Embed Size (px)
Citation preview
Alcohol and Dug Problems
in New Arrivals: fall-out from conflict zones
Dr David Jacka IMiA 2019
Addiction Medicine Specialist
The learning points
• Overview – the theory
• Background – the regions of origin
• Findings
• Case studies
• Conclusions and recommendations
2
Themes of published work
• Individual and collective trauma both impact
• Disintegrated communities
• Refugee camp/journey experience of trauma
• Region of origin determine pre-existing AOD use
• Loss of roles and family/cultural leaders
• Racism and barriers to learning and employment
• Culture ‘shock’ of new environments and laws
• Exposure to new soothing substances without cultural frameworks
3
Literature from Western Europe,
Canada, USA and Scandinavia
• The same cultural/language groups to Australia
• Intermixing with indigenous community problems
• Difficulties with new language and concepts
• Overwhelming of AOD treatment services
• Difficulty accepting ‘Western’ health models:
• Counseling, confidentiality, peer groups, ORT, rehabilitation, medications,
• Substance use normalisation
• Trust of police, hospital and government staff
• Maintenance medications/pharmacotherapies 4
Our service
• Adjacent to refugee health service
• Dandenong CBD near train station
• Complex pharmacotherapy clinic integrated into SECADA comprehensive community AOD
• No funding beyond hot-spot funding of Primary Care Service for PWUD and NSP
• Behind NSP so many injectors aware
• Most referrals from SECADA or NSP
5
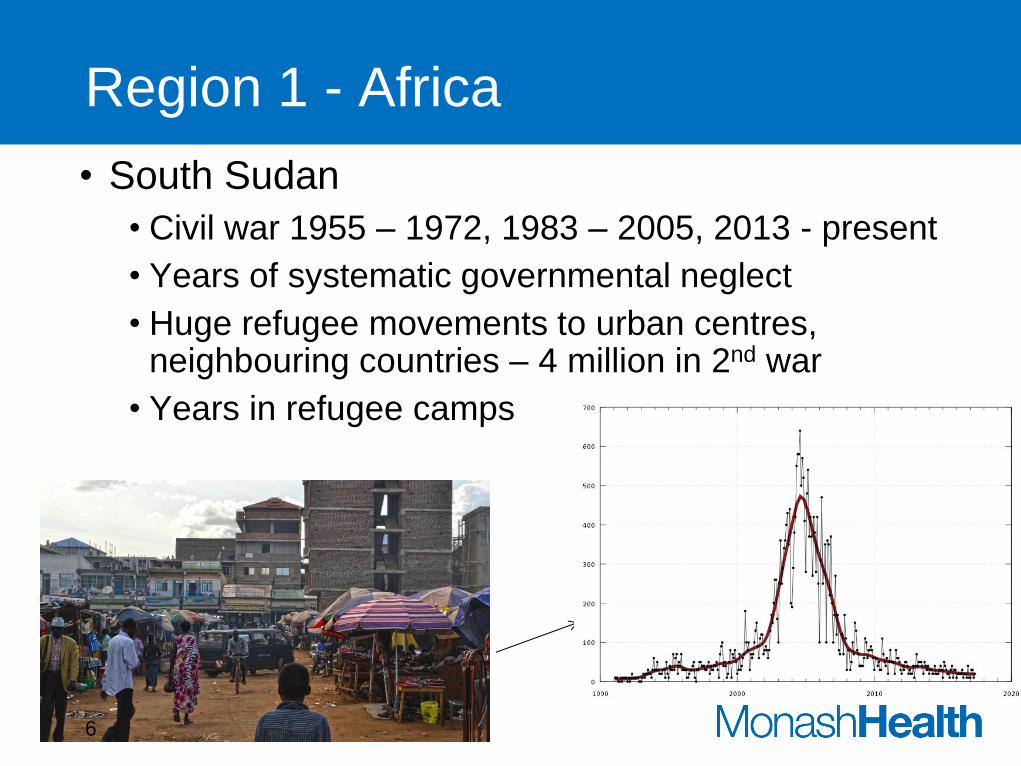
Region 1 - Africa
• South Sudan
• Civil war 1955 – 1972, 1983 – 2005, 2013 - present
• Years of systematic governmental neglect
• Huge refugee movements to urban centres, neighbouring countries – 4 million in 2nd war
• Years in refugee camps
6
Refugees – UNHCR facilitated
• South Sudan region arrivals (20,000)
• Characterised by agricultural background
• Strong village culture – absence of drug and alcohol use
• Refugee camps and battle experiences
• high stress, fear, frontier/macho cultures for men, violence
• Readily identified by colour, height,
• Many non-literate on arrival
• Educated individuals have non-negotiable quals.
