Embed Size (px)
DESCRIPTION
A beginning guide to your child's hearing and hearing loss.
Citation preview

Page
1
All About Hearing Loss
Table of Contents:
About the Author / Introduction Page 2Why should I be Concerned About my Child’s Hearing? Page 3Symptoms of a Hearing Loss Page 5Types of Hearing Loss Page 8When should I have my child’s hearing screened? Page 9The Hearing Test Page 10A Quick Anatomy Lesson Page 14Otitis Media (Ear Infection) Page 18Noise Induced Hearing Loss Page 22Treatment for Hearing Loss Page 24The Effects of Hearing Loss Page 27Supporting Your Child Page 28Resources/References Page 30
About the Author

Page
2
Stephanie Barry received her Bachelor of Science in Education from the University of Nebraska-Lincoln and then went on to receive her Master of Science in Speech-Language Pathology also from the University of Nebraska-Lincoln. She holds a Certificate of Clinical Competence from the American Speech-Language and Hearing Association, a regular license from the Arizona Department of Health Services and a Standard Teaching Certificate (speech-language impaired) from the Arizona Department of Education. She has worked in several school districts, acute care and children’s hospitals and has been in private practice for several years.
Stephanie founded Independent Speech, and online speech therapy private practice to help combat the shortage of speech pathologists. This practice serves school-aged children and adults experiencing a variety of communication disorders using real time video and audio over a secure internet site. The activities are designed by speech pathologists to be engaging and motivating and are tailored to meet each individuals specific needs. It is an exciting alternative to traditional speech therapy. To learn more please visit http://www.independentspeech.com
IntroductionThis e-book is intended to be a general overview of your child’s hearing. This book discuses things in generalities. While it may include specific examples or lists of things these are not meant to be comprehensive or set in stone.
Your child is a unique individual and their hearing is just as unique as they are. While two children may both be diagnosed with the same condition; their symptoms, treatment and/or attitudes may be different. While I have tried to include as many parameters as possible it is inevitable that something has been left out or not discussed as completely as one may like.
If after reading this book you have any questions, you may contact me directly at [email protected]. I am more than happy to provide additional information or provide you with resources that can fully answer any questions/concerns you may have.
I hope you find this e-book very informative and useful!
Why should I be concerned about my child’s hearing?Children learn to communicate through their hearing. They begin by imitating the sounds they hear around them, if they do not hear them

Page
3
they cannot learn them. However, many children have a hearing problem and their parents do not realize it! There is a large range of hearing problems that can be experienced by children. While some are quite obvious others may go undetected for several years. At this time, children with hearing loss are an underidentified and thus underserved population.
When the child’s hearing loss is severe or profound it is immediately noticeable and they are evaluated and receive services quickly. The children who go unidentified are those who experience a mild loss and sometimes a moderate loss depending on their age. Other things are blamed for the child’s misunderstandings or errors. For example, a parent thinks the child has difficulty following directions because when they say to the child “Please get me the spoons.” they come back with one spoon not because they cannot follow directions but because they heard “Plea get me the poon.” They are making this error of their hearing acuity (missing the /s/ sound) not their listening skills, language skills, attention skills, etc. They have learned what a “poon” is just as a child with normal hearing learns the meaning of “spoon” so they know what to get but in missing that plural-s they get the wrong quantity. Older children may have learned some coping behaviors such as asking questions to get more information, as in “How many?” so they avoid bringing back the wrong number. Parents also learn coping behaviors and may ask more specific questions such as “Please get me two spoons.” This is an example of why hearing screenings are so important whether or not you think there is a problem with your child’s hearing acuity.
Sometimes hearing loss is brought up by another professional. In the example above, the child may be referred for a speech-language evaluation because if they are not hearing the /s/ sound they are not producing it either. This should lead to a hearing screening and eventually a hearing test which will uncover the heart of the problem. Thus if you have any concerns about your child’s development please see a specialist. The sooner these things are identified, the earlier intervention can begin which is better for everyone.
If your child mentions it is hard to hear in the classroom, says things like “huh” or “what” frequently or mishears you often you will want to take them in for a hearing screening. Your pediatrician or the school nurse can usually complete this screening. Early intervention is very important as the earlier the hearing loss occurs in the child’s life the greater the impact is on the child’s development. However, if the hearing loss is treated early and appropriately we can minimize this impact. Typically children will have a hearing screening when they are around 4 years of age or when they

Page
4
enter school, however if you have any concerns prior to this get their hearing screened earlier – they get their first hearing screening at birth so they are never to young!
A parent wants to continually monitor their child’s hearing abilities because it is an essential part of learning. If an undetected hearing loss is present, the child may miss out on the speech and language around them. This may manifest itself later in delayed speech-language skills, delayed development, social difficulty and academic difficulties as well as impact their choice of profession. We will delve into each of these areas in later sections of this e-book.
It may surprise you to know that two out of every 100 children under 18 have a hearing loss. While hearing loss varies in degree with early intervention there are very few hearing losses that cannot be helped.
Symptoms of a Hearing LossSome parents feel that since their child passed the initial hearing screening in the hospital they do not have to worry about their child’s hearing. This is not the case. Hearing loss may appear later in childhood due to infections, trauma and noise levels. It is important to continually monitor your child’s hearing throughout their development. Remember, if you have any concerns please have your child’s hearing

