Embed Size (px)
Citation preview

© 2020 Indian Journal of Ophthalmology | Published by Wolters Kluwer - Medknow
Algorithmic approach to diagnosis and management of post-refractive surgery dry eye disease
Sharon D’Souza, Edwin James1, Rishi Swarup2, Sheetal Mahuvakar3, Aditya Pradhan4, Krati Gupta
Access this article onlineWebsite: www.ijo.inDOI: 10.4103/ijo.IJO_1957_20PMID: *****
Quick Response Code:
Dryeyedisease(DED)isaconditionthatisfastreachingepidemicproportionsaroundtheworld.Dryeyepost-refractivesurgeryistheleadingcauseofiatrogenicallyinducedDED.Thewidevarietyofpresentationsandthedisparitybetweensignsandsymptomsinmanypatientsmakethisaverychallengingaspectofour clinicalpractice.Therehasbeen aparadigmshift in thewayweapproachand treat this condition.TheInternationalDryeyeworkshophasaddednewknowledgeandfocustoourmanagementofdryeye.AwiderangeofnewerdiagnosticmodalitiesareavailableforthediagnosisofDED.Dryeyeisoneofthemostcommonsideeffectsofrefractivesurgeryandcanhaveabearingthepatient’sperceptionofsurgicaloutcomesaswell.Athoroughunderstandingofthepossibleunderlyingetiopathologiesofthisdiseaseandthedifferenceinetiopathogenesisofpostrefractivedryeyeisessentialforoptimaloutcomes.Itisimportanttoapproacheachcaseinauniquefashionandcustomizethetherapytothepatientpresentation.Thisreviewarticlecompilesalltheseaspectsofmanagementofdryeyeingeneral,andpostrefractivesurgerydryeyeinparticular;fromtheonescommonlypracticedintheclinictothenewermodalitiesoftherapywithinsightsintothediseasefromamorepracticalpointofview.
Key words:Algorithm,dryeye,management,postrefractive
Department of Cornea and Refractive, NarayanaNethralaya,Bangalore,Karnataka,1DepartmentofOphthalmology,GovernmentMedicalCollege,Paripally,Kerala,2DirectorandConsultantCornea,CataractandRefractive,SwarupEyeCentre,Hyderabad,Telangana,3Consultant Cataract Cornea and Refractive Surgery, RetinaFoundation,Ahmedabad,Gujarat, 4ConsultantCataract, CorneaandExternalDisease,Disha EyeHospital, Barrakpore,Kolkata,WestBengal,India
Correspondenceto:Dr.SharonD’Souza,ConsultantCornea,OcularSurface andRefractiveDepartment,NarayanaNethralaya, 121/c,ChordRoad,Rajajinagar, Bangalore - 560 010,Karnataka, India.E-mail:[email protected]
Received:14-Jun-2020 Revision:14-Sep-2020Accepted:02-Oct-2020 Published:23-Nov-2020
Dryeyedisease(DED)isoneoftheleadingcausesofocularmorbidity in theworldwith increasingnumber ofpeoplesuffering fromdry eye-related complaints.[1] It is known to have a variety of presenting symptoms and signs with underlyingocular surfacepathologies, hence it’sdiagnosisandmanagement can be challenging for the treatingophthalmologist.[2]DEDcanalsobeiatrogenic,secondarytomedical and surgical interventions like systemicor topicalmedications, contact lensusage, andpostsurgery includingrefractivesurgery.[3]Refractivesurgeryhasgainedimmensepopularityworld-wide,withmorethan16millionproceduresperformed globally,[4,5] and dry eye is one of the most commonlyreportedsideeffectoftheseprocedures.[6,7] Dry eye postrefractivesurgerycanalsoimpactthepostoperativequalityofvisionandqualityoflife[4]andthereforeneedsparticularattentionandcare.[8,9]
The2017InternationalDryEyeWorkshopII(DEWSII)reportalsodefineddryeyeasamultifactorialdiseaseandhighlightedtheimportanceofocularsurfaceinflammation,neurosensoryabnormalitiesandlossofhomeostasisinthiscondition.[10] An importantadditioninthisreportTFOSDEWSIIistheconcept
ofneuropathicpainanditsproposedmanagement.[3] Dry eye afterrefractivesurgerycanbeduetothegeneralunderlyingproblems like tear insufficiency and aqueous deficiency,meibomianglanddysfunction,orsecondarytotransectionofcornealnervesandotherspecificanatomicalandphysiologicalocularchangesduringtheprocedure.[11,12]
The identificationof theunderlying etiopathogenesis isintegral to the management of DED in general and helps us customizeprimary treatment strategies.This reviewarticleaimsathighlighting themethodological evaluationofDEDespeciallyrelatedtorefractivesurgeryandoutlinesaprotocolbasedcustomizedmanagement.
Etiopathogenesis of Post-Refractive Surgery DEDTheDEDseenpost-refractivesurgeryhasmultipleproposedmechanisms.
