Embed Size (px)
Citation preview

Allogeneic Peripheral Blood Stem Cell Transplantation in Children WithHematologic Malignancies From HLA-Matched Siblings
Tsutomu Watanabe, MD,1* Teruyuki Kajiume, MD,1 Takanori Abe, MD,1
Yoshifumi Kawano, MD,1 Asayuki Iwai, MD,2 Tsuyako Iwai, MD,2
Yoichi Takaue, MD,3 and Yasuhiro Kuroda, MD1
Background. Despite the ethical problem ofusing granulocyte colony-stimulating factor (G-CSF) in normal children, allogeneic peripheralblood stem cell transplantation (PBSCT) mighthave advantages over allogeneic bone marrowtransplantation (BMT). Procedure. Eleven HLA-matched sibling donors aged 2–16 years re-ceived 10 µg/kg/day G-CSF for 5 days and un-derwent apheresis to harvest peripheral bloodstem cells (PBSC). PBSC were then cryopre-served until infusion. The 11 corresponding pa-tients aged 8 months to 14 years with high-riskhematological malignancies received busulfan(16 mg/kg or 600 mg/m2) and melphalan (210mg/m2) as a preparative regimen. Graft-versus-host disease (GVHD) prophylaxis consisted ofcyclosporine and methylprednisolone. Results.All of the donors tolerated G-CSF administra-tion and apheresis procedures. The patients re-ceived a median of 5.8 (range 1.4–11.5) × 106/kg CD34+ cells, 17.2 (3.8–36.0) × 105/kgcolony forming units-granulocyte/macrophage
(CFU-GM), and 3.5 (1.4–7.1) × 108/kg CD3+
cells. All of the patients showed prompt engraft-ment, with a median time to reach an absoluteneutrophil count (ANC) above 0.5 × 109/liter of10 (9–13) days. Grade I acute GVHD occurredin seven patients (64%), whereas grade II–IVacute GVHD was not seen. Chronic GVHD oc-curred in four patients (40%) among 10 patientsevaluable for chronic GVHD. Three patientsshowed extensive chronic GVHD. Currently,eight patients (73%) are alive and disease-freefor a median follow-up of 775 (103–1,069)days. Conclusions. Allogeneic PBSCT is fea-sible in the pediatric population, and PBSC har-vest is an alternative to BM harvest in donorswho are not eligible for BM harvest. Further-more, PBSC were successfully collected in pe-diatric donors with peripheral access. Thechoice of a stem cell source should be based onthe risk/benefit assessment for both patients anddonors. Med. Pediatr. Oncol. 34:171–176,2000. © 2000 Wiley-Liss, Inc.
Key words: allogeneic peripheral blood stem cell transplantation; HLA-matchedsibling donor; pediatric patients; hematologic malignancy
INTRODUCTION
Granulocyte colony-stimulating factor (G-CSF)–mobilized peripheral blood stem cell (PBSC) from nor-mal donors has been used in place of bone marrow (BM)in allogeneic hematopoietic stem cell transplantation[1–3]. There are practical advantages to using PBSCrather than BM as a stem cell source, including rapidhematopoietic reconstitution, fewer infectious complica-tions, and possible enhancement of the graft-versus-leukemia (GVL) effect [4,5]. However, most previousstudies have included only adult patient-donor pairs, andthere is still limited information available for the pediat-ric population [6–8]. PBSC collection in normal pediatricdonors is limited because of technical problems related tovascular access and the low total blood volume [9,10].More importantly, there is a growing ethical issue re-garding the use of G-CSF in normal children. Althoughthe short-term safety of G-CSF seems to be acceptable inadult donors, there is only limited experience in pediatricdonors [7,8]. The long-term toxicities of G-CSF treat-ment for children must be carefully assessed. We report
our experience with allogeneic PBSCT in pediatric pa-tients with hematologic malignancies transplanted fromHLA-matched siblings.
