Embed Size (px)
Citation preview

Algorithms and Testing Results for West Nile/Arbovirus Testing (2002) used at Michigan Department of Community Health
H. Kapoor, P. Clark, F. P. Downes, P. Somsel, R. Oesterle, M. Casey and D. Wilkinson Michigan Department of Community Health, Lansing
Abstract Michigan reported the second highest count of human cases of West Nile Virus (WNV) during the 2002 outbreak in the US. A total of 2910 human specimens, primarily cerebrospinal fluids and sera, were received from January 1 until December 31, 2002, of which 575 tested positive. The first confirmed human case of WNV was during the week of Aug 11, 2002 with the volume of requests increasing dramatically thereafter and reaching a peak of 333 per week. In response to an unanticipated volume of specimen submissions the Bureau of Laboratories (BOL) at Michigan Department of Community Health (MDCH) developed algorithms jointly with the Bureau of Epidemiology (BOE) using the CDC case definition and guidelines for WNV/Arbovirus testing. These emergent algorithms were shared with local health departments. The first line test utilized for diagnosis of WNV was the IgM-capture enzyme-linked immunosorbent assay (MAC-ELISA). A positive IgM on CSF was sufficient to establish a confirmed case of WNV. Other tests employed were IgG ELISA and Plaque Reduction Neutralization Test (PRNT). A four-fold rise in IgG titers in paired sera drawn in acute and convalescent stages (at least 22 days apart) distinguished a recently acquired infection from a past infection. To rule out the cross- reactions between WNV and other Arbovirus infections endemic in Michigan (SLE, EEE and CGV), antibody specificity was confirmed by PRNT. Communications of the positive results were expedited using electronic reporting to local health departments, submitters and the BOE.The testing algorithms adopted at BOL, MDCH and results of serological assays are presented.
Introduction The Michigan Department of Community Health (MDCH) started
conducting WNV surveillance in a cooperative plan with the Michigan Department of Agriculture (MDA), Michigan Department of Natural Resources (MDNR), Michigan State University (MSU) Animal Health Diagnostic Laboratory (AHDL) and Department of Entomology since 2000.
The group focused on collection and testing of dead crows and blue jays, beginning May through September of 2001. The surveillance resulted in the positive birds as well mosquito pools in Michigan. Though 159 human specimens were tested in a serologic panel for the arboviruses, which includes WNV, St. Louis encephalitis (SLE), Eastern equine encephalitis (EEE) and California group virus encephalitis (CGV), none was found positive for WNV during 2001.
The surveillance guidelines were revised for the year 2002, with the addition of a hot line and a web site for reporting of dead bird sightings. Reports to the hot line alone in 2002 totaled over 35,000 calls; 73 out of 83 participating counties in the state submitted birds, which tested positive, the first collected on May 14.
Requests for human specimen testing of arbovirus panel started rising from June, 2002 with the first laboratory confirmed case reported during the week of August 11, 2002.
Materials and methods
Specimens
Cerebrospinal fluid (CSF)CSF and Serum combinationSera- Acute and Convalescent (obtained 22 days post onset)Least preferred single serum sample
Laboratory TestsCapture enzyme-linked immunosorbent assay (MAC-ELISA-IgM).Capture enzyme-linked immunosorbent assay (MAC-ELISA-IgG) and Plaque Reduction Neutralization Test (PRNT)
Ref: Antibody Capture ELISA (IgM & IgG) Protocol. CDC Fort Collins, Colorado
CDC Neutralization Test Protocol. CDC Fort Collins, Colorado
Contact InformationHema Kapoor M.D.Virology Section Manager
Bureau of LaboratoriesMichigan Department of Community Healthphone: (517) 335-8099email: [email protected]
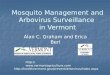
Weekly WNV Testing ( Aug-Nov)
55
94
240
266
319
270 270289
333
193
144
231
7055
422311 16 20 20
91
61 65
38 38
12 16 14 620
0
112
0
50
100
150
200
250
300
350
11-Aug
18-Aug
25-Aug
1-Sep 8-Sep 15-Sep
22-Sep
29-Sep
6-Oct 13-Oct
20-Oct
27-Oct
3-Nov 10-Nov
17-Nov
24-Nov
Weeks
Num
bers
total positive
Total Specimens (Jan, 02-Dec, 02)-2910
Results Three algorithms were developed depending upon
Algorithm-1 Algorithm-2 Algorithm-3
•CSF specimen received for testing.
• P/N ratio of 10 and above was considered a positive WNV.
•P/N between 2-10 was reported equivocal and requested for a serum sample.
•Paired sera ( Ac. & convalescent )
• P/N ratio of 5 and above was considered a presumptive WNV.
•P/N between 2-5 was reported equivocal.
•A four-fold rise in IgG titers in paired sera drawn in acute and convalescent stages (at least 22 days apart) was used to distinguish a recently acquired infection from a past infection.
•PRNT was performed on all specimens showing a four fold increase in IgG titer.
•Single serum sample received for testing.
• P/N ratio- same as in algorithm-2.
•A convalescent serum was requested on a specimen showing equivocal titers.
•To rule out the cross- reactions between WNV and other arbovirus infections (SLE, EEE and CGV), specificity of the antibody in the specimen was confirmed by PRNT.
MAC-ELISA IgM performed in singlet. Positive MAC-ELISA repeated in duplicate.
