Embed Size (px)
Citation preview

ALABAMA PSYCHIATRICPHYSICIANS CONFERENCE
APRIL 8-10, 2016SANDESTIN GOLF AND
BEACH RESORT
Prescribing Chronic Opioids Regulatory Implications.
WHAT IT WAS LIKE, WHAT HAPPENED AND WHAT IT IS
LIKE NOW
James Harrow M.D. Ph.D.Medical Director
Alabama Physician Health Program

No Disclosures
Dr. Harrow has no disclosure of real or apparent conflict related to the content of
this presentation.
Objectives
(1) To describe the history of prescription opioid abuse.
(2) To identify factors which have contributed to prescription opioid abuse in America.
(3) To summarize risks of prescribing controlled substances for chronic, non-life threatening conditions.
(4) Postscript

Psychiatrist Dr. Narendra Nagareddy from Georgia, is accused of overprescribing opiates and benzodiazepine to his patients.

Raided: Following a raid by Drug Enforcement Administration agents on Thursday, Dr. Narendra Nagareddy was arrested at his office in Jonesboro.
A doctor in Georgia has been labelled “Dr. Death” after he was arrested on suspicion of overprescribing prescription medication to his patients.
Of the 36 patients that have died within psychiatrist Narendra Nagareddy’s care, 12 have been killed from an overdose on prescribed medication.
Following a raid by Drug Enforcement Administration agents on Thursday, Dr. Nagareddy was arrested at his office in Jonesboro.
Nearly 40 federal and local agents raided his offices, before they seized assets from his home.

“He’s charged with prescribing pain medication which is outside his profession as a psychiatrist and not for a legitimate purpose for the patient,” said Clayton county district attorney Tracy Graham Lawson.
Since his license was issued in 1999, the doctor has received several online complaints referencing his prescription methods.
Aside from the criminal charges, the Clayton County District Attorney's Office has also applied to seize Nagareddy's assets under the Racketeer Influenced and Corrupt Organizations Act.

WHAT IT WAS LIKE
“Opium teaches only one thing, which is that aside from physical suffering, there is nothing real."
"There is always a need for intoxication: China has opium, Islam has hashish, the West has woman.“
André Malraux
(1901-1976)MAN'S FATE

Opium Poppy Papaver somniferumThe Plant Of Joy
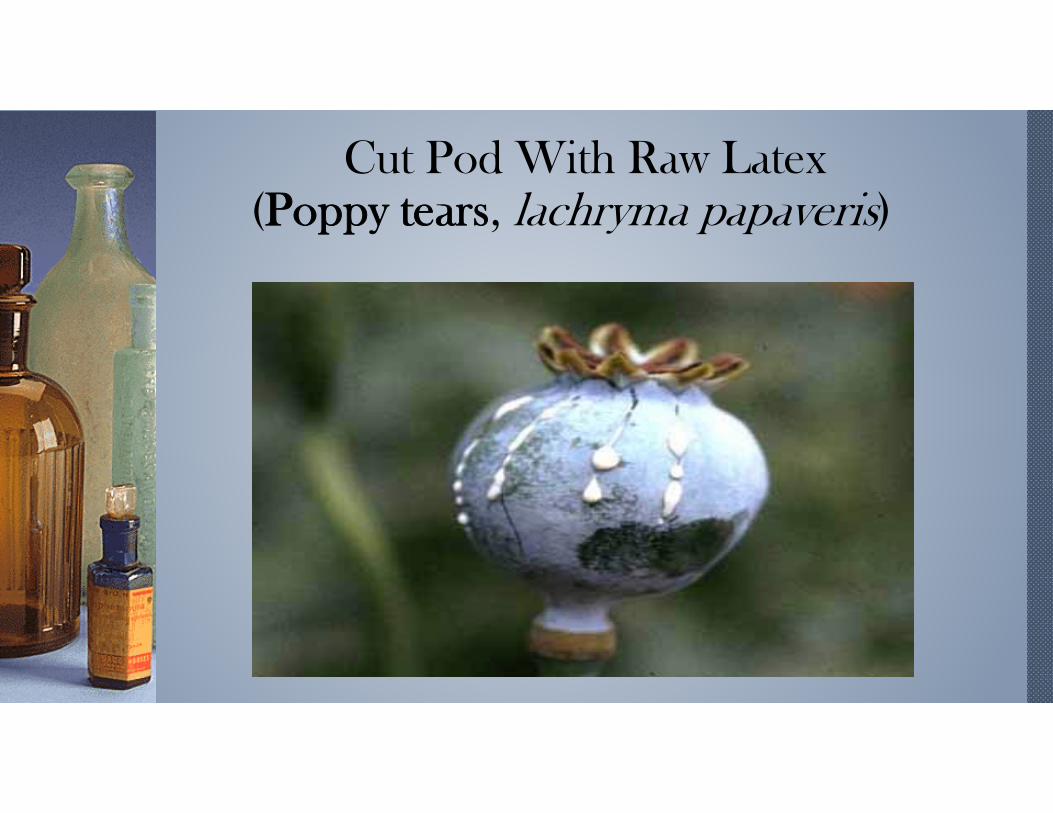
Cut Pod With Raw Latex(Poppy tears, lachryma papaveris)