Page
5
screened. The most critical time for speech and language development is birth to four years of age and the child’s hearing ability directly affects this development. The following are age appropriate behaviors for various age levels. If you notice that your child is not engaging in some of these behaviors or they previously did and have stopped you should get a hearing screening completed. You can always complete an informal test at home. Make a loud noise to see if your child startles, move a noise-making toy to see if the child will locate the sound, etc. Remember, if you have any concerns please have their hearing checked, it can only benefit you and your child!
Birth to 4 months: Awakens or startles at loud noisesCalms at the sound of a familiar voice
(recognizes parent’s or caregiver’s voice).Responds to your voice
4 to 9 months: Turns eyes or head toward source the of a soundNotices sound-making toysSeems to understand simple word/hand motions
such as saying "bye-bye" while wavingSmiles when spoken toCries differently for different needs
(hungry, needs diaper change, etc.)Makes some babbling sounds
9 to 15 months: Babbles a lot of different soundsResponds to changes in your voiceResponds to his/her nameSays "ma-ma" or "da-da"Understands simple requests/directionsRepeats/imitates some sounds you makeUses his/her voice to attract attention (screams, laughs, etc.)
15-24 months: Points to familiar objects when they are namedNames common objectsUses several different wordsPuts two or more words togetherListens to stories, songs and rhymesFollows simple directionsPoints to body parts when asked

Page
6
As your child grows watch out for these signs of a hearing loss:1) Has limited or poor speech or no speech at all2) Speaks differently than same age peers3) Has difficulty understanding what people are saying4) Uses the words “what” or “huh” many times during the day5) Is inattentive6) Shows difficulties learning7) Watches others and imitates what they are doing 8) Watches peoples faces while they are speaking9) Tries to frequently increase the volume on things (TV, radio,
etc) or sits too close10) Has trouble 11) Fails to respond to conversation level speech (you shout to
gain their attention)12) Doesn’t respond when you call him/her13) Answers questions inappropriately 14) Complains of pain in the ears or noises in the head
(ringing, buzzing, etc.)
If at any time your child complains of pain in the ear whether verbally or non-verbally (pulling at their ear, sticking their finger in their ear, etc.) take your child in to their pediatrician to ensure they do not have an ear infection or a foreign object stuck in the ear canal.
At times a child may notice a hearing difference but not be able to explain what is bothering them just that their ear is felling funny in some way. They may have excessive earwax which is making things sound quieter to the child a foreign object stuck in their ear that is uncomfortable, etc. If they complain, have it checked out by their pediatrician. It is better to be safe when dealing with your child’s hearing.
One note of caution, foreign object in the ear canal has been mentioned a few times here. There is this old adage that says “never stick anything in your ear smaller than your elbow” this is an important thing to remember as many want to clean out their child’s ears with a Q-tip. This is not the best choice for three reasons. First, you may compact the ear wax normally present in the ear down toward the eardrum making it harder for your child to hear. Secondly, little pieces of the Q-tip may be left behind in the ear canal. Finally, if you are able to stick things in your child’s ear then they should be able to as well. This may lead to sticking things like pencils, or tiny objects (that they think might fit) into their ear canal or their siblings ear canal, or they may just want to imitate you by sticking a Q-tip in their ear. However, they may insert this object too far and run the risk of puncturing their ear drum causing pain and temporary hearing loss.

Page
7
There are many other choices for cleaning out the ear if you feel it is necessary. Check with your pediatrician to determine what product he/she thinks is the best for your child. There are several types of products such as irrigation systems, earwax dissolving agents, etc. that can be used to clean out the ear canal safely. Remember, earwax is there for a reason, it is meant to protect the eardrum from foreign material (dust, etc) so you do not want to be devoid of earwax. It is when the earwax is excessive that is becomes of concern.
Types of Hearing LossThere are two categories of hearing loss; congenital and acquired. Congenital means that the loss was present at birth and acquired means the child acquired the hearing loss after birth. These hearing losses may be conductive, sinsorienural or a mixture of both.
Conductive hearing loss is experienced when a disorder in either the outer or middle ear prevent sound from moving into the inner ear. Young children often experience conductive hearing loss. Conductive hearing loss can be temporary such as when a foreign object is in the ear canal, or the child is experiencing an ear infection which casuses a block in the hearing pathway. Following treatment, the child regains their previous hearing levels. Typically, conductive hearing loss can be

Acoustic Neroma Meniere’s Disease Meningitis Diabetes Stroke
Page
8
improved either medically or surgically if treated quickly. There are several common causes of conductive hearing loss including;
Ear wax build-up Foreign object in the ear canal Infection of the ear canal or middle ear Unusual growths in the outer ear or middle ear Eardrum perforation Fluid in the middle ear Otoscherosis Dislocation of the occicles
Sensorineual hearing loss is experienced when there is damage to the inner ear that interferes with hearing. The outer and middle ear are functioning properly. The damage may be to the structures of the inner ear or to the 8th cranial nerve. This is most common among adults. Unfortunately this type of hearing loss cannot be treated medically or surgically, however people benefit from the use of hearing aids or cochlear implants. While a conductive loss can be temporary a sensorineural loss cannot. The most common cause for sensorineural hearing loss is age. As we age the sensory cells in the inner ear slowly die. Sensorineural hearing loss can also be caused by:
Heredity High fever Noise exposure Ototoxic drugs Viral infections Injury
The third type of hearing loss is a mixed hearing loss. This is diagnosed when there are components of both a conductive and sensorineural hearing loss being experienced at the same time.
When should I have my child’s hearing screened?Typically a newborn will have their hearing screened before they leave the hospital. Many states now require this to be completed prior to discharge. If not, it is presented as an option and one that you should take! It is important that their first hearing screening be completed within the first three weeks.
If your child failed this first screening a second screening should be completed within 3 months to determine if a true hearing loss was detected or if debris or fluid in the ear interfered with test. If the second screening confirmed a hearing loss you should start treatment immediately. It has been said that treatment for hearing loss can be the most effective if started before the child is six months old.

