Embed Size (px)
Citation preview

Companion animalS
524 In Practice October 2013 | Volume 35 | 524-530
doi:10.1136/inp.f5826
Derek Flaherty qualified from the University of Glasgow in 1988, after which he spent six years working for the PDSA before returning to Glasgow to undertake a residency in veterinary anaesthesia. He is both an RCVS and a European recognised specialist in veterinary anaesthesia and analgesia. He is currently professor of veterinary anaesthesia and analgesia at the University of Glasgow, with a special interest in total intravenous anaesthetic techniques.
AlphA2-Adrenoceptor agonists (alpha2-adren-ergic agonists or, more simply, alpha2-agonists) were first introduced into veterinary practice in the early 1960s for the purposes of premedication and seda-tion; however, for many years, their use in small ani-mals received a ‘bad press’ because of the significant side effects seen. With time, greater appreciation of the unique pharmacological characteristics of these agents and a better understanding of appropriate dose rates has led to increased acceptance of the effects they produce, and they are now extensively used in small animal practice.
Alpha2-adrenergic receptors (adrenoceptors) are widely dispersed throughout the body, at pre-, post- and extra-synaptic sites, and are an integral compo-nent of sympathetic nervous system activity. It is now recognised that at least three subtypes of these recep-tors exist, each with distinct functions, and this may potentially allow future development of drugs that are selective for one or more of the subtypes, rather than exhibiting generalised agonist effects across all three. It is possible, therefore, that it may become feasible to specifically target the beneficial effects (that is, seda-tion and analgesia) mediated by alpha2-adrenergic receptors, while removing some of the less desirable effects (that is, alterations in cardiovascular function).
Alpha2-agonist drugs
three alpha2-agonists are currently available for use in dogs and cats in the UK: xylazine, medetomidine and dexmedetomidine (Fig 1). Although romifidine also previously gained market authorisation, it is no longer produced for small animals, although it continues to be extensively used in equine practice; it appeared to offer no significant advantages over medetomidine or dexmedetomidine for dogs and cats in any case. All of the available alpha2-agonists additionally bind, to varying extents, to alpha1-adr-energic receptors and this presents two main issues:
some of the undesirable cardiovascular side effects are mediated through the alpha1-adrenoceptor, and it is more difficult to develop a specific antagonist for drugs that bind to multiple receptors. In terms of the three alpha2-agonists presently available for small animal use, both medetomidine and dexme-detomidine demonstrate approximately a 10-fold greater specificity for the alpha2-adrenergic receptor than seen with xylazine use. the consequences of this are that xylazine displays some adverse effects on the cardiovascular system that medetomidine and dex-medetomidine do not, and also that – although xyla-zine can be antagonised by atipamezole – the actions it mediates through the alpha1-adrenoceptor remain, since atipamezole is a specific antagonist at the alpha2-adrenoceptor. consequently, in the author’s opinion, there is little to justify the continued use of xylazine in small animal practice when more specific (‘cleaner’) drugs exist.
Alpha2-adrenoceptor agonists are widely used for premedication, sedation and, more recently, provision of analgesia in small animal practice. However, although these drugs may offer significant benefits over alternative agents, they also have a number of side effects that must be appreciated. This, the first in a series of two articles, explains how the pharmacology of these drugs leads to both the desirable and adverse effects observed with these agents. The second article, which will be published in a forthcoming issue of In Practice, will describe the most appropriate way to use alpha2-adrenoceptor agonists to optimise their clinical effects.
