Embed Size (px)
Citation preview
ALARIS IV PUMP and IV CARE
Teaching Points
Program patient account number NOT medical record number in the Alaris pump.
Program correct library. Examples: Med/Surg, Oncology, SDU/CPCU.
Check every new admit and transfer for the account number and correct library.
Check that every fluid is in correct Guardrail. NOTHING IN BASIC INFUSION.
No looping. Cap ends of lines with green curos tip.
All ports and injection ports need a green curos cap for PIVs and Central Lines.
Hang the primary infusion at least 12 – 18 inches below secondary infusions so that the secondary will infuse properly.
Date your TKO IV fluids with a label.
TKO fluids should have an order.
Check compounded medications for expiration date on the pharmacy label. Compounded IV bags made in pharmacy are good for 24 hours. Premixed and commercially made IV bags are good for 96 hours.
Patient Controlled Analgesia (PCA) for pain needs maintenance fluids (at least TKO fluids) infusing. Attach maintenance IV tubing to the Y-port of the PCA tubing.
Label all IV tubing with a label with name of what is infusing if patient has more than a maintenance fluid.
IV tubing changed every 96 hours. Label the tubing with the day it needs to be changed.
Use back prime method if patient has multiple IVPBs and compatible with the maintenance fluids.
Central line site care is weekly as long as tegaderm dressing remains intact and Biopatch is not saturated with fluid or blood. Mediport dressing change is done when needles are changed weekly.
Change out trauma field and trauma room IV sites within 24 hours.
Hand Off (shift change) Independent Double Check in patient room for all High Risk High Alert Infusions. Document in EPIC as Rate Verify. Use Handoff for Heparin infusions.
What does < mean?
What does ≥ mean?
Alarm audio volume on IV pump should not be set below level 3.
Know location of Micromedex for drug and IV fluid compatibility on the Forum
Use DRUG CALC function if the drug is not in the library. Notify the supervisor and pharmacy. select channel -> select Gaurdrail Drugs -> select DRUG CALC at the bottom of the screen -> enter appropriate parameters for the drug
7West Specific Unit Standards
Central line care is every Wednesday Tubing change and needleless connectors are changed on Sundays and Wednesdays
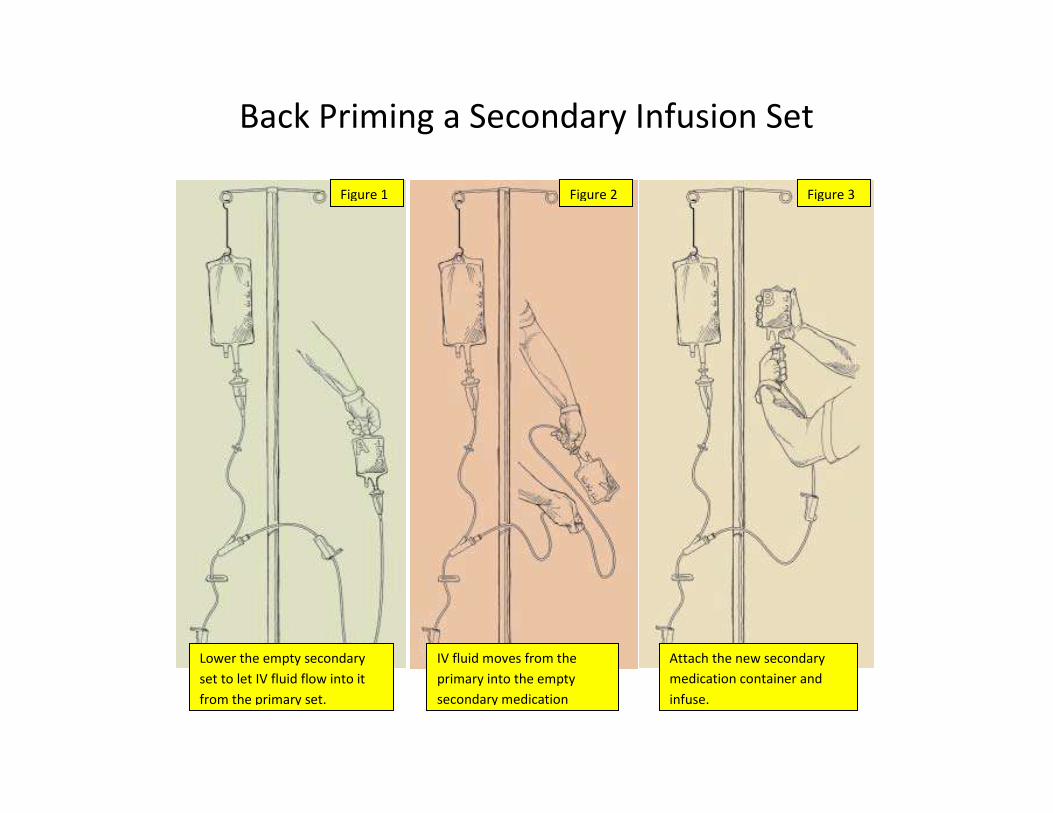
Back Priming a Secondary Infusion Set
Lower the empty secondary
set to let IV fluid flow into it
from the primary set.
