Embed Size (px)
Citation preview

“All-In-One” Imaging Protocols for the Evaluation ofPotential Living Liver Donors: Comparison of Magnetic
Resonance Imaging and Multidetector ComputedTomography
Tobias Schroeder,1 Massimo Malago,2 Jorg F. Debatin,3 Mathias Goyen,3
Silvio Nadalin,2 and Stefan G. Ruehm4
In order to compare the performance of “all-in-one” mag-netic resonance imaging (MRI) and “all-in-one” multide-tector computed tomography (MDCT) in the preharvestevaluation 25 potential living donors underwent bothMRI and MDCT. MRI was performed on a high-perfor-mance 1.5-T scanner, computed tomography (CT) on a4-row multidetector-scanner. Both scan protocolsincluded angiography of the arterial and venous hepaticsystems. CT additionally included infusion of a biliarycontrast agent. Data analysis was performed by 4 review-ers, based on source images, multiplanar reformats, andthree-dimensional (3D) postprocessing. Determination ofimage quality was based on a 4-point image quality rating(IQR) scale, ranging from 1 � nondiagnostic to 4 �excellent. Preoperative and intraoperative (n � 13) find-ings were correlated. Magnetic resonance (MR) examina-tions were generally well tolerated. Within the CT scan, 2candidates presented moderate adverse reaction to thebiliary contrast agent. MRI and CT showed the samebenign parenchymal lesions (IQR MR: 3.7; IQR CT: 3.4).Determination of liver volumes was easier based on CT(IQR MR: 3.3; IQR CT: 3.6). Magnetic resonance angiog-
raphy (MRA) revealed 10 variants of the arterial liversupply (IQR: 3.0) and computed tomographic angiogra-phy (CTA) revealed 13 variants (IQR: 3.5). Magnetic res-onance cholangiopancreatography (MRCP) identified 4biliary variants (IQR: 1.3) and CT cholangiography iden-tified 17 (IQR: 3.5). MRI and CT each showed 4 hepaticand portal venous variants (IQR MR: 3.4, CT: 2.8). CTand MR findings correlated well with intraoperative find-ings. In conclusion, both techniques proved to be efficientto evaluate potential living liver donors’ anatomy in asingle diagnostic step. The main advantage of CT lies inthe ability to accurately assess the biliary anatomy. (LiverTranspl 2005;11:776-787.)
Living donor liver transplantation has evolved into awidely accepted therapeutic option to alleviate the
persistent shortage of cadaveric liver transplants.1-3 Thisinnovative procedure allows healthy adults to donate aportion of their liver to compatible recipients sufferingfrom end-stage liver disease.4-7
Besides of augmenting the transplant organ pool,living donor liver transplantation involves the advan-tage of performing an elective operation, access to agraft in best condition, and lowering the likelihood ofrecipient death while waiting for a suitable organ.8 Incombination with improved surgical technique andhighly developed immunosuppression,9 this results inrecipient survival rates as good as those obtained afterconventional liver transplantation with full-sizeddeceased donor organs.10
The critical issue of this procedure is the risk to thedonors, who were healthy until the transplantation; thisrisk is now estimated to be 0.5% mortality and 21%postoperative morbidity.1,11,12 To reduce such risk to aminimum, and also to avoid donor-recipient mismatch,the potential donors have to undergo an extensive step-wise evaluation process before being admitted to dona-tion. Special attention is hereby paid to the determina-tion of the liver volumes13-17 and the recognition ofvascular anomalies.18-20 In fact, a majority of the candi-dates is eliminated mostly due to unfavorable hepaticparenchymal, biliary, or vascular morphology.
In the recent past, this preharvest assessment
Abbreviations: MR, magnetic resonance; MRI, magnetic reso-nance imaging; CT, computed tomography; MDCT, multidetectorcomputed tomography; 3D, 3-dimensional; IQR, image quality rat-ing; MRA, magnetic resonance angiography; CTA, computed tomo-graphic angiography; MRCP, magnetic resonance cholangiopancre-atography; 2D, 2-dimensional; TR, time of repetition; TE, time ofecho; T1, spin-lattice relaxation time; FLASH, fast low angle shot;True FISP, true fast imaging with steady-state precession; RARE,rapid acquisition with relaxation enhancement; T2, spin-spin relax-ation time; Gd-BOPTA, gadolinium-BOPTA-gadobenate dimeglu-mine; HASTE, half-Fourier single shot turbo spin echo.
From the 1Department of Diagnostic and Interventional Radiology,and 2Department of General Surgery and Transplantation, UniversityHospital Essen, Germany; 3University Hospital Eppendorf, Hamburg,Germany; and 4Department of Radiology, David Geffen School of Med-icine at University of California Los Angeles, Los Angeles, CA.
Supported in part by the German Research Society, Bonn, Germany(KFO 117/1-1;A2.2).
Address reprint requests to Tobias Schroeder, MD, Department ofDiagnostic and Interventional Radiology, University Hospital Essen,Hufelandstrasse 55, D-45122 Essen, Germany. Telephone: 49 201 7231506; FAX: 49 201 723 1548; E-mail: [email protected]
Copyright © 2005 by the American Association for the Study ofLiver Diseases
Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/lt.20429
776 Liver Transplantation, Vol 11, No 7 ( July), 2005: pp 776-787

employed a multimodal radiologic evaluation protocol,including computed tomography (CT) or magnetic res-onance imaging (MRI) for liver planimetry and exclu-sion of parenchymal lesions, catheter digital subtractionangiography for the display of the hepatic vascular sys-tem, endoscopic retrograde cholangiopancreatographyfor assessing the biliary anatomy and liver biopsy for theassessment of hepatic-cellular infiltration.21,22
In an attempt to simplify and shorten such a timeconsuming and costly23 procedure to a minimum, bothcomprehensive “all-in-one” MRI and multidetectorcomputed tomography (MDCT)-protocols have beenadvocated.24–28 Both approaches combine the advan-tage of minimal invasiveness with the simultaneousassessment of the hepatic parenchymal morphology anda detailed analysis of the biliary and vascular anatomy ina single diagnostic step.
Based on the preharvest evaluation of 25 potentialliving donors undergoing both MR and MDCT28
imaging, the purpose of this study was to compare bothmethods and to determine their specific advantages anddisadvantages.
Patients and Methods
Patient Population
Between May and October of 2001, 25 consecutive potentialliving liver donors (age range: 20-55 years, mean: 33 years)were prospectively evaluated both with “all-in-one” MDCTand “all-in-one” MRI protocols for the liver. A total of 14women (age range: 22-55 years, mean: 34 years) and 11 men(age range: 20-42 years, mean: 31 years) were enrolled in thestudy. This study was conducted in accordance with guide-lines set forth by the local ethics committee. A total of 2 of thefemale candidates and 1 male candidate were evaluated fordonation of a left lobe segment and underwent a digital sub-traction angiography study in addition, which represented amandatory step in the evaluation protocol for this sub-collec-tive. For ethical reasons, in all other subjects the application ofdigital subtraction angiography and endoscopic retrogradecholangiopancreatography was limited to those, in whommultiphase MDCT and/or MR imaging was deemed insuffi-cient to display the relevant vascular or biliary anatomy. Lab-oratory analysis had revealed normal liver function for allpotential donors prior to the examinations.
The delay between both examination protocols rangedbetween 1 and 53 days (mean: 20.4) days. A total of 12candidates obtained MDCT as the primary imaging study; inthe remaining 13 subjects MRI was performed prior toMDCT.
