Embed Size (px)
Citation preview

Journal of Advanced Nursing, 1997, 25, 509-513
Alcohol-history taking hy nurses and doctorshow accurate are they really?
Lucinda Burns RN BA(Hons) MPH (Syd)Information Manager, New South Wales Drug and Alcohol Directorate, New SouthWales Health Department
and Mereditb Adams RN Grad Dip Glin Dep studies (Macq)
Clinical Nurse Consultant, Drug and Alcohol Services, Concord Hospital, New SouthWales, Australia
Accepted for publication 15 March 1996
BURNS L. & ADAMS M. (1997) Journal of Advanced Nursing 25, 509-513Alcohol-history taking hy nurses and doctors — how accurate are they really?The aim of this study was to look at bow nurses and doctors record alcoholhistories on the patients under their care and the frequency and appropriatenessof the way they use an alcohol withdrawal scale in the acute hospital setting. Toachieve these aims patient records were audited and compared at two points intime, in 1992 and 1994. Results of the study showed that nurses and doctorstook alcohol histories from patients on approximately three-quarters ofoccasions and that this level of recording has not changed over time. Theadequacy of alcohol-history taking has, however, increased for both nurses anddoctors since 1992. At that time, 71% of the alcohol histories taken by nursesand 74% of alcohol histories taken by doctors were judged to be adequate. By1994, bowever, 79% of alcobol histories taken by nurses and 77% of historiesby doctors were rated as adequate. The increase in the adequacy of historytaking by nurses was significant (x^ = 5-05; d.f. = 1; P<0-05) and the increase bydoctors was not significant (x^ = 1-03; d.f. = 1; P> 0-05). These results are seen asbeing positively associated with the major governmental nursing initiative inNew South Wales, Australia, the New South Wales Strategic Plan for theNursing Management of Alcohol and Other Drugs.
TlVTTRfinTir'TTnM simply delivering medical treatment to a situation wherepatients are empowered with infonnation ahout their own
In recent years, the emphasis in health care has turned health and are encouraged to make healthy choices. Undertowards the promotion of health as well as the curing of this scenario nurses and doctors are asked to take a holisticillness (Commonwealth Department of Health, Housing & approach to health, to emphasize empowering communi-Community Services 1993, Boscarino 1989, Hudson 1992). cations with patients and to insist upon supportive policyThis means that hospital staff such as nurses are now faced initiatives (World Health Organization 1991, Tones 1995).with the challenge of comhining health promotion activi- One area where interactions hased on this philosophy canties with their already estahlished curative services, have particular impact is in reducing the harm associatedChanging the role of the hospital to encompass health as with problem drinking.well as illness involves a shift in the system away from In 1989/90, the Australian Bureau of Statistics together
with the New South Wales Department of Health under-Correspondence Luanda Bums, 31 CoxAveBondi, NSW2026, Australia ^^"^ ^ national health survey and found that 16% of malesRequest for reprints Lucinda Bums, NSW Drug and Alcohol Directorate, and 8% of females were drinking at medium or high-risk
NSW Health Department. LMB 961, North Sydney, NSW 2060. Australia levels (Australian Bureau of Statistics 1993). Furthermore,
© 1997 Blackwell Science Ltd 509

L. Bums andM. Adams
evidence from hospital data indicates that up to 41% ofpatients seen in the New South Wales public hospitalsystem may be drinking at problem levels (Saunders &Conigrave 1990). Together, this information indicates that,when compared with other nations, Australia ranks wellabove average in its level of alcohol consumption and isone of the highest consumers of alcohol of all the English-speaking nations (Commonwealth Department of Health,Housing & Community Services 1995). On a national scale,the negative effects of this level of alcohol consumptionare huge. For example, alcohol has played a major role inover 30% of all fatal road accidents, as well as manydrownings, non-fatal road accidents, falls and other acci-dents (Commonwealth Department of Health, Housing &Community Services 1995).