A Short History Of Opiumc.3400 B.C.
The opium poppy is cultivated in lower Mesopotamia. The Sumerians refer to it as Hul Gil, the “joy plant.”
c.1300 B.C.
In the capital city of Thebes, Egyptians begin cultivation of opium thebaicum.
c.460 B.C.
Hippocrates, "the father of medicine", dismisses the magical attributes of opium but acknowledges its usefulness as a narcotic and styptic in treating internal diseases, diseases of women and epidemics.

1300’s Opium disappears for two hundred years from European historical record. Opium had become a taboo subject for those in circles of learning during the Holy Inquisition. In the eyes of the Inquisition, anything from the East was linked to the Devil.
1500The Portuguese initiate the smoking of opium. They discovered the effects were instantaneous.
1601Ships chartered by Elizabeth I are instructed to purchase the finest Indian opium and transport it back to England.
1680English apothecary, Thomas Sydenham introduces Sydenham's Laudanum, a compound of opium, sherry wine and herbs. His pills along with others of the time become popular remedies for numerous ailments.

1700The Dutch export shipments of Indian opium to China and introduce the practice of smoking opium in a tobacco pipe to the Chinese.
1750The British East India Company assumes control of Bengal and Bihar, opium-growing districts of India. British shipping dominates the opium trade out of Calcutta to China.
1799China's emperor, Kia King, bans opium completely, making trade and poppy cultivation illegal.
1800The British Levant Company purchases nearly half of all of the opium coming out of Turkey strictly for importation to Europe and the United States.
Elizabeth Barrett Browning
The English Victorian poet Elizabeth Barrett Browning initially took laudanum to treat her childhood spinal tuberculosis. She became a lifelong addict. However, for her opium was a source of poetic inspiration; and letters between Elizabeth and her husband Robert Browning abound with images of scarlet poppies.

1803
Friedrich Serturner of Paderborn, Germany discovers the active ingredient of opium by dissolving it in acid then neutralizing it with ammonia. The result: alkaloids -Principium somniferum or morphine.
1816
John Jacob Astor of New York City joins the opium smuggling trade. His American Fur Company purchases Turkish opium then ships to Canton. Astor later leaves the China opium trade and sells solely to England.
1839
Lin Tse-Hsu, imperial Chinese commissioner in charge of suppressing the opium traffic, orders all foreign traders to surrender their opium. In response, the British send expeditionary warships to the coast of China, beginning The First Opium War.