CT Protocol
CT imaging was performed using a 4-row CT scanner (Vol-ume-Zoom; Siemens, Erlangen, Germany). The protocol
included successive acquisition of 3 image sets of the liverusing the following parameters: 120 kVp, 150-180 mAs, col-limated slice-thickness 1 mm, feed/rotation 6 mm, pitch 1.5.The in-plane matrix size was 512 � 512. Each image set wascollected over 20 to 25 seconds. The “in-room” time wasclosely monitored.
The first CT image set was acquired 30 (�5) minutesfollowing infusion of 100 mL of a biliary contrast agent (Bilis-copin; Schering, Berlin, Germany) at a rate of 0.1 mL/sthrough a 20-gauge catheter placed in an antecubital vein.The agent was administered to opacify the biliary system, thusenabling a detailed appreciation of the contrast-enhancedintra- and extrahepatic biliary tree.
Subsequently, computed tomographic angiography(CTA) was performed for display of the arterial hepatic anat-omy. For this purpose, 140 mL of an iodinated contrast agent(Imeron 350; Bracco SpA., Milan, Italy) was administeredintravenously with an automated injector (CT9000; Liebel-Flarsheim, Cincinnati, OH) at a rate of 5 mL/s. Automatedbolus tracking with bolus detection at the level of the ascend-ing aorta assured accurate timing of an early arterial phase. Forthe display of the portal and hepatic venous anatomy, a thirdCT image set was acquired 25 seconds following the arterialdata.
MR Protocol
MRI was performed on a 1.5-T scanner (Magnetom Sonata;Siemens, Erlangen, Germany), equipped with high-perfor-mance gradients (amplitude of 40 mT/m, slew rate of 200mT/m/ms). A standard phased-array torso surface coil wasused for signal reception. The scan protocol was based on a32–36-cm field of view and included intravenous adminis-tration of Gd-BOPTA (Multihance; Bracco SpA.) at a dose of0.2 mmol/kg body weight. The contrast agent was infused ata rate of 3 mL/s using an automated injector system (Spectris;Medrad, Pittsburgh, PA). The management of the contrastmedia included a test bolus technique in the aorta at the levelof the celiac trunk to determine the arrival time of contrast forarterial enhancement29 and an intermittent 25-second delaybefore scanning the portal and hepatic venous systems.
The following sequences were acquired:
1. Axial T1-weighted two-dimensional (2D) FLASH (TR/TE: 110/2.0 ms, flip angle: 60°, 8-mm sections, matrixsize: 256 � 256).
2. Axial T1-weighted TrueFISP (TR/TE: 3.5/1.7 ms, flipangle: 80°, 7-mm sections, matrix size: 256 � 256).
3. Axial T2-weighted 2D HASTE (TR/TE: 1,000/60 ms,flip angle: 160°, 8-mm sections, matrix size: 256 � 256).
4. Coronal HASTE for magnetic resonance cholangiopan-creatography (MRCP) (TR/TE: 1,000/60 ms, sectionthickness: 8 mm, matrix size: 218 � 256).
5. Coronal RARE for MRCP (TR/TE: 2,800/1,100 ms, 180-mm section, matrix size: 240 � 512).
6. Coronal 3D FLASH for magnetic resonance angiography(MRA) (TR/TE: 2.4/1.0 ms, flip angle: 25°, 48 contigu-ous 2-mm sections, matrix size: 256 � 256, 1 arterial and
777“All-In-One” Imaging of Living Liver Donors
1 portal/hepatic venous data set collected within a singlebreathhold over 17 seconds and separated by the 25-sec-ond interval, during which the candidate was permitted tobreathe).
7. Postcontrast axial T1-weighted 2D FLASH including fatsaturation (TR/TE: 114/2.0 ms, flip angle: 60°, 10-mmsections, matrix size: 256 � 256).
Image Analysis
Analysis of the image data was based on source images, mul-tiplanar reformats, and 3D volume renderings. All 3D datasets both from MRI and MDCT were postprocessed usingcommercially available software and hardware (Virtuoso; Sie-mens, Erlangen, Germany). To provide a more realistic 3Dimpression, the data was also reviewed in “Stereo” mode,including visual enhancement by artificial coloring. Datainterpretation was based on the consensus of 2 radiologistswith over 8 and 11 years of experience (T.S. and S.G.R.), and2 transplant surgeons with over 11 and more than 20 years ofexperience, who were also familiar with the review technique(M.M. and S.N.).
Analysis of the image data was focused on the followingaspects:
1. Exclusion of focal liver lesions: The hepatic parenchymawas assessed for the presence of masses based on all col-
lected image sets. Similarly other organs were assessed forconcomitant disease.
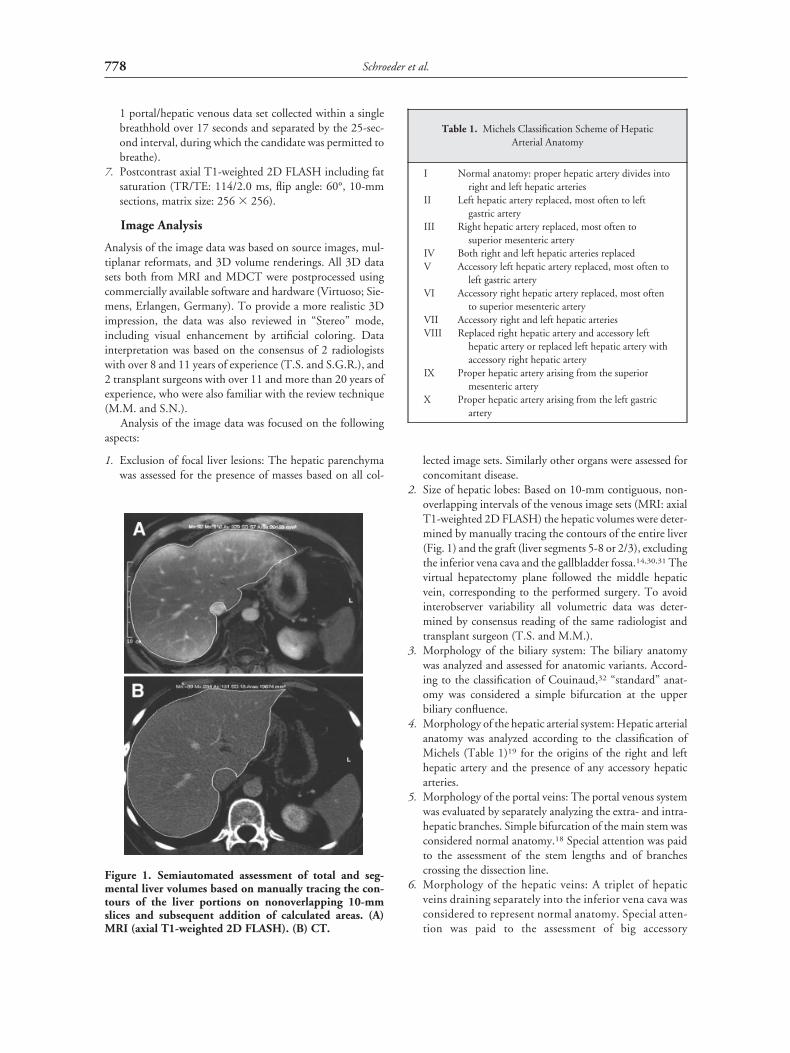
2. Size of hepatic lobes: Based on 10-mm contiguous, non-overlapping intervals of the venous image sets (MRI: axialT1-weighted 2D FLASH) the hepatic volumes were deter-mined by manually tracing the contours of the entire liver(Fig. 1) and the graft (liver segments 5-8 or 2/3), excludingthe inferior vena cava and the gallbladder fossa.14,30,31 Thevirtual hepatectomy plane followed the middle hepaticvein, corresponding to the performed surgery. To avoidinterobserver variability all volumetric data was deter-mined by consensus reading of the same radiologist andtransplant surgeon (T.S. and M.M.).