Derek Flaherty
Alpha2-adrenoceptor agonists in small animal practice 1. Why they do what they do
Fig 1: Xylazine, medetomidine and dexmedetomidine are all licensed for use in dogs and cats in the UK. There are now two commercial preparations of dexmedetomidine available, one containing 0.5 mg/ml (Dexdomitor) and one containing 0.1 mg/ml (Dexdomitor 0.1)
Flaherty_IDmanuscript.indd 524 26/09/2013 16:10
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animalS
525In Practice October 2013 | Volume 35 | 524-530
Medetomidine is a racemic mixture consisting of 50 per cent dexmedetomidine and 50 per cent levome-detomidine. dexmedetomidine is the active isomer in the mix, providing all the sedative and analgesic com-ponents of medetomidine. levomedetomidine, on the other hand, is an inactive isomer, and does not con-tribute to either of these effects. In essence, dexme-detomidine is the ‘purified’ form of medetomidine, in that it provides all the effects veterinary surgeons are actually seeking. It may be questioned if there is any issue with having levomedetomidine in the mixture if it is inactive; in actual fact, although it is described as ‘inactive’ – in that it produces no direct effect when it binds to alpha2 receptors – its presence potentially has a number of undesirable effects when it is co-administered alongside dexmedetomidine (as occurs when racemic medetomidine is given). By binding to alpha2 receptors, levomedetomidine inhibits access by dexmedetomidine to these receptors, thereby ‘blunt-ing’ the latter’s actions; in other words, levomedetomi-dine may potentially reduce the sedative and analgesic actions of dexmedetomidine. In addition, there is some suggestion from experimental studies that levo-medetomidine may worsen the cardiovascular effects of dexmedetomidine. Finally, elimination of levome-detomidine from the body requires hepatic metabo-lism and it has been demonstrated that this may delay elimination of certain other drugs from the body. In particular, hepatic clearance of ketamine may be delayed and result in a greater ‘hangover’ effect from this drug. Although each of these potential adverse effects of levomedetomidine has been demonstrated experimentally, at the moment there is little evidence that these necessarily translate into major clinical sig-nificance. however, there is an increased ‘push’ to move away from racemic drug mixtures (many drugs that are used clinically are racemates) to using ‘purer’ drug preparations, and it may be that, over time, medetomidine becomes unavailable. In addition, the theoretical pharmacological advantages of dexme-detomidine over medetomidine cannot be denied.
Effect of alpha2-agonist drugs on bodily function
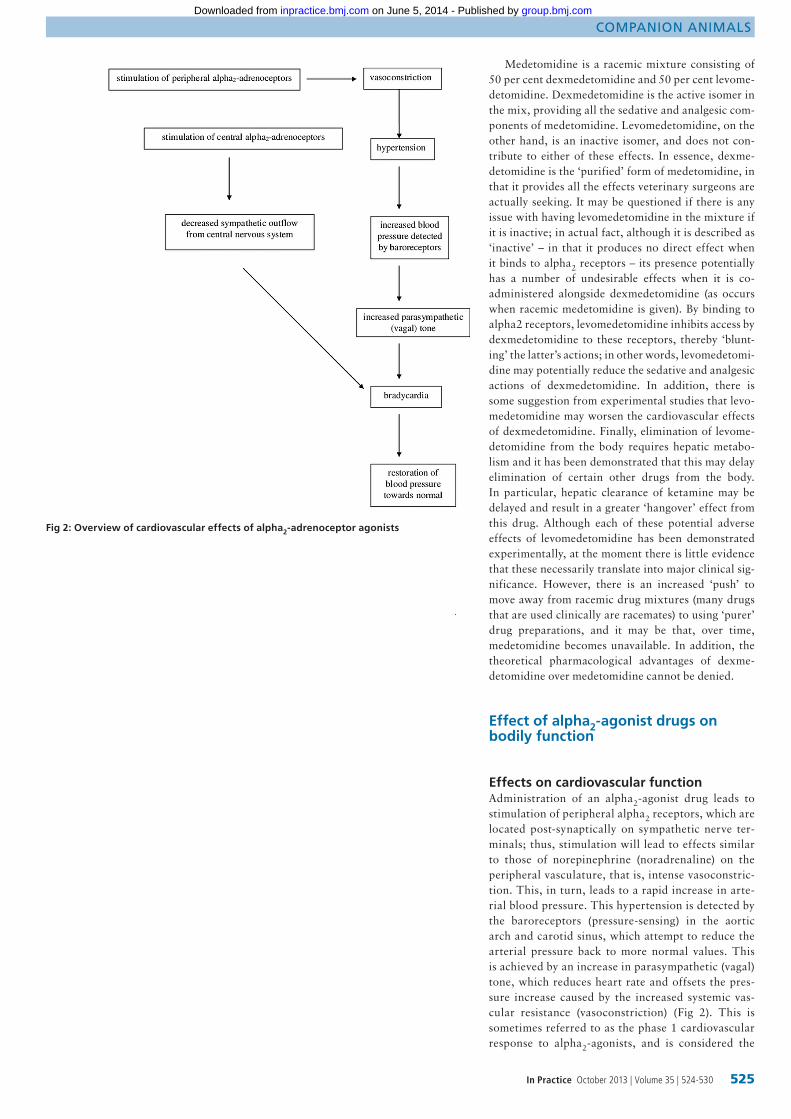