PATIENTS AND METHODSPatents and Donors
The patients (five males, six females; median age 8years, range 8 months to 14 years) were diagnosed withacute lymphoblastic leukemia (ALL; n4 5), acute my-elogeneous leukemia (AML; n4 3), myelodysplastic
1Department of Pediatrics, University of Tokushima School of Medi-cine, Tokushima, Japan2Kagawa Children’s Hospital, Zentuji, Japan3National Cancer Center Hospital, Tokyo, Japan
*Correspondence to: Tsutomu Watanabe, Department of Pediatrics,University of Tokushima School of Medicine, 3-18-15 Kuramoto-cho,Tokushima 770-8305, Japan.E-mail: [email protected]
Received 30 March 1999; Accepted 7 October 1999
Medical and Pediatric Oncology 34:171–176 (2000)
© 2000 Wiley-Liss, Inc.

syndrome (MDS; n4 2), or granulocytic sarcoma (n41) and underwent allogeneic PBSCT between May,1996, and December, 1998, at the University Hospital ofTokushima and Kagawa Children’s Hospital. The 11 cor-responding donors (seven females, four males) aged2–16 years (median 6 years) were HLA-matched sib-lings.
Before stem cell collection, the details of the proce-dure and risks of both BM harvest and PBSC collectionwere fully explained. The choice of PBSC as a stem cellsource was made by the donor’s guardian (or the donor ifover 16 years old). This choice was based on the medicalcondition of the donor [bronchial asthma (n4 5), obe-sity (n 4 1)] or the medical condition of the patients (n4 3). For the latter three donors, the choice of PBSC wasproposed in anticipation of rapid engraftment after allo-geneic PBSCT, because the patients were at high risksfor life-threatening infection (case 4, hepatosplenic can-didiasis; case 5, history ofStreptococcus mitisseptice-mia; case 11, methicillin-resistantStaphylococcus aureusinfection). In the remaining two donors, donor preferenceis a reason for preferring PBSC harvest. All of the do-nors’ guardians (or the donor if over 16 years old) pro-vided their written informed consent. This protocol wasapproved by the respective ethics committees of the Uni-versity Hospital of Tokushima and Kagawa Children’sHospital. Seven cases were sex-mismatched transplants.Two cases (cases 2 and 9) were a major blood-type-mismatched transplant, and another (case 3) was a minorblood-type-mismatched transplant.
PBSC Harvest
All of the donors received G-CSF (filgrastim, n4 7;lenograstim, n4 4) at a dose of 10mg/kg/day by sub-cutaneous injection for 5 days. On days 5 and 6 of G-CSFtreatment, donors underwent apheresis with a FenwallCS3000 Plus continuous cell separator, as described else-where [11]. Briefly, for withdrawal of blood, no centralvenous (CV) catheterization was used, and apheresis wasrun through a 20- to 24-gauge catheter in a radial arteryor a 17- to 20-gauge catheter in a cubital vein. For returnof blood, a cubital vein was used in all of the donors.Cannulation was performed without sedation. For donorsweighing less than 20 kg, the extracorporeal circuit waspreprimed with 150 ml of autologous blood or irradiatedleukocyte-depleted packed red blood cells. Autologousblood started to be collected 3 or 4 weeks before apher-esis and was drawn once per week. When blood wasdrawn the second or third time, previously saved bloodwas infused back into the donor, and 1.5 or 2 times thevolume of saved blood was drawn to prevent hypovole-mia and to save more fresh blood. A total of 150 ml ofblood was saved 1 week before apheresis to prime thefirst apheresis. At the end of the first apheresis, any bloodremaining in the machine was collected with the collec-
tion mode and used to prime the subsequent PBSC col-lection. Acid citrate dextrose (ACD) was used as an an-ticoagulant with a whole blood:anticoagulant ratio of12.7:1, and calcium gluconate was continuously admin-istered during apheresis to prevent ACD toxicity. Col-lection was performed without sedation in all of the do-nors. Two hundred to 300 ml/kg of blood (maximum 10liters) was processed at a time. Mononuclear cells(MNC) were isolated from apheresis products on Percollgradients [12] and then frozen and stored in a deepfreezer (−135°). For cell evaluation, cells were labeledwith fluorescence-conjugated anti-CD34 (HPCA) andCD3 (Leu 4) and analyzed using a flow cytometer. Forgranulocyte-macrophage colony-forming units (CFU-GM), cells were plated in quadruplicate using semisolidmedium after adding a combination of growth factors.Cultures were incubated for 14 days and colonies werescored. Cells were analyzed in each apheresis productand after thawing. Donors were followed up every 6months for blood counts.