Hospitals are therefore ideal settings for the detectionand meinagement of individuals drinking at problemlevels. Despite this fact, however, it has been noted thathealth care professionals such as nurses and doctors oftenhave difficulty in identifjring any, other than the most sev-erely alcohol and/or other drug-dependent, individuals(Bartek et al. 1987, Paton 1989). There is a paucity ofAustralian empirical data on the topic but research under-taken with American nurses has demonstrated that only61% of patients were asked about their use of alcohol eindother drugs on admission to hospital; any problems thatwere foimd were not recognized or dealt with (Briggs &Huetter 1984). Research undertaken with doctors in theUnited Kingdom indicates alcohol-history taking to beeven less prevalent, with doctors screening an average30% of all patients admitted to hospital wards (Rowlandet al. 1988).
Potential education agents
Despite these negative findings, the potential role of healthcare professionals to be education agents for clients withdrug- and edcohol-related problems hcis been recognized(Paton 1989). This recognition has led to initiatives suchas the launch of the Strategic Plan for Nurse Educationand Nursing Management of Alcohol and Other Drugsin November 1991 by the New South Wales HealthDepartment (New South Wales Health Department 1991).The overall aim of the Strategic Plan is to heighten thedrug and alcohol knowledge base of nurses and to expandtheir clinical role in the management of clients with theseproblems. One element of this expansion involves the edu-cation of nurses so that they c£in appropriately identify,assess, manage, and refer clients who are drinking alcoholat problematic levels. Appropriate management of clientsinvolves a variety of activities including assessment forthe potential to withdraw from alcohol.
It is of particular importance to anticipate possiblealcohol withdrawal and provide early intervention whereappropriate. This is because 'comprehensive and thought-
ful nursing care is often sufficient treatment without theneed to resort to sedative drugs' (Shanley 1987 p. 44).Cliniccd signs of potential alcohol withdrawal include; pre-vious episodes of withdrawal, an alcohol intake of morethan 10 standard drinks per day, regular use of alcoholwith other sedatives, previous history of alcohol-relateddisease, alcohol-related physical signs, abnormal pathol-ogy results, and any confusion or anxiety not due to othercauses. The use of £in alcohol withdrawal scale is war-ranted for such clients. Generally, withdrawal scales meas-ure the severity and duration of withdrawal, as well asproviding a guide to the appropriate management of clientswith this syndrome.
THE STUDY
To date, however, little empirical research has been under-taken to assess how nurses and doctors either use alcoholwithdrawal scales or record alcohol histories. For thisreason the present study aims to look (a) at how nursesand doctors currently record alcohol histories on thepatients under their care, (b) whether the way they takethese histories is adequate, (c) whether the adequacy ofalcohol-history taking has changed over time, and (d) thefrequency with which problem drinkers are placed onalcohol withdrawal scales.
Methods
In order to meet the aims of this study, patient files wereaudited at two points in time. The first audit of patientrecords took place in 1992 over a four-week period.The files of all patients admitted to five wards of a majorpublic hospital were examined. The wards involved weregastro-enterology, general medicine, general surgery,orthopaedics, and colorectal surgery. The adequacy ofalcohol-history taking by nurses and doctors was assessedby judging whether the history was (a) recorded in stan-dard drinks and/or grams of alcohol and (b) was time refer-enced (that is consumption was noted in days or per week).In total, 313 patient files were audited in 1992.
In 1994, a second audit of patient records took place.On this occasion the audit was conducted in five weirdsover a five-week period firom October to November 1994.The participating wards were gastroenterology, ortho-paedics, professorial medicine, psychiatry, and respiratorymedicine. Although it would have been ideal to use thesame wards that participated in 1992, this was impossiblebecause extensive hospital renovations were being under-taken which meant we could not access some of originalwards. The adequacy of alcohol-history taking wasassessed by the 1992 criteria.