Denervation of the cornea leading to decreased corneal sensitivityTheflapcreationandexcimerphotoablation in laser in situ keratomileusis(LASIK)andthefemtosecondphoto-disruptionofstromawithmanualextractionoftheintrastromallenticulein small incision lenticule extraction (SMILE) results in the
Cite this article as: D’Souza S, James E, Swarup R, Mahuvakar S, Pradhan A, Gupta K. Algorithmic approach to diagnosis and management of post-refractive surgery dry eye disease. Indian J Ophthalmol 2020;68:2888-94.
This is an open access journal, and articles are distributed under the terms of the Creative Commons Attribution‑NonCommercial‑ShareAlike 4.0 License, which allows others to remix, tweak, and build upon the work non‑commercially, as long as appropriate credit is given and the new creations are licensed under the identical terms.
For reprints contact: [email protected]
Preferred Practice
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]

December2020 D’Souza,et al.:AlgorithmpostrefractiveDEDmanagement 2889
temporarypartialdenervationofthecornea.[11]Photorefractivekeratectomy (PRK) involves excimer photoablation of thecorneawithoutflap creation andhence there canbe somedamagetothesubbasalplexusofcornealnervesbut lesstothe deeper stromal nerves than that seen in LASIK.[13] Due to thedamagetocornealnervessecondarytotheseprocedures,there is adecrease in corneal sensitivity and reduction inreflextearsecretion.ThisisoneofthemainmechanismsforDEDpost-refractivesurgery.[11,14]Theverticalsidecutofthecornea inSMILE is shorter than that in aLASIKflap, thustheremaybe less disruption of the normal corneal nerveanatomy [Fig.1aand1b].Thishasbeenevaluatedinanumberofstudieswithsomereportinglesscornealnervedamageanddry eye in SMILE than LASIK[15]andnosignificantdifferencein others.[16,17]Moreover therewasno significantdifferenceincornealreinnervationandsensitivitybetweenSMILEandLASIK at 6monthspostoperatively.[18] Even in PRK there havebeendiffering resultswith some studies claiming lessreductionintearsecretion,cornealsensitivityanddecreasedDEDinPRKcomparedtoLASIK.[13,19,20]whichwasnotprovedin other studies.[21,22]The locationof thehinge inLASIK, isanother importantpointwhich issaid tohaveabearingonthedry eye after refractive surgery. FengYF et al. in their metanalysisstatedthatahorizontalhingeledtolesscornealsensorydisturbance anddry eyeas compared to averticallocationinearlypostoperativeperiod,however,therewasnostatisticallysignificantdifferencebetweenthetwogroupsattheendof6monthspost-surgery.[23]
Thesechangestothecornealnervescanbestudiedintheeyeby invivoconfocalmicroscopy (IVCM).This techniquecanbeusedtodemonstratethetransectionofcornealnervespost-refractivesurgeryandserialimagingcanalsodemonstratetheslowregenerationofnervefibers,whichusuallytakes3–6months.[14]However,insomepatientsthenervefiberregeneration
canbesignificantlylowereven1-yearpost-surgery.[24] Tests using theCochet-Bonnetesthesiometer tocheckcorneal sensitivityshow that corneal sensation recovers topre-operative levelsbyaround6monthspost-surgery.However,somepatientsdoexperiencethesymptomsforalongerduration.[13]
Reduced blink rateThedecreasedcornealsensitivitymayaffectthecorneal-blinkreflex-lacrimalglandpathwayresultinginareducedblinkrateanddecreasedreflexaqueoustearsecretion.[11]Sinceblinkingcontributestotheexpressionofmeibumfromthemeibomianglands (MG) in theeye lids, the lipid layersecretion isalsodependenton theblink.Reduction in theblink rateandanincompleteblinkmayresult insubsequent reduction in theMGlipidsecretionandevaporativeDED.[24]
Corneal curvature change associated tear film instabilityChangesincornealcurvaturemayalterthefrictionencounteredbetweenthecorneaandlid,leadingtoanunstabletearfilmand dry eye.[25]
Mucin associated tear film instabilityThe pressure exerted due to the suction applied duringtherefractivesurgerycandamageconjunctivalgobletcellsresulting in reducedmucin secretion.[26] In addition, thecorneal nerve disruption alters themembrane-associatedmucinexpressionontheepithelium,leadingtoanunstabletearfilm.[27]
Pain without stainPostrefractivedryeyecanalsobeduetoneuropathiccornealpain(NCP)whichisalsotermedascornealallodynia,cornealneuralgia,cornealneuropathyorkeratoneuralgia.[28] This has nowbeenincludedintheTFOSDEWSIIreportasaseparatecondition needing special care.[3] The symptoms ofNCPandDED can overlapwithpatients complaining of pain,discomfort,burning,irritationandgrittinessintheeyes.[1] It canbetriggeredbyanocularsurgeryorinfectioninsomecasesorberelatedtonon-ocularcauses,neurological,orpsychiatricconditions.[29]CornealrefractivesurgerylikeLASIK,SMILEorPRKcanbeacauseforneuropathicpain.Oneclassicalfeatureis thedisproportionately increasedsymptomsascomparedto signs.
