Embed Size (px)
DESCRIPTION
alcohol
Citation preview

270
26 Alcohol-Related DisordersJohn F. Kelly, PhD, and John A. Renner Jr., MD
KEY POINTS
Incidence
• AlcoholmisuseisoneoftheleadingcausesofmorbidityandmortalityintheUS.
Epidemiology
• Thehighestratesofalcoholuse,heavybingeuse,andalcoholusedisordersoccurbetweentheagesof18and29years.
Pathophysiology
• Alcoholcausesharmthroughthreedistinct,butrelatedpathways:intoxication,toxicity,andalcoholusedisorder.
Clinical Findings
• Alcoholusedisordersareheterogeneousdisordersthatrequireassessmentandanindividualizedclinicalapproach.
• Itispossibletoscreeneffectivelyandefficientlyforthepresenceofanalcoholusedisorderusingbrief,validatedmeasures.
Differential Diagnoses
• Presentationofanalcoholusedisorderisoftencomplicatedbythepresenceofco-morbidpsychiatricsymptomsanddisordersthatrequireassessmentandmonitoring,aswellasanintegratedtreatmentapproach.
Treatment Options
• Anumberofeffectivepharmacologicalandpsychosocialtreatmentapproachesexistforalcoholusedisordersthatproduceoutcomessimilarto,orbetterthan,outcomesforotherchronicillnesses.
Complications
• Heavydrinkingcanleadtoaccidents,violence,unwantedpregnancies,andoverdoses.
OVERVIEWAlcoholisanambiguousmolecule1oftenreferredtoas“man’soldestfriendandoldestenemy”.2Comparedtomorestructur-ally complicated substances, such as cannabis (C21H30O2),cocaine(C17H21NO4),orheroin(C21H23NO5),beveragealcohol(ethanol) possesses a simple chemical structure (C2H5OH)thatbeliesthecomplexitiesofitsmedical,psychological,andsocialimpact(Figure26-1).
Whenthealcoholmoleculereachesthehumanbrainitisgenerallyperceivedasgoodnews;pleasantsubjectiveexperi-encesofeuphoria,disinhibition,anxietyreduction,andseda-tion,arethemostlikelyoutcomes.Theseareoftenencouragedand enhanced by social contexts and by culture-boundcustoms.Iftoohighadoseisimbibedtoorapidly,however,acuteintoxicationoccurs,leadingtoapredictablesequenceofbehavioral disinhibition and cognitive and motor impair-ments. Ifa largequantityofalcohol isconsumed,especially
ifitisdonerapidly,3alcohol-inducedamnesia(“blackouts”),coma,anddeath,canoccur.
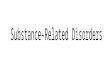
Likeseveralotherdrugs,alcoholcausesharminthreedis-tinct, but related, ways: through intoxication, toxicity, andalcohol use disorder.4 As depicted in Figure 26-2, the acuteintoxicating effects of alcohol produce physical and psycho-logicalimpairments(e.g.,ataxia,poorjudgment,visuo-spatialdeficits, sensory distortions) and disinhibition can lead toaggression,thatcanresultinaccidentsandinjuries(e.g.,fromcar crashes, falls,fights).The toxiceffectsofalcohol,on theother hand, produce harm through the chronic deleteriousactionofalcoholonthehumanbodythatcanresultinliverdamage, includingcirrhosis,aswellasdamage to thebrain,heart,andkidneys.5Becauseofthetoxicitypathwaytoharm,itispossibleforindividualswhoinfrequentlybecomeintoxi-catedto,nevertheless,developavarietyofdiseasesassociatedwithalcohol’s toxic effects, suchascirrhosisof the liveroravariety of cancers (e.g., of the colon, rectum, breast, larynx,liver,esophagus,oralcavity,pharynx6;Figure26-2).Somewhatparadoxically, cirrhosis ismorecommonamong individualswithoutalcoholaddiction,sincemorefloridmanifestationsofdependencearelikelytoresultinmorerapidremission,incar-ceration, or death, preventing the chronic damaging toxiceffectsassociatedwithprolongeduseofalcohol.7Alcoholusedisorder(AUD) is the thirdpathway throughwhichalcoholusecausesharm.AUDcontributestoarangeofchangesinthebrain that often result in alcohol addiction. This can take aheavy toll on individuals’ lives (with serious domestic andsocial problems, family disintegration, loss of employmentandincreasedriskofmortality).Relatedtothesepathwaysisthevolumeandfrequencyatwhichalcoholisconsumed.Low-risk consumption is, for men, no more than 14 drinks perweek and, for women, no more than 7 drinks in any givenweek.Thepatternofconsumptionisalsocritical,however,forobviousreasons;14drinksinonesittingforsomecouldcon-stitutea lethaldose.Thus, tominimizeharmfromintoxica-tion,andtoreducetheriskfromAUDs,nomorethan2drinksonanygivendayformenandnomorethan1forwomenisrecommended8 (Figure 26-3). It should be emphasized,however,thatthispatternofconsumptionis“lowrisk”andnot“norisk”;meta-analysesrevealevenlessthan1drinkadayisassociated with an increased risk for a number of cancers(including breast cancer in women).6 It is estimated thatalcohol is responsible for about 20%–30% of esophagealcancers,livercancer,cirrhosisoftheliver,homicide,epilepticseizures,andmotorvehicleaccidentsworldwide.9ExcessiveorriskyalcoholconsumptionisthethirdleadingcauseofdeathintheUS,accountingforapproximately100,000deathsannu-ally.10 In terms of disability-adjusted life years (DALYs) lost,alcohol accounts for more disease, disability, and mortalitycombinedintheUnitedStatesthantobaccouse,eventhoughtobaccouseaccountsforahigherdeathrate.Thisisbecausealcoholcausesmoreillness,impairmentduringtheprimeofindividuals’ lives,anddeath(e.g.,alcohol is the leadingriskfactor for death among men 15–59 worldwide).11 The eco-nomic burden attributed to alcohol-related problems in theUSapproaches$224billionannually.12,13
Alcohol-relateddisordersarecommoninthegeneralpopu-lation,areprevalentamonggeneralmedicalpatients,andareendemic among psychiatric patients. An awareness of the
Alcohol-RelatedDisorders 271
26
Figure 26-1. Molecular structure of beverage ethyl alcohol. (From UCLA Chemistry, http://www.chem.ucla.edu/harding/IGOC/E/ethanol.html)
Figure 26-2. Alcohol-related disorders associated with high-riskdrinking. (From Rehm J, Room R, Monteiro M, et al. Alcohol use. In Ezzati M, Lopez AD, Rodgers A, Murray CJL, editors: Comparativequantification of health risks: global and regional burden of diseaseattributabletoselectedmajorriskfactors. Geneva, 2004, World Health Organization.)
Effects of High-Risk Drinking
Aggressive, irrational behavior.Arguments. Violence.Depression. Nervousness.
Cancer of throat and mouth.
Frequent colds. Reducedresistance to infection.Increased risk of pneumnoia.
Liver damage.
Trembling hands.Tingling fingers.Numbness. Painful nerves.
Ulcer.
Imparied sensationleading to falls.
Numb, tingling toes.Painful nerves.
Alcohol dependence.Memory loss.
Premature aging. Drinker’s nose.Weakness of heart muscle.
Heart failure. Anemia.Impaired blood clotting.
Breast cancer.
Vitamin deficiency. Bleeding.Severe inflammation
of the stomach. Vomiting.Diarrhea. Malnutrition.
Inflammation of the pancreas.
In men:Impaired sexual performance.
In women:Risk of giving birth to deformed,
retarded babies or low birthweight babies.
Figure 26-3. Patternsofdrinkingandpathwaystoharm.(From Babor TF, Caetano R, Casswell S, et al. Alcohol:noordinarycommodity-researchandpublicpolicy. ed 2. Oxford, UK, 2010, Oxford University Press.)
Pattern of drinking Average volume
Toxic effects
Intoxication
Dependence
Chronic diseaseAccidents/
injuries (acutedisease)
Acute socialproblems
Chronic socialproblems
substantialrolesthatalcoholuse,misuse,andassociateddis-ordersplayinmedicineandpsychiatrywillenhancethedetec-tionoftheseproblemsandleadtomoreefficientandeffectivetargetingofclinicalresources.
Inthischapterwereviewpertinentclinicalmanifestationsofheavyalcoholuseandoutlinestrategiesforeffectiveman-agement of alcohol-related problems. The nature, etiology,epidemiology,andtypologiesofalcohol-relateddisordersaredescribed,andoptimalscreeningandassessmentmethods(tofacilitatedetectionandappropriateintervention)areoutlined.In the final sections, details of current knowledge regardingthemechanismsofactionofheavyalcoholuseareprovidedand effective psychosocial and pharmacological treatmentapproachesarereviewed.
DESCRIPTION AND DEFINITIONAlcohol-relateddisorderscanbedividedintotwomaingroups:alcohol-induced disorders (such as alcohol intoxication,
delirium, alcohol withdrawal, persisting alcohol-inducedamnesticdisorders,andfetalalcoholspectrumdisorders),andalcoholusedisorder(DSM-514,Box26-1).
Heavy, chronic, alcohol use may also induce psychiatricsymptoms and syndromes that mimic psychotic disorder,mood disorders, and anxiety disorders. Such syndromesmost often remit with abstinence, but the diagnosis of an

272 PART IX PsychiatricDisorders
BOX 26-1 The DSM-5 Diagnostic Criteria: Alcohol Use Disorder14
A. Aproblematicpatternofalcoholuseleadingtoclinicallysignificantimpairmentordistress,asmanifestedbyatleasttwoofthefollowing,occurringwithina12-monthperiod:1. Alcoholisoftentakeninlargeramountsoroveralonger
periodthanwasintended.2. Thereisapersistentdesireorunsuccessfuleffortstocut
downorcontrolalcoholuse.3. Agreatdealoftimeisspentinactivitiesnecessaryto
obtainalcohol,usealcohol,orrecoveryfromitseffects.4. Craving,orastrongdesireorurgetousealcohol.5. Recurrentalcoholuseresultinginafailuretofulfillmajor
roleobligationsatwork,school,orhome.6. Continuedalcoholusedespitehavingpersistentor
recurrentsocialorinterpersonalproblemscausedorexacerbatedbytheeffectsofalcohol
7. Importantsocial,occupational,orrecreationalactivitiesaregivenuporreducedbecauseofalcoholuse.
8. Recurrentalcoholuseinsituationsinwhichitisphysicallyhazardous.
9. Alcoholuseiscontinueddespiteknowledgeofhavingapersistentorrecurrentphysicalorpsychologicalproblemthatislikelytohavebeencausedorexacerbatedbyalcohol.
10. Tolerance,asdefinedbyeitherofthefollowing:a. Aneedformarkedlyincreasedamountsofalcoholto
achieveintoxicationordesiredeffect.b. Amarkedlydiminishedeffectwithcontinueduseofthe
sameamountofalcohol.11. Withdrawal,asmanifestedbyeitherofthefollowing:
a. Thecharacteristicwithdrawalsyndromeforalcoholb. Alcohol(oracloselyrelatedsubstance,suchasa
benzodiazepine)istakentorelieveoravoidwithdrawalsymptoms.
Specifyif:
In early remission:Afterfullcriteriaforalcoholusedisorderwerepreviouslymet,noneofthecriteriaforalcoholusedisorderhave
beenmetforatleast3monthsbutforlessthan12months(withtheexceptionthatCriterionA4,“Craving,orastrongdesireorurgetousealcohol,”maybemet).
In sustained remission:Afterfullcriteriaforalcoholusedisorderwerepreviouslymet,noneofthecriteriaforalcoholusedisorderhavebeenmetatanytimeduringaperiodof12monthsorlonger(withtheexceptionthatCriterionA4,“Craving,orastrongdesireorurgetousealcohol,”maybemet).
Specifyif:
In a controlled environment:Thisadditionalspecifierisusediftheindividualisinanenvironmentwhereaccesstoalcoholisrestricted.• Coding notebasedoncurrentseverity,forICD-10-CM
codes:Ifanalcoholintoxication,alcoholwithdrawal,oranotheralcohol-inducedmentaldisorderisalsopresent,donotusethecodesbelowforalcoholusedisorder.Instead,thecomorbidalcoholusedisorderisindicatedinthe4thcharacterofthealcohol-induceddisordercode(seethecodingnoteforalcoholintoxication,alcoholwithdrawal,oraspecificalcohol-inducedmentaldisorder).Forexample,ifthereiscomorbidalcoholintoxicationandalcoholusedisorder,onlythealcoholintoxicationcodeisgiven,withthe4thcharacterindicatingwhetherthecomorbidalcoholusedisorderismild,moderate,orsevere:F10.129formildalcoholusedisorderwithalcoholintoxicationorF10.229foramoderateorseverealcoholusedisorderwithalcoholintoxication.
Specifycurrentseverity:
305.00 (F10.10) Mild:Presenceof2–3symptoms.303.90 (F10.20) Moderate:Presenceof4–5symptoms.303.90 (F10.20) Severe:Presenceof6ormoresymptoms.
Reprinted with permission from the Diagnosticandstatisticalmanualofmentaldisorders, ed 5, (Copyright 2013). American Psychiatric Association.
independent co-occurring psychiatric disorder is difficult todiscern in an individual who is actively drinking. At least 4weeksofsobrietyisrecommendedtoestablishthediagnosisof an independent psychiatric disorder. The next sectionsdescribealcohol-induceddisordersandAUDs.
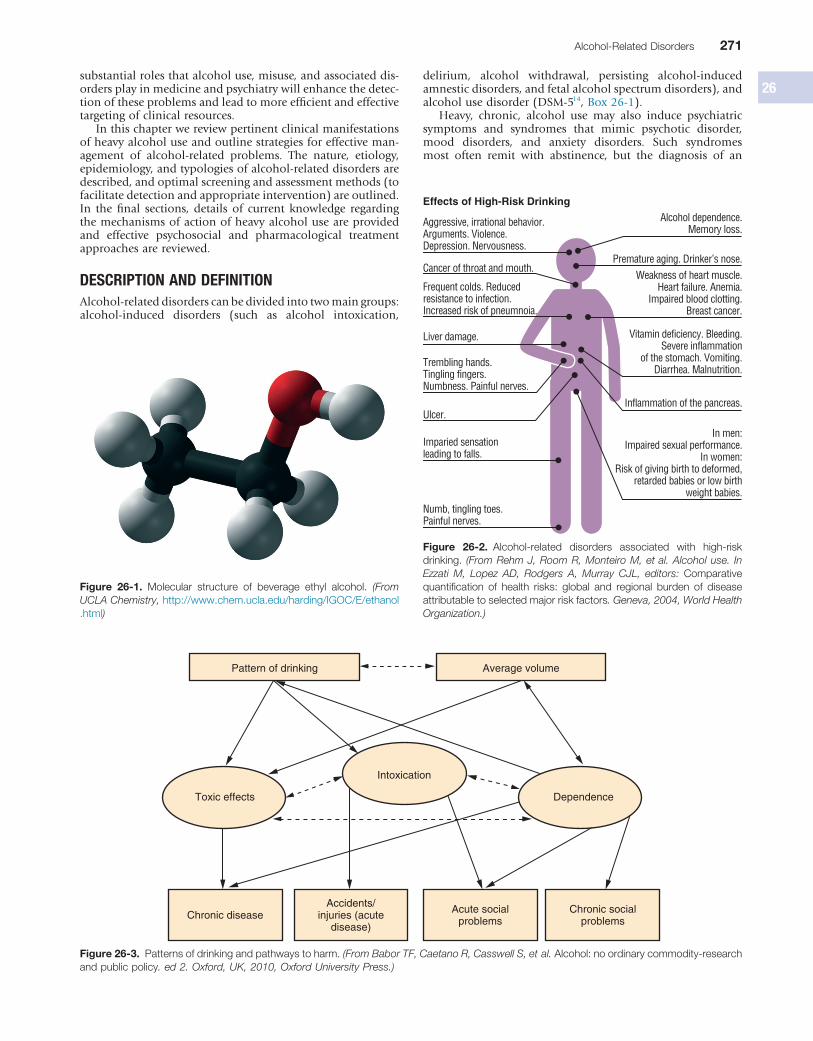
ALCOHOL-INDUCED DISORDERSAlcohol IntoxicationThe action of alcohol on the brain is complex. Low bloodalcoholconcentrations(BACs)produceactivationanddisin-hibition,whereashigherBACsproduce sedation.Behavioraldisinhibitionismediatedbyalcohol’sactionasaγ-aminobutyricacid(GABA)agonist,and its interactionswith theserotoninsystemmayaccountforitsassociationwithviolentbehavior.The GABA, N-methyl-D-aspartate (NMDA), and serotoninsystems have all been implicated in the escalation to vio-lence.15,16 Blood alcohol concentrations (BACs, measured asthepercentageofalcoholintheblood)from0.19%to29%may impair memory or lead to an alcoholic blackout, withargumentativeness or assaultiveness developing at levels of0.10%–0.19%andcomaordeathoccurringat0.40%–0.50%.Yet,chronicalcoholicsmaybefullyalertwithaBACofmorethan 0.40%, owing to tolerance. Resolution of intoxicationfollowssteady-statekinetics,sothata70-kgmanmetabolizes
approximately 10ml of absolute ethanol (or 1.5 to 2 drinkequivalents; 1 standard drink = 0.5oz of whiskey, 4oz ofwine,or12ozofbeer)perhour(Figure26-4).
TreatmentIf it becomes necessary to sedate an intoxicated individual,oneshouldbeginwithasmaller-than-usualdoseofabenzo-diazepine to avoid cumulative effects of alcohol and othersedative-hypnotics. Once the individual’s tolerance hasbeen established, a specific dose can be safely determined.Lorazepam(Ativan)(1to2mg)iseffectivelyabsorbedviaoral(PO),intramuscular(IM),orintravenous(IV)administration.Diazepam(Valium)andchlordiazepoxide(Librium)areerrat-icallyandslowlyabsorbedafterIMadministrationunlesstheyare given in large, well-perfused sites. When incoordinationsuggeststhattheadditiveeffectofabenzodiazepinehaspro-duced excessive sedation, it may be advantageous to usehaloperidol5to10mgPOorIM.Theinitialdoseshouldbefollowedbyadelayof0.5to1hourbeforethenextdose.Ifthereisnoriskofwithdrawal,thepatientcansafelybereferredtoanoutpatientprogram.Inpatientdetoxificationisprefera-bletooutpatientcareifthepatientispsychosociallyunstable;hasseriousmedical,neurological,orpsychiatricco-morbidity;has previously suffered from complications of withdrawal(suchasseizuresordeliriumtremens[DTs]);orisundergoing
Alcohol-RelatedDisorders 273
26
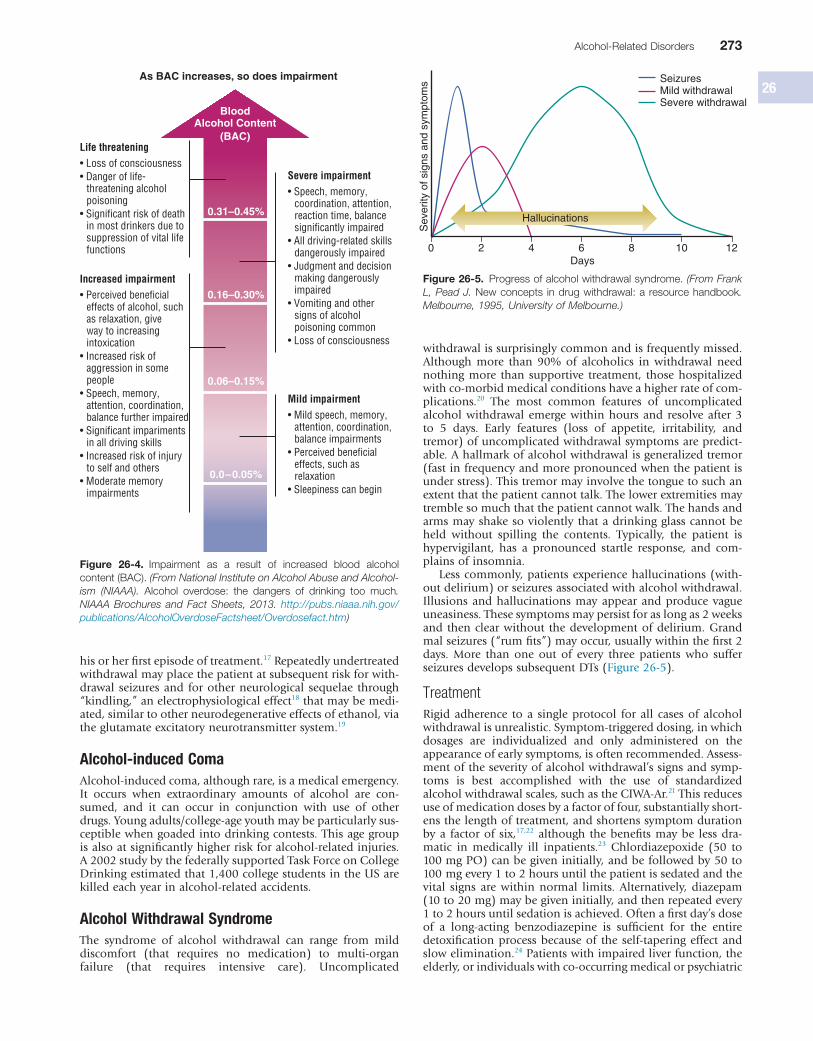
withdrawalissurprisinglycommonandisfrequentlymissed.Although more than 90% of alcoholics in withdrawal neednothingmore than supportive treatment, thosehospitalizedwithco-morbidmedicalconditionshaveahigherrateofcom-plications.20 The most common features of uncomplicatedalcoholwithdrawalemergewithinhoursand resolveafter3to 5 days. Early features (loss of appetite, irritability, andtremor)ofuncomplicatedwithdrawalsymptomsarepredict-able.Ahallmarkofalcoholwithdrawalisgeneralizedtremor(fastinfrequencyandmorepronouncedwhenthepatientisunderstress).Thistremormayinvolvethetonguetosuchanextentthatthepatientcannottalk.Thelowerextremitiesmaytremblesomuchthatthepatientcannotwalk.Thehandsandarmsmayshakesoviolently thatadrinkingglasscannotbeheld without spilling the contents. Typically, the patient ishypervigilant, has a pronounced startle response, and com-plainsofinsomnia.
Lesscommonly,patientsexperiencehallucinations(with-outdelirium)orseizuresassociatedwithalcoholwithdrawal.Illusionsandhallucinationsmayappearandproducevagueuneasiness.Thesesymptomsmaypersistforaslongas2weeksand thenclearwithout thedevelopmentofdelirium.Grandmalseizures(“rumfits”)mayoccur,usuallywithinthefirst2days. More than one out of every three patients who sufferseizuresdevelopssubsequentDTs(Figure26-5).
TreatmentRigidadherence toa singleprotocol for all casesof alcoholwithdrawalisunrealistic.Symptom-triggereddosing,inwhichdosages are individualized and only administered on theappearanceofearlysymptoms,isoftenrecommended.Assess-mentoftheseverityofalcoholwithdrawal’ssignsandsymp-toms is best accomplished with the use of standardizedalcoholwithdrawalscales,suchastheCIWA-Ar.21Thisreducesuseofmedicationdosesbyafactoroffour,substantiallyshort-ensthelengthoftreatment,andshortenssymptomdurationbya factorof six,17,22 although thebenefitsmaybe lessdra-matic in medically ill inpatients.23 Chlordiazepoxide (50 to100mgPO)canbegiveninitially,andbefollowedby50to100mgevery1to2hoursuntilthepatientissedatedandthevital signs are within normal limits. Alternatively, diazepam(10to20mg)maybegiveninitially,andthenrepeatedevery1to2hoursuntilsedationisachieved.Oftenafirstday’sdoseof a long-acting benzodiazepine is sufficient for the entiredetoxificationprocessbecauseof the self-taperingeffect andslowelimination.24Patientswithimpairedliverfunction,theelderly,orindividualswithco-occurringmedicalorpsychiatric
hisorherfirstepisodeoftreatment.17Repeatedlyundertreatedwithdrawalmayplacethepatientatsubsequentriskforwith-drawal seizuresand forotherneurological sequelae through“kindling,”anelectrophysiologicaleffect18thatmaybemedi-ated,similartootherneurodegenerativeeffectsofethanol,viatheglutamateexcitatoryneurotransmittersystem.19
Alcohol-induced ComaAlcohol-inducedcoma,althoughrare,isamedicalemergency.It occurs when extraordinary amounts of alcohol are con-sumed, and it can occur in conjunction with use of otherdrugs.Youngadults/college-ageyouthmaybeparticularlysus-ceptiblewhengoadedintodrinkingcontests.Thisagegroupisalsoatsignificantlyhigherriskforalcohol-relatedinjuries.A2002studybythefederallysupportedTaskForceonCollegeDrinkingestimatedthat1,400collegestudentsintheUSarekilledeachyearinalcohol-relatedaccidents.
Alcohol Withdrawal SyndromeThe syndrome of alcohol withdrawal can range from milddiscomfort (that requires no medication) to multi-organfailure (that requires intensive care). Uncomplicated
Figure 26-4. Impairment as a result of increased blood alcoholcontent(BAC).(From National Institute on Alcohol Abuse and Alcohol-ism (NIAAA). Alcohol overdose: the dangers of drinking too much. NIAAA Brochures and Fact Sheets, 2013. http://pubs.niaaa.nih.gov/publications/AlcoholOverdoseFactsheet/Overdosefact.htm)
BloodAlcohol Content
(BAC)
0.31–0.45%
0.16–0.30%
0.06–0.15%
0.0–0.05%
As BAC increases, so does impairment
Life threatening• Loss of consciousness• Danger of life-
threatening alcohol poisoning
• Significant risk of death in most drinkers due to suppression of vital life functions
Increased impairment• Perceived beneficial
effects of alcohol, such as relaxation, giveway to increasing intoxication
• Increased risk of aggression in some people
• Speech, memory, attention, coordination, balance further impaired
• Significant impariments in all driving skills
• Increased risk of injury to self and others
• Moderate memory impairments
Severe impairment• Speech, memory,
coordination, attention, reaction time, balance significantly impaired
• All driving-related skills dangerously impaired
• Judgment and decision making dangerously impaired
• Vomiting and other signs of alcohol poisoning common
• Loss of consciousness
Mild impairment• Mild speech, memory,
attention, coordination, balance impairments
• Perceived beneficial effects, such as relaxation
• Sleepiness can begin
Figure 26-5. Progressofalcoholwithdrawalsyndrome.(From Frank L, Pead J. Newconcepts indrugwithdrawal:aresourcehandbook. Melbourne, 1995, University of Melbourne.)
0 2 4 6 8 10 12Days
Sev
erity
of s
igns
and
sym
ptom
s SeizuresMild withdrawalSevere withdrawal
Hallucinations