Page
9
New laws have been passed to help ensure all newborn infants have a hearing screening and that those with a hearing loss or those at a high risk for a hearing loss are identified so they are able to receive follow-up services such as more frequent re-screenings. Although the system is improving, it is up to you to follow-up with additional hearing screenings if needed. Nationally, 46% of the infants born in 2006 did not complete a follow-up after they failed the newborn hearing screening (ASHA Leader, July 14, 2009). So while the laws are improving parents remain the most important advocate for their child’s hearing.
ASHA (American Speech-Language and Hearing Association) will focus on the importance of continued hearing screenings at 12 months of age and 18 months of age in addition to the prekindergarten and school-age screenings as they update the EHDI (Early Hearing Detection and Intervention) bill in the near future. They are trying to ensure that every child has frequent hearing screenings which will allow intervention to begin as quickly as possible after a loss is experienced.
If your child passed this initial screening, that is great but you are not finished with screenings yet! If your child appears to have normal hearing they should continue to have their hearing screened. This can be completed during your child’s well-check visits with their pediatrician. Most schools also complete hearing screenings at certain grade levels. Typically the child should have their hearing screened at ages 4, 5, 6, 8, 10, 12, 15 and 18 and at any time there is a concern.
The Hearing Test…There are two ways a child’s hearing can be tested, a screening and an evaluation. A screening can be done in the pediatrician’s office, an ENT’s office, the school nurses office, and by some Speech Pathologists during a speech-language evaluation or therapy or by another individual who is a licensed hearing screener. Screenings are designed to tell you if a full evaluation is needed. A child will either pass or fail a hearing screening though the practitioner cannot tell you detailed information about why a failure occurred. These screenings are done with an audiometer that presents a sound to the child through earphones (described more below). The child then indicates when they hear a sound typically by raising their hand. If they do not indicate they hear a sound when one is presented they will fail the exam and be referred for an evaluation.

Page
10
A full evaluation is completed by an Audiologist. An Audiologist is a person who is trained in hearing, hearing loss and interventions (such as hearing aids). They can see a child of any age for any hearing concern. If you have a concern about your child’s hearing an Audiologist is the best person to talk to as they are specifically trained and can provide the highest quality information. While your pediatrician may be able to provide some useful information, if you have any concerns please see an Audiologist, remember the earlier a loss is identified the earlier interventions can be put in place which minimizes the overall effects of the loss on your child’s development!
There are three parts to a typical evaluation. They include a physical examination, pure tone audiometry and speech audiometry if these cannot be completed the Audiologist will use physiologic tests. Even if pure tone and speech audiometry are completed, the Audiologist may elect to complete physiologic tests for more detailed information, such as tymponometry to assess the middle ear function.
The first thing an Audiologist will do is complete a physical examination. They will check the outer ear for malformation. They will examine the ear canal to look for excessive ear wax, a foreign object in the ear and any malformations of the ear canal. They will look at the eardrum for a perforation, signs of infection or fluid. If necessary they will make a medical referral for evaluation and treatment.
There are two types of “traditional” hearing tests. The term “traditional” is used here because these tend to be what people think of when they hear the term “hearing test”. These tests are designed to test air conduction or the sound (the sound traveling through the “air” to be heard by the listener).
The first is pure tone audiometry. This is typically the test that is completed during a hearing screening. In this test a machine known as an audiometer produces a sound (generally a beeping sound) at different volumes (decibels) and pitches (hertz) in the child’s ears. They are asked to respond when they have heard the sound, usually by raising their hand.
Conditioned play audiometry is pure tone audiometry with a twist for younger children. During this test a child is shown how to complete a play task (such as putting a block in container) each time they hear a sound. Typically this is completed in a sound treated room with or without the use of earphones. This type of test is used with children between 2½ and 5 years of age.

Page
11
A child may also complete a bone conduction test. In this test, an oscillator is placed on the bone behind the child’s ear or on the forehead. This is testing the auditory nerve through the vibration of the bones in the skull. This measures the functionality of the inner ear without the outer and middle ear being involved. We use both air conduction and bone conduction when we are hearing. This is why when you listen to your voice on a recording you sound different to yourself.
Air conduction tests can indicate a conductive or sensorineural hearing loss where as a bone conduction test only indicates a sensorineural hearing loss thus an audiologist uses the results of both tests to aid in determining which type of hearing loss is being experienced.
An audiologist will also complete speech audiometry. The first test is called a Speech Recognition Threshold (SRT) which determines the faintest level at which a person can hear and accurately repeat two-syllable words. These words are called Spondee words, they have equal stress on each syllable (for example, ice cream, hot dog, etc.). This test is completed in each ear separately and the faintest level at which 50% of the words are identified is recorded.
The second test is to determine word recognition. This test uses single syllable words at the same loudness level. This test requires the person to repeat words (or point to pictures) and the percentage of word correctly repeated (or identified) is recorded for each ear individually. There are also phsyological tests that can determine the presence of a hearing loss. They may be used independently or in conjunction with the tests described above. They can help resolve conflicting information from the behavioral testing or supplement the information obtained from these tests.
Physiological tests are not actual hearing tests but rather estimates of hearing function. These tests are completed with children who can not sit and complete the traditional test due to age, developmental delay or other medical issue. They are, at times, able to determine which function of the auditory system is causing the loss. There are four types of physiologic test that can be completed. At times, these tests are completed in addition to a traditional hearing test to gain more information about the child’s specific hearing loss.
The first type of physiologic test is the Auditory Brainstem Response test (ABR). This is the test may be completed on infants prior to their being discharged from the hospital. With this test, tiny earphones are placed in the child ear canals. Typically a click-type sound is