Figure 1 Figure 2 Figure 3
IV fluid moves from the
primary into the empty
secondary medication
container.
Attach the new secondary
medication container and
infuse.
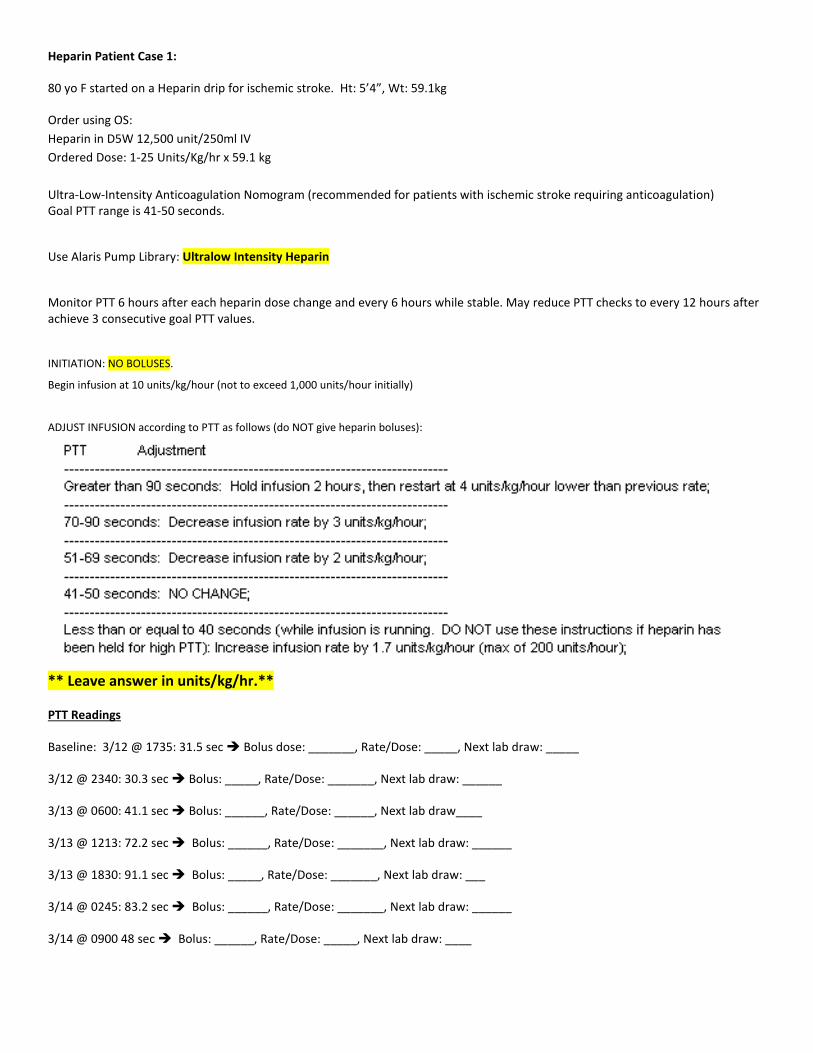
Heparin Patient Case 1:
80 yo F started on a Heparin drip for ischemic stroke. Ht: 5’4”, Wt: 59.1kg
Order using OS:
Heparin in D5W 12,500 unit/250ml IV
Ordered Dose: 1-25 Units/Kg/hr x 59.1 kg
Ultra-Low-Intensity Anticoagulation Nomogram (recommended for patients with ischemic stroke requiring anticoagulation)Goal PTT range is 41-50 seconds.
Use Alaris Pump Library: Ultralow Intensity Heparin
Monitor PTT 6 hours after each heparin dose change and every 6 hours while stable. May reduce PTT checks to every 12 hours afterachieve 3 consecutive goal PTT values.
INITIATION: NO BOLUSES.