Variouspossibleetiopathogenesisofpost-refractiveDEDhavebeensummarizedinFig.2.Inaddition,patientsmayalsosufferfromaqueousdeficiencyandevaporativedryeyenotrelatedtotherefractivesurgery.AroutinescreeningforDEDisimportantbeforeplanningrefractivesurgeryonapatientasthesepatientscanhaveasignificantworseningofthediseasepostoperativelyifundiagnosedandnotmanagedadequately.PatientsarescreenedforDEDaspernormalprotocolDEDintheout-patientdepartment.Therearenoadditional specialtestsforcheckingdryeyebeforerefractivesurgery.
Preoperative Evaluation for DED in Patients Undergoing Refractive SurgeryHistory and slit-lamp examinationA detailed history preoperatively is essential and should includehistoryofcontactlensintolerance,allergy,medicationuse,previouschemicalinjury,long-termuseofantiglaucomamedicationsandassociatedsystemicdiseaseslikerheumatoid
Figure 1: (a) Diagrammatic representation of the normal corneal nerve anatomy with distribution at various levels. (b) Diagrammatic representation of differences in nerve transection in LASIK v/s SMILE
b
a
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]

2890 Indian Journal of Ophthalmology Volume68Issue12
arthritis, Sjogren’s syndrome, rosacea, systemic lupuserythematosus.[30]Ifsuspectingunderlyingsystemicdisease,a timely referral to an immunologist/rheumatologistwillhelpinthemanagementofthesystemicconditionandbettermanagement of theDED.Overlapping demographics ofpatientsopting for a refractive surgeryand those sufferingfrom theabove-mentioned conditions emphasizes theneedforcarefulhistorytakingandevaluation.[31,32]
Patient questionnairesValidated questionnaires like theOcular SurfaceDiseaseIndex (OSDI),DryEyeQuestionnaire (DEQ-5) and Impactof Dry Eye on Everyday Living (IDEEL) are useful topreoperativelypickup symptomatology suggestiveofdryeye.[33,34]
Examination – ocular surface assessmentEvaluationoftheface,eyelidsincludingmeibomianglands,blinkpatterns,tearfilm,conjunctivaandcorneaareessentialinDED.Meibomianglanddysfunction(MGD)isgradedusingdifferentclassificationsandscales.[35]
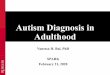
Routine tests for Dry eye evaluation including tearmeniscus height,[36] schirmers test with and withoutanesthesia,[37,38]tearbreaktime[21]andocularsurfacestainingusingfluorescein, roseBengal or lissaminegreen formarean important part of the preoperative evaluation,[39] and the same testsmust be repeatedpostoperatively if patientdevelops symptoms suggestiveofdry eye.Care shouldbetaken tonot touch the strip to the ocular surface to avoidfalse staining while instilling the dye. It is important to look foracharacteristicpatternofcornealstainingtermedLASIKinducedneuroepitheliopathy (LINE) seen inpostrefractivesurgerypatientsiftheyaresymptomatic[Fig. 3].[40]
Advanced Diagnostic Modalities can be Added to the Evaluation Preoperatively if Suspecting Dry EyeInterferometryTear film interferometry is one of the newer modalities ofdry eye assessment. Itmeasures thenature, lipid layerthickness (LLT) and lipid layerbreakupusing interferencepatterns.TheLipiView(TearScienceInc.,Morrisville,NC,USA)andIDRA(SBISistemiInc,StradaTorino,Italy)aresomeofthecommerciallyavailableinterferometers.[41]
Meibographycanbeusedtoassessthe morphology of the meibomianglandsandlossasthiscanbeacontributortothedry eye.[42]
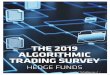
Confocal microscopyIn vivo confocalmicroscopy (IVCM) is a non-invasive,high-resolution imaging tool that images the cornea at thedifferent levels anddelineates cellular changes. It isusefulin followingup nerve and inflammation-related changesseen in the corneapostrefractive surgeryand inDED.Thenumberanddensityof sub-basalandstromalnervecells isderangedinDEDrelatedconditions.[43]Bead-likeformation,micro-neuromas, tortuosity and irregular branching andincreasedcornealdendriticcelldensity[cDCD]arealsoseenonIVCMinpatientsofDED[Fig.4a].[43,44]Changesinkeratocytecount,stromalchangesandnervedensityhavebeenshowntooccurafterrefractivesurgery.[45,46]IVCMcanalsodemonstratethecornealnerve-relatedchangespostrefractivesurgery,andnerve regeneration on serial follow up [Fig.4b].InasubsetofpatientswhohaveNCP, in vivo confocalmicroscopy(IVCM)demonstrateddecreased corneal nerves and the presence
Figure 2: Flow chart of the probable pathophysiology of post‑refractive surgery DED
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]
December2020 D’Souza,et al.:AlgorithmpostrefractiveDEDmanagement 2891
ofmicroneuromas indicativeof the swellingof the injurednerve terminal.[47,48]Thesefindingscouldaidindiagnosisandplanning management.
