Embed Size (px)
DESCRIPTION
Altered Integument Concept Maps. Gary Schofield, RN. Infections Bacterial: Folliculitis, Foruncle, Carbuncles, Cellulitis, Erysipelas Viral: Herpes (Simplex,Zoster, Varicella), Warts Fungal: Tinea, Candidiasis. INFLAMATORY - PowerPoint PPT Presentation
Citation preview
Altered Integument Concept Maps
Gary Schofield, RN
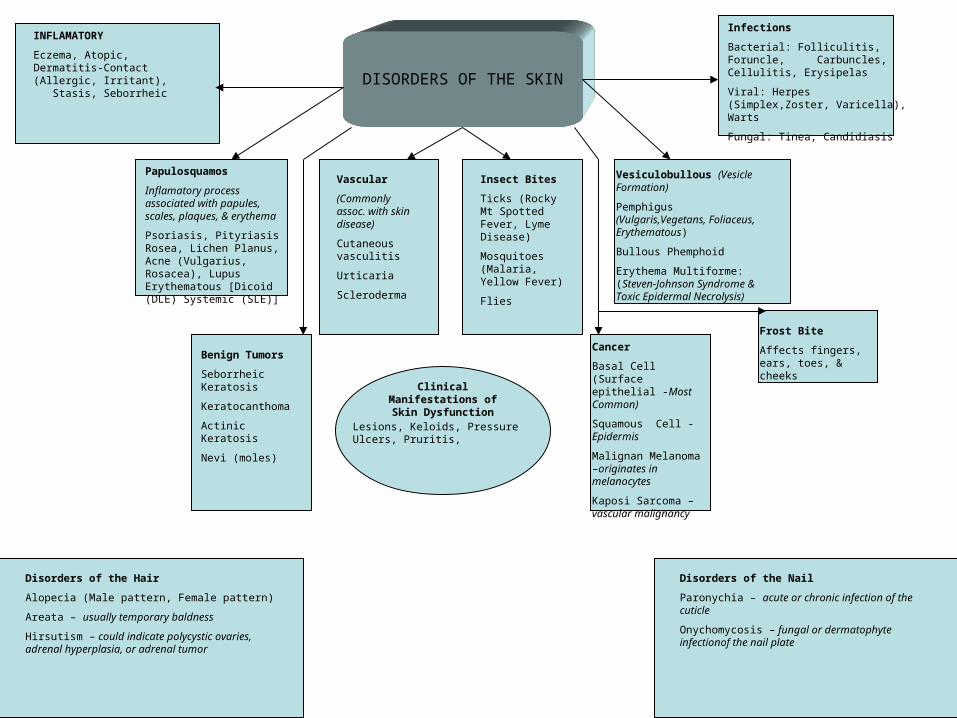
DISORDERS OF THE SKIN
INFLAMATORY
Eczema, Atopic, Dermatitis-Contact (Allergic, Irritant), Stasis, Seborrheic
Infections
Bacterial: Folliculitis, Foruncle, Carbuncles, Cellulitis, Erysipelas
Viral: Herpes (Simplex,Zoster, Varicella), Warts
Fungal: Tinea, Candidiasis
Papulosquamos
Inflamatory process associated with papules, scales, plaques, & erythema
Psoriasis, Pityriasis Rosea, Lichen Planus, Acne (Vulgarius, Rosacea), Lupus Erythematous [Dicoid (DLE) Systemic (SLE)]
Vesiculobullous (Vesicle Formation)
Pemphigus (Vulgaris,Vegetans, Foliaceus, Erythematous)
Bullous Phemphoid
Erythema Multiforme: (Steven-Johnson Syndrome & Toxic Epidermal Necrolysis)
Vascular
(Commonly assoc. with skin disease)
Cutaneous vasculitis
Urticaria
Scleroderma
Insect Bites
Ticks (Rocky Mt Spotted Fever, Lyme Disease)
Mosquitoes (Malaria, Yellow Fever)
Flies
Benign Tumors
Seborrheic Keratosis
Keratocanthoma
Actinic Keratosis
Nevi (moles)
Cancer