Begin infusion at 10 units/kg/hour (not to exceed 1,000 units/hour initially)
ADJUST INFUSION according to PTT as follows (do NOT give heparin boluses):
** Leave answer in units/kg/hr.**
PTT Readings
Baseline: 3/12 @ 1735: 31.5 sec Bolus dose: _______, Rate/Dose: _____, Next lab draw: _____
3/12 @ 2340: 30.3 sec Bolus: _____, Rate/Dose: _______, Next lab draw: ______
3/13 @ 0600: 41.1 sec Bolus: ______, Rate/Dose: ______, Next lab draw____
3/13 @ 1213: 72.2 sec Bolus: ______, Rate/Dose: _______, Next lab draw: ______
3/13 @ 1830: 91.1 sec Bolus: _____, Rate/Dose: _______, Next lab draw: ___
3/14 @ 0245: 83.2 sec Bolus: ______, Rate/Dose: _______, Next lab draw: ______
3/14 @ 0900 48 sec Bolus: ______, Rate/Dose: _____, Next lab draw: ____

Heparin Patient Case 2:
47 yo M started on a Heparin drip for a DVT. Ht: 6’3”, Wt: 125 kg
Order using OS:
Heparin in D5W 12,500 unit/250ml IV
Ordered Dose: 1-25 Units/Kg/hr x 125 kg
High-Intensity Anticoagulation Nomogram (recommended for deep vein thrombosis, pulmonary embolism, and aquapheresistherapy)
Goal PTT range is 65-90 seconds.
Use Alaris Pump Library: Hi Intensity Heparin >/= 125 kg
Monitor PTT 6 hours after each heparin dose change and every 6 hours while stable. May reduce PTT checks to every 12 hours afterachieve 3 consecutive goal PTT values.
Initial Bolus: 80 units/kg IV x 1 (equals __________ units IV x 1; do not exceed 10,000 units)
INITIATION: After initial bolus (if ordered), begin infusion at 14.4 units/kg/hour (for this patient's weight, maximum initial rate of1,800 units/hour achieved.)
ADJUST INFUSION according to PTT as follows:
** Leave answer in units/kg/hr.**
PTT Readings
Baseline: 3/12 @ 1735 : 31.5 sec Bolus dose: ____, Rate/Dose:______, Next lab draw: _____
3/12 @ 2340: 46.3 sec Bolus: __________, Rate/Dose: _______, Next lab draw: ________
3/13 @ 0600: 67.1 sec Bolus: _________, Rate/Dose: ___________, Next lab draw: ________
3/13 @ 1213: 93.2 sec Bolus: _____,__ Rate/Dose: ______________, Next lab draw: _________
3/13 @ 1830 103.1 sec Bolus: _______, Rate/Dose: ____________, Next lab draw: ___________