Transplant Procedures
A combination of busulfan [4 mg/kg/day (cases 1, 2,4, 6, 8, 10, and 11) or 150 mg/m2/day (cases 3, 5, 7, and9) orally for 4 days, days −8 to −5] and melphalan (70mg/m2/day intravenously for 3 days, days −4 to −2) wasadministered to all of the patients as a preparative regi-men. Cryopreserved apheresis products were thawed andinfused 48 hr after conditioning.
Cyclosporin (CsA) and methylprednisolone (MP)were used for graft-versus-host disease (GVHD) prophy-laxis. CsA was given at a dose of 1.5 mg/kg in twice-daily intravenous infusions from day −1 until day +28,and then at 6–9 mg/kg/day orally. MP was administeredat a dose of 0.5 mg/kg in twice-daily intravenous infu-sions starting on day +5 until day +28 and then taperedand discontinued over 2 weeks. In the absence of chronicGVHD, CsA was gradually tapered from day +100 andstopped 4–6 weeks later. Diagnosis of GVHD was basedon clinical and histologic data as described by Deeg andCottler-Fox [13]. Biopsy of skin or oral mucosa wasperformed as necessary.
All of the patients were nursed in a filtered-air-flowsingle room and managed with mask and glove isolation.No gut decontamination was given. All of the patientsreceived intravenous hyperalimentation and blood prod-ucts when needed. All blood products were irradiated andfiltered. Acyclovir was administered at 7.5 mg/kg intra-venously every 12 hr from day +5 to day + 28. Intrave-nous immunoglobulin 300–400 mg/kg was given weeklyto day +100 and monthly thereafter until 1 year. Nogrowth factor was used in any of the patients after thetransplant, except in one patient (case 2) who sufferedfrom documented infection.
172 Watanabe et al.

Engraftment Analysis
Neutrophil recovery was defined as the first of 3 con-secutive days with an absolute neutrophil count of over0.5 × 109/liter , and platelet recovery was defined as theday the platelet count was 20 or 50 × 109/liter withoutplatelet transfusion support. Hematopoietic chimerismwas evaluated by fluorescence in situ hybridization(FISH) in sex-mismatched patient-donor pairs and byDNA restriction fragment length polymorphism (finger-print study) in sex-matched pairs.
RESULTSMobilization and Collection of PBSC
The acute toxicity of G-CSF in donors was acceptable.One donor (9%) complained of bone pain and arthralgia,which was easily relieved by analgesia. The procedurefor PBSC harvest was well tolerated, and no hemody-namic instability was noted during PBSC collection. Thenumber of aphereses required was two in six donors(55%) and three in five donors (45%). For priming of thecircuit before collection, two donors (18%) received ir-radiated leukocyte-depleted blood and another five(45%) received autologous blood. For drawing blood, aradial artery was used in 10 donors (2–14 years old; 91%)and a cubital vein was used in the remaining one donor(16 years old; 9%). The blood flow rate ranged from 30to 60 ml/min. During PBSC collection, no clinical evi-dence of hypocalcemia was observed. The platelet countdecreased in all of the donors. This decrease in the plate-let count became prominent following multiple apher-eses, and the donors thus required reinfusion of their ownplatelet-rich plasma that had been obtained during cellprocessing. However, there was no clinically significantbleeding. Blood examination showed no abnormalities inall of the donors within a median follow-up of 30 (range5–36) months.