3. Morphology of the biliary system: The biliary anatomywas analyzed and assessed for anatomic variants. Accord-ing to the classification of Couinaud,32 “standard” anat-omy was considered a simple bifurcation at the upperbiliary confluence.
4. Morphology of the hepatic arterial system: Hepatic arterialanatomy was analyzed according to the classification ofMichels (Table 1)19 for the origins of the right and lefthepatic artery and the presence of any accessory hepaticarteries.
5. Morphology of the portal veins: The portal venous systemwas evaluated by separately analyzing the extra- and intra-hepatic branches. Simple bifurcation of the main stem wasconsidered normal anatomy.18 Special attention was paidto the assessment of the stem lengths and of branchescrossing the dissection line.
6. Morphology of the hepatic veins: A triplet of hepaticveins draining separately into the inferior vena cava wasconsidered to represent normal anatomy. Special atten-tion was paid to the assessment of big accessory
Figure 1. Semiautomated assessment of total and seg-mental liver volumes based on manually tracing the con-tours of the liver portions on nonoverlapping 10-mmslices and subsequent addition of calculated areas. (A)MRI (axial T1-weighted 2D FLASH). (B) CT.
Table 1. Michels Classification Scheme of HepaticArterial Anatomy
I Normal anatomy: proper hepatic artery divides intoright and left hepatic arteries
II Left hepatic artery replaced, most often to leftgastric artery
III Right hepatic artery replaced, most often tosuperior mesenteric artery
IV Both right and left hepatic arteries replacedV Accessory left hepatic artery replaced, most often to
left gastric arteryVI Accessory right hepatic artery replaced, most often
to superior mesenteric arteryVII Accessory right and left hepatic arteriesVIII Replaced right hepatic artery and accessory left
hepatic artery or replaced left hepatic artery withaccessory right hepatic artery
IX Proper hepatic artery arising from the superiormesenteric artery
X Proper hepatic artery arising from the left gastricartery
778 Schroeder et al.

branches necessitating separate anastomosis in therecipient.
Image Quality Rating and Statistical Analysis
To objectify the diagnostic performance of CT and MRI inthe visualization of the single anatomical systems, a 4-point“image quality rating” (IQR) was introduced, ranging from 1to 4: 1 � nondiagnostic; 2 � sufficient; 3 � good; 4 �excellent.
In a stepwise fashion, image analysis was performed foreach candidate separately after acquisition of all individualCT and MR data. The first step included analysis of the 2Dsource images and generation of 3D multiplanar reformatsand volume renderings by 2 experienced radiologists (T.S.and S.G.R.). Subsequently, the 2D and 3D data was reviewedtogether with 2 transplant surgeons (M.M. and S.N.). Thissuccession was chosen to assure both the highest possibleinformation extraction of the radiological data and an appro-priate understanding of the operation anatomy. Followingthis consensus reading, all 4 reviewers rated the achievedimage quality blinded to each other.
To test for statistical differences, the Wilcoxon rank testwas used; P values of less than 0.05 were regarded as statisti-cally significant differences.
Intraoperative Comparisons
The preharvest MDCT and MRI determinations regardingthe biliary and vascular morphology and the estimated vol-umes were correlated with intraoperative findings, whichserved as standard of reference. A total of 13 of the evaluatedcandidates were elected as donors and underwent right-lobetransplantation surgery. The predicted transplant volumesand the intraoperatively determined transplant weight werecompared on the basis of a 1:1 conversion factor.33–35
Results
All CT and MR examinations were diagnostic regard-ing the display of the parenchymal and vascular mor-phology, thereby obviating the need for subsequentdigital subtraction angiography and/or endoscopic ret-rograde cholangiopancreatography, apart from the 3left-lobe donation candidates.
All MR examinations (100%) and 23 (92%) of 25CT examinations were well tolerated. During the CTexamination, 2 candidates presented moderate adversereactions on the biliary contrast agent, including feeling
of heat, nausea, and erythema on face and arms. Afterstandard antihistaminic treatment in both cases com-plete recovery was achieved within 20 minutes.
The “in room” time in the MR scanner rangedbetween 15 and 23 minutes (mean: 19 minutes), com-pared to CT “in-room” time of between 9 and 13 min-utes (mean: 11 minutes). Subsequent data analysisincluding manual planimetry and assessment of the bil-iary and vascular morphology required between 25 and60 (mean: 35) minutes for the MR data, compared to25–55 (mean: 33) minutes required for the CT data(Table 2).
Liver Volumes
The determined total liver volumes ranged between1,030 and 2,166 mL (mean: 1,384 mL) in MDCT andbetween 1,095 and 2,381 mL (mean: 1,467 mL) inMRI. The peak values were found in the same patients.
The transplant volumes estimated based on the MR,in all cases showed higher liver and graft volumes. Thedifference between CT and MRI ranged between 0 and�215 mL (mean: 83 mL) or 0 and �10% (mean: 6%),respectively.
The estimated proportions (graft volume/total livervolume) in the 2 modalities were similar, both for theright- and the left-lobe donors, showing maximum dif-ferences of 3% (mean: 1.2%).
The mean IQR in the determination of the livervolumes was 3.6 for CT, compared with 3.3 for MRI.
Liver Parenchyma and Parenchymal Lesions
The same number of hepatic lesions was depicted byboth modalities (Table 3). Characterization was, how-ever, easier based on MRI (mean IQR: 3.7) than onMDCT (mean IQR: 3.4).
A total of 19 patients did not show any parenchymalabnormalities. One patient presented a lesion 2.0 �2.5 � 2.0 cm showing pathognomonic signs of a hem-angioma in segment 8. In another patient, a 1.5 �2.0 � 2.0 cm lesion of undetermined dignity was iden-tified in segment 6. Diagnostic biopsy revealed an ade-noma. Two patients showed multiple small cysts (�4
Table 2. Practical Aspects of Both “All-in-One” Protocols
MRI CT
“In-room” times 15-23 minutes (mean: 19) 9-13 minutes (mean: 11)Time for data analysis 25-60 minutes (mean: 35) 25-55 minutes (mean: 33)
779“All-In-One” Imaging of Living Liver Donors
mm) in the right hepatic lobe. Data from 2 patientsshowed signs of liver steatosis.
Biliary System
CT cholangiography visualized the intrahepatic biliarytree up to the second-, third-, and fourth-level branches(Fig. 2A).
According to the classification of Couinaud32 “stan-dard” anatomy, including a simple bifurcation at theupper biliary confluence (Type A), was seen in 12(48%) of the 25 candidates.
A total of 13 candidates (52%) presented a biliaryvariant (Table 3): trifurcation of the upper biliary con-fluence (Type B; n � 3); drainage of a right sectorialduct into the common hepatic duct (Type C; n � 4);drainage of a right sectorial duct into the left hepaticduct (Type D; n � 5); and absence of a defined upperbiliary confluence with all sectorial ducts joining sepa-rately (Type E; n � 1).
