Embed Size (px)
Citation preview

60444608-L
<date>
Dear <Member name>,
Thank you for your membership. We appreciate the opportunity to provide your care and coverage, and are committed to your health and well-being. The enclosed packet outlines changes to your plan for 2017. Your plan will renew automatically on January 1, 2017 — no action is required.
Don’t forget to take advantage of all the healthy extras your plan offers. It’s never too late to tackle a new health goal!
• Reduced rates on many health-related products and services, such as gym memberships, massage therapy, and chiropractic care. Check out your options at kp.org/choosehealthy.
• Health classes and support groups offered at our facilities. Classes vary by location and some may require a fee. Search course offerings near you at kp.org/classes.
• Online tools and resources, such as customized wellness programs, health calculators, fitness videos, podcasts, and recipes. Visit kp.org/healthyliving for a range of options.
To compare benefits and rates for different Kaiser Permanente plans, see the “Health plan benefit highlights” and 2017 monthly rates information available online at kp.org/renewalinfo. For more details on your coverage, see your Summary of Benefits and Coverage at kp.org/sbc, or get a paper copy at any time without charge by calling 1-800-759-0584. For TTY, call 711.
Thank you for choosing us as your partner in health. We look forward to helping you continue to thrive.
Sincerely,
Mitch Ross Vice President Kaiser Permanente Individual and Family Plans Kaiser Foundation Health Plan, Inc.
<Member name><Address><City, State><ZIP>
All plans offered and underwritten by <ISSUER>
<date>

60444509-RO
Dear <Member name>,
Thank you for your membership. We appreciate the opportunity to provide your care and coverage, and are committed to your health and well-being. The enclosed packet outlines changes to your plan for 2017. Your plan will renew automatically on January 1, 2017 — no action is required.
If your circumstances have changed, you have the option to move to a different plan that saves you money or more closely meets your needs. We’re here for you to discuss your options — just contact our Member Service Contact Center at 1-XXX-XXX-XXXX. You can choose a new plan during open enrollment, which runs from November 1, 2016, to January 31, 2017.
• To select a different plan through Kaiser Permanente, contact our Member Service Contact Center.
• To select a different plan through Exchange name, visit Exchange website.
• To compare benefits and rates for different Kaiser Permanente plans, see the “Health plan benefit highlights” and 2017 monthly rates information available online at kp.org/renewalinfo.
For more details on your coverage, see your Summary of Benefits and Coverage at kp.org/sbc, or get a paper copy at any time without charge by calling 1-800-759-0584. For TTY, call 711.
Thank you for choosing us as your partner in health. We look forward to helping you continue to thrive.
Sincerely,
Mitch Ross Vice President Kaiser Permanente Individual and Family Plans Kaiser Foundation Health Plan, Inc.
All plans offered and underwritten by <ISSUER>
<date>
<Member name><Address><City, State><ZIP>

60444510-RNO
Dear <Member name>,
Thank you for your membership. We appreciate the opportunity to provide your care and coverage, and are committed to your health and well-being. The enclosed packet outlines changes to your plan for 2017. Your plan will renew automatically on January 1, 2017 — no action is required.
Don’t forget to take advantage of all the healthy extras your plan offers. It’s never too late to tackle a new health goal!
• Reduced rates on many health-related products and services, such as gym memberships, massage therapy, and chiropractic care. Check out your options at kp.org/choosehealthy.
• Personal wellness coaching by phone at no cost. Get help and inspiration to tackle a range of health goals. Find out more at kp.org/wellnesscoach.
• Health classes and support groups offered at our facilities. Classes vary by location and some may require a fee. Search course offerings near you at kp.org/classes.
• Your choice of locations near you — plus 24/7 nurse advice.
For more details on your coverage, see your Summary of Benefits and Coverage at kp.org/sbc, or get a paper copy at any time without charge by calling 1-800-759-0584. For TTY, call 711. To compare different Kaiser Permanente plans, visit kp.org/renewalinfo.
Thank you for choosing us as your partners in health. We look forward to helping you continue to thrive.
Sincerely,
Mitch Ross Vice President Kaiser Permanente Individual and Family Plans Kaiser Foundation Health Plan, Inc.
All plans offered and underwritten by <ISSUER>
<date>
<Member name><Address><City, State><ZIP>
60473718_V1
CO Renewal, Off-Exchange
[Date]
[Subscriber’s First Name][Subscriber’s Last Name] [Mailing Address line 1] [Mailing Address line 2] [City][State][Zip] Dear [Subscriber’s First Name]: Your health insurance coverage is coming up for renewal. Your current plan will be offered in the upcoming 2017 plan year. If you want to keep your plan, you don’t have to do anything. You’ll be automatically enrolled and you just have to pay the monthly premium. Changes we’re making to your coverage
• Premium - Your new premium starts in January. Your new premium will be $[Future Total Rate] each month.
• Benefits – Changes to your health plan, [Future Marketing Plan Name] are listed below. The changes are also outlined in the “Health Plan Benefit Changes” pages.
Current 2016 plan benefits New 2017 plan and benefit changes [2016 plan name] [HIOS ID]
[2017 plan name] [HIOS ID]
[2016 benefits] [2017 benefit changes]
You can review more details about your plan at kp.org/plandocuments and in your Summary of Benefits and Coverage. Tax credits and other cost savings may be available to people who purchase a health plan through Connect for Health Colorado. To find out if you qualify based on your income and household size, you can visit ConnectforHealthCO.com starting November 1, 2016. What if I want to change plans?
• The 2017 Open Enrollment period is from November 1, 2016 to January 31, 2017. If you would like to switch to a different plan with coverage that starts on January 1, 2017, the deadline to enroll is December 15, 2016.
• You can choose a new plan from Kaiser Permanente, another insurance company or through Connect for Health Colorado. You or your family may also qualify for Medicaid or the Children’s Health Insurance Program (CHP+), both of which are public programs that offer low cost health coverage.
• If you qualify for financial assistance and/or lower costs, you can get those savings only if you enroll through Connect for Health Colorado.
• You can always contact Kaiser Permanente, your broker, an insurance agent, a health coverage guide, or a Connect for Health Colorado customer service representative for any help you may need.
60473718_V1
What else should I look at before deciding to keep or change my plan? Visit kp.org to make sure your doctor and other health care providers are listed in the network for the 2017 plan year. Also check to make sure any prescription medications you take will be covered. If NO broker in data: Questions?
• For plan or benefit questions, call Kaiser Foundation Health Plan of Colorado at [Issuer phone number] or visit kp.org. For TTY, call 711.
• For tax credit and eligibility questions or to learn more about qualifying for financial assistance, please call a Connect for Health Colorado customer service representative at 1-855-752-6749 (TTY: 1- 855-346-3432) or visit ConnectforHealthCO.com.
• Visit ConnectforHealthCO.com to learn more about qualifying for financial assistance, or to find local, in-person assistance.
If broker in data: Questions?
• For plan or benefit questions, call Kaiser Foundation Health Plan of Colorado at [Issuer phone number] or visit kp.org. For TTY, call 711.
• Call your broker, [Broker name] at [Broker phone]. Your broker will be happy to help you choose the right Kaiser Permanente plan for your health needs.
• For tax credit and eligibility questions or to learn more about qualifying for financial assistance, please call a Connect for Health Colorado customer service representative at 1-855-752-6749 (TTY: 1- 855-346-3432) or visit ConnectforHealthCO.com.
• Visit ConnectforHealthCO.com to learn more about qualifying for financial assistance, or to find local, in-person assistance.
Getting help in other languages English: For help in other languages, call [English NOLA phone number] and an interpreter will assist you with this notice at no cost. Spanish (español): Para obtener ayuda en español, llame al [Spanish NOLA phone number] y un intérprete le ayudará con esta notificación sin ningún costo. Sincerely,
Mitch Ross Vice President Kaiser Permanente Individual and Family Plans Kaiser Foundation Health Plan, Inc.
In Colorado, all plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.
60491610 OE Notice 2017
Annual Open Enrollment Period Notice for Individual Health Benefit Plans Kaiser Permanente for Individuals and Families
We would like to let you know that your annual open enrollment period starts this year on November 1, 2016. Your open enrollment period will last until January 31, 2017. During the open enrollment period you will be able to purchase new health coverage for the coming year. You have two choices:
• You can continue with your current plan, where you will not need to take any action; or • You can enroll in a new plan during the open enrollment period.
If you decide to choose a new plan: • You can choose your new plan from us, or any other carrier offering plans; or • You may purchase a new plan through Connect for Health Colorado, where you may qualify for
federal financial assistance (www.ConnectforHealthCO.com). Make sure you follow the termination notice requirements in your current plan so that you will be able to avoid a gap in coverage by ending your old plan and beginning your new plan on the appropriate dates. You can contact us or your health care advisor for assistance and additional information. For assistance, call the Kaiser Permanente Member Service Contact Center at the number listed below for your service area. If you work with a broker, please contact him or her. Your broker will partner with you and provide any assistance you may need. Member Services 8 a.m. to 5 p.m. weekdays (except holidays)
Denver/Boulder: 1-303-338-3800 Northern Colorado: 1-844-201-5824 Mountain Colorado: 1-844-837-6884 Southern Colorado: 1-888-681-7878
For TTY, call 711
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.
60491708 CO KPIF 2017 Benefit Modifications Notice FNL
Dear Member, Thank you for choosing Kaiser Permanente for your health care needs. Colorado law requires that we notify you of any changes in your health coverage. Please review the Health Plan Benefit Changes enclosed with this letter. These benefit changes will be effective upon your plan renewal on January 1, 2017. Colorado law also requires that whenever a benefit is modified, the policyholder be given the opportunity to purchase any other Kaiser Permanente for Individuals and Families plan at the time of renewal. Your renewal information, which you will receive before the 2017 open enrollment period (November 1, 2016 through January 31, 2017), will outline your options. You also have the option of selecting a plan through the Health Insurance Marketplace, Connect for Health Colorado, at www.ConnectforHealthCO.com or 1-855-752-6749. If you have questions regarding this letter, please contact your broker who has been informed of these benefit changes. If you are not working with a broker and have questions, you may call your regional Member Services, 8 a.m. to 5 p.m. weekdays (except holidays) at:
Denver/Boulder: 1-303-338-3800 Northern Colorado: 1-844-201-5824 Mountain Colorado: 1-844-837-6884 Southern Colorado: 1-888-681-7878
For TTY, call 711 Sincerely, KAISER FOUNDATION HEALTH PLAN OF COLORADO Administrative Services Waterpark 1 2500 South Havana St. Aurora, CO 80014
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado,
10350 E. Dakota Avenue, Denver, CO 80247.
Page 1 of 860422308 Colorado 2017
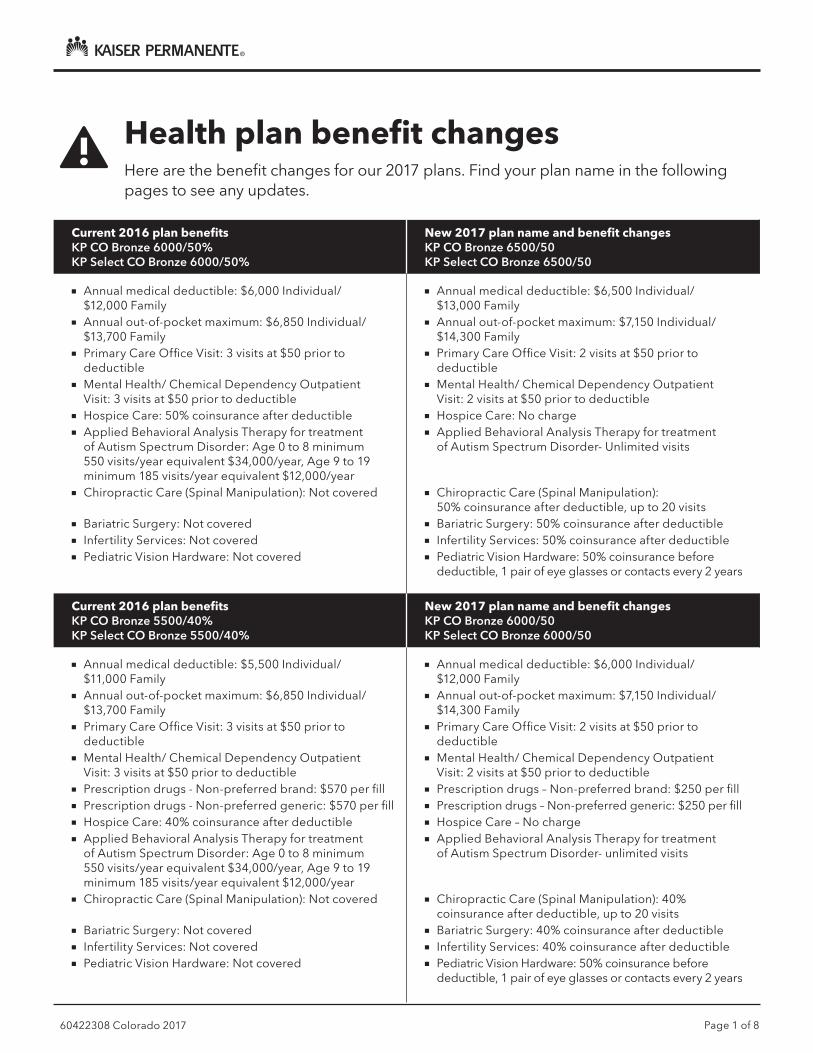
Health plan benefit changesHere are the benefit changes for our 2017 plans. Find your plan name in the following pages to see any updates.
Current 2016 plan benefitsKP CO Bronze 6000/50%KP Select CO Bronze 6000/50%
New 2017 plan name and benefit changesKP CO Bronze 6500/50KP Select CO Bronze 6500/50
■■ Annual medical deductible: $6,000 Individual/ $12,000 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Primary Care Office Visit: 3 visits at $50 prior to deductible
■■ Mental Health/ Chemical Dependency Outpatient Visit: 3 visits at $50 prior to deductible
■■ Hospice Care: 50% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $6,500 Individual/ $13,000 Family
■■ Annual out-of-pocket maximum: $7,150 Individual/ $14,300 Family
■■ Primary Care Office Visit: 2 visits at $50 prior to deductible
■■ Mental Health/ Chemical Dependency Outpatient Visit: 2 visits at $50 prior to deductible
■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder- Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 50% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 50% coinsurance after deductible■■ Infertility Services: 50% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Bronze 5500/40%KP Select CO Bronze 5500/40%
New 2017 plan name and benefit changesKP CO Bronze 6000/50 KP Select CO Bronze 6000/50
■■ Annual medical deductible: $5,500 Individual/ $11,000 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Primary Care Office Visit: 3 visits at $50 prior to deductible
■■ Mental Health/ Chemical Dependency Outpatient Visit: 3 visits at $50 prior to deductible
■■ Prescription drugs - Non-preferred brand: $570 per fill■■ Prescription drugs - Non-preferred generic: $570 per fill■■ Hospice Care: 40% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $6,000 Individual/ $12,000 Family
■■ Annual out-of-pocket maximum: $7,150 Individual/ $14,300 Family
■■ Primary Care Office Visit: 2 visits at $50 prior to deductible
■■ Mental Health/ Chemical Dependency Outpatient Visit: 2 visits at $50 prior to deductible
■■ Prescription drugs – Non-preferred brand: $250 per fill■■ Prescription drugs – Non-preferred generic: $250 per fill■■ Hospice Care – No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder- unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 40% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 40% coinsurance after deductible■■ Infertility Services: 40% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Page 2 of 860422308 Colorado 2017
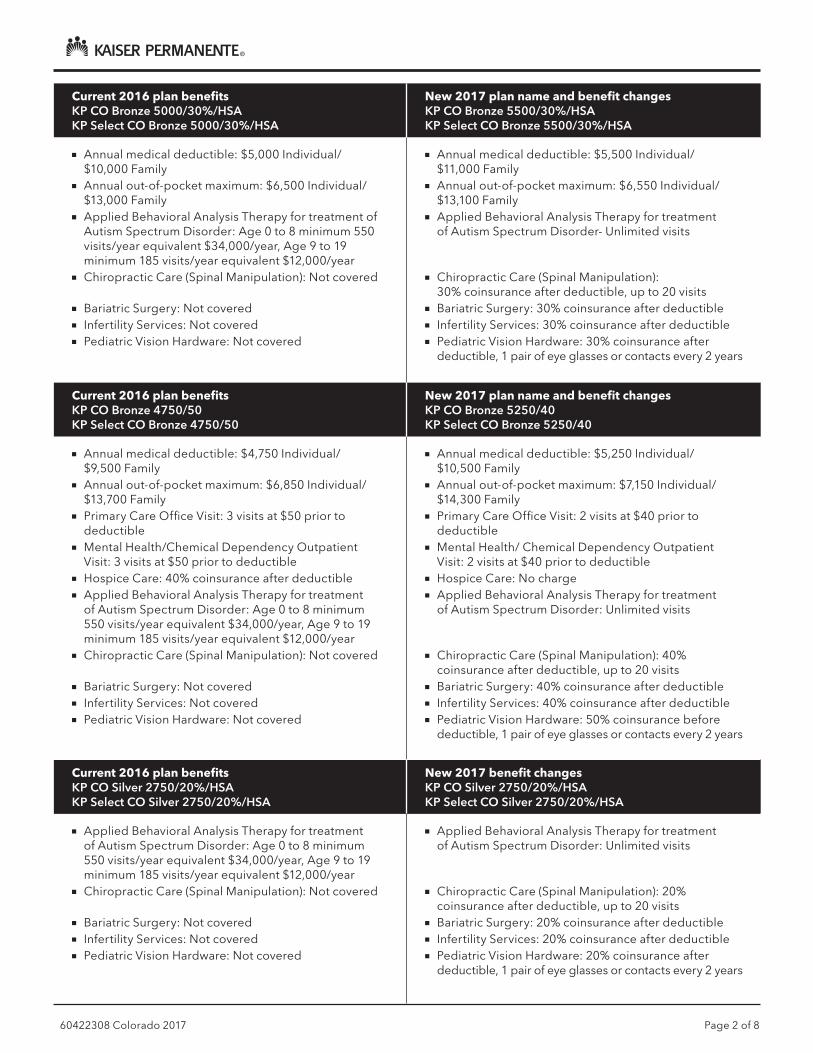
Current 2016 plan benefitsKP CO Bronze 5000/30%/HSAKP Select CO Bronze 5000/30%/HSA
New 2017 plan name and benefit changesKP CO Bronze 5500/30%/HSA KP Select CO Bronze 5500/30%/HSA
■■ Annual medical deductible: $5,000 Individual/ $10,000 Family
■■ Annual out-of-pocket maximum: $6,500 Individual/ $13,000 Family
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $5,500 Individual/ $11,000 Family
■■ Annual out-of-pocket maximum: $6,550 Individual/ $13,100 Family
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder- Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 30% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware: 30% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Bronze 4750/50KP Select CO Bronze 4750/50
New 2017 plan name and benefit changesKP CO Bronze 5250/40KP Select CO Bronze 5250/40
■■ Annual medical deductible: $4,750 Individual/ $9,500 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Primary Care Office Visit: 3 visits at $50 prior to deductible
■■ Mental Health/Chemical Dependency Outpatient Visit: 3 visits at $50 prior to deductible
■■ Hospice Care: 40% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $5,250 Individual/ $10,500 Family
■■ Annual out-of-pocket maximum: $7,150 Individual/ $14,300 Family
■■ Primary Care Office Visit: 2 visits at $40 prior to deductible
■■ Mental Health/ Chemical Dependency Outpatient Visit: 2 visits at $40 prior to deductible
■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 40% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 40% coinsurance after deductible■■ Infertility Services: 40% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 2750/20%/HSAKP Select CO Silver 2750/20%/HSA
New 2017 benefit changesKP CO Silver 2750/20%/HSAKP Select CO Silver 2750/20%/HSA
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 20% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 20% coinsurance after deductible■■ Infertility Services: 20% coinsurance after deductible■■ Pediatric Vision Hardware: 20% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years

Page 3 of 860422308 Colorado 2017
Current 2016 plan benefitsKP CO Silver 2750/20%/HSA/73% CSRKP Select CO Silver 2750/20%/HSA/73% CSR
New 2017 plan name and benefit changesKP CO Silver 1900/20%/73% CSR*KP Select CO Silver 1900/20%/73% CSR*
■■ Annual medical deductible: $1,700 Individual/ $3,400 Family
■■ Prescription drugs – Preferred brand: $35 after deductible, per fill
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $1,900 Individual/ $3,800 Family
■■ Prescription drugs – Preferred brand: $45 after deductible, per fill
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 20% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 20% coinsurance after deductible■■ Infertility Services: 20% coinsurance after deductible■■ Pediatric Vision Hardware: 20% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 2750/20%/HSA/87% CSRKP Select CO Silver 2750/20%/HSA/87% CSR
New 2017 plan name and benefit changesKP CO Silver 500/10%/87% CSR*KP Select CO Silver 500/10%/87% CSR*
■■ Annual out-of-pocket maximum: $2,250 Individual/ $4,500 Family
■■ Prescription drugs – Preferred brand: $20 after deductible, per fill
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual out-of-pocket maximum: $2,350 Individual/ $4,700 Family
■■ Prescription drugs – Preferred brand: $30 after deductible, per fill
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 10% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 10% coinsurance after deductible■■ Infertility Services: 10% coinsurance after deductible■■ Pediatric Vision Hardware: 10% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 2750/20%/HSA/94% CSRKP Select CO Silver 2750/20%/HSA/94% CSR
New 2017 plan name and benefit changesKP CO Silver 200/5%/94% CSR*KP Select CO Silver 200/5%/94% CSR*
■■ Annual medical deductible: $100 Individual/ $200 Family
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $200 Individual/ $400 Family
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 5% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 5% coinsurance after deductible■■ Infertility Services: 5% coinsurance after deductible■■ Pediatric Vision Hardware: 5% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years
*This plan is no longer qualified to be paired with an optional tax-advantaged HSA account.

