dispute of the type described intext.
88. In this author's experience, such cases represent the clear minority of malpracticedisputes. For the large majority of claims, the parties desire a decision on the merits of thenegligence claim.
A variation is the mandatory "mediated settlement conference" approach now used insome states. At this point, it is too early in the development of this process to assess itspotential applicability to malpractice.
As currently formulated, there are several potential concerns. First, the mediators' roleas a practical matter is to create pressures on both parties to settle. As noted, malpracticedefendants have a legitimate interest in refusing to settle non-meritorious claims. Also, itis clear that there is a significant amount of non-meritorious malpractice litigation. Themediation approach, by seeking settlements in all cases, may not be well suited to the needin malpractice cases to identify non-meritorious claims. Second, there is a serious questionas to the overall quality of the mediators serving in these programs. Since these programsare applied to a wide variety of civil cases and not just malpractice disputes, few of themediators have experience in handling malpractice disputes. As such, the programs raiseserious concerns about the special interest in malpractice cases of employing skilled ADRneutrals.
In other respects, a mediated settlement conference meets the established criteria in thatit is a simple procedure to administer, and it occurs early in the litigation process, thusoffering signicant cost savings if successful.
89. See generally Golann, supra note 85, at 565.
1992]

ALASKA LAW REVIEW
legal principles, thus making it responsive to the first criterion. Arbitratorsin court-ordered arbitration programs are not expected to assist the partiesin reaching a compromise solution; rather, their function is to make aninformed decision based upon the parties' presentations. As such, theprocess is also well suited among the ADR alternatives for identifying non-meritorious cases, thus qualifying under the second criterion.
Third, a court-ordered arbitration program would employ only skilleddecision-makers. As noted, most programs currently use experiencedattorneys with expertise in a variety of litigation contexts because thoseprograms cover various types of litigation. If the program were focused onmalpractice disputes, special selection criteria could ensure the quality ofthe arbitrators under the third criterion. Skilled arbitrators wouldpredictably be well suited to make consistent damage awards to the extentpossible under the current law of damages, as set forth in the fourthcriterion.
Finally, while other ADR options perhaps offer greater potentialsavings because they operate earlier in the litigation process, court-orderedarbitration occurs at an appropriate time in the development of the suit.The arbitration is held only after the parties have had a reasonableopportunity to conduct some discovery, thus avoiding an acknowledgedproblem of pre-trial screening panels, such as in Alaska. By the sametoken, the hearing should occur less than a year from the filing of theclaim, thus significantly reducing the current disposition time of mostmalpractice disputes. Overall, this particular ADR intervention pointbalances the interest in early intervention with the interest in having thedispute sufficiently developed, so that a valid decision on the merits can bemade.
As noted above, a key factor in recognizing the benefits of court-ordered arbitration is effective design and implementation of the program.While theoretically well suited to the task, existing court-ordered arbitrationprograms, which are currently targeted at a general array of smaller stakescases, may need to be restructured to maximize their potential utility formalpractice. Possible changes include: (1) specialized methods forselecting arbitrators to serve in the program; (2) development ofappropriate discovery rules; and (3) design of an arbitration format suitedto the malpractice context
VI. MALPRACTICE ADR AND ALASKA
Alaska has two statutory provisions impacting the use of ADR inmalpractice cases. First, it has an elaborate -- and controversial -- expert
452 [Vol. 9:2