Effects on cardiovascular functionAdministration of an alpha2-agonist drug leads to stimulation of peripheral alpha2 receptors, which are located post-synaptically on sympathetic nerve ter-minals; thus, stimulation will lead to effects similar to those of norepinephrine (noradrenaline) on the peripheral vasculature, that is, intense vasoconstric-tion. this, in turn, leads to a rapid increase in arte-rial blood pressure. this hypertension is detected by the baroreceptors (pressure-sensing) in the aortic arch and carotid sinus, which attempt to reduce the arterial pressure back to more normal values. this is achieved by an increase in parasympathetic (vagal) tone, which reduces heart rate and offsets the pres-sure increase caused by the increased systemic vas-cular resistance (vasoconstriction) (Fig 2). this is sometimes referred to as the phase 1 cardiovascular response to alpha2-agonists, and is considered the
Fig 2: Overview of cardiovascular effects of alpha2-adrenoceptor agonists
Flaherty_IDmanuscript.indd 525 26/09/2013 16:10
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from

Companion animalS
526 In Practice October 2013 | Volume 35 | 524-530
principle reason for the bradycardia during the first 20 minutes or so following administration of medeto-midine/dexmedetomidine.
In addition to these peripheral effects, the alpha2-agonist will cross the blood-brain barrier and exert central effects. the majority of alpha2-adrenergic receptors are located pre-synaptically in the central nervous system (unlike peripherally, where they are largely post-synaptic); in this situation, they exert a negative feedback effect on release of norepineph-rine from the nerve terminal, eliciting a decrease in sympathetic nervous system function -- this results in production of sedation, but also maintains the reduced heart rate due to decreased sympathetic tone (often referred to as the phase 2 cardiovascular response). traditionally, the overall effect on arterial blood pres-sure resulting from these alterations in cardiovascular function was described as ‘bi-phasic’, in that there is an initial hypertensive phase followed by a subsequent reduction in blood pressure that has previously been referred to as ‘hypotension’, that is, hypertension fol-lowed by hypotension. In actual fact, the vast major-ity of studies examining the cardiovascular effects of these drugs in small animals demonstrate that, while blood pressure does indeed increase, it then tends to return to approximately normal levels (or occasionally slightly below normal) when the compensatory brady-cardia is initiated. despite the commonly held belief that alpha2-agonists cause hypotension, this appears to be rare and blood pressure is actually generally well maintained at approximately normal levels following the initial hypertension.
It is important to remember, however, that although blood pressure is maintained, this is due to
the profound vasoconstriction, and occurs in the face of marked reductions in cardiac output (often greater than 50 per cent), due to both the marked bradycardia and also the increased afterload. peripheral vasocon-striction is also the reason for the pale mucous mem-branes commonly observed in animals treated with alpha2-agonists (Fig 3).