Page 4 of 860422308 Colorado 2017
Current 2016 plan benefitsKP CO Silver 2500/30KP Select CO Silver 2500/30
New 2017 plan name and benefit changesKP CO Silver 3000/30KP Select CO Silver 3000/30
■■ Annual medical deductible: $2,500 Individual/ $5,000 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Prescription drugs - Non-preferred brand: $570 per fill■■ Prescription drugs - Non-preferred generic: $570 per fill■■ Hospice Care: 30% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $3,000 Individual/ $6,000 Family
■■ Annual out-of-pocket maximum: $7,150 Individual/ $14,300 Family
■■ Prescription drugs - Non-preferred brand: $150 per fill■■ Prescription drugs - Non-preferred generic: $150 per fill■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $30 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 2500/30/73% CSRKP Select CO Silver 2500/30/73% CSR
New 2017 plan name and benefit changesKP CO Silver 2000/30/73% CSRKP Select CO Silver 2000/30/73% CSR
■■ Annual out-of-pocket maximum: $5,540 Individual/ $11,080 Family
■■ Prescription drugs - Non-preferred brand: $570 per fill■■ Prescription drugs - Non-preferred generic: $570 per fill■■ Hospice Care: 30% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual out-of-pocket maximum: $5,700 Individual/ $11,400 Family
■■ Prescription drugs - Non-preferred brand: $150 per fill■■ Prescription drugs - Non-preferred generic: $150 per fill■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment of
Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $30 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Page 5 of 860422308 Colorado 2017
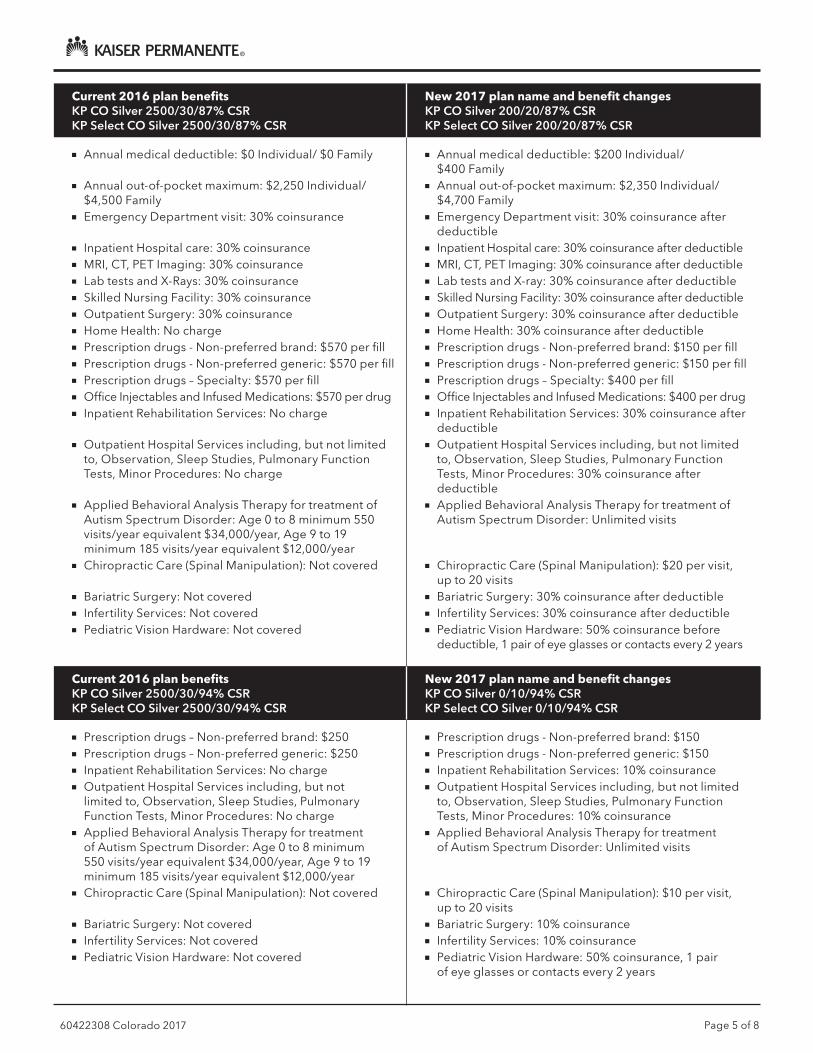
Current 2016 plan benefitsKP CO Silver 2500/30/87% CSRKP Select CO Silver 2500/30/87% CSR
New 2017 plan name and benefit changesKP CO Silver 200/20/87% CSRKP Select CO Silver 200/20/87% CSR
■■ Annual medical deductible: $0 Individual/ $0 Family
■■ Annual out-of-pocket maximum: $2,250 Individual/ $4,500 Family
■■ Emergency Department visit: 30% coinsurance
■■ Inpatient Hospital care: 30% coinsurance■■ MRI, CT, PET Imaging: 30% coinsurance■■ Lab tests and X-Rays: 30% coinsurance■■ Skilled Nursing Facility: 30% coinsurance■■ Outpatient Surgery: 30% coinsurance■■ Home Health: No charge■■ Prescription drugs - Non-preferred brand: $570 per fill■■ Prescription drugs - Non-preferred generic: $570 per fill■■ Prescription drugs – Specialty: $570 per fill■■ Office Injectables and Infused Medications: $570 per drug■■ Inpatient Rehabilitation Services: No charge
■■ Outpatient Hospital Services including, but not limited to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: No charge
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $200 Individual/ $400 Family
■■ Annual out-of-pocket maximum: $2,350 Individual/ $4,700 Family
■■ Emergency Department visit: 30% coinsurance after deductible
■■ Inpatient Hospital care: 30% coinsurance after deductible■■ MRI, CT, PET Imaging: 30% coinsurance after deductible■■ Lab tests and X-ray: 30% coinsurance after deductible■■ Skilled Nursing Facility: 30% coinsurance after deductible■■ Outpatient Surgery: 30% coinsurance after deductible■■ Home Health: 30% coinsurance after deductible■■ Prescription drugs - Non-preferred brand: $150 per fill■■ Prescription drugs - Non-preferred generic: $150 per fill■■ Prescription drugs – Specialty: $400 per fill■■ Office Injectables and Infused Medications: $400 per drug■■ Inpatient Rehabilitation Services: 30% coinsurance after
deductible■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: 30% coinsurance after deductible
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $20 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 2500/30/94% CSRKP Select CO Silver 2500/30/94% CSR
New 2017 plan name and benefit changesKP CO Silver 0/10/94% CSRKP Select CO Silver 0/10/94% CSR
■■ Prescription drugs – Non-preferred brand: $250■■ Prescription drugs – Non-preferred generic: $250■■ Inpatient Rehabilitation Services: No charge■■ Outpatient Hospital Services including, but not
limited to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: No charge
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Prescription drugs - Non-preferred brand: $150■■ Prescription drugs - Non-preferred generic: $150■■ Inpatient Rehabilitation Services: 10% coinsurance■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: 10% coinsurance
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $10 per visit, up to 20 visits
■■ Bariatric Surgery: 10% coinsurance■■ Infertility Services: 10% coinsurance■■ Pediatric Vision Hardware: 50% coinsurance, 1 pair
of eye glasses or contacts every 2 years
Page 6 of 860422308 Colorado 2017
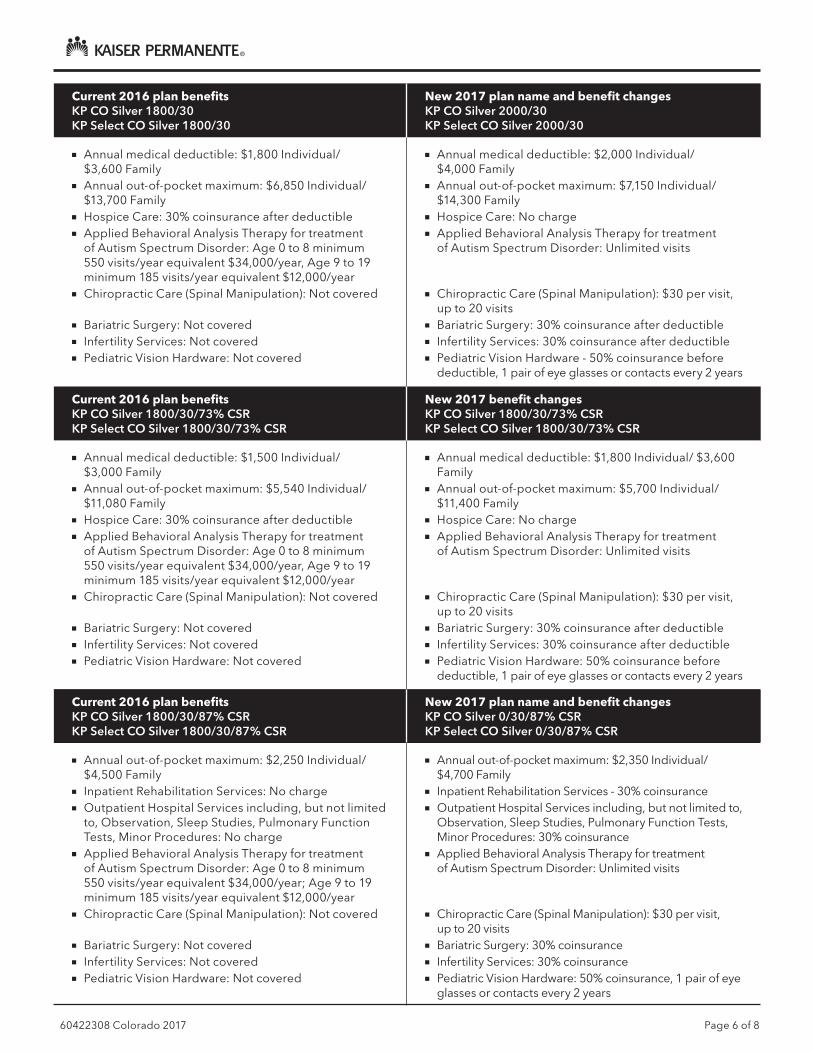
Current 2016 plan benefitsKP CO Silver 1800/30KP Select CO Silver 1800/30
New 2017 plan name and benefit changesKP CO Silver 2000/30KP Select CO Silver 2000/30
■■ Annual medical deductible: $1,800 Individual/ $3,600 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Hospice Care: 30% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $2,000 Individual/ $4,000 Family
■■ Annual out-of-pocket maximum: $7,150 Individual/ $14,300 Family
■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $30 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware - 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 1800/30/73% CSRKP Select CO Silver 1800/30/73% CSR
New 2017 benefit changesKP CO Silver 1800/30/73% CSRKP Select CO Silver 1800/30/73% CSR
■■ Annual medical deductible: $1,500 Individual/ $3,000 Family
■■ Annual out-of-pocket maximum: $5,540 Individual/ $11,080 Family
■■ Hospice Care: 30% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $1,800 Individual/ $3,600 Family
■■ Annual out-of-pocket maximum: $5,700 Individual/ $11,400 Family
■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $30 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance after deductible■■ Infertility Services: 30% coinsurance after deductible■■ Pediatric Vision Hardware: 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Silver 1800/30/87% CSRKP Select CO Silver 1800/30/87% CSR
New 2017 plan name and benefit changesKP CO Silver 0/30/87% CSRKP Select CO Silver 0/30/87% CSR
■■ Annual out-of-pocket maximum: $2,250 Individual/ $4,500 Family
■■ Inpatient Rehabilitation Services: No charge■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: No charge
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year; Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual out-of-pocket maximum: $2,350 Individual/ $4,700 Family
■■ Inpatient Rehabilitation Services - 30% coinsurance■■ Outpatient Hospital Services including, but not limited to,
Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: 30% coinsurance
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $30 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance■■ Infertility Services: 30% coinsurance■■ Pediatric Vision Hardware: 50% coinsurance, 1 pair of eye
glasses or contacts every 2 years

Page 7 of 860422308 Colorado 2017
Current 2016 plan benefitsKP CO Silver 1800/30/94% CSRKP Select CO Silver 1800/30/94% CSR
New 2017 plan name and benefit changesKP CO Silver 0/5/94% CSRKP Select CO Silver 0/5/94% CSR
■■ Inpatient Rehabilitation Services: No charge■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: No charge
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year; Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Inpatient Rehabilitation Services: 20% coinsurance■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: 20% coinsurance
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $5 per visit, up to 20 visits
■■ Bariatric Surgery: 20% coinsurance■■ Infertility Services: 20% coinsurance■■ Pediatric Vision Hardware: 50% coinsurance, 1 pair
of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO Gold 1000/20KP Select CO Gold 1000/20
New 2017 plan name and benefit changesKP CO Gold 1250/20KP Select CO Gold 1250/20
■■ Annual medical deductible: $1,000 Individual/ $2,000 Family
■■ Annual out-of-pocket maximum: $6,350 Individual/ $12,700 Family
■■ Hospice Care: 20% coinsurance after deductible■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual medical deductible: $1,250 Individual/ $2,500 Family
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Hospice Care: No charge■■ Applied Behavioral Analysis Therapy for treatment
of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $20 per visit, up to 20 visits
■■ Bariatric Surgery - 20% coinsurance after deductible■■ Infertility Services - 20% coinsurance after deductible■■ Pediatric Vision Hardware - 50% coinsurance before
deductible, 1 pair of eye glasses or contacts every 2 years

Page 8 of 860422308 Colorado 2017
Need help? For more details of your coverage, visit kp.org/renewalinfo and click on “Your 2017 Summary of Benefits and Coverage.” You can also view the Summary of Benefits and Coverage at kp.org/sbc, or get a paper copy at any time without charge by calling the number listed below for your service area.
Current 2016 plan benefitsKP CO Gold 0/20KP Select CO Gold 0/20
New 2017 benefit changesKP CO Gold 0/20KP Select CO Gold 0/20
■■ Annual out-of-pocket maximum: $6,850 Individual/ $13,700 Family
■■ Emergency Department visit: $250■■ Inpatient Hospital care: $500 per day up to 4 days■■ Inpatient Rehabilitation Services: No charge■■ MRI, CT, PET Imaging: $250■■ Prescription drugs – Non-preferred brand: $570 per fill■■ Prescription drugs – Non-preferred generic: $570 per fill■■ Prescription drugs - Specialty: $570 per fill■■ Office Injectables and Infused Medications:
$570 per drug■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: No charge
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Annual out-of-pocket maximum: $6,350 Individual/ $12,700 Family
■■ Emergency Department visit: $500■■ Inpatient Hospital care: 30% coinsurance■■ Inpatient Rehabilitation Services: 30% coinsurance■■ MRI, CT, PET Imaging: $500■■ Prescription drugs - Non-preferred brand: $150 per fill■■ Prescription drugs - Non-preferred generic: $150 per fill■■ Prescription drugs - Specialty: $500 per fill ■■ Office Injectables and Infused Medications:
$500 per drug■■ Outpatient Hospital Services including, but not limited
to, Observation, Sleep Studies, Pulmonary Function Tests, Minor Procedures: 30% coinsurance
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): $20 per visit, up to 20 visits
■■ Bariatric Surgery: 30% coinsurance■■ Infertility Services: 30% coinsurance■■ Pediatric Vision Hardware: 50% coinsurance, 1 pair
of eye glasses or contacts every 2 years
Current 2016 plan benefitsKP CO CatastrophicKP Select CO Catastrophic
New 2017 benefit changesKP CO CatastrophicKP Select CO Catastrophic
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Age 0 to 8 minimum 550 visits/year equivalent $34,000/year, Age 9 to 19 minimum 185 visits/year equivalent $12,000/year
■■ Chiropractic Care (Spinal Manipulation): Not covered
■■ Bariatric Surgery: Not covered■■ Infertility Services: Not covered■■ Pediatric Vision Hardware: Not covered
■■ Applied Behavioral Analysis Therapy for treatment of Autism Spectrum Disorder: Unlimited visits
■■ Chiropractic Care (Spinal Manipulation): 0% coinsurance after deductible, up to 20 visits
■■ Bariatric Surgery: 0% coinsurance after deductible■■ Infertility Services: 0% coinsurance after deductible■■ Pediatric Vision Hardware: 0% coinsurance after
deductible, 1 pair of eye glasses or contacts every 2 years
Changes are effective January 1, 2017, and are subject to change.
Denver/Boulder 1-303-338-3800Northern Colorado 1-844-201-5824Mountain Colorado 1-844-837-6884
Southern Colorado 1-888-681-7878For TTY, call 711.
Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
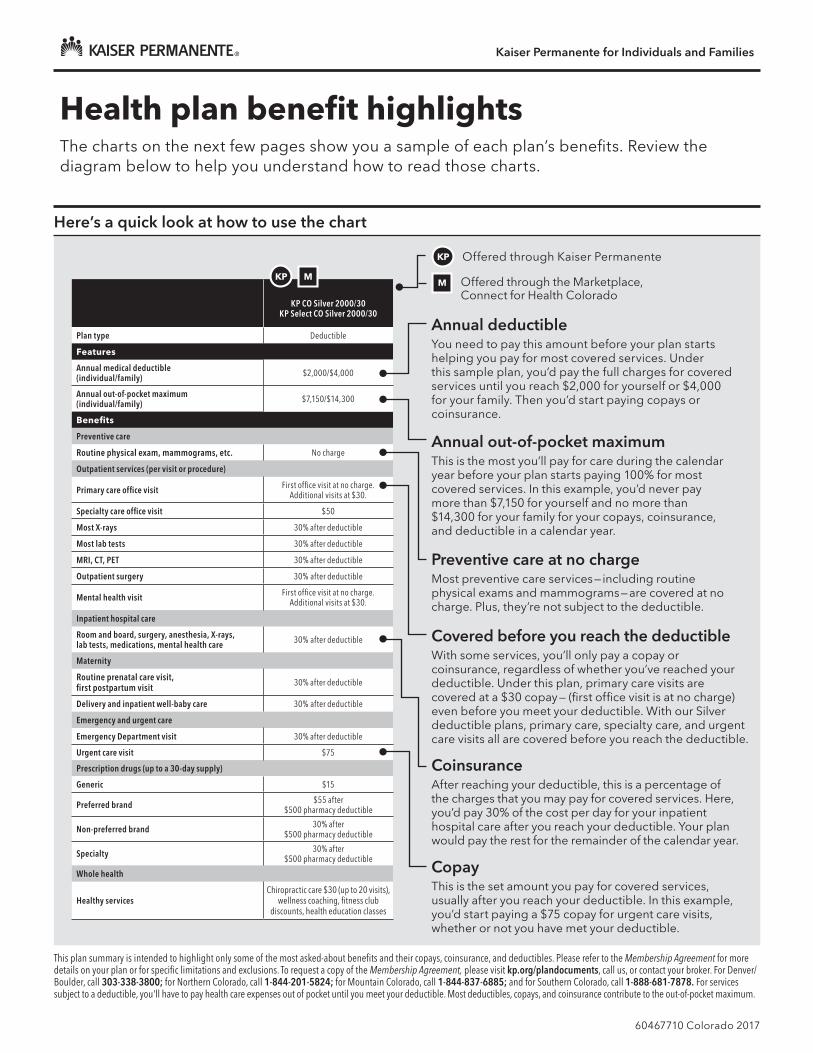
KP CO Silver 2000/30
KP Select CO Silver 2000/30
Plan type Deductible
Features
Annual medical deductible(individual/family) $2,000/$4,000
Annual out-of-pocket maximum (individual/family) $7,150/$14,300
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge
Outpatient services (per visit or procedure)
Primary care office visit First office visit at no charge. Additional visits at $30.
Specialty care office visit $50
Most X-rays 30% after deductible
Most lab tests 30% after deductible
MRI, CT, PET 30% after deductible
Outpatient surgery 30% after deductible
Mental health visit First office visit at no charge. Additional visits at $30.
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 30% after deductible
Maternity
Routine prenatal care visit, first postpartum visit 30% after deductible
Delivery and inpatient well-baby care 30% after deductible
Emergency and urgent care
Emergency Department visit 30% after deductible
Urgent care visit $75
Prescription drugs (up to a 30-day supply)
Generic $15
Preferred brand $55 after $500 pharmacy deductible
Non-preferred brand 30% after $500 pharmacy deductible
Specialty 30% after $500 pharmacy deductible
Whole health
Healthy servicesChiropractic care $30 (up to 20 visits),
wellness coaching, fitness club discounts, health education classes
Here’s a quick look at how to use the chart
Annual deductibleYou need to pay this amount before your plan starts helping you pay for most covered services. Under this sample plan, you’d pay the full charges for covered services until you reach $2,000 for yourself or $4,000 for your family. Then you’d start paying copays or coinsurance.
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Connect for Health Colorado
Preventive care at no chargeMost preventive care services — including routine physical exams and mammograms — are covered at no charge. Plus, they’re not subject to the deductible.
CoinsuranceAfter reaching your deductible, this is a percentage of the charges that you may pay for covered services. Here, you’d pay 30% of the cost per day for your inpatient hospital care after you reach your deductible. Your plan would pay the rest for the remainder of the calendar year.
Covered before you reach the deductibleWith some services, you’ll only pay a copay or coinsurance, regardless of whether you’ve reached your deductible. Under this plan, primary care visits are covered at a $30 copay — (first office visit is at no charge) even before you meet your deductible. With our Silver deductible plans, primary care, specialty care, and urgent care visits all are covered before you reach the deductible.
CopayThis is the set amount you pay for covered services, usually after you reach your deductible. In this example, you’d start paying a $75 copay for urgent care visits, whether or not you have met your deductible.
Annual out-of-pocket maximumThis is the most you’ll pay for care during the calendar year before your plan starts paying 100% for most covered services. In this example, you’d never pay more than $7,150 for yourself and no more than $14,300 for your family for your copays, coinsurance, and deductible in a calendar year.
KP M
Health plan benefit highlightsThe charts on the next few pages show you a sample of each plan’s benefits. Review the diagram below to help you understand how to read those charts.
This plan summary is intended to highlight only some of the most asked-about benefits and their copays, coinsurance, and deductibles. Please refer to the Membership Agreement for more details on your plan or for specific limitations and exclusions. To request a copy of the Membership Agreement, please visit kp.org/plandocuments, call us, or contact your broker. For Denver/Boulder, call 303-338-3800; for Northern Colorado, call 1-844-201-5824; for Mountain Colorado, call 1-844-837-6885; and for Southern Colorado, call 1-888-681-7878. For services subject to a deductible, you'll have to pay health care expenses out of pocket until you meet your deductible. Most deductibles, copays, and coinsurance contribute to the out-of-pocket maximum.
Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Connect for Health Colorado
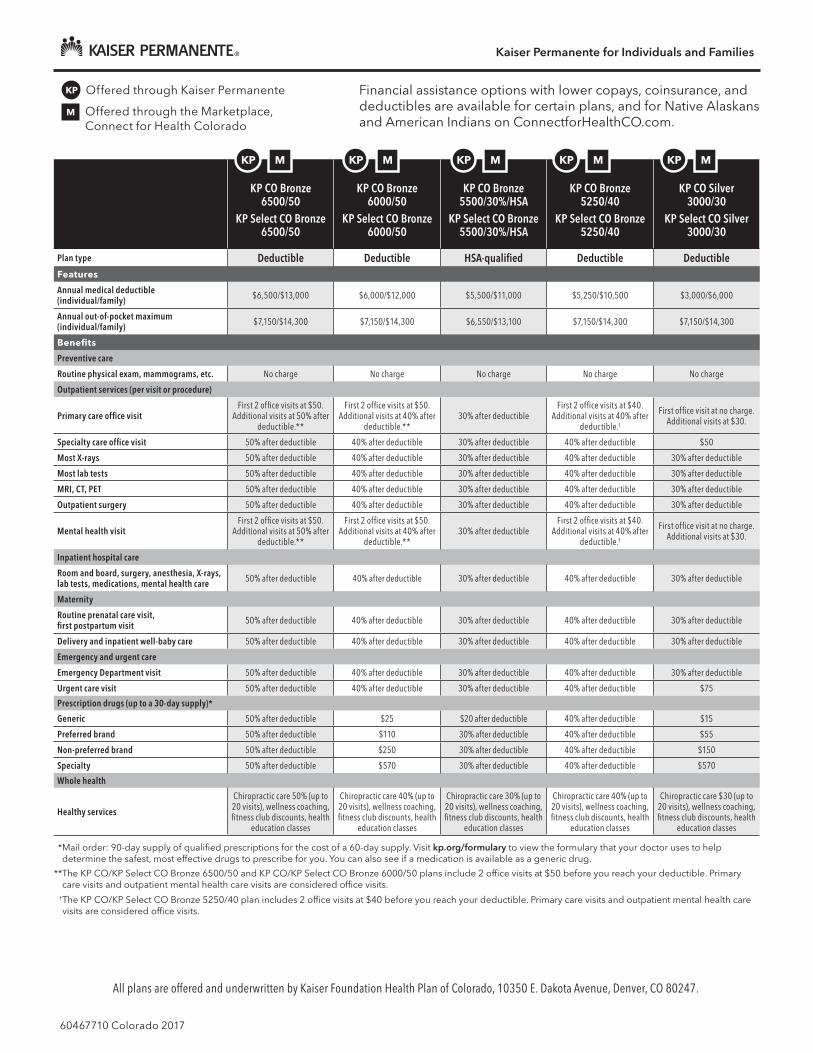
Financial assistance options with lower copays, coinsurance, and deductibles are available for certain plans, and for Native Alaskans and American Indians on ConnectforHealthCO.com.
KP CO Bronze 6500/50
KP Select CO Bronze 6500/50
KP CO Bronze 6000/50
KP Select CO Bronze 6000/50
KP CO Bronze 5500/30%/HSA
KP Select CO Bronze 5500/30%/HSA
KP CO Bronze 5250/40
KP Select CO Bronze 5250/40
KP CO Silver 3000/30
KP Select CO Silver 3000/30
Plan type Deductible Deductible HSA-qualified Deductible DeductibleFeatures
Annual medical deductible(individual/family) $6,500/$13,000 $6,000/$12,000 $5,500/$11,000 $5,250/$10,500 $3,000/$6,000
Annual out-of-pocket maximum (individual/family) $7,150/$14,300 $7,150/$14,300 $6,550/$13,100 $7,150/$14,300 $7,150/$14,300
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visitFirst 2 office visits at $50.
Additional visits at 50% after deductible.**
First 2 office visits at $50.Additional visits at 40% after
deductible.**30% after deductible
First 2 office visits at $40.Additional visits at 40% after
deductible.†
First office visit at no charge. Additional visits at $30.
Specialty care office visit 50% after deductible 40% after deductible 30% after deductible 40% after deductible $50
Most X-rays 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Most lab tests 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
MRI, CT, PET 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Outpatient surgery 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Mental health visitFirst 2 office visits at $50.
Additional visits at 50% after deductible.**
First 2 office visits at $50.Additional visits at 40% after
deductible.**30% after deductible
First 2 office visits at $40.Additional visits at 40% after
deductible.†
First office visit at no charge. Additional visits at $30.
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Maternity
Routine prenatal care visit, first postpartum visit 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Delivery and inpatient well-baby care 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Emergency and urgent care
Emergency Department visit 50% after deductible 40% after deductible 30% after deductible 40% after deductible 30% after deductible
Urgent care visit 50% after deductible 40% after deductible 30% after deductible 40% after deductible $75
Prescription drugs (up to a 30-day supply)*
Generic 50% after deductible $25 $20 after deductible 40% after deductible $15
Preferred brand 50% after deductible $110 30% after deductible 40% after deductible $55
Non-preferred brand 50% after deductible $250 30% after deductible 40% after deductible $150
Specialty 50% after deductible $570 30% after deductible 40% after deductible $570
Whole health
Healthy services
Chiropractic care 50% (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care 40% (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care 30% (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care 40% (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care $30 (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
* Mail order: 90-day supply of qualified prescriptions for the cost of a 60-day supply. Visit kp.org/formulary to view the formulary that your doctor uses to help determine the safest, most effective drugs to prescribe for you. You can also see if a medication is available as a generic drug.
** The KP CO/KP Select CO Bronze 6500/50 and KP CO/KP Select CO Bronze 6000/50 plans include 2 office visits at $50 before you reach your deductible. Primary care visits and outpatient mental health care visits are considered office visits.
† The KP CO/KP Select CO Bronze 5250/40 plan includes 2 office visits at $40 before you reach your deductible. Primary care visits and outpatient mental health care visits are considered office visits.
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.
KP M KP M KP M KP M KP M

Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
KP Offered through Kaiser Permanente
M Offered through the Marketplace, Connect for Health Colorado
Financial assistance options with lower copays, coinsurance, and deductibles are available for certain plans, and for Native Alaskans and American Indians on ConnectforHealthCO.com.
KP CO Silver 2750/20%/HSA
KP Select CO Silver 2750/20%/HSA
KP CO Silver 2000/30
KP Select CO Silver 2000/30
KP CO Gold 1250/20KP Select CO Gold
1250/20
KP CO Gold 0/20KP Select CO Gold
0/20
KP CO Catastrophic†
KP Select CO Catastrophic†
Plan type HSA-qualified Deductible Deductible Copay Deductible Features
Annual medical deductible(individual/family) $2,750/$5,500 $2,000/$4,000 $1,250/$2,500 $0 $7,150/$14,300
Annual out-of-pocket maximum (individual/family) $5,000/$10,000 $7,150/$14,300 $6,850/$13,700 $6,350/$12,700 $7,150/$14,300
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit 20% after deductible First office visit at no charge. Additional visits at $30. $20 $20
First 3 office visits at no charge. Additional visits at
no charge after deductible.††
Specialty care office visit 20% after deductible $50 $40 $40 No charge after deductible
Most X-rays 20% after deductible 30% after deductible 20% after deductible 30% No charge after deductible
Most lab tests 20% after deductible 30% after deductible 20% after deductible 30% No charge after deductible
MRI, CT, PET 20% after deductible 30% after deductible 20% after deductible $500 No charge after deductible
Outpatient surgery 20% after deductible 30% after deductible 20% after deductible 30% No charge after deductible
Mental health visit 20% after deductible First office visit at no charge. Additional visits at $30. $20 $20
First 3 office visits at no charge. Additional visits at
no charge after deductible.††
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 20% after deductible 30% after deductible 20% after deductible 30% No charge after deductible
Maternity
Routine prenatal care visit, first postpartum visit 20% after deductible 30% after deductible 20% after deductible No charge No charge after deductible
Delivery and inpatient well-baby care 20% after deductible 30% after deductible 20% after deductible 30% No charge after deductible
Emergency and urgent care
Emergency Department visit 20% after deductible 30% after deductible 20% after deductible $500 No charge after deductible
Urgent care visit 20% after deductible $75 $75 $75 No charge after deductible
Prescription drugs (up to a 30-day supply)*
Generic $15 after deductible $15 $10 $10 No charge after deductible
Preferred brand $55 after deductible $55 after $500 pharmacy deductible $30 $30 No charge after deductible
Non-preferred brand 20% after deductible 30% after $500 pharmacy deductible 20% $150 No charge after deductible
Specialty 20% after deductible 30% after $500 pharmacy deductible 20% $500 No charge after deductible
Whole health
Healthy services
Chiropractic care 20% (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care $30 (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care $20 (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care $20 (up to 20 visits), wellness coaching, fitness club discounts, health
education classes
Chiropractic care no charge after deductible (up to 20 visits), wellness coaching,
fitness club discounts,health education classes
* Mail order: 90-day supply of qualified prescriptions for the cost of a 60-day supply. Visit kp.org/formulary to view the formulary that your doctor uses to help determine the safest, most effective drugs to prescribe for you. You can also see if a medication is available as a generic drug.
† Only applicants younger than age 30 or applicants age 30 and older who receive an exemption due to lack of affordable coverage or hardship may enroll in this plan. To apply for an exemption, please go to marketplace.cms.gov/applications-and-forms/hardship-exemption.pdf and follow the instructions.
†† The KP CO/KP Select CO Catastrophic plan includes 3 office visits at no charge before you reach your deductible. Primary care visits and outpatient mental health care visits are considered office visits.
KP M KP M KP M KP M KP M
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.

Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
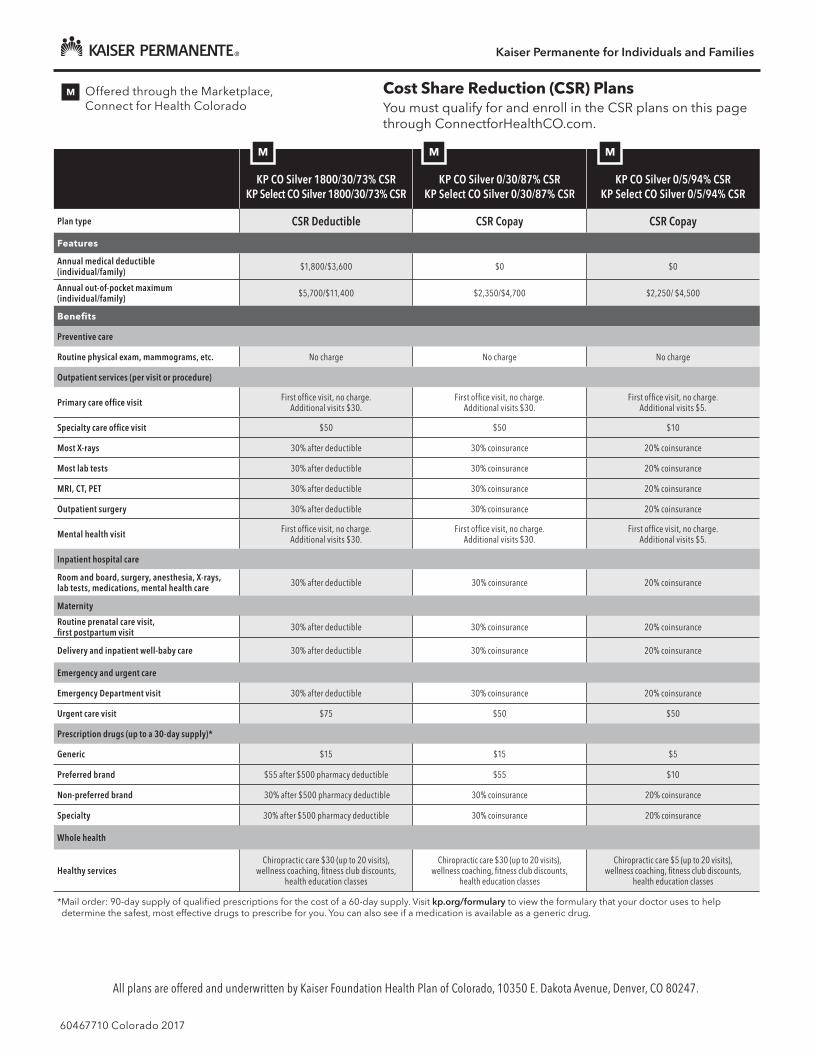
KP CO Silver 2000/30/73% CSR
KP Select CO Silver 2000/30/73% CSR
KP CO Silver 200/20/87% CSR
KP Select CO Silver 200/20/87% CSR
KP CO Silver 0/10/94% CSR
KP Select CO Silver 0/10/94% CSR
Plan type CSR Deductible CSR Deductible CSR Copay
Features
Annual medical deductible(individual/family) $2,000/$4,000 $200/$400 $0
Annual out-of-pocket maximum (individual/family) $5,700/$11,400 $2,350/$4,700 $2,250/ $4,500
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $20.
First office visit, no charge.Additional visits $10.
Specialty care office visit $50 $40 $20
Most X-rays 30% after deductible 30% after deductible 10% coinsurance
Most lab tests 30% after deductible 30% after deductible 10% coinsurance
MRI, CT, PET 30% after deductible 30% after deductible 10% coinsurance
Outpatient surgery 30% after deductible 30% after deductible 10% coinsurance
Mental health visit First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $20.
First office visit, no charge.Additional visits $10.
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 30% after deductible 30% after deductible 10% coinsurance
Maternity
Routine prenatal care visit, first postpartum visit 30% after deductible 30% after deductible 10% coinsurance
Delivery and inpatient well-baby care 30% after deductible 30% after deductible 10% coinsurance
Emergency and urgent care
Emergency Department visit 30% after deductible 30% after deductible 10% coinsurance
Urgent care visit $75 $50 $50
Prescription drugs (up to a 30-day supply)*
Generic $15 $10 $5
Preferred brand $55 $45 $10
Non-preferred brand $150 $150 $150
Specialty $570 $400 $250
Whole health
Healthy servicesChiropractic care $30 (up to 20 visits),
wellness coaching, fitness club discounts, health education classes
Chiropractic care $20 (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
Chiropractic care $10 (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
* Mail order: 90-day supply of qualified prescriptions for the cost of a 60-day supply. Visit kp.org/formulary to view the formulary that your doctor uses to help determine the safest, most effective drugs to prescribe for you. You can also see if a medication is available as a generic drug.
M Offered through the Marketplace, Connect for Health Colorado
Cost Share Reduction (CSR) Plans You must qualify for and enroll in the CSR plans on this page through ConnectforHealthCO.com.
M M M
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.

Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
KP CO Silver 1900/20%/73% CSR†
KP Select CO Silver 1900/20%/73% CSR†
KP CO Silver 500/10%/87% CSR†
KP Select CO Silver 500/10%/87% CSR†
KP CO Silver 200/5%/94% CSR†
KP Select CO Silver 200/5%/94% CSR†
Plan type CSR Deductible CSR Deductible CSR Deductible
Features
Annual medical deductible(individual/family) $1,900/$3,800 $500/$1,000 $200/$400
Annual out-of-pocket maximum (individual/family) $5,000/$10,000 $2,350/$4,700 $2,250/$4,500
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit 20% after deductible 10% after deductible 5% after deductible
Specialty care office visit 20% after deductible 10% after deductible 5% after deductible
Most X-rays 20% after deductible 10% after deductible 5% after deductible
Most lab tests 20% after deductible 10% after deductible 5% after deductible
MRI, CT, PET 20% after deductible 10% after deductible 5% after deductible
Outpatient surgery 20% after deductible 10% after deductible 5% after deductible
Mental health visit 20% after deductible 10% after deductible 5% after deductible
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 20% after deductible 10% after deductible 5% after deductible
Maternity
Routine prenatal care visit, first postpartum visit 20% after deductible 10% after deductible 5% after deductible
Delivery and inpatient well-baby care 20% after deductible 10% after deductible 5% after deductible
Emergency and urgent care
Emergency Department visit 20% after deductible 10% after deductible 5% after deductible
Urgent care visit 20% after deductible 10% after deductible 5% after deductible
Prescription drugs (up to a 30-day supply)*
Generic $10 after deductible $10 after deductible $5 after deductible
Preferred brand $45 after deductible $30 after deductible $10 after deductible
Non-preferred brand 20% after deductible 10% after deductible 5% after deductible
Specialty 20% after deductible 10% after deductible 5% after deductible
Whole health
Healthy servicesChiropractic care 20% (up to 20 visits),
wellness coaching, fitness club discounts, health education classes
Chiropractic care 10% (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
Chiropractic care 5% (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
* Mail order: 90-day supply of qualified prescriptions for the cost of a 60-day supply. Visit kp.org/formulary to view the formulary that your doctor uses to help determine the safest, most effective drugs to prescribe for you. You can also see if a medication is available as a generic drug.
† This plan is no longer qualified to be paired with an optional tax-advantaged HSA account.
M Offered through the Marketplace, Connect for Health Colorado
Cost Share Reduction (CSR) Plans You must qualify for and enroll in the CSR plans on this page through ConnectforHealthCO.com.
M M M
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.
Kaiser Permanente for Individuals and Families
60467710 Colorado 2017
KP CO Silver 1800/30/73% CSR
KP Select CO Silver 1800/30/73% CSR
KP CO Silver 0/30/87% CSR
KP Select CO Silver 0/30/87% CSR
KP CO Silver 0/5/94% CSR
KP Select CO Silver 0/5/94% CSR
Plan type CSR Deductible CSR Copay CSR Copay
Features
Annual medical deductible(individual/family) $1,800/$3,600 $0 $0
Annual out-of-pocket maximum (individual/family) $5,700/$11,400 $2,350/$4,700 $2,250/ $4,500
Benefits
Preventive care
Routine physical exam, mammograms, etc. No charge No charge No charge
Outpatient services (per visit or procedure)
Primary care office visit First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $5.
Specialty care office visit $50 $50 $10
Most X-rays 30% after deductible 30% coinsurance 20% coinsurance
Most lab tests 30% after deductible 30% coinsurance 20% coinsurance
MRI, CT, PET 30% after deductible 30% coinsurance 20% coinsurance
Outpatient surgery 30% after deductible 30% coinsurance 20% coinsurance
Mental health visit First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $30.
First office visit, no charge.Additional visits $5.
Inpatient hospital care
Room and board, surgery, anesthesia, X-rays, lab tests, medications, mental health care 30% after deductible 30% coinsurance 20% coinsurance
Maternity
Routine prenatal care visit, first postpartum visit 30% after deductible 30% coinsurance 20% coinsurance
Delivery and inpatient well-baby care 30% after deductible 30% coinsurance 20% coinsurance
Emergency and urgent care
Emergency Department visit 30% after deductible 30% coinsurance 20% coinsurance
Urgent care visit $75 $50 $50
Prescription drugs (up to a 30-day supply)*
Generic $15 $15 $5
Preferred brand $55 after $500 pharmacy deductible $55 $10
Non-preferred brand 30% after $500 pharmacy deductible 30% coinsurance 20% coinsurance
Specialty 30% after $500 pharmacy deductible 30% coinsurance 20% coinsurance
Whole health
Healthy servicesChiropractic care $30 (up to 20 visits),
wellness coaching, fitness club discounts, health education classes
Chiropractic care $30 (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
Chiropractic care $5 (up to 20 visits), wellness coaching, fitness club discounts,
health education classes
* Mail order: 90-day supply of qualified prescriptions for the cost of a 60-day supply. Visit kp.org/formulary to view the formulary that your doctor uses to help determine the safest, most effective drugs to prescribe for you. You can also see if a medication is available as a generic drug.
M Offered through the Marketplace, Connect for Health Colorado
Cost Share Reduction (CSR) Plans You must qualify for and enroll in the CSR plans on this page through ConnectforHealthCO.com.
M M M
All plans are offered and underwritten by Kaiser Foundation Health Plan of Colorado, 10350 E. Dakota Avenue, Denver, CO 80247.
Rate chart guideDenver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado
Kaiser Permanente for Individuals and Families n January 2017
To use the Rate Chart Guide, first determine your rate area by finding your ZIP code and county in the chart beginning on page 2. Then locate the page listing your rate area. Your monthly rate will appear in the box where your age and plan intersect.
Rates are determined individually, whether you apply individually or as a family, and are based on the following:
n The plan you select
n Where you live, based on your ZIP code and county
n Your age on the plan’s effective or renewal date
n Whether you use tobacco
If you move and change your home ZIP code and county, your monthly rate may change. If you move to a ZIP code and county that aren’t covered by Kaiser Permanente, your coverage may not continue.
Tobacco use
Rates shown in this guide are for those individuals who do not use tobacco. Tobacco users 21 and older may pay higher rates than those shown here.
Although family members can enroll in different plans, there are some advantages to enrolling family members in the same plan:
n Children can be covered under your plan until they reach age 26, whether or not they’re in school or living at home.
n If you have more than 3 children under age 21 on the same plan, you will only be charged for the 3 oldest. Other children under 21 are covered at no additional cost.
n If you have a child-only account and everyone on the account is under 21, you’ll only be charged for the subscriber (the oldest child on the plan) and the next 3 oldest children under 21.
Health plans include pediatric dental benefits for children 18 and younger.
You may qualify for federal financial assistance
If you qualify for federal financial assistance, these rates will not apply to you. If you are eligible, the federal government will pay the financial assistance to Kaiser Permanente directly.
