Embed Size (px)
Citation preview

209
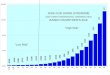
MEAN SERU,A-IIAMUNGGLOBULINS (mg/dl) IN 19 PATIENTS WITHRHEUMATOID ARTHRITIS BEFORE AND AFTER LEVAMISOLE TREATMENT
stimulation of skin delayed-hypersensitivity tests was associatedwith depression of serum-immunoglobulins. This observationis consistent with the findings of Huskisson et al.3 A late de-crease in antibody titres was observed by Renoux et al. inelderly levamisole-treated patients immunised with influenzavaccine. Levamisole should therefore be considered rather asan immunomodulating agent than as a general immunostimu-lant. Yaron et al. gave an indication that levamisole can havean anti-inflammatory action independent of its effect on theimmune system. We are tempted to suggest that further com-parisons between the clinical effects of levamisole and im-
munoreactivity and intensity of inflammatory process in R.A.would make it possible to select patients who could benefitfrom this drug. H. SZPILMAN
S. LUFTD. GLIŃSKA-URBANW. FISCHERM. PLACHECKA
Institute of Rheumatology,Spartańska 1,02-637 Warsaw, Poland
ALPHA-FETOPROTEIN ASSAY IN ALLAMNIOCENTESIS SAMPLES
SIR,-We envy Broch and Scrimgeour’s false-positive rateof zero,8 and suspect we understand the reason. They regardan amniotic-fluid sample containing fetal blood as unusable,while our results9 simply reflect a total experience withoutprior sample selection. We do not feel that a sample contami-nated with fetal blood should be discarded since some 47% offluids derived from pregnancies where the fetus had anen-cephaly contained fetal hoemoglobin.10 Since fetal blood seemsto be present so often in these particular cases, repeat amnio-centeses may be of no avail.We have lately been able to modify our assay, which is now
more sensitive. Over 800 samples have been re-assayed, includ-ing the 15 (0-4) reported as "definite" false positives out ofthe 3536 cases studied.2 With the modified assay, only 5 ofthese now remain with A.F.P. values >3 S.D. above the mean.This suggests a very similar false-positive rate z 1%) to thatreported in the European Medical Research Council report."Since we have not re-assayed all 3536 cases, our exact ratecannot now be stated, but it is clearly in the range whereroutine A.F.P. assays of all amniotic fluids would be justified.Even by declaring samples with fetal haemoglobin unusable,
we predict that a zero false-positive rate will not be main-tained. We offer ultrasound and amniographic studies as addi-tional approaches when faced with borderline elevations ofA.F.P., and do not rely solely on the A.F.P. value.Eunice Kennedy Shriver Center,W altham, and MassachusettsGeneral Hospital,Boston, Massachusetts, U S A
AUBREY MILUNSKYMARGARET E. KIMBALL
6 Renoux, G . Renoux, M., Morand, P., Dartigues, P. Rev. med. Tours, 1973,7, 797.
7 Yaron, M. Yaron, I., Herzberg, M Lancer, Feb. 14, 1976, p. 3698 Brock, D J H., Scrimgeour, J. B Lancet, 1976, i, 1404.9 Milunsky, A . Alpert, E. ibid. 1976, i, 1015.10 Milunsky, A.. Alpert, E Obstet Gynec. in the press .11 Lindsten, J, Zetterstrom, R., Ferguson-Smith, M. in Prenatal Diagnosis of
Genetic Disorders of the Fœtus. I N.S.E R.M., Paris, 1976.
THE HEPARIN-THROMBIN CLOTTING-TIME
SIR,-The heparin-thrombin clotting-time (H.T.C.T.) isreferred to in your exemplary editorial’ about antithrombinand the diagnosis of prethrombotic states. In case there’couldbe any confusion, I write to emphasise that this H.T.c.T. testis not influenced by antithrombin levels. Since we use the pa-tient’s plasma as substrate, theoretically such an influence ispossible; however, we accept an H.T.c.T. result only if a dilute-thrombin clotting-time is strictly normal.You refer to this test as possibly useful in distinguishing
between a diagnosis of acute myocardial infarction and "non-specific chest pain". We continue to find the H.T.c.T. valuablein this situation, but the most striking abnormality in true in-farction may not develop for two to four days. (The originalstudies were "between the first and the seventh day".)
I think the H.T.c.T. may have greater value in detecting aprethrombotic state; the test has twice shown significantlyshorter clotting-times in groups of patients studied long aftervarious kinds of thrombosis who presumably are at greater riskthan normal of further trouble_2 3
You do not mention that we think this test measures plateletfactor 4 released from platelets and so reflects the degree ofplatelet activation.
Portsmouth and South East HampshireDistrict Pathology Service,St. Mary’s Hospital, Portmouth PO3 6AG J. R. O’BRIEN
LEVAMISOLE AS ADJUNCT TO DAPSONE INLEPROSY
SIR,-Levamisole has a stimulatory effect on some aspectsof the cellular immunity mechanism of the host. The mechan-ism of action is unclear. It has been suggested that levamisolehas a immunostimulatory effect in leprosy patients with
depressed cell-mediated immunity.5 6 We have tried to find outif levamisole would affect the course of the disease in patientswith lepromatous and dimorphic leprosy treated with dapsone.
Patients with nodular lepromatous or nodular dimorphicleprosy took part in the study. These patients were receiving-dapsone, by mouth or by injection. Patients were evaluatedmonthly for clinical lesions and reactions. Clinical lesions weregraded zero or 1-4, 4 being a nodular lesion and zero beinga totally flat lesion (macule). The same observer graded theselesions every time but the treatment was unknown to theobserver. Smears were read and graded by the same laboratorypersonnel who did not know the patient’s name or treatment.Sixteen patients were treated with dapsone 25mg by mouthevery day and four received 450mg acedapsone intramuscu-larly once every two months. These patients were advised totake an additional pill, which was either levamisole (150 mg)or placebo, one pill every two weeks.
At the end of six months of therapy, 12 patients finished thetrial from the 20 who had started. All 12 had been clinical
grade 4 at the start. The 6 who had been on levamisole inaddition to their dapsone (or acedapsone) had lesions of 1+ orzero at the end of the trial. Of the 6 patients taking placebo4 ended as -3 and 2 as 0. This is what one would expect tosee with dapsone alone.
1 Lancet, 1976, i. 13332. O’Brien, J. R, Etherington, M. D., Jamieson, S, Klaber, M. R . Lincoln,
S. V Thromb Diath. Hœmorrh 1974, 31, 2793 O’Brien, J R., Etherington, M. D., Jamieson, S., Lawford, P., Lincoln,
S V. Alkjaersig, N J ibid 1975, 34, 483.4 Symoens, J. in Proceedings of the 2nd International Conference on Modula-
tion of Host Resistance in the Prevention or Treatment of Induced Neo-
plasias Bethesda, 1975 edited by M A Chirigos U S Government
Printing Office in the press5 Cardama, J E., Gatti, J. C., Balina, I. H . Cabrera, H N, Fliess, L L Int.
J Leprosy, 1973, 41, 567.6 Saint-Andre, P., Louvet, M. Med Arm. 1976, 4, 223.