274 PART IX PsychiatricDisorders
described in themedical literaturemore than150yearsagoand it has been frequently observed ever since, DTs still goundiagnosedinalargenumberofcases.Itismissedbecausephysicians tend to forget thatalcoholismis rampantamongpeopleofallbackgroundsandappearances.30Becausedeathshaveoccurredin10%ofpatientswithuntreatedalcoholwith-drawaldeliriumandin25%ofthosepatientswithmedicalorconcomitantsurgicalcomplications,itisimperativetobeonthealertforthislife-threateningcondition.
It is difficult to predict who will develop DTs. Until adecadeago,DTsrarelydevelopedinpatientsyoungerthan30years of age. This is no longer true. Today the condition isfrequently observed in young patients who may have had adecadeormoreofchronicheavyalcoholconsumption.Themechanisms may involve NMDA-glutamate receptor super-sensitivity.18 Although delirium is regarded as a withdrawalsyndrome,someheavydrinkersfailtodevelopdeliriumaftersudden withdrawal of ethanol. Infection, head trauma, andpoornutritionarepotentiallycontributingfactorstodelirium.AhistoryofDTsisthemostobviouspredictoroffutureDTs.31
TheincidenceofDTsisapproximately5%amonghospital-izedalcoholicsandabout33%inpatientswithalcoholwith-drawalseizures.IfDTsdooccur,theygenerallydosobetween24 and 72 hours after abstinence begins. There have beenreports,however,ofcasesinwhichtheclinicalpictureofDTsdidnotemergeuntil7daysafterthelastdrink.Theprincipalfeaturesaredisorientation(totime,place,orperson),tremor,hyperactivity,markedwakefulness,fever,increasedautonomictone,andhallucinations.Hallucinationsaregenerallyvisual,buttheymaybetactile(inwhichcasetheyareprobablyasso-ciatedwithaperipheralneuritis),olfactory,orauditory.Ves-tibulardisturbancesarecommonandoftenhallucinatory.Thepatientmaycomplainofthefloormovingorofbeingonanelevator.Thehallucinatoryexperienceisalmostalwaysfright-ening,suchasseeingspidersandsnakesthatmayhaveaddi-tional characteristics (e.g., more vivid colors and mice orinsects sensed on the skin). Once the condition manifestsitself,DTsusually last2 to3days,often resolving suddenlyafteranightofsoundsleep.Shoulditpersist,aninfectionorsubduralhematomamaybethecause.Thereare,however,asmallnumberofindividualswhosecourseischaracterizedbyrelapses with intervals of complete lucidity. These patientsoffertheclinicianthemostchallengingdiagnosticopportuni-ties.Asaruleofthumb,itisalwayswisetoincludeDTsinthelistofdiagnosesconsideredwheneverdeliriumappears.Evenskilled clinicians are apt tomiss thediagnosisofDTswhenthe patient’s manner, social position, or reputation belies apreconceivedanddistortedstereotypeofan“alcoholic.”Theclinicianisalsofrequentlymisledwhenthedeliriumisinter-mittent and the patient is examined during a lucid stage.AlthoughacourseofintermittentepisodesishighlyatypicalforDTs,itcanoccur.
TheprognosisforDTsisreasonablygoodifthepatientisaggressivelymedicated,butdeathcanoccurasthesyndromeprogressesthroughconvulsionstocomaanddeath.Deathcanalso result fromheart failure, an infection (chieflypneumo-nia),orinjuriessustainedduringtherestlessperiod.InasmallproportionofpatientsthedeliriummaymergeintoWernicke–Korsakoffsyndrome,inwhichcasethepatientmaynotregainfull mentation. This is more apt to happen in those withcloselyspacedepisodesofDTsandintheelderly,butitshouldbeassessedandcontinuallymonitored.32
TreatmentPrevention is thekey.Symptom-triggereddosing foralcoholwithdrawalhasbeenshowntoreduceDTsmorethanuseofstandingdosesofbenzodiazepineinmedicallyillinpatients.23
conditions are often better managed with a shorter-actingagent,suchaslorazepam1to4mgPOorIM,or0.5mg/minslow IV infusion in severe withdrawal, repeated after 1 to 2hours,withdosetaperingby25%perdayoverthesubsequent3to6days.
The α2-agonist dexmedetomidine is sometimes used incasesofalcoholwithdrawal,especiallywhenpatientsrequireescalating doses of benzodiazepines and additional intuba-tion and mechanical ventilation to protect airways, whichcan lead to complications and prolonged hospital stays.25Similarly,phenobarbitalisusedtoaugmentbenzodiazepine-assisted alcohol withdrawal to prevent the need for intu-bation and ICU admission. A prospective, randomized,double-blind,placebo-controlledstudywith102patients,halfof whom received either a single dose of IV phenobarbital(10mg/kgin100mlofnormalsaline)orplacebo(100mlofnormalsaline)inadditiontoasymptom-guidedlorazepam-basedalcoholwithdrawalprotocol, found that patients whoreceivedphenobarbitalhad fewer ICU admissions (8% vs.25%),andtherewerenodifferencesinadverseevents.26
Alcohol Withdrawal SeizuresWithdrawal seizures occur in roughly 1% of unmedicatedalcoholicsundergoingwithdrawal,althoughtheprevalenceisincreased in individualswith inadequately treatedpriorepi-sodes of alcohol withdrawal, prior alcohol withdrawal sei-zures,seizuredisorders,andpreviousbraininjuries.Althoughbrainimagingmaynotbenecessaryinpatientswiththeirfirstepisode,27seizuresduringalcoholwithdrawalrequirecarefulevaluation for other causes. Indications for imaging includeneurological and other physical findings suggestive of focallesions, meningitis, or subarachnoid hemorrhage—all ofwhichmayoccurinapatientwithahistoryofalcoholwith-drawal seizures. Multiple prior detoxifications predisposepatients to withdrawal seizures more than the quantity orduration of a drinking history, implying a kindling cause.28Seizures may occur following a rapid drop in the BAC orduringthe6to24hoursafterdrinkingcessation.Generalizedseizurestypicallyoccur(i.e.,in75%ofcases)intheabsenceoffocalfindings,andinindividualswithotherwiseunremark-ableelectroencephalogram(EEG)findings.Repeatedseizuresmayoccurovera24-hourperiod;however,statusepilepticusoccursinlessthan10%ofthosewhoseize.
TreatmentInpatientswithoutaprior seizuredisorder,diphenylhydan-toin offers no benefit over placebo, and given the potentialfor side effects, diphenylhydantoin is therefore not recom-mended.28 Also, given that loading with carbamazepine orvalproatemaynotaddresstherapidtimecourseofwithdrawalseizures, the most parsimonious approach remains effectivetreatment with benzodiazepines. Prompt treatment of earlywithdrawalsymptoms,asdescribedbelow,isthemosteffec-tivemeasuretopreventthedevelopmentofseizures.Incaseswhere there is a known seizure disorder, however, conven-tionalmanagementwithananticonvulsantisinorder.
Alcohol Withdrawal DeliriumDeliriumtremens,or“DTs,”themajoracutecomplicationofalcoholwithdrawal,wasrenamed“alcoholwithdrawaldelir-ium”intheDiagnostic and Statistical Manual of Mental Disor-ders,ed4(DSM-IV).29Untilopen-heartproceduresspawnednewpostoperativedeliria,DTswerebyfarthemostfrequentlyencountereddelirium ingeneralhospitals, reportedlyoccur-ring in 5% of hospitalized alcoholics. Although it was first
Alcohol-RelatedDisorders 275
26
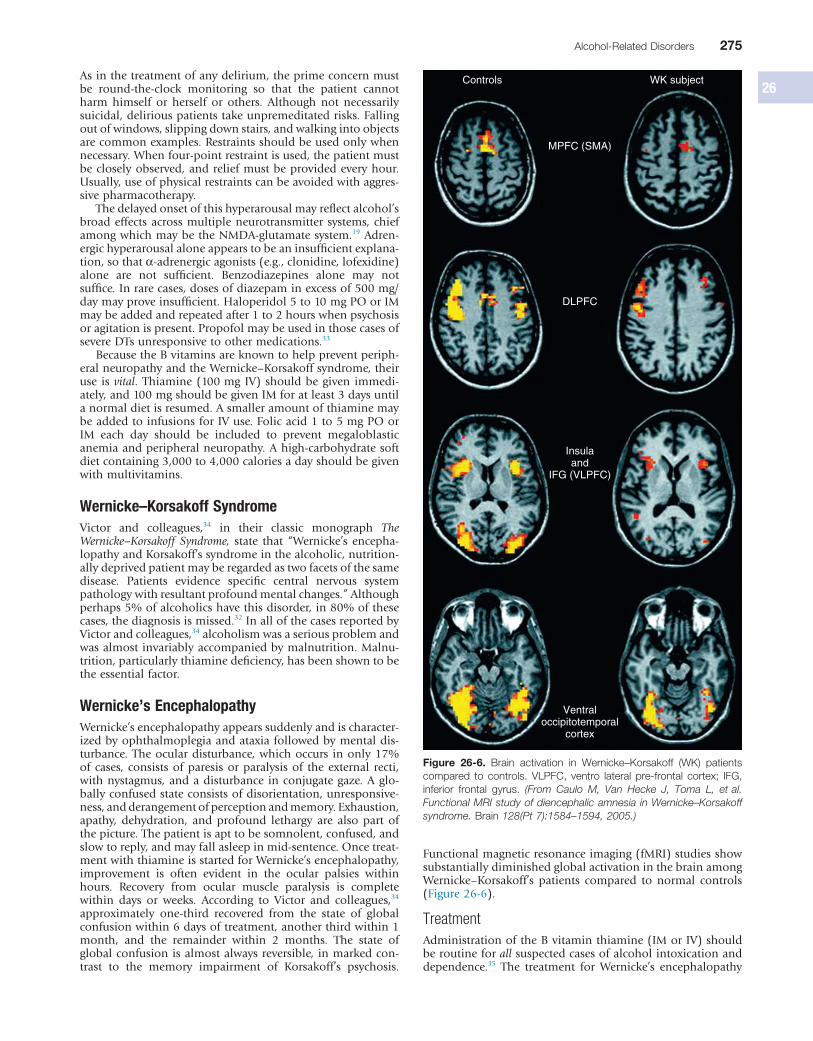
Functionalmagneticresonanceimaging(fMRI)studiesshowsubstantiallydiminishedglobalactivationinthebrainamongWernicke–Korsakoff’s patients compared to normal controls(Figure26-6).
TreatmentAdministrationoftheBvitaminthiamine(IMorIV)shouldberoutineforallsuspectedcasesofalcoholintoxicationanddependence.35 The treatment for Wernicke’s encephalopathy
Asinthetreatmentofanydelirium,theprimeconcernmustbe round-the-clock monitoring so that the patient cannotharm himself or herself or others. Although not necessarilysuicidal,deliriouspatientstakeunpremeditatedrisks.Fallingoutofwindows,slippingdownstairs,andwalkingintoobjectsarecommonexamples.Restraintsshouldbeusedonlywhennecessary.Whenfour-pointrestraintisused,thepatientmustbecloselyobserved,andreliefmustbeprovidedeveryhour.Usually,useofphysicalrestraintscanbeavoidedwithaggres-sivepharmacotherapy.
Thedelayedonsetofthishyperarousalmayreflectalcohol’sbroadeffectsacrossmultipleneurotransmittersystems,chiefamongwhichmaybetheNMDA-glutamatesystem.19Adren-ergichyperarousalaloneappearstobeaninsufficientexplana-tion,sothatα-adrenergicagonists(e.g.,clonidine,lofexidine)alone are not sufficient. Benzodiazepines alone may notsuffice.Inrarecases,dosesofdiazepaminexcessof500mg/daymayproveinsufficient.Haloperidol5to10mgPOorIMmaybeaddedandrepeatedafter1to2hourswhenpsychosisoragitationispresent.PropofolmaybeusedinthosecasesofsevereDTsunresponsivetoothermedications.33
BecausetheBvitaminsareknowntohelppreventperiph-eralneuropathyandtheWernicke–Korsakoffsyndrome,theiruse isvital.Thiamine(100mg IV) shouldbegiven immedi-ately,and100mgshouldbegivenIMforatleast3daysuntilanormaldietisresumed.AsmalleramountofthiaminemaybeaddedtoinfusionsforIVuse.Folicacid1to5mgPOorIM each day should be included to prevent megaloblasticanemiaandperipheralneuropathy.Ahigh-carbohydratesoftdietcontaining3,000to4,000caloriesadayshouldbegivenwithmultivitamins.
Wernicke–Korsakoff SyndromeVictor and colleagues,34 in their classic monograph The Wernicke–Korsakoff Syndrome, state that “Wernicke’s encepha-lopathyandKorsakoff’ssyndromeinthealcoholic,nutrition-allydeprivedpatientmayberegardedastwofacetsofthesamedisease. Patients evidence specific central nervous systempathologywithresultantprofoundmentalchanges.”Althoughperhaps5%ofalcoholicshavethisdisorder,in80%ofthesecases,thediagnosisismissed.32InallofthecasesreportedbyVictorandcolleagues,34alcoholismwasaseriousproblemandwasalmostinvariablyaccompaniedbymalnutrition.Malnu-trition,particularlythiaminedeficiency,hasbeenshowntobetheessentialfactor.
Wernicke’s EncephalopathyWernicke’sencephalopathyappearssuddenlyandischaracter-izedbyophthalmoplegiaandataxiafollowedbymentaldis-turbance.Theoculardisturbance,whichoccurs inonly17%of cases, consistsofparesisorparalysisof theexternal recti,withnystagmus,andadisturbance inconjugategaze.Aglo-ballyconfusedstateconsistsofdisorientation,unresponsive-ness,andderangementofperceptionandmemory.Exhaustion,apathy, dehydration, and profound lethargy are also part ofthepicture.Thepatientisapttobesomnolent,confused,andslowtoreply,andmayfallasleepinmid-sentence.Oncetreat-mentwiththiamineisstartedforWernicke’sencephalopathy,improvement is often evident in the ocular palsies withinhours. Recovery from ocular muscle paralysis is completewithin days or weeks. According to Victor and colleagues,34approximately one-third recovered from the state of globalconfusionwithin6daysoftreatment,anotherthirdwithin1month, and the remainder within 2 months. The state ofglobalconfusionisalmostalwaysreversible,inmarkedcon-trast to the memory impairment of Korsakoff’s psychosis.
Figure 26-6. Brain activation in Wernicke–Korsakoff (WK) patientscompared to controls. VLPFC, ventro lateral pre-frontal cortex; IFG,inferior frontal gyrus. (From Caulo M, Van Hecke J, Toma L, et al. Functional MRI study of diencephalic amnesia in Wernicke–Korsakoff syndrome. Brain 128(Pt 7):1584–1594, 2005.)
Controls WK subject
MPFC (SMA)
DLPFC
Insulaand
IFG (VLPFC)
Ventraloccipitotemporal
cortex

276 PART IX PsychiatricDisorders
known as “fetal alcohol syndrome,” these disorders canincludeasetofbirthdefectscausedbyalcoholduringpreg-nancy.38 Children with this condition typically have facialdeformities, a mis-proportioned head, mental retardation,andbehavioralproblems(Figure26-7).
However,evenwhentheseabnormalitiesarenotevident,brain damage may still have occurred. Approximately30%–40%ofallwomenwhodrinkheavilyduringpregnancywillhaveababywithsomedegreeofFASD.ItistheleadingcauseofpreventablementalretardationintheWesternHemi-sphere.StudiesusingMRItoviewthebrainsofchildrenwithFASDshowthatbrainareasthatregulatemovementandcog-nitiveprocessesrelatedtoattention,perception,thinking,andmemory are particularly sensitive to pre-natal alcohol expo-sure,andthatbrainsizeisreduced.39
The minimum amount of alcohol needed to produceharmfuleffects inexposedchildren isnotknown.Thus, thesafest approach is to completely avoid alcohol during preg-nancy.Peoplewithpre-natalalcoholexposurehaveahighriskof learning and mental disabilities, school dropout, delin-quency,alcoholandotherdrugusedisorders,mentalillness,and poor psychosocial function. Education, screening, andearlyinterventionarecritical.
ALCOHOL USE DISORDERSAlcohol use disorder has been re-classified in DSM-5 into asingle,11-item,categoryof“alcoholusedisorder”whichwasconstructed by combining three of the four former “abuse”criteria (repeated legal consequenceswasdropped)with theseven“alcoholdependence”criteriaspecifiedinDSM-IV,andbyaddinganew“craving”criterion.Theothermajorclassifica-tion system, the International Classification of Diseases,Version10(ICD-10),however,hasmaintaineditsdistinctionbetween “alcohol dependence” and “harmful use”. Impor-tantly, both systems delineate “polythetic” classifications ofAUD,sinceonlytwofromalistof11symptomsarerequiredtomeetadiagnosticthresholdinDSM-5andthreeinICD-10for a “dependence” diagnosis. This highlights a degree ofheterogeneitywithin the syndrome thathas typological and
and Korsakoff’s psychosis is identical, and both are medical emergencies. Because subclinical cognitive impairments canoccur even in apparently well-nourished patients, routinemanagementshouldincludethiamine,folicacid,andmulti-vitaminswithminerals,particularlyzinc.Promptuseofvita-mins, particularly thiamine, prevents advancement of thedisease and reverses at least a portion of the lesions wherepermanent damage has not yet been done. The response totreatmentisthereforeanimportantdiagnosticaid.Inpatientswhoshowonlyocularandataxicsigns,thepromptadminis-trationof thiamineiscrucial inpreventingthedevelopmentofanirreversibleandincapacitatingamnesticdisorder.Treat-mentconsistsof100mgof thiamineand1mgof folicacid(givenIV)immediatelyand100mgIMofthiamineeachdayuntilanormaldietisresumed,followedbyoraldosesfor30days.ParenteralfeedingsandtheadministrationofB-complexvitaminsbecomenecessaryifthepatientcannoteat.Ifarapidheart rate, feeble heart sounds, pulmonary edema, or othersignsofmyocardialweaknessappear,thepatientmayrequiredigitalis. Because these patients have impaired mental func-tion,nursingpersonnelshouldbealertedtothepatient’sten-dencytowander,tobeforgetful,andtobecomeobstreperouslypsychotic.
Korsakoff’s Psychosis (Alcohol-induced Persisting Amnestic Disorder)Korsakoff’s psychosis, also referred to as confabulatory psy-chosisandalcohol-inducedpersistingamnesticdisorder,29 ischaracterizedbyimpairedmemoryinanotherwisealertandresponsiveindividual.Thisconditionisslowtostartandmaybe the end stage of a lengthy alcohol-dependence process.Hallucinations and delusions are rarely encountered. Curi-ously,confabulation,longregardedasthehallmarkofKorsa-koff’s psychosis, was exhibited in only a limited number ofcases in the large series collected and studied by Victor andcolleagues.34Mostofthesepatientshavediminishedsponta-neous verbal output, have a limited understanding of theextentoftheirmemoryloss,andlackinsightintothenatureoftheirillness.
Thememorylossisbipartite.Theretrogradecomponentistheinabilitytorecallthepast,andtheanterogradecomponentisthelackofcapacityforretentionofnewinformation.Intheacute stage of Korsakoff’s psychosis, the memory gap is soblatantthatthepatientcannotrecallsimpleitems(suchastheexaminer’sname,theday,orthetime)eventhoughthepatientisgiventhisinformationseveraltimes.Asmemoryimproves,usually within weeks to months, simple problems can besolved,limitedalwaysbythepatient’sspanofrecall.
Patients with Korsakoff’s psychosis tend to improve withtime.36 Among Victor and colleagues’ patients,34 21% recov-eredmoreor lesscompletely,26%showednorecovery,andtherestrecoveredpartially.29Duringtheacutestage,however,thereisnowayofpredictingwhowillimproveandwhowillnot. The EEG may be unremarkable or may show diffuseslowing, and magnetic resonance imaging (MRI) may showchanges in the periaqueductal area and medial thalamus.18ThespecificmemorystructuresaffectedinKorsakoff’spsycho-sis are the medial dorsal nucleus of the thalamus and thehippocampalformations.
Fetal Alcohol Spectrum DisorderFetalalcoholspectrumdisorder(FASD) isanumbrella termthatdescribes the rangeofeffects that canoccur inan indi-vidualwhosemotherdrankalcoholduringpregnancy.Theseeffectsmay includephysical,mental,behavioral,or learningdisabilities with possible life-long implications.37 Formerly
Figure 26-7. Characteristicsoffetalalcoholspectrumdisorder.(From Wattendorf DJ, Muenke M. Fetal alcohol spectrum disorders. AmFamPhysician 72(2):279–282, 285, 2005.)
Epicanthal folds
Flat nasal bridge
Thin upper lip
“Railroad track” earsSmall palpebral fissures
Upturned noseSmooth philtrum

