Embed Size (px)
Citation preview

Alternative designs of benefits packages and their implications for coverage and financial
risk The Case of breast cancer in Colombia
Ramiro GuerreroAna María Amarís
Héctor Castro
Acknowledgments• This presentation is based on a case study on
cancer in Colombia prepared by PROESA as a background paper for the Global Task Force on Cancer Care and Control in Developing Countries, with funding from the Harvard Global Equity Intiative.
The Colombian Health System Reform
• Before 1993: Services for catastrophic illnesses were mostly directly paid out of pocket.– WHO: out of pocket expenditure in Colombia was
44% of private spending in 1993. • In 1993: Universal social health insurance is
adopted, with a basic mandatory benefits package.– Two modalities: contributory and subsidized
insurance
The Colombian Health System today
• Universal Coverage is almost achieved.• The basic package covers surgery,
chemotherapy, radiotherapy and drugs, such as tamoxifen, doxorubicin and paclitaxel.
• Increasing amount of “tutelas” for claiming oncologic services in the courts.
- 2009: Almost US$120 million were spent in oncologic excluded drugs.
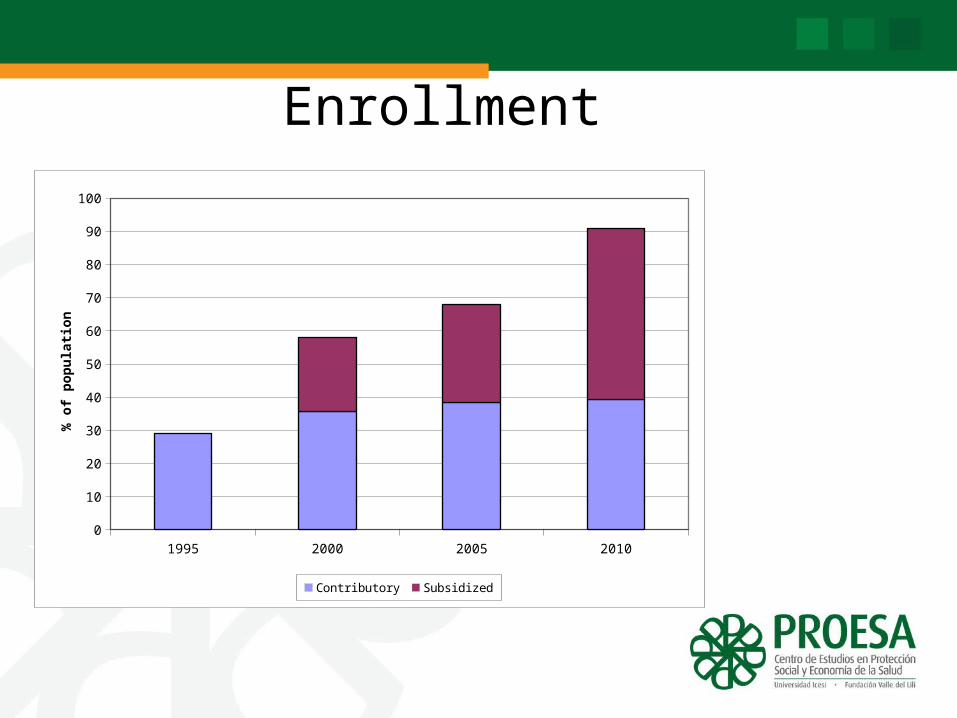
Enrollment
1995 2000 2005 20100
10
20
30
40
50
60
70
80
90
100
Contributory Subsidized
% o
f p
op
ula
tio
n
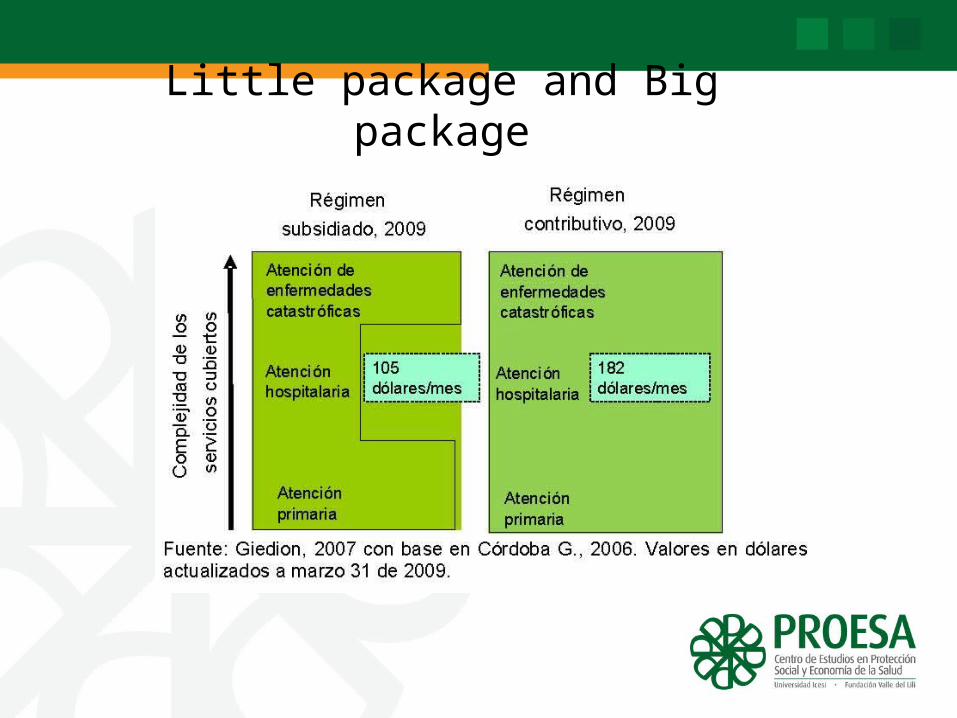
Little package and Big package
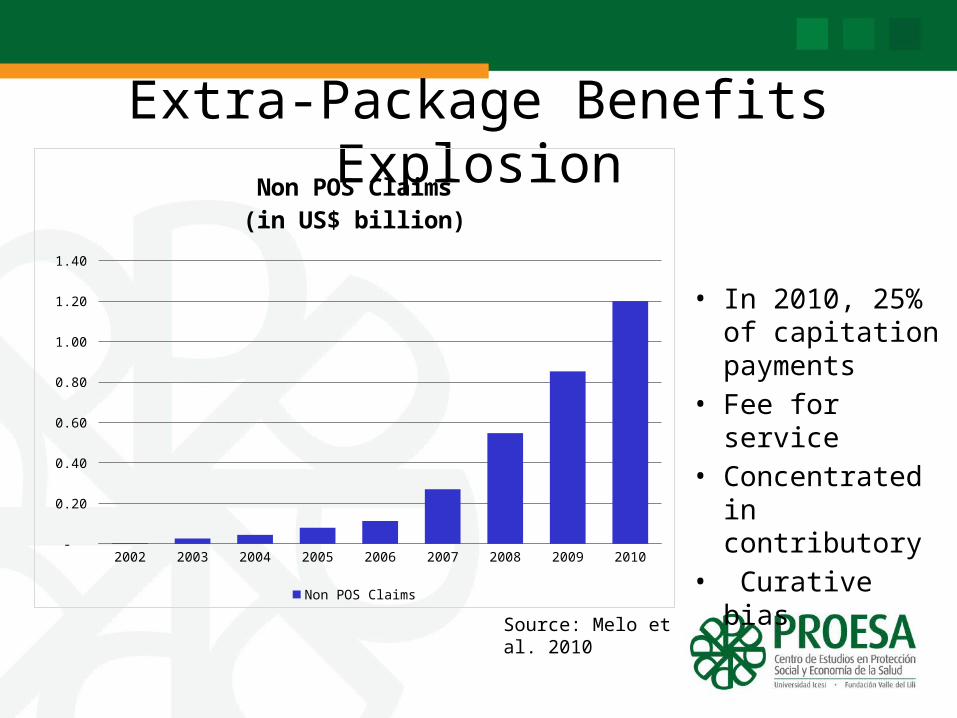
Extra-Package Benefits Explosion
• In 2010, 25% of capitation payments
• Fee for service• Concentrated in
contributory• Curative bias2002 2003 2004 2005 2006 2007 2008 2009 2010
-
0.20
0.40
0.60
0.80
1.00
1.20
1.40
Non POS Claims(in US$ billion)
Non POS Claims
Source: Melo et al. 2010
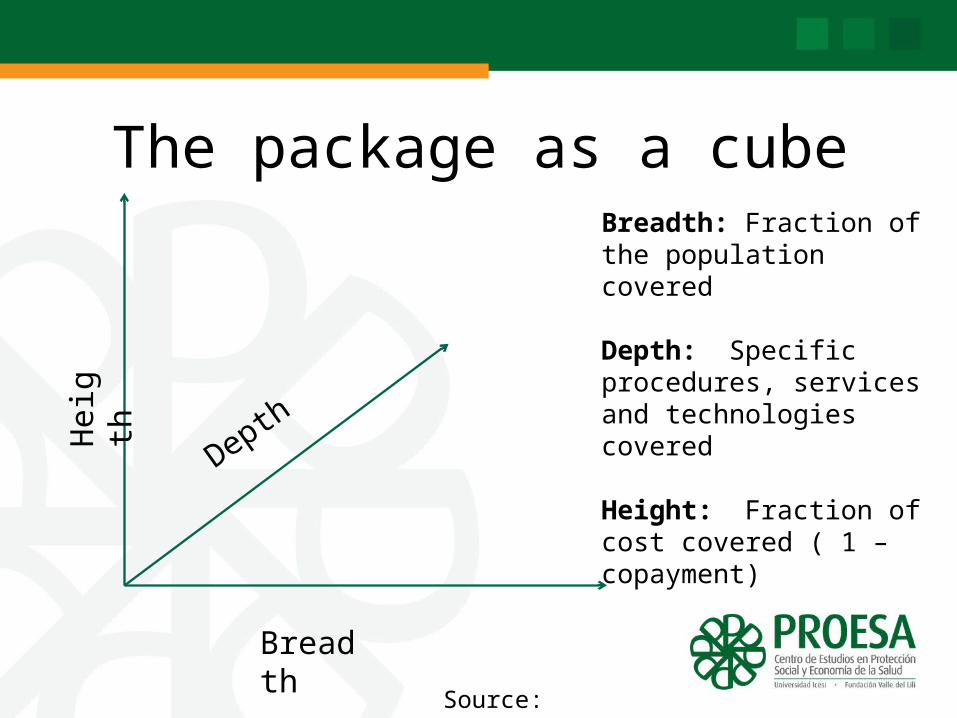
The package as a cubeH
eigt
h
Depth
Breadth