1843
Dr. Alexander Wood of Edinburgh administers morphine with a syringe. He finds the effects of morphine on his patients instantaneous and three times more potent.
1856
The British and French at war with China in the Second Opium War. China is forced to pay another indemnity. The importation of opium is legalized.
1874
English researcher, C.R. Wright first synthesizes heroin, or diacetylmorphine, by boiling morphine over a stove.

1895
Heinrich Dreser working for the Bayer Company finds that diluting morphine with acetyls produces a drug without the common morphine side effects. Bayer begins production of diacetylmorphine and coins the name "heroin." Heroin would not be introduced commercially for another three years.
Early 1900s
The philanthropic Saint James Society in the U.S. mounts a campaign to supply free samples of heroin through the mail to morphine addicts who are trying give up their habits.
1905
U.S. Congress bans opium.
Dec. 17, 1914
The passage of Harrison Narcotics Act to curb drug (especially cocaine but also heroin) abuse and addiction. It requires doctors, pharmacists and others who prescribed narcotics to register and pay a tax.

William Stewart HalsteadThe "father of American surgery" took morphine for the last thirty years of his extremely successful life. From 1889, William Stewart Halsted was first chief of the Department of Surgery at Johns Hopkins Hospital. In 1892 he was promoted to Professor of Surgery. Halsted's drug habit was revealed in William Osler's posthumously published The Inner History of Johns Hopkins Hospital. Few of Halsted's colleagues had any idea that their brilliant mentor was addicted to morphine. Halsted had ready access to inexpensive, high-grade morphine. So he did not encounter some of the problems common to users of street narcotics in prohibitionist society.

1964
Methadone maintenance began as a research project at the Rockefeller University in 1964, under the joint direction of Dr. Vincent P. Dole and Dr. Marie E. Nyswander.
1970
Comprehensive Drug Abuse Prevention and Control Act of 1970 regulates manufacture, importation, possession, use and distribution of certain substances. Created the five Schedules of controlled substances.
2000
The Drug Addiction Treatment Act permits physicians who meet certain qualifications to treat opioid addiction with Schedule III, IV and V narcotic medications that have been specifically approved by the Food and Drug Administration for that indication.

Prior Opioid Addiction Epidemics
1. Late 1800s: MorphineMainly middle classFemale > Male
2. Early 1900s: Heroin (pharmaceutical grade)First generation Italians, Jews, IrishMale > Female
3. 1950s-1970s- Heroin (illicit)African American/Latinos Male > Female
“God's Own Medicine”Sir William Osler

Morphine, 9-14%, opiate analgesic , named after Morpheus, the Greek God of dreams.
Codeine, 0.5%, opiate analgesic.
Thebaine, 1.5-0.3%. Important intermediate for the synthesis of semisynthetic opioids e.g. Buprenorphine.
Papaverine 1%, smooth muscle relaxant.
(Poppy Seeds) UDS--Opiate, Morphine, Codeine.
Opium Alkaloids

OpioidsMorphine
Codeine
Thebaine
Diacetylmorphine (Heroin)
Hydrocodone (Vicodin)
Oxycodone (Oxycontin)
Oxymorphone (Opana)
Hydromorphone (Dilaudid)
Naturally occurring opiates or opioids
Semi-synthetic opioids

Metabolism Of Opioids

The Mesolimbic Reward Pathway

The Reward Pathway

Why Do People Like Opioids
Extremely powerful psychotherapeutic effects which are likely much stronger than the pain relieving effects.
Relieve the emotional distress of pain.
Excellent at relieving anxiety and treating depression for a limited time.
Treatment of choice for short-term, end of life situations.