It will be apparent from the preceding discus-sion that many of the undesirable cardiovascular effects of alpha2-agonists are related to stimulation of peripheral alpha2-adrenergic receptors, while the desirable sedative and analgesic effects are produced centrally. thus, if it were possible to ‘block’ these peripheral effects while maintaining central activ-ity, this would be advantageous. A peripheral-acting alpha2-antagonist known as MK-467 has been inves-tigated in a number of experimental studies, and has been shown to attenuate or prevent the haemo-dynamic changes associated with administration of alpha2-agonists, while maintaining the desirable effects. Although not yet commercially available, this drug may offer potential for future co-administration alongside alpha2-agonists in the clinical setting.
Effects on tissue perfusionthe logical question to ask, based on the low cardiac output and marked vasoconstriction, is whether tis-sue perfusion is therefore likely to be impaired follow-ing administration of alpha2-agonists. Most studies have demonstrated that, although organ blood flow is reduced with these drugs, it is still sufficient to pro-vide ‘adequate’ perfusion, chiefly based on the fact that tissues maintain aerobic metabolism while under the influence of alpha2-agonists, and therefore appear to be obtaining sufficient oxygen from the circulat-ing blood. laboratory-based studies of this nature, however, are generally performed on healthy animals, and the reduction in tissue perfusion may not be toler-ated by patients with organ function that is already impaired for whatever reason. In these cases, it is pos-sible that the reduced oxygen/nutrient delivery to the tissue may be sufficient to induce further tissue dam-age with subsequent organ failure. consequently, great care must be taken whenever these drugs are administered to animals with any evidence of organ impairment; this would include geriatric patients, where organ dysfunction may be more likely. It is also important to remember that pre-anaesthetic blood screening may not identify organ impairment in all cases; in particular, approximately 75 per cent of func-tional renal mass must be lost before increases in urea/creatinine may be seen.
If alpha2-agonists are to be used in geriatric ani-mals, it is important that only low doses are admin-istered to minimise the effects on the cardiovascular system, since functional cardiovascular reserve may be limited even in seemingly healthy geriatrics.
Effects on heart rhythmIn addition to having a significantly lower alpha2:alpha1 ratio compared to medetomidine and dexmedetomi-dine, and thus being a relatively ‘dirty’ drug, xylazine also sensitises the heart to the effects of epinephrine and norepinephrine, and may lead to severe cardiac arrhythmias including ventricular fibrillation. this may
Fig 3: Before (a) and after (b) photos of a dog that has been administered 10 µg/kg medetomidine combined with 0.1 mg/kg butorphanol, intravenously. Note the pale mucous membranes in (b), as well as cyanosis of the tongue
(a)
(b)
Flaherty_IDmanuscript.indd 526 26/09/2013 16:10
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from
Companion animalS
529In Practice October 2013 | Volume 35 | 524-530
account for the high mortality rate associated with this agent in some small animal anaesthetic mortality stud-ies (Clarke and Hall 1990). Medetomidine and dexme-detomidine, on the other hand, have been demonstrated either to have no effect on myocardial sensitisation or to produce a protective effect against catecholamines; thus, the latter appear to be ‘safer’ agents from a cardio-vascular standpoint when compared to xylazine.