Page
12
introduced through the earphones and electrodes measure the nerve’s response to the sounds. A computer will then average the responses and generate a waveform. These waveforms are then compared to a waveform for normal hearing. A normal ABR can predict a baby’s hearing is normal fairly well. An abnormal ABR does not necessarily mean there is a hearing loss, there may be another medical condition present or measurement difficulties. If your child receives an abnormal ABR there hearing should be rescreened to determine if a hearing loss is truly present.
The second type of physiologic test is an Auditory Steady State Response test (ASSR). This is a new test that currently must be done with the ABR to assess hearing. This is similar to the ABR in that sound is transmitted through the ear canals and is recorded by a computer that automatically establishes the hearing level. This test is currently under development.
Third is the Otoacoustic Emissions test (OAE). A tiny probe is placed in the child’s ear canal. Then many pulse-type sounds are introduced and an echo response is recorded. These recordings are averaged by a computer and a normal result is associated with normal inner ear function and thus reflects normal hearing. This test is only effective in determining if an inner ear problem is present. They may receive a normal OAE result but have a problem in a different part of the hearing pathway. This test may be completed prior to an infant being discharged from the hospital either in conjunction with an ABR or in lieu of the ABR.
The final type is Tympanometry. This test shows how well the eardrum moves when a soft sound and air pressure are introduced into the ear canal. This test is used to identify middle ear problems such as fluid in the middle ear. This test gives us a graphic image of the eardrum movement. If the graph is a flat line this may indicate that the eardrum is not moving which is consistent with hearing problems. If the graph shows a peaked pattern this often indicates normal hearing function. A visual ear exam should be performed in conjunction with tympanometry.
You will receive a report following the completion of the exam. This report will detail the findings of the audiologist. They will provide recommendations based on the test results which may include the fitting of hearing aids, speech-language therapy and/or medical intervention if necessary (such as the placement of PE tubes). This report may include an audiogram which indicates where your child’s hearing falls on the spectrum. This is a visual representation of what your child is hearing.

Page
13
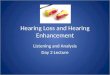
Below is an audiogram showing the hearing levels that correspond to normal hearing as well as a mild, moderate, severe and profound hearing loss.
The audiogram alone does not diagnose any hearing loss. The audiologist will look at the results of all the examinations completed to determine if it is a conductive loss, sensorineural loss or a mixed loss as well as what intervention is most appropriate for this child. Please ask any questions you may have, the audiologist is the best person to discuss these results with you to ensure you have a complete understanding of your child’s hearing status.
A Quick Anatomy LessonThere are four parts to your hearing pathway. These parts include the outer ear, middle ear, inner ear and brain. This section will describe these parts and hearing problems associated with each part. Please note that there can be damage to any part of the ear that causes problems with hearing. Included in each section are just a few of the diseases/disorders that can affect a persons hearing. There are many other factors that affect a person’s hearing such as noise levels, trauma, heredity, medication, etc. which are not referenced in this section.
The first part of the hearing pathway is the outer ear. This consists of the outer ear (pinna) and ear canal. The pinna is the part of the ear we
Frequency (HZ)250 500 1000 2000 4000 8000
-10
25
45
65
85
130
Hea
ring
Leve
l (in
dB)

Page
14
see. Its job is to collect and direct sound into the ear canal. It serves to protect the eardrum and middle ear.
The ear canal directs sound toward the ear drum. It also creates earwax (cerumen) to help protect the eardrum. However, if there is too much earwax present it may negatively impact your child’s hearing as the sound cannot get to the eardrum.
The second part of the hearing pathway is the middle ear. The middle ear starts at the eardrum (tympanic membrane). The middle ear is an air filled chamber that houses three tiny bones called the ossicles. These bones got their name because of their shape, and can be referred to by their technical or common names (noted in parentheses). These bones are the malleus (hammer), incus (anvil) and stapes (stirrup).
The eardrum vibrates when sound is presented. This starts a domino affect in the middle ear. The eardrum is connected to the first ossicle and when the eardrum starts to vibrate it causes the malleus to vibrate which in turn cases the incus and finally the stapes to vibrate. This vibration pathway moves the sound toward the inner ear. The stapes has the unique job of converting the sound energy into mechanical energy so it can be interpreted by the inner ear. The stapes attaches to the oval window which is the beginning of the inner ear.
The final part of the middle ear is the eustachian tube. This tube connects the middle ear to the throat. This connection makes the middle ear susceptible to ear infections. Younger children are at a higher risk because the eustachian tube is flat and this allows for more fluid to enter and remain in the middle ear. As the child grows the eustachian tube begins to move to a more vertical position and thus the potential for ear infections decreases. The eustachian tube is a pressure equalizer; its job is to ensure that there is the same pressure on both sides of the eardrum.
There are many disorders/diseases associated with the middle ear. The most common is an ear infection (otitis media) which we will discuss in detail in a later section. Below is a description of some of the other middle ear diseases/disorders.
Mastoiditis: This is a bacterial infection that affects the mastoid process. This is a bone located behind the ear. This infection occurs when acute otitis media has not been treated (or treated correctly) and the infection spreads to the mastoid process.