Engraftment Results
The number of progenitor cells infused and engraft-ment results are shown in Table I. The patients receiveda median of 5.8 (range 1.4–11.5) × 106/kg CD34+ cells,17.2 (3.8–36.0) × 105/kg colony forming units-granulocyte/macrophage (CFU-GM), and 3.5 (1.4–7.1) ×108/kg CD3+ cells. All of the patients recovered theirperipheral blood cell counts. The median number of daysto a neutrophil count of greater than 0.5 × 109/liter was10 (range 9–13), whereas that to a platelet count ofgreater than 20 and 50 × 109/liter was 10 (8–32) and 16(11–45), respectively. At 1 month after transplant, FISHand fingerprint studies showed complete chimera in all ofthe patients except case 4, who showed mixed chimeraand subsequently relapsed on day +240.
GVHD
All of the patients were evaluable for acute GVHD,and 10 who survived 100 days or more were evaluablefor chronic GVHD (Table I). Clinical grades 0 andgrades I acute GVHD were observed in four (36%) andseven patients (64%), respectively. None of the patientsshowed clinical grade II–IV acute GVHD. ChronicGVHD developed in four patients (40%) after acuteGVHD. Three patients (30%) had extensive forms, in-volving the oral mucosa, eyes, upper gastrointestinaltract, liver, and lung. One patient (case 2) presented withclinical symptoms and findings similar to those of diffusesystemic sclerosis at day +300. Another patient (case 3)died from progressive lung disease probably related tochronic lung disease at day +539. The remaining patient(case 9) with extensive chronic GVHD was recoveringfrom gut, hepatic, and pulmonary GVHD with steroidtherapy. The median number of CD3+ cells infused was3.5 (range 1.4–7.1) × 108/kg, and this was not correlatedwith the development of acute GVHD (P 4 0.0925) orchronic GVHD (P 4 0.6493).
Infection and Other Toxicity
All of the patients became febrile shortly after trans-plant. However, fever subsided within 5 days in all of thepatients with antibiotic therapy. Four patients (36%) re-ceived intravenous amphotericin B during febrile epi-sodes. Documented CV catheter infection developed intwo patients (18%), and the identifiable pathogens wereStaphylococcus epidermis(case 2) andCandida albicans(case 7). Cytomegalovirus (CMV) antigenemia was seenin one patient (9%; case 1), who was successfully treatedwith ganciclovir.
Seven patients (64%) developed mild to moderate oro-pharyngeal pain, and one required narcotics to relievepain. Hemorrhagic cystitis occurred in two patients(18%) at day +60 (case 2) and day +90 (case 1). How-ever, urine cultures were negative for viruses in bothpatients. Renal dysfunction was mild, and none of thepatients developed a creatinine level of more than 2.0mg/dl. However, the dose of CsA had to be reduced inthree patients (cases 1, 2, and 4) because their creatininelevel was twice that pretransplant. Skin toxicity that waslikely to be related to busulfan was severe in one patient(case 2). One patient (case 8) died from hepatic venooc-clusive disease on day +63.
Outcomes
Two patients (18%) relapsed during the period of thisstudy. One patient (case 4) relapsed at day +240 and isnow in his second complete remission (CR) after beingtreated with chemotherapy combined with infusion of thedonor’s lymphocytes (DLI). Another (case 6) relapsed atday +229 and died from progressive disease at day +385.
