Embed Size (px)
Citation preview

hen Dr. Bruce S.Bochner was beingconsidered in 2002
to head the Johns HopkinsDivision of Allergy & ClinicalImmunology, other centersaround the country were try-ing to recruit him. But, Dr.Bochner says, when Hopkinsmade the offer, it really wasa no-brainer: “This being thelargest, most successful and,humbly put, best allergygroup in the country, whenthe opportunity came along, I took it.” We caught up withthis clinician scientist to hearhis thoughts about the futureof the division.
First, what do you see as the division’s strengths?We’re an internationally rec-ognized program, one of thefew in the country with anNational Institutes of Health(NIH) grant for training aca-demic allergists. One of ourgreatest strengths is having 30faculty who see patients, teachand/or do research, collabo-
rating to study all aspects ofallergic diseases. While ourexpertise is diverse, we needto recruit new young faculty,but it’s not like building fromscratch. It may be a whilebefore the division has myinfluence and flavor. But I’drather take over as command-er of the best ship in the fleetthan build the next big ship inthe fleet.
New clinical challenges? I take great pride in the quali-ty of care provided by our fac-ulty, fellows, and staff. In auniversity setting, we can takethe time to practice medicinethe right way, without worry-ing about the profit motive.
However, one goal is to pro-vide more efficient clinicalcare. At certain times of theyear, patients have to wait toolong to get an appointment.Because complicated patientsare often referred to us, clinicsdo not always run on time,and patients may wait toolong before being seen.Finally, I would like to expandsome of our more uniqueservices, like testing for food,drug, and latex allergies andchallenging and desensitizingfor drugs such as aspirin.
Your research goals? Because there are no perfectanimal models for asthma andallergic diseases, it’s really crit-ical to move new therapiesinto humans as efficiently aspossible. Our group is reallygood at developing researchideas in the laboratory thatcan be safely tried in humans.
The battle against asthma? We have good medicines tocontrol asthma, but not acure. We’re involved in devel-oping and testing new thera-pies because they may providenew treatments for thosewith asthma, including oursickest patients.
Any new technologies? We’re using gene chips, whichallow you to measure thepresence of thousands ofgenes from cells or a tissuesample. For example, we cannow compare normal andasthmatic lung specimens,and determine what genes areover- and under-expressed.
Then what? Then the job is to figure outwhich of those genes actual-ly cause or perpetuate thedisease. The approach yieldsbroad, unbiased snapshotsof what’s going on. This maysuggest new and unanticipa-ted targets for future thera-peutic research.
There’s still plenty of that? Yes, the good news is that theNIH has doubled its budget.We used to have a 10 to 15percent chance of getting agrant funded, which was adeterrent for the junior per-son considering an academiccareer. Now there’s a 20 to 25percent chance of funding.
The take-home message? Bigger salaries can be found inprivate practice and in the pharmaceutical industry.We chose academic medicinebecause it allows us to helpmany patients, as well as toengage in the intellectual challenges of teaching anddoing research. We all enjoyinteracting with colleaguesand presenting our work atmeetings around the world. In academics, we can reallymake a difference.
AllergicReactions
A semiannual publication ofJ O H N S H O P K I N S M E D I C I N EDivision of Allergy & Clinical Immunology
Volume 1, Number 1Spring/Summer 2004
W
An Interview With the New Allergy Division Director
Inside this issue
Stop and Smell the Roses 2
Allergen Season Calendar 3
Medication Update 4
New Website Launched 4
Our Mission 5
Our Clinical Practice 5
“In academics, we canreally make a difference.”