Alcohol-RelatedDisorders 277
26functional genetic variants of alcohol dehydrogenase thatdemonstratehighalcoholoxidizingactivity, and thegeneticvariantofaldehydedehydrogenasethathaslowacetaldehydeoxidizingactivity,protectagainstheavydrinkingandalcohol-ism48); impulsivityanddisinhibition(e.g.,dopinergicDRD2genes49), psychiatric disorders (e.g., the miRNA biogenesispathway50 and individuals’ level of response to alcohol47,51),although the latter be reflect differences in alcohol-metabolizinggenes.
The relative contributions of genetic and environmentalfactorstothemanifestationofAUDscanbeexpressedasthepopulation-attributableriskpercent,meaningthepercentageofdiseaseincidencethatwouldbeeliminatediftheriskfactorwere removed. A genetic heritability estimate for alcoholdependence is sometimes estimated at approximately 50%,withtheother50%(equaling“100%”)attributableto“envi-ronmental causes.” However, these estimates are misleadingsince the attributable risks for a complex disease, such asalcoholdependence,canaddtowellover100%becausethedisorder can be avoided in many different ways and can beincreasedbymanydifferentgeneticvariants.Theseadditionalpercentagescanbedescribedasinteractionsamongthevariousriskfactors(e.g.,gene–environmentinteractions).Forexample,ageneticabnormalitymaybenecessaryforadiseasetooccur,butthediseasewillnotoccurwithoutthepresenceofanenvi-ronmental risk factor. Thus, the attributable risks for thegeneticaberrationandtheenvironmentalfactorwouldbothbe100%.Phenylketonuria isanexampleof this: thediseasecanbeavoidedeitherbynothavingthegeneticabnormalityorbyeliminatingphenylalaninefromthediet.52Similarly,regard-lessofanindividual’shighgeneticriskforAUD,thedisordercanbecompletelyavoidediftheindividualchoosestoabstain,orifthereisnoaccesstoalcoholintheenvironment.AUDsareheterogeneousdisorders.Heritablegeneticfactorsincreasetherisk for developing alcohol dependence, but it should berememberedthatmanyindividualswithoutanyfamilyhistoryofAUDsmaystillmeetcriteriaforalcoholdependence.
Factors that influence the initiation of alcohol consump-tion shouldbedistinguished from those that affectpatternsofconsumptiononcedrinkingisinitiated.Studiesofadoles-cent twins have demonstrated that initiation of drinking isprimarilyinfluencedbythedrinkingstatusofparents,siblings,andfriendsaswellasbyenvironmentalvariationacrossgeo-graphicalregionswhereadolescenttwinsreside.Severalcross-national studies, including studies in the US, indicate thatinitiation of alcohol use during adolescence is influencedchiefly by cultural rather than genetic factors.53–55 The influ-enceofgeneticfactorsisnegligible.Conversely,onceinitiated,alcohol use topography is strongly influenced by geneticfactors. However, these influences are modulated also bysiblingandpeer-contexteffects(e.g.,collegesettings)andbyregionalenvironmentalvariation.56
Pedigree, twin, and adoption studies all point to anincreasedriskforalcoholdependenceinoffspringwhenthereis a history of such disorders in the family.57 For example,familystudiesindicateafour-foldincreasedriskfordepend-enceamongrelativesofindividualswithalcoholdependence,with higher vulnerabilities for those with a greater number(higherdensity)ofalcohol-dependentcloserelatives.58Thesegenesinfluenceavarietyofcharacteristicsorendophenotypes(such as impulsivity, disinhibition, and sensation seeking),enzymes(suchasalcoholandaldehydedehydrogenases),andalowlevelofresponsetoalcohol’seffects.Thesecharacteris-ticsthencorrelatewithandinteractwithenvironmentaleventstoincreasetheriskforthecondition.58–60Hence,geneticpre-dispositionsarenotdeterministic.AUDsarecausedbyacom-bination of interacting factors. These consist of genetic,biological,andenvironmentalfactors.
clinical implications for detecting and treating the disorder.TheDSM-5criteriacanbeseeninBox26-1.
The alcohol dependence syndrome was first described inthe1970s40andhassincebeenvalidatedandgeneralized todescribethedependencesyndrome(alsooftenreferredtoas“addiction”)acrossallpsychoactivesubstances.EdwardsandGross40noted that thedependence syndromemaybe recog-nizedbytheclusteringofcertainelements.Notallelementsneed be present or present to the same degree, but withincreasing intensity the syndrome is likely to show logicalconsistency. It isconceptualizedasan integrationofphysio-logicalandpsychologicalprocessesthatleadstoapatternofheavyalcoholusethatisincreasinglyunresponsivetoexternalcircumstancesortoadverseconsequences.Furthermore,theyviewedthesyndromenotasanall-or-nothingdichotomy,butas occurring with graded intensity, and its presentation asbeinginfluencedbypersonality,aswellasbysocialandcul-tural contexts. Their conceptualization also introduced a“bi-axial”modelwiththedependencesyndromeconstitutingoneaxisandalcohol-relatedproblemstheother.
IntheUSbeforeDSM-III41therewasonlyasingledescrip-tivecategory,“alcoholism,”whichhithertohadbeenviewedasapersonalitydisorder.DSM-IIIwasinfluencedbythesyn-drome and bi-axial concepts of Edwards and Gross40 and,consequently,introducedadistinctionbetween“dependence”and “abuse.” DSM-III was the first diagnostic manual ofmentaldisordersintheUStointroduceactualitemizedcrite-ria,increasingthereliabilityofthesediagnoses.42
The term alcoholism was originally coined to describealcohol dependence/addiction and is often still used as analternative to dependence. However, it is often used morebroadly todescribe alcoholdependence aswell asharmful/hazardous use, sometimes without explicit mention of thefact.“Dependence”hasalsobeenusedtodifferentiatephysi-ologicaldependenceonadrug(e.g.,onopiatesfollowingpainmanagement after surgery) from “addiction”, which may ormaynotincludephysiologicaldependence,butisasyndromethat involvesdrug-seekingbehaviorandagreatdealof timeseeking,using,andgettingovertheeffectsofthedrug.Thesevariations in usage can be confusing.43 It may also lead toerrorsinclinicalandscientificcommunicationasithasimpli-cations for inferences that are drawn from clinical data andmay ultimately affect treatment policy decisions.43 Thus, webelievecareshouldbetakeninchoosingdescriptivetermsandinusingthemaccuratelyandconsistently.44–46
As described in Box 26-1, AUD is characterized by thebroad elements of neuroadaptation (tolerance and with-drawal) and an impaired ability to alter or to stop alcoholconsumption for very long, despite the personal suffering itcauses(impairedcontroloveruse).Asaconstruct,assessmentofAUDhasbeen shown tobe reliableand topossessgoodconstructandpredictivevalidity.Furthermore,TheAUDcon-structhasdemonstratedconstructandpredictivevalidityandcanbereliablymeasured.
ETIOLOGY AND EPIDEMIOLOGYEtiologyKnowledgeabouttheonsetandcourseofAUDsprovidesvalu-ableinformationforthetailoringandtimingofassessments,aswellasforpreventionandinterventionstrategies.Alcoholdependenceisconsideredacomplexdisorderwithmanypath-waysthatleadtoitsdevelopment.Geneticandotherbiologi-cal factors, along with temperament, cognitive, behavioral,psychological, and sociocultural factors, are involved in theemergence of AUD.47 Genes confer at least four separatedomains of risk: alcohol metabolizing enzymes (e.g., the
278 PART IX PsychiatricDisorders
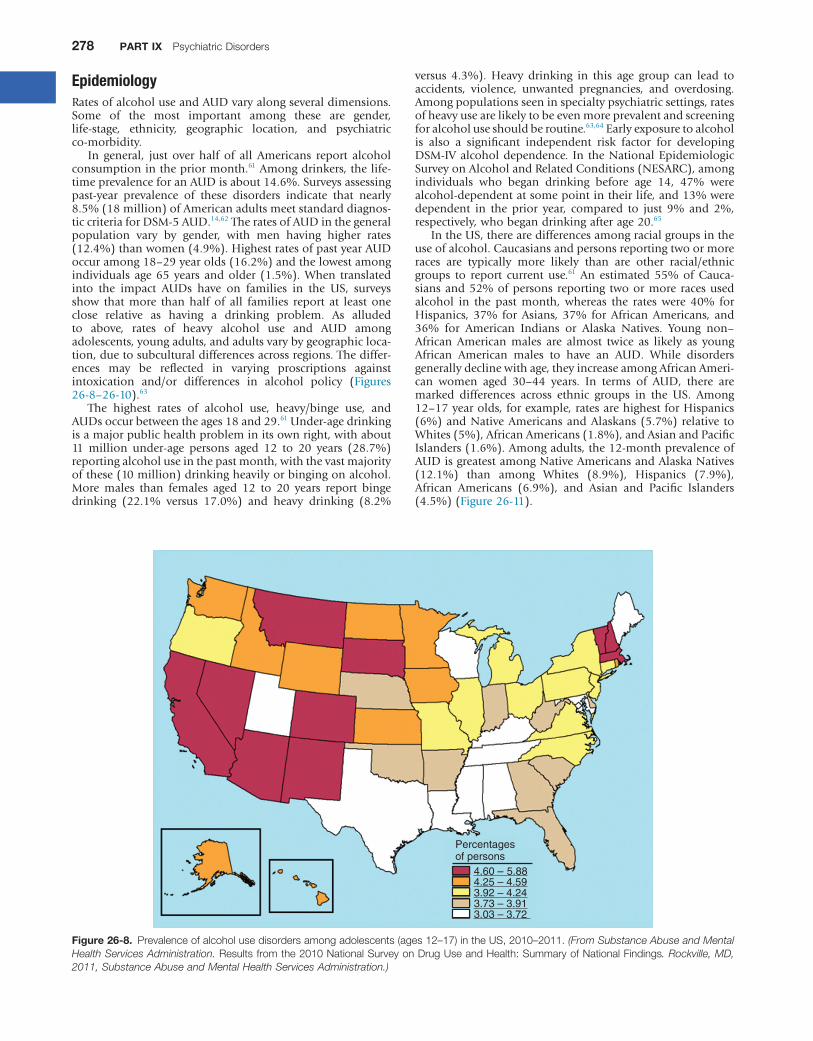
Figure 26-8. Prevalenceofalcoholusedisordersamongadolescents(ages12–17)intheUS,2010–2011.(From Substance Abuse and Mental Health Services Administration. Resultsfromthe2010NationalSurveyonDrugUseandHealth:SummaryofNationalFindings. Rockville, MD, 2011, Substance Abuse and Mental Health Services Administration.)
Percentagesof persons
4.60 – 5.884.25 – 4.593.92 – 4.243.73 – 3.913.03 – 3.72
EpidemiologyRatesofalcoholuseandAUDvaryalongseveraldimensions.Some of the most important among these are gender,life-stage, ethnicity, geographic location, and psychiatricco-morbidity.
In general, just over half of all Americans report alcoholconsumptioninthepriormonth.61Amongdrinkers,thelife-timeprevalenceforanAUDisabout14.6%.Surveysassessingpast-year prevalence of these disorders indicate that nearly8.5%(18million)ofAmericanadultsmeetstandarddiagnos-ticcriteriaforDSM-5AUD.14,62TheratesofAUDinthegeneralpopulation vary by gender, with men having higher rates(12.4%)thanwomen(4.9%).HighestratesofpastyearAUDoccuramong18–29yearolds(16.2%)andthelowestamongindividuals age65years andolder (1.5%).When translatedinto the impact AUDs have on families in the US, surveysshow that more than half of all families report at least oneclose relative as having a drinking problem. As alludedto above, rates of heavy alcohol use and AUD amongadolescents,youngadults,andadultsvarybygeographicloca-tion,duetosubculturaldifferencesacrossregions.Thediffer-ences may be reflected in varying proscriptions againstintoxication and/or differences in alcohol policy (Figures26-8–26-10).63
The highest rates of alcohol use, heavy/binge use, andAUDsoccurbetweentheages18and29.61Under-agedrinkingisamajorpublichealthprobleminitsownright,withabout11 million under-age persons aged 12 to 20 years (28.7%)reportingalcoholuseinthepastmonth,withthevastmajorityofthese(10million)drinkingheavilyorbingingonalcohol.More males than females aged 12 to 20 years report bingedrinking (22.1% versus 17.0%) and heavy drinking (8.2%
versus 4.3%). Heavy drinking in this age group can lead toaccidents, violence, unwanted pregnancies, and overdosing.Amongpopulationsseeninspecialtypsychiatricsettings,ratesofheavyusearelikelytobeevenmoreprevalentandscreeningforalcoholuseshouldberoutine.63,64Earlyexposuretoalcoholis also a significant independent risk factor for developingDSM-IValcoholdependence. In theNationalEpidemiologicSurveyonAlcoholandRelatedConditions(NESARC),amongindividuals who began drinking before age 14, 47% werealcohol-dependentatsomepointintheirlife,and13%weredependent in the prior year, compared to just 9% and 2%,respectively,whobegandrinkingafterage20.65
IntheUS,therearedifferencesamongracialgroupsintheuseofalcohol.Caucasiansandpersonsreportingtwoormoreraces are typically more likely than are other racial/ethnicgroups to report current use.61 An estimated 55% of Cauca-siansand52%ofpersons reporting twoormore racesusedalcohol in the past month, whereas the rates were 40% forHispanics, 37% for Asians, 37% for African Americans, and36% for American Indians or Alaska Natives. Young non–African American males are almost twice as likely as youngAfrican American males to have an AUD. While disordersgenerallydeclinewithage,theyincreaseamongAfricanAmeri-can women aged 30–44 years. In terms of AUD, there aremarked differences across ethnic groups in the US. Among12–17yearolds,forexample,ratesarehighestforHispanics(6%)andNativeAmericansandAlaskans(5.7%)relative toWhites(5%),AfricanAmericans(1.8%),andAsianandPacificIslanders(1.6%).Amongadults,the12-monthprevalenceofAUDisgreatestamongNativeAmericansandAlaskaNatives(12.1%) than among Whites (8.9%), Hispanics (7.9%),African Americans (6.9%), and Asian and Pacific Islanders(4.5%)(Figure26-11).

Alcohol-RelatedDisorders 279
26
Figure 26-10. Prevalenceofalcoholusedisorderamongpersonsaged12andolderandintheUnitedStates,2010–2011. (From Substance Abuse and Mental Health Services Administration. Resultsfromthe2010NationalSurveyonDrugUseandHealth:SummaryofNationalFind-ings. Rockville, MD, 2011, Substance Abuse and Mental Health Services Administration.)
7.87 – 10.777.18 – 7.866.66 – 7.175.58 – 6.654.59 – 5.57
Percentagesof persons
Figure 26-9. Prevalenceofalcoholusedisorderamongyoungadults(ages18–25)intheUS,2010–2011.(From Addiction Treatment Strategies. Finger tapping study shows alcoholics may recruit other brain regions. 2012; http://www.addictionts.com/2012/08/17/finger-tapping-study-shows-alcoholics-may-recruit-other-brain-regions/, 2013.)
17.66 – 20.7015.98 – 17.6514.88 – 15.9713.33 – 14.8710.13 – 13.32
Percentagesof persons

280 PART IX PsychiatricDisorders
strongcorrelationbetweentheseverityofmentalillnessandtheprevalenceofAUD.66
There are several possible explanations for these co-occurrences. Both conditions may be due to a commonpathway (e.g., a genetic predisposition). One disorder maysubstantiallyinfluencetheonsetoftheother,suchaswhenanindividualbeginstousealcoholtocopewithpsychiatricdis-tress(e.g.,socialanxiety),orwhentherearemethodologicaldeterminants(e.g.,unmeasuredcommoncausesorselectionbiasesinsomeclinicalstudies).
These co-morbidities can be regarded clinically in twoways: a patient may present with an AUD, perhaps in anaddiction-treatmentsetting,andalsoaco-occurringpsychiat-ricillness;andapatientmaypresentwithapsychiatricdisor-der,perhapsinamentalhealthclinic,andanadditionalAUD.AmongpatientswithAUDs seen inaddiction-treatment set-tings,more thanhalfwillhaveat leasta life-timehistoryofanotherco-occurringDSMpsychiatricdisorder,andmanywillhaveacontinuingpsychiatricdisturbanceinoneoftheseotherareasinadditiontotheiralcoholuse.Thejobofthediscerningclinicianwillbetopatientlyandcarefullydeterminethepres-ence of non–substance-induced syndromes that may persistperniciouslywithabstinence.The“dualdiagnosis”patientcanbechallengingasheorshemaynotrespondaswelltostand-ardaddictiontreatment,andmayhavegreaterratesofrelapse,attrition,andre-admissions.However,ifaco-morbidpsychi-atricdisorderisobservedordetected,determiningtherelativeonsetofthetwodisordersmayhaveclinicalsignificance,sinceprimary disorders (i.e., those emerging first) tend to be ofgreater long-term clinical significance. For instance, patientswhose bipolar disorder precedes the onset of their alcoholdependencetendtohavebetteralcoholoutcomes(andworsebipolar outcomes) than those whose alcohol dependenceoccurredfirst;thesepatientstendtohaveworsealcoholout-comesandbetterbipolaroutcomes.67Nevertheless,bothdis-orderswillneedtobeattendedtosimultaneouslyforoptimumresults.68,69
Forpatientsenteringprimarymentalhealthsettings,AUDsoftengoundetected.Leftunnoticed,thesedisorderscanunder-mine the salutary effects of psychotropic and psychosocialinterventionsaimedatamelioratingthesymptomsofpsychiat-ricillness.Itisimportanttonotethatanygeneralizationsabout“dualdiagnosis”patientsshouldbemadewithcaution.Thetermobviouslycoversanimmenseamountofclinicalterritory,sinceitnotonlycoversthepresenceofanalcoholorotherdrugusedisorder,whichinthemselvesareheterogeneousandvarygreatlyinseverity,butalsoavastarrayofpsychopathologicaldisturbances,eachwithitsownsub-variationsanddegreesofseverity.Thus, the specific type, severity, and relative clinicalsignificance of the co-morbid psychiatric disorder on thepatient’s presentation and future function should always beconsideredwhenapproachingthesedualproblems.Ifagener-alizationcanbemadeitisthatbothtypesofdisordersshouldalwaysbeassessedandpsychiatric symptomsmonitored forcontinued and independent influence in the context of sus-tainedabstinencefromalcohol(oranotherdrug).70,71Ifpresent,theseconditionsshouldbetreatedinanintegratedfashion.69
TypologiesAUDsarecomplexandheterogeneous.Hence,attemptshavebeen made to try to identify more homogeneous subtypes.Varioustypologies,someformalandotherslessformal,havebeenproposedduringthepast50years.Earlytypologiesreliedmore on theoretically-framed, clinical observations. Morerecently, data-driven, multi-variate sub-classifications havebeenderivedthathaveetiologicalsignificanceandpredictivevalidity,andmayhaveclinicalutility.
ALCOHOL USE DISORDERS AND CO-OCCURRING PSYCHIATRIC ILLNESSThe co-occurrence of AUDs with other psychiatric disordershas been widely recognized.66 Large-scale epidemiologicalsurveysonco-morbidityintheUShavebeencompletedinthegeneral household population. The most common life-timeoccurrences of psychiatric disorders for individuals withalcoholdependenceareanxietydisorders(47%),otherdrugusedisorders(43%),andaffectivedisorders(41%);thesearefollowedbyconduct(32%)andantisocialpersonalitydisor-der (13%).As shown inFigure26-12, there isamoderately
Figure 26-11. Twelve-month prevalence of alcohol use disordersacrossrace/ethnicsubgroupsoftheUS.(From Substance Abuse and Mental Health Services Administration. Resultsfromthe2010NationalSurveyonDrugUseandHealth:SummaryofNationalFindings. Rock-ville, MD, 2011, Substance Abuse and Mental Health Services Administration.)
Twelve-month Prevalence of Alcohol Use Disorder AcrossRace/Ethnic Subgroups of the US
14
12
10
8
6
4
2
0
Per
cent
age
Hispanics Native Whites African Asian Americans Americans Americans and Alaska and Pacific Natives Islanders
Race/ethnicity
12–17 year oldsAdults
Figure 26-12. Pastyearalcoholusedisorderamongadultsaged18orolder,bylevelofmentalillness:2011.(From Substance Abuse and Mental Health Services Administration. Resultsfromthe2010NationalSurveyonDrugUseandHealth:SummaryofNationalFindings. Rock-ville, MD, 2011, Substance Abuse and Mental Health Services Administration.)
20
18
16
14
12
10
8
6
4
2
0
Per
cent
with
AU
D
Serious Moderate Low (mild) No mental mental mental mental illness illness illness illness