Page
15
Eardrum Perforation: A hole in the eardrum. This perforation can be caused my middle ear infections, a change in air pressure (Barotruama) or objects being placed in the ear such as Q-tips.
Barotrauma: This is damage to the middle ear due to unequal air pressure on both sides of the eardrum. We experience this when we are taking off or landing in an airplane. The eustachian tube helps to maintain equal air pressure to prevent any damage to the middle ear however if the eustachian tube is blocked it is unable to do its job.
Otosclerosis: The abnormal growth of bone of the middle ear which prevents the ossicles from working properly and causes hearing loss.
Infectious Myringitis: An infection of the eardrum by a virus or bacteria.
Temporal This bone is part of the skull that contains a Bone Fracture: portion of the ear canal as well as the middle and
inner ears. A fracture occurs when there has been a significant blow to the head. The fracture can rupture the eardrum and may damage the ossicles and/or cochlea.
Tinnitus: A noise (typically a ringing or buzzing sound) that is coming from in the ear rather than in the environment. It can be a symptom of damage to the ear, an ear infection, blockage of the eustachian tube or hearing loss.
The inner ear is the third part of the hearing pathway. It consists of a maze or labyrinth of fluid filled tubes that run through the temporal bone of the skull. There are two labyrinths the bony labyrinth and membranous labyrinth. It is the membranous labyrinth that contains the hearing cells which are called the hair cells of the organ of corti.
The bony labyrinth has three main sections. The first is the cochlea which looks like a snail. The cochlea is responsible for hearing. The second section is the semicircular canals which aid in maintaining balance. Between these two sections is the vestibule which houses the sense organs that are responsible for balance (the utricle and saccule).

Page
16
The fluid of the inner ear is set into motion when the oval window begins to vibrate which is caused by the vibration of the stapes (the third ossicle in the middle ear). There is also a round window which acts as a pressure valve. The nerve impulses that are generated in the inner ear travel along the vestibulocochlear nerve which leads to the brain for interpretation.
Diseases of the inner ear include:Meniere’s disease: This is characterized by recurring attacks of
vertigo (dizziness), hearing loss and tinnitus (ringing in the ear). It is thought to be caused by an imbalance of the fluid that is present in the inner ear.
Auditory Nerve Tumor: A noncancerous tumor that originates in the cells that surround the auditory nerve.
The brain is the fourth part in the hearing pathway. It interprets the information sent by the eighth cranial nerve also known as the vestibulocochlear nerve. This nerve has two parts; the cochlear nerve and vestibular nerve. The cochlear nerve transmits information about hearing while the vestibular nerve transmits information about balance. The brain then interprets the information and we hear.
People may experience an Auditory Processing Disorder (APB). A person with ABP has normal hearing acuity but has difficulty processing this information. This may be due to a problem with the 8th
cranial nerve or the portions in the brain associated with hearing.
A quick recap of the hearing pathway1) The outer ear collects and directs sound toward the ear canal. 2) The ear canal channels sound to the eardrum3) The eardrum vibrates causing the ossicles of the middle ear to
vibrate in succession4) The stirrup causes the oval window to vibrate which sets the
cochlea into motion creating electrical impulses 5) These impulses move up the 8th cranial never to the brain for
interpretation6) The brain interprets the impulses and we hear!

Page
17
Otitis Media (Ear infection)It has been said that 75%-80% of children will experience at least one ear infection before their third birthday, whereas 50% will have three or more ear infections during these first three years. Children who had their first ear infection before six months of age are at a higher risk for recurring ear infections (until the age of five). Otitis media is very common and while some discount the severity of this disease because of its common occurrence we must remember that the critical period for language development is from birth to four years of age and that ear infections often diminish a child’s hearing acuity.
So what is Otitis Media? Well, it is an infection or inflammation of the middle ear. Often they are brought on by sore throats, colds or other respiratory problems that have spread to the middle ear.
There are four types of Otitis Media, they are:Acute Otitis Media This typically starts quick but
doesn’t last long. Fluid is present in the middle ear.
Otitis Media without effusion An inflammation of the middle ear without fluid being present.
Otitis Media with effusion While there is fluid in the middle ear but there are no signs or symptoms of an ear infection. This can also be referred to as Serous Otitis Media
Chronic Otitis Media When the ear infection lasts for a great deal of time (at least a month). This causes continuous damage to the middle ear and eardrum.

Page
18
What are the symptoms of acute otitis media? Typically the child will complain of pain in the ear, if your child complains that their ear hurts this may be a sign of an ear infection. However, below you will find other symptoms of otitis media. They include:
runny or stuffy nose, cough fever drainage of pus or fluid from the ear dizziness or a loss of balance irritability (crankier than usual) signs of hearing difficulty such as missing quiet sounds or
wanting the TV volume very loudWhile the most common symptom is ear pain, some children are too young to tell you their ear hurts with their words so they will try to show you. Here are some additional signs to watch for that may indicate an ear infection is present (the signs above apply to very young children as well):
Tugging or pulling at their ear Sticking their finger in their era Crying more than usual Trouble sleeping
Why are young children more at risk?Children between the ages of 6 and 18 months are at the highest risk though ear infections are common up to the third birthday. There are several factors that make this group highly susceptible to ear infections.
Children, especially young children, have more difficulty fighting infection as their immune systems are still developing. Thus they are more likely to get respiratory or other infections that can lead to an ear infection.
The Eustachian tube is more horizontal in young children (and shorter) this allows bacteria and viruses easier access to the middle ear than older children and adults. The Eustachian tube may be blocked and thus is unable to ventilate the middle ear. This allows fluid to build up in the middle ear which leads to an ear infection.
Children have large adenoids. Adenoids help fight infection but because of their position in the upper part of the throat they may affect the Eustachian tubes ability to open. In addition, they may become infected and this infection will spread to the Eustachian tube and thus the middle ear.