Go Ahead: Stop and Smell the Roses
What are rosefever and hayfever?
“Rosefever” is really afolk name for allergicsymptoms that occur during the peak seasonfor grass pollen allergies—in late spring to earlysummer, when roses arein bloom. “Hayfever” isa common name for symp-toms that occur during thepeak season for ragweedpollen allergies—in latesummer to early fall,when hay is harvested.Neither is associated witha fever.
Why does smelling arose sometimes make me sneeze, even if I am not allergic to it?
Some people with allergiescan be particularly sensitive to strong scents—especially during theirallergy seasons, when theyare already experiencingsymptoms. This sensitivityis not a true allergicresponse, but more like anirritation. Other exam-ples of such irritantsinclude cigarette smokeand strong perfumes.
Rarely, florists, profes-sional rose growers andavid rose gardening hob-byists may develop trueallergic responses to rosepollens while handling theroses, since they mayshake the heavy pollengrains directly into con-tact with the nose or eyes.
ye-catching, heaven-
scented blooms
should be enjoyed,
not avoided—even by most
allergy sufferers. If you
have kept a wary distance
for years, you may have
trouble approaching that
red, red rose. But this kind
of red is not an alert to
danger, because ornamental
plants generally do not pro-
duce aeroallergens.
Aeroallergens are tiny,
airborne particles that
can trigger allergic
reactions when they
come in contact with
a membrane lining the
nose or throat or covering
the eye. While sneezing,
coughing, and red-rimmed
eyes can be caused by pol-
lutants, irritants, and infec-
tions, true allergic symp-
toms only can be caused by
an aeroallergen if a person
is allergic to it, if enough
particles are present to pro-
duce an allergic reaction in
that person, and if the par-
ticles are small enough to
interact with the human
immune system. When an
Eaeroallergen floats onto a
membrane, it initiates a
microscopic chain reaction,
which results in the release
of substances like histamine
and leukotrienes with the
consequent allergic symp-
toms. Allergic symptoms
may include sneezing
and/or a runny, clogged
nose, coughing, post-nasal
drip, itchy eyes, nose and
throat, and watery, red-
rimmed, swollen eyes.
Showy, fragrant flower-
ing plants typically do not
produce allergic reactions,
because their pollens are
not airborne, are small in
number, and are large in
size. Their big, sticky,
heavy pollen grains are car-
ried by insects like butter-
Q & A
flies and bees, instead of by
the wind. In contrast,
plainer-looking plants like
trees, grasses, and weeds, as
well as some molds, pro-
duce microscopically small,
lightweight pollens or
spores in great number,
that are easily carried by
the wind.
One major exception is
ragweed. This weed agres-
sively invades the land-
scape, filling large fields,
and is showy in its produc-
tion of enormous clus-
ters of tiny pollen
grains. A single
plant can produce a million
pollen grains, and it takes
as few as ten grains to pro-
duce symptoms in allergic
individuals. The yellow of
ragweed is a warning signal
to ragweed allergy sufferers
that they should be taking
allergy medication. Because
ragweed’s pollen grains are
numerous and windborne,
victims will suffer allergic
symptoms whether they
are blocks away from a
ragweed plant or up close
and personal.
For more information about allergy medications, talk to your doctor or visit us at www.hopkins-allergy.org.
2

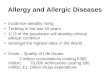
TREE POLLENS
Juniper
Willow
Elm
Maple
Birch
Alder
Poplar
Beech
Sycamore
Ash
Oak
Hickory
Walnut
GRASS POLLENS
Timothy
Orchard
Bermuda
WEED POLLENS
Sorrel
Plantain
Lambsquarters
Pigweed
Sage
Ragweed
MOLD SPORES
Aspergillus
Penicillium
Alternaria
Fusarium
Cladosporium
Helminthosporium
Botrytis
DUST PART ICLES
Dust mites
Roaches
ANIMALS
Cats
Dogs
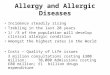
JAN FEB MAR APR JUN JUL AUG SEP OCT NOV DECMAY
ALLERGENS
Season Peak of season
Allergy Season Calendar*
* F o r t h e m i d - A t l a n t i c r e g i o n
Courtesy of J O H N S H O P K I N S M E D I C I N EDivision of Allergy & Clinical Immunology
Clinical Care Unit: (410) 550-2300
3