Basal Cell (Surface epithelial -Most Common)
Squamous Cell -Epidermis
Malignan Melanoma –originates in melanocytes
Kaposi Sarcoma –vascular malignancy
Clinical Manifestations of Skin Dysfunction
Lesions, Keloids, Pressure Ulcers, Pruritis,
Disorders of the Hair
Alopecia (Male pattern, Female pattern)
Areata – usually temporary baldness
Hirsutism – could indicate polycystic ovaries, adrenal hyperplasia, or adrenal tumor
Disorders of the Nail
Paronychia – acute or chronic infection of the cuticle
Onychomycosis – fungal or dermatophyte infectionof the nail plate
Frost Bite
Affects fingers, ears, toes, & cheeks
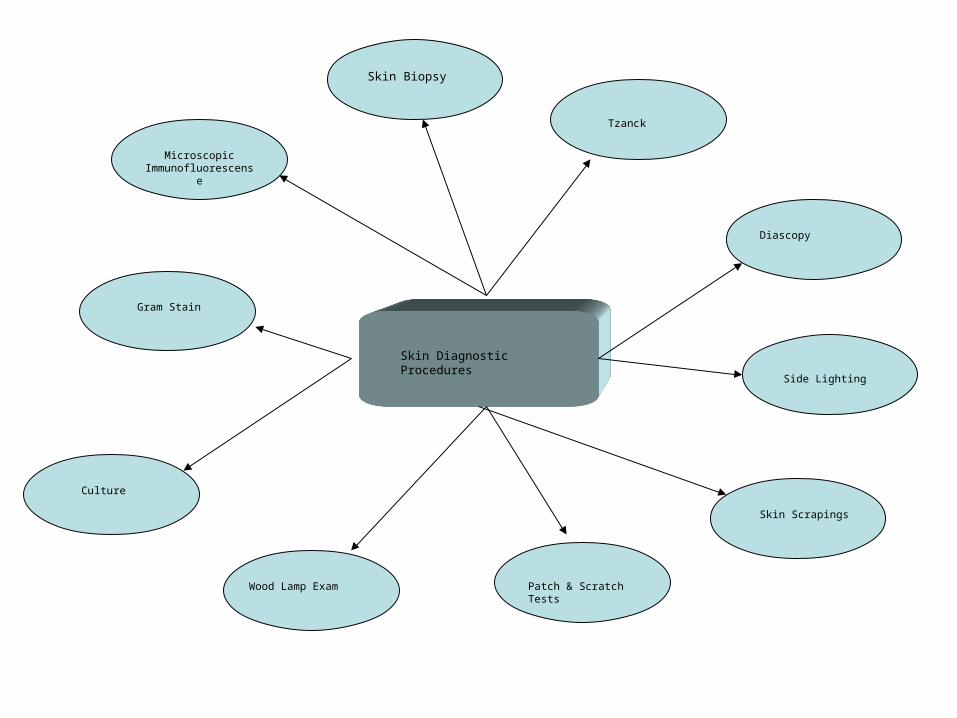
Skin Diagnostic Procedures
Skin Biopsy
Microscopic Immunofluorescense
Gram Stain
Culture
Wood Lamp Exam Patch & Scratch Tests
Skin Scrapings
Side Lighting
Diascopy
Tzanck
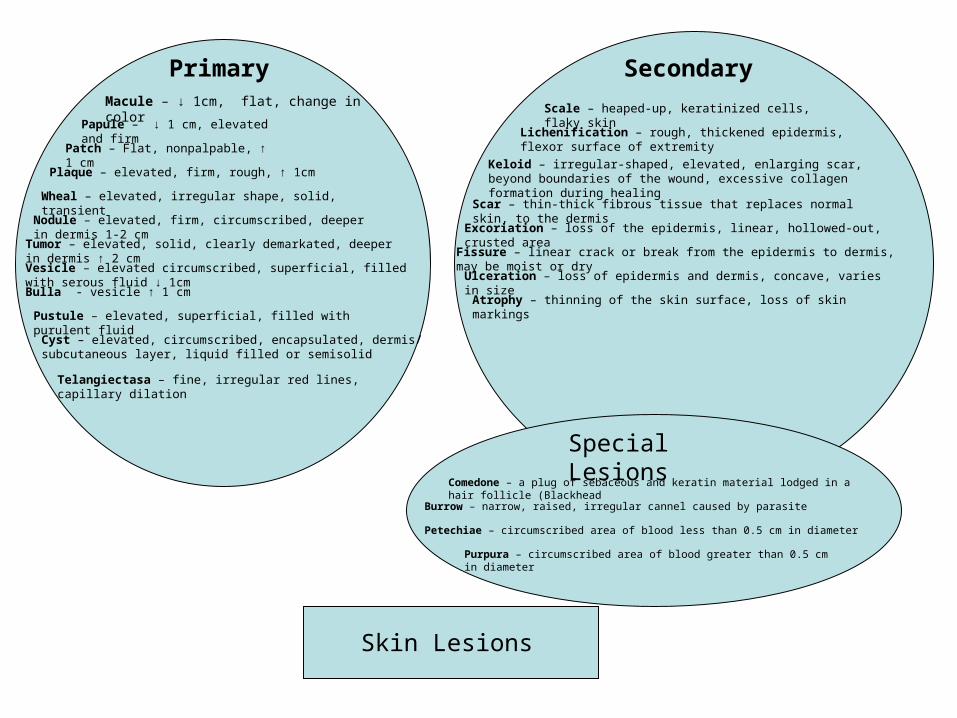
Skin Lesions
Primary SecondaryMacule – ↓ 1cm, flat, change in color
Papule – ↓ 1 cm, elevated and firm
Patch – Flat, nonpalpable, ↑ 1 cm
Plaque – elevated, firm, rough, ↑ 1cm
Wheal – elevated, irregular shape, solid, transient
Nodule – elevated, firm, circumscribed, deeper in dermis 1-2 cm
Tumor – elevated, solid, clearly demarkated, deeper in dermis ↑ 2 cm
Vesicle – elevated circumscribed, superficial, filled with serous fluid ↓ 1cm
Bulla - vesicle ↑ 1 cm
Pustule – elevated, superficial, filled with purulent fluid