Current Preferences of Drug SeekersShort acting narcotics: oxycodone, hydrocodone
Used fentanyl patches; 28-84% of drug remains in used patches
Tramadol alone or in combination
Sustained release drugs
Heroin increased availability

US Consumption of Global Supply of Opioids:2010
55% of all morphine
56% of all hydromorphone
80% of all oxycodone
99% of all hydrocodone
Americans represent 5.2% of the earth’s population(International Narcotics Control Board 2011 Report)
111 Tons Dispensed in 2010!!!
69 tons of pure oxycodone
42 tons of pure hydrocodone
(NSDUH, 2011 reported in CDC Vital Signs, January 2012)

Alabama Consumption of Opioids
#1 prescribed drug in Alabama 2012 Hydrocodone/acetaminophen
(ProPublica Report, 2013)

WHAT HAPPENED
A Drug Looking For a Disease

The Eye of the Perfect Storm…
The use of opioids for chronic non cancer pain (CNCP)

The Fifth Vital Sign

Industry-Funded Organizations Campaignedfor Greater Use of Opioids
Pain Patient Groups
Professional Societies
The Joint Commission
The Federation of State Medical Boards

How the Industry Frames the Problem
Source: Slide presented by Lynn R. Webster MD at FDA meeting on hydrocodone up scheduling, January 25th, 2013.

Opioid Manufacturers Continue to Advertiseas Safe and Effective for Chronic Pain
How Many Americans Have Chronic Pain
“moderate to severe chronic pain that limits activities and diminishes quality of life”
25 million Americans
(Annals of Internal Medicine. Position Paper.2015;162:295-300)

Opioid addiction is rare in pain patients.
Physicians are needlessly allowing patients to suffer
because of “opiophobia.”
Opioids are safe and effective for chronic pain.
Opioid therapy can be easily discontinued.
Industry Funded Education Emphasizes:

Industry Marketing
Purdue “aggressively” promoted the use of opioidsfor use in the “non-malignant pain market.”
Targeted primary care.
“Risk of addiction much less than 1%.”
1998 training video sent to thousands of physicians.
(OxyContin Marketing Plan, 1999; Purdue Pharma, Stamford, CN, 1999)

Industry Marketing
Pseudoaddiction: Describes patients whomanifest aberrant, drug-seeking behavior.
“Result of untreated pain, not addiction.”
Recommended treatment: dose escalation.
Problem: how to differentiate from addiction orhyperalgesia?

Industry Maxim
Opioids are safe and effective for chronic pain.
Opioid addiction is rare in pain patients.
Opioid therapy can be easily discontinued.
Opiophobia: causes patients to needlessly suffer.

Introduction of OxyContin: 1996
Active ingredient: oxycodone
Manufactured by Purdue Pharma
$44 million in sales in 1996
(OxyContin Marketing Plan, 1999)

Dollars Spent Marketing OxyContin 1996 - 2001
› Source: United States General Accounting Office: Dec. 2003, “OxyContin Abuse and Diversion and Efforts to Address the Problem.”

OxyContin Sales 2010
$3.1 billion in sales in 2010
Over $17 billion in sales 2000-2010
(IMS Health, National
Prescription Audit
December 2010)
Purdue Pharma Pays $634.5 Million
US Senate investigation resulted in guilty plea on
May 10, 2007.
Misled regulators, doctors and patients about the
enormous addiction and abuse potential of OxyContin.

Opioid Prescriptions Dispensed per Year(Oxycodone and Hydrocodone)

Opioid Prescriptions Dispensed by RetailPharmacies United States, 1991 - 2011
76 78 8086
9196
100109
120
131139
144151
158
169
180
192201 202
210219
0
50
100
150
200
250
1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Nu
mb
er o
f Pre
scri
pti
on
s (i
n m
illio
ns)
Year