Allogeneic PBSCT in Children 173
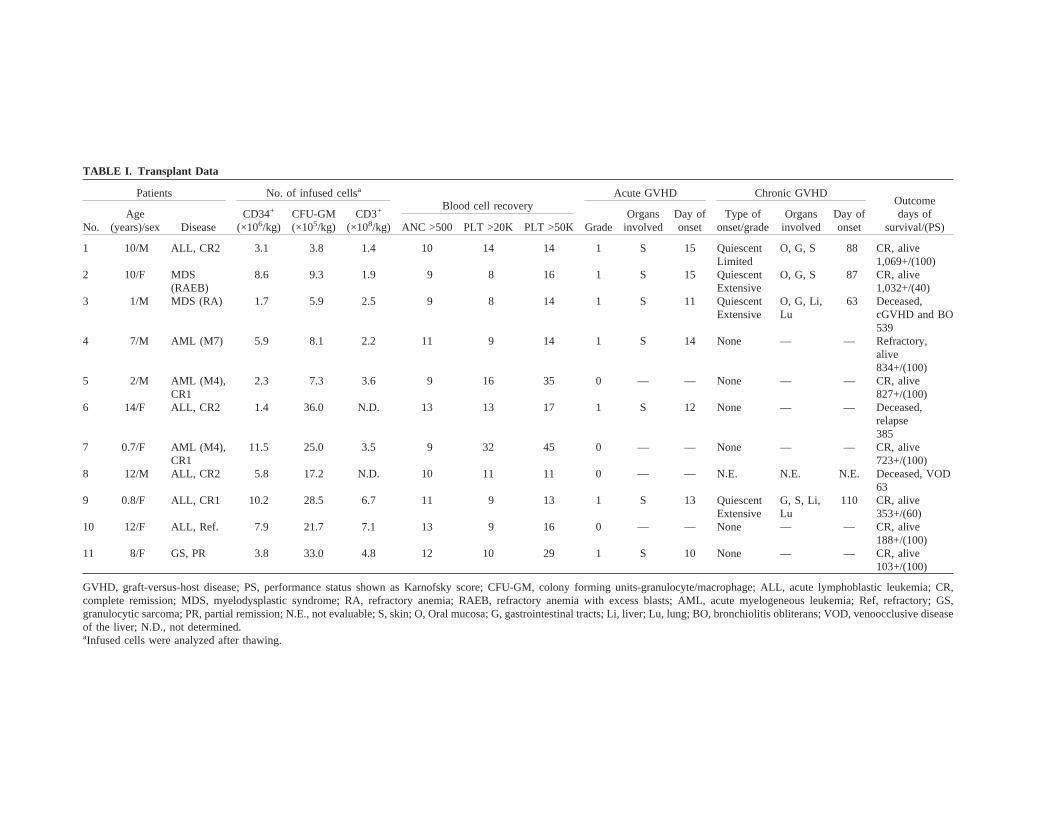
TABLE I. Transplant Data
Patients No. of infused cellsa
Blood cell recoveryAcute GVHD Chronic GVHD
Outcomedays of
survival/(PS)No.Age
(years)/sex DiseaseCD34+
(×106/kg)CFU-GM(×105/kg)
CD3+
(×108/kg) GradeOrgans
involvedDay ofonset
Type ofonset/grade
Organsinvolved
Day ofonsetANC >500 PLT >20K PLT >50K
1 10/M ALL, CR2 3.1 3.8 1.4 10 14 14 1 S 15 QuiescentLimited
O, G, S 88 CR, alive1,069+/(100)
2 10/F MDS(RAEB)
8.6 9.3 1.9 9 8 16 1 S 15 QuiescentExtensive
O, G, S 87 CR, alive1,032+/(40)
3 1/M MDS (RA) 1.7 5.9 2.5 9 8 14 1 S 11 QuiescentExtensive
O, G, Li,Lu
63 Deceased,cGVHD and BO539
4 7/M AML (M7) 5.9 8.1 2.2 11 9 14 1 S 14 None — — Refractory,alive834+/(100)
5 2/M AML (M4),CR1
2.3 7.3 3.6 9 16 35 0 — — None — — CR, alive827+/(100)
6 14/F ALL, CR2 1.4 36.0 N.D. 13 13 17 1 S 12 None — — Deceased,relapse385
7 0.7/F AML (M4),CR1
11.5 25.0 3.5 9 32 45 0 — — None — — CR, alive723+/(100)
8 12/M ALL, CR2 5.8 17.2 N.D. 10 11 11 0 — — N.E. N.E. N.E. Deceased, VOD63
9 0.8/F ALL, CR1 10.2 28.5 6.7 11 9 13 1 S 13 QuiescentExtensive
G, S, Li,Lu
110 CR, alive353+/(60)
10 12/F ALL, Ref. 7.9 21.7 7.1 13 9 16 0 — — None — — CR, alive188+/(100)
11 8/F GS, PR 3.8 33.0 4.8 12 10 29 1 S 10 None — — CR, alive103+/(100)
GVHD, graft-versus-host disease; PS, performance status shown as Karnofsky score; CFU-GM, colony forming units-granulocyte/macrophage; ALL, acute lymphoblastic leukemia; CR,complete remission; MDS, myelodysplastic syndrome; RA, refractory anemia; RAEB, refractory anemia with excess blasts; AML, acute myelogeneous leukemia; Ref, refractory; GS,granulocytic sarcoma; PR, partial remission; N.E., not evaluable; S, skin; O, Oral mucosa; G, gastrointestinal tracts; Li, liver; Lu, lung; BO, bronchiolitis obliterans; VOD, venoocclusive diseaseof the liver; N.D., not determined.aInfused cells were analyzed after thawing.

Thus, eight patients (73%) are alive without evidence ofdisease with a median follow-up of 775 (range 103–1,069) days and their performance status is excellent,except for two patients with severe chronic GVHD (cases2 and 9).
DISCUSSION