ADR STRATEGIES
screening panel procedure.90 In light of the descriptions provided in partm, the Alaska panel system is a hybrid. Although commonly referred toas a screening panel, the Alaska process differs from the panels enactedelsewhere in that it operates not as a pre-trial review system, but ratheronly with respect to claims in which lawsuits have already been filed.Moreover, the panel is composed exclusively of medical professionals,unlike the usual mix of physician, lawyer, and lay members utilized inother states. Finally, the panel's task is not to decide the case, but ratherto offer a neutral expert opinion. In fact, in terms of the ADR categoriesshown in Illustration 2, the process is probably more akin to an earlyneutral evaluation process focused solely on the issues of theappropriateness of the medical care rendered. In short, the panel systemis best characterized as requiring the court appointment of neutral experts.
Alaska also has in place an arbitration statute ostensibly designed tofacilitate the use of private arbitration.9 ' In fact, however, none of thosefamiliar with malpractice litigation are aware of any claim resolvedpursuant to an arbitration agreement under the auspices of this statute.Accordingly, for whatever reason, the malpractice arbitration statute hashad no impact on the resolution of malpractice claims in Alaska.
As discussed above, an appropriate ADR strategy is to attempt toreinvigorate the use of private arbitration agreements. In Alaska, at aminimum, this would require removing or scaling back some of thedisclosure requirements which interfere with physicians and patientsentering into a binding arbitration contract, substituting in their placemeasures to insure the quality of the arbitration process. As noted, thiseffort is unlikely in the short-term to radically transform malpracticelitigation. Many physicians will continue to elect not to offer thearbitration option to patients. Moreover, unless the Alaska Legislature iswilling to permit physicians to require patients to sign such agreements asa condition of receipt of services (which is probably politically unlikely, inlight of the serious concerns with access to health care in Alaska), aconsiderable number of patients will continue to refuse to sign arbitrationagreements. Thus, while a revised, more pro-arbitration, statute is neededin order to recognize the benefits that this process offers both patients andphysicians, this change by itself is likely to have only marginal short-termimpact.
Fundamentally reconstructing the expert panel system will have asignificantly greater influence. It is clear that there are several practicalproblems associated with the administration of the expert panels. It is
90. ALASKA STAT. § 09.55.536 (Supp. 1992). A detailed description of the expert panelsystem is contained in Aronie, supra note 56.
91. ALASKA STAT. § 09.55.535 (Supp. 1992).
1992]

ALASKA LAW REVIEWV
becoming increasingly difficult to form the three-member panels. 2
Alaska has a small physician pool, and many have potentially disqualifyingconflicts that prevent them from serving on panels involving their businesspartners or close friends. As currently operated, the panels, either owingto the difficulty of formation or the scheduling of meetings, are delayingthe resolution of claims. Also, inconsistent quality of the panel reports iscasting a cloud over the reliability of the process.
As noted above, the best suited ADR option for Alaska is the court-ordered arbitration model. Requiring malpractice cases to be submitted toa mandatory but non-binding process offers significant promise forachieving the goals set forth above.
The court-ordered arbitration model proposed for Alaska is based uponthe federal court program described in part mI.E. The essential elementsof the proposal include: (1) providing an appropriate period for the partiesto conduct discovery, (2) developing a qualified list of attorney arbitratorsskilled in tort litigation;9 (3) allowing for party choice in selecting thearbitrator for the non-binding arbitration from among the group of qualifiedarbitrators; (4) requiring pre-hearing exchange of information; (5)conducting a hearing of sufficient length to permit fair exchange of theissues in the case;95 (6) preparing a reasoned decision to assist the partiesin resolving the case; and (7) providing either party the opportunity to seektrial de novo, perhaps allowing the arbitrator's decision to be admissible atthe subsequent trialY6
92. See Aronie, supra note 56, at 419.93. Id. at 418.94. The list need not be long. It would appear from various insurance and litigation
sources that there are about 40 medical malpractice cases filed per year in Alaska.Experience from other court-ordered arbitration programs has shown that a fair number ofsettlements or dismissals occur prior to the scheduling of the arbitration hearing. Thus, onaverage, it may be necessary to conduct 30 arbitration hearings a year. A small but highlyqualified group of five to ten arbitrators would be sufficient to handle this caseload. Usinga smaller, carefully selected group of arbitrators rather than a larger list makes it easier totrain the group in how to conduct the sessions and permits the court to be more selectivein terms of desired qualifications.
95. Based upon this author's experience in administering arbitrations in malpracticecases, there is no one time period that is perfectly suited to a malpractice dispute. ThePrivate Adjudication Center has conducted arbitrations as short as two hours where the issueinvolved simply determining a plaintiff's damages in a case in which the physician-defendant had accepted responsibility for the injury. On the other extreme was a two anda half day arbitration involving a complex causation and damage issue following a drugoverdose. The court-ordered arbitration rules should provide for the arbitrator to establishthe length following a presentation by the parties on the nature of the issues involved in thecase. In general, one day would be sufficient for the majority of malpractice cases. Therules should also provide a maximum of two or three days. It should also be possible insome cases for the hearing to last a half day or less.
96. Ordinarily, arbitrations do not result in a formal explanation of the arbitrator'sdecision; rather, an award is simply announced. This orientation, however, is not required.It makes more sense in this context to ask the arbitrator to explain briefly his or her
[Vol. 9:2