Breadth: Fraction of the population covered
Depth: Specific procedures, services and technologies covered
Height: Fraction of cost covered ( 1 – copayment)
Source: Schreyogg 2005
Breast Cancer in Colombia• The most frequent type among Colombian women.• In 2008 = 6.655 new cases (Globocan).• 21.5% of all types of cancer among women.• Increasing mortality:
-2000 = 7.5 of each 100.000.-2007 = 9.6 of each 100.000.
• Low coverage of mammography (16% of women over 40)• 77.8% of breast cancer patients first consult in advanced
stages.
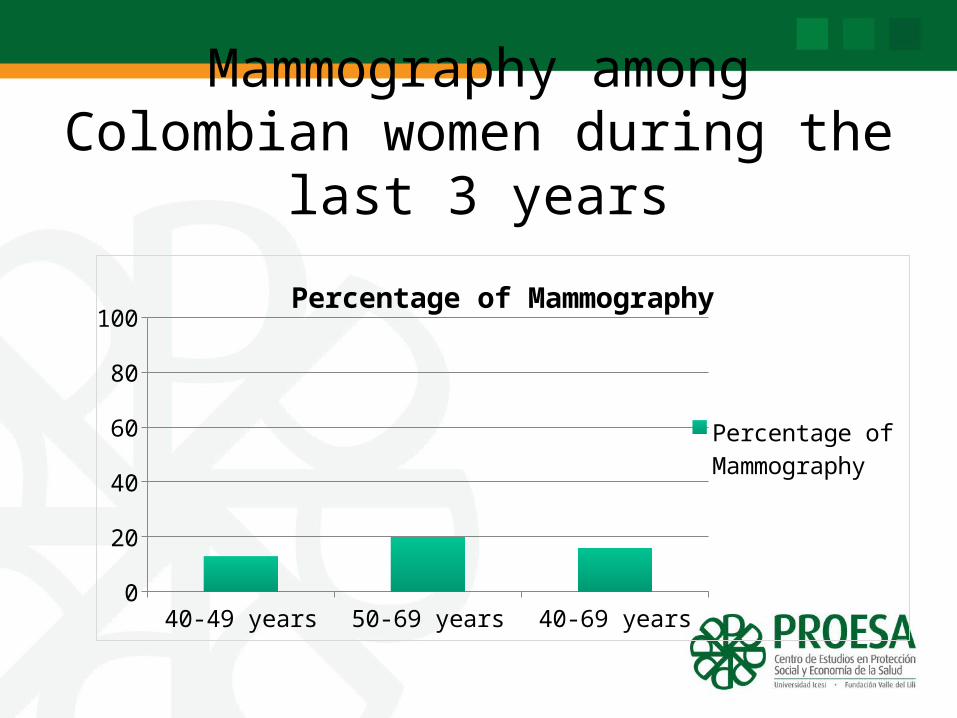
Mammography among Colombian women during the last 3 years
40-49 years 50-69 years 40-69 years0
102030405060708090
100Percentage of Mammography
Percentage of Mam-mography
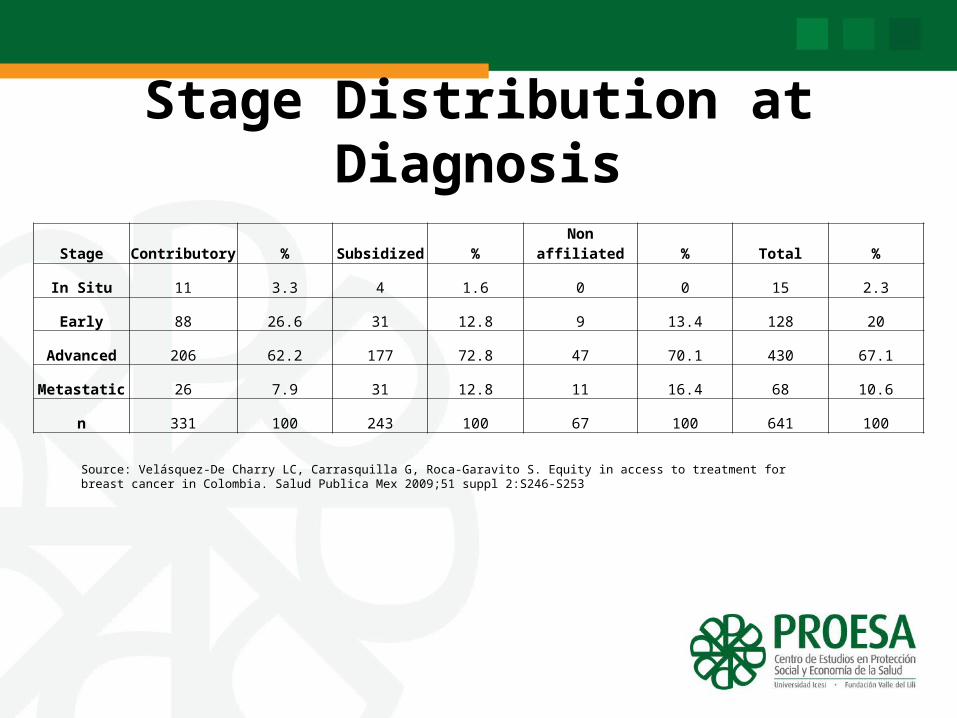
Stage Distribution at Diagnosis
Stage Contributory % Subsidized % Non affiliated % Total %
In Situ 11 3.3 4 1.6 0 0 15 2.3
Early 88 26.6 31 12.8 9 13.4 128 20
Advanced 206 62.2 177 72.8 47 70.1 430 67.1
Metastatic 26 7.9 31 12.8 11 16.4 68 10.6
n 331 100 243 100 67 100 641 100
Source: Velásquez-De Charry LC, Carrasquilla G, Roca-Garavito S. Equity in access to treatment for breast cancer in Colombia. Salud Publica Mex 2009;51 suppl 2:S246-S253
Cancer in the basic package (POS)• Important services excluded:– Mammography not included in subsidized regime.- Trastuzumab, rituximab, leuprolide acetate,
imatinib excluded from both packages.• Increasing amount of “tutelas” for claiming
oncologic services in the courts.

The trade offs of benefit packages design
Stage 0: Universal coverage and POS equalizationStage 1: Horizontal vs. Vertical Approach
- Early diagnosis vs. full coverage of treatment?Stage 2: Scope and Depth of coverage
- Reimbursement of all new costly medicines vs increasing out of pocket spending?