Inflammatory biomarkersOneoftheimportantunderlyingfactorsinthepathogenesisofDEDisocularsurface inflammation.[49] IdentificationandquantificationoftheinflammatorymarkersinDEDcanhelptheclinicianstocustomizeDEDmanagementespeciallyifitisdetectedinapre-refractivesurgerypatientastheassociatedinflammationcanhavean impactonhealingandoutcomespostrefractivesurgery.[49-51]Matrixmetalloproteinase9(MMP9)isoneofthecommonlystudiedinflammatorymarkersandcannowbemeasuredusinganoutpatientpointofcarediagnostictest called the InflammaDry (Rapid Pathogen Screening,QuidelCorporation).[33]However,aneasydiagnostickitwhichcouldmeasurealargerrangeofinflammatoryfactorsknowntobeassociatedwith this condition couldgivemuchmoreinformationandhelpcustomizetreatment.[49]
Management of dry eye related to refractive surgeryTheTFOSDEWSIIhasgivenverycomprehensiverecommendationsformanagementofDED. It elaborateson treatmentaspectsrangingfromeducationofthepatientregardingenvironmentalmodificationsanddiseaseprognosticationtotreatmentoptionsavailable fordifferent typesofDED. It also talksabout thenewerthermalandlight-basedtherapies forMGDandroleofanti-inflammatoryagents,autologousserumandoralsecretagoguesacrossdisease severity.[52] Thepostrefractive surgeryDEDmanagementremainsthesame,exceptthatpostoperativelythetopicalanti-inflammatoryandimmunomodulatorymedicationslikecyclosporinemayneedtobecontinuedforlongerduration(upto4months)dependingoncertainpreoperativecharacteristics.[53]
Post-operative topical medications to treat and prevent dry eyeTear substitutesTear substitutes help in lubricating the surface and alsorelievepatientsymptomatologyprotectingthesurfaceagainstdesiccationandpromotingtearretention.[52,54]Alargenumberoftopicalformulationsareavailablecontainingcarboxymethylcellulose (CMC), hydroxypropylmethylcellulose (HPMC),sodiumhyaluronate,polyvinylalcohol,polyvinylpyrrolidoneandpolyethyleneglycol.SodiumHyaluronate(HA)inaddition
hasbeenshowntobindwelltoocularsurfaceandhaspotentialwound healing properties.[55]Lubricatingeyedropsareselectedbasedon themechanismof action, composition, viscosity,osmolarity/osmolality,pHandpreservativeagents.
Preservativeintearscanincreaseinflammationandhencepreservative-freemedicationsarepreferred,especiallywhenthedropshavetobeinstilledmorethan4timesadayoverlongperiods of time.[54,56]Benzalkoniumchlorideandchlorobutanolpreservatives in excess candamage the corneal epitheliumresulting in symptomsmimicking theDED itself.Newerpreservativeslikepurite(sodiumchlorite)sodiumperborate,areshowntocauselessharmtotheocularsurface.[57,58]Thus,preservative-freeeyedropsshouldberecommendedtopatientswhorequiremorefrequentinstillationofeyedropsinordertoprevent thepreservative relateddamage to corneal andconjunctivalsurfacehealth.
Anti‑inflammatory treatmentsInflammationisaknownunderlyingfeatureofvarioustypesofDEDandisfurtherincreasedpost-refractivesurgery.Useof anti-inflammatorymedications like topical steroids andcyclosporinemayhavean important role inpost-operativecare.Thishelpsinreducingandbreakingtheinflammatorycascadewhich iskey to alleviating symptomsand treatingthe disease.[10,52]
Topical steroids - Steroids act on the inflammatorycascade, byblocking cyclooxygenase. They alsohave localimmuno-modulatoryactivitybyinhibitingcertaintranscriptionfactors.[59]Topicalcorticosteroidusedecreasesocularirritationand inflammation.[52] Since they are a part of the normalpost-operative regime in refractive surgery, theyarekey toreducingtheincidenceofdryeyesymptomsinthesepatientsintheearlypost-operativeperiodandcanbeusedfor4-6weeksin tapering doses.[52] The strength of steroid used would depend ontheseverityofinflammationintheeye.Patientsprescribedtopical corticosteroids fordry eye shouldbemonitored foradverseeffectslikeraisedintraocularpressureandcataract.[52]
TopicalCyclosporineA(CsA)-TopicaladministrationofCyclosporineA(CsA)hasanimportantrole intreatmentofDEDpost-refractivesurgery.]ItactsbypreventingactivationofT-cellsandproductionofinflammatorycytokines.[60] It has also shownsomeeffectonincreasingtearsecretionandimproveboththesymptomsandsignsofDEDinseveralstudies.[60,61] Sincethepathophysiologyofdryeyepost-refractivesurgeryisslightlydifferentfromregulardryeye,itisimportanttocontroltheinflammationwhichmayimprovepatientsymptomseven