2017 Enrollment
60467809 January 2017 Colorado

Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 2
Service area ZIP codes for Denver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado
ZIP Code County Rate Area
69128 Weld 6
69145 Weld 6
80001 Jefferson 3
80002 Jefferson 3
80002 Adams 3
80003 Adams 3
80003 Jefferson 3
80004 Jefferson 3
80005 Jefferson 3
80006 Jefferson 3
80007 Jefferson 3
80010 Adams 3
80010 Arapahoe 3
80011 Arapahoe 3
80011 Adams 3
80012 Arapahoe 3
80013 Arapahoe 3
80014 Arapahoe 3
80014 Denver 3
80015 Arapahoe 3
80016 Arapahoe 3
80017 Arapahoe 3
80018 Arapahoe 3
80019 Adams 3
80020 Jefferson 3
80020 Adams 3
80020 Broomfield 3
80020 Boulder 1
80021 Broomfield 3
80021 Jefferson 3
80022 Adams 3
80023 Adams 3
80023 Broomfield 3
80024 Adams 3
80025 Boulder 1
80026 Boulder 1
80027 Boulder 1
80030 Adams 3
80031 Adams 3
80031 Jefferson 3
80033 Jefferson 3
80034 Jefferson 3
80035 Adams 3
80036 Adams 3
80037 Adams 3
80038 Broomfield 3
ZIP Code County Rate Area
80040 Adams 3
80041 Arapahoe 3
80042 Adams 3
80044 Arapahoe 3
80045 Adams 3
80046 Arapahoe 3
80047 Arapahoe 3
80102 Elbert 3
80102 Adams 3
80102 Arapahoe 3
80104 Douglas 3
80107 Elbert 3
80108 Douglas 3
80109 Douglas 3
80110 Arapahoe 3
80110 Denver 3
80111 Denver 3
80111 Arapahoe 3
80112 Arapahoe 3
80112 Denver 3
80112 Douglas 3
80113 Arapahoe 3
80116 Douglas 3
80117 Elbert 3
80120 Douglas 3
80120 Arapahoe 3
80121 Arapahoe 3
80122 Arapahoe 3
80123 Denver 3
80123 Arapahoe 3
80123 Jefferson 3
80124 Douglas 3
80125 Jefferson 3
80125 Douglas 3
80126 Douglas 3
80127 Jefferson 3
80128 Arapahoe 3
80128 Jefferson 3
80129 Arapahoe 3
80129 Douglas 3
80130 Douglas 3
80131 Douglas 3
80134 Elbert 3
80134 Douglas 3
80135 Teller 2
80135 Jefferson 3
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 3
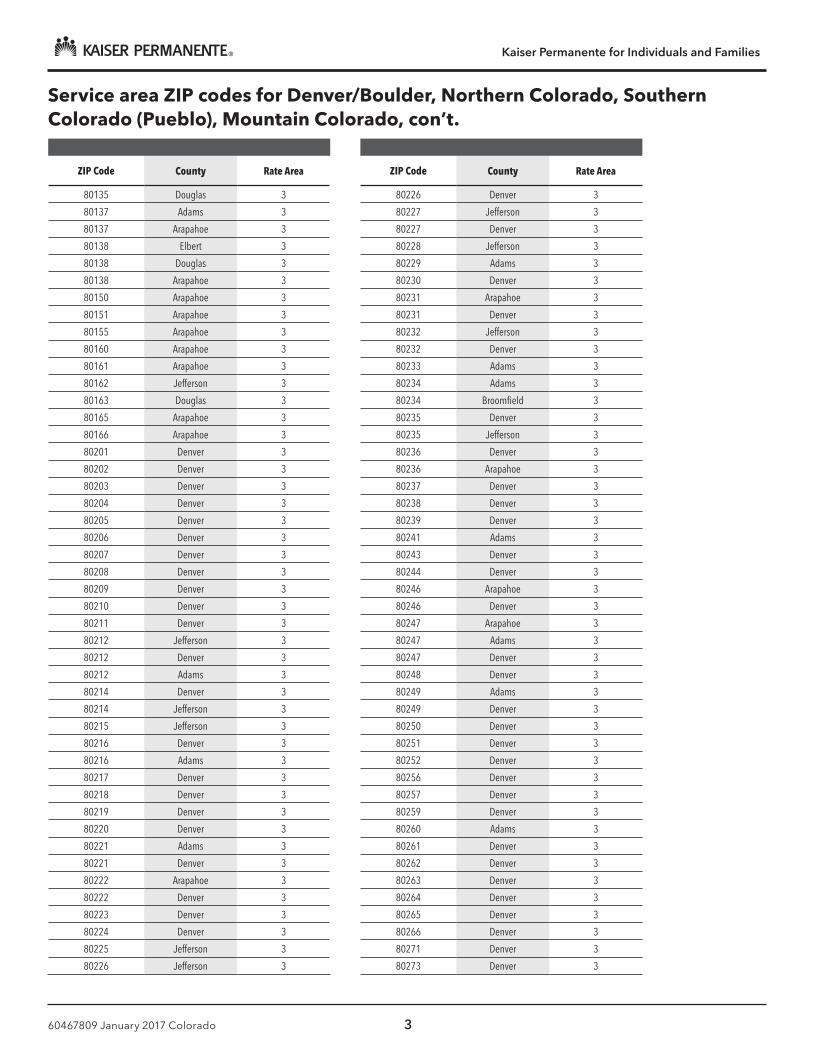
Service area ZIP codes for Denver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado, con’t.
ZIP Code County Rate Area
80135 Douglas 3
80137 Adams 3
80137 Arapahoe 3
80138 Elbert 3
80138 Douglas 3
80138 Arapahoe 3
80150 Arapahoe 3
80151 Arapahoe 3
80155 Arapahoe 3
80160 Arapahoe 3
80161 Arapahoe 3
80162 Jefferson 3
80163 Douglas 3
80165 Arapahoe 3
80166 Arapahoe 3
80201 Denver 3
80202 Denver 3
80203 Denver 3
80204 Denver 3
80205 Denver 3
80206 Denver 3
80207 Denver 3
80208 Denver 3
80209 Denver 3
80210 Denver 3
80211 Denver 3
80212 Jefferson 3
80212 Denver 3
80212 Adams 3
80214 Denver 3
80214 Jefferson 3
80215 Jefferson 3
80216 Denver 3
80216 Adams 3
80217 Denver 3
80218 Denver 3
80219 Denver 3
80220 Denver 3
80221 Adams 3
80221 Denver 3
80222 Arapahoe 3
80222 Denver 3
80223 Denver 3
80224 Denver 3
80225 Jefferson 3
80226 Jefferson 3
ZIP Code County Rate Area
80226 Denver 3
80227 Jefferson 3
80227 Denver 3
80228 Jefferson 3
80229 Adams 3
80230 Denver 3
80231 Arapahoe 3
80231 Denver 3
80232 Jefferson 3
80232 Denver 3
80233 Adams 3
80234 Adams 3
80234 Broomfield 3
80235 Denver 3
80235 Jefferson 3
80236 Denver 3
80236 Arapahoe 3
80237 Denver 3
80238 Denver 3
80239 Denver 3
80241 Adams 3
80243 Denver 3
80244 Denver 3
80246 Arapahoe 3
80246 Denver 3
80247 Arapahoe 3
80247 Adams 3
80247 Denver 3
80248 Denver 3
80249 Adams 3
80249 Denver 3
80250 Denver 3
80251 Denver 3
80252 Denver 3
80256 Denver 3
80257 Denver 3
80259 Denver 3
80260 Adams 3
80261 Denver 3
80262 Denver 3
80263 Denver 3
80264 Denver 3
80265 Denver 3
80266 Denver 3
80271 Denver 3
80273 Denver 3
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 4
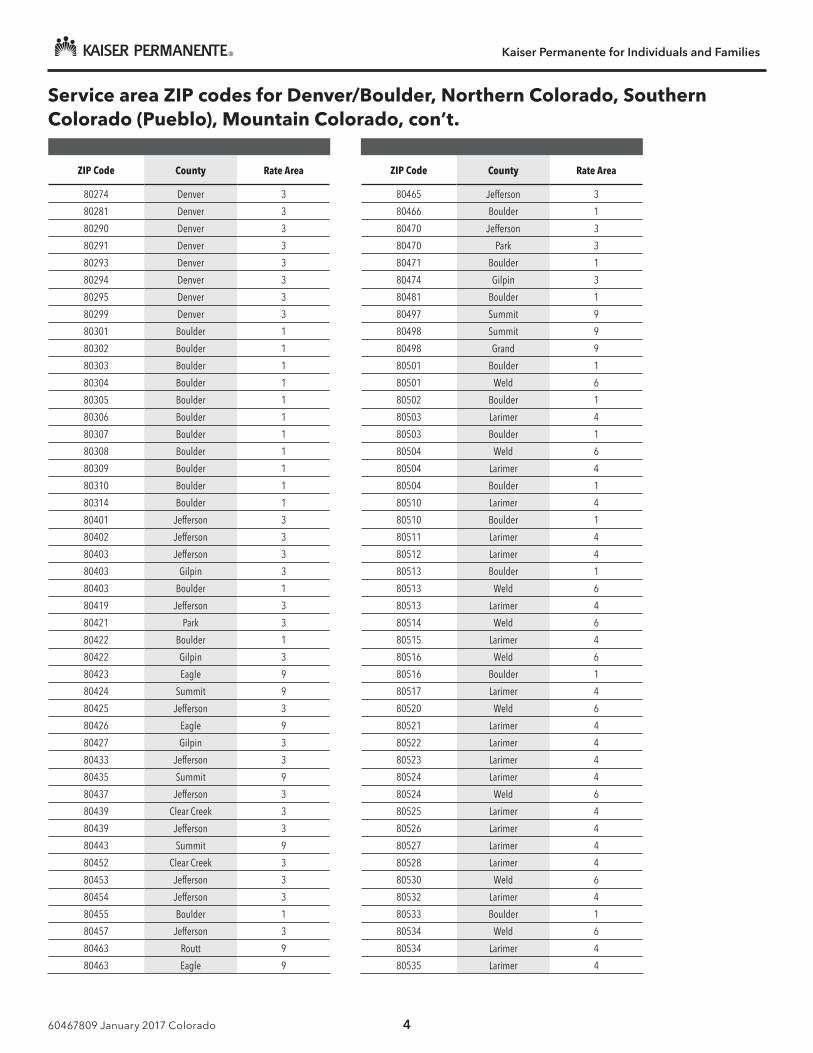
Service area ZIP codes for Denver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado, con’t.
ZIP Code County Rate Area
80274 Denver 3
80281 Denver 3
80290 Denver 3
80291 Denver 3
80293 Denver 3
80294 Denver 3
80295 Denver 3
80299 Denver 3
80301 Boulder 1
80302 Boulder 1
80303 Boulder 1
80304 Boulder 1
80305 Boulder 1
80306 Boulder 1
80307 Boulder 1
80308 Boulder 1
80309 Boulder 1
80310 Boulder 1
80314 Boulder 1
80401 Jefferson 3
80402 Jefferson 3
80403 Jefferson 3
80403 Gilpin 3
80403 Boulder 1
80419 Jefferson 3
80421 Park 3
80422 Boulder 1
80422 Gilpin 3
80423 Eagle 9
80424 Summit 9
80425 Jefferson 3
80426 Eagle 9
80427 Gilpin 3
80433 Jefferson 3
80435 Summit 9
80437 Jefferson 3
80439 Clear Creek 3
80439 Jefferson 3
80443 Summit 9
80452 Clear Creek 3
80453 Jefferson 3
80454 Jefferson 3
80455 Boulder 1
80457 Jefferson 3
80463 Routt 9
80463 Eagle 9
ZIP Code County Rate Area
80465 Jefferson 3
80466 Boulder 1
80470 Jefferson 3
80470 Park 3
80471 Boulder 1
80474 Gilpin 3
80481 Boulder 1
80497 Summit 9
80498 Summit 9
80498 Grand 9
80501 Boulder 1
80501 Weld 6
80502 Boulder 1
80503 Larimer 4
80503 Boulder 1
80504 Weld 6
80504 Larimer 4
80504 Boulder 1
80510 Larimer 4
80510 Boulder 1
80511 Larimer 4
80512 Larimer 4
80513 Boulder 1
80513 Weld 6
80513 Larimer 4
80514 Weld 6
80515 Larimer 4
80516 Weld 6
80516 Boulder 1
80517 Larimer 4
80520 Weld 6
80521 Larimer 4
80522 Larimer 4
80523 Larimer 4
80524 Larimer 4
80524 Weld 6
80525 Larimer 4
80526 Larimer 4
80527 Larimer 4
80528 Larimer 4
80530 Weld 6
80532 Larimer 4
80533 Boulder 1
80534 Weld 6
80534 Larimer 4
80535 Larimer 4
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 5
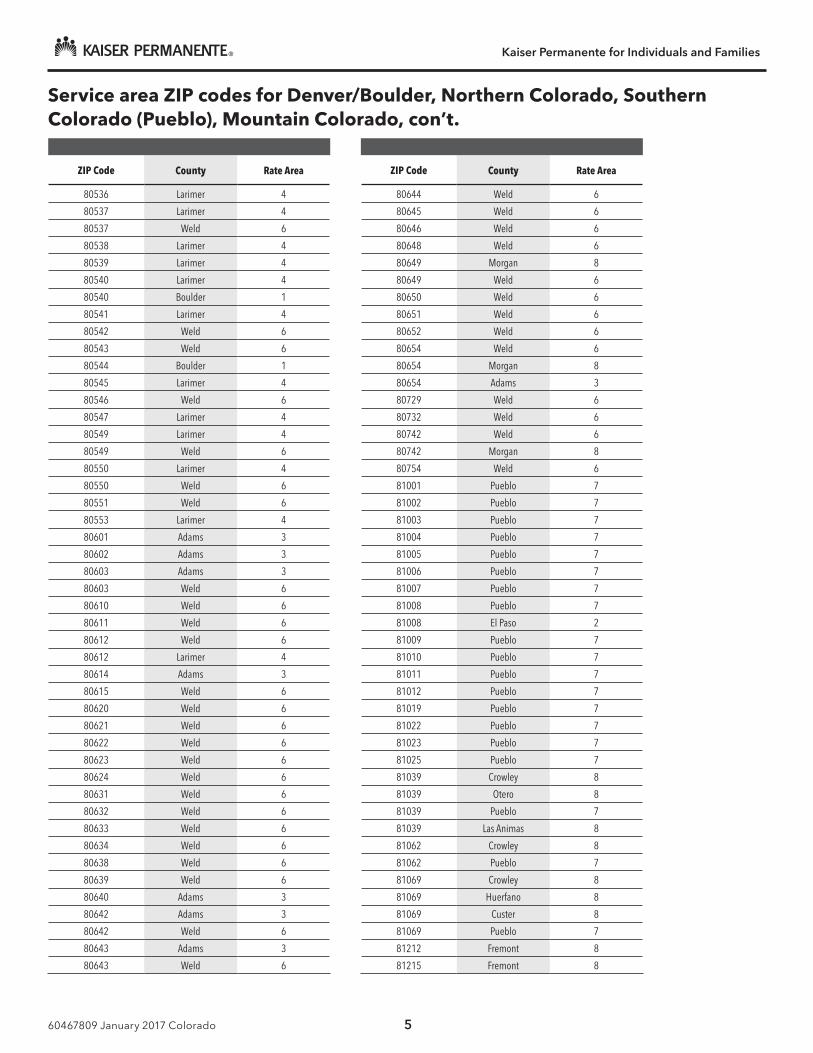
Service area ZIP codes for Denver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado, con’t.
ZIP Code County Rate Area
80536 Larimer 4
80537 Larimer 4
80537 Weld 6
80538 Larimer 4
80539 Larimer 4
80540 Larimer 4
80540 Boulder 1
80541 Larimer 4
80542 Weld 6
80543 Weld 6
80544 Boulder 1
80545 Larimer 4
80546 Weld 6
80547 Larimer 4
80549 Larimer 4
80549 Weld 6
80550 Larimer 4
80550 Weld 6
80551 Weld 6
80553 Larimer 4
80601 Adams 3
80602 Adams 3
80603 Adams 3
80603 Weld 6
80610 Weld 6
80611 Weld 6
80612 Weld 6
80612 Larimer 4
80614 Adams 3
80615 Weld 6
80620 Weld 6
80621 Weld 6
80622 Weld 6
80623 Weld 6
80624 Weld 6
80631 Weld 6
80632 Weld 6
80633 Weld 6
80634 Weld 6
80638 Weld 6
80639 Weld 6
80640 Adams 3
80642 Adams 3
80642 Weld 6
80643 Adams 3
80643 Weld 6
ZIP Code County Rate Area
80644 Weld 6
80645 Weld 6
80646 Weld 6
80648 Weld 6
80649 Morgan 8
80649 Weld 6
80650 Weld 6
80651 Weld 6
80652 Weld 6
80654 Weld 6
80654 Morgan 8
80654 Adams 3
80729 Weld 6
80732 Weld 6
80742 Weld 6
80742 Morgan 8
80754 Weld 6
81001 Pueblo 7
81002 Pueblo 7
81003 Pueblo 7
81004 Pueblo 7
81005 Pueblo 7
81006 Pueblo 7
81007 Pueblo 7
81008 Pueblo 7
81008 El Paso 2
81009 Pueblo 7
81010 Pueblo 7
81011 Pueblo 7
81012 Pueblo 7
81019 Pueblo 7
81022 Pueblo 7
81023 Pueblo 7
81025 Pueblo 7
81039 Crowley 8
81039 Otero 8
81039 Pueblo 7
81039 Las Animas 8
81062 Crowley 8
81062 Pueblo 7
81069 Crowley 8
81069 Huerfano 8
81069 Custer 8
81069 Pueblo 7
81212 Fremont 8
81215 Fremont 8
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 6
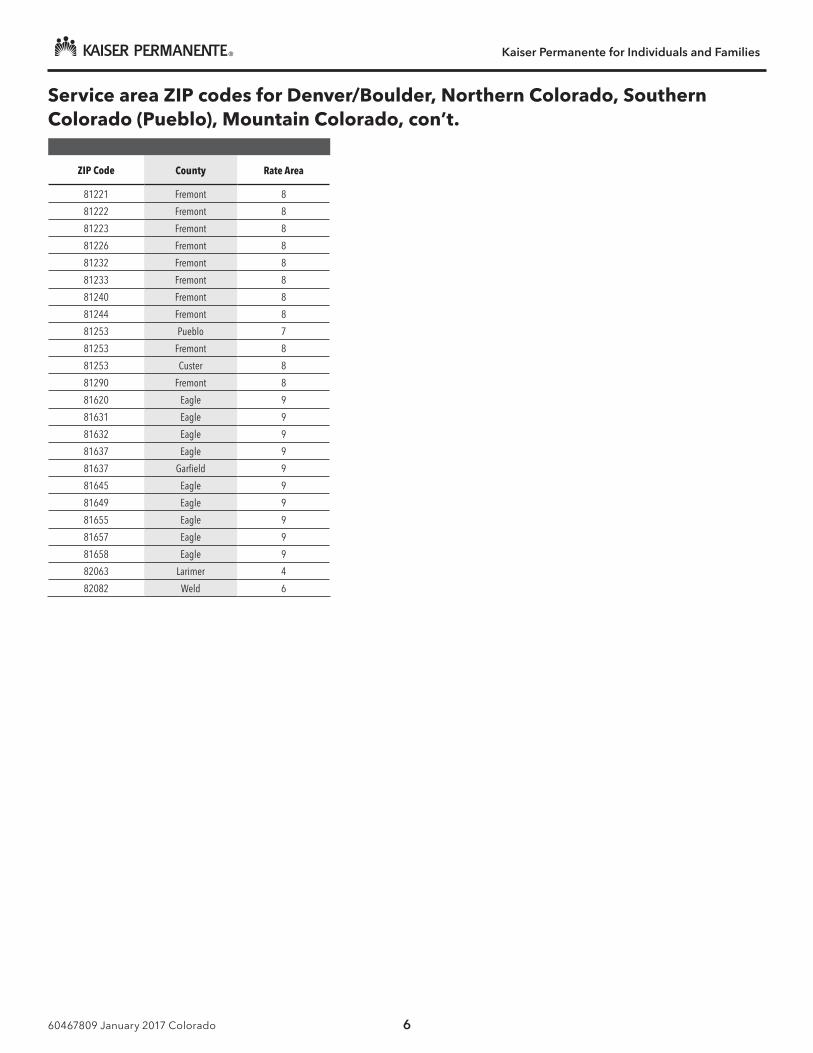
Service area ZIP codes for Denver/Boulder, Northern Colorado, Southern Colorado (Pueblo), Mountain Colorado, con’t.