Alcohol-RelatedDisorders 281
26criteria for alcohol addiction actually receive treatment.81Thus,themajorityofindividualssufferingfromalcoholaddic-tionaremissed,biasingourknowledgetoonlythosealcohol-dependentcasesthatseektreatment—aphenomenonknownas“Berkson’bias.”Consequently,usingdatafromtheNationalEpidemiological Survey on Alcohol and Related Conditions(NESARC),Moss,Chen,andYi82discoveredfivesubtypesofalcohol dependence, distinguished by family history, age ofdependenceonset,endorsementofDSM-IVAUDcriteria,andthepresenceofco-morbidpsychiatricandsubstanceusedis-orders. These general population-derived subtypes awaitfurtherstudy,buttheymayenhanceourunderstandingoftheetiology and natural history of AUD, and lead to improvedandmoretargetedtreatmentinterventions.
PATHOPHYSIOLOGY AND IMAGINGThe deleterious effect of alcohol is diffuse. However, theimpact on the brain is central to the development of AUDsandrelatedconditions.Oftheapproximately18millionindi-viduals with an AUD in the US, approximately one-half totwo-thirdsdevelopsomesortofimpairmentincognitiveand/ormotorprocessesandupto2millionpeoplesufferenoughalcohol-induceddamagetorequirelife-longcare.83Thesecon-ditions,suchasalcohol-inducedpersistingamnesticdisorder(i.e.,Wernicke–Korsakoffsyndrome)anddementia,seriouslyaffect memory, reasoning, language, and problem-solvingabilities.
Importantly, many individuals with a history of alcoholdependenceandneuropsychologicalimpairmentsshowsomeimprovement in function within a year of abstinence, butothers take considerably longer.84–87 Unfortunately, little isknown about the rate and extent to which people recoverspecific structures and functions once abstinence has beenachieved,buttherateofrecoverywilllikelyco-varywiththetopographyandchronicityofalcoholuse,dietaryfactors,andindividual variables related to family history and biologicalvulnerability.Thecerebralcortex(dorsolateralandorbitofron-talcortex),88andsubcorticalareas,suchasthelimbicsystem(e.g., amygdala), the thalamus (involved with communica-tionswithinthebrain),thehypothalamus(involvedwithhor-mones that affect sexual function and behavior, as well asreproduction),andthebasalforebrain(involvedwithlearningandmemory)arethekeybrainregionssusceptibletoalcohol-relateddamage.89Areasthatinfluencepostureandmovement,suchas thecerebellum,also seem tobeaffected.86MRIanddiffusion tensor imaging (DTI) canbeused in combinationtoassessapatient’sbrainwhenheorshefirststopsdrinkingand again after long periods of sobriety, to monitor brainchangesandtodetectcorrelatesofrelapse.
MRI and DTI studies reveal a loss of brain tissue, andneuropsychologicaltestsshowcognitiveimpairmentsinindi-viduals who either have an AUD or are heavy drinkers.90Abnormalitiesonscanshavebeenreported in50%ormoreofindividualswithchronicalcoholdependence.Theseabnor-malities can occur in individuals in whom there is neitherclinical nor neuropsychological test evidence of cognitivedefects.Inindividualswithbingedrinkingandchronicalcoholdependence, MRI has demonstrated accelerated gray matterloss,91whichistosomeextentreversiblewithabstinence,sug-gestingthatsomeofthesechangesaresecondarytochangesinbraintissuehydration.92
Thefrontalareasofthebrainareparticularlysusceptibletoalcohol-related damage despite the fact that alcohol hasdiffusebilateralcorticaleffects.86,89,93Theprefrontalcortexhasbeenshowntobeimportantincognitiveandemotionalfunc-tionandinterpersonalbehavior.Becausetheprefrontalcortexisnecessaryforplanningandforregulationofbehavior,good
Oneofthefirstandmostwell-knownwasJellinek’stypol-ogyconsistingoffivesubspeciesofalcoholismsimplylabeledusing thefirstfive lettersof theGreekalphabet:alpha,beta,delta, gamma, epsilon.72 Jellinek’s very broad definition ofalcoholism as any use that causes harm yielded a similarlybroad typology. Jellinek’s typologywasnot successfullyvali-dated,butitdidhighlighttheimportanttopicofheterogene-ity and it sparked further interest and efforts to identifyparticular subtypesof individuals suffering fromalcoholismforthepurposesoftailoringtreatments.
During the past 25 years, multi-variate typologies havebeeninvestigatedwiththeuseofmorecomplexdataextrac-tion methods (e.g., cluster and factor analysis). Cloninger’sTypeIorTypeIIandBabor’sTypeAorBwerethefirstofthese.Cloninger and colleagues73 identified two separate forms ofalcoholismbasedondifferencesinalcohol-relatedsymptoms,patternsoftransmission,andpersonalitycharacteristicsusingdataderivedfromacross-fosteringstudyofSwedishadoptees.TypeIwascharacterizedbyeithermildorseverealcoholuseintheprobandsandnocriminalityinthefathers.TheseTypeI alcoholics came from relatively high socioeconomic back-groundsandwerefrequentlyassociatedwithmaternalalcoholuse.TypeIalcoholicswerethoughttobemoreresponsivetoenvironmental influence, to have relatively mild alcohol-relatedproblems,andtohavealateageofonset(olderthan25years).Ontheotherhand,Cloninger’sTypeIIalcoholismis characterized as being associated with a family history,having severe alcoholproblems,havingotherdruguse, andhavinganearlyonset(beforeage25).Althoughmulti-variatestatisticalmethodswereusedtoidentifysubtypes,Cloninger’stypes of alcoholism have been criticized due to the smallsamplesizes(lessthan200),sampleselectionmethods,andindirectassessmentoffamilyvariables.74
AsecondtypologywasproposedbyBaborandcolleagues75basedonasampleof321alcoholicinpatients.Babor’sTypeAresembledCloninger’sType1,andwascharacterizedbyalaterage of onset, fewer childhood behavior problems, and lesspsychopathology. Type B resembled Type II alcoholism andwasdefinedbyahighprevalenceofchildhoodbehaviorprob-lems, familial alcoholism, early onset of alcohol problems,morepsychopathology,more life stress,andamorechronictreatmenthistory.
Abroaddistinctionofearly-onsetversuslate-onsetalcoholdependencemayhavesomeclinicalmatchingutility,althoughevidence is limited. For example, use of selective serotoninreuptake inhibitors (SSRIs) has produced modest drinkingreductionsthatmaybemoreapparentinmenwithdepressionand late-onset type alcoholism.76,77 Also, double-blindplacebo-controlled studies of anti-craving medications (e.g.,ondansetron)haveshownefficacy forearly-onsetalcoholics,as have others (e.g., topiramate) for a broad range of unse-lectedalcoholicpatients.
Laterstudiesexaminingtypologieshavefoundmorethantwo subtypes that have clinical and etiological significance,particularlyregardinggender,andinternalizing/externalizingdisorders,inadditiontofamilyhistoryandageofonset.Forexample, several multi-variate, multi-dimensional analyseshave revealed that there may be as many as four general,homogeneous subtypes of alcohol dependence78,79: chronic/severe, depressed/anxious, mildly affected, and antisocial.80Thesefoursubtypesofalcoholdependencearefoundwithinbothgendersandacrossdifferentethnicsubgroups,butmoreprospectiveresearchisneededtoexaminetheirrelativeclini-calcourseandresponsivenesstovariouspharmacologicalandpsychosocialinterventions.TheseapproachestoAUDtypolo-gieshaveemployedeitherempiricalorclinical/observationalstrategies using data derived principally from treatmentsamples.However,onlyaboutone-fourthofthosewhomeet
282 PART IX PsychiatricDisorders
year.101 Hence, blackouts should be viewed as a potentialconsequenceofacuteintoxicationandnotspecifictoalcoholdependence.
Glutamatereceptorsadapttothepresenceofalcoholandthus become overactive during alcohol withdrawal; thisprocesscanleadtostrokeandseizure.102Deficienciesofthia-mine caused by malnutrition, common among individualswith alcohol dependence, may exacerbate this potentiallydestructiveoveractivity.103
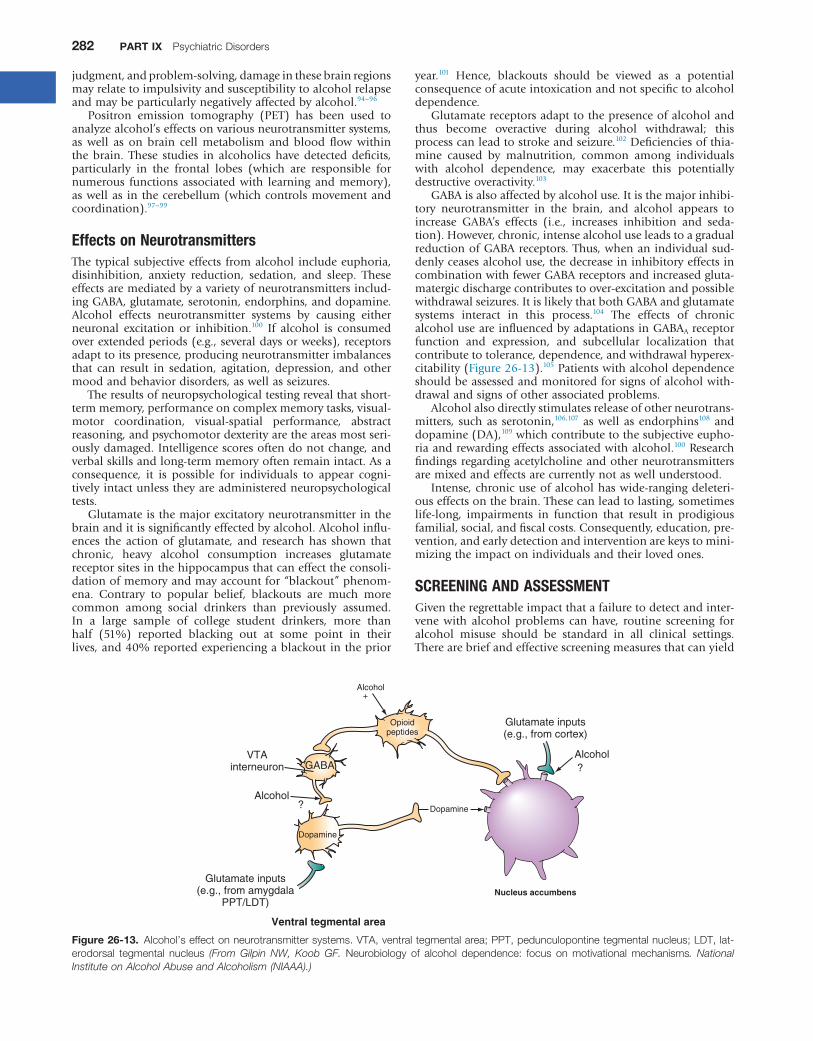
GABAisalsoaffectedbyalcoholuse.Itisthemajorinhibi-tory neurotransmitter in the brain, and alcohol appears toincrease GABA’s effects (i.e., increases inhibition and seda-tion).However,chronic,intensealcoholuseleadstoagradualreductionofGABAreceptors.Thus,whenanindividualsud-denlyceasesalcoholuse,thedecreaseininhibitoryeffectsincombinationwithfewerGABAreceptorsandincreasedgluta-matergicdischargecontributestoover-excitationandpossiblewithdrawalseizures.ItislikelythatbothGABAandglutamatesystems interact in this process.104 The effects of chronicalcoholuseareinfluencedbyadaptationsinGABAAreceptorfunction and expression, and subcellular localization thatcontributetotolerance,dependence,andwithdrawalhyperex-citability(Figure26-13).105Patientswithalcoholdependenceshouldbeassessedandmonitoredforsignsofalcoholwith-drawalandsignsofotherassociatedproblems.
Alcoholalsodirectlystimulatesreleaseofotherneurotrans-mitters, suchas serotonin,106,107 aswell as endorphins108 anddopamine(DA),109whichcontributetothesubjectiveeupho-riaandrewardingeffectsassociatedwithalcohol.100Researchfindingsregardingacetylcholineandotherneurotransmittersaremixedandeffectsarecurrentlynotaswellunderstood.
Intense,chronicuseofalcoholhaswide-rangingdeleteri-ouseffectsonthebrain.Thesecanleadtolasting,sometimeslife-long, impairments in function that result in prodigiousfamilial,social,andfiscalcosts.Consequently,education,pre-vention,andearlydetectionandinterventionarekeystomini-mizingtheimpactonindividualsandtheirlovedones.
SCREENING AND ASSESSMENTGiventheregrettableimpactthatafailuretodetectandinter-vene with alcohol problems can have, routine screening foralcohol misuse should be standard in all clinical settings.Therearebriefandeffectivescreeningmeasuresthatcanyield
judgment,andproblem-solving,damageinthesebrainregionsmayrelatetoimpulsivityandsusceptibilitytoalcoholrelapseandmaybeparticularlynegativelyaffectedbyalcohol.94–96
Positron emission tomography (PET) has been used toanalyzealcohol’seffectsonvariousneurotransmittersystems,as well as on brain cell metabolism and blood flow withinthe brain. These studies in alcoholics have detected deficits,particularly in the frontal lobes (which are responsible fornumerous functions associated with learning and memory),aswellas in thecerebellum(whichcontrolsmovementandcoordination).97–99
Effects on NeurotransmittersThetypicalsubjectiveeffects fromalcohol includeeuphoria,disinhibition, anxiety reduction, sedation, and sleep. Theseeffectsaremediatedbyavarietyofneurotransmittersinclud-ingGABA,glutamate,serotonin,endorphins,anddopamine.Alcohol effects neurotransmitter systems by causing eitherneuronal excitation or inhibition.100 If alcohol is consumedoverextendedperiods(e.g.,severaldaysorweeks),receptorsadapttoitspresence,producingneurotransmitterimbalancesthat can result in sedation, agitation, depression, and othermoodandbehaviordisorders,aswellasseizures.
Theresultsofneuropsychologicaltestingrevealthatshort-termmemory,performanceoncomplexmemorytasks,visual-motor coordination, visual-spatial performance, abstractreasoning,andpsychomotordexterityaretheareasmostseri-ouslydamaged.Intelligencescoresoftendonotchange,andverbalskillsandlong-termmemoryoftenremainintact.Asaconsequence, it is possible for individuals to appear cogni-tivelyintactunlesstheyareadministeredneuropsychologicaltests.
Glutamateisthemajorexcitatoryneurotransmitterinthebrainanditissignificantlyeffectedbyalcohol.Alcoholinflu-ences the action of glutamate, and research has shown thatchronic, heavy alcohol consumption increases glutamatereceptorsitesinthehippocampusthatcaneffecttheconsoli-dationofmemoryandmayaccountfor“blackout”phenom-ena. Contrary to popular belief, blackouts are much morecommon among social drinkers than previously assumed.In a large sample of college student drinkers, more thanhalf (51%) reported blacking out at some point in theirlives,and40%reportedexperiencingablackoutintheprior
Figure 26-13. Alcohol’seffectonneurotransmittersystems.VTA,ventraltegmentalarea;PPT,pedunculopontinetegmentalnucleus;LDT,lat-erodorsal tegmental nucleus (From Gilpin NW, Koob GF. Neurobiology of alcohol dependence: focus on motivational mechanisms. National Institute on Alcohol Abuse and Alcoholism (NIAAA).)
Alcohol
Alcohol?
?
Nucleus accumbens
Glutamate inputs(e.g., from amygdala
PPT/LDT)
Alcohol
VTAinterneuron
+
Ventral tegmental area
Glutamate inputs(e.g., from cortex)
GABA
Dopamine
Dopamine
Opioidpeptides
Alcohol-RelatedDisorders 283
26
“Amnesia,”everwantedto/triedto“Cutdown”),isbriefandhasgoodpsychometricproperties,butsimilartotheCAGEisa“life-time”measureandlackssensitivitytodetecthazardousdrinking.TheMichiganAlcoholismScreeningTest(MAST)isanotherself-reportmeasurewithgoodpsychometricproper-ties,butislongerthantheAUDIT.
ForadolescentstheCRAFFTscreenisrecommended,whichis the acronym for having ever ridden in a CAR driven bysomeone (including yourself) who was “high” or had beenusingalcoholordrugs;everusedalcoholordrugstoRELAX,feelbetteraboutyourself,orfitin;everusealcoholordrugswhile ALONE; ever FORGOT things while using alcohol ordrugs;FAMILYorFRIENDSeverrecommendcuttingdownondrinkingordruguse;evergottenintoTROUBLEwhileusingalcoholordrugs.Thesequestionshaveexcellentsensitivityandspecificity.115Onepointisgivenforeachpositivelyendorseditemandascoreof2ormoreisindicativeofapotentialAUDthatrequiresfurtherassessment.Figure26-15showstheprob-abilityofanAUDbasedonderivedscreeningscore.
Medicalbiomarker screensmayalsobeuseful. Screeningfor recent alcohol use can be a carried out with a Breatha-lyzer or a sample of urine or saliva. For more chronic use,laboratorymarkers,suchastheserumγ-glutamyltranspepti-dase(GGT),themeancorpuscularvolume(MCV),20andthepercent carbohydrate-deficient transferrin (% CDT) can beused.CDTis thenewestalcoholbiomarkerapprovedbytheFood and Drug Administration (FDA) in 2001.116 It is theonlylaboratorytestapprovedspecificallyforthedetectionofheavy drinking.117 An average daily consumption of 60g ofalcoholormore(i.e.,approximately5standarddrinksintheUS)foratleasttheprevious2weekscausesahigherpercent-ageoftransferrin.CDT,quantifiedasapercentoftotalserumtransferring,ratherthantheabsolutelevelofCDT,isrecom-mendedas it corrects for individualvariations in transferrinlevels.Laboratorytestresultsofmorethan2.5%suggestheavy
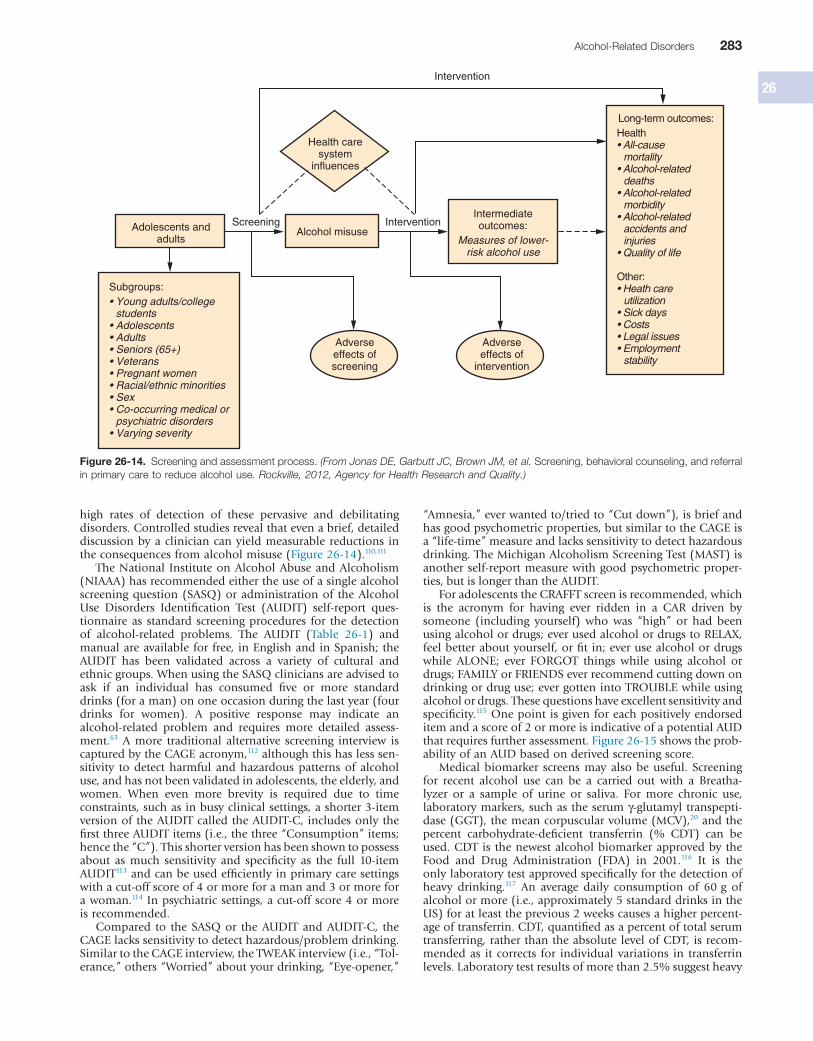
high rates of detection of these pervasive and debilitatingdisorders.Controlledstudiesrevealthatevenabrief,detaileddiscussionbyacliniciancanyieldmeasurable reductions intheconsequencesfromalcoholmisuse(Figure26-14).110,111
TheNational InstituteonAlcoholAbuseandAlcoholism(NIAAA)hasrecommendedeithertheuseofasinglealcoholscreeningquestion(SASQ)oradministrationof theAlcoholUse Disorders Identification Test (AUDIT) self-report ques-tionnaireas standard screeningprocedures for thedetectionof alcohol-related problems. The AUDIT (Table 26-1) andmanualareavailableforfree, inEnglishandinSpanish;theAUDIT has been validated across a variety of cultural andethnicgroups.WhenusingtheSASQcliniciansareadvisedtoask if an individual has consumed five or more standarddrinks(foraman)ononeoccasionduringthelastyear(fourdrinks for women). A positive response may indicate analcohol-related problem and requires more detailed assess-ment.63 A more traditional alternative screening interview iscapturedbytheCAGEacronym,112althoughthishaslesssen-sitivity to detect harmful and hazardous patterns of alcoholuse,andhasnotbeenvalidatedinadolescents,theelderly,andwomen. When even more brevity is required due to timeconstraints,suchasinbusyclinicalsettings,ashorter3-itemversionoftheAUDITcalledtheAUDIT-C,includesonlythefirstthreeAUDITitems(i.e.,thethree“Consumption”items;hencethe“C”).Thisshorterversionhasbeenshowntopossessabout as much sensitivity and specificity as the full 10-itemAUDIT113andcanbeusedefficientlyinprimarycaresettingswithacut-offscoreof4ormoreforamanand3ormoreforawoman.114Inpsychiatricsettings,acut-offscore4ormoreisrecommended.
Compared to theSASQor theAUDITandAUDIT-C, theCAGElackssensitivitytodetecthazardous/problemdrinking.SimilartotheCAGEinterview,theTWEAKinterview(i.e.,“Tol-erance,”others“Worried”aboutyourdrinking,“Eye-opener,”
Figure 26-14. Screeningandassessmentprocess.(From Jonas DE, Garbutt JC, Brown JM, et al. Screening,behavioralcounseling,andreferralinprimarycaretoreducealcoholuse. Rockville, 2012, Agency for Health Research and Quality.)
Intervention
Intervention
Health caresystem
influences
ScreeningAlcohol misuse
Intermediateoutcomes:
Measures of lower-risk alcohol use
Adolescents andadults
Adverseeffects ofscreening
Adverseeffects of
intervention
Subgroups:• Young adults/college
students• Adolescents• Adults• Seniors (65+)• Veterans• Pregnant women• Racial/ethnic minorities• Sex• Co-occurring medical or
psychiatric disorders• Varying severity
Long-term outcomes:Health• All-cause
mortality• Alcohol-related
deaths• Alcohol-related
morbidity• Alcohol-related
accidents and injuries
• Quality of life
Other:• Heath care
utilization• Sick days• Costs• Legal issues• Employment
stability
284 PART IX PsychiatricDisorders
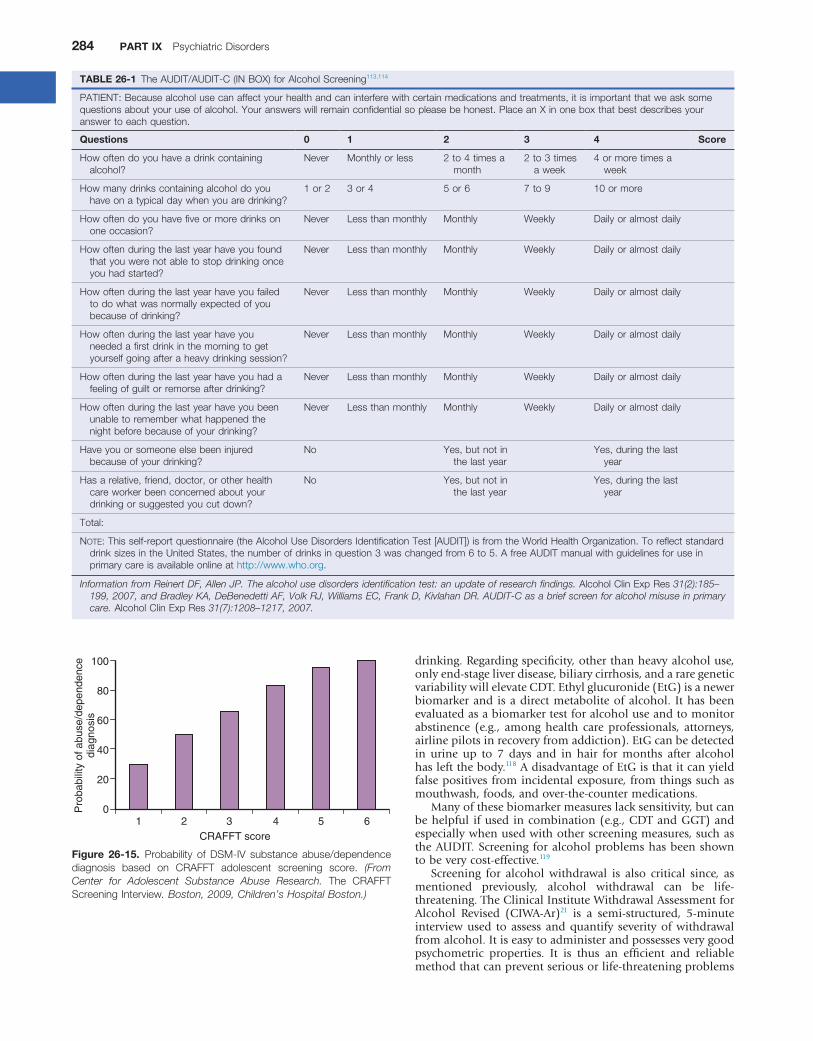
TABLE 26-1 TheAUDIT/AUDIT-C(INBOX)forAlcoholScreening113,114
PATIENT:Becausealcoholusecanaffectyourhealthandcaninterferewithcertainmedicationsandtreatments,itisimportantthatweasksomequestionsaboutyouruseofalcohol.Youranswerswillremainconfidentialsopleasebehonest.PlaceanXinoneboxthatbestdescribesyouranswertoeachquestion.
Questions 0 1 2 3 4 Score
Howoftendoyouhaveadrinkcontainingalcohol?
Never Monthlyorless 2to4timesamonth
2to3timesaweek
4ormoretimesaweek
Howmanydrinkscontainingalcoholdoyouhaveonatypicaldaywhenyouaredrinking?
1or2 3or4 5or6 7to9 10ormore
Howoftendoyouhavefiveormoredrinksononeoccasion?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Howoftenduringthelastyearhaveyoufoundthatyouwerenotabletostopdrinkingonceyouhadstarted?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Howoftenduringthelastyearhaveyoufailedtodowhatwasnormallyexpectedofyoubecauseofdrinking?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Howoftenduringthelastyearhaveyouneededafirstdrinkinthemorningtogetyourselfgoingafteraheavydrinkingsession?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Howoftenduringthelastyearhaveyouhadafeelingofguiltorremorseafterdrinking?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Howoftenduringthelastyearhaveyoubeenunabletorememberwhathappenedthenightbeforebecauseofyourdrinking?
Never Lessthanmonthly Monthly Weekly Dailyoralmostdaily
Haveyouorsomeoneelsebeeninjuredbecauseofyourdrinking?
No Yes,butnotinthelastyear
Yes,duringthelastyear
Hasarelative,friend,doctor,orotherhealthcareworkerbeenconcernedaboutyourdrinkingorsuggestedyoucutdown?
No Yes,butnotinthelastyear
Yes,duringthelastyear
Total:
NOTE:Thisself-reportquestionnaire(theAlcoholUseDisordersIdentificationTest[AUDIT])isfromtheWorldHealthOrganization.ToreflectstandarddrinksizesintheUnitedStates,thenumberofdrinksinquestion3waschangedfrom6to5.AfreeAUDITmanualwithguidelinesforuseinprimarycareisavailableonlineathttp://www.who.org.
Information from Reinert DF, Allen JP. The alcohol use disorders identification test: an update of research findings. AlcoholClinExpRes 31(2):185–199, 2007, and Bradley KA, DeBenedetti AF, Volk RJ, Williams EC, Frank D, Kivlahan DR. AUDIT-C as a brief screen for alcohol misuse in primary care. AlcoholClinExpRes 31(7):1208–1217, 2007.
Figure 26-15. Probability of DSM-IV substance abuse/dependencediagnosis based on CRAFFT adolescent screening score. (From Center for Adolescent Substance Abuse Research. The CRAFFTScreeningInterview. Boston, 2009, Children’s Hospital Boston.)
100
80
60
40
20
01 2 3 4 5 6
CRAFFT score
Pro
babi
lity
of a
buse
/dep
ende
nce
diag
nosi
s
drinking.Regardingspecificity,otherthanheavyalcoholuse,onlyend-stageliverdisease,biliarycirrhosis,andararegeneticvariabilitywillelevateCDT.Ethylglucuronide(EtG)isanewerbiomarkerand isadirectmetaboliteofalcohol. Ithasbeenevaluatedasabiomarkertestforalcoholuseandtomonitorabstinence (e.g., among health care professionals, attorneys,airlinepilotsinrecoveryfromaddiction).EtGcanbedetectedin urine up to 7 days and in hair for months after alcoholhasleftthebody.118AdisadvantageofEtGisthatitcanyieldfalsepositivesfromincidentalexposure,fromthingssuchasmouthwash,foods,andover-the-countermedications.
Manyofthesebiomarkermeasureslacksensitivity,butcanbehelpful ifused incombination(e.g.,CDTandGGT)andespeciallywhenusedwithotherscreeningmeasures,suchastheAUDIT.Screeningforalcoholproblemshasbeenshowntobeverycost-effective.119
Screening for alcohol withdrawal is also critical since, asmentioned previously, alcohol withdrawal can be life-threatening.TheClinicalInstituteWithdrawalAssessmentforAlcohol Revised (CIWA-Ar)21 is a semi-structured, 5-minuteinterviewused toassess andquantify severityofwithdrawalfromalcohol.Itiseasytoadministerandpossessesverygoodpsychometric properties. It is thus an efficient and reliablemethodthatcanpreventseriousorlife-threateningproblems