Figure 3: Clinical photograph of LASIK induced neurotrophic epitheliopathy staining (LINE)
Figure 4: (a) Beading of nerves , increased tortuosity of corneal nerves (arrow), increased dendritic cells (star) seen on IVCM in patients of DED. (b) Early nerve regeneration post LASIK seen on IVCM
ba
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]

2892 Indian Journal of Ophthalmology Volume68Issue12
without signs. Topical cyclosporine is usually prescribedfor aminimumdurationof 3monthsbecause theonset ofactionisslowerthansteroids,andcanalsobestarted1monthpreoperatively if patient is having dry eye preoperatively.[53,62]
Treatment of meibomian gland dysfunctionIfthepatienthaschronicMGDpreoperatively,itisadvisableto treat this before planning refractive surgery to avoidpostoperative complications.Thegoal of all treatments forMGDistoimprovetheflowofmeibomianglandsecretionsand reduce inflammation thus leading tonormal tearfilmstability.Thiscanbedonebyconventionalmethodslikelidhygiene,warmcompress,glandexpression,oralandtopicalmedicationsornewerprocedural therapies like the thermalpulsation system[63,64] and Intense pulsed light[65,66] if the
patientisnonresponsiveorfasterresolutionisrequired.Theseprocedureshaveshowngoodeffecteveninpostrefractivedryeye,butcaremustbetakennottoperformthermalpulsationinearlypostoperativeperiodtoavoidflaprelatedissues.
Essentialfattyacids- Usage of oral Omega-3fattyacidslikeeicosapentaenoicacid[EPA]anddocosahexaenoicacid[DHA]andplant-basedsources5-aminolevulinate[ALA]havebeenshowntoimprovesymptomsanddecreaseinflammationandocularsurfacestaininginsomestudies,[67]butnotinothers.[68]
RoleofVitaminDinDED-AsignificantassociationhasbeenfoundbetweenDEDandvitaminDandaprotectiveroleofVitaminDhasalsobeenpostulated.[69] It has an important role inwoundhealingandanassociationhasalsobeenfoundwiththecornealdendriticcelldensityandinflammatoryfactorsin
Figure 5: Algorithmic approach to evaluation and management of DED pre and post refractive surgery with emphasis on subdivision by type and grade of disease
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]

December2020 D’Souza,et al.:AlgorithmpostrefractiveDEDmanagement 2893
tears,[70,71]ItcanbeusedasadjuvanttherapyforpatientswithDEDnon-responsivetoconventionaltherapy.
Fig.5summarizesthealgorithmicapproachtodiagnosingandmanagingDEDrelatedtorefractivesurgery.Inadditiontothefeaturesspecifictopostrefractivedryeye,itisimportantnottomisseasilydiagnosablecausesforDEDpreoperatively.AsdiscussedintheTFOSDEWSIIreport,sinceDEDcanhavealotofoverlapbetweenaqueousandevaporativedisease,itisusefultoplantherapybasedontheseverityofdiseaseaswell as the symptoms and signs.[52]Thishastobedonebothpreoperativelyandpostoperativelyifpatientissymptomatic.
ConclusionThe management of DED is evolving and the treatment of post refractivedryeyeneedsacomprehensiveunderstandingofthepossiblepathomechanisms.Inthisarticlewedetailthedifferentaspectsofpostrefractivedryeyeandpresentanalgorithmicapproach for it’smanagement.A combinationofdetailedhistory,simpletestsandneweradvancesinunderstandingwillhelpoptimizeoutcomesinthesepatients.Duetothevariedpathophysiology in thepostrefractiveDED, this algorithmmaybefurthercustomizedforoptimalresults.Asystematicapproachtothediseasewithabalanceoftestsanddiagnosticsasdiscussed,followedbyappropriatemedicationsforadequatedurationwillgivethebestoutcomes.
Financial support and sponsorshipNil.
Conflicts of interestTherearenoconflictsofinterest.
References1. ŞimşekC,DoğruM,KojimaT,TsubotaK.Currentmanagement
andtreatmentofdryeyedisease.TurkJOphthalmol2018;48:309-13.2. ZeevMS,MillerDD,LatkanyR.Diagnosisofdryeyediseaseand
emergingtechnologies.ClinOphtalmol2014;8:581-90.3. Gomes JAP,AzarDT, BaudouinC, EfronN,HirayamaM,
Horwath-Winter J, et al.TFOSDEWS II iatrogenic report.OculSurf2017;15:511-38.
4. SolomonKD,FernandezdeCastroLE, SandovalHP,GroatB,NeffKD,YingMS,et al.LASIKworldliteraturereview:Qualityoflifeandpatientsatisfaction.Ophthalmology2009;116:691-701.
5. Statista.NumberofLASIKsurgeries in theUnitedStates from1996to2020.Statista;2019.Availablefrom:https://www.statista.com/statistics/271478/number-of-lasik-surgeries-in-the-us/. [Lastaccessedon2019Dec08].