ZIP Code County Rate Area
81221 Fremont 8
81222 Fremont 8
81223 Fremont 8
81226 Fremont 8
81232 Fremont 8
81233 Fremont 8
81240 Fremont 8
81244 Fremont 8
81253 Pueblo 7
81253 Fremont 8
81253 Custer 8
81290 Fremont 8
81620 Eagle 9
81631 Eagle 9
81632 Eagle 9
81637 Eagle 9
81637 Garfield 9
81645 Eagle 9
81649 Eagle 9
81655 Eagle 9
81657 Eagle 9
81658 Eagle 9
82063 Larimer 4
82082 Weld 6
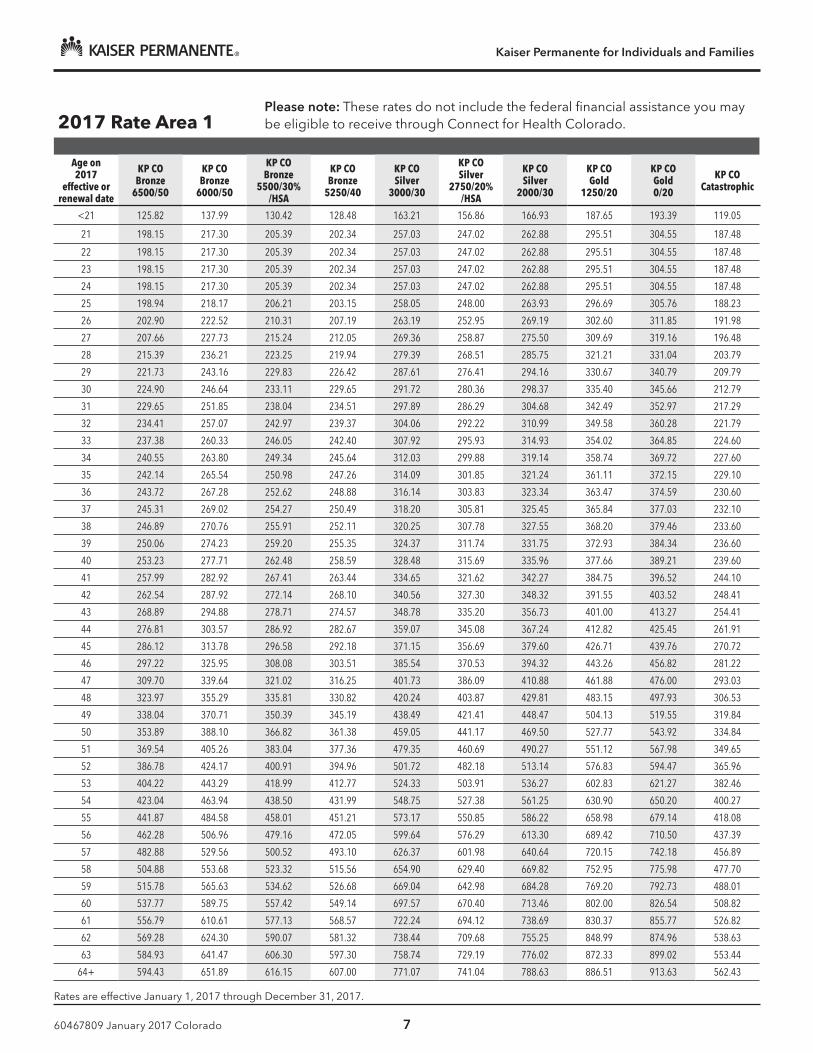
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 7
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 1Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 125.82 137.99 130.42 128.48 163.21 156.86 166.93 187.65 193.39 119.05
21 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
22 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
23 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
24 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
25 198.94 218.17 206.21 203.15 258.05 248.00 263.93 296.69 305.76 188.23
26 202.90 222.52 210.31 207.19 263.19 252.95 269.19 302.60 311.85 191.98
27 207.66 227.73 215.24 212.05 269.36 258.87 275.50 309.69 319.16 196.48
28 215.39 236.21 223.25 219.94 279.39 268.51 285.75 321.21 331.04 203.79
29 221.73 243.16 229.83 226.42 287.61 276.41 294.16 330.67 340.79 209.79
30 224.90 246.64 233.11 229.65 291.72 280.36 298.37 335.40 345.66 212.79
31 229.65 251.85 238.04 234.51 297.89 286.29 304.68 342.49 352.97 217.29
32 234.41 257.07 242.97 239.37 304.06 292.22 310.99 349.58 360.28 221.79
33 237.38 260.33 246.05 242.40 307.92 295.93 314.93 354.02 364.85 224.60
34 240.55 263.80 249.34 245.64 312.03 299.88 319.14 358.74 369.72 227.60
35 242.14 265.54 250.98 247.26 314.09 301.85 321.24 361.11 372.15 229.10
36 243.72 267.28 252.62 248.88 316.14 303.83 323.34 363.47 374.59 230.60
37 245.31 269.02 254.27 250.49 318.20 305.81 325.45 365.84 377.03 232.10
38 246.89 270.76 255.91 252.11 320.25 307.78 327.55 368.20 379.46 233.60
39 250.06 274.23 259.20 255.35 324.37 311.74 331.75 372.93 384.34 236.60
40 253.23 277.71 262.48 258.59 328.48 315.69 335.96 377.66 389.21 239.60
41 257.99 282.92 267.41 263.44 334.65 321.62 342.27 384.75 396.52 244.10
42 262.54 287.92 272.14 268.10 340.56 327.30 348.32 391.55 403.52 248.41
43 268.89 294.88 278.71 274.57 348.78 335.20 356.73 401.00 413.27 254.41
44 276.81 303.57 286.92 282.67 359.07 345.08 367.24 412.82 425.45 261.91
45 286.12 313.78 296.58 292.18 371.15 356.69 379.60 426.71 439.76 270.72
46 297.22 325.95 308.08 303.51 385.54 370.53 394.32 443.26 456.82 281.22
47 309.70 339.64 321.02 316.25 401.73 386.09 410.88 461.88 476.00 293.03
48 323.97 355.29 335.81 330.82 420.24 403.87 429.81 483.15 497.93 306.53
49 338.04 370.71 350.39 345.19 438.49 421.41 448.47 504.13 519.55 319.84
50 353.89 388.10 366.82 361.38 459.05 441.17 469.50 527.77 543.92 334.84
51 369.54 405.26 383.04 377.36 479.35 460.69 490.27 551.12 567.98 349.65
52 386.78 424.17 400.91 394.96 501.72 482.18 513.14 576.83 594.47 365.96
53 404.22 443.29 418.99 412.77 524.33 503.91 536.27 602.83 621.27 382.46
54 423.04 463.94 438.50 431.99 548.75 527.38 561.25 630.90 650.20 400.27
55 441.87 484.58 458.01 451.21 573.17 550.85 586.22 658.98 679.14 418.08
56 462.28 506.96 479.16 472.05 599.64 576.29 613.30 689.42 710.50 437.39
57 482.88 529.56 500.52 493.10 626.37 601.98 640.64 720.15 742.18 456.89
58 504.88 553.68 523.32 515.56 654.90 629.40 669.82 752.95 775.98 477.70
59 515.78 565.63 534.62 526.68 669.04 642.98 684.28 769.20 792.73 488.01
60 537.77 589.75 557.42 549.14 697.57 670.40 713.46 802.00 826.54 508.82
61 556.79 610.61 577.13 568.57 722.24 694.12 738.69 830.37 855.77 526.82
62 569.28 624.30 590.07 581.32 738.44 709.68 755.25 848.99 874.96 538.63
63 584.93 641.47 606.30 597.30 758.74 729.19 776.02 872.33 899.02 553.44
64+ 594.43 651.89 616.15 607.00 771.07 741.04 788.63 886.51 913.63 562.43
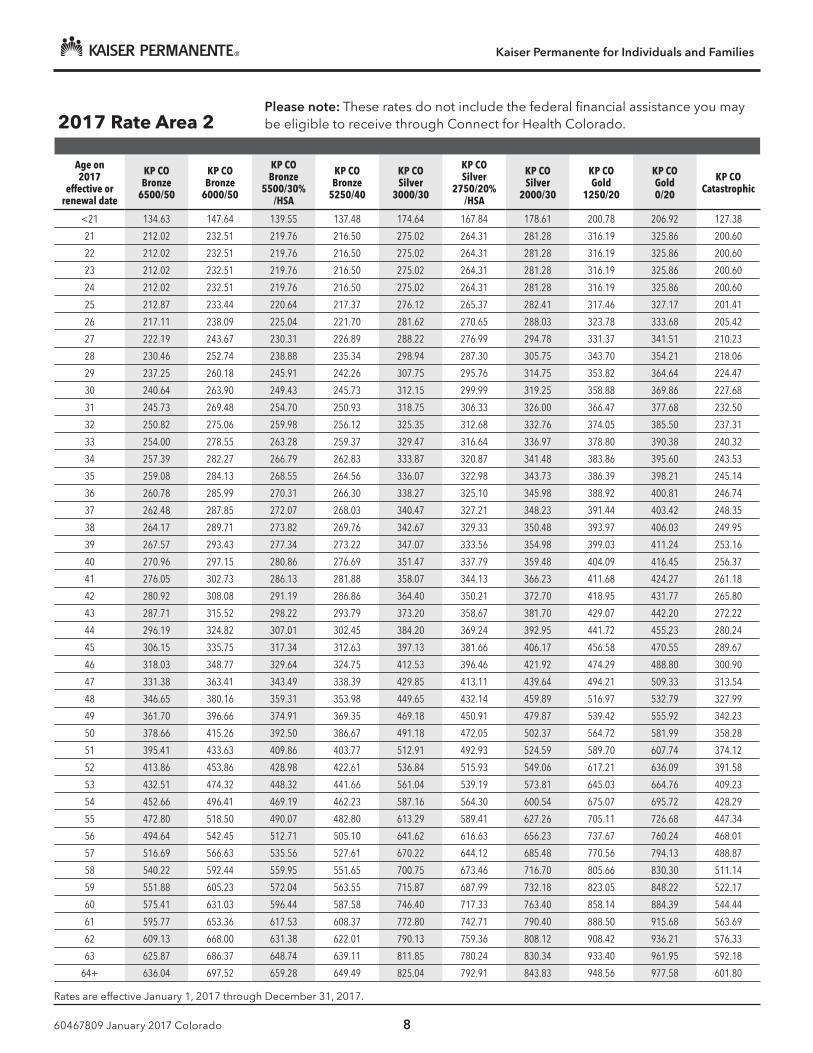
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 8
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 2Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 134.63 147.64 139.55 137.48 174.64 167.84 178.61 200.78 206.92 127.38
21 212.02 232.51 219.76 216.50 275.02 264.31 281.28 316.19 325.86 200.60
22 212.02 232.51 219.76 216.50 275.02 264.31 281.28 316.19 325.86 200.60
23 212.02 232.51 219.76 216.50 275.02 264.31 281.28 316.19 325.86 200.60
24 212.02 232.51 219.76 216.50 275.02 264.31 281.28 316.19 325.86 200.60
25 212.87 233.44 220.64 217.37 276.12 265.37 282.41 317.46 327.17 201.41
26 217.11 238.09 225.04 221.70 281.62 270.65 288.03 323.78 333.68 205.42
27 222.19 243.67 230.31 226.89 288.22 276.99 294.78 331.37 341.51 210.23
28 230.46 252.74 238.88 235.34 298.94 287.30 305.75 343.70 354.21 218.06
29 237.25 260.18 245.91 242.26 307.75 295.76 314.75 353.82 364.64 224.47
30 240.64 263.90 249.43 245.73 312.15 299.99 319.25 358.88 369.86 227.68
31 245.73 269.48 254.70 250.93 318.75 306.33 326.00 366.47 377.68 232.50
32 250.82 275.06 259.98 256.12 325.35 312.68 332.76 374.05 385.50 237.31
33 254.00 278.55 263.28 259.37 329.47 316.64 336.97 378.80 390.38 240.32
34 257.39 282.27 266.79 262.83 333.87 320.87 341.48 383.86 395.60 243.53
35 259.08 284.13 268.55 264.56 336.07 322.98 343.73 386.39 398.21 245.14
36 260.78 285.99 270.31 266.30 338.27 325.10 345.98 388.92 400.81 246.74
37 262.48 287.85 272.07 268.03 340.47 327.21 348.23 391.44 403.42 248.35
38 264.17 289.71 273.82 269.76 342.67 329.33 350.48 393.97 406.03 249.95
39 267.57 293.43 277.34 273.22 347.07 333.56 354.98 399.03 411.24 253.16
40 270.96 297.15 280.86 276.69 351.47 337.79 359.48 404.09 416.45 256.37
41 276.05 302.73 286.13 281.88 358.07 344.13 366.23 411.68 424.27 261.18
42 280.92 308.08 291.19 286.86 364.40 350.21 372.70 418.95 431.77 265.80
43 287.71 315.52 298.22 293.79 373.20 358.67 381.70 429.07 442.20 272.22
44 296.19 324.82 307.01 302.45 384.20 369.24 392.95 441.72 455.23 280.24
45 306.15 335.75 317.34 312.63 397.13 381.66 406.17 456.58 470.55 289.67
46 318.03 348.77 329.64 324.75 412.53 396.46 421.92 474.29 488.80 300.90
47 331.38 363.41 343.49 338.39 429.85 413.11 439.64 494.21 509.33 313.54
48 346.65 380.16 359.31 353.98 449.65 432.14 459.89 516.97 532.79 327.99
49 361.70 396.66 374.91 369.35 469.18 450.91 479.87 539.42 555.92 342.23
50 378.66 415.26 392.50 386.67 491.18 472.05 502.37 564.72 581.99 358.28
51 395.41 433.63 409.86 403.77 512.91 492.93 524.59 589.70 607.74 374.12
52 413.86 453.86 428.98 422.61 536.84 515.93 549.06 617.21 636.09 391.58
53 432.51 474.32 448.32 441.66 561.04 539.19 573.81 645.03 664.76 409.23
54 452.66 496.41 469.19 462.23 587.16 564.30 600.54 675.07 695.72 428.29
55 472.80 518.50 490.07 482.80 613.29 589.41 627.26 705.11 726.68 447.34
56 494.64 542.45 512.71 505.10 641.62 616.63 656.23 737.67 760.24 468.01
57 516.69 566.63 535.56 527.61 670.22 644.12 685.48 770.56 794.13 488.87
58 540.22 592.44 559.95 551.65 700.75 673.46 716.70 805.66 830.30 511.14
59 551.88 605.23 572.04 563.55 715.87 687.99 732.18 823.05 848.22 522.17
60 575.41 631.03 596.44 587.58 746.40 717.33 763.40 858.14 884.39 544.44
61 595.77 653.36 617.53 608.37 772.80 742.71 790.40 888.50 915.68 563.69
62 609.13 668.00 631.38 622.01 790.13 759.36 808.12 908.42 936.21 576.33
63 625.87 686.37 648.74 639.11 811.85 780.24 830.34 933.40 961.95 592.18
64+ 636.04 697.52 659.28 649.49 825.04 792.91 843.83 948.56 977.58 601.80
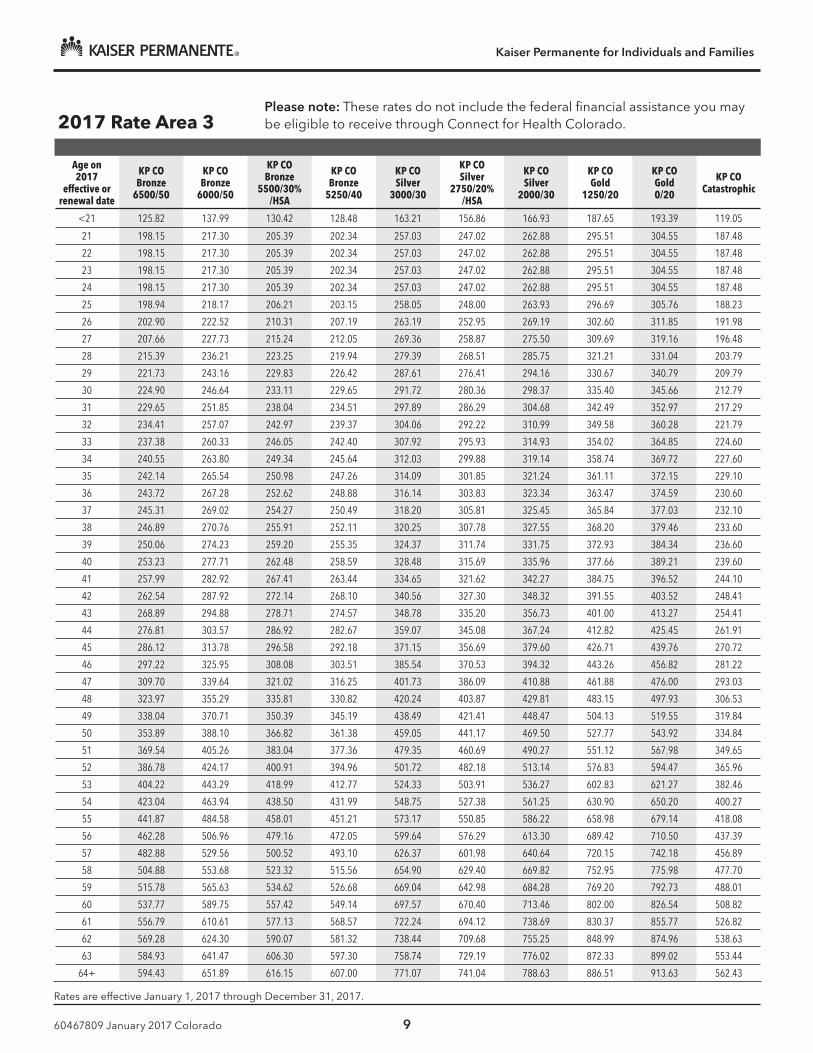
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 9
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 3Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 125.82 137.99 130.42 128.48 163.21 156.86 166.93 187.65 193.39 119.05
21 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
22 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
23 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
24 198.15 217.30 205.39 202.34 257.03 247.02 262.88 295.51 304.55 187.48
25 198.94 218.17 206.21 203.15 258.05 248.00 263.93 296.69 305.76 188.23
26 202.90 222.52 210.31 207.19 263.19 252.95 269.19 302.60 311.85 191.98
27 207.66 227.73 215.24 212.05 269.36 258.87 275.50 309.69 319.16 196.48
28 215.39 236.21 223.25 219.94 279.39 268.51 285.75 321.21 331.04 203.79
29 221.73 243.16 229.83 226.42 287.61 276.41 294.16 330.67 340.79 209.79
30 224.90 246.64 233.11 229.65 291.72 280.36 298.37 335.40 345.66 212.79
31 229.65 251.85 238.04 234.51 297.89 286.29 304.68 342.49 352.97 217.29
32 234.41 257.07 242.97 239.37 304.06 292.22 310.99 349.58 360.28 221.79
33 237.38 260.33 246.05 242.40 307.92 295.93 314.93 354.02 364.85 224.60
34 240.55 263.80 249.34 245.64 312.03 299.88 319.14 358.74 369.72 227.60
35 242.14 265.54 250.98 247.26 314.09 301.85 321.24 361.11 372.15 229.10
36 243.72 267.28 252.62 248.88 316.14 303.83 323.34 363.47 374.59 230.60
37 245.31 269.02 254.27 250.49 318.20 305.81 325.45 365.84 377.03 232.10
38 246.89 270.76 255.91 252.11 320.25 307.78 327.55 368.20 379.46 233.60
39 250.06 274.23 259.20 255.35 324.37 311.74 331.75 372.93 384.34 236.60
40 253.23 277.71 262.48 258.59 328.48 315.69 335.96 377.66 389.21 239.60
41 257.99 282.92 267.41 263.44 334.65 321.62 342.27 384.75 396.52 244.10
42 262.54 287.92 272.14 268.10 340.56 327.30 348.32 391.55 403.52 248.41
43 268.89 294.88 278.71 274.57 348.78 335.20 356.73 401.00 413.27 254.41
44 276.81 303.57 286.92 282.67 359.07 345.08 367.24 412.82 425.45 261.91
45 286.12 313.78 296.58 292.18 371.15 356.69 379.60 426.71 439.76 270.72
46 297.22 325.95 308.08 303.51 385.54 370.53 394.32 443.26 456.82 281.22
47 309.70 339.64 321.02 316.25 401.73 386.09 410.88 461.88 476.00 293.03
48 323.97 355.29 335.81 330.82 420.24 403.87 429.81 483.15 497.93 306.53
49 338.04 370.71 350.39 345.19 438.49 421.41 448.47 504.13 519.55 319.84
50 353.89 388.10 366.82 361.38 459.05 441.17 469.50 527.77 543.92 334.84
51 369.54 405.26 383.04 377.36 479.35 460.69 490.27 551.12 567.98 349.65
52 386.78 424.17 400.91 394.96 501.72 482.18 513.14 576.83 594.47 365.96
53 404.22 443.29 418.99 412.77 524.33 503.91 536.27 602.83 621.27 382.46
54 423.04 463.94 438.50 431.99 548.75 527.38 561.25 630.90 650.20 400.27
55 441.87 484.58 458.01 451.21 573.17 550.85 586.22 658.98 679.14 418.08
56 462.28 506.96 479.16 472.05 599.64 576.29 613.30 689.42 710.50 437.39
57 482.88 529.56 500.52 493.10 626.37 601.98 640.64 720.15 742.18 456.89
58 504.88 553.68 523.32 515.56 654.90 629.40 669.82 752.95 775.98 477.70
59 515.78 565.63 534.62 526.68 669.04 642.98 684.28 769.20 792.73 488.01
60 537.77 589.75 557.42 549.14 697.57 670.40 713.46 802.00 826.54 508.82
61 556.79 610.61 577.13 568.57 722.24 694.12 738.69 830.37 855.77 526.82
62 569.28 624.30 590.07 581.32 738.44 709.68 755.25 848.99 874.96 538.63
63 584.93 641.47 606.30 597.30 758.74 729.19 776.02 872.33 899.02 553.44
64+ 594.43 651.89 616.15 607.00 771.07 741.04 788.63 886.51 913.63 562.43
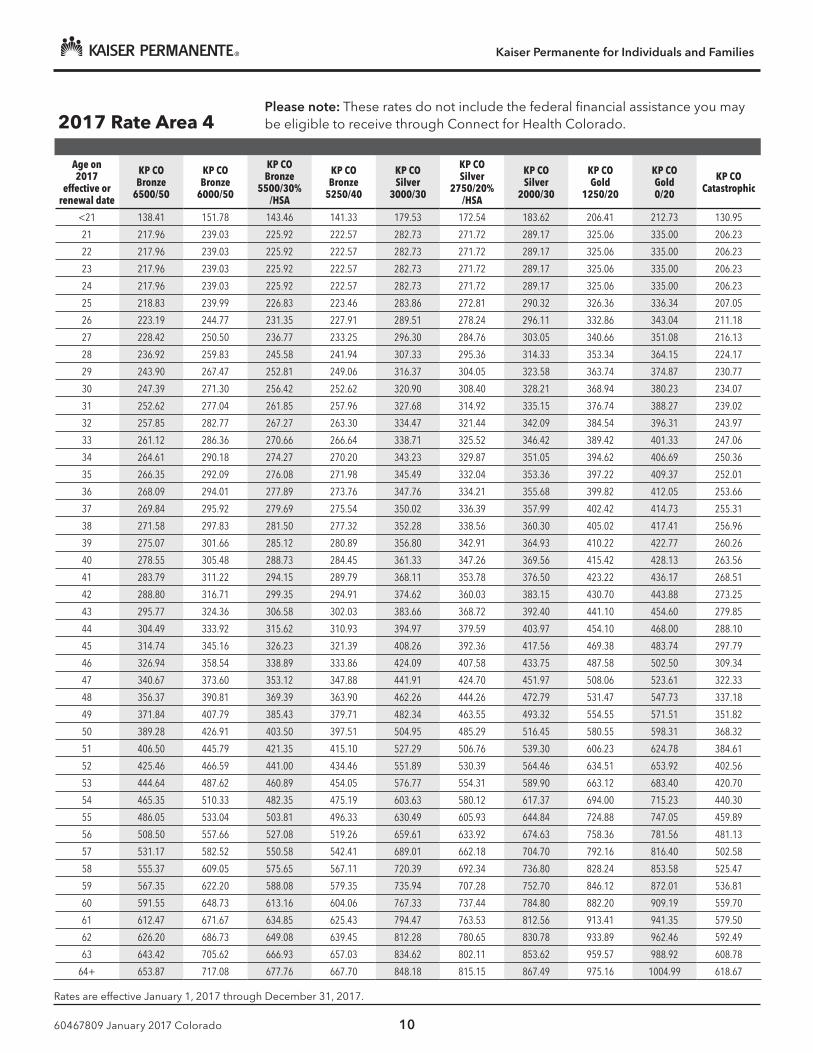
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 10
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 4Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 138.41 151.78 143.46 141.33 179.53 172.54 183.62 206.41 212.73 130.95
21 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
22 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
23 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
24 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
25 218.83 239.99 226.83 223.46 283.86 272.81 290.32 326.36 336.34 207.05
26 223.19 244.77 231.35 227.91 289.51 278.24 296.11 332.86 343.04 211.18
27 228.42 250.50 236.77 233.25 296.30 284.76 303.05 340.66 351.08 216.13
28 236.92 259.83 245.58 241.94 307.33 295.36 314.33 353.34 364.15 224.17
29 243.90 267.47 252.81 249.06 316.37 304.05 323.58 363.74 374.87 230.77
30 247.39 271.30 256.42 252.62 320.90 308.40 328.21 368.94 380.23 234.07
31 252.62 277.04 261.85 257.96 327.68 314.92 335.15 376.74 388.27 239.02
32 257.85 282.77 267.27 263.30 334.47 321.44 342.09 384.54 396.31 243.97
33 261.12 286.36 270.66 266.64 338.71 325.52 346.42 389.42 401.33 247.06
34 264.61 290.18 274.27 270.20 343.23 329.87 351.05 394.62 406.69 250.36
35 266.35 292.09 276.08 271.98 345.49 332.04 353.36 397.22 409.37 252.01
36 268.09 294.01 277.89 273.76 347.76 334.21 355.68 399.82 412.05 253.66
37 269.84 295.92 279.69 275.54 350.02 336.39 357.99 402.42 414.73 255.31
38 271.58 297.83 281.50 277.32 352.28 338.56 360.30 405.02 417.41 256.96