Finally, information was also collected from thepatients' files as to whether they had been placed on analcohol withdrawal scale during their stay. The with-
510 © 1997 Blackwell Science Ltd, Joumal of Advanced Nursing, 25, 509-513

Alcohol-history taking by nurses and doctors
drawal scale used by the hospital was a shortened (nine-item) version ofthe 15-item Clinical Institute WithdrawalAssessment for Alcohol (CIWA-A). The dWA-A has beenpreviously reported as a reliable and valid measure ofalcohol withdrawal (Shaw et al. 1981). In order to assessthe use of the alcohol withdrawl scale against a 'goldstandard', nurses on the participating wards were alsorequested to ask each patient coming through the nomi-nated wards to complete an Alcohol Use DisordersIdentification Test (AUDIT). The AUDIT is a 10-itemscreening questionnaire used to detect both hazardousand harmful drinking. The questionnaire was developedby the World Health Organization, and previous researchhas noted the questionnaire to be both reliable andvalid (see Saunders et al. 1993 for an assessment ofpsychometric properties of AUDIT). Scores on theAUDIT range from 0 to 40. Zero to 7 indicates a safe levelof drinking, 8-13 indicates a hazardous level of consump-tion and 13 and over indicates harmful consiimption.Self-reported information about levels of alcohol con-sumption were then correlated with the use of thealcohol withdrawal scale to establish the proportionof clients who were drinking at hazardous levelsand who were also placed on an alcohol withdrawalscale.
whether patients had been placed on an alcohol with-drawal scale during their hospital stay and patient demo-graphics including age, gender, and medical condition onadmission.
RESULTS
Over the 1994 study period, 489 patient records were aud-ited. Of these patients, 38% were female and 62% weremale. The median age of the population was 66 years,reflecting the veteran nature of the population serviced bythe hospital. Admitting diagnoses were too diverse toallow coding.
Patients scores on the AUDIT screeningquestionnaire
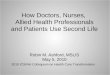
Ofthe 489 patient records that were analysed in 1994, 27%did not have completed AUDIT forms at all. The modalscore for AUDITs that were completed was zero (that isthe most frequently cited consumption category was non-drinker). Of those who scored more than zero, as Figure 1demonstrates, the mode was 1-0 and the median AUDITscore was 4-0; a safe level of drinking for both males andfemales.
Consent As the 1994 study required further patientinvolvement than the 1992 audit, consent for the studywas sought and obtained from the hospital EthicsCommittee. Consent was then also obtained to use theAUDIT from the nursing unit managers and medical direc-tors of each of the nominated wards. If they agreed to par-ticipate, the nursing unit managers of each ward werere-contacted and the study explained to them in furtherdetail. Patient consent was not sought from the patients asthe study was not regarded by the Ethics Committee as aninvasive or new procedure, and patients were alreadybeing asked about their alcohol consumption by bothdoctors and nurses.
Educational sessions were then organized and run forthe nurses on each of these wards. In these sessions, theaim and methods of the study were explained and nurseswere then requested to ask all eligible patients to completean AUDIT form during the study period. Patients wereclassified as eligible for participation in the study if theywere over 16 years of age, could speak adequate English,were well enough and consented to complete the form. Ifa patient was not eligible or refused to complete theAUDIT, nurses were asked to indicate the reason fornon-response on the questionnaire.
During the trial period each ward was visited by amember of tbe project staff daily. During this time theAUDIT forms were collected. Project staff then auditedeach of the patients records to collect information on theadequacy of alcohol-history taking by nurses and doctors,
The adequacy of alcohol-history taking hy nursesand over time
Alcohol-history taking by both nurses and doctors wereassessed for accuracy by setting them against the followingcriteria: (a) the history had to be recorded in grams ofalcohol or standard drinks, and (b) the record had to betime referenced, for example, 10 standard drinks per week.