6. SolomonR,DonnenfeldED,PerryHD.TheeffectsofLASIKontheocularsurface.OculSurf2004;2:34-44.
7. AmbrósioR,TervoT,WilsonSE.LASIK-associateddryeyeandneurotrophicepitheliopathy:Pathophysiologyandstrategiesforpre-ventionandtreatment.JRefractSurg2008;24:396-407.
8. AngRT,DarttDA,TsubotaK.Dryeyeafterrefractivesurgery.CurrOpinOphthalmol2001;12:318-22.
9. NarianiA,GuptaP.Dryeyeandrefractivesurgeryoutcomes.CurrOphthalmolRep2016;4:8-14.
10. Craig JP,NicholsKK,AkpekEK,CafferyB,DuaHS, JooCK,et al.TFOSDEWSIIdefinitionandclassificationreport.OculSurf2017;15:276-83.
11. KobashiH,KamiyaK,ShimizuK.Dryeyeafter small incisionlenticule extraction and femtosecond laser-assisted LASIK:Meta-analysis.Cornea2017;36:85-91.
12. D’Souza S, PetznickA,TongL, et al.Comparative analysis oftwo femtosecondLASIKplatformsusing iTRAQquantitativeproteomics.InvestOphthalmolVisSci2014;55:3396-402.
13. BowerKS,SiaRK,RyanDS,MinesMJ,DarttDA.Chronicdryeyeinphotorefractivekeratectomyand laser in situ keratomileusis:Manifestations,incidence,andpredictivefactors.JCataractRefractSurg2015;41:2624-34.
14. LeeB,MclarenJ,EricJ,HodgeD,BourneW.ReinnervationinthecorneaafterLASIK.InvestOphthalmolVisSci2002;43:3660-4.
15. CaiWT,LiuQY,RenCD,WeiQQ,LiuJL,WangQY,et al. Dry eye andcornealsensitivityaftersmallincisionlenticuleextractionandfemtosecondlaserassisted in situ keratomileusis:Ameta-analysis.IntJOphthalmol2017;18;10:632-8.
16. ZhangC,DingH,HeM,LiuL,LiuL,LiG,et al.Comparisonofearlychanges inocularsurfaceand inflammatorymediatorsbetween femto- second lenticule extraction and small-incisionlenticuleextraction.PLoSOne2016;11:e0149503.
17. XuY,YangY.DryeyeaftersmallincisionlenticuleextractionandLASIKformyopia.JRefractSurg2014;30:186-90.
18. LiM,NiuL,QinB,ZhouZ,NiK,LeQ,et al.Confocalcomparisonofcornealreinnervationaftersmallincisionlenticuleextractionandfemtosecondlaser in situ keratomileusis.PLoSOne2013;8:e81435.
19. LeeJB,RyuCH,KimJ,KimEK,KimHB.Comparisonoftearsecretionandtearfilminstabilityafterphotorefractivekeratectomyandlaser in situ keratomileusis.JCataractRefractSurg2000;26:1326-31.
20. MatsuiH,KumanoY,ZushiI,YamadaT,MatsuiT,NishidaT.Cornealsensationaftercorrectionofmyopiabyphotorefractivekeratectomyand laser in situ keratomileusis.JCataractRefractSurg2001;27:370-3.
21. DooleyI,D’ArcyF,O’KeefeM.Comparisonofdry-eyediseaseseverity after laser in situ keratomileusis and laser-assistedsubepithelialkeratectomy.JCataractRefractSurg2012;38:1058-64.
22. ErieJC,McLarenJW,HodgeDO,BourneWM.RecoveryofcornealsubbasalnervedensityafterPRKandLASIK.AmJOphthalmol2005;140:1059-64.
23. FengYF,YuJG,WangDD,LiJH,HuangJH,ShiJL,et al.TheeffectofhingelocationoncornealsensationanddryeyeafterLASIK:Asystematic reviewandmeta-analysis.GraefesArchClinExpOphthalmol2013;251:357-66.
24. BattatL,MacriA,DursunD,PflugfelderSC.Effectsoflaser in situ keratomileusisontearproduction,clearance,andtheocularsurface.Ophthalmology2001;108:1230-5.
25. SzczesnaDH,KulasZ,KasprzakHT,SteneviU.Examinationoftearfilmsmoothnessoncorneaeafterrefractivesurgeriesusinganon-invasiveinterferometricmethod.JBiomedOpt2009;14:064029.
26. KonomiK,ChenLL,TarkoRS,ScallyA,SchaumbergDA,AzarD,et al.PreoperativecharacteristicsandapotentialmechanismofchronicdryeyeafterLASIK.InvestOphthalmolVisSci2008;49:168-74.