3/14 @ 0245: 93.4 sec Bolus: _____, Rate/Dose: _____________, Next lab draw: __________
3/14 @ 0900 63 sec Bolus: ______, Rate/Dose: ______________, Next lab draw: __________
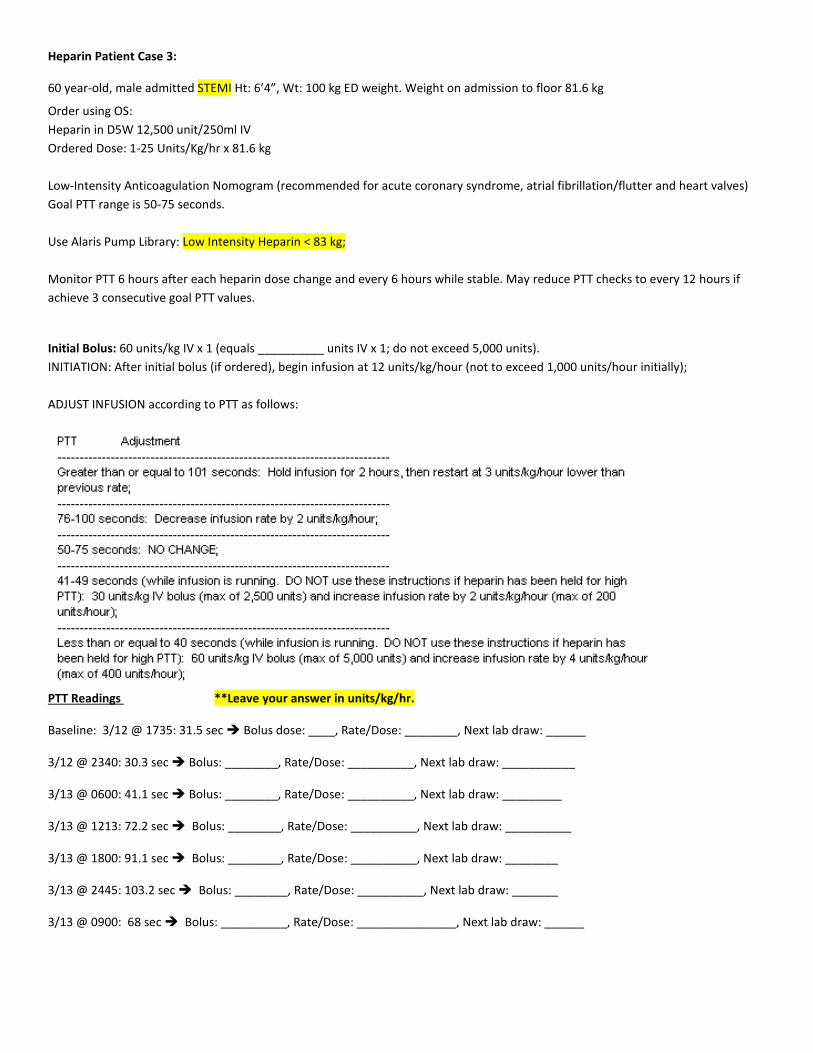
Heparin Patient Case 3:
60 year-old, male admitted STEMI Ht: 6’4”, Wt: 100 kg ED weight. Weight on admission to floor 81.6 kg
Order using OS:
Heparin in D5W 12,500 unit/250ml IV
Ordered Dose: 1-25 Units/Kg/hr x 81.6 kg
Low-Intensity Anticoagulation Nomogram (recommended for acute coronary syndrome, atrial fibrillation/flutter and heart valves)
Goal PTT range is 50-75 seconds.
Use Alaris Pump Library: Low Intensity Heparin < 83 kg;
Monitor PTT 6 hours after each heparin dose change and every 6 hours while stable. May reduce PTT checks to every 12 hours if
achieve 3 consecutive goal PTT values.
Initial Bolus: 60 units/kg IV x 1 (equals __________ units IV x 1; do not exceed 5,000 units).
INITIATION: After initial bolus (if ordered), begin infusion at 12 units/kg/hour (not to exceed 1,000 units/hour initially);
ADJUST INFUSION according to PTT as follows:
PTT Readings **Leave your answer in units/kg/hr.
Baseline: 3/12 @ 1735: 31.5 sec Bolus dose: ____, Rate/Dose: ________, Next lab draw: ______
3/12 @ 2340: 30.3 sec Bolus: ________, Rate/Dose: __________, Next lab draw: ___________
3/13 @ 0600: 41.1 sec Bolus: ________, Rate/Dose: __________, Next lab draw: _________
3/13 @ 1213: 72.2 sec Bolus: ________, Rate/Dose: __________, Next lab draw: __________
3/13 @ 1800: 91.1 sec Bolus: ________, Rate/Dose: __________, Next lab draw: ________
3/13 @ 2445: 103.2 sec Bolus: ________, Rate/Dose: __________, Next lab draw: _______
3/13 @ 0900: 68 sec Bolus: __________, Rate/Dose: _______________, Next lab draw: ______
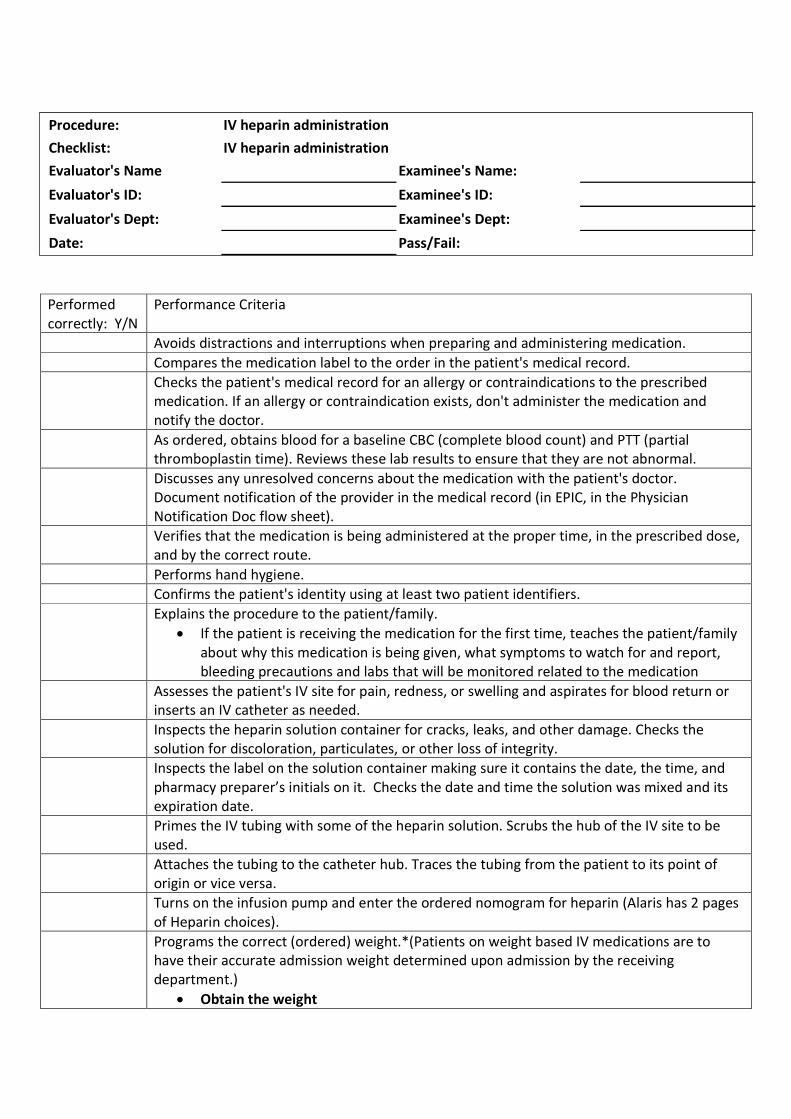
Procedure: IV heparin administration
Checklist: IV heparin administration
Evaluator's Name Examinee's Name:
Evaluator's ID: Examinee's ID:
Evaluator's Dept: Examinee's Dept:
Date: Pass/Fail:
Performedcorrectly: Y/N
Performance Criteria
Avoids distractions and interruptions when preparing and administering medication.