WHAT IS IT LIKE NOW
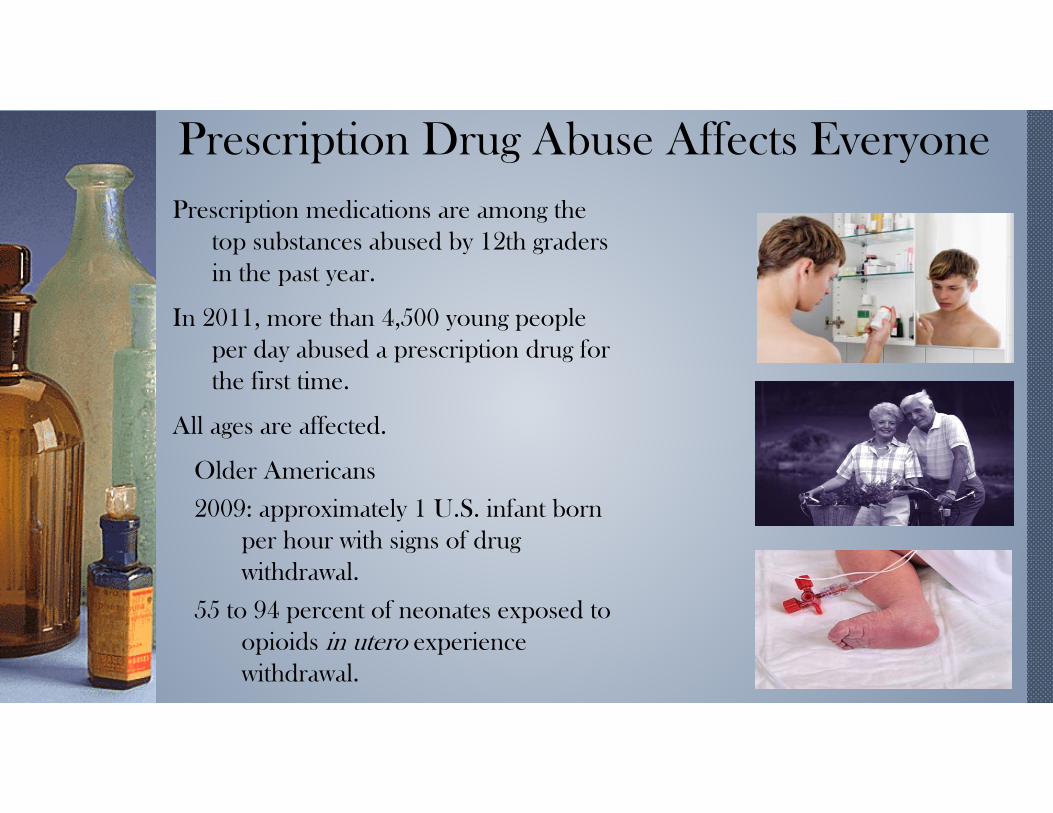
Prescription Drug Abuse Affects Everyone Prescription medications are among the
top substances abused by 12th graders in the past year.
In 2011, more than 4,500 young people per day abused a prescription drug for the first time.
All ages are affected.
Older Americans
2009: approximately 1 U.S. infant born per hour with signs of drug withdrawal.
55 to 94 percent of neonates exposed to opioids in utero experience withdrawal.

People taking high daily doses of opioids. People who “doctor shop.”People using multiple substances like opioids,benzodiazepines, other CNS depressants, illicit drugs.Low-income people and those living in rural areas.Medicaid populations.People with substance abuse or other mental healthissues.
High Risk Populations
White AG, Birnbaum HG, Schiller M, Tang J, Katz NP. Analytic models to identify patients at risk for prescription opioid abuse. Am J Managed Care 2009;15(12):897-906. Hall AJ, Logan JE, Toblin RL, Kaplan JA, Kraner JC, Bixler D, et al. Patterns of abuse among unintentional pharmaceutical overdose fatalities. JAMA 2008;300(22):2613-20. Paulozzi LJ, Logan JE, Hall AJ, et al. A comparison of drug overdose deaths involving methadone and other opioid analgesics in West Virginia. Addiction 2009;104(9):1541-8. Dunn KM, Saunders KW, Rutter CM, Banta-Green CJ, Merrill JO, Sullivan MD, et al. Opioid prescriptions for chronic pain and overdose: a cohort study. Ann Intern Med2010;152(2):85-92. Bohnert AS, Valenstein M, Bair MJ, Ganoczy D, McCarthy JF, Ilgen MA, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA2011;305(13):1315-1321.