Alcohol-RelatedDisorders 285
26on these problems. These range from brief interventions tomore intensive and extensive individual and group-basedpsychosocial interventions and, increasingly, pharmacologi-calinterventions.134
Brief InterventionA concerned and focused assessment with brief advice by ahealthcareprovidercanmakeapositivedifferencetodrinkingproblems. Brief interventions are generally recommendedforthosewhodrinktoexcess,butaregenerallynotshowingsignsofaddiction.Thus, its goalmaybemoderatedrinkingratherthanabstinence.135–137Briefinterventionsaregenerallyrestrictedtofourorfewersessions,lastingfromafewminutesto1houreach,designed tobe conductedbyclinicians,notnecessarilyspecializedinaddiction.138
Research indicates that brief interventions for alcoholproblems are more effective than no intervention139–142 and,in some cases, can be as effective as more extensive inter-vention.135,143Capitalizingonthesefindings,andinordertoexpandaccesstotreatmentforalcohol-relatedproblems,theCenterforSubstanceAbuseTreatment(CSAT)hasdevisedaninitiative known as “Screening, Brief Intervention, Referral,andTreatment”(SBIRT).Thegoaloftheinitiativeisintendedto shift theemphasis toalcoholuserswhomthe traditionalsystemhas largely ignored—thelargenumberof individualswho consume more than the medically-accepted limits butarenotyetdependent.Rejectingthenotionthatonlypeoplewithveryheavyalcoholuselevelsorwhoarealcoholdepend-ent need targeted interventions, SBIRT assumes that every-one, regardlessofcurrent levelofalcoholconsumption,canbenefit fromlearning the factsabout safealcoholconsump-tionandknowinghowtheirownusagecomparestoacceptedlimits.UsingtheAUDIT/AUDIT-Casascreeningdevice,front-line clinicians in any setting can assess for alcohol-relatedproblemsquicklyandeasily.SBIRTtriageguidelinesproviderecommendations along the linesof an individual’s alcoholinvolvement. Simple clinical advice to cut down or stop isrecommended if someone scores between 7 and 16 on theAUDIT;multiplesessionsofbrief treatmentandmonitoringarerecommendedifanindividualscoresbetween16and19(orhas consumedalcohol to intoxicationfiveormoredaysper month, as disclosed on screening interview); and if anindividual has an AUDIT score of 20 or more a referral formoreintensiveassessmentandtreatmentisrecommended.144
Whatisitaboutbriefinterventionsthatmakethemeffec-tive?After reviewing thekey ingredients inavarietyofbriefintervention protocols, Miller and Sanchez145 proposed sixcritical elements that they summarized with the acronymFRAMES: Feedback, Responsibility, Advice, Menu, Empathy,and Self-efficacy. The clinician completes some assessmentandprovidesFeedbackonthepatient’salcohol-relatedprob-lems(“Yourresultsshow.…”),stressesthepatient’sRespon-sibility toaddress theproblem(“It’syourchoice.…”),givesclear Advice to change drinking behavior (“I would recom-mend that you cut down or stop. …”), provides a Menu oftreatmentstrategies(“Thereanumberofdifferentthingsyoumightdo.…”),expressesEmpathyforthepatient’sproblem(“This can be difficult to hear and making changes is notalwayseasy,but.…”),andstressesSelf-efficacy(“However,itisquitepossibleforyoutoachievethis.…”)—theexpectationisthatthepatienthastheskillsneededtosuccessfullyresolvehisorherdrinkingproblems.Additionalcomponentsofgoal-setting, follow-up, and timing also have been identified asimportanttotheeffectivenessofbriefinterventions.136,146Evenbriefcontactwithanaddictionspecialisthasbeenshowntoyieldimprovementin30%to50%ofpatients.However,briefinterventionsaremoreeffectivewiththosewhohavenoprior
and is useful to help clinicians determine levels of care.21Recentevidencesuggests,however,thatthisscalemayunder-estimate symptoms of alcohol withdrawal in certain ethnicgroups,suchasNativeAmericans.120
Thereareseveralmeasuresthatcanbeemployedtoassessthe presence of an AUD and the degree of dependence andimpairment. The choice of each may depend on the timedemandsandspecializationoftheclinicalsetting.Forclinicaldiagnostic purposes, the Structured Clinical Interview forDiagnosis (SCID), Substance Use Disorders module, can beused.Thisisavalidandreliable,semi-structured,assessmenttoolthatwillgivelife-timeandcurrentdiagnosesforAUDandcan be completed in approximately 20 minutes.121 Also, asdetailedmorebelowinthesectiononBriefInterventions,theAlcoholUseDisorders IdentificationTest (AUDIT)122 canbeused as a screening tool and to help determine treatmentrecommendations.
The Addiction Severity Index (ASI) is a semi-structuredinterview that assesses multiple domains of function (e.g.,legal,work,andpsychiatric,aswellasalcoholanddruguse)and is widely used in clinical and research settings. It hasadequate psychometrics and can be completed in approxi-mately 30 to 40 minutes. The Alcohol Dependence Scale(ADS)isaself-reportmeasurethatfocusesonthecoredepend-encesyndrome.Itcontains25itemsandtakesapproximately5minutestocomplete.Itassessespast-yearsymptoms,withascoreof9ormoreindicativeofalcoholdependence.TheLeedsDependenceQuestionnaire(LDQ)123,124isabrief10-itemself-reportmeasurethatmeasuresseverityofaddictionacrossmul-tiplesubstances,includingalcohol.TheDrinkerInventoryofConsequences(DRINC)isa50-item,multi-dimensionalself-reportthattakesabout5minutestocomplete.Itisavalidatedmeasure of drinking consequences with good psychometricproperties. There are a variety of other assessment toolsavailable that assess drinking topography, chronicity, andimpact.125,126 Many of these measures have clinical utility astheycanelucidatethedrinkingtopography,chronicity,addic-tion severity, and degree of impairment that can informthe type and level of treatment intensity.127 Also, these maybecome increasingly important as health systems move toperformance-basedpayments.128
TREATMENT FOR ALCOHOL USE DISORDERSAs with most difficulties that individuals encounter duringtheirlives,individualssufferingfromAUDsfirsttrytoresolvetheir problems without help. They may mobilize their ownskillsand,throughaprocessoftrialanderror,learnwaystominimizeorresolvetheseproblems.Successfulresolutionofan alcohol problem without formal intervention is oftencalled “natural recovery”.129 Others use informal resources,suchasamemberoftheclergy,afriend,orafamilymember,oraccessAlcoholicsAnonymous(AA)oranothermutual-helpgroup.Whentheseresourcesarerealizedtobeinsufficienttocope with the magnitude of the problem, individuals oftenseekformaltreatment,althoughinformalresources(e.g.,AA)maycontinuetobeusedaseffectiveadjuncts.130,131
Giventhevariabilityinthedemographicanddrinkingpat-ternsofpatients,and theaddictionseverityand impact thatalcohol use has had in their lives, a number of treatmentoptions should be available to help patients.2 The NationalInstitute of Alcohol Abuse and Alcoholism (NIAAA) wasfounded in 1970. This began a federally supported publichealth initiative that increased research efforts to develop,test, and implement effective interventions for risky alcoholuse,aswellasforabuseanddependence.Numerousreviewsof the treatment literature132–135 indicate thatawidearrayofempirically-based,effectivetreatmentscanbebroughttobear

286 PART IX PsychiatricDisorders
interviewing153 are a particularly useful framework in thisregardandhavestrongempiricalsupportforuseamongindi-vidualswithAUDs(Table26-2).Themainprinciplesherearetoavoidarguingwithapatient,to“rollwithresistance”(e.g.,trytounderstandthepatients’frameofreference),todevelopdiscrepancies between the patient’s values and his or herbehavior, to support the patient’s self-efficacy/confidence toachieve thedesiredoutcome,and tobeempathic.Therearefour main processes of MI: engaging (establishing a helpfulconnectionandworking relationship), focusing (developingandmaintainingspecificdirectionintheconversationaboutchange), evoking (eliciting the patients’ own motives aboutchange), and planning (developing commitment to changeandformingaspecificactionplantochange).146
Emanating from the brief intervention literature andhumanistic psychology, motivational interviewing has beenshowntobeanimportantandeffectivewaytointeractwithpatientswitharangeofalcoholproblems,includingdepend-ence. Ithasbeendefinedasapatient-centered,yetdirective,method for enhancing intrinsic motivation to change byexploringandresolvingpatientambivalence.153Thisapproachhasbeenshowntobehelpfulformanypatients.161–163Itcanbeusedasastand-aloneinterventionbutcanalsobeaneffec-tivewaytocommunicatewithpatientswhileprovidingotherinterventions.
Studiesoftreatmentoutcomeshowthatpatientstreatedforaddictionhavesimilarratesofimprovementaspatientstreatedfor other chronic medical diseases.164 For example, between40% and 60% of patients treated for addiction to alcoholremainabstinentafterayearandanother15%maintainclini-callymeaningfulimprovementintheiralcoholuseproblems.Similarly, during the course of a year, 60% of patients withhighbloodpressureorasthmaand70%ofdiabeticsmaintainimprovements in their symptoms.39,165 While full remissionandrecoverycantakemanyyearstoachievefollowinginitialattemptstostop,166fullsustainedremissionisthemostlikelyultimateoutcome.167Consequently,AUDcanbeconsideredagoodprognosisdisorderwithadequateextensivemonitoring,management,andre-interventionwhennecessary.46
Engagingandretainingindividualsintreatmentforatleast90 days is associated with better long-term treatment out-comes.168Individualorgroupcounselingandotherbehavioraltherapies are critical components of effective treatment foralcoholaddiction.Behavioraltherapyalsofacilitatesinterper-sonalrelationshipsandtheindividual’sabilitytofunctioninthefamilyandcommunitycontexts.Intherapy,issuesofmoti-vationcanbeaddressed,andassertiveness,goal-settingskills,andproblem-solvingstrategiescanbelearnedalongwithnewwaystoreplacealcohol-relatedactivitieswithotherconstruc-tiveandrewardingactivities.
Pharmacological InterventionsThree medications have been approved by the FDA for thetreatment of alcohol dependence: disulfiram (approved in1947), intended to prevent any drinking through the
psychiatricillnessorhistoryofaddictiontreatmentandgoodsocialfunctionandresources.147Althoughnon-specialistclini-cians,suchasprimarycareproviders,canhaveanimpactonheavyorat-riskdrinkingthroughappropriatebrief interven-tion, patients with alcohol dependence tend to experiencebetter outcomes when seen by addiction specialists (e.g.,counselors, social workers, and addiction-trained nurses, orphysicians with specialized addiction training) than generalpractitioners,148,149perhapsdue to theirmore specificeduca-tionandtrainingonaddiction.Forexample,comparedwithgeneral consultation psychiatrists, specialist addiction nurseconsultantswerefoundtodoubletherateofpatientfollow-throughandcompletioninrehabilitation.150
Intensive-Extensive InterventionsThreebroadelementsareimportantinrecoveryfromAUDs:deconditioning,skillstraining,andcognitivere-structuring.151There is a broad array of evidence-based interventions forAUDs that address these critical elements.132,133,152 Some ofthese include Twelve-Step Facilitation (TSF), a professionaltherapy designed to engage patients and support long-terminvolvement in the fellowshipofAA;motivationalenhance-menttherapy(MET),aninterventionbasedontheprinciplesof motivational interviewing146,153; a variety of cognitive-behavioral approaches, such as the Community Reinforce-mentApproach(CRA),designedtoengagemultipletherapeuticelementsinthecommunity;interpersonalsystem-basedinter-ventions,suchasbehavioralmaritaltherapy(BMT)andfamilytherapies; and pharmacotherapies (e.g., naltrexone/depotnatrexone,acamprosate,ordisulfiram).
Although most interventions are directly focused on theprimarysufferer(theindividualwiththeAUD),itisclearthatloved ones also suffer greatly as a result of the AUD. Com-munityReinforcementandFamilyTraining(CRAFT)isavali-dated approach based on the concept that a supportiveenvironment “community” will help the alcohol-dependentpersonachieverecovery.CRAFTtargetsindividualswhorefuseto participate in treatment through their loved ones. It pro-videsspecific,contingency-basedstrategiesthatsupportfamilymembersandfriendsintheirefforts tohelptheir lovedonebecomeengagedintreatment.Ithasbeenshownalsotosub-stantiallyreducepsychologicaldistressandsymptomsamongthefamilymembersthemselves.154
Despitevastlydiffering theoreticalassumptions regardingthespecificsoftreatmentcontent,andforhowlong,atwhatintensity, and by whom the treatment should be delivered,comparisonsoftherelativeefficacyofactivetreatmentsrevealsurprisinglysimilareffects,suggestingthattheymayallmobi-lizecommonchangeprocesses.155However,itseemsclearthatit istheduration and continuityofcarethatislinkedtotreat-mentoutcomeratherthanamountorintensity.46,155–157Con-sequently, there have been recent shifts from intensiveinpatient services to“extensive”outpatientmodelsofaddic-tion recovery management and ongoing assessment andre-interventionthatmatchthechronicrelapse-pronenatureofaddictivedisorders(e.g.,telephonecasemonitoringandlong-termoutpatienttreatment).158–160
Inrecentyears,therehastendedtobeanalmostexclusivefocus on high-fidelity delivery of manualized treatmentcontentratherthanafocusonthecharacteristicsoftheclini-cian who delivers the content and how it is delivered. Theissue of therapeutic alliance and successfully gaining thepatient’strustisoftenfundamentaltothesuccessoftreatment,yet is seldom specifically addressed. A respectful, empathic,patient-centeredapproachappearstobemosthelpful,andaharsh, confrontational approach may increase the patient’sresistance.132 The principles and practices of motivational
TABLE 26-2 MotivationalInterviewingProcesses
Engaging Establishingahelpfulconnectionandworkingrelationship
Focusing Developingandmaintainingspecificdirectionintheconversationaboutchange
Evoking Elicitingthepatients’ownmotivesaboutchangePlanning Developingcommitmenttochangeandforming
aspecificactionplantochange
From Miller WR, Rollnick S. Motivationalinterviewing:helpingpeoplechange, ed 3. New York, 2012, Guilford Press.