39 275.07 301.66 285.12 280.89 356.80 342.91 364.93 410.22 422.77 260.26
40 278.55 305.48 288.73 284.45 361.33 347.26 369.56 415.42 428.13 263.56
41 283.79 311.22 294.15 289.79 368.11 353.78 376.50 423.22 436.17 268.51
42 288.80 316.71 299.35 294.91 374.62 360.03 383.15 430.70 443.88 273.25
43 295.77 324.36 306.58 302.03 383.66 368.72 392.40 441.10 454.60 279.85
44 304.49 333.92 315.62 310.93 394.97 379.59 403.97 454.10 468.00 288.10
45 314.74 345.16 326.23 321.39 408.26 392.36 417.56 469.38 483.74 297.79
46 326.94 358.54 338.89 333.86 424.09 407.58 433.75 487.58 502.50 309.34
47 340.67 373.60 353.12 347.88 441.91 424.70 451.97 508.06 523.61 322.33
48 356.37 390.81 369.39 363.90 462.26 444.26 472.79 531.47 547.73 337.18
49 371.84 407.79 385.43 379.71 482.34 463.55 493.32 554.55 571.51 351.82
50 389.28 426.91 403.50 397.51 504.95 485.29 516.45 580.55 598.31 368.32
51 406.50 445.79 421.35 415.10 527.29 506.76 539.30 606.23 624.78 384.61
52 425.46 466.59 441.00 434.46 551.89 530.39 564.46 634.51 653.92 402.56
53 444.64 487.62 460.89 454.05 576.77 554.31 589.90 663.12 683.40 420.70
54 465.35 510.33 482.35 475.19 603.63 580.12 617.37 694.00 715.23 440.30
55 486.05 533.04 503.81 496.33 630.49 605.93 644.84 724.88 747.05 459.89
56 508.50 557.66 527.08 519.26 659.61 633.92 674.63 758.36 781.56 481.13
57 531.17 582.52 550.58 542.41 689.01 662.18 704.70 792.16 816.40 502.58
58 555.37 609.05 575.65 567.11 720.39 692.34 736.80 828.24 853.58 525.47
59 567.35 622.20 588.08 579.35 735.94 707.28 752.70 846.12 872.01 536.81
60 591.55 648.73 613.16 604.06 767.33 737.44 784.80 882.20 909.19 559.70
61 612.47 671.67 634.85 625.43 794.47 763.53 812.56 913.41 941.35 579.50
62 626.20 686.73 649.08 639.45 812.28 780.65 830.78 933.89 962.46 592.49
63 643.42 705.62 666.93 657.03 834.62 802.11 853.62 959.57 988.92 608.78
64+ 653.87 717.08 677.76 667.70 848.18 815.15 867.49 975.16 1004.99 618.67
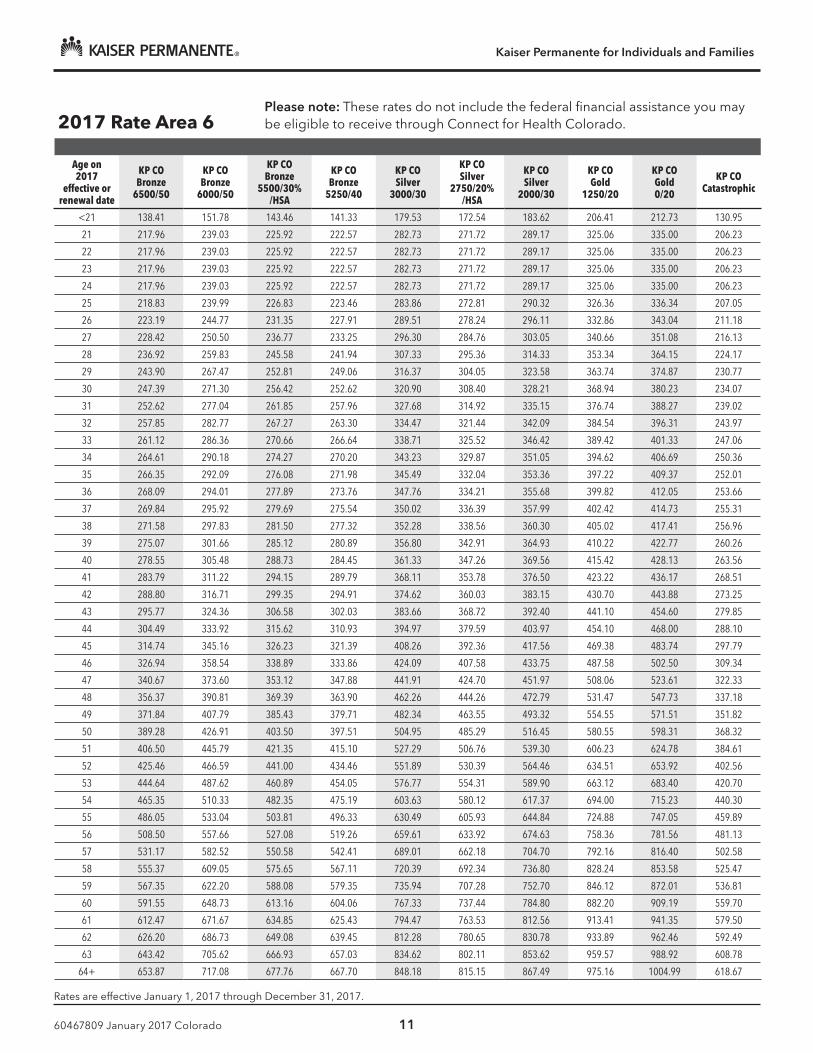
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 11
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 6Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 138.41 151.78 143.46 141.33 179.53 172.54 183.62 206.41 212.73 130.95
21 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
22 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
23 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
24 217.96 239.03 225.92 222.57 282.73 271.72 289.17 325.06 335.00 206.23
25 218.83 239.99 226.83 223.46 283.86 272.81 290.32 326.36 336.34 207.05
26 223.19 244.77 231.35 227.91 289.51 278.24 296.11 332.86 343.04 211.18
27 228.42 250.50 236.77 233.25 296.30 284.76 303.05 340.66 351.08 216.13
28 236.92 259.83 245.58 241.94 307.33 295.36 314.33 353.34 364.15 224.17
29 243.90 267.47 252.81 249.06 316.37 304.05 323.58 363.74 374.87 230.77
30 247.39 271.30 256.42 252.62 320.90 308.40 328.21 368.94 380.23 234.07
31 252.62 277.04 261.85 257.96 327.68 314.92 335.15 376.74 388.27 239.02
32 257.85 282.77 267.27 263.30 334.47 321.44 342.09 384.54 396.31 243.97
33 261.12 286.36 270.66 266.64 338.71 325.52 346.42 389.42 401.33 247.06
34 264.61 290.18 274.27 270.20 343.23 329.87 351.05 394.62 406.69 250.36
35 266.35 292.09 276.08 271.98 345.49 332.04 353.36 397.22 409.37 252.01
36 268.09 294.01 277.89 273.76 347.76 334.21 355.68 399.82 412.05 253.66
37 269.84 295.92 279.69 275.54 350.02 336.39 357.99 402.42 414.73 255.31
38 271.58 297.83 281.50 277.32 352.28 338.56 360.30 405.02 417.41 256.96
39 275.07 301.66 285.12 280.89 356.80 342.91 364.93 410.22 422.77 260.26
40 278.55 305.48 288.73 284.45 361.33 347.26 369.56 415.42 428.13 263.56
41 283.79 311.22 294.15 289.79 368.11 353.78 376.50 423.22 436.17 268.51
42 288.80 316.71 299.35 294.91 374.62 360.03 383.15 430.70 443.88 273.25
43 295.77 324.36 306.58 302.03 383.66 368.72 392.40 441.10 454.60 279.85
44 304.49 333.92 315.62 310.93 394.97 379.59 403.97 454.10 468.00 288.10
45 314.74 345.16 326.23 321.39 408.26 392.36 417.56 469.38 483.74 297.79
46 326.94 358.54 338.89 333.86 424.09 407.58 433.75 487.58 502.50 309.34
47 340.67 373.60 353.12 347.88 441.91 424.70 451.97 508.06 523.61 322.33
48 356.37 390.81 369.39 363.90 462.26 444.26 472.79 531.47 547.73 337.18
49 371.84 407.79 385.43 379.71 482.34 463.55 493.32 554.55 571.51 351.82
50 389.28 426.91 403.50 397.51 504.95 485.29 516.45 580.55 598.31 368.32
51 406.50 445.79 421.35 415.10 527.29 506.76 539.30 606.23 624.78 384.61
52 425.46 466.59 441.00 434.46 551.89 530.39 564.46 634.51 653.92 402.56
53 444.64 487.62 460.89 454.05 576.77 554.31 589.90 663.12 683.40 420.70
54 465.35 510.33 482.35 475.19 603.63 580.12 617.37 694.00 715.23 440.30
55 486.05 533.04 503.81 496.33 630.49 605.93 644.84 724.88 747.05 459.89
56 508.50 557.66 527.08 519.26 659.61 633.92 674.63 758.36 781.56 481.13
57 531.17 582.52 550.58 542.41 689.01 662.18 704.70 792.16 816.40 502.58
58 555.37 609.05 575.65 567.11 720.39 692.34 736.80 828.24 853.58 525.47
59 567.35 622.20 588.08 579.35 735.94 707.28 752.70 846.12 872.01 536.81
60 591.55 648.73 613.16 604.06 767.33 737.44 784.80 882.20 909.19 559.70
61 612.47 671.67 634.85 625.43 794.47 763.53 812.56 913.41 941.35 579.50
62 626.20 686.73 649.08 639.45 812.28 780.65 830.78 933.89 962.46 592.49
63 643.42 705.62 666.93 657.03 834.62 802.11 853.62 959.57 988.92 608.78
64+ 653.87 717.08 677.76 667.70 848.18 815.15 867.49 975.16 1004.99 618.67

Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 12
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 7Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 147.21 161.44 152.59 150.33 190.96 183.52 195.31 219.55 226.26 139.29
21 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
22 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
23 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
24 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
25 232.76 255.26 241.26 237.68 301.92 290.17 308.80 347.12 357.74 220.23
26 237.40 260.34 246.07 242.42 307.94 295.95 314.95 354.04 364.87 224.62
27 242.96 266.44 251.84 248.10 315.16 302.88 322.33 362.34 373.42 229.88
28 252.00 276.36 261.21 257.33 326.88 314.15 334.33 375.82 387.32 238.43
29 259.42 284.50 268.90 264.91 336.51 323.40 344.17 386.89 398.72 245.45
30 263.13 288.56 272.74 268.69 341.32 328.03 349.09 392.42 404.42 248.96
31 268.69 294.67 278.51 274.38 348.54 334.96 356.47 400.71 412.97 254.23
32 274.26 300.77 284.28 280.06 355.75 341.90 363.85 409.01 421.52 259.49
33 277.73 304.58 287.88 283.61 360.26 346.23 368.47 414.20 426.87 262.78
34 281.44 308.65 291.73 287.40 365.08 350.86 373.39 419.73 432.57 266.29
35 283.30 310.68 293.65 289.29 367.48 353.17 375.85 422.50 435.42 268.05
36 285.15 312.72 295.57 291.18 369.89 355.48 378.31 425.26 438.27 269.80
37 287.01 314.75 297.49 293.08 372.29 357.79 380.77 428.03 441.12 271.56
38 288.86 316.78 299.42 294.97 374.70 360.11 383.23 430.79 443.97 273.31
39 292.57 320.85 303.26 298.76 379.51 364.73 388.15 436.33 449.67 276.82
40 296.28 324.92 307.10 302.55 384.32 369.35 393.07 441.86 455.37 280.33
41 301.84 331.02 312.87 308.23 391.54 376.29 400.46 450.16 463.93 285.59
42 307.18 336.87 318.40 313.67 398.46 382.94 407.53 458.11 472.12 290.64
43 314.60 345.01 326.09 321.25 408.08 392.19 417.37 469.17 483.52 297.66
44 323.87 355.17 335.70 330.72 420.11 403.75 429.67 483.00 497.78 306.43
45 334.77 367.12 346.99 341.85 434.24 417.33 444.13 499.25 514.52 316.74
46 347.75 381.36 360.45 355.10 451.08 433.51 461.35 518.61 534.48 329.03
47 362.35 397.38 375.59 370.02 470.03 451.72 480.73 540.39 556.93 342.85
48 379.04 415.68 392.89 387.06 491.68 472.53 502.88 565.29 582.58 358.64
49 395.51 433.74 409.95 403.87 513.03 493.05 524.71 589.84 607.88 374.21
50 414.05 454.07 429.18 422.81 537.09 516.17 549.32 617.49 636.38 391.76
51 432.37 474.16 448.16 441.51 560.84 539.00 573.62 644.81 664.53 409.09
52 452.54 496.28 469.07 462.11 587.01 564.15 600.38 674.89 695.53 428.17
53 472.94 518.65 490.21 482.94 613.47 589.58 627.44 705.31 726.89 447.48
54 494.96 542.80 513.04 505.43 642.04 617.04 656.66 738.16 760.74 468.31
55 516.98 566.96 535.87 527.92 670.61 644.49 685.88 771.00 794.59 489.15
56 540.86 593.14 560.62 552.30 701.58 674.26 717.56 806.62 831.29 511.75
57 564.97 619.59 585.61 576.92 732.86 704.32 749.55 842.57 868.35 534.56
58 590.71 647.81 612.29 603.20 766.24 736.40 783.69 880.95 907.90 558.91
59 603.46 661.79 625.50 616.22 782.78 752.29 800.60 899.97 927.50 570.97
60 629.19 690.01 652.18 642.50 816.16 784.37 834.74 938.34 967.05 595.32
61 651.45 714.42 675.25 665.23 845.03 812.12 864.27 971.53 1001.25 616.38
62 666.05 730.43 690.39 680.14 863.97 830.32 883.65 993.32 1023.70 630.19
63 684.37 750.52 709.37 698.84 887.73 853.16 907.94 1020.63 1051.85 647.52
64+ 695.49 762.71 720.89 710.20 902.15 867.02 922.70 1037.22 1068.94 658.04
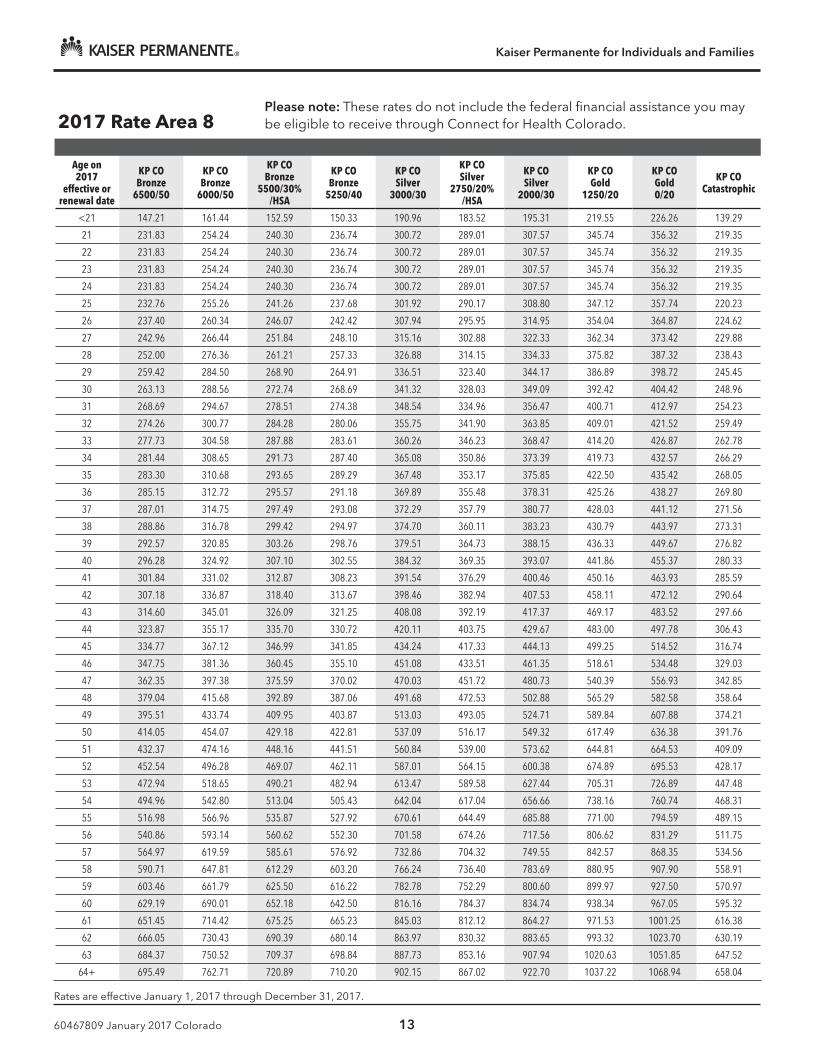
Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 13
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 8Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 147.21 161.44 152.59 150.33 190.96 183.52 195.31 219.55 226.26 139.29
21 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
22 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
23 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
24 231.83 254.24 240.30 236.74 300.72 289.01 307.57 345.74 356.32 219.35
25 232.76 255.26 241.26 237.68 301.92 290.17 308.80 347.12 357.74 220.23
26 237.40 260.34 246.07 242.42 307.94 295.95 314.95 354.04 364.87 224.62
27 242.96 266.44 251.84 248.10 315.16 302.88 322.33 362.34 373.42 229.88
28 252.00 276.36 261.21 257.33 326.88 314.15 334.33 375.82 387.32 238.43
29 259.42 284.50 268.90 264.91 336.51 323.40 344.17 386.89 398.72 245.45
30 263.13 288.56 272.74 268.69 341.32 328.03 349.09 392.42 404.42 248.96
31 268.69 294.67 278.51 274.38 348.54 334.96 356.47 400.71 412.97 254.23
32 274.26 300.77 284.28 280.06 355.75 341.90 363.85 409.01 421.52 259.49
33 277.73 304.58 287.88 283.61 360.26 346.23 368.47 414.20 426.87 262.78
34 281.44 308.65 291.73 287.40 365.08 350.86 373.39 419.73 432.57 266.29
35 283.30 310.68 293.65 289.29 367.48 353.17 375.85 422.50 435.42 268.05
36 285.15 312.72 295.57 291.18 369.89 355.48 378.31 425.26 438.27 269.80
37 287.01 314.75 297.49 293.08 372.29 357.79 380.77 428.03 441.12 271.56
38 288.86 316.78 299.42 294.97 374.70 360.11 383.23 430.79 443.97 273.31
39 292.57 320.85 303.26 298.76 379.51 364.73 388.15 436.33 449.67 276.82
40 296.28 324.92 307.10 302.55 384.32 369.35 393.07 441.86 455.37 280.33
41 301.84 331.02 312.87 308.23 391.54 376.29 400.46 450.16 463.93 285.59
42 307.18 336.87 318.40 313.67 398.46 382.94 407.53 458.11 472.12 290.64
43 314.60 345.01 326.09 321.25 408.08 392.19 417.37 469.17 483.52 297.66
44 323.87 355.17 335.70 330.72 420.11 403.75 429.67 483.00 497.78 306.43
45 334.77 367.12 346.99 341.85 434.24 417.33 444.13 499.25 514.52 316.74
46 347.75 381.36 360.45 355.10 451.08 433.51 461.35 518.61 534.48 329.03
47 362.35 397.38 375.59 370.02 470.03 451.72 480.73 540.39 556.93 342.85
48 379.04 415.68 392.89 387.06 491.68 472.53 502.88 565.29 582.58 358.64
49 395.51 433.74 409.95 403.87 513.03 493.05 524.71 589.84 607.88 374.21
50 414.05 454.07 429.18 422.81 537.09 516.17 549.32 617.49 636.38 391.76
51 432.37 474.16 448.16 441.51 560.84 539.00 573.62 644.81 664.53 409.09
52 452.54 496.28 469.07 462.11 587.01 564.15 600.38 674.89 695.53 428.17
53 472.94 518.65 490.21 482.94 613.47 589.58 627.44 705.31 726.89 447.48
54 494.96 542.80 513.04 505.43 642.04 617.04 656.66 738.16 760.74 468.31
55 516.98 566.96 535.87 527.92 670.61 644.49 685.88 771.00 794.59 489.15
56 540.86 593.14 560.62 552.30 701.58 674.26 717.56 806.62 831.29 511.75
57 564.97 619.59 585.61 576.92 732.86 704.32 749.55 842.57 868.35 534.56
58 590.71 647.81 612.29 603.20 766.24 736.40 783.69 880.95 907.90 558.91
59 603.46 661.79 625.50 616.22 782.78 752.29 800.60 899.97 927.50 570.97
60 629.19 690.01 652.18 642.50 816.16 784.37 834.74 938.34 967.05 595.32
61 651.45 714.42 675.25 665.23 845.03 812.12 864.27 971.53 1001.25 616.38
62 666.05 730.43 690.39 680.14 863.97 830.32 883.65 993.32 1023.70 630.19
63 684.37 750.52 709.37 698.84 887.73 853.16 907.94 1020.63 1051.85 647.52
64+ 695.49 762.71 720.89 710.20 902.15 867.02 922.70 1037.22 1068.94 658.04

Kaiser Permanente for Individuals and Families
60467809 January 2017 Colorado 14
Rates are effective January 1, 2017 through December 31, 2017.
