Embed Size (px)
Citation preview

156 Hripf C’ommunications .imuary, 1989
American Heart Journal
impulse propagation from the conducting bundle branch into the blocked contralateral bundle branch is responsi- ble for several manifestations of concealed intraventricu- lar conduction.R This study suggests that “reversed” Wenckebach periodicity may also be a peculiar manifesta- tion of concealed reentry in the ventricles.
REFERENCES
I.
2.
3 I
4.
5 < .
6.
I.
a.
Wenckebach KF, Winterberg H: Die unregelmassige Herztb- tigkeit. Leipzig, 1927, Wilhelm Engelmann, p 339. Mack I, Langendorf R, Katz LN: The supernormal phase of recovery of conduction in the human heart. AM HEART .I 34:374, 1947. Katz LN, Pick A: Clinical electrocardiography. 1. The arrhythmias. Philadelphia, 1956, Lea & Febiger, p. 622. Pick A. Langendorf R, Katz LN: The supernormal phase of atrioventricular conduction. I. Fundamental mechanisms. Circulation 26:388,1962. Rosenbaum MB, Elizari MV, Lazzari JO, Halpern MS, Nau GJ: Bilateral bundle branch block: Its recognition and signif- icance. Cardiovasc Clin 2:152, 1971. Hoffman BF, Cranefield PF: Electrophysiology of the heart. New York, 1960, McGraw-Hill Book Co, p 175. Moe GK, Mendez C. Han J: Aberrant A-V impulse propaga- tion in the dog heart: A study of functional bundle branch block. Circ Res 16:261, 1965. Langendorf R, Pick A: Concealed intraventricular conduction in the human heart. Adv Cardiol 14:40, 1975.
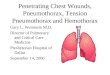
Fig. 1. X-ray picture taken shortly after admission, demonstrating left pneumothorax and right pulmonary edema. Arrow points to tip of Swan-Ganz catheter in right pulmonary arterv.
Alternating unilateral pulmonary edema following pneumothorax in acute myocardial infarction
Andre Keren, M.D., Dan Tzivoni, M.D., and Shlomo Stern, M.D. Jerusalem, Israel
Unilateral pulmonary edema is a rare condition, associ- ated usually with one-sided damage of the ventilation and/or perfusion capacity of the ipsilateral or contralater- al lung.’ Most cases are reported to occur following reexpansion of a lung after pneumothorax,2g and sporadic cases were described in localized emphysema,‘O following systemic-pulmonary artery shunts,” in congenital absence of a pulmonary artery,‘” in pulmonary thrombo- embolism,” or induced by left-sided heart failure.‘? In spite of the relatively large number of cases described following pneumothorax, the pathophysiologic mecha- nism of this unilateral pulmonary edema remains poorly understood,4 especially since hemodynamic measurements were performed in none of the patients described and the theories proposed to explain its pathogenesis are conjec-
From the Heiden Department of Cardiology, Bikur Cholim Hospital. and Hebrew University-Hadassah Medical School.
Received for publication Sept. 21, 1981; accepted Oct. 26, 1981.
Reprint requests: Shlomo Stern, M.D., Heiden Department of Cardiology, Bikur Cholim Hospital, P.O. Box 449, Jerusalem, Israel.
tural.,’ To the best of our knowledge, the patient described herein is the first who initially had alternating unilateral pulmonary edema, first on the contralateral and subse- quently on the ipsilateral side of a pneumothorax. Fur- t.hermore, concomitant hemodynamic monitoring in this patient permitted us to test the prevailing theories con- cerning the factors involved in the appearance of unilater- al pulmonary edema during and after evacuation of a pneumothorax.
L.A., a 58-year-old woman, was brought to the emergen- cy department in a semiconscious state. She showed signs of severe respiratory distress with shallow breathing and central cyanosis. There were signs of circulatory shock with cold extremities and a systolic blood pressure of 50 mm Hg. The left hemithorax showed no respiratory expansion, whereas on the right side rales compatible with pulmonary edema were found. An ECG showed an acute anteroseptal infarction. Chest x-ray film revealed left- sided pneumothorax and right-sided pulmonary edema (Fig. 1). The pneumothorax was explained by faulty attempts by the rescue team to insert a subclavian venous catheter on the way to the hospital. The oxygen tension in the arterial blood (Pa,,,,) was 32 mm Hg, and hemodynam- ic measurements with- the use of a Swan-Ganz catheter revealed marked increase in pulmonary vascular resis- tance (1126 dyne-set-cm-“), with secondary right-sided heart failure (right ventricular tilling pressure of 18 mm Hg) in the presence of a low filling pressure of the left
0002.8703/83/010156+04$00.40/0 c.1983 The C.V. Mosby Co.