Alcohol-RelatedDisorders 287
26
SSRIs have produced only modest drinking reductions—independent of antidepressant effects—through an anti-cravingeffect.Thiseffectmaybemoreapparentinmenwithdepression and late-onset alcoholism.76,77 The SSRIs do notappeartohaveanyrelapse-preventioneffectinwomen.Recentdouble-blindplacebo-controlledstudieshaveshownefficacyforondansetroninearly-onsetalcoholicsandtopiramatehasshownpromise as an effectivepharmacotherapy for alcoholdependenceinabroadrangeofalcohol-dependentindividu-als.176,177 All of these agents are gaining renewed interest asadjuncts to a comprehensive psychosocial recovery programandshouldbeconsideredinthetreatmentofallindividualswithAUD.
Substance-induced psychiatric symptoms are commonbefore admission fordetoxificationandmaypersist for2–4weeksafterdetoxification.70,71Ifsymptomscontinueforlongerthan 4 weeks, it suggests the existence of an independentco-occurringpsychiatricdisorder.Inthesesituations,aspecificpsychiatric treatment plan is required to address theco-occurringdisorder.StudiessupportinitiationofanSSRIforco-occurring major depression, mood stabilizers for bipolarillness, buspirone for generalized anxiety, and second-generation antipsychotics for a psychotic illness.178 The bestoutcomesareseenwhentreatmentforanyco-occurringpsy-chiatric disorder is integrated into the addiction recoveryprogram.69,179
Alcoholics Anonymous and Long-term SupportAs with other chronic illnesses, relapses to alcohol use canoccur during or after successful treatment episodes. Hence,addicted individuals often require prolonged treatment andmultipleepisodesofcaretoachievelong-termabstinenceandfullyrestoredfunction.Participationinmutual-helporganiza-tions,suchasAA,duringandfollowingtreatmentisoftenalsohelpful and cost-effective in helping patients achieve andmaintainrecovery.180–186OtherorganizationssuchasSMARTRecovery,SecularOrganization forSobriety,andWomen forSobrietyarealsolikelytobehelpfultomanypatients,butareless available and little is known about their effective-ness.181,184,185,187 A recent randomized comparative trial,however,foundbenefitforproblem-drinkerswhowererand-omizedtoreceiveeitheranon-linecognitive-behavioralinter-ventionfeaturingtheelementsofSMARTRecovery,attendanceat SMART Recovery meetings, or both, and found that allgroupsimprovedsignificantlyacrossthe3-monthfollow-up.188
AApossessesseveralelementsthatmakeitattractiveasanongoingadjuncttoformalAUDtreatment.Itisaccessibleandflexible,withmeetingsheldseveraltimesadayinmanycom-munities,andpatientscanself-selectmeetingsthatseemlikeagoodfit.AAmembersalsooftenmakethemselvesavailable“ondemand”(e.g.,bytelephone),providingadegreeofflex-ibility not available in professional settings. This degree ofavailabilitymeansthatAAisself-adaptive:patientscanaccesstheseresourcesattimesofhighrelapserisk(e.g.,unstructured
anticipated threat of the very unpleasant reaction caused bythe alcohol–disulfiram interaction; naltrexone (approved asan oral formulation in 1994 with the long-acting injectableformulationapprovedin2006),intendedtoreducetherein-forcingeffectofalcoholandtoreducetheseverityofrelapseandtheextentofheavydrinking;andacamprosate(approvedin2004),intendedtoreducetheprobabilityofanydrinkingbyreducingsymptomsassociatedwithpostacutewithdrawal/cravingfollowinginitialdetoxification(Table26-3).
Disulfiraminhibitsacetaldehydedehydrogenase,leadingtoabuild-upoftheethanolmetaboliteacetaldehyde.Ithasbeenshowntoreducedrinkingdaysinalcohol-dependentpersonsby approximately 50%.169 If a patient drinks alcohol aftertaking disulfiram, the build-up of acetaldehyde producesflushing,hypotension,headache,nausea,andvomiting(Table26-3).Treatmentofseveredisulfiram–ethanolreactionsmayrequireamodifiedTrendelenburgposition,ananticholinergicagentforbradycardia,andascorbicacid1mgIVevery1to2hours.Theeffectivenessofdisulfiramiscompromisedbypoorcompliance.However,ifaspouseorsignificantotheriswillingto participate and to observe and monitor the compliancewith the medication, effectiveness increases substantially. Awritten contract in this regard between spouse and partner,which is often done in behavioral marital therapy (BMT),enhancescomplianceandoutcomes.170–172
The opiate antagonist naltrexone which has no specificadverse reaction with alcohol has produced reductions indrinking-days presumably through diminished reward fromalcohol secondary to actions on central brain reward path-ways.173,174TherecentFDA-approvalforalong-actingIMfor-mulation of naltrexone in April 2006 significantly expandspharmacotherapyoptions.Bestresultshavebeenreportedinpatients able to sustain a week of abstinence before theirfirstinjection.Naltrexonealsoappearstobemosteffectiveinpatientswitha strong familyhistoryofalcoholism.Becausebothnaltrexoneanddisulfiramhaveaslightriskforhepato-toxicity, liver function studies are recommended at baselineandthenat1,3,andevery6monthsthereafter.Also,pharma-cogeneticresearchsuggeststhatindividualswiththeOPRM1genotypemayrespondparticularlywelltonaltrexone.175
Acamprosate is another drug that has been approved forrelapse-preventionamongindividualssufferingfromalcoholaddiction. It is thought toactprimarilyatglutamate-NMDAreceptors by moderating symptoms related to prolongedalcoholwithdrawal(i.e.,post-acutewithdrawal),and is thusmosteffectiveinpatientswhohaverecentlycompleteddetoxi-fication. It is preferred for patients with liver damage sinceacamprosateismetabolizedthroughthekidneysandnottheliver. Meta-analyses suggest that, in keeping with the pur-portedmechanismsofactionofnaltrexoneandacamprosate,naltrexone has stronger effects on reducing heavy drinking(presumably through diminishing alcohol’s mu opioidreceptor-mediated rewarding effects), while acamprosate isbetteratincreasingcompleteabstinence(presumablythroughattenuatingreboundglutamate-NMDAmediatedexcitation).
TABLE 26-3 PharmacologicalTreatmentsforAlcoholism
Drug (Trade Name) Pharmacokinetics/Pharmacodynamics Effects
Disulfiram(Antabuse) Inhibitsacetaldehydedehydrogenase,leadingtoabuild-upofacetaldehyde
Producesundesirableconsequenceswhenalcoholisconsumed,includingflushing,palpitations,nausea,vomiting,andheadache
Naltrexone(ReVia,Longacting=Vivitrol)
µ-opioidreceptorantagonist Reducesthereinforcement/euphoriaproducedbyalcohol
Acamprosate AntagonistatglutamatergicN-methyl-D-aspartate(NMDA)receptorsandagonistatgamma-aminobutyricacid(GABA)typeAreceptors
Reducesalcoholcravings
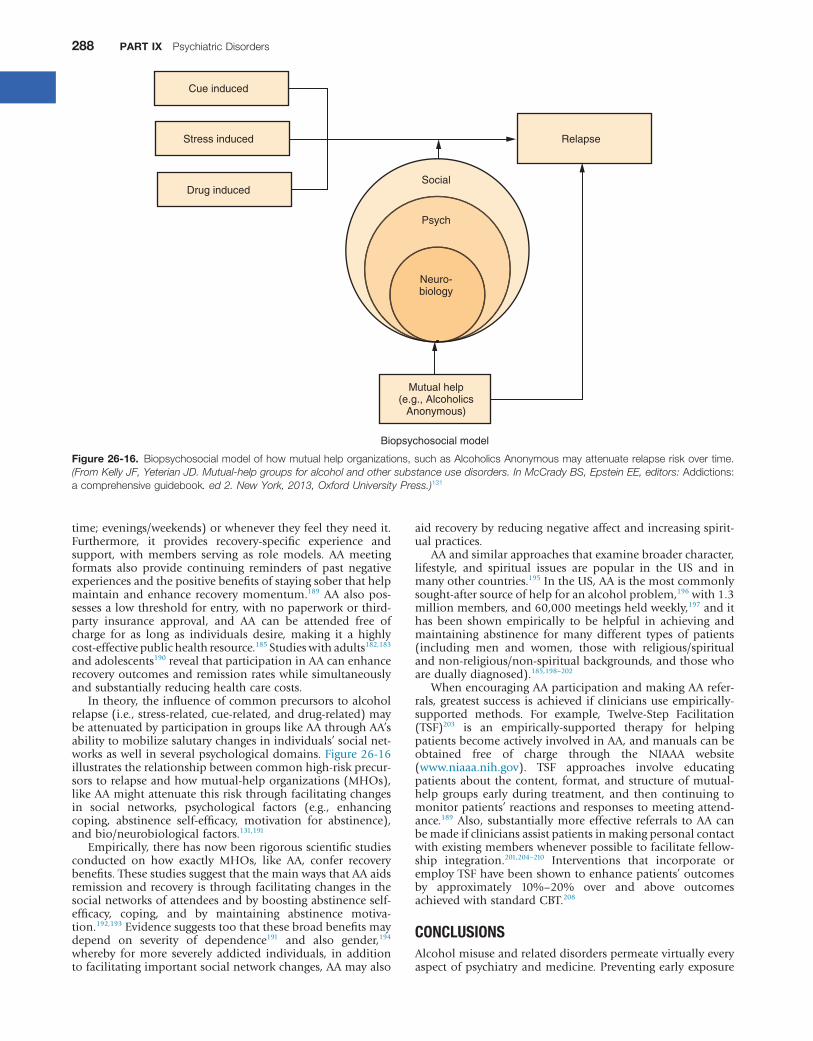
288 PART IX PsychiatricDisorders
aidrecoverybyreducingnegativeaffectandincreasingspirit-ualpractices.
AAandsimilarapproachesthatexaminebroadercharacter,lifestyle, and spiritual issues are popular in the US and inmanyothercountries.195IntheUS,AAisthemostcommonlysought-aftersourceofhelpforanalcoholproblem,196with1.3millionmembers,and60,000meetingsheldweekly,197andithas been shown empirically to be helpful in achieving andmaintaining abstinence for many different types of patients(including men and women, those with religious/spiritualandnon-religious/non-spiritualbackgrounds,andthosewhoareduallydiagnosed).185,198–202
WhenencouragingAAparticipationandmakingAArefer-rals,greatestsuccess isachievedifcliniciansuseempirically-supported methods. For example, Twelve-Step Facilitation(TSF)203 is an empirically-supported therapy for helpingpatientsbecomeactivelyinvolvedinAA,andmanualscanbeobtained free of charge through the NIAAA website(www.niaaa.nih.gov). TSF approaches involve educatingpatientsabout thecontent, format,andstructureofmutual-help groups early during treatment, and then continuing tomonitorpatients’reactionsandresponsestomeetingattend-ance.189Also, substantiallymoreeffective referrals toAAcanbemadeifcliniciansassistpatientsinmakingpersonalcontactwithexistingmemberswheneverpossibletofacilitatefellow-ship integration.201,204–210 Interventions that incorporate oremployTSFhavebeenshowntoenhancepatients’outcomesby approximately 10%–20% over and above outcomesachievedwithstandardCBT.208
CONCLUSIONSAlcoholmisuseandrelateddisorderspermeatevirtuallyeveryaspectofpsychiatryandmedicine.Preventingearlyexposure
time;evenings/weekends)orwhenevertheyfeeltheyneedit.Furthermore, it provides recovery-specific experience andsupport, with members serving as role models. AA meetingformats also provide continuing reminders of past negativeexperiencesandthepositivebenefitsofstayingsoberthathelpmaintainandenhance recoverymomentum.189AAalsopos-sessesalowthresholdforentry,withnopaperworkorthird-party insurance approval, and AA can be attended free ofcharge for as long as individuals desire, making it a highlycost-effectivepublichealthresource.185Studieswithadults182,183andadolescents190revealthatparticipationinAAcanenhancerecoveryoutcomesandremissionrateswhilesimultaneouslyandsubstantiallyreducinghealthcarecosts.
Intheory,theinfluenceofcommonprecursorstoalcoholrelapse(i.e.,stress-related,cue-related,anddrug-related)maybeattenuatedbyparticipationingroupslikeAAthroughAA’sabilitytomobilizesalutarychangesinindividuals’socialnet-worksaswellinseveralpsychologicaldomains.Figure26-16illustratestherelationshipbetweencommonhigh-riskprecur-sorstorelapseandhowmutual-helporganizations(MHOs),likeAAmightattenuatethisriskthroughfacilitatingchangesin social networks, psychological factors (e.g., enhancingcoping, abstinence self-efficacy, motivation for abstinence),andbio/neurobiologicalfactors.131,191
Empirically,therehasnowbeenrigorousscientificstudiesconducted on how exactly MHOs, like AA, confer recoverybenefits.ThesestudiessuggestthatthemainwaysthatAAaidsremissionandrecoveryisthroughfacilitatingchangesinthesocialnetworksofattendeesandbyboostingabstinenceself-efficacy, coping, and by maintaining abstinence motiva-tion.192,193Evidencesuggeststoothatthesebroadbenefitsmaydepend on severity of dependence191 and also gender,194whereby for more severely addicted individuals, in additiontofacilitatingimportantsocialnetworkchanges,AAmayalso
Figure 26-16. Biopsychosocialmodelofhowmutualhelporganizations,suchasAlcoholicsAnonymousmayattenuaterelapseriskovertime.(From Kelly JF, Yeterian JD. Mutual-help groups for alcohol and other substance use disorders. In McCrady BS, Epstein EE, editors: Addictions:acomprehensiveguidebook. ed 2. New York, 2013, Oxford University Press.)131
Cue induced
Stress induced
Drug induced
Relapse
Social
Mutual help(e.g., Alcoholics
Anonymous)
Psych
Neuro-biology
Biopsychosocial model

Alcohol-RelatedDisorders 289
2694. EverittBJ,RobbinsTW.Neuralsystemsofreinforcementfordrug
addiction:fromactionstohabitstocompulsion.Nature Neurosci8(11):1481–1489,2005.
110. Fleming MF. Brief interventions and the treatment of alcoholuse disorders: current evidence. Rec Dev Alcohol 16:375–390,2003.
130. Kelly JF,YeterianJD.Empiricalawakening: thenewscienceonmutualhelpandimplicationsforcostcontainmentunderhealthcarereform.Subst Abus33(2):85–91,2012.
131. KellyJF,YeterianJD.Mutual-helpgroupsforalcoholandothersubstance use disorders. In McCrady BS, Epstein EE, editors:Addictions: A comprehensive guidebook, ed 2, New York, 2013,OxfordUniversityPress.
133. MoyerA,FinneyJW,SwearingenCE,etal.Briefinterventionsforalcoholproblems:ameta-analyticreviewofcontrolledinvestiga-tions in treatment-seeking and non-treatment-seeking popula-tions.Addiction97(3):279–292,2002.
134. Maisel NC, Blodgett JC, Wilbourne PL, etal. Meta-analysis ofnaltrexoneandacamprosate for treatingalcoholusedisorders:whenarethesemedicationsmosthelpful?Addiction108(2):275–293,2013.
138. MadrasBK,ComptonWM,AvulaD,etal.Screening,briefinter-ventions,referraltotreatment(SBIRT)forillicitdrugandalcoholuse at multiple healthcare sites: comparison at intake and 6monthslater.Drug Alcohol Depend99(1–3):280–295,2009.
157. White WL. Recovery management and recovery-oriented systems of care: scientific rationale and promising practices, 2008, NortheastAddiction Technology Transfer Center, Great Lakes AddictionTechnologyTransferCenter,PhiladelphiaDepartmentofBehav-ioralHealth/MentalRetardationServices.
158. Dennis ML, Scott CK. Four-year outcomes from the EarlyRe-Intervention (ERI) experiment using Recovery ManagementCheckups(RMCs).Drug Alcohol Depend121(1–2):10–17,2012.
164. McClellan A, Lewis D, O’Brien C, etal. Drug dependence, achronic medical illness: implications for treatment, insurance,andoutcomesevaluation.JAMA284(13):1689–1695,2000.
167. White WL. Recovery/remission from substance use disorders: An analysis of reported outcomes in 415 scientific reports, 1868–2011,2012,PhiladelphiaDepartmentofBehavioralHealthandIntel-lectual disability Services, Great Lakes Addiction TechnologyTransferCenter.
181. HumphreysK.Circles of recovery: self-help organizations for addic-tions,Cambridge,UK,2004,CambridgeUniversityPress.
187. Kelly JF, White W. Broadening the base of addiction recoverymutualaid.J Groups Addict Recover7(2–4):82–101,2012.
192. KellyJF,MagillM,StoutRL.Howdopeoplerecoverfromalcoholdependence?AsystematicreviewoftheresearchonmechanismsofbehaviorchangeinAlcoholicsAnonymous.Addict Res Theory17(3):236–259,2009.
194. KellyJF,HoeppnerB.DoesAlcoholicsAnonymousworkdiffer-ently for men and women? A moderated multiple-mediationanalysisinalargeclinicalsample.Drug Alcohol Depend130(1–3):186–193,2013.
toalcoholamongyouth,minimizingheavyuse,andscreeningfor thepresenceof alcohol-induced, andalcoholuse,disor-derscanhelppreventanarrayofacuteandchronicdebilitat-ingmorbiditiesand lossof life.Anenhancedsensitivity for,andappreciationof,themagnitudeandpervasivenessofalco-hol’seffectsonmentalandphysicalfunctionshouldadvancethe use of routine assessment and appropriate interventionthatcanleadtosimilarlywidespreadindividual,family,andsocietalbenefits.
Access the complete reference list and multiple choice questions (MCQs) online at https://expertconsult.inkling.com
KEY REFERENCES4. Babor TF, Caetano R, Casswell S, etal. Alcohol: no ordinary
commodity-research and public policy, ed 2, Oxford, UK, 2010,OxfordUniversityPress.
6. BagnardiV,RotaM,BotteriE,etal.Lightalcoholdrinkingandcancer:ameta-analysis.Ann Oncol24(2):301–308,2013.
8. U.S. Department of Health and Human Services and U.S.Department of Agriculture. Dietary Guidelines for Americans,2005,Washington,DC,2005,HHSandUSDA.
11. World Health Organization. Global status report on alcohol and health,Geneva,Switzerland,2011,WorldHealthOrganization.
12. Bouchery EE, Harwood HJ, Sacks JJ, etal. Economic costs ofexcessivealcoholconsumptionintheU.S.2006.Am J Prev Med41(5):516–524,2011.
26. RosensonJ,ClementsC,SimonB,etal.Phenobarbitalforacutealcohol withdrawal: a prospective randomized double-blindplacebo-controlled study. J Emerg Med 44(3):592–598, e592,2013.
32. Isenberg-GrzedaE,KutnerHE,NicolsonSE.Wernicke–Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics53(6):507–516,2012.
45. KellyJF,WesterhoffCM.Doesitmatterhowwerefertoindividu-als with substance-related conditions? A randomized study oftwocommonlyusedterms.Int J Drug Policy21:202–207,2010.
46. Kelly JF, White WL, eds. Addiction Recovery Management. InRosenbaumJF,editor:Current clinical psychiatry,NewYork,2011,Springer.
47. SchuckitMA.Anoverviewofgenetic influences inalcoholism.J Subst Abuse Treat36(1):S5–S14,2009.
57. UrbanoskiKA,KellyJF.Understandinggeneticriskforsubstanceuseandaddiction:aguidefornon-geneticists.Clin Psychol Rev32(1):60–70,2012.
58. SchuckitMA.Vulnerability factors for alcoholism,Baltimore,2002,LippincottWilliams&Wilkins.
63. NationalInstituteonAlcoholAbuseandAlcoholism(NIAAA).Helping patients who drink too much: a clinician’s guide and related professional support services: National Institute on Alcohol and Alco-holism,Washington,DC,2005,USDHHS.
81. DawsonDA,GrantBF,StinsonFS,etal.RecoveryfromDSM-IValcohol dependence: United States, 2001–2002. Addiction100(3):281–292,2005.