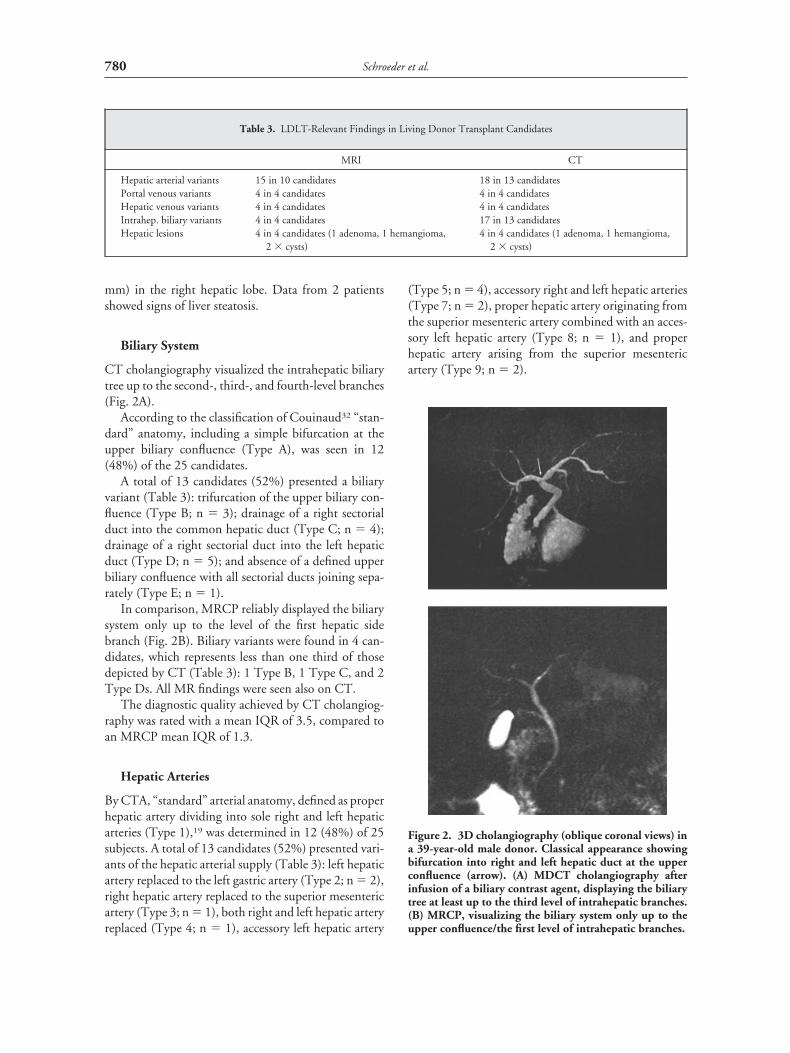
In comparison, MRCP reliably displayed the biliarysystem only up to the level of the first hepatic sidebranch (Fig. 2B). Biliary variants were found in 4 can-didates, which represents less than one third of thosedepicted by CT (Table 3): 1 Type B, 1 Type C, and 2Type Ds. All MR findings were seen also on CT.
The diagnostic quality achieved by CT cholangiog-raphy was rated with a mean IQR of 3.5, compared toan MRCP mean IQR of 1.3.
Hepatic Arteries
By CTA, “standard” arterial anatomy, defined as properhepatic artery dividing into sole right and left hepaticarteries (Type 1),19 was determined in 12 (48%) of 25subjects. A total of 13 candidates (52%) presented vari-ants of the hepatic arterial supply (Table 3): left hepaticartery replaced to the left gastric artery (Type 2; n � 2),right hepatic artery replaced to the superior mesentericartery (Type 3; n � 1), both right and left hepatic arteryreplaced (Type 4; n � 1), accessory left hepatic artery
(Type 5; n � 4), accessory right and left hepatic arteries(Type 7; n � 2), proper hepatic artery originating fromthe superior mesenteric artery combined with an acces-sory left hepatic artery (Type 8; n � 1), and properhepatic artery arising from the superior mesentericartery (Type 9; n � 2).
Table 3. LDLT-Relevant Findings in Living Donor Transplant Candidates
MRI CT
Hepatic arterial variants 15 in 10 candidates 18 in 13 candidatesPortal venous variants 4 in 4 candidates 4 in 4 candidatesHepatic venous variants 4 in 4 candidates 4 in 4 candidatesIntrahep. biliary variants 4 in 4 candidates 17 in 13 candidatesHepatic lesions 4 in 4 candidates (1 adenoma, 1 hemangioma,
2 � cysts)4 in 4 candidates (1 adenoma, 1 hemangioma,
2 � cysts)
Figure 2. 3D cholangiography (oblique coronal views) ina 39-year-old male donor. Classical appearance showingbifurcation into right and left hepatic duct at the upperconfluence (arrow). (A) MDCT cholangiography afterinfusion of a biliary contrast agent, displaying the biliarytree at least up to the third level of intrahepatic branches.(B) MRCP, visualizing the biliary system only up to theupper confluence/the first level of intrahepatic branches.
780 Schroeder et al.
In comparison, MRA (Fig. 3B) revealed variants in10 subjects (40%) (Type 2: n � 1, Type 3: n � 1, Type4: n � 1; Type 5: n � 2, Type 7: n � 2, Type 8: n � 1;Type 9: n � 2), whereas normal arterial anatomy wasseen in 15 candidates (60%). All MR findings werevisualized by CT as well. While visible on CT, MRImissed 1 replacement of the left hepatic artery and 2accessory left hepatic arteries; however, this did notaffect right lobe donation. The right hepatic variantswere similarly determined as on CT.
Considering the achieved diagnostic quality, CTAwas rated with an overall IQR of 3.5, whereas the meanIQR for MRA was 3.0.
Portal Veins
Both CT and MR imaging of the portal veins (Fig.4A-B) revealed 4 variants (Table 3), including: origin of
the portal venous branch to the dorsolateral liver seg-ments directly from the portal bifurcation (n � 2);short (�1 cm) stem of the right portal vein (n � 1); anddoubled right portal vein (n � 2). The IQRs deter-mined were 2.8 for the CT data and 3.4 for the MRdata.