Compares the medication label to the order in the patient's medical record.
Checks the patient's medical record for an allergy or contraindications to the prescribedmedication. If an allergy or contraindication exists, don't administer the medication andnotify the doctor.
As ordered, obtains blood for a baseline CBC (complete blood count) and PTT (partialthromboplastin time). Reviews these lab results to ensure that they are not abnormal.
Discusses any unresolved concerns about the medication with the patient's doctor.Document notification of the provider in the medical record (in EPIC, in the PhysicianNotification Doc flow sheet).
Verifies that the medication is being administered at the proper time, in the prescribed dose,and by the correct route.
Performs hand hygiene.
Confirms the patient's identity using at least two patient identifiers.
Explains the procedure to the patient/family.
If the patient is receiving the medication for the first time, teaches the patient/familyabout why this medication is being given, what symptoms to watch for and report,bleeding precautions and labs that will be monitored related to the medication
Assesses the patient's IV site for pain, redness, or swelling and aspirates for blood return orinserts an IV catheter as needed.
Inspects the heparin solution container for cracks, leaks, and other damage. Checks thesolution for discoloration, particulates, or other loss of integrity.
Inspects the label on the solution container making sure it contains the date, the time, andpharmacy preparer’s initials on it. Checks the date and time the solution was mixed and itsexpiration date.
Primes the IV tubing with some of the heparin solution. Scrubs the hub of the IV site to beused.
Attaches the tubing to the catheter hub. Traces the tubing from the patient to its point oforigin or vice versa.
Turns on the infusion pump and enter the ordered nomogram for heparin (Alaris has 2 pagesof Heparin choices).
Programs the correct (ordered) weight.*(Patients on weight based IV medications are tohave their accurate admission weight determined upon admission by the receivingdepartment.)