Alcohol-RelatedDisorders 289.e1
26REFERENCES1. EdwardsG.Alcohol: the world’s favorite drug,NewYork,2000,St
Martin’sPress.2. InstituteofMedicine.Broadening the base of treatment for alcohol
problems,Washington,DC,1990,NationalAcademyPress.3. Goodwin DW, Crane JB, Guze SB. Alcoholic “blackouts”: a
review and clinical study of 100 alcoholics. Am J Psychiatry126(2):191–198,1969.
4. Babor TF, Caetano R, Casswell S, etal. Alcohol: no ordinary commodity-research and public policy, ed 2, Oxford, UK, 2010,OxfordUniversityPress.
5. Yao H, Takashima Y, Hashimoto M, etal. Subclinical cerebralabnormalitiesinchronickidneydisease.Contrib Nephrol179:24–34,2013.
6. BagnardiV,RotaM,BotteriE,etal.Lightalcoholdrinkingandcancer:ameta-analysis.Ann Oncol24(2):301–308,2013.
7. Wodak AD, Saunders JB, Ewusi-Mensah I, etal. Severity ofalcoholdependence inpatientswithalcoholic liverdisease.Br Med J (Clin Res Ed)287(6403):1420–1422,1983.
8. U.S. Department of Health and Human Services and U.S.Department of Agriculture. Dietary Guidelines for Americans,2005,Washington,DC,2005,HHSandUSDA.
9. WorldHealthOrganization.Global status report on alcohol 2004,Geneva,2004,DMHSA.
10. Mokdad AH, Marks JS, Stroup DF, etal. Actual causes ofdeath in the United States, 2000. JAMA 291(10):1238–1245,2004.
11. World Health Organization. Global status report on alcohol and health,Geneva,Switzerland,2011,WorldHealthOrganization.
12. Bouchery EE, Harwood HJ, Sacks JJ, etal. Economic costs ofexcessivealcoholconsumptionintheU.S.2006.Am J Prev Med41(5):516–524,2011.
13. Harwood H. Updating estimates of the economic costs of alcohol abuse in the United States: estimate, update methods and data,Wash-ington, DC, 2000, National Institute on Alcohol Abuse andAlcoholism,NationalInstitutesofHealth,DepartmentofHealthandHumanServices.
14. American Psychiatric Association. Diagnostic and statistical manual of mental disorders,ed5,Arlington,2013,AmericanPsy-chiatricAssociation.
15. Miczek KA, Fish EW, De Almeida RM, etal. Role of alcoholconsumption in escalation to violence. Ann N Y Acad Sci1036:278–289,2004.
16. HeinzAJ,BeckA,Meyer-LindenbergA,etal.Cognitiveandneu-robiologicalmechanismsofalcohol-relatedaggression.Naturereviews.Neurosci12(7):400–413,2011.
17. Daeppen JB, Gache P, Landry U, etal. Symptom-triggered vsfixed-scheduledosesofbenzodiazepineforalcoholwithdrawal:arandomizedtreatmenttrial.Arch Int Med162(10):1117–1121,2002.
18. BoothBM,BlowFC.Thekindlinghypothesis:furtherevidencefrom a U.S. national study of alcoholic men. Alcohol Alcohol28(5):593–598,1993.
19. Tsai G, Gastfriend DR, Coyle JT. The glutamatergic basis ofhumanalcoholism.Am J Psychiatry152(3):332–340,1995.
20. CastanedaR,CushmanP.Alcoholwithdrawal:areviewofclini-calmanagement.J Clin Psychiatry50(8):278–284,1989.
21. Sullivan JT, Sykora K, Schneiderman J, etal. Assessment ofalcohol withdrawal: the revised clinical institute withdrawalassessmentforalcoholscale(CIWA-Ar).Br J Addict84(11):1353–1357,1989.
22. SaitzR,Mayo-SmithMF,RobertsMS,etal.Individualizedtreat-mentforalcoholwithdrawal.Arandomizeddouble-blindcon-trolledtrial.JAMA272(7):519–523,1994.
23. JaegerTM,LohrRH,PankratzVS.Symptom-triggeredtherapyforalcoholwithdrawalsyndromeinmedicalinpatients.Mayo Clinic Proceed76(7):695–701,2001.
24. SellersEM,NaranjoCA,HarrisonM,etal.Diazepamloading:simplifiedtreatmentofalcoholwithdrawal.Clin Pharmacol Ther34(6):822–826,1983.
25. Rayner SG, Weinert CR, Peng H, etal. Dexmedetomidine asadjuncttreatmentforseverealcoholwithdrawalintheICU.Ann Intensive Care2(1):12,2012.
26. RosensonJ,ClementsC,SimonB,etal.Phenobarbitalforacutealcohol withdrawal: a prospective randomized double-blind
placebo-controlled study. J Emerg Med 44(3):592–598, e592,2013.
27. SchoenenbergerRA,HeimSM.Indicationforcomputedtomog-raphyofthebraininpatientswithfirstuncomplicatedgeneral-isedseizure.BMJ309(6960):986–989,1994.
28. Alldredge BK, Lowenstein DH, Simon RP. Placebo-controlledtrialofintravenousdiphenylhydantoinforshort-termtreatmentofalcoholwithdrawalseizures.Am J Med87(6):645–648,1989.
29. American Psychiatric Association. Diagnostic and statistical manual of mental disorders,ed4,Washington,DC,1994,Ameri-canPsychiatricAssociation.
30. AwissiDK,LebrunG,CoursinDB,etal.Alcoholwithdrawalanddelirium tremens in the critically ill: a systematic review andcommentary.Int Care Med39(1):16–30,2013.
31. EyerF,SchusterT,FelgenhauerN,etal.Riskassessmentofmod-eratetoseverealcoholwithdrawal—predictorsforseizuresanddelirium tremens in the course of withdrawal. Alcohol Alcohol46(4):427–433,2011.
32. Isenberg-GrzedaE,KutnerHE,NicolsonSE.Wernicke–Korsakoff-syndrome: under-recognized and under-treated. Psychosomatics53(6):507–516,2012.
33. CoomesTR,SmithSW.Successfuluseofpropofolinrefractorydeliriumtremens.Ann Emerg Med30(6):825–828,1997.
34. VictorM,AdamsRD,CollinsGH.TheWernicke-Korsakoffsyn-drome.Aclinicalandpathologicalstudyof245patients,82withpost-mortemexaminations.Contemp Neurol Ser7:1–206,1971.
35. Brust J. Neurological aspects of substance abuse, Boston, 1993,Butterworth-Heinemann.
36. ThomsonAD,MarshallEJ.Thenaturalhistoryandpathophysi-ologyofWernicke’sEncephalopathyandKorsakoff’sPsychosis.Alcohol Alcohol41(2):151–158,2006.
37. deSanctisL,MemoL,PichiniS,etal.Fetalalcoholsyndrome:newperspectivesforanancientandunderestimatedproblem.J Matern Fetal Neonatal Med24(1):34–37,2011.
38. Lipinski RJ, Hammond P, O’Leary-Moore SK, etal. Ethanol-inducedface-braindysmorphologypatternsarecorrelativeandexposure-stagedependent.PLoS ONE7(8):e43067,2012.
39. NationalInstituteonAlcoholAbuseandAlcoholism(NIAAA).10th special report to the U.S. Congress on alcohol and health: high-lights from current research from the Secretary of Health and Human Services,Washington,DC,2000,USDHHS.
40. EdwardsG,GrossMM.Alcoholdependence:provisionaldescrip-tionofaclinicalsyndrome.BMJ1(6017):1058–1061,1976.
41. American Psychiatric Association. Diagnostic and statistical manual of mental disorders: DSM-III-R, Washington, DC, 1980,AmericanPsychiatricAssociation.
42. HasinD,LiQ,McCloudS,etal.AgreementbetweenDSM-III,DSM-III-R, DSM-IV and ICD-10 alcohol diagnoses in UScommunity-sampleheavydrinkers.Addiction91(10):1517–1527,1996.
43. Kelly JF. Towardanaddiction-ary: aproposal formorepreciseterminology.Alcohol Treat Q24(3):241–250,2004.
44. Kelly JF,DowSJ,WesterhoffC.Doesour choiceof substance-related terms influence perceptions of treatment need? Anempiricalinvestigationwithtwocommonlyusedterms.J Drug Iss40:805–818,2011.
45. KellyJF,WesterhoffCM.Doesitmatterhowwerefertoindividu-als with substance-related conditions? A randomized study oftwocommonlyusedterms.Int J Drug Policy21:202–207,2010.
46. Kelly JF, White WL, eds. Addiction Recovery Management. InRosenbaumJF,editor:Current clinical psychiatry,NewYork,2011,Springer.
47. SchuckitMA.Anoverviewofgeneticinfluencesinalcoholism.J Subst Abuse Treat36(1):S5–S14,2009.
48. LiTK.Pharmacogeneticsofresponsestoalcoholandgenesthatinfluencealcoholdrinking.J Stud Alcohol61(1):5–12,2000.
49. Filbey FM, Claus ED, Morgan M, etal. Dopaminergic genesmodulateresponseinhibitioninalcoholabusingadults.Addict Biol17(6):1046–1056,2012.
50. Mulligan MK, Dubose C, Yue J, etal. Expression, covariation,andgeneticregulationofmiRNABiogenesisgenesinbrainsup-portstheirroleinaddiction,psychiatricdisorders,anddisease.Front Genet4:126,2013.
51. Schuckit MA, Tapert S, Matthews SC, etal. fMRI differencesbetweensubjectswithlowandhighresponsestoalcoholduringastopsignaltask.Alcohol Clin Exper Res36(1):130–140,2012.
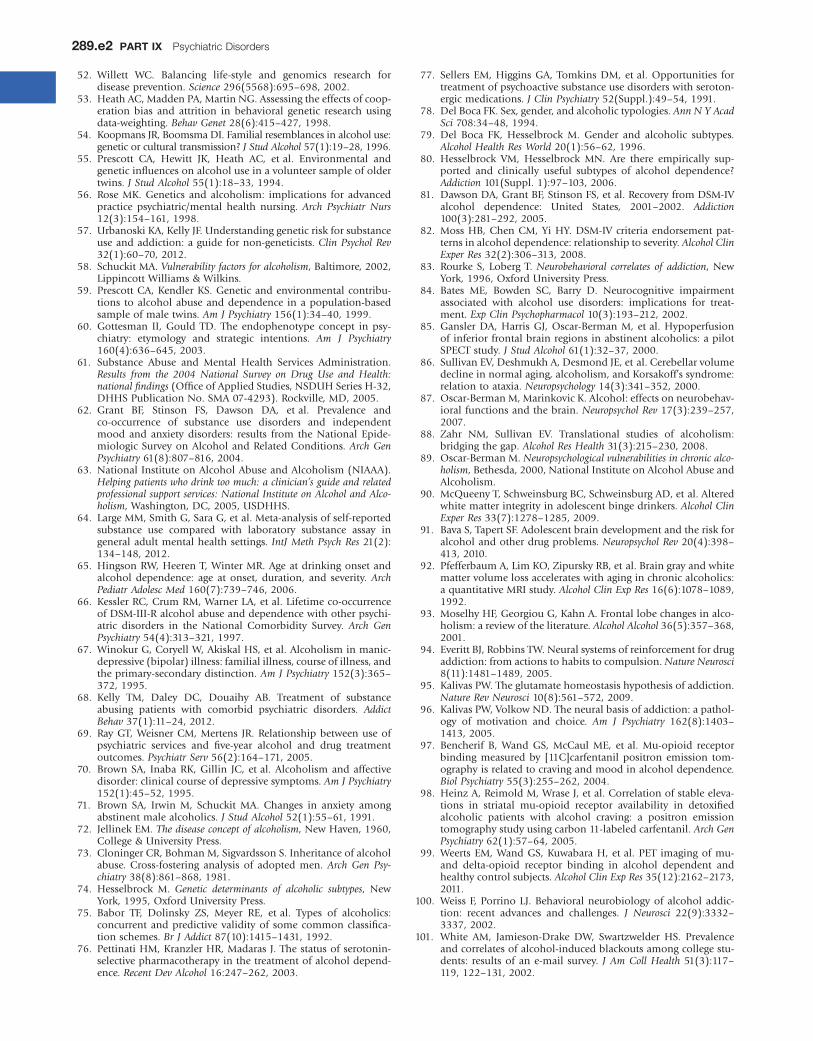
289.e2 PART IX PsychiatricDisorders
52. Willett WC. Balancing life-style and genomics research fordiseaseprevention.Science296(5568):695–698,2002.
53. HeathAC,MaddenPA,MartinNG.Assessingtheeffectsofcoop-eration bias and attrition in behavioral genetic research usingdata-weighting.Behav Genet28(6):415–427,1998.
54. KoopmansJR,BoomsmaDI.Familialresemblancesinalcoholuse:geneticorculturaltransmission?J Stud Alcohol57(1):19–28,1996.
55. Prescott CA, Hewitt JK, Heath AC, etal. Environmental andgeneticinfluencesonalcoholuseinavolunteersampleofoldertwins.J Stud Alcohol55(1):18–33,1994.
56. RoseMK.Genetics andalcoholism: implications for advancedpractice psychiatric/mental health nursing. Arch Psychiatr Nurs12(3):154–161,1998.
57. UrbanoskiKA,KellyJF.Understandinggeneticriskforsubstanceuseandaddiction:aguidefornon-geneticists.Clin Psychol Rev32(1):60–70,2012.
58. SchuckitMA.Vulnerability factors for alcoholism,Baltimore,2002,LippincottWilliams&Wilkins.
59. PrescottCA,KendlerKS.Geneticandenvironmentalcontribu-tions toalcoholabuseanddependence inapopulation-basedsampleofmaletwins.Am J Psychiatry156(1):34–40,1999.
60. Gottesman II, Gould TD. The endophenotype concept in psy-chiatry: etymology and strategic intentions. Am J Psychiatry160(4):636–645,2003.
61. Substance Abuse and Mental Health Services Administration.Results from the 2004 National Survey on Drug Use and Health: national findings(OfficeofAppliedStudies,NSDUHSeriesH-32,DHHSPublicationNo.SMA07-4293).Rockville,MD,2005.
62. Grant BF, Stinson FS, Dawson DA, etal. Prevalence andco-occurrence of substance use disorders and independentmood and anxiety disorders: results from the National Epide-miologicSurveyonAlcoholandRelatedConditions.Arch Gen Psychiatry61(8):807–816,2004.
63. NationalInstituteonAlcoholAbuseandAlcoholism(NIAAA).Helping patients who drink too much: a clinician’s guide and related professional support services: National Institute on Alcohol and Alco-holism,Washington,DC,2005,USDHHS.
64. LargeMM,SmithG,SaraG,etal.Meta-analysisofself-reportedsubstance use compared with laboratory substance assay ingeneraladultmentalhealthsettings.IntJ Meth Psych Res21(2):134–148,2012.
65. HingsonRW,HeerenT,WinterMR.Ageatdrinkingonsetandalcohol dependence: age at onset, duration, and severity. Arch Pediatr Adolesc Med160(7):739–746,2006.
66. KesslerRC,CrumRM,WarnerLA,etal.Lifetimeco-occurrenceofDSM-III-Ralcoholabuseanddependencewithotherpsychi-atric disorders in the National Comorbidity Survey. Arch Gen Psychiatry54(4):313–321,1997.
67. WinokurG,CoryellW,AkiskalHS,etal.Alcoholisminmanic-depressive(bipolar)illness:familialillness,courseofillness,andtheprimary-secondarydistinction.Am J Psychiatry152(3):365–372,1995.
68. Kelly TM, Daley DC, Douaihy AB. Treatment of substanceabusing patients with comorbid psychiatric disorders. Addict Behav37(1):11–24,2012.
69. RayGT,WeisnerCM,Mertens JR.Relationshipbetweenuseofpsychiatric services and five-year alcohol and drug treatmentoutcomes.Psychiatr Serv56(2):164–171,2005.
70. BrownSA, InabaRK,Gillin JC, etal.Alcoholismandaffectivedisorder:clinicalcourseofdepressivesymptoms.Am J Psychiatry152(1):45–52,1995.
71. Brown SA, Irwin M, Schuckit MA. Changes in anxiety amongabstinentmalealcoholics.J Stud Alcohol52(1):55–61,1991.
72. JellinekEM.The disease concept of alcoholism,NewHaven,1960,College&UniversityPress.
73. CloningerCR,BohmanM,SigvardssonS.Inheritanceofalcoholabuse. Cross-fostering analysis of adopted men. Arch Gen Psy-chiatry38(8):861–868,1981.
74. Hesselbrock M. Genetic determinants of alcoholic subtypes, NewYork,1995,OxfordUniversityPress.
75. Babor TF, Dolinsky ZS, Meyer RE, etal. Types of alcoholics:concurrentandpredictivevalidityof somecommonclassifica-tionschemes.Br J Addict87(10):1415–1431,1992.
76. PettinatiHM,KranzlerHR,MadarasJ.Thestatusofserotonin-selectivepharmacotherapyinthetreatmentofalcoholdepend-ence.Recent Dev Alcohol16:247–262,2003.
77. SellersEM,HigginsGA,TomkinsDM,etal.Opportunities fortreatmentofpsychoactivesubstanceusedisorderswithseroton-ergicmedications.J Clin Psychiatry52(Suppl.):49–54,1991.
78. DelBocaFK.Sex,gender,andalcoholictypologies.Ann N Y Acad Sci708:34–48,1994.
79. Del Boca FK, Hesselbrock M. Gender and alcoholic subtypes.Alcohol Health Res World20(1):56–62,1996.
80. Hesselbrock VM, Hesselbrock MN. Are there empirically sup-ported and clinically useful subtypes of alcohol dependence?Addiction101(Suppl.1):97–103,2006.
81. DawsonDA,GrantBF,StinsonFS,etal.RecoveryfromDSM-IValcohol dependence: United States, 2001–2002. Addiction100(3):281–292,2005.
82. MossHB,ChenCM,YiHY.DSM-IVcriteriaendorsementpat-ternsinalcoholdependence:relationshiptoseverity.Alcohol Clin Exper Res32(2):306–313,2008.
83. RourkeS, LobergT.Neurobehavioral correlates of addiction,NewYork,1996,OxfordUniversityPress.
84. Bates ME, Bowden SC, Barry D. Neurocognitive impairmentassociated with alcohol use disorders: implications for treat-ment.Exp Clin Psychopharmacol10(3):193–212,2002.
85. GanslerDA,HarrisGJ,Oscar-BermanM, etal.Hypoperfusionofinferiorfrontalbrainregionsinabstinentalcoholics:apilotSPECTstudy.J Stud Alcohol61(1):32–37,2000.
86. SullivanEV,DeshmukhA,DesmondJE,etal.Cerebellarvolumedeclineinnormalaging,alcoholism,andKorsakoff’ssyndrome:relationtoataxia.Neuropsychology14(3):341–352,2000.
87. Oscar-BermanM,MarinkovicK.Alcohol:effectsonneurobehav-ioralfunctionsandthebrain.Neuropsychol Rev17(3):239–257,2007.
88. Zahr NM, Sullivan EV. Translational studies of alcoholism:bridgingthegap.Alcohol Res Health31(3):215–230,2008.
89. Oscar-BermanM.Neuropsychological vulnerabilities in chronic alco-holism,Bethesda,2000,NationalInstituteonAlcoholAbuseandAlcoholism.
90. McQueenyT,SchweinsburgBC,SchweinsburgAD,etal.Alteredwhitematterintegrityinadolescentbingedrinkers.Alcohol Clin Exper Res33(7):1278–1285,2009.
91. BavaS,TapertSF.Adolescentbraindevelopmentandtheriskforalcoholandotherdrugproblems.Neuropsychol Rev20(4):398–413,2010.
92. PfefferbaumA,LimKO,ZipurskyRB,etal.Braingrayandwhitemattervolumelossaccelerateswithaginginchronicalcoholics:aquantitativeMRIstudy.Alcohol Clin Exp Res16(6):1078–1089,1992.
93. MoselhyHF,GeorgiouG,KahnA.Frontallobechangesinalco-holism:areviewoftheliterature.Alcohol Alcohol36(5):357–368,2001.
94. EverittBJ,RobbinsTW.Neuralsystemsofreinforcementfordrugaddiction:fromactionstohabitstocompulsion.Nature Neurosci8(11):1481–1489,2005.
95. KalivasPW.Theglutamatehomeostasishypothesisofaddiction.Nature Rev Neurosci10(8):561–572,2009.
96. KalivasPW,VolkowND.Theneuralbasisofaddiction:apathol-ogy of motivation and choice. Am J Psychiatry 162(8):1403–1413,2005.
97. Bencherif B, Wand GS, McCaul ME, etal. Mu-opioid receptorbinding measured by [11C]carfentanil positron emission tom-ographyisrelatedtocravingandmoodinalcoholdependence.Biol Psychiatry55(3):255–262,2004.
98. HeinzA,ReimoldM,WraseJ,etal.Correlationofstableeleva-tions in striatal mu-opioid receptor availability in detoxifiedalcoholic patients with alcohol craving: a positron emissiontomographystudyusingcarbon11-labeledcarfentanil.Arch Gen Psychiatry62(1):57–64,2005.
99. WeertsEM,WandGS,KuwabaraH,etal.PET imagingofmu-and delta-opioid receptor binding in alcohol dependent andhealthycontrolsubjects.Alcohol Clin Exp Res35(12):2162–2173,2011.
100. WeissF,PorrinoLJ.Behavioralneurobiologyofalcoholaddic-tion: recent advances and challenges. J Neurosci 22(9):3332–3337,2002.
101. White AM, Jamieson-Drake DW, Swartzwelder HS. Prevalenceandcorrelatesofalcohol-inducedblackoutsamongcollegestu-dents: resultsofane-mail survey. J Am Coll Health51(3):117–119,122–131,2002.
Alcohol-RelatedDisorders 289.e3
26102. Oscar-BermanM,MarinkovicK.Alcoholismandthebrain:an
overview.Alcohol Res Health27(2):125–133,2003.103. CrewsFT,BraunCJ,HoplightB,etal.Bingeethanolconsump-
tioncausesdifferentialbraindamage inyoungadolescent ratscompared with adult rats. Alcohol Clin Exp Res 24(11):1712–1723,2000.
104. Valenzuela CF. Alcohol and neurotransmitter interactions.Alcohol Health Res World21(2):144–148,1997.
105. KumarS,PorcuP,WernerDF,etal.TheroleofGABA(A)recep-tors in the acute and chronic effects of ethanol: a decade ofprogress.Psychopharmacology (Berl)205(4):529–564,2009.
106. Enoch MA, Gorodetsky E, Hodgkinson C, etal. Functionalgenetic variants that increase synaptic serotonin and 5-HT3receptor sensitivity predict alcohol and drug dependence. Mol Psychiatry16(11):1139–1146,2011.
107. Sari Y, Johnson VR, Weedman JM. Role of the serotonergicsysteminalcoholdependence: fromanimalmodels toclinics.Prog Mol Biol Transl Sci98:401–443,2011.
108. GianoulakisC. Influenceof theendogenousopioidsystemonhighalcohol consumptionandgeneticpredisposition to alco-holism.J Psychiatry Neurosci26(4):304–318,2001.
109. RamchandaniVA,UmhauJ,PavonFJ,etal.Ageneticdetermi-nantofthestriataldopamineresponsetoalcoholinmen.Mol Psychiatry16(8):809–817,2011.
110. FlemingMF.Briefinterventionsandthetreatmentofalcoholusedisorders:currentevidence.Rec Dev Alcohol16:375–390,2003.
111. LangenbucherJ.Rxforhealthcarecosts:resolvingaddictionsinthe general medical setting. Alcohol Clin Exp Res 18(5):1033–1036,1994.
112. EwingJA.Detectingalcoholism.TheCAGEquestionnaire.JAMA252(14):1905–1907,1984.
113. ReinertDF,AllenJP.Thealcoholusedisordersidentificationtest:anupdateofresearchfindings.Alcohol Clin Exp Res31(2):185–199,2007.
114. BradleyKA,DeBenedettiAF,VolkRJ,etal.AUDIT-Casabriefscreen foralcoholmisuse inprimarycare.Alcohol Clin Exp Res31(7):1208–1217,2007.
115. Knight JR, Sherritt L, Shrier LA, etal. Validity of the CRAFFTsubstanceabusescreeningtestamongadolescentclinicpatients.Arch Pediatr Adolesc Med156(6):607–614,2002.
116. Anton RF. Carbohydrate-deficient transferrin for detection andmonitoringofsustainedheavydrinking.Whathavewelearned?Wheredowegofromhere?Alcohol25(3):185–188,2001.
117. MillerPM,AntonRF.Biochemicalalcoholscreeninginprimaryhealthcare.Addict Behav29(7):1427–1437,2004.
118. Thon N, Weinmann W, Yegles M, etal. Direct metabolites ofethanolasbiologicalmarkersofalcoholuse:basicaspectsandapplications.Fortschr Neurol Psychiatr2013.
119. Purshouse RC, Brennan A, Rafia R, etal. Modelling the cost-effectiveness of alcohol screening and brief interventions inprimarycareinEngland.Alcohol Alcohol48(2):180–188,2013.
120. Rappaport D, Chuu A, Hullett C, etal. Assessment of alcoholwithdrawal in Native American patients utilizing the ClinicalInstitute Withdrawal Assessment of Alcohol Revised Scale.J Addict Med7(3):196–199,2013.
121. SpitzerRL,WilliamsJB,GibbonM,etal.TheStructuredClinicalInterview for DSM-III-R (SCID). I: History, rationale, anddescription.Arch Gen Psychiatry49(8):624–629,1992.
122. BaborTF,Higgins-Biddle JC,Saunders JB,etal.The alcohol use disorders identification test: Guidelines for use in primary care,ed2,Geneva,Switzerland,2001,WorldHealthOrganization.
123. KellyJF,MagillM,SlaymakerV,etal.PsychometricvalidationoftheLeedsDependenceQuestionnaire (LDQ) inayoungadultclinicalsample.Addict Behav35(4):331–336,2010.
124. Raistrick D, Bradshaw J, Tober G, etal. Development of theLeeds Dependence Questionnaire (LDQ): a questionnaire tomeasurealcoholandopiatedependenceinthecontextofatreat-mentevaluationpackage.Addiction89(5):563–572,1994.
125. AmericanPsychiatricAssociation.Handbook of psychiatric meas-ures,Washington,DC,2000,AmericanPsychiatricAssociation.
126. AntonyMM,BarlowDH.Handbook of assessment and treatment planning for psychological disorders, New York, 2000, GuilfordPress.
127. AmericanSocietyofAddictionMedicine.Patient placement crite-ria, ed 2, Chevy Chase, 1994, American Society of AddictionMedicine.
128. SweetmanJ,RaistrickD,MdegeND,etal.Asystematic reviewof substance misuse assessment packages. Drug Alcohol Rev32(4):347–355,2013.
129. Sobell LC, Ellingstad TP, Sobell MB. Natural recovery fromalcohol and drug problems: methodological review of theresearch with suggestions for future directions. Addiction95(5):749–764,2000.
130. Kelly JF,YeterianJD.Empiricalawakening: thenewscienceonmutualhelpandimplicationsforcostcontainmentunderhealthcarereform.Subst Abus33(2):85–91,2012.
131. KellyJF,YeterianJD.Mutual-helpgroupsforalcoholandothersubstance use disorders. In McCrady BS, Epstein EE, editors:Addictions: A comprehensive guidebook, ed 2, New York, 2013,OxfordUniversityPress.
132. MillerWR,WilbournePL.MesaGrande:amethodologicalanal-ysis of clinical trials of treatments for alcohol use disorders.Addiction97(3):265–277,2002.
133. MoyerA,FinneyJW,SwearingenCE,etal.Briefinterventionsforalcoholproblems:ameta-analyticreviewofcontrolledinvestiga-tions in treatment-seeking and non-treatment-seeking popula-tions.Addiction97(3):279–292,2002.
134. Maisel NC, Blodgett JC, Wilbourne PL, etal. Meta-analysis ofnaltrexoneandacamprosate for treatingalcoholusedisorders:whenarethesemedicationsmosthelpful?Addiction108(2):275–293,2013.
135. BienTH,MillerWR,ToniganJS.Briefinterventionsforalcoholproblems:areview.Addiction88(3):315–335,1993.
136. Graham A, Fleming M. Brief interventions, Chevy Chase, 1998,AmericanSocietyofAddictionMedicine.
137. O’ConnorPG,SchottenfeldRS.Patientswithalcoholproblems.N Eng J Med338(9):592–602,1998.
138. Madras BK, Compton WM, Avula D, etal. Screening, briefinterventions, referral to treatment (SBIRT) for illicitdrugandalcohol use at multiple healthcare sites: comparison at intakeand 6 months later. Drug Alcohol Depend 99(1–3):280–295,2009.
139. FlemingMF,BarryKL,ManwellLB,etal.Briefphysicianadviceforproblemalcoholdrinkers.Arandomizedcontrolledtrialincommunity-basedprimarycarepractices.JAMA277(13):1039–1045,1997.
140. KristensonH,OhlinH,Hulten-NosslinMB,etal.Identificationandinterventionofheavydrinkinginmiddle-agedmen:resultsandfollow-upof24–60monthsoflong-termstudywithrand-omizedcontrols.Alcohol Clin Exp Res7(2):203–209,1983.
141. Wallace P, Cutler S, Haines A. Randomised controlled trial ofgeneral practitioner intervention in patients with excessivealcoholconsumption.BMJ297(6649):663–668,1988.
142. Group WHOBIS. A cross-national trial of brief interventionswith heavy drinkers. Am J Public Health 86(7):948–955,1996.
143. EdwardsG,OrfordJ,EgertS,etal.Alcoholism:Acontrolledtrialof “treatment” and “advice”. J Stud Alcohol 38(5):1004–1031,1977.
144. Substance Abuse and Mental Health Services Administration.Thealcoholusedisorders identification test (AUDIT),<http://pathwayscourses.samhsa.gov/aaap/aaap_4_supps_pg3.htm>;2002.
145. MillerWR,SanchezV.Motivating young adults for treatment and lifestyle change, Notre Dame, 1994, University of Notre DamePress.
146. Miller WR, Rollnick S. Motivational interviewing: helping people change,ed3,NewYork,2012,GuilfordPress.
147. AlajaR,SeppaK.Six-monthoutcomesofhospital-basedpsychi-atricsubstanceuseconsultations.Gen Hosp Psychiatry25(2):103–107,2003.
148. EttnerSL,HermannRC,TangH.Differencesbetweengeneralistsand mental health specialists in the psychiatric treatment ofMedicarebeneficiaries.Health Serv Res34(3):737–760,1999.
149. Moos RH, Finney JW, Federman EB, etal. Specialty mentalhealthcareimprovespatients’outcomes:findingsfromanation-wideprogramtomonitor thequalityof care forpatientswithsubstanceusedisorders.J Stud Alcohol61(5):704–713,2000.
150. Hillman A, McCann B, Walker NP. Specialist alcohol liaisonservices in general hospitals improve engagement in alcoholrehabilitation and treatment outcome. Health Bull 59(6):420–423,2001.
289.e4 PART IX PsychiatricDisorders
151. MarlattGA,GordonJR,editors:Relapse prevention: Maintenance strategies in the treatment of addictive behaviors,NewYork,1985,GuilfordPress.
152. Swearingen CE, Moyer A, Finney JW. Alcoholism treatmentoutcome studies,1970–1998.Anexpanded lookat thenatureoftheresearch.Addict Behav28(3):415–436,2003.
153. MillerWR,RollnickS.Motivational interviewing: preparing people to change addictive behaviour,NewYork,1991,GuilfordPress.
154. Meyers RJ, Smith JE, Lash DN. The community reinforcementapproach.Rec Dev Alcohol16:183–195,2003.
155. MoosRH.Addictivedisordersincontext:principlesandpuzzlesofeffectivetreatmentandrecovery.Psychol Addict Behav17(1):3–12,2003.
156. Humphreys K, Tucker JA. Romance, realism and the future ofalcoholinterventionsystems.Addiction97(2):138–140,2002.
157. White WL. Recovery management and recovery-oriented systems of care: scientific rationale and promising practices, 2008, NortheastAddiction Technology Transfer Center, Great Lakes AddictionTechnologyTransferCenter,PhiladelphiaDepartmentofBehav-ioralHealth/MentalRetardationServices.
158. Dennis ML, Scott CK. Four-year outcomes from the EarlyRe-Intervention (ERI) experiment using Recovery ManagementCheckups(RMCs).Drug Alcohol Depend121(1–2):10–17,2012.
159. McKay J, Lynch K, Shepard D. Do patient characteristics andinitial progress in treatment moderate the effectiveness oftelephone-based continuing care for substance use disorders?Addiction100(2):216–226,2005.
160. Stout RL, Rubin A, Zwick W, etal. Optimizing the cost-effectivenessofalcoholtreatment:arationaleforextendedcasemonitoring.Addict Behav24(1):17–35,1999.
161. MillerWR,BenefieldRG,ToniganJS.Enhancingmotivationforchange in problem drinking: a controlled comparison of twotherapiststyles.J Consult Clin Psychol61(3):455–461,1993.
162. Project MATCH Research Group. Project MATCH secondary apriorihypotheses.Addiction92(12):1671–1698,1997.
163. Stephens RS, Roffman RA, Curtin L. Comparison of extendedversusbrieftreatmentsformarijuanause.J Consult Clin Psychol68(5):898–908,2000.
164. McClellan A, Lewis D, O’Brien C, etal. Drug dependence, achronic medical illness: implications for treatment, insurance,andoutcomesevaluation.JAMA284(13):1689–1695,2000.
165. Fuller RK, Hiller-Sturmhofel S. Alcoholism treatment in theUnited States. An overview. Alcohol Res Health 23(2):69–77,1999.
166. DennisML,ScottCK,FunkR,etal.Thedurationandcorrelatesofaddictionandtreatmentcareers.J Subst Abuse Treat28(Suppl.1):S51–S62,2005.
167. White WL. Recovery/remission from substance use disorders: An analysis of reported outcomes in 415 scientific reports, 1868–2011,2012,PhiladelphiaDepartmentofBehavioralHealthandIntel-lectual disability Services, Great Lakes Addiction TechnologyTransferCenter.
168. SimpsonDD,JoeGW,Rowan-SzalGA,etal.Drugabusetreat-mentprocesscomponentsthatimproveretention.J Subst Abuse Treat14(6):565–572,1997.
169. FullerRK,BrancheyL,BrightwellDR,etal.Disulfiramtreatmentof alcoholism. A Veterans Administration cooperative study.JAMA256(11):1449–1455,1986.
170. O’FarrellTJ,AllenJP,LittenRZ.Disulfiram(antabuse)contractsin treatment of alcoholism. NIDA Res Monogr 150:65–91,1995.
171. O’FarrellTJ,CutterHS,ChoquetteKA,etal.Behavioralmartialtherapy for male alcoholics: marital and drinking adjustmentduring the two years after treatment. Behav Ther 23(4):529,1992.
172. O’FarrellTJ,CutterHS,FloydFJ.Evaluatingbehavioralmaritaltherapy formalealcoholics:effectsonmaritaladjustmentandcommunication from before to after treatment. Behav Ther16(2):147,1985.
173. Froehlich J,O’MalleyS,HyytiaP,etal.Preclinicalandclinicalstudiesonnaltrexone:whathavetheytaughteachother?Alcohol Clin Exp Res27(3):533–539,2003.
174. VolpicelliJR,AltermanAI,HayashidaM,etal.Naltrexoneinthetreatmentofalcoholdependence.Arch Gen Psychiatry49(11):876–880,1992.
175. ChamorroAJ,MarcosM,Miron-CaneloJA,etal.Associationofmicro-opioid receptor (OPRM1) gene polymorphism withresponse to naltrexone in alcohol dependence: a systematicreviewandmeta-analysis.Addict Biol17(3):505–512,2012.
176. ArbaizarB,Diersen-SotosT,Gomez-Acebo I, etal. Topiramatein the treatmentofalcoholdependence:ameta-analysis.Actas Esp Psiquiatr38(1):8–12,2010.
177. PaparrigopoulosT,TzavellasE,KaraiskosD,etal.Treatmentofalcohol dependence with low-dose topiramate: an open-labelcontrolledstudy.BMC Psychiatry11:41,2011.
178. CorneliusJR,BuksteinO,SalloumI,etal.Alcoholandpsychi-atriccomorbidity.Rec Dev Alcohol16:361–374,2003.
179. RennerJA.Drugsubstitutiontreatmentsandaddictionpharma-cotherapies: integrating pharmacotherapy into the addictionsyndrome treatment paradigm. In Shaffer HA, LaPlante DA,NelsonSE,editors:The American Psychological Association Addic-tion Syndrome Handbook,Washington,DC,2012,AmericanPsy-chologicalAssociation.
180. EmrickC,ToniganJ,MontgomeryH,etal.Alcoholics Anonymous: what is currently known, Piscataway, 1993, Rutgers Center ofAlcoholStudies.
181. HumphreysK.Circles of recovery: self-help organizations for addic-tions,Cambridge,UK,2004,CambridgeUniversityPress.
182. Humphreys K, Moos R. Can encouraging substance abusepatients to participate in self-help groups reduce demand forhealth care?Aquasi-experimental study.Alcohol Clin Exper Res25(5):711–716,2001.
183. Humphreys K, Moos RH. Encouraging posttreatment self-helpgroupinvolvementtoreducedemandforcontinuingcareserv-ices: two-year clinical and utilization outcomes. Alcohol Clin Exper Res31(1):64–68,2007.
184. KellyJF.Self-helpforsubstanceusedisorders:history,effective-ness, knowledge gaps, and research opportunities.Clin Psychol Rev23(5):639–663,2003.
185. Kelly JF, Stout R, Zywiak W, etal. A 3-year study of addictionmutual-helpgroupparticipationfollowingintensiveoutpatienttreatment.Alcohol Clin Exper Res30(8):1381–1392,2006.
186. Moos RH, Moos BS. The interplay between help-seeking andalcohol-related outcomes: divergent processes for professionaltreatmentandself-helpgroups.Drug Alcohol Depend75(2):155–164,2004.
187. Kelly JF, White W. Broadening the base of addiction recoverymutualaid.J Groups Addict Recover7(2–4):82–101,2012.
188. HesterRK,LenbergKL,CampbellW,etal.Overcomingaddic-tions,aweb-basedapplication,andSMARTrecovery,anonlineandin-personmutualhelpgroupforproblemdrinkers,Part1:three-monthoutcomesofarandomizedcontrolledtrial.J Med Internet Res15(7):e134,2013.
189. KellyJF,HumphreysK,YoungsonH.Mutualaidgroups.InHar-risonS,CarverV,editors:Alcohol and drug problems: A practical guide for counselors,ed4,Toronto,2012,CentreforAddictionandMentalHealth,pp169–197.
190. MundtMP,ParthasarathyS,ChiFW,etal.12-Stepparticipationreducesmedicalusecostsamongadolescentswithahistoryofalcoholandotherdrugtreatment.Drug Alcohol Depend126(1–2):124–130,2012.
191. Kelly JF,HoeppnerB, StoutRL, etal.Determining the relativeimportanceofthemechanismsofbehaviorchangewithinAlco-holics Anonymous: a multiple mediator analysis. Addiction107(2):289–299,2012.
192. KellyJF,MagillM,StoutRL.Howdopeoplerecoverfromalcoholdependence?AsystematicreviewoftheresearchonmechanismsofbehaviorchangeinAlcoholicsAnonymous.Addict Res Theory17(3):236–259,2009.
193. Kelly JF, Stout RL, Magill M, etal. Mechanisms of behaviorchange inalcoholicsanonymous:doesAlcoholicsAnonymouslead to better alcohol use outcomes by reducing depressionsymptoms?Addiction105(4):626–636,2010.
194. KellyJF,HoeppnerB.DoesAlcoholicsAnonymousworkdiffer-ently for men and women? A moderated multiple-mediationanalysisinalargeclinicalsample.Drug Alcohol Depend130(1–3):186–193,2013.
195. Mäkela K. Alcoholics Anonymous as a mutual-help movement: A study in eight societies,Madison,WI,1996,UniversityofWiscon-sinPress.