27. ShinSY,LeeYJ.ConjunctivalchangesinducedbyLASIKsuctionringinarabbitmodel.OphthalmicRes2006;38:343-9.
28. DieckmannG,Goyal S,HamrahP.Neuropathic cornealpain:Approachesformanagement.Ophthalmology2017;124:S34-47.
29. Shehadeh-MashorR,MimouniM,ShapiraY,SelaT,MunzerG,Kaiserman I.Risk factors fordry eye after refractive surgery.Cornea2019;38:1495-9.
30. BronAJ,dePaivaCS,ChauhanSK,BoniniS,GabisonEE,JainS,et al. TFOSDEWSIIpathophysiologyreport.OculSurf2017;15:438-510.
31. BelmonteC,NicholsJJ,CoxSM,BrockJA,BegleyCG,BereiterDA,et al. TFOSDEWS II pain and sensation report. Ocul Surf2017;15:404-37.
32. StefanskiAL,TomiakC,PleyerU,DietrichT, BurmesterGR,DörnerT.Thediagnosis and treatmentofSjögren’s syndrome.DtschArzteblInt2017;114:354-61.
33. Wolffsohn JS,Arita R, Chalmers R, DjalilianA, DogruM,
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]

2894 Indian Journal of Ophthalmology Volume68Issue12
DumbletonK,et al.TFOSDEWSIIdiagnosticmethodologyreport.OculSurf2017;15:539-74.
34. Barber L, Khodai O, Croley T, Lievens C,Montaquila S,ZiemanskiJ,et al.Dryeyesymptomsandimpactonvision-relatedfunctionacrossInternationalTaskForceguidelinesseveritylevelsintheUnitedStates.BMCOphthalmol2018;18:260.
35. TomlinsonA,BronAJ,KorbDR,AmanoS,PaughJR,PearceEI,et al.Theinternationalworkshoponmeibomianglanddysfunction:Reportofthediagnosissubcommittee.InvestOphthalmolVisSci2011;52:2006-49.
36. Thulasi P,DjalilianAR.Update in current diagnostics andtherapeuticsofdryeyedisease.Ophthalmology2017;124:S27-33.
37. ShapiroA,MerinS.Schirmertestandbreak-uptimeoftearfilminnormalsubjects.AmJOphthalmol1979;88:752-7.
38. LiN,DengXG,HeMF.ComparisonoftheSchirmerItestwithandwithouttopicalanesthesiafordiagnosingdryeye.IntJOphthalmol2012;5:478-81.
39. BronAJ,ArguesoP,IrkecM,BrightFV.Clinicalstainingoftheocularsurface:Mechanismsandinterpretations.ProgRetineyeRes2015;44:36e61.
40. AmbrósioRJr,TervoT,WilsonSE.LASIK-associateddryeyeandneurotrophicepitheliopathy:Pathophysiologyandstrategiesforpreventionandtreatment.JRefractSurg2008;24:396-407.
41. EomY,Lee JS,KangSY,KimH,Song JS.Correlationbetweenquantitativemeasurementsoftearfilmlipidlayerthicknessandmeibomiangland loss inpatientswithobstructivemeibomiangland dysfunction and normal controls.Am JOphthalmol2013;155:1104-10.
42. AritaR,SuehiroJ,HaraguchiT,ShirakawaR,TokoroH,AmanoS.Objective image analysis of themeibomian gland area. Br JOphthalmol2014;98:746-55.
43. KhamarP,NairAP,ShettyR,VaidyaT,SubramaniM,PonnalaguM,et al.Dysregulatedtearfluidnociception-associatedfactors,cornealdendriticcelldensity,andvitaminDlevelsinevaporativedryeye.InvestOphthalmolVisSci2019;60:2532-42.
44. TuominenIS,KonttinenYT,VesaluomaMH,MoilanenJA,HelintöM,TervoTM.Corneal innervationandmorphologyinprimarySjögren’ssyndrome.InvestOphthalmolVisSci2003;44:2545-9.
45. Moilanen JA,VesaluomaMH,MullerLJ,TervoTM.Long-termcornealmorphologyafterPRKby in vivo confocalmicroscopy.InvestOphthalmolVisSci2003;44:1064-9.
46. LinnaTU,VesaluomaMH,Perez-SantonjaJJ,PetrollMW,AlióJL,TervoTMT.Effectofmyo-picLASIKoncornealsensitivityandmorphologyofsubbasalnerves.IOVS2000;41:393-7.
47. TheophanousC, JacobsDS,HamrahP.CornealneuralgiaafterLASIK.OptomVisSci2015;92:e233-40.
48. MoeinHR,DieckmannG,AbboudaA,PondelisN, JamaliN,Salem Z. In vivo confocalmicroscopydemonstratesthepresenceofmicroneuromasandmayallowdifferentiationofpatientswithcornealneuropathicpainfromdryeyedisease.InvestOphthalmolVisSci2017;58ARVOE-Abstract 2656.
49. D’SouzaS,TongL.Practicalissuesconcerningtearproteinassaysindryeye.EyeVis2014;1:6.
50. KumarNR,KhamarP,ShettyR,SharmaA,ShettyN,PahujaN,et al. Identificationofnovelpredictive factors forpost surgicalcornealhaze.SciRep2019;9:16980.
