Embed Size (px)
Citation preview
Alice Moseley, Graham Smith & Gerry StokerDepartment of Politics & International Relations University of Southampton, Rediscovering the Civic Project, Universities of Manchester & Southampton
UK Surveys report 65%-90% in favour of donating
their organs (New et al 2004)
Yet only 26% on ODR (NHSBT, 2009)
8000 people waiting for a transplant
1000 people died waiting in 07/08
50% more organs are needed
Gradual increase in donors but gap between supply
and demand growing faster (8% per year) (DH, 2008)
Repertoire of policy tools based around behavioural
economics principles (Thaler & Sunstein, 2008)
Heuristics: Cognitive limitations so shortcuts, rules of
thumb, eg following the herd or status quo
Loss aversion: We care more about losses than potential
gains
Hyperbolic discounting: Calculations that are in our
short term but not our long terms interests – ‘Buy now, pay
later!’
Yet preferences are constructed not fixed so amenable to
govt influence
Govts use nudges to encourage behavioural change (by
taking on role of ‘choice architect’)
Eg Changing defaults: recognises status quo bias within
decision-making
Eg Information provision: Enabling people to make more
informed choices
Organ Donation…. From informed consent to
presumed consent? Or mandated choice? Changing
defaults
Information nudges
Rather than nudging citizens, government
merely provides opportunities for them to think
Deliberation, dialogue, debate, peer education
Deliberative turn in democratic theory &
practice
Focus on collective rather than individual
behaviour Organ Donation…. Educative effect of discussing and debating.. Lack of awareness one of biggest obstacles…
Research Qs How effective is information provision
alone compared to information & deliberation for increasing ODR?
How does information and deliberation affect attitudes towards ODR?
Methodology Post-test only RCT amongst HE students Data collection via survey administered in
lecture theatres
Control group: Questionnaire only
Treatment Group A: Information + (NUDGE) Questionnaire
Treatment Group B: Information + Dialogue (NUDGE & THINK) + Questionnaire
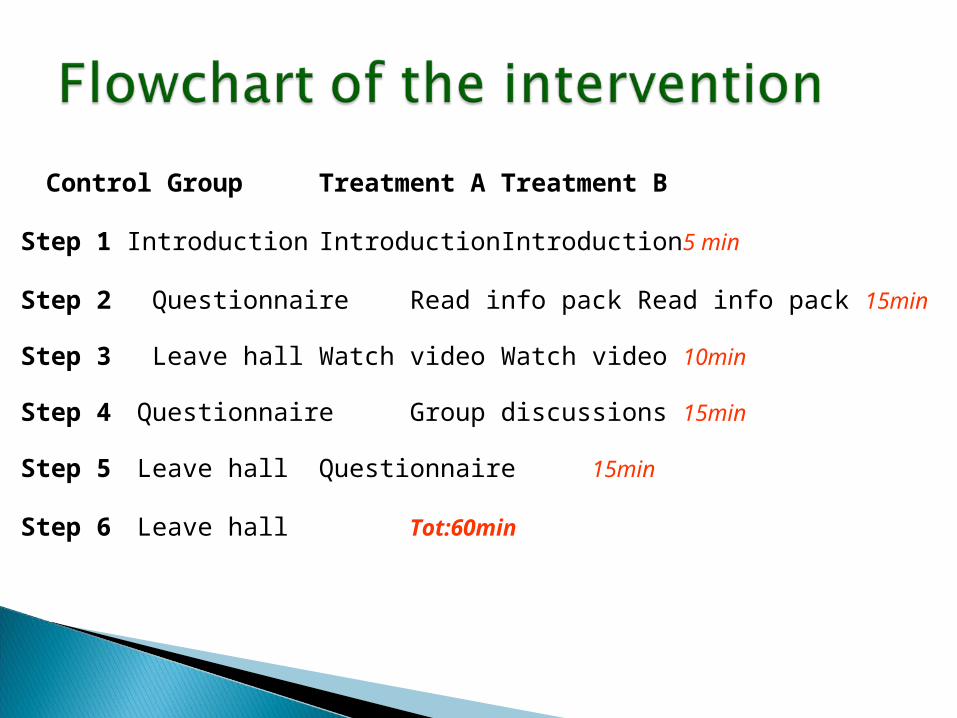
Control Group Treatment ATreatment B
Step 1 Introduction Introduction Introduction 5 min
Step 2 Questionnaire Read info pack Read info pack15min
Step 3 Leave hall Watch video Watch video 10min
Step 4 Questionnaire Group discussions 15min
Step 5 Leave hall Questionnaire 15min
Step 6 Leave hall Tot:60min
Dependent on gatekeepers
Permission to link study to actual
registration
Non-attendance
Student sample: external validity
Fresher’s Fair contamination
Research Qs How do informed consent (opt in), presumed
consent (opt out) and mandated choice questions impact on ODR?