The results of this study suggest that the collection ofPBSC from pediatric donors is feasible with acceptableadverse effects, although the long-term effects of G-CSFadministration should be monitored for a longer period.Although G-CSF has a theoretical risk of producing leu-kemia and myelodysplasia [14], no adverse clinical orhematological events have occurred with at most a 5-yearfollow-up in a limited number of donors [15]. The po-tential risks of G-CSF treatment should be seriouslyweighed against the existing risks of marrow aspirationunder general anesthesia, especially in a pediatric popu-lation. Donors should have the option of two proceduresfor donating stem cells.
Placement of a central venous (CV) line to achieveadequate venous flow for PBSC collection may not bejustified in this donor population. Placement of CV cath-eters is accompanied by serious complications such aspneumothorax, perforation of the superior vena cava andvenous thrombosis [16,17]. Furthermore, placement of aCV catheter requires general anesthesia in small children.Placement of the catheter in a radial artery can avoidproblems related to the placement of a CV line and gen-eral anesthesia. Potential complications of radial arterycannulation includes ischemia from clot formation andinfection in the field of neonatology or intensive caremedicine. However, in our PBSC harvesting program,there were no serious complications related to the tem-porary radial artery cannulation. Priming the cell separa-tor for children weighing less than 20 kg is necessary,and autologous blood must be used to avoid the potentialrisk of allogeneic blood transfusion.
There have been reports in adult patients that alloge-neic PBSCT resulted in rapid hematopoietic reconstitu-tion without excessive acute GVHD compared to alloge-neic BMT [1–3]. Neutrophil and platelet recoveries ap-peared to be more rapid than would have been expectedwith BMT and were associated with fewer infectiouscomplications and a shorter hospitalization [18,19]. Inthis study, all of the patients engrafted in a median of 10days, and no life-threatening infectious complicationswere observed even in patients at high risk for infection.Early engraftment of allogeneic PBSCT is one of itsadvantages over BMT, and the choice of PBSC as a stemcell source might be considered for patients at high riskfor life-threatening infection.
