Embed Size (px)
Citation preview
Matthew Grissinger, RPh, FISMP, FASCPDirector, Error Reporting Programs
Institute for Safe Medication PracticesManager, Medication Safety AnalysisPennsylvania Patient Safety Authority
Aligning the Lines:An Analysis of IV Line Errors
1
Disclosure Statement
• Disclosure Statement – These individuals have nothing to disclose concerning possible financial or personal relationships with commercial entities (or their competitors) that may be referenced in this presentation. • Amanda Wollitz, PharmD• Matthew Grissinger, RPh, FISMP, FASCP
2
MethodologyInitial
Classification“DEV3”
Query Medication Errors
for “DEV3”
907 reports June 2004‐August
2013
Error Category Assigned
High‐Alert Evaluation
3
Methodology
• Greater than 20 categories of error were identified
• Facility provided– Event description– Medication name– Route– Patient care area– Harm score
4
Analysis
• Errors identified– IV setup– IV administration
• “Unknown” cause of error (6.9%, n = 63)• Most frequent errors
– Rate or line mix‐up (22.6%, n = 205)– IV lines not attached to patients (15.6%, n = 132)– Errors with piggyback infusions (12.8%, n = 116)
5
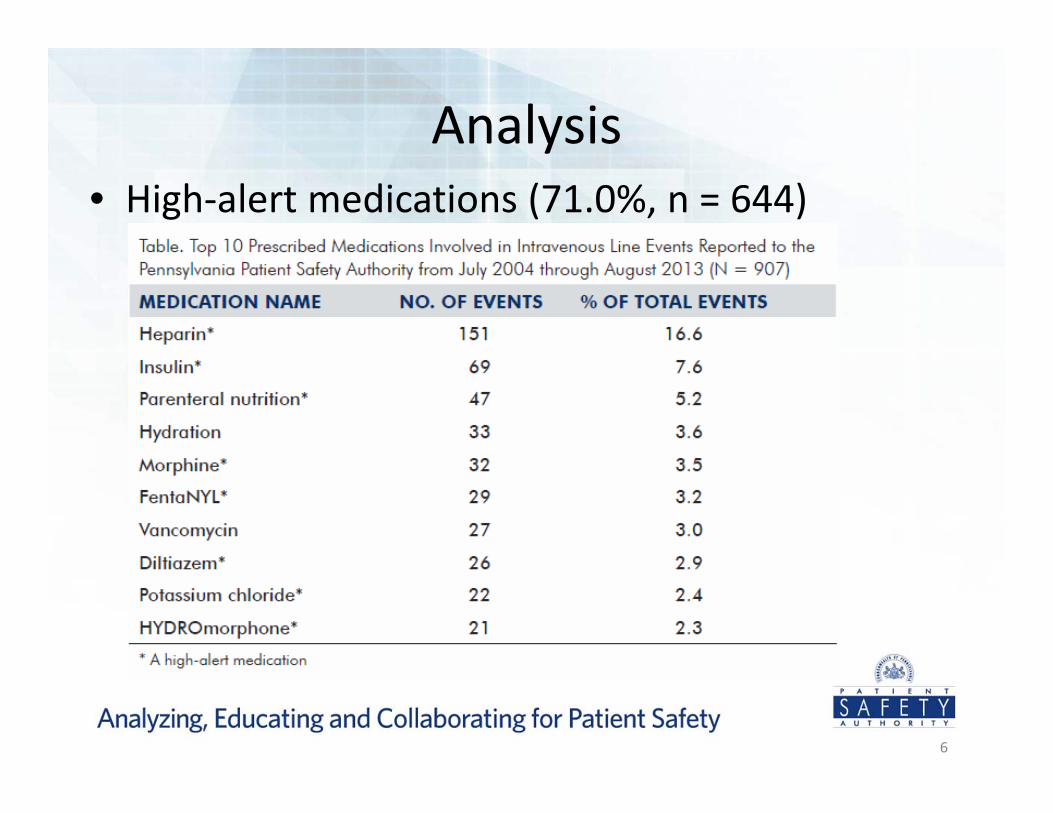
Analysis• High‐alert medications (71.0%, n = 644)
6
Analysis
• Patients less than 18 years (11.1%, n = 101)• Medical unit
– Intensive care (30.2%, n = 274)– Medical‐surgical (14.1%, n = 128)– Telemetry (6.6%, n = 60)
• Errors reached the patient (95.6%, n = 867)
7
Analysis
• IV line associated harm score– D or greater (48.1%, n = 436)– E or greater (6.2%, n = 56)
• Authority’s 2012 annual report (0.5%)• 12 times more than other medication errors
8
Rate or Line Mix‐Ups
• Most frequent event (22.6%, n = 205)– Rate mix‐up (9.5%, n = 86)– Line mix‐up (13.1%, n = 119)
• Heparin was most frequent medication for both subcategories
• What IV rates were most frequently interchanged?– Heparin switched with IV hydration (47.2%, n = 17)– Parenteral nutrition switched with intralipids (77.3%, n = 17)
– Insulin switched with IV hydration (70.0%, n = 7)
9
Rate of Line Mix‐up• A patient with nitroglycerin and heparin infusions complained of a headache.