Pain Patients
“DrugAbusers”
63% admitted to using opioids forpurposes other than pain
35% met DSM V criteria for addiction
.
This is a false dichotomy as aberrant druguse behaviors are common in pain patients
92% of opioid OD decedents were prescribed opioids for chronic pain.

Toxicology Results in Chronic PainPatients on Opioid Therapy

Emergency Department Visits Related toMisuse or Abuse United States, 2004-2010
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
1,600,000
2004 2005 2006 2007 2008 2009 2010
Nu
mb
er o
f ED
Vis
its
Year
Illicit Drugs Pharmaceuticals Opioid Pain Relievers Benzodiazepines

Primary Substance of Abuse at TreatmentAdmission – United States, 2000-2010
0
2
4
6
8
10
12
14
16
18
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Ad
mis
sio
ns
per
10
,00
0 P
op
ula
tio
n
Year
Alcohol only Alcohol w/secondary drug Heroin
Other opiates Cocaine Marijuana/hashish
Stimulants Other drugs

Opiate-Related Admissions to SUD Treatment(Rates per 100,000 population >12; non-heroin)
Rates for opiates were 400 % higher in 2010 than in 2000.
Rates increased in every year from 2000-2010.
TEDS 2012
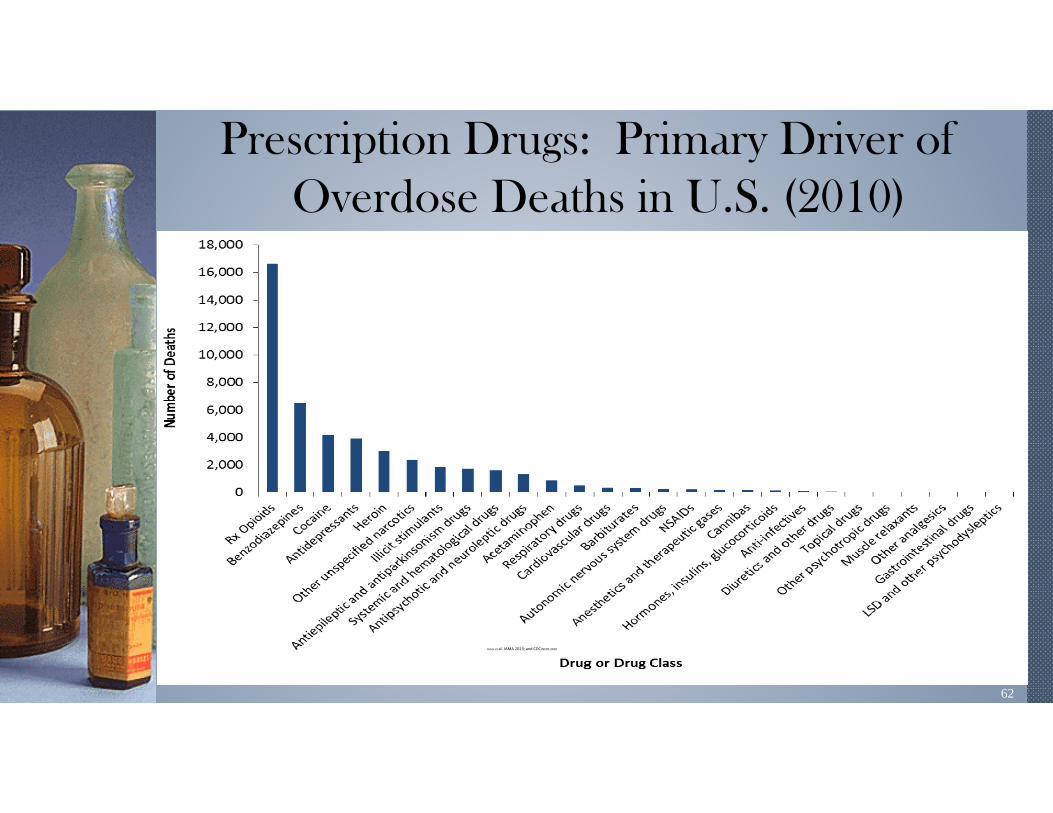
62
Prescription Drugs: Primary Driver ofOverdose Deaths in U.S. (2010)
Jones et al. JAMA 2013; and CDC/NCHS 2010.

