Embed Size (px)
Citation preview
Alterna(veTreatmentModalityintheManagementofPost-SurgicalEsotropiawithAnomalousCorrespondence
AlexandriaTilley,O.D.,TharanieAmarawardana,O.D.,KimberlyHamianO.D.,M.H.EstherHan,O.D.,F.C.O.V.D,F.A.A.O.
IntroducBonTheves(bulo-ocularreflex(VOR)occurswhenthesemi-circularcanalsdetectchangesinangularaccelera(onofthehead.Uponcessa(onofaconstant-velocitymovement,post-rotarynystagmusoccursoppositetheini(alheadrota(on.Thedirec(onofthepost-rotarynystagmuscanpromoteabduc(oninapa(entwithesotropia.Techniquesinvolvingthesesubcor(calreflexesarethebasisforthistreatmentmodality.
VesBbulo-OcularReflex• Keepsimagesstableonthere(naduringbriefheadmovements• Servestopreventre(nalimageslip,whichcanleadtooscillopsiaandvisualblur• Theeyesrotateatthesamevelocity,butintheoppositedirec(on,asheadrota(on• Example:ifoneisfixa(ngatargetstraightaheadandrotatestheirheadtotheleN,theeyes
shouldmovetotheright• Latencyof16ms• Madeupofaslowcomponentandafastcomponent
• Theslowcomponent,whichisthesubcor(calpor(on,ispresentatbirth• Thefastsaccadicreturn,whichiscor(callydriven,mayormaynotbepresentatbirth
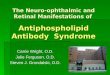
VesBbularAnatomyPeripheralves(bularsystem(Fig.1)• Threesemi-circularcanals• Otoliths:utricle,saccule
Centralves(bularprojec(ons• Ves(bularnuclei• Ascendingtracts• Descendingtracts
Semi-circularcanals• Anterior(Superior)• Posterior(Inferior)• Horizontal(Lateral)
• Eachsemi-circularcanalisoriented90degreesawayfromeachother• Anteriorandposteriorcanals:oriented45degreesoneithersideoftheparasagi\alplane• Horizontalcanal:oriented30degreesabovetheaxialplane• Thesemi-circularcanalsactlikefunc(onalpairs
• Ifyouexciteasemi-circularcanalononesideofthehead,youinhibittheotherontheoppositesideoftheheadthatliesroughlywithinthesameplane
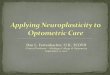
Physiology• Eachsemi-circularcanalcontainsendolymph,aviscousfluid.• Ononepor(onofeachsemi-circularcanal,thereisadila(on,knownasanampulla,inwhicha
gela(nousmass,knownasacupula,islocated(Figure2).• Withinthecupulaareves(bularhaircells,innervatedbybipolarsensoryneuronsofthe
ves(bularnerve.• Withrota(onalaccelera(onofthehead,endolymph,duetoiner(a,doesnotmoveini(ally
withtheheadrota(on• Thereisanetdisplacementoftheendolymphthatpushesonthecupula,andbendsthe
embeddedhaircells.Thiscausesreleaseofanac(onpoten(alandac(va(onoftheves(bularnerve.
References1.BaxstromC,CloptonJ.COPECourse:Ves(bularprocessing–Akeycomponentoffunc(onandbalance,January2017.2.CohenHS.Neuroscienceforrehabilita(on.Philadelphia:Lippinco\Williams&Wilkins,1999.3.LeighRJ,ZeeDS.Theneurologyofeyemovements:4thedi(on.NewYork,NY:OxfordUniv.Press,2015.4.WongAM.Eyemovementdisorders.Oxford:OxfordUniv.Press,2007.Fig1:h\ps://www.nidcd.nih.gov/health/balance/balance_disorders.aspFig2:publicdomainimage:originalsourcefromNASA’sar(cle“TheEffectsofSpaceFlightontheHumanVes(bularSystem”h\ps://commons.wikimedia.org/wiki/File:Inner_ear%27s_cupula_transmipng_indica(on_of_accelera(on.jpgFig3:“Push-pullprincipleintheves(bularsystem,forahorizontalhead-movmenettotheright:therighthorizontalsemicircularcanalgetsexcited,whiletheleNhorizontalcanalgetsinhibited”byThomasHaslwanter.GFDLPermission.h\ps://commons.wikimedia.org/wiki/File:Ves(bular_PushPull.svgTable1:Adaptedfrom:LeighRJ,ZeeDS.Theneurologyofeyemovements:4thedi(on-Table3-2.NewYork,NY:OxfordUniv.Press,2015.