Some numbers to depict the opportunity costs
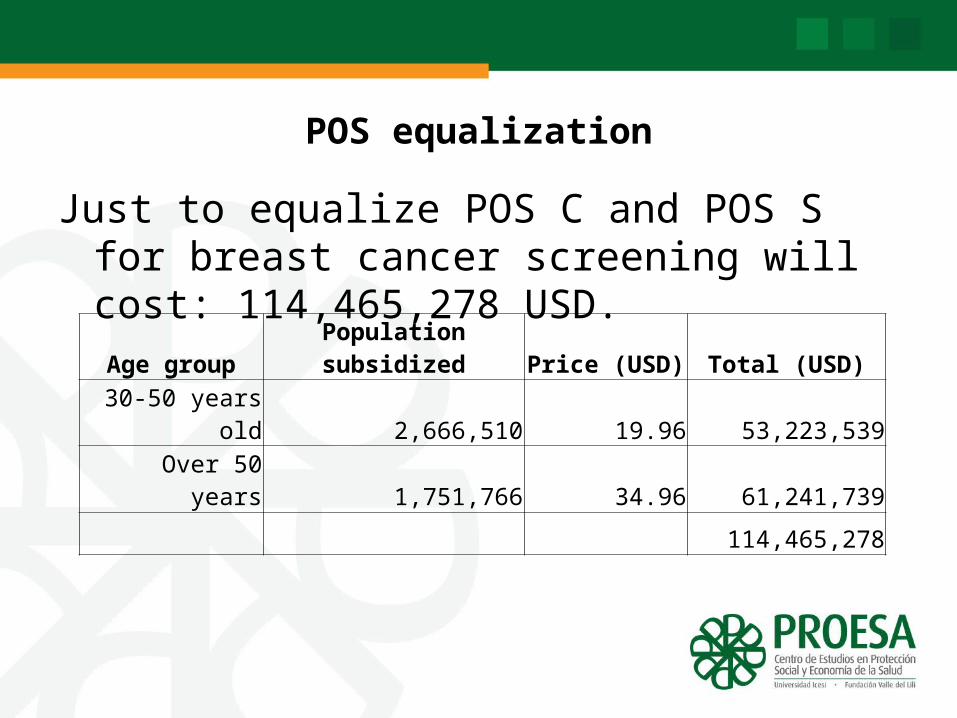
POS equalization
Just to equalize POS C and POS S for breast cancer screening will cost: 114,465,278 USD.
Age group Population subsidized Price (USD) Total (USD)
30-50 years old 2,666,510 19.96 53,223,539
Over 50 years 1,751,766 34.96 61,241,739
114,465,278
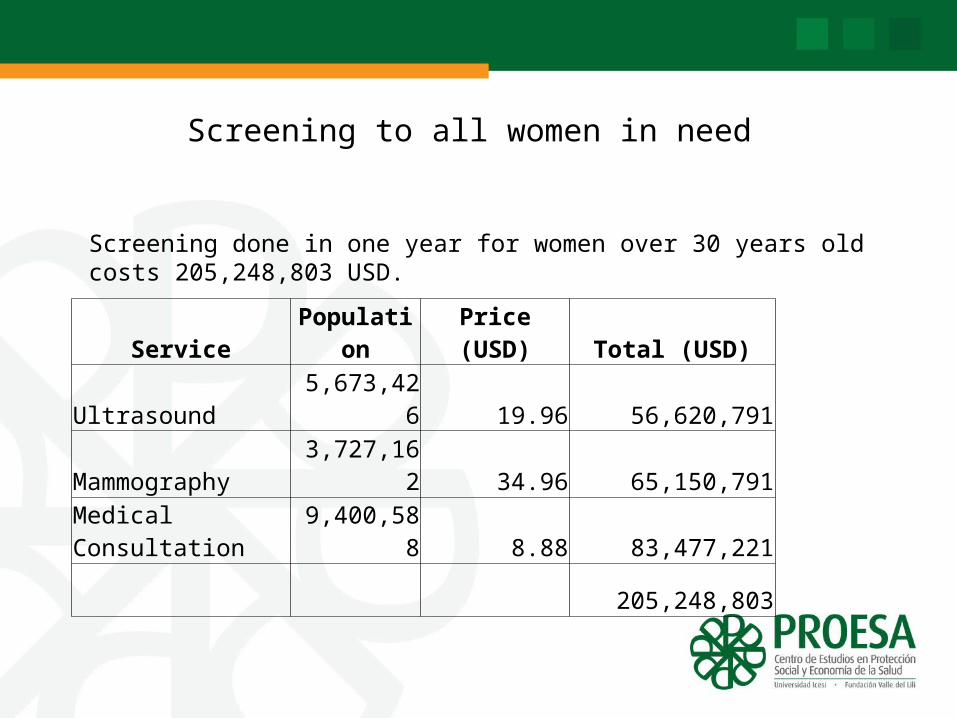
Screening to all women in need
Service Population Price (USD) Total (USD)
Ultrasound 5,673,426 19.96 56,620,791
Mammography 3,727,162 34.96 65,150,791
Medical Consultation 9,400,588 8.88 83,477,221
205,248,803
Screening done in one year for women over 30 years old costs 205,248,803 USD.