Obtain the weight
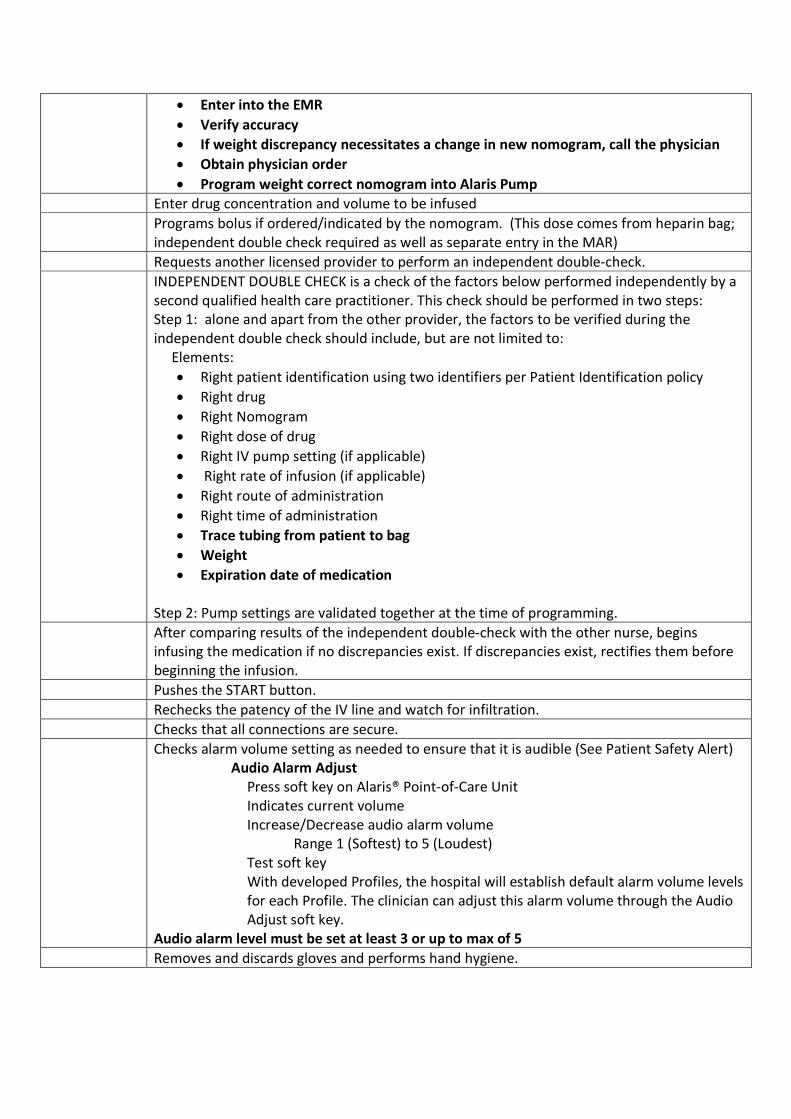
Enter into the EMR
Verify accuracy
If weight discrepancy necessitates a change in new nomogram, call the physician
Obtain physician order
Program weight correct nomogram into Alaris Pump
Enter drug concentration and volume to be infused
Programs bolus if ordered/indicated by the nomogram. (This dose comes from heparin bag;independent double check required as well as separate entry in the MAR)
Requests another licensed provider to perform an independent double-check.
INDEPENDENT DOUBLE CHECK is a check of the factors below performed independently by asecond qualified health care practitioner. This check should be performed in two steps:Step 1: alone and apart from the other provider, the factors to be verified during theindependent double check should include, but are not limited to:
Elements:
Right patient identification using two identifiers per Patient Identification policy
Right drug
Right Nomogram
Right dose of drug
Right IV pump setting (if applicable)
Right rate of infusion (if applicable)
Right route of administration
Right time of administration
Trace tubing from patient to bag
Weight
Expiration date of medication
Step 2: Pump settings are validated together at the time of programming.
After comparing results of the independent double-check with the other nurse, beginsinfusing the medication if no discrepancies exist. If discrepancies exist, rectifies them beforebeginning the infusion.
Pushes the START button.
Rechecks the patency of the IV line and watch for infiltration.
Checks that all connections are secure.
Checks alarm volume setting as needed to ensure that it is audible (See Patient Safety Alert)Audio Alarm Adjust
Press soft key on Alaris® Point-of-Care UnitIndicates current volumeIncrease/Decrease audio alarm volume
Range 1 (Softest) to 5 (Loudest)Test soft keyWith developed Profiles, the hospital will establish default alarm volume levelsfor each Profile. The clinician can adjust this alarm volume through the AudioAdjust soft key.
Audio alarm level must be set at least 3 or up to max of 5
Removes and discards gloves and performs hand hygiene.
Annual Competency Validation Documentation
Employee Name _______________________ Job Title _____________________ Dept/Unit _______________
Competency Resource Codes Competency evaluated according to the most current version of the following:
A. Policy & Procedure (Include title / section of P&P) B. Unit Specific Policy (Include title / section of P&P) C. Nursing Reference Center Plus D. Manufacturer’s Instructions E. Required Reading
F. Required DVDG. Age Specific Binder H. National Organization Guidelines (Organization) I. Order Set
Validation Method Codes Procedural / Technical Competency.
Validation Method
Process Competency.