Hepatic Veins
Both CT and MR imaging of the hepatic veins (Fig.4A-B) revealed 4 variants relevant for operation (Table3), including common drainage of the middle and theleft hepatic vein into the inferior vena cava (n � 2) andaccessory branches crossing the dissection line (n � 2),thus requiring an additional anastomosis. The deter-
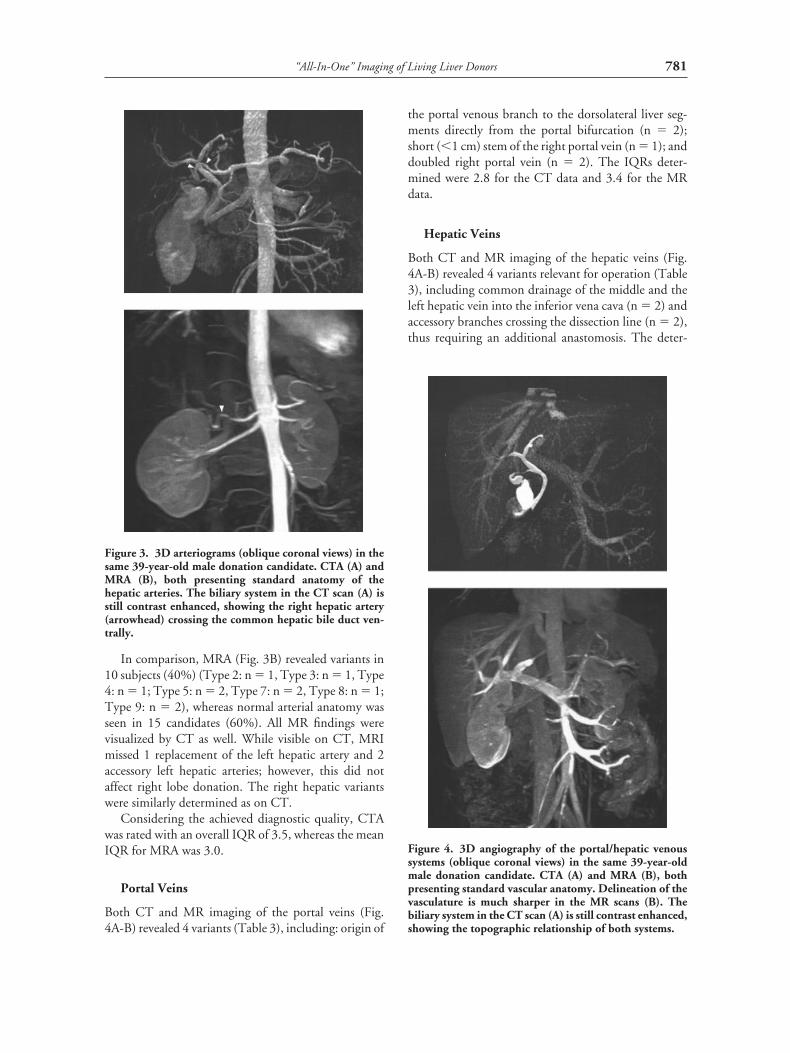
Figure 3. 3D arteriograms (oblique coronal views) in thesame 39-year-old male donation candidate. CTA (A) andMRA (B), both presenting standard anatomy of thehepatic arteries. The biliary system in the CT scan (A) isstill contrast enhanced, showing the right hepatic artery(arrowhead) crossing the common hepatic bile duct ven-trally.
Figure 4. 3D angiography of the portal/hepatic venoussystems (oblique coronal views) in the same 39-year-oldmale donation candidate. CTA (A) and MRA (B), bothpresenting standard vascular anatomy. Delineation of thevasculature is much sharper in the MR scans (B). Thebiliary system in the CT scan (A) is still contrast enhanced,showing the topographic relationship of both systems.
781“All-In-One” Imaging of Living Liver Donors
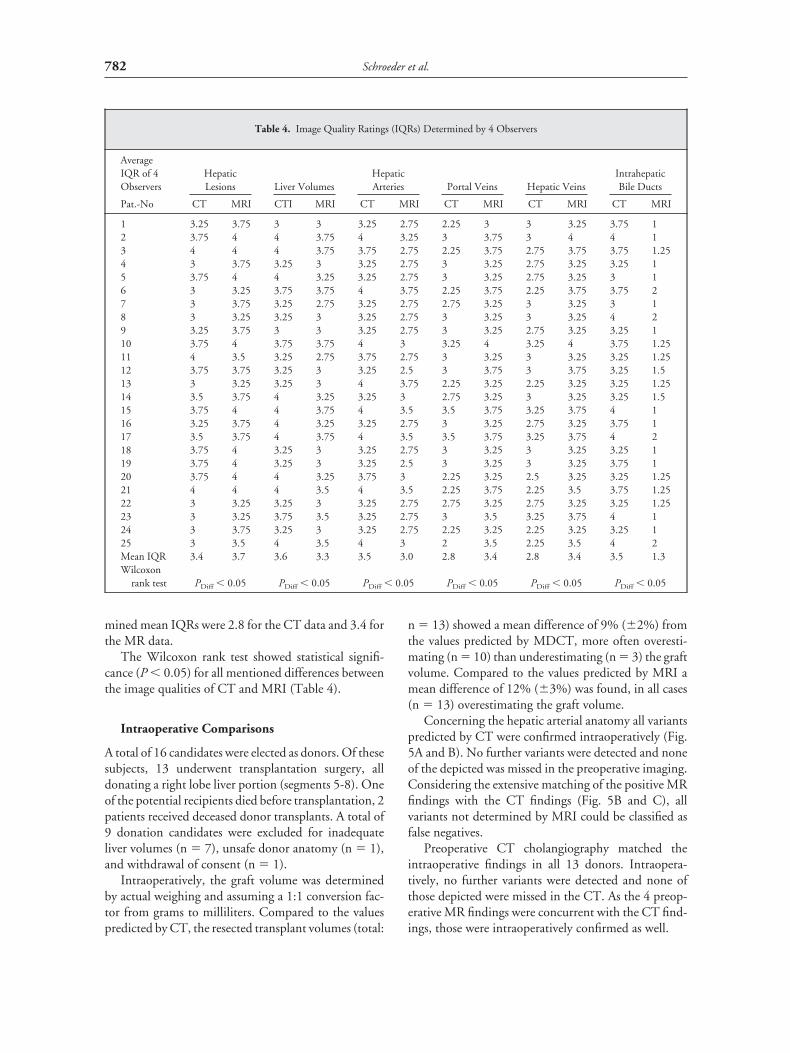
mined mean IQRs were 2.8 for the CT data and 3.4 forthe MR data.
The Wilcoxon rank test showed statistical signifi-cance (P � 0.05) for all mentioned differences betweenthe image qualities of CT and MRI (Table 4).
Intraoperative Comparisons
A total of 16 candidates were elected as donors. Of thesesubjects, 13 underwent transplantation surgery, alldonating a right lobe liver portion (segments 5-8). Oneof the potential recipients died before transplantation, 2patients received deceased donor transplants. A total of9 donation candidates were excluded for inadequateliver volumes (n � 7), unsafe donor anatomy (n � 1),and withdrawal of consent (n � 1).
Intraoperatively, the graft volume was determinedby actual weighing and assuming a 1:1 conversion fac-tor from grams to milliliters. Compared to the valuespredicted by CT, the resected transplant volumes (total:
n � 13) showed a mean difference of 9% (�2%) fromthe values predicted by MDCT, more often overesti-mating (n � 10) than underestimating (n � 3) the graftvolume. Compared to the values predicted by MRI amean difference of 12% (�3%) was found, in all cases(n � 13) overestimating the graft volume.
Concerning the hepatic arterial anatomy all variantspredicted by CT were confirmed intraoperatively (Fig.5A and B). No further variants were detected and noneof the depicted was missed in the preoperative imaging.Considering the extensive matching of the positive MRfindings with the CT findings (Fig. 5B and C), allvariants not determined by MRI could be classified asfalse negatives.
Preoperative CT cholangiography matched theintraoperative findings in all 13 donors. Intraopera-tively, no further variants were detected and none ofthose depicted were missed in the CT. As the 4 preop-erative MR findings were concurrent with the CT find-ings, those were intraoperatively confirmed as well.