51. ShettyR,SethuS,ChevourP,DeshpandeK,PahujaN,NagarajaH,et al.LowervitaminDlevelanddistincttearcytokineprofilewereobserved inpatientswithmilddry eye signsbut exaggeratedsymptoms.TranslVisSciTechnol2016;5:16.
52. JonesL,DownieLE,KorbD,Benitez-Del-CastilloJM.TFOSDEWSIImanagementandtherapyreport.OculSurf2017;15:575-628.
53. Shtein RM. Post-LASIK dry eye. Expert Rev Ophthalmol
2011;6:575-82.54. AsbellPA.Increasingimportanceofdryeyesyndromeandthe
idealartificialtear:Consensusviewsfromaroundtablediscussion.CurrMedResOpin2006;22:2149-57.
55. HoWT,ChiangTH,Chang SW,ChenYH,Hu FR,Wang IJ.Enhanced cornealwound healingwith hyaluronic acid andhigh-potassiumartificialtears.ClinExpOptom2013;96:536-41.
56. JeeD,ParkSH,KimMS,KimEC.Antioxidantandinflammatorycytokineintearsofpatientswithdryeyesyndrometreatedwithpreservative-freeversuspreservedeyedrops.InvestOphthalmolVisSci2014;55:5081-9.
57. GöbbelsM, SpitznasM. Influenceof artificial tears on cornealepithelium in dry-eye syndrome. GraefesArch Clin ExpOphthalmol1989;227:139-41.
58. Noecker RJ, Herrygers LA,Anwaruddin R. Corneal andconjunctival changes caused by commonly used glaucomamedications.Cornea2004;23:490-6.
59. PflugfelderSC,MaskinSL,AndersonB,ChodoshJ,HollandEJ,DePaivaCS,et al.Arandomized,double-masked,placebo-controlled,multicenter comparison of loteprednol etabonate ophthalmicsuspension,0.5%,andplacebofortreatmentofkeratoconjunctivitissicca inpatientswithdelayedtearclearance.AmJOphthalmol2004;138:444-57.
60. UtineCA,SternM,AkpekEK.Clinicalreview:TopicalophthalmicuseofcyclosporinA.OculImmunolInflammation2010;18:352-61.
61. SallK, StevensonOD,MundorfTK,ReisBL.Twomulticenter,randomized studies of the efficacy and safetyof cyclosporineophthalmicemulsioninmoderatetoseveredryeyedisease.CsAPhase3StudyGroup.Ophthalmology2000;107:631-9.
62. PerryHD,SolomonR,DonnenfeldED,PerryAR,WittpennJR,GreenmanHE, et al. Evaluationof topical cyclosporine for thetreatmentofdryeyedisease.ArchOphthalmol2008;126:1046-50.
63. Lane SS, DuBinerHB, Epstein RJ, Ernest PH, Greiner JV,HardtenDR,et al.Anewsystem,theLipiFlow,forthetreatmentofmeibomianglanddysfunction.Cornea2012;31:396-404.
64. Schallhorn CS, Schallhorn JM, Hannan S, Schallhorn SC.Effectivenessof aneyelid thermalpulsationprocedure to treatrecalcitrantdryeyesymptomsafterlaservisioncorrection.JRefractSurg2017;33:30-6.
65. VigoL,GiannaccareG, Sebastiani S, PellegriniM,Carones F.Intensepulselightforthetreatmentofdryeyeowingtomeibomianglanddysfunction.JVisExp2019.doi:10.3791/57811.
66. DellSJ.Intensepulsedlightforevaporativedryeyedisease.ClinOphthalmol2017;11:1167-73.
67. Wojtowicz JC, Butovich I,UchiyamaE,Aronowicz J,Agee S,McCulley JP. Pilot, prospective, randomized, double-masked,placebo-controlledclinicaltrialofanomega-3supplementfordryeye.Cornea2011;30:308-14.
68. RosenbergES,AsbellPA.Essentialfattyacidsinthetreatmentofdryeye.OculSurf2010;8:18-28.
69. AskariG,RafieN,MiraghajaniM,HeidariZ,ArabA.AssociationbetweenvitaminDanddryeyedisease:Asystematicreviewandmeta-analysisofobservational studies.ContLensAnteriorEye2020;43:418-25.
70. D’souzaS,GhoshA,PahujaN,DeshmukhR,AhujaP,SainaniK,et al.Dysregulatedtearfluidnociception-associatedfactors,cornealdendriticcelldensity,andvitaminDlevelsinevaporativedryeye.InvestOphthalmolVisSci2019;60:2532-42.
71. HwangJS,LeeYP,ShinYJ.VitaminDenhances theefficacyoftopical artificial tears inpatientswithdry eyedisease.Cornea2019;38:304-10.
[Downloaded free from http://www.ijo.in on Friday, February 12, 2021, IP: 93.148.225.148]