Page
19
The child may be fighting off an infection in the middle ear. This leads to a collection of white blood cells who not only kill the bacteria but die themselves. This leads to a thick yellow-white fluid in the middle ear (pus) and thus an ear infection.
How is otitis media diagnosed?Your pediatrician will examine the child’s ear canal and ear drum with a device called and otoscope (an illuminated magnifying glass that fits in the ear canal). They are looking for redness and fluid (or pus) behind the eardrum. They will also look for eardrum perforations.
They may also want to determine how well the eardrum moves in response to air pressure. They can use a special otoscope called a pneumatic otoscope that blows a puff of air onto the eardrum to test for movement. They may want to complete tympanometry (described in the evaluation section), a hearing screening or acoustic reflectometry which determines if there is fluid in the middle ear based on how sound waves are reflected off the eardrum.
How is otitis media treated?Typically antibiotics are prescribed. Amoxicillin is a common antibiotic though about 10% of children do not respond to this antibiotic and an alternative must be chosen. Even after the course of antibiotics has been completed 40% of children have some fluid remaining in the middle ear which can impact their hearing for 3 to 6 weeks. However, this fluid eventually disappears on its own (in most children). If pain is present a pain reliever may also be prescribed or recommended.
Antihistamines or decongestants may help the underlying cause of the ear infection but they do not help the ear infection itself and thus are not a recommended treatment option in most cases.If this fluid remains for more than 3 months and is impacting the child’s hearing the pediatrician may recommend the insertion of PE tubes (Pressure Equalizing). The procedure is called a myringotomy and is done on an outpatient basis. The surgeon makes a small hole in the middle ear and inserts a tube so that this hole remains in the eardrum. This tube may remain in the eardrum for 6 to 12 months and generally comes out on its own.
Some will recommend the removal of the tonsils and or adenoids. Removal of the adenoids has been shown to reduce the number of ear infections in some children but not in children under the age of 4. Removal of the tonsils has shown no impact on the number of ear infections.
Can you prevent otitis media?

Page
20
The simple answer is no. Just as you cannot prevent a cold you cannot prevent an ear infection. However, there are some things you can do to reduce your child’s chances of getting an ear infection.
If your child is in a large daycare setting (10 or more children) and has had frequent ear infections described as more than 3 in a six month period or more than four in a 12 month period. They may benefit from a move to a setting with less children as this reduces their risk of catching a cold which may lead to an ear infection.
Avoid exposure to second hand smoke. Researchers say that children who are exposed to cigarette smoke during the first three years of life have almost double the risk of frequent or persistent ear infections. Even if you are not smoking around your child, "The tobacco smoke remains in the parent's clothing, remains on the parent's breath," says Dr. Wendell Todd, a pediatrician. "So the child is exposed to some even though the actual smoking is happening in a separate place." (taken from the CNN website)
Receiving the annual flu vaccine for children over six months of age is recommended. Being immunized has been shown to reduce the incidence of ear infections by almost one-third. There is a new infant pneumococcal conjugate vaccine which will also be helpful in reducing the likelihood of ear infections in young infants.
What if otitis media isn’t treated?Generally, otitis media causes temporary hearing loss. The child’s hearing is restored with the infection has cleared. However, if left untreated an ear infection may lead to permanent hearing loss. Ear infections commonly occur during the critical time for speech and language development, this loss of hearing may lead to speech and language disabilities and possibly learning difficulties as well.
In addition, the infection may worsen or travel to other parts of the head including the brain. Otitis media can cause severe pain and other serious complications. If you have any concerns that your child may have an ear infection please visit your pediatrician.
There is a device called the EarCheck Middle Ear monitor. This is a device you use at home that tells you if there is fluid in the middle ear and can be used as early as 6 months of age. While nothing replaces the pediatrician this may help in determining when to take your child in. It has mixed reviews so use your best judgment and remember ear infections do not always have fluid present so for those ear infections this device would not be helpful.

Page
21
Noise Induced Hearing LossNoise induced hearing loss occurs when there is damage to a child’s hearing due to exposure to loud noises. Typically this loss occurs gradually as the child is exposed to loud noise over a period of time. However, it can occur suddenly if they are exposed to an extremely loud sound. For example, being near an explosion would immediately cause a hearing loss.
So, how loud is too loud? Research shows that a person who is exposed to noise levels at 85 decibels or higher for a prolonged period of time is at risk for hearing loss. Let’s look at how loud common things are:
A normal conversation 60 decibels A lawnmower 90 decibels An MP3 player 105 decibels (at max level) A car horn and rock concert 110 decibels A firecracker 140 decibels
How can I tell if something is too loud? A good general rule is that if you have to raise your voice to be heard by someone else the noise around you (stereo, etc) is at 85 decibels or higher!
Of course you also have to take into consideration how close you are to the sound. Watching firecrackers, for example, doesn’t give you the full 140 decibels as you are a great distance from the actual source of the sound. However, MP3 players, most of which use ear buds that sit inside your ear are delivering the full 105 decibels to your ears.
The length of time also has an impact. Eight hours of 90-dB sound can cause damage to your hearing. Exposure to 100 decibels should be limited to no more than 15 minutes while regular exposure of more than 1 minute at 110 decibels risks permanent hearing loss (think of those iPods). If you have any exposure to 140-dB sound it causes immediate damage and actual pain.
When asked to think of who is most at risk for noise induced hearing loss, typically we think of the teenager who is listening to their iPod and we can hear it standing next to them or the car stereo we can hear in our car – two cars away. Some think of people love to go to rock concerts and who always sit in the front row. While others think of