Validation Method 1. Demonstration / Observation 2. Skills Lab 3. Proficiency Testing / Quality Control
4. Demonstration / Observation 5. Chart Review 6. Verbalization 7. Peer Review
Completed Competencies Evaluator’s Signature Indicates Validation of Competency
Title of competency Competency Resource (Use Codes/title/date/section)
Validation (Use Codes)
Alaris Pump D. Alaris Pump 1,2,4,6
Date Employee Signature Evaluator Signature
Title of competency Competency Resource (Use Codes/title/date/section)
Validation (Use Codes)
Heparin Calculations & Pump Programming A. Therapeutic Anticoagulant with Heparin Products
I. Adult Therapeutic Anticoagulation Order Set
1,2,4,5,6
Date Employee Signature Evaluator Signature
Title of competency Competency Resource
(Use Codes/title/date/section) Validation
(Use Codes)Heparin Independent Double Check A. Medications High Alert & High Risk 1,2,4,5,6
Date Employee Signature Evaluator Signature
Comments- ______________________________________________________________________ ________________________________________________________________________________
Employee # _____________
Heparin Tips and Tricks
Reminders to aid you in administering and monitoring Heparin infusions:
When documenting a bolus or a rate change, to ensure consistency, document the dose not the rate.
When giving a bolus, make sure to document on the corresponding bolus section of the MAR as
total units administered. ONCE as the initial bolus when initiating the infusion and PRN for ongoing boluses based on PTT.
Always use the Heparin dose calculator to determine any dose changes. Order a one-time Timed draw if it is a lab draw. Use the PRN PTT order to print a label on the unit
if it is a nurse draw.
Draw PTT on time, 30 minute grace before and after due time. When starting the infusion, make sure to select the correct infusion pump profile for your unit. Upon patient transfer, make sure the patient is in the correct infusion pump profile for your unit. Upon initiation and during handoff, confirm that there is the appropriate anticoagulation signage
above the patient’s bed per unit standard. When performing an independent double check, each verifying nurse checks the information that
is entered in the IV pump and MAR. When ordering ongoing PTTs, if the value is therapeutic and there is no dose change, order the
next PTT based on the time of the last draw, not the time you receive the value. When ordering ongoing PTTs, if the value is NOT therapeutic, order the next PTT based on the
time of the dose change. If you have stopped an infusion for a PTT that is too great, remember to restart in 2 hours as
ordered less than prior rate and check PTT in 6 hours. If there is any kind of delay in therapy or monitoring, always notify the physician and document
the reason in your nurse’s note. Lock the IV pump so that settings can’t be changed accidently per unit standard.
Do not change the weight on the Alaris pump. The weight in the initial orders and MAR must match the pump even as the patient weight changes and is upated in EPIC.
Heparin infusion dose changes and new bags are checked with the unit supervisor per unit standard.

Name: _________________________________________________________ Unit: __________________________
Employees Initials upon completion
Task number and description
1: Manual Priming PCA administration set I understand importance to prime set prior to attaching to patient and to clamp set preventing uncontrolled flow.
2: Alaris® PCA Module Channel Release Lever I understand the channel release lever is located behind the PCA Module door.
3: System Start-Up
I understand what happens when I select NEW PATIENT? “YES” or “NO”. I understand what a Patient Care Profile is and how to change it.
4: Loading Syringe I understand the importance to identify the syringe manufacture and syringe size when loading syringe.
I understand to insert syringe barrel flange between Barrel Flange Grippers (gray in color). I understand to always clamp off fluid flow to patient to prevent accidental bolus before loading or unloading syringe.
5: Preparing Infusion – Selecting Syringe Type & Size I understand to press and hold the prime key to deliver 2 mL prime volume and repeat step as needed.
6: Programming “PCA Dose Only” Infusion Mode
I understand to follow onscreen prompts when programming this Infusion Mode and all Infusion Modes. I understand to always select “Max Limit” soft-key to program a Maximum Hourly Limit.
7: Changing Infusion Mode to “PCA Dose + Continuous”
I understand (if this feature is enabled) how to give an additional clinician bolus dose. 9: Stopping a Programmed PCA Dose, Loading Dose or Bolus Dose
I understand how to stop a PCA Dose, Loading Dose or Bolus Dose once it has been initiated. Change Programming Parameters During Infusion I understand how to change programming during infusion. Patient History Viewing and Clearing I understand Patient History has the option to view in 1, 2, 4, 8, 12 or 24 hour intervals. Viewing Drug Event History Viewing PCA Pause Alarm Event Data I understand to access Drug Event History function to view patient PCA Pause value and time of event. Clinical Advisory: I understand user message appears reminding of specific hospital standards of practice. Guardrails® Soft Limits I understand pressing “YES” to Guardrails® Soft Limit will override soft limit set by hospital. I understand Guardrails® Hard Limit must be “Reprogrammed” and cannot be overridden. Check Syringe Alarm: I understand to check Syringe Barrel Clamp and / or Plunger Grippers. Channel Disconnected Alarm: I understand channel became disconnected while in operation. Hourly Maximum Limit Alarm I understand the Maximum Drug amount has been delivered for programmed hourly dose interval. I understand how to silence alarm tone and the alarm tone will re-sound if additional dose is requested
during Maximum Limit Alarm. Occluded – Patient Side Alarm: I understand the PCA Module has detected increased back pressure. Powering Off I understand how to power off the Alaris® System. I understand if only one module was in operation and that one module was powered off that the Alaris®
System will power off.