Table 4. Image Quality Ratings (IQRs) Determined by 4 Observers
AverageIQR of 4Observers
HepaticLesions Liver Volumes
HepaticArteries Portal Veins Hepatic Veins
IntrahepaticBile Ducts
Pat.-No CT MRI CTI MRI CT MRI CT MRI CT MRI CT MRI
1 3.25 3.75 3 3 3.25 2.75 2.25 3 3 3.25 3.75 12 3.75 4 4 3.75 4 3.25 3 3.75 3 4 4 13 4 4 4 3.75 3.75 2.75 2.25 3.75 2.75 3.75 3.75 1.254 3 3.75 3.25 3 3.25 2.75 3 3.25 2.75 3.25 3.25 15 3.75 4 4 3.25 3.25 2.75 3 3.25 2.75 3.25 3 16 3 3.25 3.75 3.75 4 3.75 2.25 3.75 2.25 3.75 3.75 27 3 3.75 3.25 2.75 3.25 2.75 2.75 3.25 3 3.25 3 18 3 3.25 3.25 3 3.25 2.75 3 3.25 3 3.25 4 29 3.25 3.75 3 3 3.25 2.75 3 3.25 2.75 3.25 3.25 110 3.75 4 3.75 3.75 4 3 3.25 4 3.25 4 3.75 1.2511 4 3.5 3.25 2.75 3.75 2.75 3 3.25 3 3.25 3.25 1.2512 3.75 3.75 3.25 3 3.25 2.5 3 3.75 3 3.75 3.25 1.513 3 3.25 3.25 3 4 3.75 2.25 3.25 2.25 3.25 3.25 1.2514 3.5 3.75 4 3.25 3.25 3 2.75 3.25 3 3.25 3.25 1.515 3.75 4 4 3.75 4 3.5 3.5 3.75 3.25 3.75 4 116 3.25 3.75 4 3.25 3.25 2.75 3 3.25 2.75 3.25 3.75 117 3.5 3.75 4 3.75 4 3.5 3.5 3.75 3.25 3.75 4 218 3.75 4 3.25 3 3.25 2.75 3 3.25 3 3.25 3.25 119 3.75 4 3.25 3 3.25 2.5 3 3.25 3 3.25 3.75 120 3.75 4 4 3.25 3.75 3 2.25 3.25 2.5 3.25 3.25 1.2521 4 4 4 3.5 4 3.5 2.25 3.75 2.25 3.5 3.75 1.2522 3 3.25 3.25 3 3.25 2.75 2.75 3.25 2.75 3.25 3.25 1.2523 3 3.25 3.75 3.5 3.25 2.75 3 3.5 3.25 3.75 4 124 3 3.75 3.25 3 3.25 2.75 2.25 3.25 2.25 3.25 3.25 125 3 3.5 4 3.5 4 3 2 3.5 2.25 3.5 4 2Mean IQR 3.4 3.7 3.6 3.3 3.5 3.0 2.8 3.4 2.8 3.4 3.5 1.3Wilcoxon
rank test PDiff � 0.05 PDiff � 0.05 PDiff � 0.05 PDiff � 0.05 PDiff � 0.05 PDiff � 0.05
782 Schroeder et al.

The concurrent CT and MR findings concerningthe venous systems were also intraoperatively verified.No further variants were detected and none of thosedepicted were missed in the preoperative imaging.
Discussion
Both “all-in-one” MDCT and “all-in-one” MRI proved tobe feasible and robust concepts to evaluate potential livingliver donors in a single diagnostic step. Despite shorterscan times, the entire CT protocol is more time consum-ing, due to the necessity of administering the biliary con-trast agent prior to the scan. Moreover, with regard to theseveral focuses of the preharvest liver analysis, bothapproaches show specific strengths and weaknesses.
Biliary System
Regarding the high incidence of biliary variants,32,36-38
thorough analysis of the biliary anatomy is essential forthe surgical outcome in living donor liver transplanta-tion. Failure to recognize even minor intrahepaticbranches crossing the dissection line can result in severepostoperative biliary leakage.39 Even though the preop-erative acquired information will rarely lead to exclu-sion of the donation process or a dramatic change of thesurgical approach, awareness of biliary variations mayprompt thorough exploration to localize the criticalstructures. Furthermore, a better understanding of theanatomy allows for operating in a more goal-directedmanner.
Contrast enhanced CT cholangiography displayedthe biliary tree at least up to the second intrahepaticbranches in all patients. In comparison, MRCP allowedreliable visualization of the biliary system only up to thebifurcation of the common hepatic duct (Fig. 2). Forthe entire patient collective MRCP revealed about one
third of the biliary variants displayed on CT cholan-giography. This not only demonstrates the superiorityof MDCT cholangiography, but also supports theimportance of preoperative cholangiography in general.This is also mirrored by an excellent correlation withintraoperative findings and is supported by recentreports demonstrating complete agreement betweenCT cholangiography and endoscopic retrogradecholangiopancreatography.40,41
It has to be considered, however, that the techniqueused for MRCP was based on heavily T2-weightedimages and did not involve any “positive” enhancementof the biliary tree. Since this technique has been shownto be accurate regarding the analysis of the central bileducts,42 the detection of ductal dilatation, and presenceof calculi or masses,43-45 it has been established as thediagnostic standard in many centers.
The results of this study, however, illustrate that theanatomical detail achievable by this technique is not suffi-cient to depict the crucial intrahepatic branches in healthyliver donors. To compensate for such weakness, newMRCP techniques—either based on optimized sequencesor involving the administration of dedicated biliary con-trast agents (e.g., mangafodipir trisodium)—are underinvestigation. Even though recent studies report a signifi-cantly improved delineation of the intrahepatic biliarytree,46,47 the value of such techniques remains being con-troversially discussed. Recently, Yeh et al.47 performedcomparison of contrast-enhanced CT and MR cholan-giography in potential liver donors confirmed a signifi-cantly better visualization of the biliary tract by CT. How-ever, further clinical experience needs to be gained.
Hepatic Arteries
The patency of all supplying and draining vessels ismandatory for the graft and the remnant liver survival;
Figure 5. Intraoperative comparison in the same 39-year-old male donation candidate; oblique coronal views onto theproper/right hepatic artery and the upper biliary confluent (arrow: common hepatic duct; arrowhead: right hepaticartery). (A) Intraoperative appearance. (B) 3D CT arteriogram with underlying biliary tree. (C) 3D MR arteriogram.
783“All-In-One” Imaging of Living Liver Donors


the associated exposure to ionizing radiation. The effec-tive dose is estimated to range between 15 and 20 mSv.This compares to 7-12 mSv for a standard CT scan ofthe abdomen, to 0.2 mSv for a chest X-ray in 2 projec-tions, and to 2.4 mSv of natural radiation exposure peryear. Another disadvantage of the CT protocol is thenecessity of administering considerable volumes ofpotentially nephrotoxic iodinated contrast agents.Therefore, confirmation of normal renal function priorto the CT examination is mandatory. In particular, thebiliary contrast agent has been known to be associatedwith a high incidence of adverse reactions, ranging frommild and self-resolving symptoms like sensation ofwarmth, nausea, and erythema (2%) to moderate andsevere systemic adverse reactions up to shock-syndromeand death (0.01%).40,56 In addition, the administrationof the biliary agent requires normal hepatic (secretory)function and a bilirubin level below 2-4 mg/dL.41 Sinceonly patients with normal hepatic laboratory parame-ters enter the donor program, this aspect does not rep-resent a true limitation.