Page
22
farmers or factory workers who work around loud machines. However, one does not generally think of a child playing with their toys.
Toys can cause noise induced hearing loss as well. Some toy sirens and squeaky rubber toys have a sound that is around 90 decibels whereas your vacuum cleaner runs at 70 decibels. One must also consider the distance from the ear. Children often hold toys directly up to their ear which can raise the decibel level. Some toys held up to the ear expose the child to 120 decibels – the same level as a jet plane taking off. These levels can cause pain and permanent hearing loss.
So what can you do? Inspect the toys sound level. If is sounds loud to you then it probably isn’t the best choice for your child’s hearing. If your child is likely to place the toy up to the ear, then listen to the toy with it up to your ear to determine if it is too loud at this distance. Remember, their hearing is more sensitive than yours so if you have any concern about how loud the toy is…it is probably too loud. If a toy you already have is too loud you may want to take out the batteries or check for loudness level buttons (which are on many toys) that allow you to soften the sound of the toy.
Several MP3 players come with a volume control so you are not able to listen at max level. Wear earplugs if you are going to be somewhere you know will be loud (a concert, 4th of July fireworks, etc.) and turn it down, make sure when you watch TV or listen to the stereo you can also talk to someone else without having to raise your voice, especially in the car where the sound is more contained.
So what can you do? Inspect the toys sound level. If is sounds loud to you then it probably isn’t the best choice for your child’s hearing. If your child is likely to place the toy up to the ear, then listen to the toy with it up to your ear to determine if it is too loud at this distance. Remember, their hearing is more sensitive than yours so if you have any concern about how loud the toy is…it is probably too loud. If a toy you already have is too loud you may want to take out the batteries or check for loudness level buttons (which are on many toys) that allow you to soften the sound of the toy.
This is a good habit to get into and to teach your child as they mature and enter the world of MP3 players and loud movies, video games, concerts…the list goes on and on. Teach them how to determine if something is too loud. Their ears will thank you later!
Treatment for Hearing Loss

Page
23
There are many types of treatment for hearing loss ranging from simple medical intervention to extensive surgery. They type of treatment depends on the type and degree of the loss. For example if the hearing loss is due to a foreign object in the ear canal the doctor can remove this object restoring the hearing pathway.
The most common type of treatment for hearing loss is a hearing aid. There are several styles of hearing aids all of which have pros and cons. You and your audiologist will determine the style that is best for you child depending on age, type and degree of loss and other factor such as the use of assistive listening devices (FM systems).
The most common type of hearing aid for children is called “Behind the Ear” or BTE hearing aids. This has a plastic case that is worn behind the ear that houses the electronics of the unit. Then in a traditional BTE there is an ear mold that fits inside the outer ear. In an attempt to make these more desirable to the child, many Audiologists will offer a variety of colors and/or designs for the ear mold. Thus the child can have purple ear molds that have glitter in them or tie die molds, etc. A newer type of BTE has the case behind the ear but the ear mold has been removed and a tube is inserted into the canal which some prefer as they are less obvious. These aids can be used with any level of loss and with a person of any age.
The second type is called “In he Ear” or ITE hearing aids. These aids fit completely inside the outer ear. They are more desirable than the BTE for teenagers and young adults as they are much less obvious. Typically these are not worn by young children because as the child grows the casting (mold) of the hearing aid would have to be replaced. This would occur often as the aid needs to fit securely in the ear canal.The third type is called “In the Canal” or ITC and “Completely in the Canal” or CIC. These aids are housed in the ear canal. The main difference is that you can see a little of the ITC whereas the ICI is completely hidden from view. These are good for adults and older teenagers with mild to moderate loss. Their small size limits the power and volume as well s the ability for additional hardware such as a telecoil.
A telecoil is a small coil that allows people to receive sound through the circuitry of the hearing aid rather than the microphone. Many public facilities have sound systems called Induction Loop systems these telecoils help people hear in places that have this system.
FM SystemsAn FM system is often used in the classroom to help minimize distracting background noise such as kids moving around, the air

Page
24
conditioner turning on, etc. They also help maintain a consistent loudness level in regards to the teacher’s voice. The teacher may walk around the room, turn to write on the chalkboard, etc. these movements change the loudness level of his/her voice. These things cause difficulties with hearing and understanding.
An FM system transmits the teacher’s voice directly to the child at a consistent level. The teacher wears a microphone and transmitter. This transmitter sends a signal directly to the child who is wearing a receiver. These work well with the Behind the Ear hearing aids.
There are a variety of FM systems that can be used in the classroom. The teacher, school personnel, audiologist, the child and parents should work together to choose the system that would work best in this child’s situation.
Cochlear ImplantsFor those with severe to profound hearing loss that cannot benefit from the use of hearing aids there is an option called a cochlear implant. This is a small electronic device that consists of an external and internal portion. The internal portion is implanted under the skin just behind the ear. The external portion attaches to the internal portion though magnets. A cochlear implant directly stimulates the auditory nerve and the impulses generated by the implant are sent to the brain who interprets these impulses. It doesn’t sound like normal hearing and it takes time to adjust and learn how to use this device thus speech therapy is vital to the use of a cochlear implant. However, with appropriate therapy the person can learn to “hear” fairly well with the implant. The FDA has approved implants for children as young as 12 months of age which allows them to have access to speech and language during the critical period for development. The cochlear implant is something that should be discussed with the child’s audiologist and implant specialist, etc. to determine if this is the right choice for you and your child.
Speech-Language TherapyNo matter what method is chosen to aid your child’s hearing they may benefit from speech-language therapy. These benefits range from articulation therapy to help them learn to distinguish the sounds they have been missing and how to accurately produce these sounds to language therapy to help them acquire language skills that may be delayed due to their hearing loss. After your child has been fitted for aids it is a good idea to have an evaluation completed by a Speech Pathologist to determine if they can help the child acquire delayed skills. Again remember that you may not realize what coping behaviors your child is using to get around language delays so even if