2017 Rate Area 9Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP CO Bronze
6500/50
KP CO Bronze
6000/50
KP CO Bronze
5500/30% /HSA
KP CO Bronze
5250/40
KP CO Silver
3000/30
KP CO Silver
2750/20% /HSA
KP CO Silver
2000/30
KP CO Gold
1250/20
KP CO Gold 0/20
KP CO Catastrophic
<21 163.57 179.38 169.55 167.03 212.18 203.91 217.01 243.94 251.40 154.76
21 257.59 282.49 267.00 263.04 334.13 321.12 341.74 384.16 395.91 243.72
22 257.59 282.49 267.00 263.04 334.13 321.12 341.74 384.16 395.91 243.72
23 257.59 282.49 267.00 263.04 334.13 321.12 341.74 384.16 395.91 243.72
24 257.59 282.49 267.00 263.04 334.13 321.12 341.74 384.16 395.91 243.72
25 258.62 283.62 268.07 264.09 335.47 322.41 343.11 385.69 397.49 244.70
26 263.77 289.27 273.41 269.35 342.15 328.83 349.95 393.38 405.41 249.57
27 269.96 296.05 279.82 275.66 350.17 336.54 358.15 402.60 414.91 255.42
28 280.00 307.07 290.23 285.92 363.20 349.06 371.48 417.58 430.35 264.93
29 288.24 316.11 298.77 294.34 373.90 359.34 382.41 429.87 443.02 272.73
30 292.37 320.63 303.05 298.55 379.24 364.47 387.88 436.02 449.36 276.63
31 298.55 327.41 309.45 304.86 387.26 372.18 396.08 445.24 458.86 282.47
32 304.73 334.19 315.86 311.18 395.28 379.89 404.28 454.46 468.36 288.32
33 308.59 338.42 319.87 315.12 400.29 384.70 409.41 460.22 474.30 291.98
34 312.72 342.94 324.14 319.33 405.64 389.84 414.88 466.37 480.63 295.88
35 314.78 345.20 326.28 321.43 408.31 392.41 417.61 469.44 483.80 297.83
36 316.84 347.46 328.41 323.54 410.99 394.98 420.34 472.51 486.97 299.78
37 318.90 349.72 330.55 325.64 413.66 397.55 423.08 475.59 490.14 301.73
38 320.96 351.98 332.68 327.75 416.33 400.12 425.81 478.66 493.30 303.68
39 325.08 356.50 336.96 331.96 421.68 405.26 431.28 484.81 499.64 307.58
40 329.20 361.02 341.23 336.16 427.02 410.39 436.75 490.95 505.97 311.48
41 335.38 367.80 347.64 342.48 435.04 418.10 444.95 500.17 515.47 317.33
42 341.31 374.30 353.78 348.53 442.73 425.49 452.81 509.01 524.58 322.93
43 349.55 383.34 362.32 356.94 453.42 435.76 463.75 521.30 537.25 330.73
44 359.85 394.64 373.00 367.47 466.79 448.61 477.42 536.67 553.09 340.48
45 371.96 407.92 385.55 379.83 482.49 463.70 493.48 554.72 571.69 351.94
46 386.39 423.73 400.50 394.56 501.20 481.68 512.62 576.24 593.86 365.58
47 402.61 441.53 417.32 411.13 522.25 501.91 534.15 600.44 618.81 380.94
48 421.16 461.87 436.55 430.07 546.31 525.03 558.75 628.10 647.31 398.49
49 439.45 481.93 455.50 448.74 570.03 547.83 583.01 655.37 675.42 415.79
50 460.06 504.53 476.86 469.79 596.76 573.52 610.35 686.11 707.09 435.29
51 480.41 526.84 497.96 490.57 623.16 598.89 637.35 716.45 738.37 454.54
52 502.82 551.42 521.19 513.45 652.23 626.83 667.08 749.88 772.81 475.75
53 525.49 576.28 544.68 536.60 681.63 655.09 697.16 783.68 807.65 497.19
54 549.96 603.12 570.05 561.59 713.38 685.60 729.62 820.18 845.27 520.35
55 574.43 629.95 595.41 586.58 745.12 716.10 762.09 856.67 882.88 543.50
56 600.96 659.05 622.91 613.67 779.54 749.18 797.29 896.24 923.66 568.61
57 627.75 688.43 650.68 641.03 814.29 782.57 832.83 936.19 964.83 593.95
58 656.34 719.78 680.32 670.22 851.37 818.22 870.76 978.83 1008.78 621.01
59 670.51 735.32 695.00 684.69 869.75 835.88 889.56 999.96 1030.55 634.41
60 699.10 766.68 724.64 713.89 906.84 871.52 927.49 1042.60 1074.50 661.46
61 723.83 793.80 750.27 739.14 938.92 902.35 960.30 1079.48 1112.50 684.86
62 740.06 811.59 767.09 755.71 959.97 922.58 981.83 1103.68 1137.45 700.22
63 760.41 833.91 788.19 776.49 986.36 947.95 1008.83 1134.03 1168.72 719.47
64+ 772.76 847.46 800.99 789.11 1002.39 963.36 1025.22 1152.46 1187.72 731.16

Rate chart guide
Kaiser Permanente for Individuals and Families n January 2017
KP Select - Southern Colorado (Colorado Springs and surrounding areas)
To use the Rate Chart Guide, first determine your rate area by finding your ZIP code and county in the chart on page 2. Then locate the page listing your rate area. Your monthly rate will appear in the box where your age and plan intersect.
Rates are determined individually, whether you apply individually or as a family, and are based on the following:
n The plan you select
n Where you live, based on your ZIP code and county
n Your age on the plan’s effective or renewal date
n Whether you use tobacco
If you move and change your home ZIP code and county, your monthly rate may change. If you move to a ZIP code and county that aren’t covered by Kaiser Permanente, your coverage may not continue.
Tobacco use
Rates shown in this guide are for those individuals who don’t use tobacco. Tobacco users 21 and older may pay higher rates than those shown here.
Although family members can enroll in different plans, there are some advantages to enrolling family members in the same plan:
n Children can be covered under your plan until they reach age 26, whether or not they’re in school or living at home.
n If you have more than 3 children under age 21 on the same plan, you’ll only be charged for the 3 oldest. Other children under 21 are covered at no additional cost.
n If you have a child-only account and everyone on the account is under 21, you’ll only be charged for the subscriber (the oldest child on the plan) and the next 3 oldest children under 21.
Health plans include pediatric dental benefits for children 18 and younger.
You may qualify for federal financial assistance
If you qualify for federal financial assistance, these rates will not apply to you. If you’re eligible, the federal government will pay the financial assistance to Kaiser Permanente directly.
2017 Enrollment
60467709 January 2017 Colorado
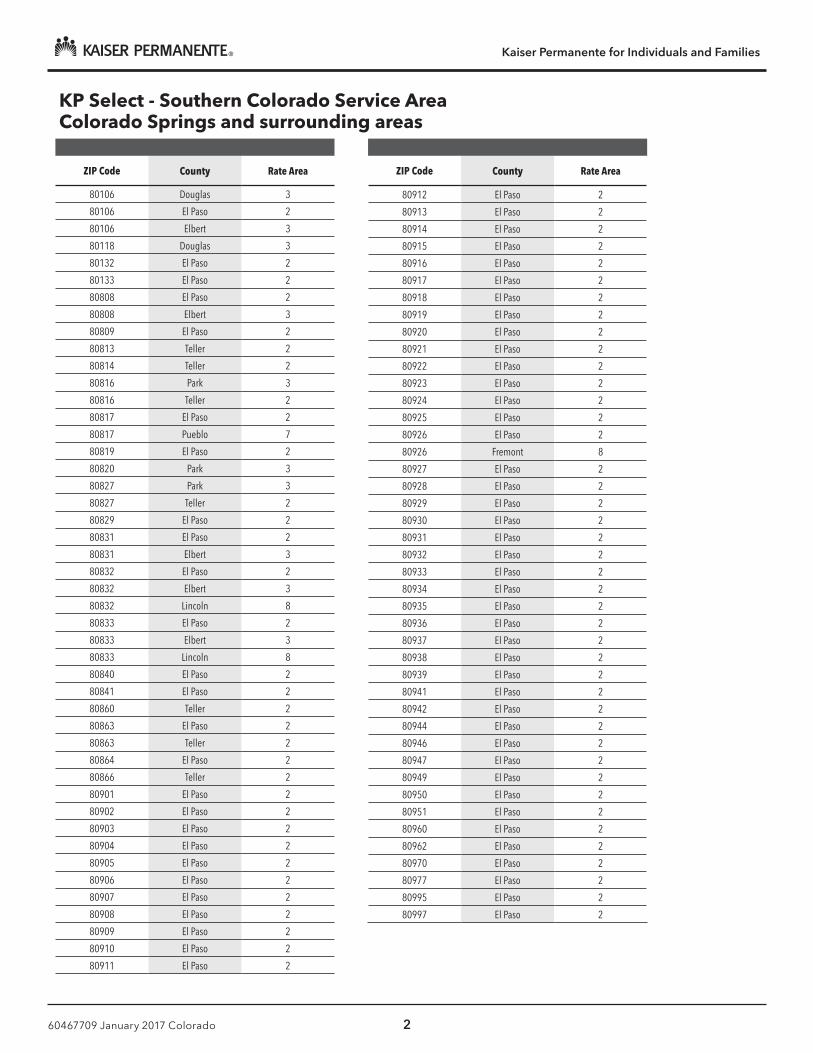
Kaiser Permanente for Individuals and Families
60467709 January 2017 Colorado 2
KP Select - Southern Colorado Service AreaColorado Springs and surrounding areas
ZIP Code County Rate Area
80106 Douglas 3
80106 El Paso 2
80106 Elbert 3
80118 Douglas 3
80132 El Paso 2
80133 El Paso 2
80808 El Paso 2
80808 Elbert 3
80809 El Paso 2
80813 Teller 2
80814 Teller 2
80816 Park 3
80816 Teller 2
80817 El Paso 2
80817 Pueblo 7
80819 El Paso 2
80820 Park 3
80827 Park 3
80827 Teller 2
80829 El Paso 2
80831 El Paso 2
80831 Elbert 3
80832 El Paso 2
80832 Elbert 3
80832 Lincoln 8
80833 El Paso 2
80833 Elbert 3
80833 Lincoln 8
80840 El Paso 2
80841 El Paso 2
80860 Teller 2
80863 El Paso 2
80863 Teller 2
80864 El Paso 2
80866 Teller 2
80901 El Paso 2
80902 El Paso 2
80903 El Paso 2
80904 El Paso 2
80905 El Paso 2
80906 El Paso 2
80907 El Paso 2
80908 El Paso 2
80909 El Paso 2
80910 El Paso 2
80911 El Paso 2
ZIP Code County Rate Area
80912 El Paso 2
80913 El Paso 2
80914 El Paso 2
80915 El Paso 2
80916 El Paso 2
80917 El Paso 2
80918 El Paso 2
80919 El Paso 2
80920 El Paso 2
80921 El Paso 2
80922 El Paso 2
80923 El Paso 2
80924 El Paso 2
80925 El Paso 2
80926 El Paso 2
80926 Fremont 8
80927 El Paso 2
80928 El Paso 2
80929 El Paso 2
80930 El Paso 2
80931 El Paso 2
80932 El Paso 2
80933 El Paso 2
80934 El Paso 2
80935 El Paso 2
80936 El Paso 2
80937 El Paso 2
80938 El Paso 2
80939 El Paso 2
80941 El Paso 2
80942 El Paso 2
80944 El Paso 2
80946 El Paso 2
80947 El Paso 2
80949 El Paso 2
80950 El Paso 2
80951 El Paso 2
80960 El Paso 2
80962 El Paso 2
80970 El Paso 2
80977 El Paso 2
80995 El Paso 2
80997 El Paso 2
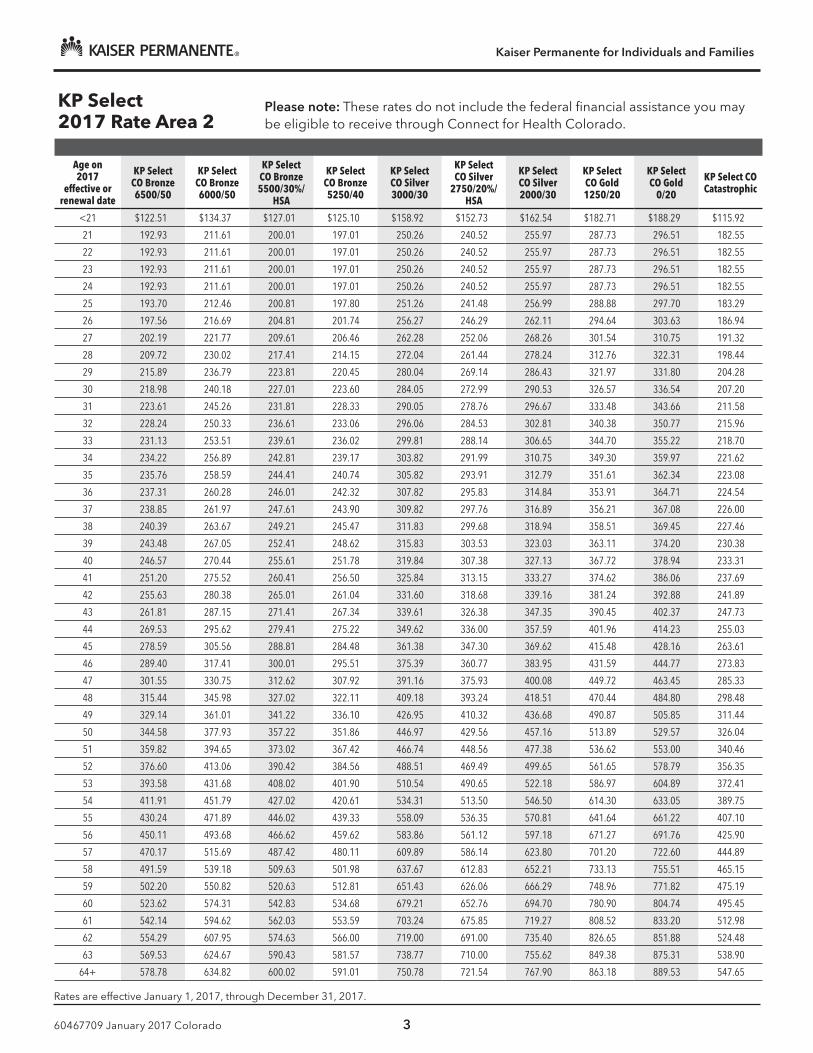
Kaiser Permanente for Individuals and Families
60467709 January 2017 Colorado 3
KP Select2017 Rate Area 2
Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP Select CO Bronze 6500/50
KP Select CO Bronze 6000/50
KP Select CO Bronze 5500/30%/
HSA
KP Select CO Bronze 5250/40
KP Select CO Silver 3000/30
KP Select CO Silver
2750/20%/HSA
KP Select CO Silver 2000/30
KP Select CO Gold 1250/20
KP Select CO Gold
0/20
KP Select CO Catastrophic
<21 $122.51 $134.37 $127.01 $125.10 $158.92 $152.73 $162.54 $182.71 $188.29 $115.92
21 192.93 211.61 200.01 197.01 250.26 240.52 255.97 287.73 296.51 182.55
22 192.93 211.61 200.01 197.01 250.26 240.52 255.97 287.73 296.51 182.55
23 192.93 211.61 200.01 197.01 250.26 240.52 255.97 287.73 296.51 182.55
24 192.93 211.61 200.01 197.01 250.26 240.52 255.97 287.73 296.51 182.55
25 193.70 212.46 200.81 197.80 251.26 241.48 256.99 288.88 297.70 183.29
26 197.56 216.69 204.81 201.74 256.27 246.29 262.11 294.64 303.63 186.94
27 202.19 221.77 209.61 206.46 262.28 252.06 268.26 301.54 310.75 191.32
28 209.72 230.02 217.41 214.15 272.04 261.44 278.24 312.76 322.31 198.44
29 215.89 236.79 223.81 220.45 280.04 269.14 286.43 321.97 331.80 204.28
30 218.98 240.18 227.01 223.60 284.05 272.99 290.53 326.57 336.54 207.20
31 223.61 245.26 231.81 228.33 290.05 278.76 296.67 333.48 343.66 211.58
32 228.24 250.33 236.61 233.06 296.06 284.53 302.81 340.38 350.77 215.96
33 231.13 253.51 239.61 236.02 299.81 288.14 306.65 344.70 355.22 218.70
34 234.22 256.89 242.81 239.17 303.82 291.99 310.75 349.30 359.97 221.62
35 235.76 258.59 244.41 240.74 305.82 293.91 312.79 351.61 362.34 223.08
36 237.31 260.28 246.01 242.32 307.82 295.83 314.84 353.91 364.71 224.54
37 238.85 261.97 247.61 243.90 309.82 297.76 316.89 356.21 367.08 226.00
38 240.39 263.67 249.21 245.47 311.83 299.68 318.94 358.51 369.45 227.46
39 243.48 267.05 252.41 248.62 315.83 303.53 323.03 363.11 374.20 230.38
40 246.57 270.44 255.61 251.78 319.84 307.38 327.13 367.72 378.94 233.31
41 251.20 275.52 260.41 256.50 325.84 313.15 333.27 374.62 386.06 237.69
42 255.63 280.38 265.01 261.04 331.60 318.68 339.16 381.24 392.88 241.89
43 261.81 287.15 271.41 267.34 339.61 326.38 347.35 390.45 402.37 247.73
44 269.53 295.62 279.41 275.22 349.62 336.00 357.59 401.96 414.23 255.03
45 278.59 305.56 288.81 284.48 361.38 347.30 369.62 415.48 428.16 263.61
46 289.40 317.41 300.01 295.51 375.39 360.77 383.95 431.59 444.77 273.83
47 301.55 330.75 312.62 307.92 391.16 375.93 400.08 449.72 463.45 285.33
48 315.44 345.98 327.02 322.11 409.18 393.24 418.51 470.44 484.80 298.48
49 329.14 361.01 341.22 336.10 426.95 410.32 436.68 490.87 505.85 311.44
50 344.58 377.93 357.22 351.86 446.97 429.56 457.16 513.89 529.57 326.04
51 359.82 394.65 373.02 367.42 466.74 448.56 477.38 536.62 553.00 340.46
52 376.60 413.06 390.42 384.56 488.51 469.49 499.65 561.65 578.79 356.35
53 393.58 431.68 408.02 401.90 510.54 490.65 522.18 586.97 604.89 372.41
54 411.91 451.79 427.02 420.61 534.31 513.50 546.50 614.30 633.05 389.75
55 430.24 471.89 446.02 439.33 558.09 536.35 570.81 641.64 661.22 407.10
56 450.11 493.68 466.62 459.62 583.86 561.12 597.18 671.27 691.76 425.90
57 470.17 515.69 487.42 480.11 609.89 586.14 623.80 701.20 722.60 444.89
58 491.59 539.18 509.63 501.98 637.67 612.83 652.21 733.13 755.51 465.15
59 502.20 550.82 520.63 512.81 651.43 626.06 666.29 748.96 771.82 475.19
60 523.62 574.31 542.83 534.68 679.21 652.76 694.70 780.90 804.74 495.45
61 542.14 594.62 562.03 553.59 703.24 675.85 719.27 808.52 833.20 512.98
62 554.29 607.95 574.63 566.00 719.00 691.00 735.40 826.65 851.88 524.48
63 569.53 624.67 590.43 581.57 738.77 710.00 755.62 849.38 875.31 538.90
64+ 578.78 634.82 600.02 591.01 750.78 721.54 767.90 863.18 889.53 547.65
Rates are effective January 1, 2017, through December 31, 2017.