CasePresentaBonA9yearoldmalepresentedtotheUniversityEyeCenterwithconcernsofdecreasedvisioninhisrighteyeandaconstantrightesotropia.Hismotherreportsthatsheini(allyno(cedtheeyeturnpriorto6monthsofage,andhehadstrabismussurgeryonhisrighteyewhenhewasfiveyearsold.Uponini(alevalua(on,hismotherreportedshedidnotwanttoundergoanotherstrabismussurgeryandwasinterestedinonlypursuingvisiontherapyPost-RotaryNystagmus• Ajerknystagmusthatoccurssecondarytocessa(onofaconstant-velocityrota(on.• Occurssecondarytothecon(nuedmovementoftheendolymphsecondarytoiner(alforces• Theslowphaseoccursinthedirec(onofini(alheadrota(on,whilethefastphaseoccursinthe
oppositedirec(on.• Forexample:ifonerotatestotheleNataconstantvelocityandthenquicklystopsmovement,a
jerknystagmuswouldbeobservedwiththeslowphasetotheleNandafastphasetotheright.
Table3:RelaBonshipBetweenSemi-CircularCanalsandExtra-OcularMuscles
DiscussionofTechniquesMonocularfixa2onwithheadrota2ons:Inordertopromoteabduc(onoftherighteye,thepa(entworeapatchoverhisleNeye.Hethenfixatedonatargetin-frontofhim.He(ltedhischindownby30degreesandrotatedhisheadfromsidetosidelaterallywhilemaintainingfixa(onstraightahead.WhenhisheadwastowardstheleNside,hisrighteye,bywayoftheves(bulo-ocularreflex,wasinaposi(onofabduc(on.Thereby,thevisual-ves(bularinterac(onwasusedinordertoincreaserangeofmo(onoftherightesotropiceye.
Spinningwithpost-rotarynystagmus:Thepa(entclosedhiseyesand(ltedhisheaddownwardsby30degrees.Hewasthenspuninachairupwardsoften(mestotheright.ANer10chairspins,hehadtoquicklystop,openhiseyes,andperformhartchartsaccades.Thistechniquewasimplementedbecauseuponstop-rota(onbotheyescon(nuedtomovewithajerknystagmus,withtheslowphasetowardstheright.Theslowphaseservedtomovebotheyestotherightinayokedfashion,promo(ngabduc(onofhisrighteyeinasubcor(calmanner,whilehavinghimperformhartchartsaccadesintroducedcor(calprocessingtothetechnique.
ConclusionS(mula(ngrota(onalinputusingpost-rotaryresponsesinvolvingvisual-ves(bularinterac(onswereu(lizedwiththispa(entsincetradi(onalbinoculartechniqueswerecontraindicatedandstrabismussurgerywasnotanop(on.Theu(liza(onoftheves(bularocularreflexandpost-rotaryresponsescanbeconsideredasanalterna(vetotradi(onalstrabismustherapy.
Ini(alevalua(on
• DVAcc:20/200OD,20/20OS• Refrac(veerror:+3.50sphOD,+2.25sphOS• DCT:35ΔV-pa\ernconstantrightesotropia• NCT:50ΔV-pa\ernconstantrightesotropia• Extra-ocularmo(li(es:abduc(ondeficitOD,OS,DVD
nearhisneutralpoint• Worth4Dot:esodiplopia
Re-evalua(on:session8
• DVAcc:20/200OD,20/20OS• Amblyoscope:Horrorfusionalisresponses• DCT:35ΔV-pa\ernconstantrightesotropia• NCT:50ΔV-pa\ernconstantrightesotropia
Re-evalua(onatconclusionof21sessionsofin-officevisiontherapy
• DVAcc:20/100OD,20/20OS• Refrac(veerror:+3.50sphOD,+2.25sphOS• DCT:25ΔV-pa\ernconstantrightesotropia• NCT:25ΔV-pa\ernconstantrightesotropia
Threemonthre-evalua(on
• DVAcc:20/100OD,20/20OS• DCT:25ΔVpa\ernconstantrightesotropia• NCT:25ΔVpa\ernconstantrightesotropia• AmblyoscopeanomalouscorrespondenceThepa(entwasinstructedtodiscon(nueves(bular-basedexercisestoseeifsizeofthedevia(onpersisted.