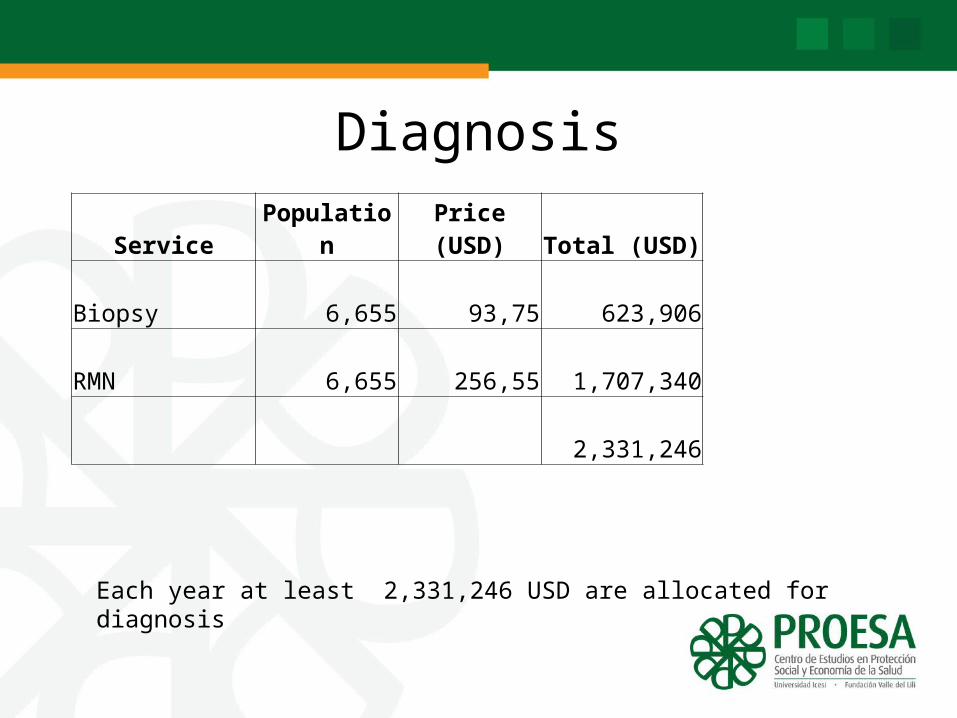
Diagnosis
Service Population Price (USD) Total (USD)
Biopsy 6,655 93,75 623,906
RMN 6,655 256,55 1,707,340
2,331,246
Each year at least 2,331,246 USD are allocated for diagnosis
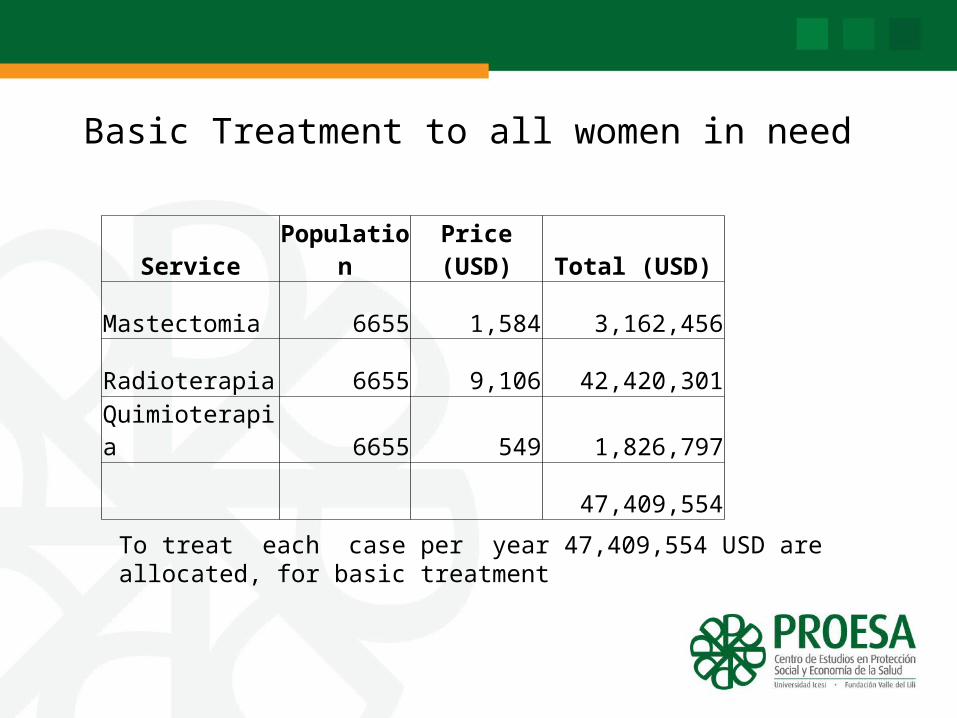
Basic Treatment to all women in need
Service Population Price (USD) Total (USD)
Mastectomia 6655 1,584 3,162,456