The MR strategy, on the other hand, obviates theneed for exposing the potential donor to ionizingradiation and the administration of nephrotoxic con-trast agents. The Gd-based agents used for MRA arecharacterized by a much superior safety profile ascompared to iodinated contrast agents; there is norenal nephrotoxicity57 and anaphylactic reactions areexceedingly rare.58 On the downside, the long exam-ination might produce discomfort to the most andserious limitations to claustrophobic donation can-didates.
Conclusion
Both “all-in-one” MDCT and “all-in-one” MRI arewell suited to extensively assess the liver anatomy ofpotential donors in a single diagnostic step. This mightreduce the need for multimodality evaluation proto-cols, hence relieving the medical infrastructure, but alsoaugmenting the candidate’s acceptance of the pretrans-plantation survey.
The favorable choice at present is, however,MDCT, owing to its superiority in the display of theintrahepatic bile ducts and arteries, its easy accessi-bility, and its shorter examination time. In our insti-tution, MDCT currently represents the standardprocedure, almost completely eliminating the needof further examinations to determine the candidate’sanatomy. Due to its lack of harm to the voluntarydonation candidates and the positive results of otherresearch groups, “all-in-one” MRI nevertheless rep-
resents both a promising and a desirable evaluationstrategy for the future. Further experiences with ded-icated MR contrast agents and improved scan tech-niques are expected to clarify whether the currentpreferences can be changed.
References1. Adam R, McMaster P, O’Grady JG, Castaing D, Klempnauer
JL, Jamieson N, et al. Evolution of liver transplantation inEurope: report of the European Liver Transplant Registry. LiverTranspl 2003;9:1231-1243.
2. Broelsch CE, Frilling A, Testa G, Malago M. Living donor livertransplantation in adults. Eur J Gastroenterol Hepatol 2003;15:3-6.
3. Malago M, Testa G, Frilling A, Nadalin S, Valentin-Gamazo C,Paul A, et al. Right living donor liver transplantation: an optionfor adult patients: single institution experience with 74 patients.Ann Surg 2003;238:853-862; discussion 862-853.
4. Raia S, Nery JR, Mies S. Liver transplantation from live donors.Lancet 1989:497-498.
5. Rogiers X, Burdelski M, Broelsch CE. Liver transplantation fromliving donors. Br J Surg 1994;81:1251-1253.
6. Broelsch CE, Emond JC, Whitington PF, Thistlethwaite JR,Baker AL, Lichtor JL. Application of reduced-size liver trans-plants as split grafts, auxiliary grafts, and living related segmentaltransplants. Ann Surg 1989;212:368-375.
7. Hashikura Y, Makuuchi M, Kawasaki S, Matsunami H, IkegamiT, Nakasawa Y, et al. Successful living-related partial liver trans-plantation to an adult patient. Lancet 1994;343:1233-1234.
8. Broelsch CE, Testa G, Alexandrou A, Malago M. Living relatedliver transplantation: medical and social aspects of a controversialtherapy. Gut 2002;50:143-145.
9. Mueller AR, Pascher A, Platz KP, Schulz RJ, Rayes N, SeehoferD, et al. Immunosuppressive management following intestinaltransplantation in adult patients. Transplant Proc 2003;35:2075-2077.
10. Settmacher U, Neuhaus P. [Innovations in liver surgery throughtransplantation from living donors]. Chirurg 2003;74:536-546.[Ger]
11. Broelsch CE, Malago M, Testa G, Valentin-Gamazo C. Livingdonor liver transplantation in adults: outcome in Europe. LiverTranspl 2000;6:64-65.
12. Grewal HP, Thistlewaite JR Jr, Loss GE, Fisher JS, Cronin DC,Siegel CT, et al. Complications in 100 living-liver donors. AnnSurg 1998;228:214-219.
13. Emond JC, Renz JF, Ferrell LD, Rosenthal P, Lim RC, RobertsJP, et al. Functional analysis of grafts from living donors. Impli-cations for the treatment of older recipients. Ann Surg 1996;224:544-552.
14. Gonzalez-Chamorro A, Loinaz Segurola C, Moreno Gonzalez E,Jimenez Romero C, Gonzalez-Pinto Arrillaga I, Gomez Sanz R,et al. Graft mass and volume calculation in living related donorsfor liver transplantation. Hepatogastroenterology 1998;45:510-513.
15. Lo CM. Complications and long-term outcome of living liverdonors: a survey of 1,508 cases in five Asian centers. Transplan-tation 2003;75:12-15.
16. Lo CM, Fan ST, Liu CL, Chan JK, Lam BK, Lau GK, et al.Minimum graft size for successful living donor liver transplanta-tion. Transplantation 1999;68:1112-1116.
785“All-In-One” Imaging of Living Liver Donors

17. Tanaka H, Harihara Y, Kita Y, Kawarasaki H, Hashizume K,Takayama T, et al. Changes in graft volume after living-relatedliver transplantation. Transplant Proc 1999;31:2895-2896.
18. Akgul E, Inal M, Soyupurak S, Binokay F, Aksungur E, Oguz M.Portal venous variations: prevalence with contrast enhanced heli-cal CT. Acta Radiol 2002;43:315-319.
19. Michels NA. Newer anatomy of the liver and its variant bloodsupply and collateral circulation. Am J Surg 1966;112:337-347.
20. Noah EM, Klinzing S, Zwaan M, Schramm U, Bruch HP, WeissHD. [Normal variation of arterial liver supply in mesenterico-celiacography]. Anat Anz 1995;177:305-312. [Ger]
21. Valentin-Gamazo C, Malago M, Karliova M, Lutz JT, Frilling A,Nadalin S, et al. Experience after the evaluation of 700 potentialdonors for living donor liver transplantation in a single center.Liver Transpl 2004;10:1087-1096.
22. Pomfret EA, Pomposelli JJ, Lewis WD, Gordon FD, Burns DL,Lally A, et al. Live donor adult liver transplantation using rightlobe grafts: donor evaluation and surgical outcome. Arch Surg2001;136:425-433.
23. Hoffmann V, Richter GM, Funk H, Otto G, Kauffmann GW.[Liver transplantation and diagnostic radiology: socioeconomicaspects]. Rofo 1996;165:113-117. [Ger]
24. Bassignani MJ, Fulcher AS, Szucs RA, Chong WK, Prasad UR,Marcos A. Use of imaging for living donor liver transplantation.Radiographics 2001;21:39-52.
25. Goyen M, Barkhausen J, Debatin JF, Kuhl H, Bosk S, Testa G,et al. Right-lobe living related liver transplantation: evaluation ofa comprehensive magnetic resonance imaging protocol forassessing potential donors. Liver Transpl 2002;8:241-250.
26. Lee VS, Morgan GR, Teperman LW, John D, Diflo T, Pan-dharipande PV, et al. MR imaging as the sole preoperative imag-ing modality for right hepatectomy: a prospective study of livingadult-to-adult liver donor candidates. AJR Am J Roentgenol2001;176:1475-1482.
27. Kamel IR, Kruskal JB, Pomfret EA, Keogan MT, WarmbrandG, Raptopoulos V. Impact of multidetector CT on donor selec-tion and surgical planning before living adult right lobe livertransplantation. AJR Am J Roentgenol 2001;176:193-200.
28. Schroeder T, Nadalin S, Stattaus J, Debatin JF, Malago M,Ruehm SG. Potential living liver donors: evaluation with anall-in-one protocol with multi-detector row CT. Radiology2002;224:586-591.
29. Earls JP, Rofsky NM, DeCorato DR, Krinsky GA, Weinreb JC.Breath-hold single-dose gadolinium-enhanced three-dimen-sional MR aortography: usefulness of a timing examination andMR power injector. Radiology 1996;201:705-710.