In this study, seven of the eleven patients (64%) de-veloped acute GVHD, all involving the skin. Four (40%)
developed chronic GVHD, mostly involving the gastro-intestinal tract. Three patients (30%) suffered from se-vere chronic GVHD; one died from progressive lungdisease probably related to chronic GVHD, and anotherpresented with clinical symptoms and findings similar tothose of diffuse systemic sclerosis, and only the thirdpatient responded to steroid therapy. Interestingly, thenumber of CD3+ cells infused showed no correlationwith the development of acute or chronic GVHD. Theabsolute number of T cells in allogeneic PBSC graftsmay not be the crucial factor that determines the severityof GVHD. The development of mild acute GVHD andsevere chronic GVHD suggests that different mecha-nisms are responsible for acute and chronic GVHD. Al-though the grade of acute GVHD was negligible, thisincidence and severity of chronic GVHD might be highconsidering that all of the patients were children whoreceived a graft from a matched sibling [20–22]. How-ever, an increased incidence of GVHD may contribute toa decreased incidence of leukemia relapse by inducing aGVL effect [23,24], although this issue is still controver-sial [25]. Allogeneic PBSCT may be indicated for high-risk hematological malignancies. Its impact on survivaland performance status should be judged over a longerfollow-up period.
CONCLUSIONS
In summary, allogeneic PBSCT is feasible in the pe-diatric population, and PBSC harvest is an alternative toBM harvest in donors who are not eligible for BM har-vest, although the long-term effects of G-CSF adminis-tration are yet to be determined. Furthermore, PBSCwere successfully collected in pediatric donors with pe-ripheral access. Rapid engraftment was observed withoutincreased severity of acute GVHD. Chronic GVHD re-mains a problem after allogeneic PBSCT. The choice ofa stem cell source (PBSC or BM) should be based on therisk/benefit assessment for both patients and donors.
ACKNOWLEDGMENTS
We are indebted to the pediatric BMT physicians(Drs. Toshihiro Onishi, MD, Sachiyo Kanamaru, MD,Kentaro Suenaga, MD, Hiroko Suzuya, MD, AtsushiMakimoto, MD, and Ryuji Nakagawa, MD) and nursesfor providing excellent patient care.
REFERENCES
1. Korbling M, Przepiorka D, Huh YO, et al. Allogeneic blood stemcell transplantation for refractory leukemia and lymphoma: poten-tial advantage of blood over marrow allografts. Blood 1995;83:1659–1665.
2. Bensinger WI, Clift R, Martin P, et al. Allogeneic peripheral blood
Allogeneic PBSCT in Children 175

stem cell transplantation in patients with advanced hematologicmalignancy: a retrospective comparison with marrow transplan-tation. Blood 1996;88:2794–2800.
3. Schmitz N, Bacigalupo A, Labopin M, et al. Transplantation ofperipheral blood progenitor cells from HLA-identical sibling do-nors. Br J Haematol 1996;95:715–723.
4. To LB, Haylock DN, Simmons PJ, et al. The biology and clinicaluses of blood stem cells. Blood 1997;89:2233–2258.
5. Glass B, Uharek L, Zeis M, et al. Allogeneic peripheral bloodprogenitor cell transplantation in a murine model: Evidence for animproved graft-versus-leukemia effect. Blood 1997;90:1694–1700.
6. Zecca M, Perotti C, Marradi P, et al. Recombinant human G-CSF-mobilized peripheral blood stem cells for second allogeneic trans-plant after bone marrow graft rejection in children. Br J Haematol1996;92:432–434.
7. Diaz MA, Alegre A, Villa M et al. Allogeneic peripheral bloodprogenitor cell (PBPC) transplantation in children with haemato-logical malignancies. Br J Haematol 1997;96:161–164.
8. Li CK, Yuen PMP, Chik KW, et al. Allogeneic peripheral bloodstem cell transplant in children. Med Pediatr Oncol 1998;30:147–151.