7
Alcohol consumption
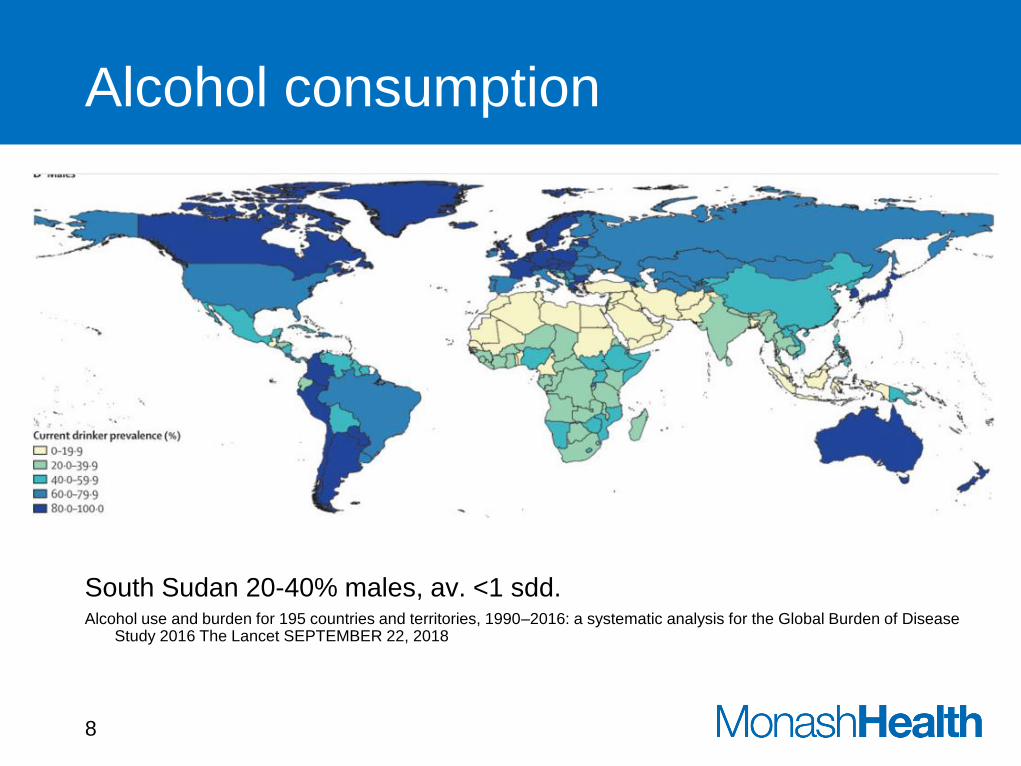
South Sudan 20-40% males, av. <1 sdd. Alcohol use and burden for 195 countries and territories, 1990–2016: a systematic analysis for the Global Burden of Disease
Study 2016 The Lancet SEPTEMBER 22, 2018
8
Peter 40yrs
• Arrived Australia 2005 from 15yrs in Kenyan Refugee Camp (>90,000 pop) with his sister
• Minimal English, barely literate
• ‘Bright’ but shy – not comfortable at school.
• Within 12 months had been taken to ED following assault in street while intoxicated
9
Peter now
• 15yrs heavy alcohol abuse 12 - 20sdd or more
• SDH x 3, Basal skull #
• Pancreatitis 3 times
• 69 hospital attendances since 2010 – mostly intoxicated
• 31 inpatient stays
• >$100,000 unpaid fines for intoxication, fights, fares
• Developed Grand Mal Seizures 2016 2° to ABI
• “I have no other friends, nothing else to do but drink”
• VCAT – OPA/State Trustees 2017
• Moved to SRS mid 2018 - medications supervised.
• no hospital attendances since.
10
MGD – “55yrs” female
• Previous ‘farmer’, daughter + 2 g’daughters in Juba
• Brought to Australia by two ‘nephews’
• Unable to work with back pain, looks older
• Not literate and little English.
• Daughter’s application for resettlement refused
• Started drinking whiskey 20sdd
• Lonely, sad and isolated
• Falls when intoxicated
• Sees no hope.
-> Engaged with NGO 11
Region 2 - South Asia
• South Asia (partic. Sri Lanka)
• Increasing alcohol use and heroin at home
• Disrupted community, some battle trauma and sea voyages
• Expectation of financial remittances back home
• Expectation of family decision making
• Arranged marriages and employment “who you know”
• Difficult if pre-existing issues and loneliness
12

GB 54yrs – Sri Lankan Tamil by boat
Self referred to Drug Treatment
• 2 yrs use of traditional Ayervedic Medicine
• Unable to stop using and financial problems
• Buying from local Dandenong Indian Shop
• Unclear indication
• Taking up to ‘40tab’/day
• $100/bottle
• Cannot sleep without
• Back pain worsening
• Discord with wife/family
13
What is Multani KAMINI VIDRAWAN RAS?
