Embed Size (px)
Citation preview

ALS
Lori Hoffman, MS, ANP-BC, MSCN
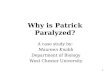
Amyotrophic Lateral Sclerosis (ALS)
First described by
Jean-Martin Charcot in 1874
Rapidly progressive neurologic disease that causes degeneration of motor neurons and ends in death
Commonly known as “Lou Gehrig’s Disease”
Lou Gehrig

Epidemiology
• Uniform distribution worldwide—no regards to race, ethnicity or socioeconomics
• •Annual incidence is 2 per 100,000 people
• •Most common age of onset 40-60 years of age
• •Men more often affected than women
• •Average life expectancy is 2-5 years from time of diagnosis. – However, the disease is variable approximately:
• 20% will live 5+ years after diagnosis
• 10% will live 10+ years after diagnosis
• 5% will live 20+ years after diagnosis

Neuron Degeneration
• Both upper motor neurons (UMNs) and lower motor neurons (LMNs) degenerate in ALS.
• Results of denervation:
~from loss of LMNs, muscles become weak, atrophied, and begin to fasciculate.
~loss of UMNs = spasticity and stiffness
•Other types of neurons are not affected in this disease

Symptoms
• Early symptoms are often mild, overlooked and attributed to something else
• Weakness in one or more limbs
– Tripping, difficulty with sports, difficulty on stairs
Fasiculations
Spasticity
Difficulty with speech
Diagnosis
• electrodiagnostic tests including electomyography (EMG) and nerve conduction velocity (NCV)
• blood and urine studies including high resolution serum protein electrophoresis, thyroid and parathyroid hormone levels and 24-hour urine collection for heavy metals
• spinal tap • x-rays, including magnetic resonance imaging (MRI) • myelogram of cervical spine • muscle and/or nerve biopsy • thorough neurological examination
Treatment
• Riluzole (Rilutek®)
50mg PO BID
Best Practices
• Who should manage these patients?
Neurology?
Medicine?
Pulmonology?
Primary Care?
Home Based Care?
Spinal Cord Injury?

Multidisciplinary Approach
• Complex needs require a team of specialists working together
• Syracuse VA approach to ALS Care – Neurologist handles medical management
– SCI team handles symptomatic care and functional needs
– Pulmonary is involved early
– SLP is involved early
– Patients often co-follow with ALS Clinic at University Hospital

Focus on Symptom Management
• Breathing
• Swallowing/Sialorrhea
• Speech
• Pain
• Paralysis
• Depression
Supportive Care
• Breathing
– Restriction
• BiPAP--pressurized air is delivered at two alternating levels. The inspiratory positive airway pressure is higher and supports a breath as it is taken in. The expiratory positive airway pressure is a lower pressure that allows you to breathe out.
• AVAP--Average Volume Assured Pressure Support—non invasive home ventilation
• Ventilator
Nursing Considerations
• Discussions regarding wishes for mechanical ventilation need to be had early
• Fit of masks
• Tolerability of BiPap/AVAP/Ventilator
• Anxiety
• Skin breakdown
• Care of equipment
• Is there a caregiver that can manage it???
Dysphagia
Wishes regarding PEG tube need to be made relatively early. PEG tubes need to be put in prior to FVC being <50% of predicted A patient may need to have a tube put in before they start having difficulty swallowing A patient may go from no trouble breathing/swallowing to a lot of trouble very quickly Speech Language Pathologist should be consulted for swallow evaluation and follow regularly Thickened liquids may be necessary Even with severe dysphagia, patients may elect for some food/drink for oral gratification

PEG TUBE WISDOM
Education!!!
PEG tube will not prolong life
Having a way to provide fluids and medications will increase comfort
Best outcomes when put in under interventional radiology
Try to get pt admitted and kept overnight to monitor for complications
Designate someone to troubleshoot skin problems, tube problems once the pt goes home
Have dietician on board ahead of time to give tube feed/flush orders
Communication
• “Augmentative/Alternative Communication” (AAC)
• Eye Gaze software
Pain
• Make sure that pain is managed
• Frequently complain of shoulder pain, as arms hang
• Remember, ALS patients may be paralyzed, but they are sensory intact
• Spasticity can be painful…manage spasticity
Meeting Jim
• 56yo male with a 3 month history of right arm weakness who was referred to Neurology Clinic.
• PMH: none • Social Hx: employed full time in supervisory capacity
working with computers. Married. Living w/ spouse in a split level home with 4 steps to enter, bed and bathroom on the 2nd floor. Has 2 sons in college and 2 adult children who live out of state. Has supportive wife who does not work. Smokes tobacco. No ETOH or illicit drug use.
• Medications: none • Symptoms: insidious onset right arm weakness that he
attributes to a golf injury
Exam/Work Up
• Neurologic exam: – VS: T 98.6, HR 90, RR 18, BP 120/70, O2 sat 99% on r/a. – CN II-XII intact – hyper-reflexic – fasiculations in the arms and legs – Strength is 4/5 in the left upper extremity and is 3+ to 4- in the right
biceps, triceps, and 3+/4 intrinsics. Hip flexors 4/5, otherwise LE’s 5/5 – Sensation intact to light touch and pinprick – Proprioception intact – Coordination intact – Ambulates with steady gait.
• MRI Brain and C Spine: negative for any brain lesions or spinal cord lesions.
• Labwork was normal.