ADR STRATEGIES
The opportunity also exists in Alaska to incorporate a modified versionof the current expert panel system into the proposed court-orderedarbitration program. The power to use court-appointed experts is wellestablished.' In connection with the proposed arbitration procedure, thecourt could also appoint a neutral medical expert who would testify duringthe non-binding arbitration hearing, thus serving the same function as thatserved by the current panel. In order to overcome the administrative delaysassociated with the current panel procedure, the number of experts involvedshould be reduced from three to one.9"
VII. CONCLUSION
Procedural reform by itself is unlikely to solve the perceived problemswith our malpractice litigation system. Nonetheless, the increased use ofADR offers much promise. This comment has set forth a structure forconsidering available ADR options as well as a reasoned set of criteria fordistinguishing among them. Based upon those factors and taking intoaccount the current Alaskan procedures, development of a court-orderedarbitration program for malpractice disputes offers to make the malpracticelitigation system fairer to all parties, more consistent, and less costly.
reasoning in reaching the decision that was made. Cf. WEILER, supra note 1, at 115-16(describing AMA plan to require hearing officers to explain their decisions). Providing awritten explanation would assist the parties in settling. Such a decision could also be madeadmissible at the subsequent trial should any party request a trial de novo.
97. See FED. R. EVID. 706. For an analysis of one state's use of court-appointedexperts in appellate cases, see Francis E. McGovern, Toward a Fundamental Approach forManaging Complex Litigation, 53 U. CI. L. REV. 440, 468-78 (1986).
98. Other changes in the current system would also be advisable. First, the currentprovision could be simplified so that the parties were responsible for providing the neutralexpert with information rather than forcing the physician to independently investigate thematter. Second, the series of questions which the panel now is required to answer could besimplified. This author proposes that the neutral expert be asked to report on the liabilityand causation issues, in addition to any specific questions posed by the arbitrator. In mostcases, the expert would be expected to testify at the hearing (either in person or bytelephone).
1992]

ALASKA LAW REVIEW
APPENDiX A
Verdict
Pre-TrialConference
Summaryo ~ Judgment
00)0
Filing
Incident <
[Vol. 9:2
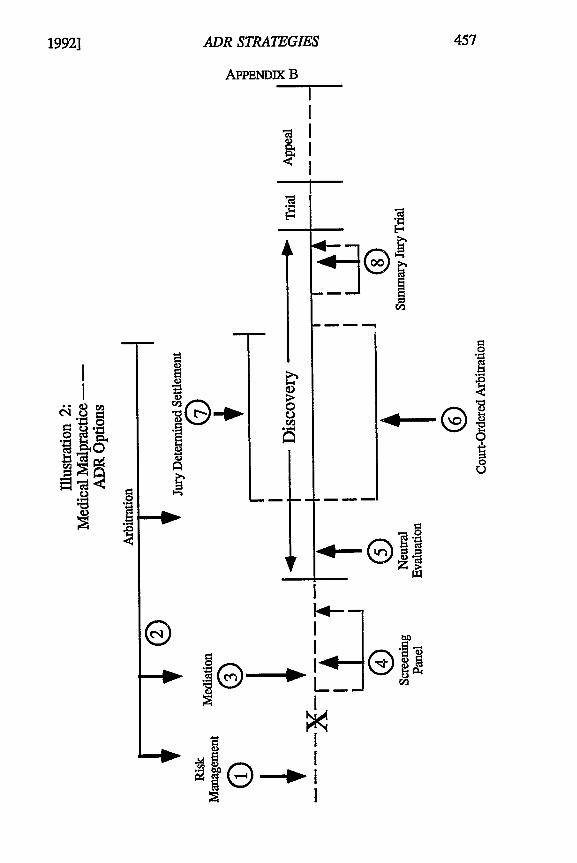
1992]
00
ADR STRATEGIES
APPENDIX B
<I
0
--®
.,4--® '
INII
IA64
"- R.IG


















![Alternative dispute resolution[1]](https://img.pdfslide.us/doc/110x75/54b85d744a79595f4b8b458a/alternative-dispute-resolution1.jpg)