CSF at MDCH 0 day
IgM ELISA 1st Run
NotificationVia EPIC toSubmitter,
LDH & EPI 3-4 day
PosNegReport via
E PIC
InvestigationIgM ELISA 2nd Run
Confirmed positive reportsVia
EPIC 5-6day
pos
Quantity Sufficient
pos
Equivocal
Request a convalescent serum sample
QNS
To report a Probable case
request a serum sample
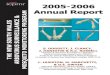
Interpretations for the Algorithm 11. CSF was the highest priority specimen at MDCH.2. If the result was negative, then the submitter and the local health department
were informed via EPIC, the lab reporting system
3. If the result was positive on the first run, then this was considered a Presumptive Positive and a notification was made to the to the submitter, local health department and the Bureau of Epidemiology.
4. If there was sufficient CSF, the EIA test was repeated in duplicate, and a repeat positive result was reported out via EPIC to the submitter and the local health department as a confirmed positive result. This would meet the case definition of a confirmed case of West Nile Virus encephalitis for surveillance purposes. If the test result is equivocal, a request was made for convalescent serum. This case would be classified as a probable case of West Nile Virus encephalitis.
5. If there was insufficient CSF for a repeat test, the result was reported out as QNS (quantity not sufficient) and a request was made from the submitter for a serum sample.
Algorithm 1
PRNT on pair
IgM ELISA 2nd Run
Slide 3
Report Via
EPIC
NegPos
4x rise in titer
YesNo
PRNT on acute serum (Convalescent sample not possible )
Convalescent serum
Confirmed positive reportsVia
EPIC
Pos
IgM ELISA 1st Run
Acute Serum at MDCH (0day)
Reported a presumptive positive (LAB) & probable case (EPI) Via EPIC with a request for a convalescent serum
Pos
Pos
Notificationvia Remedy to
LDH & EPI
Investigation
No 4x increase
Slide 3
Algorithm 2
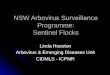
Interpretations for the algorithm 2
• Serum specimens did not receive priority unless they were accompanied by clinical information which suggested CNS involvement.
• If the IgM EIA result was negative, then the submitter and the local health department were informed via EPIC, the lab reporting system. These were classified as No Case.
• When the IgM EIA result was positive then this was a preliminary positive and was reported to the local health department to initiate an investigation. Please note this was only preliminary positive and not a confirmation. This test result was not characterized as positive for WNV at this stage. The serum was then retested in duplicate by EIA. If this was again positive, then the test result was considered a presumptive positive and the case could be classified as a Probable Case of West Nile Virus. The submitter and the local health department were notified of the result via EPIC. The submitter was asked to submit a convalescent serum, taken at least 22 days after the acute specimen.
• If a convalescent serum was not available then a Plaque Reduction Neutralization test (PRNT) was performed on the acute specimen. If specific neutralizing antibodies were detected, the test result was considered positive and the case was classified as a Confirmed Case of WNV.
• If a convalescent serum was available it was tested along with the acute serum in a PRNT and the titers compared. A four-fold increase in titer was evidence of a recent infection and the test result was reported as positive and the case considered a Confirmed Case of WNV. If a four fold increase in titer was not observed, but specific neutralizing antibodies detected, the test result was reported as positive and the case considered a confirmed case of WNV.
Single serum with Documented CNS symptoms or paired sera without 4 x increase in titer
IgM ELISA (+) PRNT (-)
No WNV CaseProbable WNV Case
Test for EEE and CGV
Neg
NoYes
Single serum collected too early
(0-8 d) after onset of symptoms
Paired sera
Yes
Algorithm 3
Interpretations for the algorithm 3• In a few cases there were situations where results were more difficult
to interpret. • A single serum sample from a patient who had documentation of CNS
symptoms, and who had a positive WNV IgM EIA and a negative WNV/SLE PRNT could have an encephalitis due to another flavivirus. The EIA could be positive because of the cross-reactivity that can occur with flaviviruses, whereas the PRNT is considerably more specific and can discriminate between the viruses.
• If the IgM and PRNT for EEE or the California group of encephalitic viruses (CGV) were positive, then the case could be reported and investigated as a EEE or other viral encephalitis.
• If the IgM & PRNT for EEE and CGV were negative, it might be that the serum was collected too early for the generation of sufficient IgG antibody to be detected in the plaque reduction neutralization test. If the serum was collected within 8 days of symptom onset the case was classified as a Probable case of WNV.
• If the serum was collected more than 8 days after the onset of symptoms, the test result would not be considered positive and the case was classified as not a Case.
ConclusionsWe found these algorithms to be a handy tool for use by laboratory personnel, especially during the initial phases of WNV outbreak when the laboratory was overwhelmed with clinical specimens.We had an easy and useful way of communicating
laboratory results to the Epidemiologists, Local Health Departments and the submitters engaged in the investigation
of the outbreak using these algorithms.
AcknowledgementsWe wish to acknowledge the CDC for ELC (Epi/ Lab Cooperative agreement) grants (regular and supplemental #U50/CCU514403-05-2 and the following organizations and their staff who helped in completing the Arbovirus testing for this outbreak. MDCH Bureau of Laboratories. MDCH Bureau of Epidemiology. Michigan Department of Agriculture. Michigan Department of Natural Resources. Michigan State University Animal Health Diagnostic Laboratory and Department of Entomology.
















![Odrl downes-prez.ppt [repaired]](https://img.pdfslide.us/doc/110x75/58738b8d1a28ab272d8b6b95/odrl-downes-prezppt-repaired.jpg)