Radioterapia 6655 9,106 42,420,301
Quimioterapia 6655 549 1,826,797
47,409,554
To treat each case per year 47,409,554 USD are allocated, for basic treatment
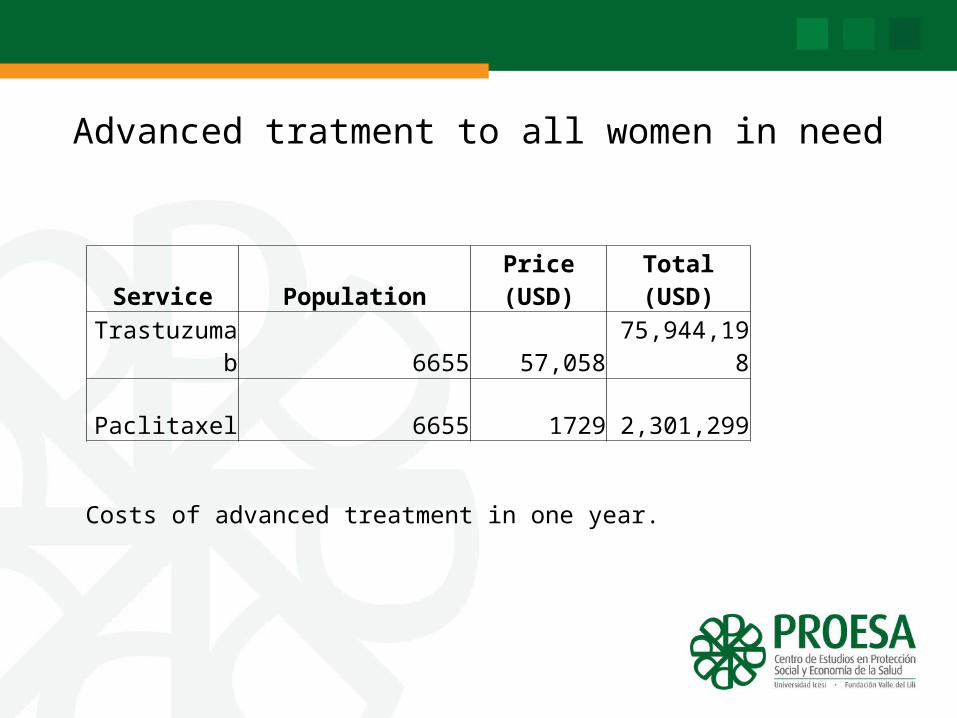
Advanced tratment to all women in need
Service Population Price (USD) Total (USD)
Trastuzumab 6655 57,058 75,944,198
Paclitaxel 6655 1729 2,301,299
Costs of advanced treatment in one year.