Volume 105
Number 1 Brief Communications 157
Table I. Summary of hemodynamic and arterial blood gas values
On admission* 2 days after admissiont Before discharge
Pressures (mm Hg) Systemic Right atrium Pulmonary artery
Right Left
Pulmonary artery wedge Right Left
Cardiac output (L/min) Cardiac index (L/min/M? Pulmonary vascular resistance (dynes-set-cm-‘) Systemic vascular resistance (dynes-set-cm-‘) Pulmonary-systemic vascular resistance (TO )
P%? (mm Hg) Room air Respiratorj
‘Left pneumothorax, right pulmonary edema. ?Left pulmonary edema.
50/30, mean 38 mean 18
70/30, mean 45
mean 4
2.84 1.67 1126
563 200
32 48
90160, mean 12 mean 8
38115, mean 25 38115, mean 25
mean 11 mean 11
3.80 2.23 294
1347 22
-
88
loo/SO, mean 75 mean 5
28115, mean 20 28115, mean 20
mean 14 mean 14
4.20 2.47
114 1371
8
94
IAfter lS minutes, FI,, of I without positive end-expiratory pressure.
ventricle (4 mm Hg) and a low cardiac output (2.84 L/min) (Table I). In view of these hemodynamic findings, the diagnosis of unilateral adult respiratory distress syndrome was made. The patient was artificially ventilated by means of positive end-expiratory pressure ranging between 5 and 10 cm H,O. The pneumothorax was drained by intercostal tube under negative pressure. Dopamine infusion at a rate of 5 to 10 pg/min/kg was administered. Diuretics and digoxin were not used.
A few hours later, a repeat chest x-ray film showed reexpansion of the left lung with progressively increasing congestion of the same lung field. The advancing increase in congestion on the left side, together with its regression on the right side, created at this stage an x-ray appearance compatible with bilateral pulmonary edema (Fig. 2). The hemodynamic measurements, performed bilaterally from this stage onward, showed identical values on both sides, i.e., reduction in pulmonary arterial pressure and resis- tance, to 45/25 mm Hg and 600 dyne-see-cm+, respective- ly, and a slight increase in wedge pressure, to 8 mm Hg. Blood gas values improved slightly (Pa,, 60 mm Hg on FIo, of 1). Corticosteroids and albumin were added, and in addition to previous therapy, the patient also received crystalloid fluids, which seemed mandatory for restoring blood pressure, left ventricular filling pressure, and cardi- ac output.
Fig. 2. X-ray picture taken 4 hours after admission, demonstrating regression of right pulmonary edema and increasing congestion in reexpanded left lung. Arrow points to tip of Swan-Ganz catheter in right pulmonary artery.
Forty-eight hours after admission, while the patient was still hypoxemic and required respiratory support (Pk, of 88 mm Hg on FIo, of l), the chest x-ray film showed unilateral pulmonary edema on the left side (Fig. 3). The hemodynamic data showed marked improvement, i.e., slightly increased pulmonary arterial pressure and resis- tance, as well as normal wedge pressure and cardiac output (Table I). The above-mentioned therapy was con- tinued, and the clinical picture and blood gas values
improved progressively, although the x-ray picture of left-sided pulmonary congestion still persisted. On the fifth day of hospitalization the patient was extubated, but the left lung became clear on the chest x-ray film only after a lag period of 5 additional days. The patient was discharged from the hospital 2 weeks later, when the arterial blood gas values, hemodynamic measurements, and chest x-ray films were normal (Table I, Fig. 4).

158 Brie/ Communications January, 1983
American Heart Journal
Fig. 3. X-ray picture taken 2 days after admission, dem- onstrating edema in the reexpanded left lung and clear right lung. Arrow points to tip of Swan-Ganz catheter in left pulmonary artery. Similar chest x-ray pictures were obtained during next 7 days as well.