Curing Premature Ejaculation Sexual Disorder in Males (from EBAY)
• Multani Kamini Vidrawan Ras also acts well in other men disorders such as Erectile Dysfunction, Low Libido and Impotency. It has such wonderful ingredients which boosts energy level in men to achieve extreme pleasure and satisfaction. It is safe to use ayurvedic medicine with no side effects.
• Multani Kamini Vidrawan Ras is a herbo-mineral safe to use ayurvedic medicine, which comes in the form of pills having excellent results in curing Premature Ejaculation Sexual Disorder in males. Premature Ejaculation which also known as early discharge disorder happens due to high anxiety level, stress, lack of energy, long sitting jobs and bad life style.
• Kamini Vidrawan Ras controls the excitement level which gives more time to men to satisfy himself and his partner.
Benefits of Multani Kamini Vidrawan Ras :
• Cures Premature Ejaculation or Early discharge by increase sexual intercourse time.
• Helps in low erection by increasing flow of blood in the penis which is best for harder erections.
• Treatment of Impotency.
• Cures Lack of Libido.
• Thickens the Semen.
Dosage of Multani Kamini Vidrawan Ras 40 tab (10gm)(Papaver somniferum) :
• In general person suffering from sexual disorders such as premature ejaculation and erection problem can take 1-2 Pills of Kamini Vidrawan Ras after breakfast and 1-2 Pills before bed with milk.
Did very well on Suboxone and referred back to GP.
14
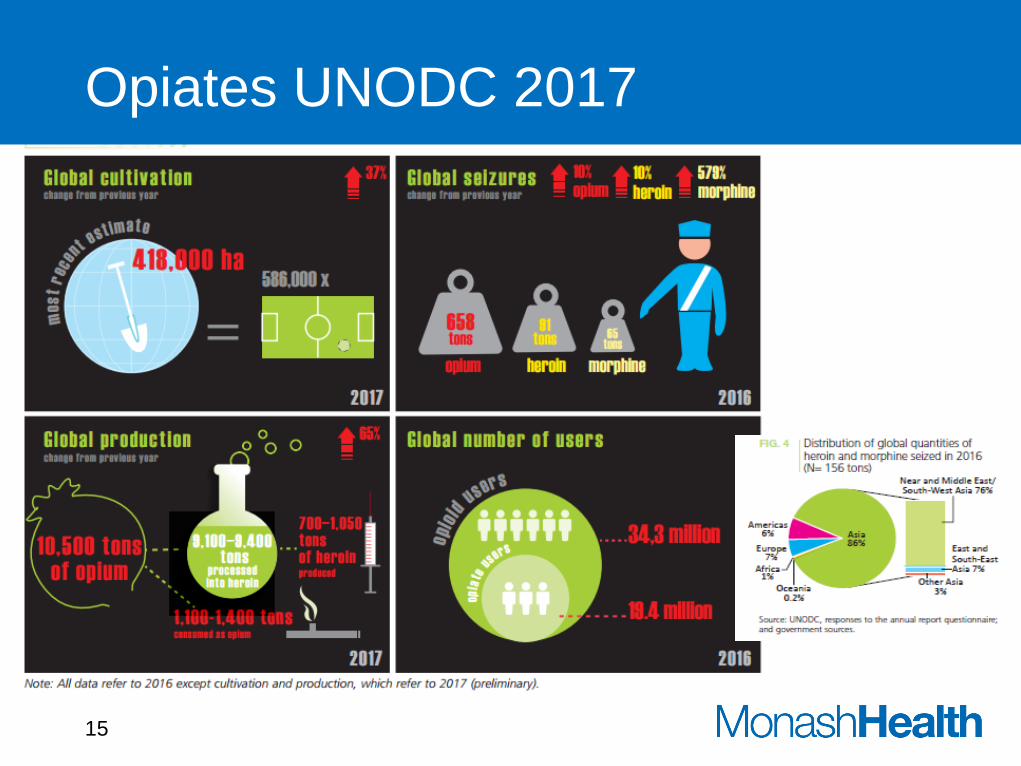
Opiates UNODC 2017
15
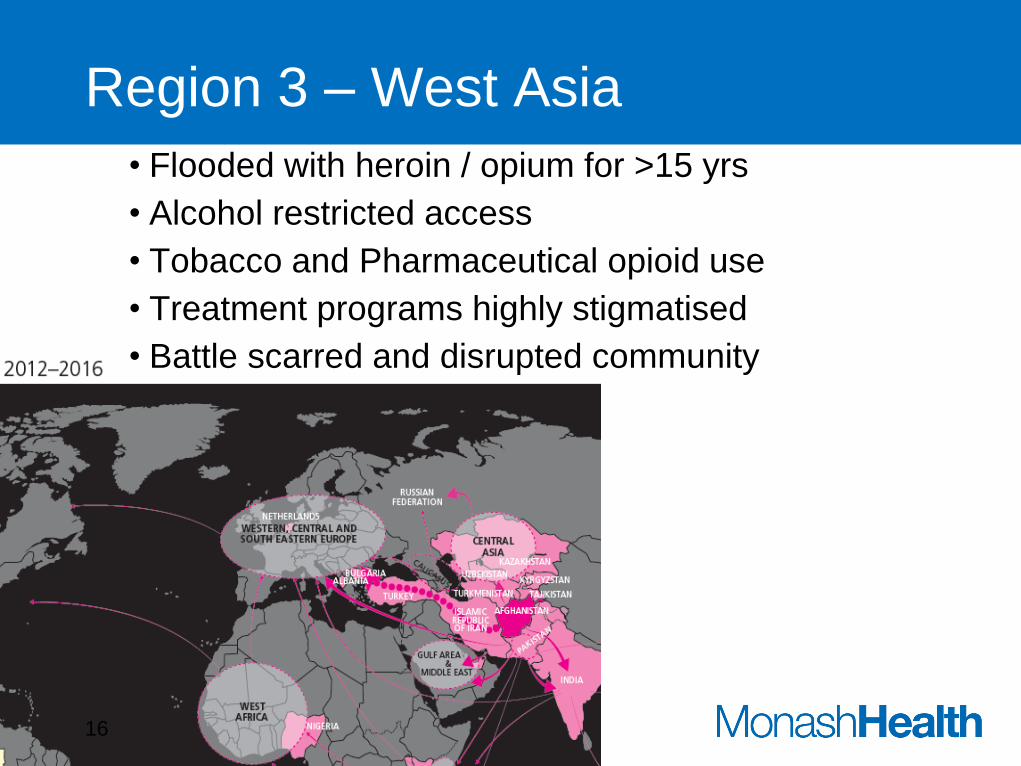
Region 3 – West Asia
• Flooded with heroin / opium for >15 yrs
• Alcohol restricted access
• Tobacco and Pharmaceutical opioid use
• Treatment programs highly stigmatised
• Battle scarred and disrupted community
16
‘Mo’ 33 yrs male – by boat
• Iraq (Kurdish)
• Sustained war, heroin transit,
• Political limitations, disrupted economy/education
• Smoking heroin, opium and ‘black tar’ since 14yrs age
• Lost two close family members in war
• In Australia
• Had visa rejected – no Medicare!
• Injured leg at work
• Restarted oxycodone, then heroin
• Depressed, suicide attempts x 2
• Diagnosed PTSD, MDD, ? ICE psychosis