The level of alcohol-history recording by botb nursesand doctors has not changed appreciably over time. In1992, nurses took alcohol histories on 73% of occasionsand in 1994 on 71% of occasions. With regard to doctors,in 1992 alcohol histories were taken on 72% of occasionsand in 1994 on 73% of occasions.
The adequacy of alcohol-history recording has, however,increased for both nurses and doctors since 1992. At thattime, 71% of the alcohol histories taken by nurses and74% of alcohol histories taken by doctors were judged tobe adequate. By 1994, however, 79% of alcohol historiestaken by nurses and 77% of histories by doctors were ratedas adequate. The increase in the adequacy of history takingby nurses was significant (x^ = 5-05; d.f. = l; P<0-05). Theincrease by doctors was not significant (x^ = l-03; d.f. = 1;F>0-05).
Use ofthe alcohol withdrawal scale
Overall, 19 patients (4% of the sample) were noted tohave been placed on alcohol withdrawal scales during
11997 Blackwell Science Ltd. Joumal of Advanced Nursing, 25, 509-513 511

L. Bums and M. Adams
70
60
50
^ 40co" 30
20
10
011 13
Score on AUDIT15 17 19 24 29
Figure 1 AUDIT scores
the 1994 study period. The mean age of these 19 individ-uals was 54 years and 79% of them were male. When useof the alcohol withdrawal scale was cross-tabulated withlevel of consumption it was noted that, of the 19 casesplaced on an alcohol withdrawal scale, 13 of thesepatients (68%) had AUDIT scores of 13 or more, that is,were drinking at harmful levels and had the potential togo into alcohol withdrawaL However, of the remainingpatients who had not been placed on alcohol withdrawalscales, 11 (4%) had AUDIT scores of 13 or more, i.e. weredrinking at a level warranting placement on an alcoholwithdrawal scale.
DISCUSSION
Results of past research in the area of drug- and alcohol-history taking has proved inconclusive. A study ofAmerican nurses found that only 61% took drug andalcohol histories on the patients under their care (Barteket al. 1987). An examination of history taking hy doctorsin the UK, however, has shown only 30% took alcoholhistories from their patients (Paton 1989). Our study hasgenerated more positive findings hy showing that approxi-mately three-quarters of both nurses and doctors askedpatients ahout their level of alcohol consumption and, inthe majority of cases, these histories were adequate.Furthermore, the proportion of hoth nurses and doctorswho adequately record these histories has increased overtime.
To what can we attribute this success? Past research hasdemonstrated that education about alcohol-related prob-lems is associated with an improvement in the manner inwhich alcohol histories Eire recorded (Rowland et al. 1988).In New South Wales, Australia, over the past decade therehas heen a strong level of governmental commitment made
to drug and alcohol education for hoth nurses and doctors.A major strategy in New South Wales was the StrategicPlan for the Nursing Management of Alcohol and OtherDrugs, launched in 1991 hy the New South WalesDepartment of Health. The overall mission of this particu-lar strategy was to improve the ability of nurses to assess,manage and/or refer patients with alcohol- and/or drug-related problems.
The strategy has been directed at two major sets ofactivities over this time, the production of drug andalcohol resources for clinical nurses and moves to main-stream drug and alcohol nursing hy its inclusion as a corecurriculum requirement in undergraduate nurse training.It may well he the case that the significant increase in theadequacy of history taking hy nurses is associated withthese activities.
Limitations
However, when interpreting the results of this study sev-eral hmitations should he kept in mind. Firstly, the averageage ofthe population in the study was noted to be 66 years,not surprising as the hospital was until recently a servicefor war veterans. This means the results may not be gen-eralizahle to a younger population. Nurses and doctorsmay he either more or less willing to ask a younger groupsof people about their alcohol consumption.
Secondly, the inclusion of some different wards in thesecond phase of the study could have influenced theresults. It may he the case, for example, that there was adifferent subgroup of patients on some wards and, as such,it may have proved easier to take histories on this suh-group. However, given the fact that renovations made allthe original wards inaccessible on the second audit thiswas the most practical solution available.