Canal Excita(on
Righthorizontalcanal RightmedialrectusLeNlateralrectus
LeNhorizontalcanal LeNmedialrectusRightlateralrectus
LeNanteriorcanal LeNsuperiorrectusRightinferioroblique
LeNposteriorcanal LeNinferiorobliqueRightsuperiorrectus
Rightanteriorcanal RightsuperiorrectusLeNinferioroblique
Rightposteriorcanal RightsuperiorobliqueLeNinferiorrectus
Techniquesusedinvisiontherapy:sessions1-7
Tradi(onalvisiontherapytechniqueswerea\empted:• Brockstring• Lusterapprecia(on• Quoitvectograms• GTVT• Polamirror• Accommoda(verock• VTS3vergence• Steppingstonestofusion• PatchOS2hours/day
Techniquesusedinvisiontherapy:sessions9-21
Ves(bular-basedtechniqueswereused:• Post-rotarynystagmuswithchairspinstopromote
abduc(onoftherighteye• Monocularfixa(onswhilerota(ngtheheadlaterally• Turnandclap• Seevideofordemonstra(onoftechniques
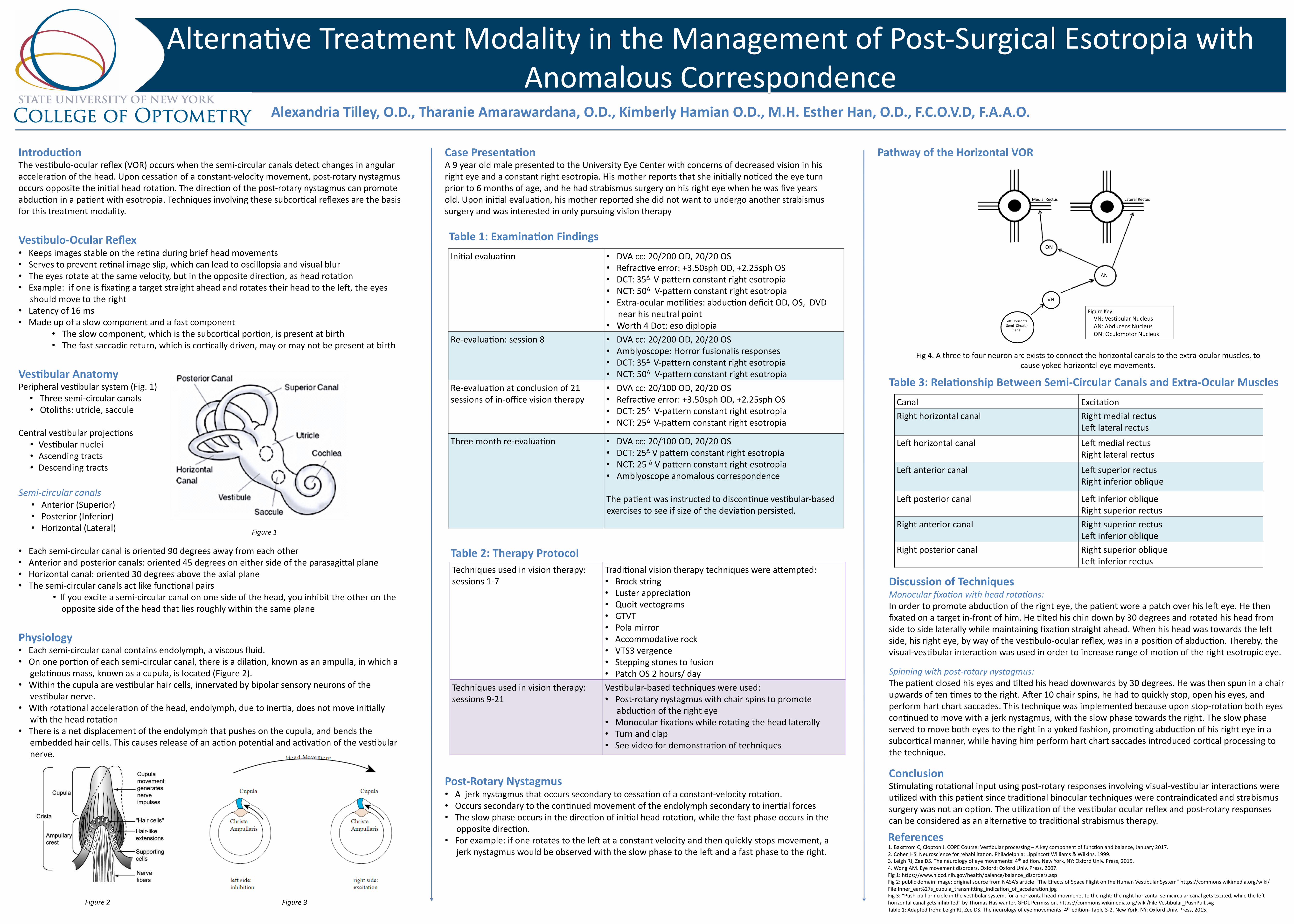
PathwayoftheHorizontalVOR
Fig4.Athreetofourneuronarcexiststoconnectthehorizontalcanalstotheextra-ocularmuscles,tocauseyokedhorizontaleyemovements.
LeNHorizontalSemi-Circular
Canal
VN
AN
ON
MedialRectus LateralRectus
FigureKey:VN:Ves(bularNucleusAN:AbducensNucleusON:OculomotorNucleus
Figure1
Figure2 Figure3
Table1:ExaminaBonFindings
Table2:TherapyProtocol