• The nitroglycerin was ordered to infuse at 1.5 mL/hr, and the heparin was ordered to infuse at 30 mL/hr.
• The pump was set correctly, but the lines were crossed and the nitroglycerin was infusing at 30 mL/hr and heparin was infusing at 1.5 mL/hr.
10
Rate of Line Mix‐up• A patient was on an insulin drip at 5 mL/hr and a maintenance IV at 100 mL/hr.
• While changing the patient’s gown, the IVs were switched and the patient received the insulin drip at 100 mL/hr, or 20 units/hr for approximately two hours.
• [By late morning,] the BS [blood sugar] was less than 35 [mg/dL], so the insulin drip was turned off, which was when the error was discovered.
11
IV Line Not Attached to Patient
• Second most common event type• Unattached lines (14.6%, n = 132)• High‐alert medications (66.7%, n = 88)
– Heparin (16.7%, n = 22)– Morphine (8.3%, n = 11)– Insulin (6.1%, n = 8)
12
IV Line Not Attached to Patient • Insulin gtt [drip] started as ordered for hyperglycemia. Two hours later, glucose was checked as ordered, and the result was greater than 400 [mg/dL].
• Upon assessment, noted tubing disconnected. • Physician notified and new orders received. Insulin bolus [was administered] and then gtt [started] at 4.5 units/hr.
13
IV Line Not Attached to Patient
• According to the RN supervisor, patient ordered norepinephrine (Levophed®) IV drip titrate to keep SBP [systolic blood pressure] >90.
• The patient had• an episode of hypotension, BP [blood pressure] = 68/36. House physician ordered IV NSS wide, Trendelenburg, 100% FIO2 [fraction of inspired oxygen].
• While assessing lines, found Levophed infusion disconnected, and the line was reconnected.
14
Piggyback Infusions
• Third most frequent event (12.8%, n = 116)• Heparin most common (10.3%, n = 12)• Error during setup process
– Connection below infusion pump– Secondary IV hung lower than primary IV– Piggyback clamped– Incorrect pump programming
15
Piggyback Infusions
• Heparin drip was running at 1,400 units/hr (14 mL/hr).
• A 4 g magnesium rider IV was piggybacked at 25 mL/hr; therefore, heparin drip ran at 25 mL/hr for over 30 minutes as rider had been clamped.
• Drip stopped [after] approximately 15 mL [heparin] went in.
• Physician notified and stated to restart drip and monitor for signs and symptoms of bleeding.
16
Piggyback Infusions
• IV insulin 100 units/100 mL was infused over approximately 1 hr.
• IV was connected at the wrong place, piggybacked below the pump. D50 [dextrose 50%] 25 mL was pushed slowly as per protocol.