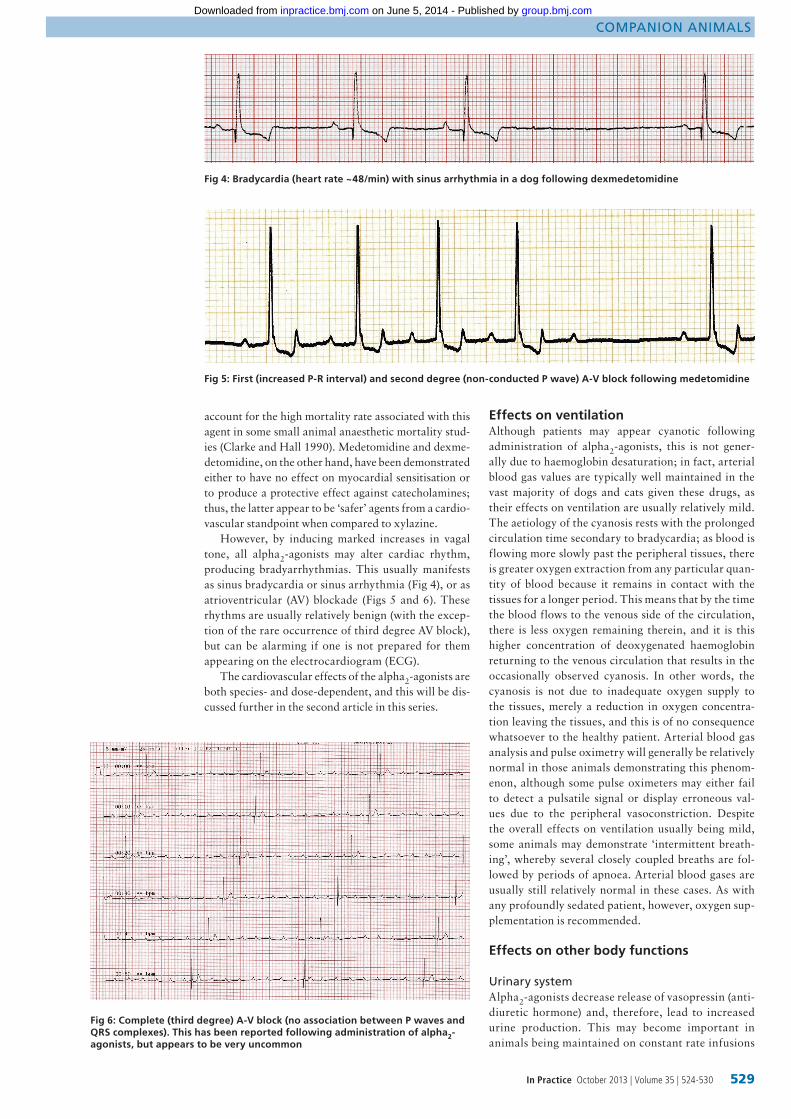
However, by inducing marked increases in vagal tone, all alpha2-agonists may alter cardiac rhythm, producing bradyarrhythmias. This usually manifests as sinus bradycardia or sinus arrhythmia (Fig 4), or as atrioventricular (AV) blockade (Figs 5 and 6). These rhythms are usually relatively benign (with the excep-tion of the rare occurrence of third degree AV block), but can be alarming if one is not prepared for them appearing on the electrocardiogram (ECG).
The cardiovascular effects of the alpha2-agonists are both species- and dose-dependent, and this will be dis-cussed further in the second article in this series.
Fig 4: Bradycardia (heart rate ~48/min) with sinus arrhythmia in a dog following dexmedetomidine
Fig 5: First (increased P-R interval) and second degree (non-conducted P wave) A-V block following medetomidine
Fig 6: Complete (third degree) A-V block (no association between P waves and QRS complexes). This has been reported following administration of alpha2- agonists, but appears to be very uncommon
Effects on ventilationAlthough patients may appear cyanotic following administration of alpha2-agonists, this is not gener-ally due to haemoglobin desaturation; in fact, arterial blood gas values are typically well maintained in the vast majority of dogs and cats given these drugs, as their effects on ventilation are usually relatively mild. The aetiology of the cyanosis rests with the prolonged circulation time secondary to bradycardia; as blood is flowing more slowly past the peripheral tissues, there is greater oxygen extraction from any particular quan-tity of blood because it remains in contact with the tissues for a longer period. This means that by the time the blood flows to the venous side of the circulation, there is less oxygen remaining therein, and it is this higher concentration of deoxygenated haemoglobin returning to the venous circulation that results in the occasionally observed cyanosis. In other words, the cyanosis is not due to inadequate oxygen supply to the tissues, merely a reduction in oxygen concentra-tion leaving the tissues, and this is of no consequence whatsoever to the healthy patient. Arterial blood gas analysis and pulse oximetry will generally be relatively normal in those animals demonstrating this phenom-enon, although some pulse oximeters may either fail to detect a pulsatile signal or display erroneous val-ues due to the peripheral vasoconstriction. Despite the overall effects on ventilation usually being mild, some animals may demonstrate ‘intermittent breath-ing’, whereby several closely coupled breaths are fol-lowed by periods of apnoea. Arterial blood gases are usually still relatively normal in these cases. As with any profoundly sedated patient, however, oxygen sup-plementation is recommended.