Page
25
you think their language skills are fine, it is not a bad idea to have their speech-language skills evaluated. Even if the Speech Pathologist does not recommend therapy, they can provide tips and strategies for you to use at home.
The Effects of Hearing LossThere are four main ways hearing loss effects a child’s development. The first is vocabulary. A child who is experiencing a hearing loss acquires vocabulary at a slower rate. In addition, they have difficulties with certain types of vocabulary such as multiple meaning words, abstract words (such as jealous) and function words such as “the” or “a”. Their strength tends to lie in learning concrete words such as;

Page
26
dog, run, ten, blue. The vocabulary gap between a child with a hearing loss and a child with normal hearing only increases with age.
The second is sentence structure. Children who experience a hearing loss tend to understand and use sentences that are simpler and shorter than those of children with normal hearing. These children also experience difficulty with complex sentences such as passive voice sentences. They may miss important parts of words such as word ending (the plural “s” for example) and thus have trouble with things like verb tense, possessives, plurals, etc.
The third affect of hearing loss on a child’s development is their articulation skills. Children with a hearing loss may not be able to hear the quieter speech sounds such as /s/, /f/, /t/, /k/ and “sh” thus they do not produce them. This leads to speech that is difficult to understand. In addition to their articulation development, their speech may also be impacted by their loudness level; they might speak very loudly or very quietly and may sound like they are mumbling as they are missing the cues that help us learn appropriate intonation and rate of speech.
All academic areas are impacted though reading and math seem to be the areas where the most difficulty is experienced. Even if the loss is mild or moderate a child can be performing one to four grade levels below their normal hearing peers (without intervention). Children who experience a severe or profound loss may not achieve skills higher than the third or fourth grade level without early intervention.
Finally, a child’s social skills are affects as they may find it difficult to interact with their peers. Even if the loss is mild, they may have to constantly ask for clarification (saying things like “huh” or “What?”) which may make them uncomfortable and may cause them or other children to limit interaction. Social issues may lead to the child feeling that they do not have any friends and may lead to them being unhappy in school.
Supporting your childThere are many things you can do to help your child cope with their hearing loss. They are going to need your help and support to manage with this hearing loss. It doesn’t matter if the loss was present at birth or if they acquired it later in childhood. Below are some general ways to help as well as some ways to aid in communication.
Understanding the facts Learn as much as you can about your child’s hearing loss. You are the child’s best advocate so the more you know about the

Page
27
loss the better equipped you are to work with your child’s school and teacher to ensure your child’s success in school.
Be Patient Things may come slower for your child. Help them work at their page in order to build self-confidence. They can do it!
Pay Attention Stay involved in the child’s day to day activities. Your interest may prevent them from feeling isolated.
Encourage Friendships They may need a little help to strike up a friendship but this should get easier with practice. Find ways to interact with other children with a hearing loss as well as children with normal hearing. Identifying/interacting with others may help the child feel part of a group which will help their self-esteem.
Learn about the aid If your child uses a hearing aid or cochlear implant learn about how to take care of it and do it together. Don’t take this responsibility for the child. Even if they are very young there is something they can do to help take care of their hearing aid.
Keep sentences short We all ramble on at times. For children with a hearing loss this is particularly daunting as they are working harder to hear as well as trying to figure out the important parts of your sentence. Try to use short, clear sentences.
Slow down Talk slower and clearer. Do not yell – the hearing aid’s job is to amplify sound not the speakers (remind friends and family of this as well). Try not to rush through your sentence but say each word as an individual word. For example, on a TV show the following dialog took place:
Actor A) I have 1 word for you, “letitgo”
Actor B) That’s three wordsActor A) Not the way I say it

Page
28
Make sure to include that tiny break between words.
Try alternative words If you can sense your child did not understand you, try another word that means the same thing or rephrase the sentence to explain it a different way. You are not only helping the child understand but are helping to teach them new vocabulary. If they didn’t know the word before you are helping them assign meaning to this word.
Help in groups Sometimes in group situations such as at dinner time. More than one person may be talking at a time and there may be competing background noise. If your child seems lost or confused help them by giving them quick explanations.
Be Affectionate Tell your child that you love them for who they are – let them know that being different makes them special.
Resources/References
http://www.hearingaidscentral.com/Diseases_and_Disorders_of_the_Middle_ear.asp
http://www.merck.com/mmhe/sec19/ch220/ch220h.html
http://webschoolsolutions.com/patts/systems/ear.htm
http://www.medicinenet.com/script/main/art.asp?articlekey=21685
http://www.nidcd.nih.gov/health/hearing/hearingaid.htm#10

Page
29
http://www.boystownhospital.org/Hearing/info/understanding.asp
http://www.asha.org/public/hearing/disorders/causes.htm
http://www.medicinenet.com/detecting_hearing_loss_in_children/article.htm
http://www.babyhearing.org/HearingAmplification/HearingLoss/audiogram.asp