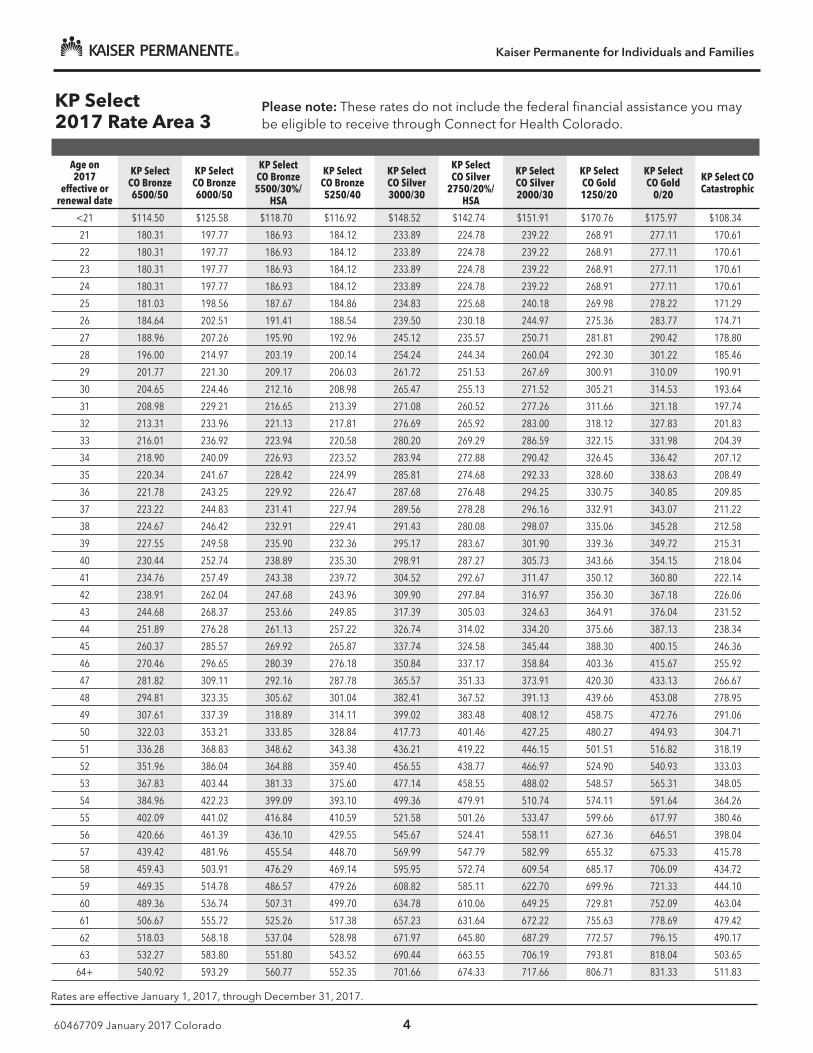
Kaiser Permanente for Individuals and Families
60467709 January 2017 Colorado 4
KP Select2017 Rate Area 3
Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP Select CO Bronze 6500/50
KP Select CO Bronze 6000/50
KP Select CO Bronze 5500/30%/
HSA
KP Select CO Bronze 5250/40
KP Select CO Silver 3000/30
KP Select CO Silver
2750/20%/HSA
KP Select CO Silver 2000/30
KP Select CO Gold 1250/20
KP Select CO Gold
0/20
KP Select CO Catastrophic
<21 $114.50 $125.58 $118.70 $116.92 $148.52 $142.74 $151.91 $170.76 $175.97 $108.34
21 180.31 197.77 186.93 184.12 233.89 224.78 239.22 268.91 277.11 170.61
22 180.31 197.77 186.93 184.12 233.89 224.78 239.22 268.91 277.11 170.61
23 180.31 197.77 186.93 184.12 233.89 224.78 239.22 268.91 277.11 170.61
24 180.31 197.77 186.93 184.12 233.89 224.78 239.22 268.91 277.11 170.61
25 181.03 198.56 187.67 184.86 234.83 225.68 240.18 269.98 278.22 171.29
26 184.64 202.51 191.41 188.54 239.50 230.18 244.97 275.36 283.77 174.71
27 188.96 207.26 195.90 192.96 245.12 235.57 250.71 281.81 290.42 178.80
28 196.00 214.97 203.19 200.14 254.24 244.34 260.04 292.30 301.22 185.46
29 201.77 221.30 209.17 206.03 261.72 251.53 267.69 300.91 310.09 190.91
30 204.65 224.46 212.16 208.98 265.47 255.13 271.52 305.21 314.53 193.64
31 208.98 229.21 216.65 213.39 271.08 260.52 277.26 311.66 321.18 197.74
32 213.31 233.96 221.13 217.81 276.69 265.92 283.00 318.12 327.83 201.83
33 216.01 236.92 223.94 220.58 280.20 269.29 286.59 322.15 331.98 204.39
34 218.90 240.09 226.93 223.52 283.94 272.88 290.42 326.45 336.42 207.12
35 220.34 241.67 228.42 224.99 285.81 274.68 292.33 328.60 338.63 208.49
36 221.78 243.25 229.92 226.47 287.68 276.48 294.25 330.75 340.85 209.85
37 223.22 244.83 231.41 227.94 289.56 278.28 296.16 332.91 343.07 211.22
38 224.67 246.42 232.91 229.41 291.43 280.08 298.07 335.06 345.28 212.58
39 227.55 249.58 235.90 232.36 295.17 283.67 301.90 339.36 349.72 215.31
40 230.44 252.74 238.89 235.30 298.91 287.27 305.73 343.66 354.15 218.04
41 234.76 257.49 243.38 239.72 304.52 292.67 311.47 350.12 360.80 222.14
42 238.91 262.04 247.68 243.96 309.90 297.84 316.97 356.30 367.18 226.06
43 244.68 268.37 253.66 249.85 317.39 305.03 324.63 364.91 376.04 231.52
44 251.89 276.28 261.13 257.22 326.74 314.02 334.20 375.66 387.13 238.34
45 260.37 285.57 269.92 265.87 337.74 324.58 345.44 388.30 400.15 246.36
46 270.46 296.65 280.39 276.18 350.84 337.17 358.84 403.36 415.67 255.92
47 281.82 309.11 292.16 287.78 365.57 351.33 373.91 420.30 433.13 266.67
48 294.81 323.35 305.62 301.04 382.41 367.52 391.13 439.66 453.08 278.95
49 307.61 337.39 318.89 314.11 399.02 383.48 408.12 458.75 472.76 291.06
50 322.03 353.21 333.85 328.84 417.73 401.46 427.25 480.27 494.93 304.71
51 336.28 368.83 348.62 343.38 436.21 419.22 446.15 501.51 516.82 318.19
52 351.96 386.04 364.88 359.40 456.55 438.77 466.97 524.90 540.93 333.03
53 367.83 403.44 381.33 375.60 477.14 458.55 488.02 548.57 565.31 348.05
54 384.96 422.23 399.09 393.10 499.36 479.91 510.74 574.11 591.64 364.26
55 402.09 441.02 416.84 410.59 521.58 501.26 533.47 599.66 617.97 380.46
56 420.66 461.39 436.10 429.55 545.67 524.41 558.11 627.36 646.51 398.04
57 439.42 481.96 455.54 448.70 569.99 547.79 582.99 655.32 675.33 415.78
58 459.43 503.91 476.29 469.14 595.95 572.74 609.54 685.17 706.09 434.72
59 469.35 514.78 486.57 479.26 608.82 585.11 622.70 699.96 721.33 444.10
60 489.36 536.74 507.31 499.70 634.78 610.06 649.25 729.81 752.09 463.04
61 506.67 555.72 525.26 517.38 657.23 631.64 672.22 755.63 778.69 479.42
62 518.03 568.18 537.04 528.98 671.97 645.80 687.29 772.57 796.15 490.17
63 532.27 583.80 551.80 543.52 690.44 663.55 706.19 793.81 818.04 503.65
64+ 540.92 593.29 560.77 552.35 701.66 674.33 717.66 806.71 831.33 511.83
Rates are effective January 1, 2017, through December 31, 2017.
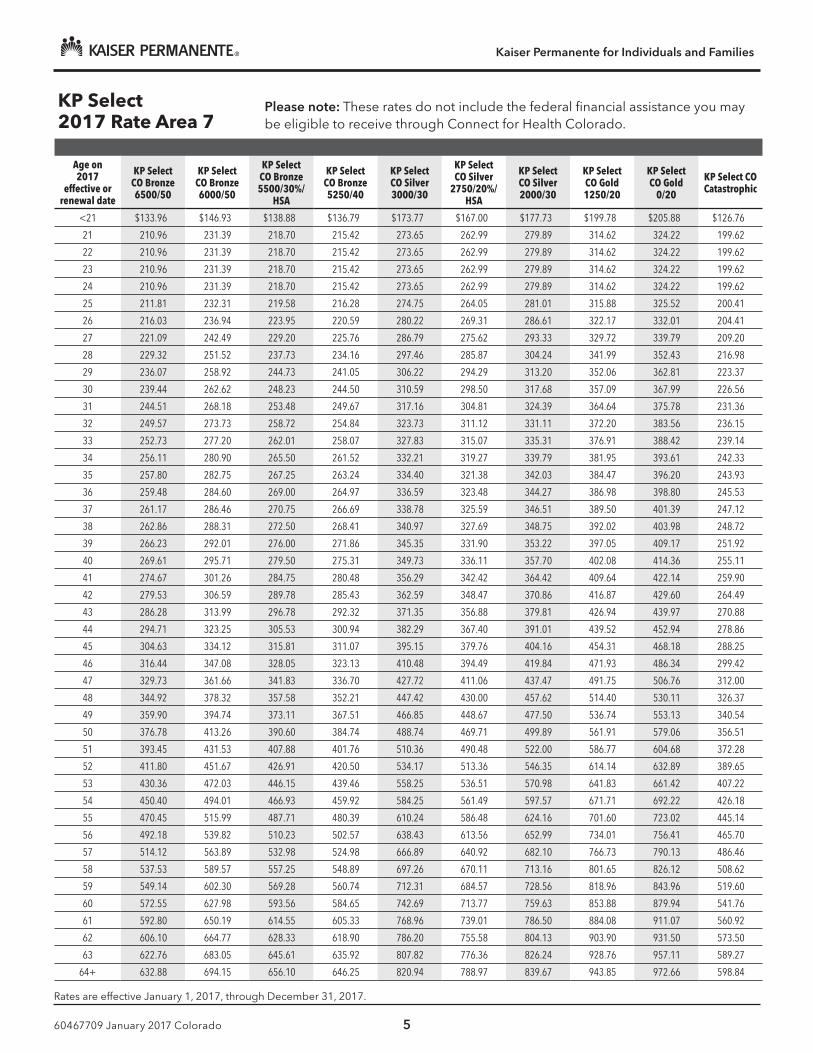
Kaiser Permanente for Individuals and Families
60467709 January 2017 Colorado 5
KP Select2017 Rate Area 7
Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP Select CO Bronze 6500/50
KP Select CO Bronze 6000/50
KP Select CO Bronze 5500/30%/
HSA
KP Select CO Bronze 5250/40
KP Select CO Silver 3000/30
KP Select CO Silver
2750/20%/HSA
KP Select CO Silver 2000/30
KP Select CO Gold 1250/20
KP Select CO Gold
0/20
KP Select CO Catastrophic
<21 $133.96 $146.93 $138.88 $136.79 $173.77 $167.00 $177.73 $199.78 $205.88 $126.76
21 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
22 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
23 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
24 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
25 211.81 232.31 219.58 216.28 274.75 264.05 281.01 315.88 325.52 200.41
26 216.03 236.94 223.95 220.59 280.22 269.31 286.61 322.17 332.01 204.41
27 221.09 242.49 229.20 225.76 286.79 275.62 293.33 329.72 339.79 209.20
28 229.32 251.52 237.73 234.16 297.46 285.87 304.24 341.99 352.43 216.98
29 236.07 258.92 244.73 241.05 306.22 294.29 313.20 352.06 362.81 223.37
30 239.44 262.62 248.23 244.50 310.59 298.50 317.68 357.09 367.99 226.56
31 244.51 268.18 253.48 249.67 317.16 304.81 324.39 364.64 375.78 231.36
32 249.57 273.73 258.72 254.84 323.73 311.12 331.11 372.20 383.56 236.15
33 252.73 277.20 262.01 258.07 327.83 315.07 335.31 376.91 388.42 239.14
34 256.11 280.90 265.50 261.52 332.21 319.27 339.79 381.95 393.61 242.33
35 257.80 282.75 267.25 263.24 334.40 321.38 342.03 384.47 396.20 243.93
36 259.48 284.60 269.00 264.97 336.59 323.48 344.27 386.98 398.80 245.53
37 261.17 286.46 270.75 266.69 338.78 325.59 346.51 389.50 401.39 247.12
38 262.86 288.31 272.50 268.41 340.97 327.69 348.75 392.02 403.98 248.72
39 266.23 292.01 276.00 271.86 345.35 331.90 353.22 397.05 409.17 251.92
40 269.61 295.71 279.50 275.31 349.73 336.11 357.70 402.08 414.36 255.11
41 274.67 301.26 284.75 280.48 356.29 342.42 364.42 409.64 422.14 259.90
42 279.53 306.59 289.78 285.43 362.59 348.47 370.86 416.87 429.60 264.49
43 286.28 313.99 296.78 292.32 371.35 356.88 379.81 426.94 439.97 270.88
44 294.71 323.25 305.53 300.94 382.29 367.40 391.01 439.52 452.94 278.86
45 304.63 334.12 315.81 311.07 395.15 379.76 404.16 454.31 468.18 288.25
46 316.44 347.08 328.05 323.13 410.48 394.49 419.84 471.93 486.34 299.42
47 329.73 361.66 341.83 336.70 427.72 411.06 437.47 491.75 506.76 312.00
48 344.92 378.32 357.58 352.21 447.42 430.00 457.62 514.40 530.11 326.37
49 359.90 394.74 373.11 367.51 466.85 448.67 477.50 536.74 553.13 340.54
50 376.78 413.26 390.60 384.74 488.74 469.71 499.89 561.91 579.06 356.51
51 393.45 431.53 407.88 401.76 510.36 490.48 522.00 586.77 604.68 372.28
52 411.80 451.67 426.91 420.50 534.17 513.36 546.35 614.14 632.89 389.65
53 430.36 472.03 446.15 439.46 558.25 536.51 570.98 641.83 661.42 407.22
54 450.40 494.01 466.93 459.92 584.25 561.49 597.57 671.71 692.22 426.18
55 470.45 515.99 487.71 480.39 610.24 586.48 624.16 701.60 723.02 445.14
56 492.18 539.82 510.23 502.57 638.43 613.56 652.99 734.01 756.41 465.70
57 514.12 563.89 532.98 524.98 666.89 640.92 682.10 766.73 790.13 486.46
58 537.53 589.57 557.25 548.89 697.26 670.11 713.16 801.65 826.12 508.62
59 549.14 602.30 569.28 560.74 712.31 684.57 728.56 818.96 843.96 519.60
60 572.55 627.98 593.56 584.65 742.69 713.77 759.63 853.88 879.94 541.76
61 592.80 650.19 614.55 605.33 768.96 739.01 786.50 884.08 911.07 560.92
62 606.10 664.77 628.33 618.90 786.20 755.58 804.13 903.90 931.50 573.50
63 622.76 683.05 645.61 635.92 807.82 776.36 826.24 928.76 957.11 589.27
64+ 632.88 694.15 656.10 646.25 820.94 788.97 839.67 943.85 972.66 598.84
Rates are effective January 1, 2017, through December 31, 2017.
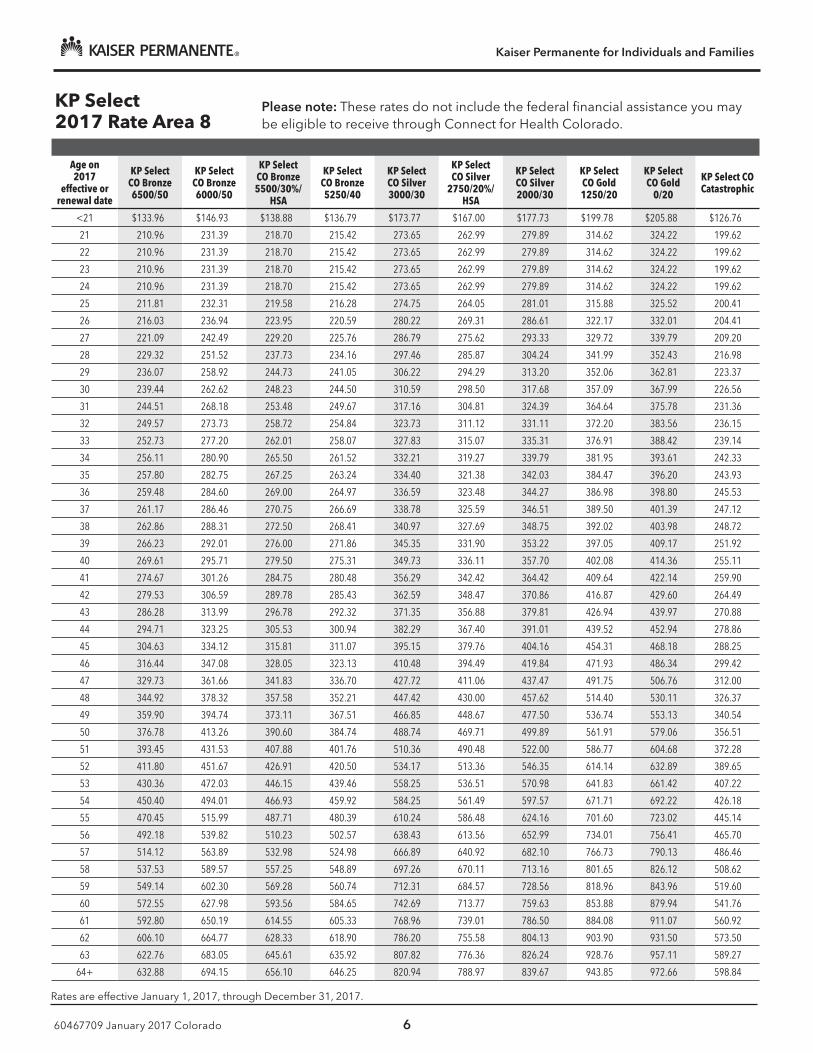
Kaiser Permanente for Individuals and Families
60467709 January 2017 Colorado 6
KP Select2017 Rate Area 8
Please note: These rates do not include the federal financial assistance you may be eligible to receive through Connect for Health Colorado.
Age on 2017
effective or renewal date
KP Select CO Bronze 6500/50
KP Select CO Bronze 6000/50
KP Select CO Bronze 5500/30%/
HSA
KP Select CO Bronze 5250/40
KP Select CO Silver 3000/30
KP Select CO Silver
2750/20%/HSA
KP Select CO Silver 2000/30
KP Select CO Gold 1250/20
KP Select CO Gold
0/20
KP Select CO Catastrophic
<21 $133.96 $146.93 $138.88 $136.79 $173.77 $167.00 $177.73 $199.78 $205.88 $126.76
21 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
22 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
23 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
24 210.96 231.39 218.70 215.42 273.65 262.99 279.89 314.62 324.22 199.62
25 211.81 232.31 219.58 216.28 274.75 264.05 281.01 315.88 325.52 200.41
26 216.03 236.94 223.95 220.59 280.22 269.31 286.61 322.17 332.01 204.41
27 221.09 242.49 229.20 225.76 286.79 275.62 293.33 329.72 339.79 209.20
28 229.32 251.52 237.73 234.16 297.46 285.87 304.24 341.99 352.43 216.98
29 236.07 258.92 244.73 241.05 306.22 294.29 313.20 352.06 362.81 223.37
30 239.44 262.62 248.23 244.50 310.59 298.50 317.68 357.09 367.99 226.56
31 244.51 268.18 253.48 249.67 317.16 304.81 324.39 364.64 375.78 231.36
32 249.57 273.73 258.72 254.84 323.73 311.12 331.11 372.20 383.56 236.15
33 252.73 277.20 262.01 258.07 327.83 315.07 335.31 376.91 388.42 239.14
34 256.11 280.90 265.50 261.52 332.21 319.27 339.79 381.95 393.61 242.33
35 257.80 282.75 267.25 263.24 334.40 321.38 342.03 384.47 396.20 243.93
36 259.48 284.60 269.00 264.97 336.59 323.48 344.27 386.98 398.80 245.53
37 261.17 286.46 270.75 266.69 338.78 325.59 346.51 389.50 401.39 247.12
38 262.86 288.31 272.50 268.41 340.97 327.69 348.75 392.02 403.98 248.72
39 266.23 292.01 276.00 271.86 345.35 331.90 353.22 397.05 409.17 251.92
40 269.61 295.71 279.50 275.31 349.73 336.11 357.70 402.08 414.36 255.11
41 274.67 301.26 284.75 280.48 356.29 342.42 364.42 409.64 422.14 259.90
42 279.53 306.59 289.78 285.43 362.59 348.47 370.86 416.87 429.60 264.49
43 286.28 313.99 296.78 292.32 371.35 356.88 379.81 426.94 439.97 270.88
44 294.71 323.25 305.53 300.94 382.29 367.40 391.01 439.52 452.94 278.86
45 304.63 334.12 315.81 311.07 395.15 379.76 404.16 454.31 468.18 288.25
46 316.44 347.08 328.05 323.13 410.48 394.49 419.84 471.93 486.34 299.42
47 329.73 361.66 341.83 336.70 427.72 411.06 437.47 491.75 506.76 312.00
48 344.92 378.32 357.58 352.21 447.42 430.00 457.62 514.40 530.11 326.37
49 359.90 394.74 373.11 367.51 466.85 448.67 477.50 536.74 553.13 340.54
50 376.78 413.26 390.60 384.74 488.74 469.71 499.89 561.91 579.06 356.51
51 393.45 431.53 407.88 401.76 510.36 490.48 522.00 586.77 604.68 372.28
52 411.80 451.67 426.91 420.50 534.17 513.36 546.35 614.14 632.89 389.65
53 430.36 472.03 446.15 439.46 558.25 536.51 570.98 641.83 661.42 407.22
54 450.40 494.01 466.93 459.92 584.25 561.49 597.57 671.71 692.22 426.18
55 470.45 515.99 487.71 480.39 610.24 586.48 624.16 701.60 723.02 445.14
56 492.18 539.82 510.23 502.57 638.43 613.56 652.99 734.01 756.41 465.70
57 514.12 563.89 532.98 524.98 666.89 640.92 682.10 766.73 790.13 486.46
58 537.53 589.57 557.25 548.89 697.26 670.11 713.16 801.65 826.12 508.62
59 549.14 602.30 569.28 560.74 712.31 684.57 728.56 818.96 843.96 519.60
60 572.55 627.98 593.56 584.65 742.69 713.77 759.63 853.88 879.94 541.76
61 592.80 650.19 614.55 605.33 768.96 739.01 786.50 884.08 911.07 560.92
62 606.10 664.77 628.33 618.90 786.20 755.58 804.13 903.90 931.50 573.50
63 622.76 683.05 645.61 635.92 807.82 776.36 826.24 928.76 957.11 589.27
64+ 632.88 694.15 656.10 646.25 820.94 788.97 839.67 943.85 972.66 598.84
Rates are effective January 1, 2017, through December 31, 2017.





