Discussion
• The political imperative of unifying the packages• High nominal coverage with low effective coverge– Infrastructure and training– The mix of services (insufficient detection)
• The redesign of the package (an opportunity)• New institutions for priority setting• The rationing model, the infinite plan and
sustainability
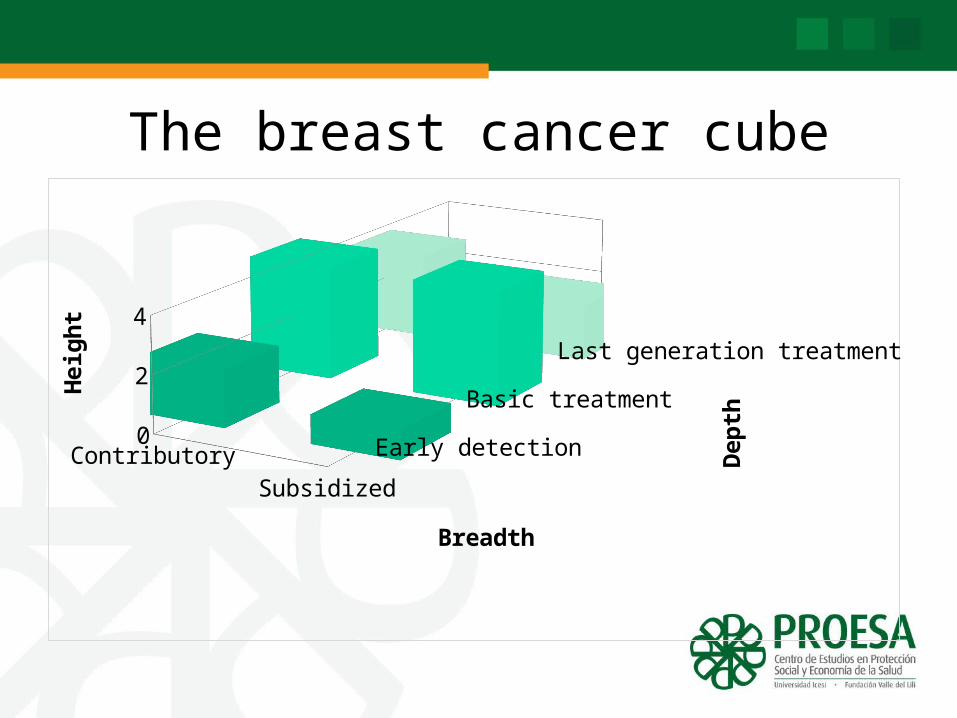
The breast cancer cube
Contribu-tory Subsidized
01234
Early detection
Basic treatment
Last generation treatment
Breadth
Hei
ght
Dep
th
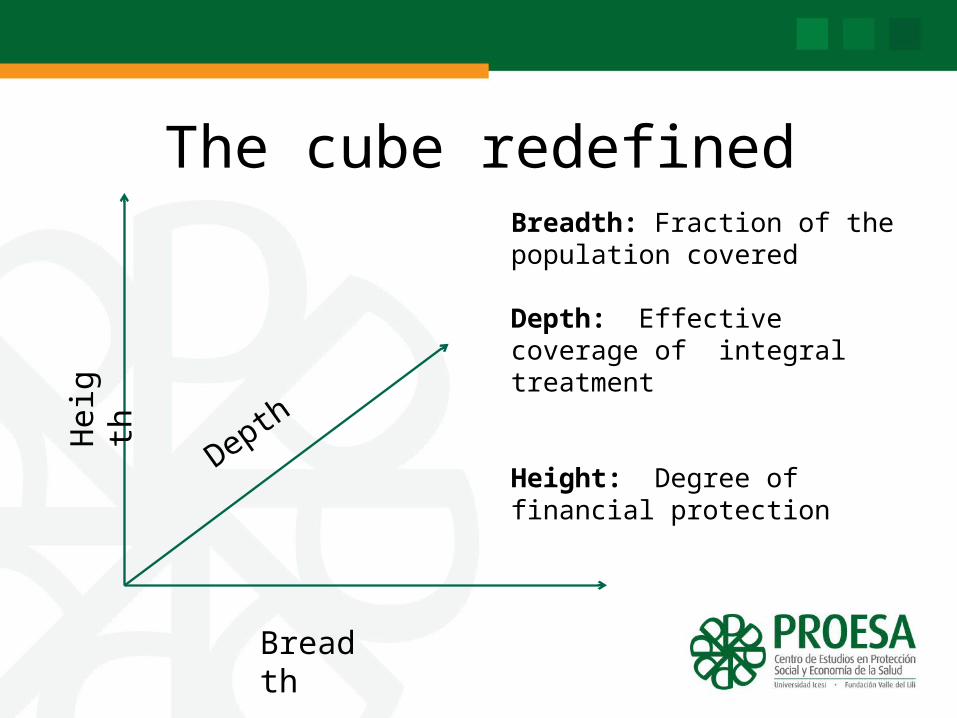
The cube redefinedH
eigt
h
Depth
Breadth
Breadth: Fraction of the population covered
Depth: Effective coverage of integral treatment
Height: Degree of financial protection
Effective Coverage of Integral Treatment
The maximum possible health gain an individual with a given health care need can expect to receive from the health system.
For intervention j and individual i
1 ijijijij NUQEC
Conclusions
• Costs of universal:– Screening: US$205M– Diagnosis: US$2,3M– Basic tratment: US$47M– Advanced treament: US$78M
• Coverage by component:– Screeing (16% of the challenge)– Basic treatment (most of the challenge)– Advanced treatment (nearly half)
• Impact of this mix? – Allocative efficiency seems to dominate the results