Cyst – elevated, circumscribed, encapsulated, dermis/ subcutaneous layer, liquid filled or semisolid
Telangiectasa – fine, irregular red lines, capillary dilation
Scale – heaped-up, keratinized cells, flaky skin
Lichenification – rough, thickened epidermis, flexor surface of extremity
Keloid – irregular-shaped, elevated, enlarging scar, beyond boundaries of the wound, excessive collagen formation during healing
Scar – thin-thick fibrous tissue that replaces normal skin, to the dermis
Excoriation – loss of the epidermis, linear, hollowed-out, crusted area
Fissure – linear crack or break from the epidermis to dermis, may be moist or dry
Ulceration – loss of epidermis and dermis, concave, varies in size
Atrophy – thinning of the skin surface, loss of skin markings
Special Lesions
Comedone – a plug of sebaceous and keratin material lodged in a hair follicle (Blackhead
Burrow – narrow, raised, irregular cannel caused by parasite
Petechiae – circumscribed area of blood less than 0.5 cm in diameter
Purpura – circumscribed area of blood greater than 0.5 cm in diameter
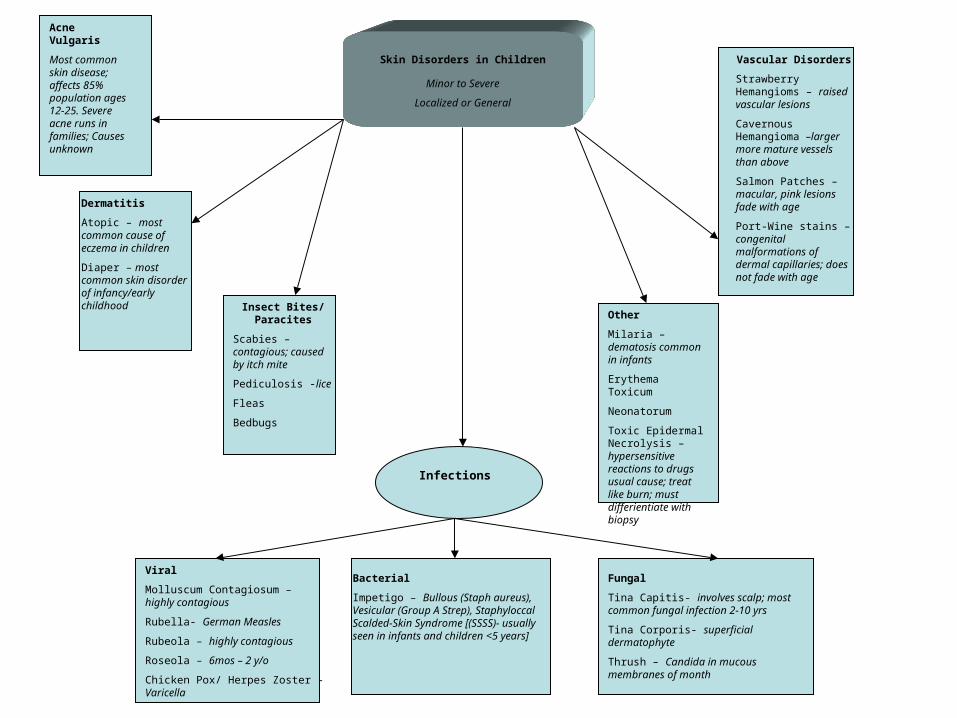
Skin Disorders in Children
Minor to Severe
Localized or General
Acne Vulgaris
Most common skin disease; affects 85% population ages 12-25. Severe acne runs in families; Causes unknown
Dermatitis