Postpneumothorax unilateral pulmonary edema is mainly an x-ray phenomenon and only seldom gives clinical manifestations.3,d According to several authors,2 4 it usually follows reexpansion of the lung on the ipsilateral side and occurs mainly after large pneumothoraces in which the collapse was prolonged for periods of at least 3 days and negative pressure was applied to the pleural cavity. However, in a few reports, the unilaterally develop- ing pulmonary edema did not have these characteristics. For example, the two patients of SteckeY developed pulmonary edema contralateral to the site of the pneumo- thorax, and three other patients developed ipsilateral pulmonary edema after short periods of lung collapse.T-g
The supposed mechanism of contralateral pulmonary edema in the previously reported patients with pneumo- thorax6 was acute left-sided heart failure, associated with increased capillary permeability and high pulmonary vas- cular resistance on the side of the noncollapsed lung. However, in spite of immediate therapy for the pneumo- thorax and rapid reexpansion of the collapsed lung, the pulmonary edema did not become bilateral, as could be expected to happen in the presence of acute left-sided heart failure. Our patient, although suffering from acute anteroseptal infarction, developed contralateral pulmo- nary edema without signs of left ventricular failure, as indicated by hemodynamic measurements, which demon-
Fig. 4. X-ray picture taken on discharge demonstrates clear lung fields.
strated a low left ventricular filling pressure. However, we found a marked increase in pulmonary vascular resistance, associated with right-sided heart failure and leading to reduced flow through the lungs and a low-output state. In our opinion, the causes of the contralateral pulmonary edema in our patient were the acute severe pulmonary hypertension and the associated capillary damage, which was induced by systemic hypotension and hypoxemia. These factors could also affect the surfactant-producing type 2 cells in the functioning lung.“’ It is possible that in other patients left ventricular failure may be an important contributing factor in the development of contralateral pulmonary edema, but this remains to be proved by hemodynamic measurements.
The reexpansion pulmonary edema on the ipsilateral side is considered to be induced by capillary hypoxemic damage during long-standing pneumothoraces, with sud- den increase in flow during a short reexpansion period.?-” The capillary permeability may be further increased by applying negative pressure to the pleural space.L.“.‘, In our patient the reexpansion pulmonary edema occurred only after 3 hours of lung collapse and persisted, together with severe disturbances in blood gas values, for a longer period than in most previously reported cases. This can possibly be explained by the severe hypoxemic damage induced by both the contralateral pulmonary edema present during the pneumothorax period and the use of negative intra- pleural pressure and rapid reexpansion of the lung. During this ipsilateral pulmonary edema, the pulmonary vascular resistance decreased dramatically (from 1126 to 294 dyne- set-cm+), with rapid improvement of all the hemodynam-

Volume 105
Number 1
ic parameters and without signs of left ventricular failure. Thus the acute pulmonary hypertension seemed to be a major factor only in the contralateral, but not in the ipsilateral, reexpansion pulmonary edema. The identity of bilateral pressure measurements in our patient makes doubtful the earlier hypothesis concerning the inequalities in capillary or venous pressures in the two sides of the lungs.14, I5 We also ruled out positional-gravitational fac- tors15, I6 by changing our patient’s position frequently, which did not influence the chest x-ray findings.
As mentioned above, only rarely was a postpneumotho- rax pulmonary edema associated with the clinical picture of marked respiratory distress. Our patient, however, exhibited clinical symptoms of severe respiratory insuffi- ciency and extremely low Pa,+ values, the x-ray picture revealed pulmonary edema, and there was no left ventric- ular failure. Thus the criteria for adult respiratory distress syndrome were fulfilled.13 The importance of hemodynam- ic measurements for diagnosing this syndrome in patients with bilateral pulmonary edema and for application of proper therapy is well established.‘3,17 Our report not only presents a new and unusual form of unilateral noncardiac edema alternating sequentially in the two lungs but stresses again the importance of hemodynamic measure- ments in a clinical entity in which the pathophysiology may be obscure.@
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
Calenoff L, Kruglick GD, Woodruff A: Unilateral pulmonary edema. Radiology 126:19, 1978. Ziskind MM, Weill H, George RA: Acute pulmonary edema following the treatment of spontaneous pneumothorax with excessive negative intrapleural pressure. Am Rev Respir Dis 92:632, 1965. Waqaruddin M, Bernstein A: Reexpansion pulmonary ede- ma. Thorax 30:54, 1975. Mahajan VK, Simon M, Huber GL: Reexpansion pulmonary edema. Chest 75:192, 1979. Miller WC, Toon R, Palat H, Lacroix J: Experimental pulmonary edema following reexpansion of pneumothorax. Am Rev Respir Dis 108:654, 1973. Steckel RJ: Unilateral nulmonarv edema after tmeumotho- rax. N Engl J Med 289:621, 1973: Ravin CE, Dahmash NS: Reexpansion pulmonary edema (Letter to the Editor). Chest 77:709, 1980. Sherman S, Ravikrishnan KP: Unilateral pulmonary edema following reexpansion of pneumothorax of brief duration (Letter to the Editor). Chest 77:714, 1980. Humphreys RL, Berne AS: Rapid reexpansion of pneumotho- rax. Radiology 96:509, 1970. Hublitz UF, Shapiro JH: Atypical pulmonary patterns of congestive failure in chronic lung disease. Radiology 93:995, 1969. Albers WH, Nadas AS: Unilateral chronic pulmonary edema and pleural effusion after systemic-pulmonary artery shunts for cyanotic congenital heart disease. Am J Cardiol 19:861, 1967: Richman SM, Godar TJ: Unilateral pulmonary edema. N Engl J Med 264:1146, 1961. Petty TL, Ashbaugh DG: The adult respiratory distress syndrome: Clinical features, factors influencing prognosis and principles of management. Chest 60:233, 1971. Goodrich WA: Pulmonary edema: A correlation of x-ray ;;;;.arance and physiological changes. Radiology 51:58,
15.