How acceptable do participants find these alternative systems?
Methodology Post test only RCT amongst HE students Data collected via online survey
Group 1: INFORMED CONSENT/ OPT IN (Status quo)
Group 2: PRESUMED CONSENT/(NUDGE 1) OPT OUT (Alternative A)Group 3: FORCED CHOICE (NUDGE 2) (Alternative B)
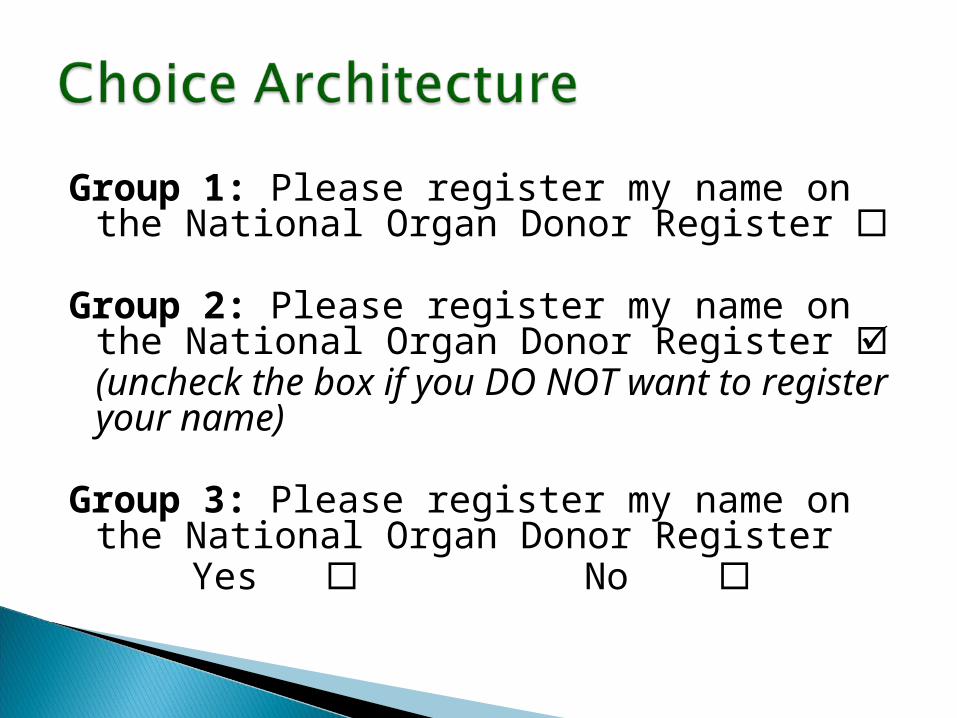
Group 1: Please register my name on the National Organ Donor Register
Group 2: Please register my name on the National Organ Donor Register (uncheck the box if you DO NOT want to register your name)
Group 3: Please register my name on the National Organ Donor Register
Yes No
Permission to link study to actual registration:
will provide opp. to retrospectively re-register
Student sample: external validity
Dealing with non-response/ self-selection bias
May not be possible to include all students:
again dependent on gatekeepers