Atopic – most common cause of eczema in children
Diaper – most common skin disorder of infancy/early childhood Insect Bites/
Paracites
Scabies – contagious; caused by itch mite
Pediculosis -lice
Fleas
Bedbugs
Infections
Vascular Disorders
Strawberry Hemangioms – raised vascular lesions
Cavernous Hemangioma –larger more mature vessels than above
Salmon Patches – macular, pink lesions fade with age
Port-Wine stains – congenital malformations of dermal capillaries; does not fade with age
Other
Milaria –dematosis common in infants
Erythema Toxicum
Neonatorum
Toxic Epidermal Necrolysis – hypersensitive reactions to drugs usual cause; treat like burn; must differientiate with biopsy
Viral
Molluscum Contagiosum – highly contagious
Rubella- German Measles
Rubeola – highly contagious
Roseola – 6mos – 2 y/o
Chicken Pox/ Herpes Zoster - Varicella
Bacterial
Impetigo – Bullous (Staph aureus), Vesicular (Group A Strep), Staphyloccal Scalded-Skin Syndrome [(SSSS)- usually seen in infants and children <5 years]
Fungal
Tina Capitis- involves scalp; most common fungal infection 2-10 yrs
Tina Corporis- superficial dermatophyte
Thrush – Candida in mucous membranes of month
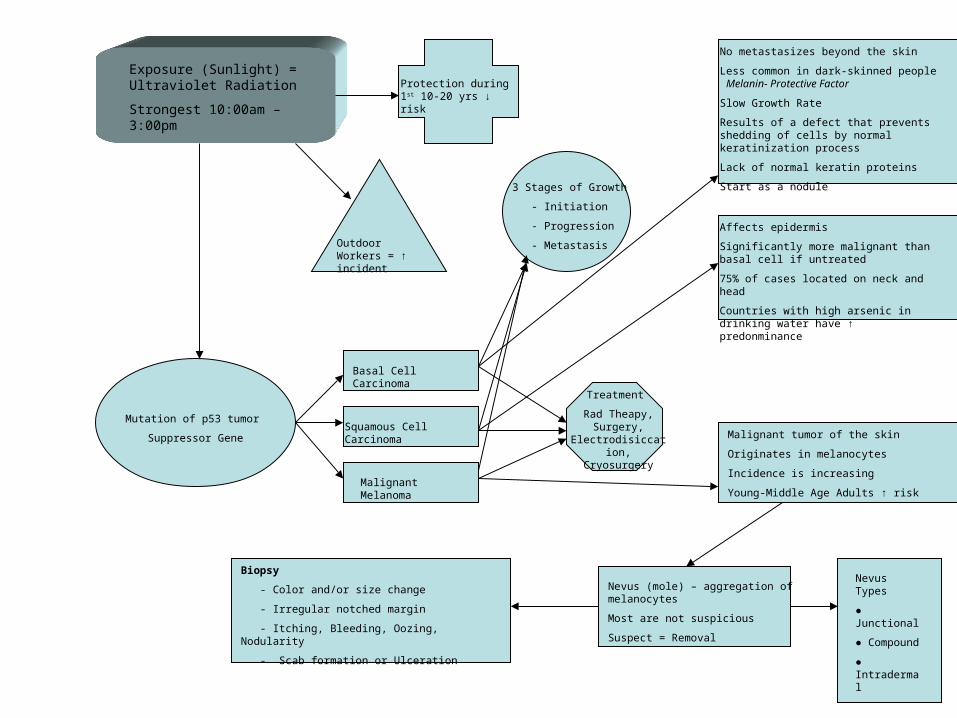
Exposure (Sunlight) = Ultraviolet Radiation
Strongest 10:00am – 3:00pm
Protection during 1st 10-20 yrs ↓ risk
Mutation of p53 tumor