Alcohol-RelatedDisorders 289.e5
26196. Room R, Greenfield T. Alcoholics anonymous, other 12-step
movements and psychotherapy in the US population, 1990.Addiction88(4):555–562,1993.
197. Kelly JF, Yeterian JD. Mutual-help groups. In O’Donohue W,Cunningham JA, editors: Evidence-based adjunctive treatments,NewYork,NY,2008,Elsevier.
198. KellyJF,McKellarJD,MoosR.Majordepressioninpatientswithsubstance use disorders: relationship to 12-Step self-helpinvolvementandsubstanceuseoutcomes.Addiction98(4):499–508,2003.
199. KellyJF,MyersMG,BrownSA.Amultivariateprocessmodelofadolescent12-stepattendanceandsubstanceuseoutcomefol-lowinginpatienttreatment.Psychol Addict Behav14(4):376–389,2000.
200. Kelly JF, Myers MG, Brown SA. Do adolescents affiliate with12-stepgroups?Amultivariateprocessmodelofeffects. J Stud Alcohol63(3):293–304,2002.
201. TimkoC,DebenedettiA,BillowR.Intensivereferralto12-Stepself-helpgroupsand6-monthsubstanceusedisorderoutcomes.Addiction101(5):678–688,2006.
202. Bergman BG, Greene MC, Hoeppner BB, etal. Psychiatriccomorbidityand12-stepparticipation:Alongitudinalinvestiga-tionoftreatedyoungadults.Alcohol Clin Exp Res38(2):501–510,2014.
203. Nowinski J, Baker S, Carroll K, editors: Twelve-Step facilitation therapy manual: A clinical research guide for therapists treating
individuals with alcohol abuse and dependence, Rockville, MD,1992, National Institute on Alcohol Abuse and Alcoholism,ProjectMATCHMonographSeries;No.4.
204. ScottCK,DennisML,FossMA.UtilizingRecoveryManagementCheckupstoshortenthecycleofrelapse,treatmentreentry,andrecovery.Drug Alcohol Depend78(3):325–338,2005.
205. SissonRW,Mallams JH.Theuseof systematic encouragementand community access procedures to increase attendance atAlcoholicAnonymousandAl-Anonmeetings.Am J Drug Alcohol Abuse8(3):371–376,1981.
206. DonovanDM,DaleyDC,BrighamGS, etal. Stimulantabusergroups to engage in 12-step: a multisite trial in the NationalInstitute on Drug Abuse Clinical Trials Network. J Subst Abuse Treat44(1):103–114,2013.
207. KahlerCW,ReadJP,RamseySE,etal.Motivationalenhancementfor 12-step involvement among patients undergoing alcoholdetoxification.J Consult Clin Psychol72(4):736–741,2004.
208. KaskutasLA,SubbaramanMS,WitbrodtJ,etal.EffectivenessofMakingAlcoholicsAnonymousEasier: a group format12-stepfacilitationapproach.J Subst Abuse Treat37(3):228–239,2009.
209. LittMD,KaddenRM,Kabela-CormierE,etal.Changingnetworksupportfordrinking:networksupportproject2-yearfollow-up.J Consult Clin Psychol77(2):229–242,2009.
210. WalitzerKS,DermenKH,BarrickC.FacilitatinginvolvementinAlcoholics Anonymous during out-patient treatment: a rand-omizedclinicaltrial.Addiction104(3):391–401,2009.

289.e6 PART IX PsychiatricDisorders
MULTIPLE CHOICE QUESTIONS
Select the appropriate answer.Q1 Whichofthefollowingstatementsaboutalcohol-
relatedproblemsisLEASTlikelytobeaccurate?
○ Excessive or risky alcohol consumption is the thirdleadingcauseofdeathintheUnitedStates,accountingforapproximately85,000deathsannually.
○ If a largequantity is consumed, andespeciallywhenrapidly consumed, alcohol-induced amnesia (“black-outs”)canoccur.
○ Itisestimatedthatalcoholcausesabout70%to80%ofesophagealcancer,livercancer,cirrhosisoftheliver,homicide, epileptic seizures, and motor vehicle acci-dentsworldwide.
○ Some common consequences of alcohol misuseinclude motor vehicle and other accidents, violenceandvandalism,unwantedsexualexperiences,liverandcardiovasculardiseases,cancers,fetalalcoholspectrumdisorders,depression,panicattacks,andsuicide.
○ The economic burden attributed to alcohol-relatedproblemsintheUnitedStatesapproaches$200billionannually.
Q2 TrueorFalse.A70kgmanmetabolizesapproximately10mlofabsoluteethanol(or1.5to2drinkequivalents;1standarddrink= 1
2ozofwhiskey,4ozofwine,or12ozofbeer)perhour.
○ True
○ False
Q3 TrueorFalse.Symptomsofalcoholwithdrawaltypicallyemerge2to3daysafterdiscontinuationofalcoholandresolvewithin3to5daysoftheirappearance.
○ True
○ False
Q4 Whichofthefollowingconditionsistypicallymanifestbyophthalmoplegia,ataxia,andconfusion?
○ Alcoholintoxication
○ Alcoholwithdrawal
○ Deliriumtremens
○ Korsakoffsyndrome
○ Wernicke’sencephalopathy
Q5 WhichofthefollowingisconsideredtobetheBESTtreatmentforapatientwithWernicke’sencephalopathy?
○ Benztropine
○ Chlordiazepoxide
○ Haloperidol
○ Naloxone
○ Thiamine
Q6 TrueorFalse.MRIandDTIstudiestypicallyrevealalossofbraintissue,andneuropsychologicaltestsshowcognitiveimpairmentsinindividualswhoeitherhaveanalcoholusedisorderorareheavydrinkers.
○ True
○ False
Q7 Whichofthefollowingisa4-itemscreeningtestforalcoholuseandabuse?
○ TheAUDIT
○ TheCAGE
○ TheCIWA-AD
○ TheMAST
○ TheSASQ
MULTIPLE CHOICE ANSWERSQ1 The answer is: It is estimated that alcohol causes
about 70% to 80% of esophageal cancer, liver cancer, cirrhosis of the liver, homicide, epileptic seizures, and motor vehicle accidents worldwide.
Itisestimatedthatalcoholcausesabout20%to30%(i.e.,not70% to80%)of esophageal cancer, liver cancer, cirrhosisoftheliver,homicide,epilepticseizures,andmotorvehicleacci-dentsworldwide.
Q2 The answer is: True.
Resolutionofintoxicationfollowssteady-statekinetics,sothata 70kg man metabolizes approximately 10ml of absoluteethanol(or1.5to2drinkequivalents;1standarddrink=1
2ozofwhiskey,4ozofwine,or12ozofbeer)perhour.
Q3 The answer is: False.
Uncomplicatedwithdrawalissurprisinglycommonandisfre-quentlymissed.Themostcommonfeaturesofuncomplicatedalcoholwithdrawalemergewithinhours,andresolveafter3to5days.
Early features (irritability, tremor, and loss of appetite) ofuncomplicatedwithdrawalsymptomsarepredictable.Ahall-markofthewithdrawalsyndromeisgeneralizedtremor(fastinfrequencyandmorepronouncedwhenthepatientisunderstress).Thistremormayinvolvethetonguetosuchanextentthatthepatientcannottalk.Thelowerextremitiesmaytremblesomuch that thepatient cannotwalk. Thehands andarmsmay shake soviolently thatadrinkingglass cannotbeheldwithoutspilling thecontents.Thepatientmaybehypervigi-lant, have a pronounced startle response, and complain ofinsomnia.
Lesscommonly,patientsexperiencehallucinationsorseizuresassociated with alcohol withdrawal. These symptoms maypersistforaslongas2weeksandthenclearwithoutthedevel-opment of delirium. Grand mal seizures (“rum fits”) mayoccur, usually within the first 2 days after abstinence. Morethanoneoutofeverythreepatientswhosufferseizuresdevel-opssubsequentdeliriumtremens(DTs).
Q4 The answer is: Wernicke’s encephalopathy.
Wernicke’sencephalopathyappearssuddenlyandischaracter-ized by ophthalmoplegia and ataxia followed by mental

Alcohol-RelatedDisorders 289.e7
26disturbance. The ocular disturbance, which occurs in only17%of cases, consistsofparesisorparalysisof the externalrecti,nystagmus,andadisturbanceinconjugategaze.Aglobalconfusionalstateconsistsofdisorientation,unresponsiveness,and derangement of perception and memory. Exhaustion,apathy, dehydration, and profound lethargy are also part ofthepicture.Thepatientisapttobesomnolent,confused,slowtoreply,andmayfallasleepinmid-sentence.
Q5 The answer is: Thiamine.
Once treatment with thiamine is started for Wernicke’sencephalopathy, improvement isoftenevident in theocularpalsieswithinhours.Recoveryfromocularmuscleparalysisiscompletewithindaysorweeks.According toVictor and co-workers,approximatelyone-thirdrecoveredfromthestateofglobal confusion within 6 days of treatment, another thirdwithin 1 month, and the remainder within 2 months. Thestate of global confusional is almost always reversible, inmarked contrast to the memory impairment of Korsakoff’spsychosis.
Administrationof theBvitamin, thiamine(givenIMorIV),shouldberoutineforallsuspectedcasesofalcoholintoxica-tionanddependence.ThetreatmentforWernicke’sencepha-lopathy and Korsakoff’s psychosis is identical, and both aremedical emergencies. Because subclinical cognitive impair-mentscanoccureveninapparentlywell-nourishedpatients,routinemanagementshouldincludethiamine,folicacid,andmultivitaminswithminerals,particularlyzinc.Promptuseofvitamins,particularlythiamine,preventsadvancementofthedisease and reverses at least a portion of the lesions wherepermanent damage has not yet been done. The response totreatmentisthereforeanimportantdiagnosticaid.Inpatientswhoshowonlyocularandataxicsigns,thepromptadminis-trationof thiamineiscrucial inpreventingthedevelopmentofanirreversibleandincapacitatingamnesticdisorder.Treat-mentconsistsof100mgof thiamineand1mgof folicacid(given IV) immediately and 100mg IM thiamine each dayuntil a normal diet is resumed, followed by oral doses for30days.
Q6 The answer is: True.
MRIandDTIstudiestypicallyrevealalossofbraintissue,andneuropsychologicaltestsshowcognitiveimpairmentsinindi-vidualswhoeitherhaveanalcoholusedisorderorareheavydrinkers.Abnormalitiesonscanshavebeenreportedin50%or more of individuals with chronic alcohol dependence.Theseabnormalitiescanoccurinindividualsinwhomthereisneitherclinicalnorneuropsychologicaltestevidenceofcog-nitive defects. In individuals with chronic alcohol depend-ence,MRIhasdemonstratedacceleratinggraymatterlosswith
age,whichis tosomeextentreversiblewithabstinence,sug-gestingthatsomeofthesechangesaresecondarytochangesinbraintissuehydration.
Q7 The answer is: The CAGE.
The National Institute on Alcohol Abuse and Alcoholism(NIAAA)hasrecommendedeithertheuseofasinglealcoholscreeningquestion(SASQ)oradministrationofthe10-ques-tionAlcoholUseDisorders IdentificationTest (AUDIT) self-reportquestionnaireasstandardscreeningproceduresforthedetection of alcohol-related problems. The AUDIT with amanual is available for free (and inSpanish), andhasbeenvalidatedacrossavarietyofculturalandethnicgroups.WhenusingtheSASQcliniciansareadvisedtoaskifanindividualhas consumedfiveormore standarddrinks (for aman)ononeoccasionduringthelastyear(fourdrinksforwomen).Apositive response may indicate an alcohol-related problemandrequiresmoredetailedassessment.
Amoretraditionalalternativescreeninginterviewiscapturedbythe4-questionCAGEacronym.However,comparedtotheSASQortheAUDITtheCAGElackssensitivitytodetecthaz-ardous/problemdrinking.SimilartotheCAGEinterview,theTWEAK interview (i.e., “Tolerance,” others “Worried” aboutyourdrinking,“Eye-opener,”“Amnesia,”everwantedto/triedto“Cutdown”), isbriefandhasgoodpsychometricproper-ties,butsimilartotheCAGElackssensitivitytodetecthazard-ousdrinking.
The24-questionMichiganAlcoholismScreeningTest(MAST)isanotherself-reportmeasurewithgoodpsychometricproper-ties,butislongerthantheAUDIT.
Medicalscreensmayalsobeused.Screeningforrecentalcoholusecanbeacarriedoutwithabreathalyzer,ora sampleofurineorsaliva.Formorechronicuse,laboratorymarkers,suchas the serum gamma-glutamyl transpeptidase (GGT), themean corpuscular volume (MCV), and the carbohydrate-deficienttransferrin(CDT),canbeused.However,thesemeas-ureslacksensitivity,butcanbehelpfulifusedincombinationand when used with other screening measures, such as theAUDIT.
Screeningforalcoholwithdrawalisalsocriticalsince,asmen-tioned previously, the alcohol withdrawal syndrome can belife-threatening.TheClinicalInstituteWithdrawalAssessmentfor Alcohol Dependence (CIWA-AD) is a semi-structured,8-item,5-minuteinterview,usedtoassessandquantifysever-ity of withdrawal from alcohol. It is easy to administer andpossesses very good psychometric properties. Thus, it is anefficient and reliable method that can prevent serious, life-threatening problems and is useful to help clinicians deter-minelevelsofcare.