My signature verifies that I have completed and understand the tasks described above. In addition, I verify that I have received the
Alaris® PCA Module training.
Employee Signature: ______________________________________ Date: ______________________
Evaluator Signature: ______________________________________ Date: ______________________
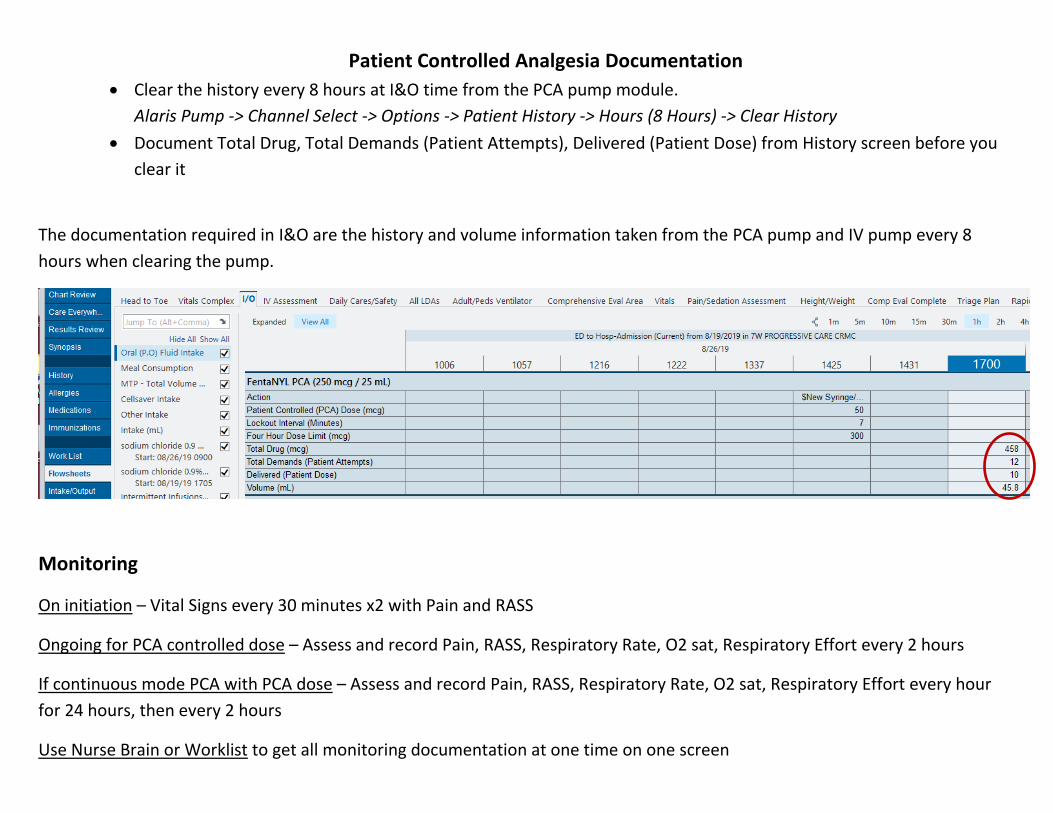
Patient Controlled Analgesia Documentation
Clear the history every 8 hours at I&O time from the PCA pump module.
Alaris Pump -> Channel Select -> Options -> Patient History -> Hours (8 Hours) -> Clear History
Document Total Drug, Total Demands (Patient Attempts), Delivered (Patient Dose) from History screen before you
clear it
The documentation required in I&O are the history and volume information taken from the PCA pump and IV pump every 8
hours when clearing the pump.
Monitoring
On initiation – Vital Signs every 30 minutes x2 with Pain and RASS
Ongoing for PCA controlled dose – Assess and record Pain, RASS, Respiratory Rate, O2 sat, Respiratory Effort every 2 hours
If continuous mode PCA with PCA dose – Assess and record Pain, RASS, Respiratory Rate, O2 sat, Respiratory Effort every hour
for 24 hours, then every 2 hours
Use Nurse Brain or Worklist to get all monitoring documentation at one time on one screen




