16.
17.
18.
Brief Communications 159
Gleason DC, Steiner RE: The lateral roentgenogram in pulmonary edema. Am J Roentgen01 98:279, 1966. Leeming BWA: Gravitational edema of the lungs observed during assisted respiration. Chest 64:719, 1973. Keren A, Klein J, Stern S: Adult respiratory distress syn- drome in the course of acute myocardial infarction. Chest 77:161, 1980. Nessa CB, Rigler LG: The roentgenological manifestations of pulmonary edema. Radiology 37:35, 1941.
Prediction of subclinical perhexiline neuropathy in a patient with inborn error of debrisoquine hydroxylation
Rashmi R. Shah, B.Sc., M.R.C.P., Nicholas S. Oates, Ph.D., Jeffrey R. Idle, Ph.D., Robert L. Smith, D.Sc., and J. Dennis F. Lockhart, M.B.B.Ch., D.P.H. Paddington and Middleser, England
Perhexiline is an effective antianginal agent.’ Its use however, has been associated with occasional serious side effects, notably peripheral neuropathy: severe weight loss,’ and effects on hepatic function, including cirrhosis.3 Perhexiline is metabolized by oxidation to more polar hydroxylated metabolites prior to its elimination.4 Recently, human studies of debrisoquine metabolism have shown the occurrence of a genetic polymorphism in drug oxidation, approximately 9% of British white persons being defective in this respect.5 Furthermore, individuals with impaired debrisoquine oxidizing ability cannot metabolize normally a number of other drugs.5 As a consequence, they are susceptible to various adverse drug reactions such as debrisoquine-induced postural hypoten- sion, phenformin-induced lactic acidosis, phenacetin- induced methemoglobinemia, and nortriptyline-induced vertigo, dizziness, and confusional state6 We describe a patient for whom the determination of debrisoquine hydroxylation status was of value in alerting us to investi- gating and demonstrating the existence of subclinical peripheral neuropathy, which might otherwise have escaped recognition until it had developed to the point of becoming clinically overt.
G.A., a 60-year-old man with a past medical history of duodenal ulcer and treatment with cimetidine, was admit- ted in 1978 with extensive anterior myocardial ischemia. His ECG showed severe ST-T changes without any accom- panying changes in serum enzyme levels. Following recov- ery, he continued to experience angina at rest, during
From the Department of Biochemical and Experimental Pharmacology, St. Mary’s Hospital Medical School, and Merrell Pharmaceuticals Limited.
Received for publication Oct. 7, 1981; accepted Nov. 23, 1981.
Reprint requests: Rashmi R. Shah, B.&z., M.R.C.P., Department of Biochemical/Experimental Pharmacology, St. Mary’s Hospital Medical School, Paddington, London W2 lPG, England.
0002.8703/83/010159 + 03$00.30/O d 1983 The C. V. Mosby Co.










![arXiv:2001.08817v1 [cs.LG] 23 Jan 2020 · three different critical findings (pneumothorax, pneumonia, and pulmonary edema) from three different CXR datasets. Index Terms— chest](https://img.pdfslide.us/doc/110x75/5fb3fa175cfeae2d5f16acdc/arxiv200108817v1-cslg-23-jan-2020-three-different-critical-indings-pneumothorax.jpg)