Suppressor Gene
Outdoor Workers = ↑ incident
Basal Cell Carcinoma
Squamous Cell Carcinoma
Malignant Melanoma
3 Stages of Growth
- Initiation
- Progression
- Metastasis
Treatment
Rad Theapy, Surgery,
Electrodisiccation, Cryosurgery
No metastasizes beyond the skin
Less common in dark-skinned people Melanin- Protective Factor
Slow Growth Rate
Results of a defect that prevents shedding of cells by normal keratinization process
Lack of normal keratin proteins
Start as a nodule
Affects epidermis
Significantly more malignant than basal cell if untreated
75% of cases located on neck and head
Countries with high arsenic in drinking water have ↑ predonminance
Malignant tumor of the skin
Originates in melanocytes
Incidence is increasing
Young-Middle Age Adults ↑ risk
Nevus (mole) – aggregation of melanocytes
Most are not suspicious
Suspect = Removal
Biopsy
- Color and/or size change
- Irregular notched margin
- Itching, Bleeding, Oozing, Nodularity
- Scab formation or Ulceration
Nevus Types
● Junctional
● Compound
● Intradermal
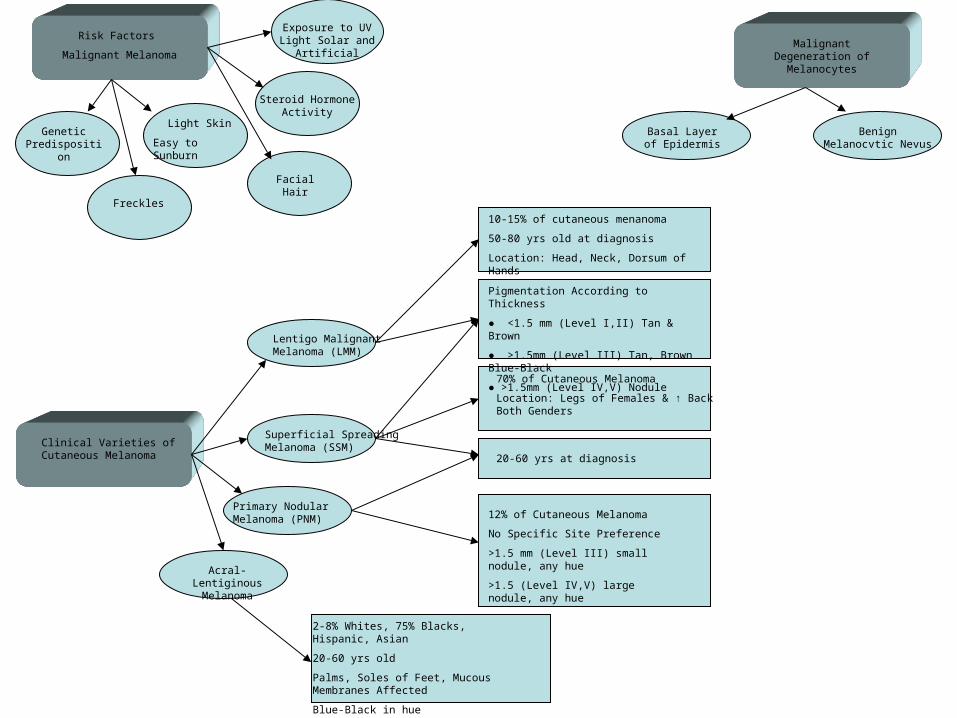
Clinical Varieties of Cutaneous Melanoma
Primary Nodular Melanoma (PNM)
Superficial Spreading Melanoma (SSM)
Lentigo Malignant Melanoma (LMM)
Malignant Degeneration of
Melanocytes
Basal Layer of Epidermis
Benign Melanocvtic Nevus
10-15% of cutaneous menanoma