Further Testing
• Neurology sent pt for EMG which showed the presence of simultaneous acute denervation potentials with chronic denervation potentials in the right upper extremity, right lower extremity, left lower extremity, right T7 paraspinal muscles, and the acute denervation
potentials in the right masseter--consistent with motor neuron disease
Diagnosis
Prior to seeing the pt in clinic---
– Neurologist read EMG and determined pt had ALS.
– WHAT CONSIDERATIONS COME TO MIND WHEN DIAGNOSING THIS PATIENT?
BEST PRACTICES
– Neurologist called Social Worker and gave “heads up”
– Social Worker planned to meet w/ pt and spouse at the appt where pt would get diagnosis
– Neurologist met w/ pt “face to face” and gave diagnosis
– Patient and wife have another member of the team to call for support once this starts to sink in
Immediate Needs
What are the immediate medical needs?
Riluzole 50mg PO BID
Check PFT’s for a baseline
Pneumovax and flu vaccination as appropriate
What other needs can we anticipate him needing in the short term?

3 months later
• Jim returns to his 3 month follow up with Neurology and had PFT’s prior to the visit
• FVC 55% of predicted, FEV1 50% of predicted • He is starting to slur his speech, he is noticed to have excessive saliva. • His arms have gotten noticeably weaker, but he is able to wipe the saliva from his
mouth, but by bending his mouth down to his hands • He is still ambulatory, but slowly • Exam shows that his legs are 3+/4- strength, his arms are trace shoulders, trace
biceps, trace triceps, and 2/5 wrist extensors and 2/5 intrinsics. • He denies any difficulty swallowing, but his wife notes that he is not eating much
and often coughs when he eats • His wife is still working her full time job as a teacher • Jim is home alone all day • He is continent of bladder and bowel • He spends most of his day sitting in the recliner watching tv • His wife reports exhaustion and is coming home from work at lunchtime to assist
him with feeding and toileting
What are Jim’s Needs?
• Declining PFT’s
• Sialorrhea
• Functional loss of arms
– Safety
– Falls
– Nutrition
– Toileting
– Bathing/Dressing
What We Did for Jim
• Referral made to IR for immediate PEG tube placement, as Jim wanted a PEG.
• He had this in the hospital, stayed overnight and things went well. While he was there, nursing did PEG teaching. SLP did a swallow eval as well as an assistive technology eval. He did well w/ his swallowing and did not need thickened liquids. He was suggested to be on a soft consistency diet. Dynavox was ordered in anticipation of continued progression of speech loss. OT saw pt and ordered a power w/c head array and attendant control. They also ordered ROHO cushion. Social Work set him up w/ a Life Alert system and Advanced Directives were done. However, he still wanted to be FULL CODE. He was resistant to accept a home health aide, but we offered. He was started on a scopolamine patch to dry secretions. Jim was reluctant to meet w/ the Psychologist.

6 months after diagnosis
• Jim’s wife calls the social worker upset. Jim is having difficulty breathing and has a fever. The Social Worker instructs wife to call 911. Pt is brought to ER where he is admitted w/ pneumonia. He is placed in ICU for 24 hours, then moved to SCI floor. He is being treated with antibiotics for pneumonia and responding well. He was on BiPap in ICU and then weaned to just at HS and prn. He is seen by SLP and he is aspirating all consistencies. It is recommended that he have all nutrition and fluid per PEG, and be NPO d/t risk of aspiration.
• Jim is accepting of this during his hospitalization until day #5 of hospitalization, when he started hysterically crying because he wanted chocolate milk. Nursing has grown quite attached to Jim and is feeling emotional. There is an NPO order in the chart. Jim has not yet come to terms fully with his disease and still wants to be “FULL CODE”
What Is The Right Answer?
• What emotions does this bring up for you?
• How would you have handled it?

9 months after diagnosis
• Jim is quadriplegic from ALS. He still retains sensation. He is fed formula by tube and gets oral swabs for his mouth. He can use eye gaze software to communicate. He requires BiPap almost around the clock. He is verbalizing that he is ready to die and does not want to live like this any longer. He remains cognitively intact. His wife has taken a sabbatical from her teaching job and is caring for him full time. They have a home health aide 2 hours 7 days per week, which is not enough.
• Jim cannot put the bipap on or take it off himself. He would like to stop the bipap all together.
• His wife is having a difficult time accepting this and wants pt to consider ventilation.

Palliative Care
• Jim’s right to choose
• Hospice consult

![Linking RNA Dysfunction and Neurodegeneration in ...Amyotrophic lateral sclerosis (ALS) was initially described over 100 years ago by Jean-Martin Charcot [1], and is now recognized](https://img.pdfslide.us/doc/110x75/60eced5e6c40c757204b5ec3/linking-rna-dysfunction-and-neurodegeneration-in-amyotrophic-lateral-sclerosis.jpg)