17
Risk Reduction Strategies
• Set up infusions completely and one at a time• Administer high‐alert medications as primary infusions
• Utilize infusion sets with back‐check valves• Label lines• Restrict pump operation to qualified and credentialed personnel
• Place IV pumps and epidural pumps on opposite sides of the patient’s bed
• Raise awareness
18
Risk Reduction Strategies
• Set up infusions completely and one at a time– Handle one IV solution at a time when using multiple‐channel pumps
– Physically tracing the line can help ensure that the correct channel has been used to program the infusions
– Trace all lines back to their origin– Develop consistent process for IV medication setup
19
Risk Reduction Strategies
• Administer high‐alert medications as primary infusions– No other medications attached to the dedicated line– High alerts administered as secondary infusion could lead to errors
• Primary and secondary line confusion• Secondary infusion delay due to absence of alarm• Medication delay due to tubing volume• Increased risk of subsequent programming and setup errors
20
Risk Reduction Strategies
• Utilize infusion sets with back‐check valves– Pressure sensitive device to prevent flow from high pressure to low
– Backflow could result in administration of indeterminate amounts of each IV fluid
21
Risk Reduction Strategies
• Label lines– Medication name affixed to IV line
• End closest to patient• Above each channel on pump
• Restrict pump operation to qualified and credentialed personnel– Patient transfer– Include training and prohibitions on this task during orientation
22
Risk Reduction Strategies
• Place IV pumps and epidural pumps on opposite sides of patient’s bed– Wrong route has high potential for patient harm– Label pump “Epidural Only”
• Raise awareness– Reports reveal incidence and severity– Use information to raise staff awareness of prevalence of IV administration error
23
Conclusion
• Administration process responsible for nearly 50% of errors involving IV lines
• Difficult to determine cause due to practice variation for setup
• Patients and practitioners could benefit from standard guidelines
• Continued research necessary to identify causes and risk reduction strategies
24
ReferencesHicks RW, Cousins DD, Williams RL. Summary of information submitted to MEDMARXSM in the year 2002: the quest for quality. Rockville (MD): US Pharmacopeial Convention, Inc.; 2003. Husch M. Insights from the sharp end of intravenous medication errors: implications for infusion pump technology. Qual Saf Health Care 2005;14(2):80‐6. Vanderveen T. Averting highest‐risk errors is first priority [online]. Patient Saf Qual Healthc 2005 [cited 2013 Nov 8]. http:// www.psqh.com/mayjun05/averting.html Cassano‐Piché A, Fan M, Sabovitch S, et al. Multiple intravenous infusions phase 1b: practice and training scan [online]. 2012 May [cited 2013 Nov 8]. http://www.hqontario.ca/en/eds/tech/ pdfs/2012/multipleinfusions1b_May.pdf Institute for Safe Medication Practices. ISMP’s list of high‐alert medications [online]. 2012 [cited 2013 Nov 11]. http://www.ismp.org/Tools/institutional highAlert.asp National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP). NCC MERP index for categorizing medication errors [online]. 2001 [cited 2013 Nov 16]. http://www. nccmerp.org/medErrorCatIndex.html Pennsylvania Patient Safety Authority. Pennsylvania Patient Safety Authority 2012 annual report [online]. 2013 Apr [cited 2014 Jan 8]. http://www.patient safetyauthority.org/PatientSafety Authority/Documents/Annual%20 Report%202012%20.pdf Cohen MR. Preventing medication errors related to drug delivery devices. Chapter 12. In: Cohen MR, ed. Medication errors. 2nd ed. Washington (DC): American Pharmacist Association; 2007:278. Joint Commission. Tubing misconnections—a persistent and potentially deadly occurrence [online]. Sentinel Event Alert 2006 Apr 3 [cited 2014 Jan 31]. http:// www.jointcommission.org/assets/1/18/ SEA_36.PDF Health Technology Safety Research Team, Institute for Safe Medication Practices Canada. Mitigating the risks associated with multiple IV infusions: recommendations based on a field study of twelve Ontario hospitals [online]. 2012 [cited 2014 Jan 7]. http://www.aami.org/ htsi/infusion/wg/multiple/MultipleI VInfusions_Phase1bSummary_ Recommendations%20and%20Rationale_ June%202012.pdf Medication errors occurring in the radio‐logic services department. Pa Patient Saf Advis [online] 2009 Jun [cited 2013 Nov 27]. http://www.patientsafety authority.org/ADVISORIES/Advisory Library/2009/Jun6(2)/Pages/46.aspx Institute for Safe Medication Practices. Problems persist with life‐threatening tubing misconnections. ISMP Med Saf Alert Acute Care 2004 Jun 17;9(12):1‐2. Institute for Safe Medication Practices IV potassium given epidurally: getting to the “route” of the problem. ISMP Med Saf Alert Acute Care 2006 Apr 6;11(7):1‐2.
25





