9. Nussbaumer W, Schonitzer D, Trieb T, et al. Peripheral bloodstem cell (PBSC) collection in extremely low-weight infants.Bone Marrow Transplant 1996;18:15–17.
10. Galacki DM. An overview of therapeutic apheresis in pediatrics.J Clin Apheresis 1997;12:1–3.
11. Takaue Y, Kawano Y, Abe T, et al. Collection and transplantationof peripheral blood stem cell in very small children weighing 20kg or less. Blood 1995;86:372–380.
12. Takaue Y, Watanabe T, Kawano Y, et al. Isolation and storage ofperipheral blood hematopoietic stem cells for the autotransplan-tation in cancer children. Blood 1989;74:1245–1251.
13. Deeg HJ, Cottler-Fox M. Clinical spectrum and pathophysiologyof acute graft-versus-host disease. In: Burakoff SJ, Deeg HJ, Fer-rara J, Atkinson K, editors. Graft-vs-host disease: immunology,pathophysiology, and treatment. New York: Marcel Dekker; 1990.p 311–336.
14. Welte K, Gabrilove J, Bronchud MH, et al. Filgrastim (r-metHuG-CSF): The first 10 years. Blood 1996;88:1907–1929.
15. Anderlini P, Przepiorka D, Champlin R, et al. Biological andclinical effects of granulocyte colony-stimulating factor in normalindividuals. Blood 1996;88:2819–2825.
16. Goldberg SL, Hangan KF, Klumpp TR, et al. Complications ofperipheral blood stem cell harvesting: review of 554 PBSC leu-kaphereses. J Hematother 1995;4:85–90.
17. Diaz MA, Alegre A, Benito A, et al. Peripheral blood progenitorcell collection by large-volume leukapheresis in low-weight chil-dren. J Hematother 1998;7:63–68.
18. Pavletic ZS, Bishop MR, Tarantolo SR, et al. Hematopoietic re-covery after allogeneic blood stem-cell transplantation comparedwith bone marrow transplantation in patients with hematologicmalignancies. J Clin Oncol 1997;15:1608–1616.
19. Przepiorka D, Anderlini P, Ippoliti C, et al. Allogeneic blood stemcell transplantation in advanced hematologic cancers. Bone Mar-row Transplant 1997;19:455–460.
20. Majolino I, Saglio G, Scime` R, et al. High incidence of chronicGVHD after primary allogeneic peripheral blood stem cell trans-plantation in patients with hematologic malignancies. Bone Mar-row Transplant 1996;17:555–560.
21. Storek J, Gooley T, Siadak M, et al. Allogeneic peripheral bloodstem cell transplantation may be associated with a high risk ofchronic graft-versus-host disease. Blood 1997;90:4705–4709.
22. Miflin G, Russell NH, Hutchinson RM, et al. Allogeneic periph-eral blood stem cell transplantation for haematological malignan-cies—an analysis of kinetics of engraftment and GVHD risk.Bone Marrow Transplant 1997;19:9–13.
23. Rambaldi A, Viero P, Bassan R, et al. G-CSF-mobilized periph-eral blood progenitor cells for allogeneic transplantation of resis-tant or relapsing acute leukemia. Leukemia 1996;10:860–865.
24. Glass B, Majolino I, Dreger P, et al. Allogeneic peripheral bloodprogenitor cells for treatment of relapse after bone marrow trans-plantation. Bone Marrow Transplant 1997;20:533–541.
25. Schmitz N, Bacigalupo A, Hasenclever D, et al. Allogeneic bonemarrow transplantation vs filgrastim-mobilised peripheral bloodprogenitor cell transplantation in patients with early leukemia:first results of a randomized multicentre trial of the EuropeanGroup for Blood and Marrow Transplantation. Bone MarrowTransplant 1998;21:995–1003.
176 Watanabe et al.