30. Tudoret L. [Measurement of the volume of the liver by 3Dcomputed tomography with anatomic correlation]. Ann Radiol(Paris) 1994;37:401-404. [Fre]
31. Kamel IR, Kruskal JB, Warmbrand G, Goldberg SN, PomfretEA, Raptopoulos V. Accuracy of volumetric measurements aftervirtual right hepatectomy in potential donors undergoing livingadult liver transplantation. AJR Am J Roentgenol 2001;176:483-487.
32. Couinaud C. The surgical anatomy of the liver revisited. Paris:Maugein & Cie, 1989:84-89, 96-101, 108-117.
33. Schiano TD, Bodian C, Schwartz ME, Glajchen N, Min AD.Accuracy and significance of computed tomographic scan assess-ment of hepatic volume in patients undergoing liver transplan-tation. Transplantation 2000;69:545-550.
34. Lemke AJ, Brinkmann MJ, Pascher A, Steinmuller T, Settma-cher U, Neuhaus P, et al. [Accuracy of the CT-estimated weight
of the right hepatic lobe prior to living related liver donation(LRLD) for predicting the intraoperatively measured weight ofgraft]. Rofo 2003;175:1232-1238. [Ger]
35. Frericks BB, Kiene T, Stamm G, Shin H, Galanski M. [CT-based liver volumetry in a porcine model: impact on clinicalvolumetry prior to living donated liver transplantation]. Rofo2004;176:252-257. [Ger]
36. Schroeder T, Malago M, Debatin JF, Testa G, Nadalin S, Bro-elsch CE, et al. Multidetector computed tomographic cholan-giography in the evaluation of potential living liver donors.Transplantation 2002;73:1972-1973.
37. Smadja C, Blumgart LH. The biliary tract and the anatomy ofbiliary exposure, 2nd ed. Edinburgh: Churchill Livingstone,1994:11-24.
38. Ohkubo M, Nagino M, Kamiya J, Yuasa N, Oda K, Arai T, et al.Surgical anatomy of the bile ducts at the hepatic hilum as appliedto living donor liver transplantation. Ann Surg 2004;239:82-86.
39. Testa G, Malago M, Broelsch CE. Complications of biliary tractin liver transplantation. World J Surg 2001;25:1296-1299.
40. Cheng YF, Lee TY, Chen CL, Huang TL, Chen YS, Lui CC.Three-dimensional helical computed tomographic cholangiog-raphy: application to living related hepatic transplantation. ClinTransplant 1997;11:209-213.
41. Fleischmann D, Ringl H, Schofl R, Potzi R, Kontrus M, HenkC, et al. Three-dimensional spiral CT cholangiography inpatients with suspected obstructive biliary disease: comparisonwith endoscopic retrograde cholangiography. Radiology 1996;198:861-868.
42. Taourel P, Bret PM, Reinhold C, Barkun AN, Atri M. Anatomicvariants of the biliary tree: diagnosis with MR cholangiopancre-atography. Radiology 1996;199:521-527.
43. Hall-Craggs MA, Allen CM, Owens CM, Theis BA, Donald JJ,Paley M, et al. MR cholangiography: clinical evaluation in 40cases. Radiology 1993;189:423-427.
44. Romagnuolo J, Bardou M, Rahme E, Joseph L, Reinhold C,Barkun AN. Magnetic resonance cholangiopancreatography: ameta-analysis of test performance in suspected biliary disease.Ann Intern Med 2003;139:547-557.
45. Sica GT, Braver J, Cooney MJ, Miller FH, Chai JL, Adams DF.Comparison of endoscopic retrograde cholangiopancreatogra-phy with MR cholangiopancreatography in patients with pan-creatitis. Radiology 1999;210:605-610.
46. Lee VS, Krinsky GA, Nazzaro CA, Chang JS, Babb JS, Lin JC, etal. Defining intrahepatic biliary anatomy in living liver trans-plant donor candidates at mangafodipir trisodium-enhancedMR cholangiography versus conventional T2-weighted MRcholangiography. Radiology 2004;233:659-666.
47. Yeh BM, Breiman RS, Taouli B, Qayyum A, Roberts JP, Coak-ley FV. Biliary tract depiction in living potential liver donors:comparison of conventional MR, mangafodipir trisodium-en-hanced excretory MR, and multi-detector row CT cholangiog-raphy—initial experience. Radiology 2004;230:645-651.
48. Fulcher AS, Szucs RA, Bassignani MJ, Marcos A. Right lobeliving donor liver transplantation: preoperative evaluation of thedonor with MR imaging. AJR Am J Roentgenol 2001;176:1483-1491.
49. Vogl TJ, Pegios W, McMahon C, Balzer J, Waitzinger J,Pirovano G, et al. Gadobenate dimeglumine—a new contrastagent for MR imaging: preliminary evaluation in healthy volun-teers. AJR Am J Roentgenol 1992;158:887-892.
50. Yamashita Y, Mitsuzaki K, Miyazaki T, Namimoto T, Sumi S,Urata J, et al. Gadolinium-enhanced breath-hold three-dimen-
786 Schroeder et al.

sional MR angiography of the portal vein: value of the magneti-zation-prepared rapid acquisition gradient-echo sequence. Radi-ology 1996;201:283-288.
51. Rodgers PM, Ward J, Baudouin CJ, Ridgway JP, Robinson PJ.Dynamic contrast-enhanced MR imaging of the portal venoussystem: comparison with x-ray angiography. Radiology 1994;191:741-745.
52. Peterstein J, Spinazzi A, Giovagnoni A, Soyer P, Terrier F, Len-cioni R. Focal liver lesions: evaluation of the efficacy of gado-benate dimeglumine in MR imaging—a multicenter phase IIIclinical study. Radiology 2000;215:727-736.
53. Hawighorst H, Schoenberg SO, Knopp MV, Essig M, Miltner P,van Kaick G. Hepatic lesions: morphologic and functional charac-terization with multiphase breath-hold 3D gadolinium-enhancedMR angiography—initial results. Radiology 1999;210:89-96.
54. Rinella ME, Alonso E, Rao S, Whitington P, Fryer J, AbecassisM, et al. Body mass index as a predictor of hepatic steatosis inliving liver donors. Liver Transpl 2001;7:409-414.
55. Higashiyama H, Yamaguchi T, Mori K, Nakano Y, YokoyamaT, Takeuchi T, et al. Graft size assessment by preoperative com-puted tomography in living related partial liver transplantation.Br J Surg 1993;80:489-492.
56. Nilsson U. Adverse reactions to iotroxate at intravenous cholan-giography. A prospective clinical investigation and review of theliterature. Acta Radiol 1987;28:571-575.
57. Prince MR, Arnoldus C, Frisoli JK. Nephrotoxicity of high-dosegadolinium compared with iodinated contrast. J Magn ResonImaging 1996;6:162-166.
58. Shellock FG, Kanal E. Safety of magnetic resonance imagingcontrast agents. J Magn Reson Imaging 1999;10:477-484.
787“All-In-One” Imaging of Living Liver Donors





























![[2016] Computed Tomography Imaging in Oncology](https://img.pdfslide.us/doc/110x75/577c7d591a28abe0549e6f04/2016-computed-tomography-imaging-in-oncology.jpg)