50-80 yrs old at diagnosis
Location: Head, Neck, Dorsum of Hands
Pigmentation According to Thickness
● <1.5 mm (Level I,II) Tan & Brown
● >1.5mm (Level III) Tan, Brown Blue-Black
● >1.5mm (Level IV,V) Nodule
70% of Cutaneous Melanoma
Location: Legs of Females & ↑ Back Both Genders
20-60 yrs at diagnosis
12% of Cutaneous Melanoma
No Specific Site Preference
>1.5 mm (Level III) small nodule, any hue
>1.5 (Level IV,V) large nodule, any hue
Risk Factors
Malignant Melanoma
Genetic Predisposition
Facial Hair
Freckles
Light Skin
Easy to Sunburn
Steroid Hormone Activity
Exposure to UV Light Solar and Artificial
Acral-Lentiginous Melanoma
2-8% Whites, 75% Blacks, Hispanic, Asian
20-60 yrs old
Palms, Soles of Feet, Mucous Membranes Affected
Blue-Black in hue
References:Corwin, E. J. (2000). Handbook of Pathophysiology (2nd ed.). Philadelphia, PA: Lippincott.
Nicol, N. H. & Huether, S. E. (2006). Alterations of the integument in children. In K. L. McCance & S. Huether (Eds.), Pathophsiology: The Biologic Basis for Disease in Adults & Children (pp.1609- 1623). St Louis, MO: ElSevier Mosby.
Nicol, N. H., Huether, S. E. & Weber, R. (2006). Structure, function, and disorders of the integument. In K. L. McCance & S. Huether (Eds.), Pathophsiology: The Biologic Basis for Disease in Adults & Children (pp.1573-1607). St Louis, MO: ElSevier Mosby.