512 11997 Blackwell Science Ltd, Journal of Advanced Nursmg, 25, 509-513

Alcohol-history taking by nurses and doctors
Future researchThe study has opened several interesting areas for futureresearch. The fact that a number of patients comingthrough the hospital were drinking at harmful levels butwere not placed on alcohol withdrawal scales is a worryingtrend. Thus, one recommendation for future researchwould be to investigate the most appropriate means ofensuring tbat all nurses and doctors are educated in tbedetection of harmful drinkers in order to ensure tbatalcobol witbdrawal is detected early and negative bealthconsequences avoided,
A second area worth consideration is tbe investigationof stmctural issues in tbe clinical environment tbat mayinhibit the ability of both nurse and doctors in their abilityto identify and manage clients witb alcobol- and otberdrug-related problems. Results of reseMcb in tbis areacould be used to provide guidelines on tbe most effectivemetbods of retaining and enhancing drug- and alcobol-related knowledge by clinicians witbin tbe clinical con-text, Tbis information will, in tum, serve to increase andmaintain tbeir skills and knowledge in tbis area ofcritical concern
References
Australian Bureau of Statistics (1993) State of Health in NewSouth Wales. Commonwealth of Australia, Canberra,
Bartek J,, Lindeman M,, Newton M , Fitzgerald A & Hawks J(1987) Nurse-identified problems in the management ofalcoholic patients, Joumal of Studies on Alcohol 49, 62-70,
Boscarino J, (1989) Hospital wellness centres- Strategic implemen-tation, marketing and management. Health Care ManagementReview 14(2), 25-29,
Bnggs T & Huettner J (1984) Detection of the alcoholic patient
in the acute care setting In Alcoholism Treatment andRecovery (Coby M, ed), Catholic Health Care Association ofUSA, St Louis,
Commonwealth Department of Health, Housing & CommunityServices (1993) Pathways to Better Health ComcmonwealthDepartment of Health, Housing and Community Services,Canberra,
Commonwealth Department of Health, Housing & CommunityServices (1995) Statistics on Drug Abuse m Australia 1994.Commonwealth Department of Health, Housing andCommunity Services, Canberra,
Hudson T (1992) Hospitals strive to provide communities withbenefits. Hospitals July 5, 102-110
New South Wales Health Department (1991) Strategic Plan for theNursing Management of Alcohol and Other Drugs. New SouthWales Health Department, Sydney,
Paton A, (1989) Alcohol misuse and the hospital doctor, BritishJournal of Hospital Medicine 42, 394-398
Rowland N , Maynard A , Kennedy W,, Wintersgill W, & StonesW (1988) Teaching doctors to take alcohol histories- A limitedsuccess story Medical Education 22, 539-42,
Saunders J, & Conigrave K, (1990) Early identification of alcoholproblems, Canadian Medical Journal 143, 1060-1069,
Saunders J,, Aasland O,, Babor T,, De la Fuente J, & Grant M,(1993) Development ofthe alcohol use disorders identificationtest (AUDIT)- WHO collaborative project on early detection ofpersons with harmful alcohol consumption — II Addiction88, 617-629,
Shanley C, (1987) Nursing management of alcohol withdrawal.The Australian Nurses Joumal 16(11), 5-6
Sbaw J,, Kolesar C, Sellers E,, Kaplan H, & Sandor P (1981)Development of optimal treatment tactics for alcohol with-drawal, 1, Assessment and effectiveness of supportive careJoumal of Clinical Psychopharmacology 1(6), 382-9,
Tones K, (1995) The health promoting hospital Health EducationResearch • Theory and Practice August, i-iv
World Health Organization (1991) The Budapest Declaration onHealth Promoting Hospitals Budapest, 31 May-1 June 1991,
I 1997 Blackwell Science Ltd, Joumal of Advanced Nursing, 25, 509-513 513