RXolair Offers Relief Xolair (Omalizumab) has
been approved by the U.S.
FDA (Food and Drug
Administration) for treat-
ment of patients with mod-
erate to severe persistent
asthma. It is recognized
that a significant number
of asthmatic patients have
an allergic basis to their
disease because they pro-
duce too much of a certain
protein in the body, called
IgE antibody. Xolair binds
to this allergic antibody in
the blood stream and hence
neutralizes (blocks) its
actions.
Xolair is indicated for
adults and adolescents (≥12
years age) who have moder-
ate to severe asthma that is
Asthma Medication Update
not currently controlled
with inhaled corticoster-
oids, and are sensitive
(allergic) to year-round,
aeroallergens (for example:
dust mites, household pets,
cockroaches, and certain
molds).
Xolair has been shown
to decrease the number of
asthma attacks in patients
with moderate to severe
asthma, and in some
patients it allows a reduc-
tion, and perhaps complete
elimination, of other asth-
ma medications.
For more information,
go to our website at
www.hopkins-allergy.org.
No More CFC Propellants In 1987, the United States
signed an international
treaty, the Montreal
Protocol, agreeing to stop
using chlorofluorocarbons
(CFCs) as refrigerants and
aerosol propellents. CFCs
are the chemical propellants
that have been used in
metered-dose inhalers,
devices that effectively
deliver medicine to the
lungs of people who suffer
from asthma and other lung
diseases like emphysema.
Pharmaceutical companies
have developed metered-
dosed inhalers based on
other propellants as well as
dry powder inhalers, but it
will be a few years before
CFCs will be completely
phased out.
Visit us on the WebNow you can check out our
division’s new website at
www.hopkins-allergy.org to
access more information
about patient care services,
our faculty, or allergic and
immunologic diseases and
their treatments. You also
will find campus maps,
contact information, and
links to other helpful sites
at the Johns Hopkins
Medical Institutions.
w w w .
4
Support Our MissionFinancial support from concerned individuals isessential for high quality patient care and sponsorshipof innovative medical research. If you are interestedin supporting the work of the Johns HopkinsDivision of Allergy & Clinical Immunology, contact:
Bruce S. Bochner, M.D.Director, Division of Allergy & Clinical ImmunologyJohns Hopkins Asthma & Allergy Center5501 Hopkins Bayview Circle, Room 2B.71 Baltimore, MD 21224(410) 550 - 2101

5
Our M issionJ O H N S H O P K I N S M E D I C I N EDivision of Allergy & Clinical Immunology
Director: Bruce S. Bochner, MDClinical Director: Peter S. Creticos, MD
The mission of the Division of Allergy & Clinical Immunology at Johns Hopkins is to promote the treatment and understanding of allergic and immunologic diseases,including asthma, in order to provide optimal patient health by
• providing compassionate, state-of-the-art diagnostic and therapeutic care of adultswith allergic and immunologic diseases
• fostering basic, clinical, and translational allergy and immunology research• training physicians and scientists for academic careers in allergy and immunology
Our C linicalPracticeFaculty:
N. Franklin Adkinson, Jr., MDBruce S. Bochner, MDPeter S. Creticos, MDPhilip S. Norman, MD
Sarbjit Saini, MDAlvin Sanico, MD
Glenn M. Silber, MDAlkis Togias, MD
All of our faculty have expertise in the diagnosis and treatment of asthma, allergicrhinitis, sinusitis, anaphylaxis, urticaria, angioedema, adverse reactions to foods,drugs, latex, and insect stings, and non-AIDS-related deficiencies of the immune system. Some faculty have additional interests and expertise in specialized areas.Evaluations include: allergen skin testing, methacholine challenge, spirometry, andfood and drug challenges. The Dermatology, Allergy and Clinical Immunology(DACI) Reference Laboratory is a full service laboratory that provides specializeddiagnostic measurements to allergists, dermatologists, and clinical immunologists.
Contact us at (410) 550 - 2300 for appointments and referrals.