Effects on other body functions
Urinary systemAlpha2-agonists decrease release of vasopressin (anti-diuretic hormone) and, therefore, lead to increased urine production. This may become important in animals being maintained on constant rate infusions
Flaherty_IDmanuscript.indd 529 26/09/2013 16:10
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from

Companion animalS
530 In Practice October 2013 | Volume 35 | 524-530
(CRIs) of these drugs, and allowance may have to be made for increased fluid losses.
Gastrointestinal tractAlthough alpha2-agonists may cause vomiting, this is much less common with medetomidine and dex- medetomidine than it is with xylazine. However, the potential still exists and these drugs should be avoided in situations where vomiting may be detrimental to the animal. These drugs also cause slowing of the gastro-intestinal tract, and this must be taken into account if one is interpreting radiographic contrast studies of this area.
In addition, alpha2-agonists block insulin release from the beta cells of the pancreas leading to hypergly-caemia. This is generally not of sufficient magnitude to exceed the renal threshold for glucose (so glycosu-ria is not usually a feature) but elevated blood glucose may be seen in animals sampled under the influence of these drugs, and it is important that diabetes mellitus is not diagnosed on this basis.
Pregnancy/uterine effectsAlpha2-agonists may case fetal abnormalities if admin-istered in the first trimester of pregnancy, and prema-ture parturition in the last trimester. Therefore, their use in pregnant animals should only be undertaken following a careful assessment of the risk:benefit ratio. None of these drugs currently has a licence for preg-nant animals in the UK.
Summary
The alpha2-adrenoceptor agonists have a range of pharmacological features that markedly impact on how these drugs behave in a clinical setting, and an appreciation of these effects is necessary for their safe use and to gain maximum benefit from their desir-able characteristics. ‘Modern’ alpha2-agonists, such as dexmedetomidine, may offer significant benefits over most of their predecessors.
AcknowledgementsThe author would like to thank Paul Wotton for sup-plying the ECG traces.
ReferenceCLARKE, K. W. & HALL, L. W. (1990) A survey of anaesthesia in small animal practice: AVA/BSAVA report. Veterinary Anaesthesia and Analgesia 17, 4-10
Further readingMURRELL, J. C. & HELLEBREKERS, L. J. (2005) Medetomidine and dexmedetomidine: a review of cardiovascular effects and antinociceptive properties in the dog. Veterinary Anaesthesia and Analgesia 32, 117-127
Flaherty_IDmanuscript.indd 530 26/09/2013 16:10
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from
doi: 10.1136/inp.f5826 2013 35: 524-530In Practice
Derek Flaherty
doanimal practice 1. Why they do what they -adrenoceptor agonists in small2Alpha
http://inpractice.bmj.com/content/35/9/524.full.htmlUpdated information and services can be found at:
These include:
References http://inpractice.bmj.com/content/35/9/524.full.html#ref-list-1
This article cites 2 articles
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on June 5, 2014 - Published by inpractice.bmj.comDownloaded from














![Adrenoceptor Agents [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/577d26cc1a28ab4e1ea236f9/adrenoceptor-agents-compatibility-mode.jpg)