• Settled with Suboxone Methadone 17
Hossein 51yr old male by boat
• In Iran, truck driver
• Islamic theocracy – not religious.
• 5% opiate dep. males – denies use.
• Limited opportunity – conflict with neighbours and work
• In Australia 3yrs with wife and adult children
• Dependent on Cigarettes, Pandeine Forte, OTC codeine
• Reluctant to work with back pain
• Depressed and reluctant to engage with Suboxone
• Settled eventually with on/off Suboxone
• Happy!!
18
When to Consider Pharmacotherapy
• Medication Assisted Treatment is the new standard of care for opiates, tobacco, alcohol.
• Peak efficacy requires MAT, counselling, peer or group support and frequent physician monitoring.
• Depression and unemployment a high priority for treatment
19
Counselling / behaviour motivation
• CBT teaches individuals to recognize and stop negative
patterns of thinking and behavior.
• Help be aware of the stressors, situations, and feelings that lead to
substance use so that the person
• Help avoid stressors or act differently when they occur.
• Motivational enhancement therapy
• helps people with substance use disorders to build motivation and
commit to specific plans to engage in treatment and seek recovery.
• Difficult to engage family with male domination an extra impediment
• 12-step facilitation therapy
• Rarely helpful with refugee groups
• Language, culture, religion,
20
Conclusions
Identify the need of your patients for urgent treatment - work and remittances a high priority Difficult to identify with all of the background and priorities of these people for whom transparency and trust are an issue Replacement pharmacotherapies remarkably effective without transgenerational drug use or trauma. ORT daily cost a big issue. Difficult to maintain medication adherence initially for an appropriately chronic disease trajectory – want for ‘quick fix’ Difficult care in absence of Medicare for fees, pathology, radiology or referral for specialist opinion Language appropriate GPs just as reluctant to accept ORT - many have no desire to be seen in/by their own ‘community’.
21
Acknowledgements
• Complex Pharmacotherapy clinic staff
• Dandenong Refugee Health Service
• Nurse Practitioner and our Registrars
22