Drug Overdose Deaths by Major DrugUnited States, 1999-2010
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Nu
mb
er o
f Dea
ths
Year
Opioids Heroin Cocaine Benzodiazepines
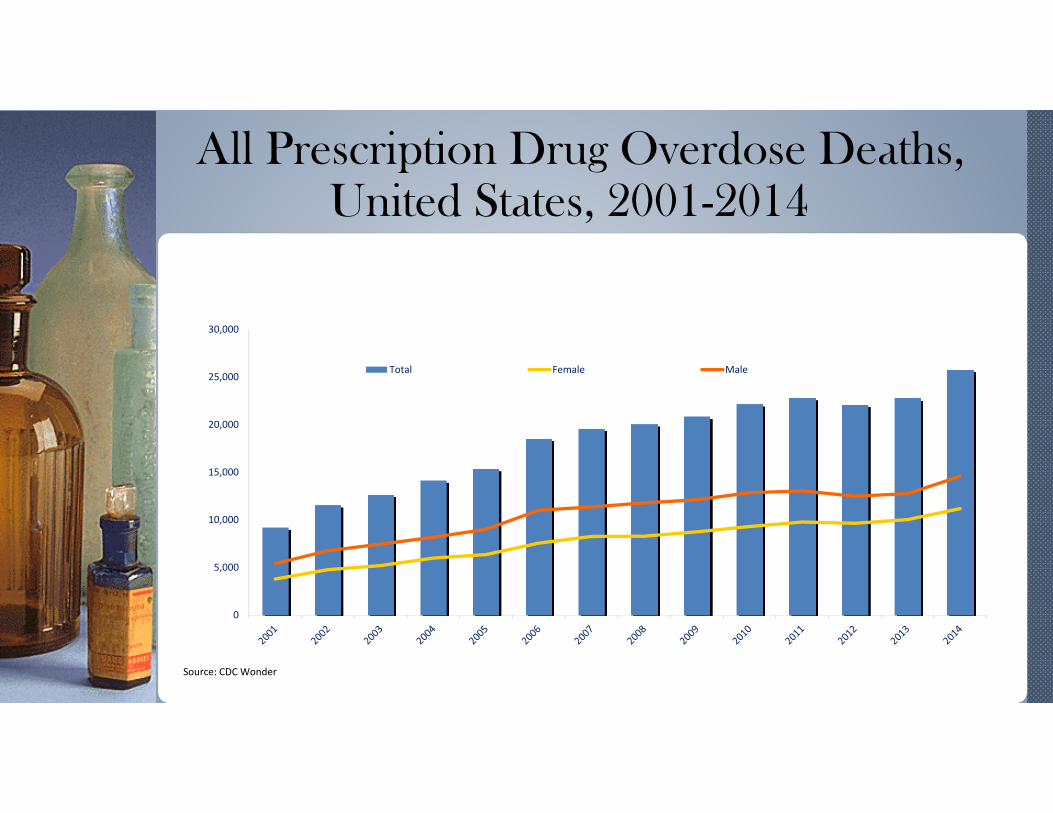
All Prescription Drug Overdose Deaths,United States, 2001-2014
0
5,000
10,000
15,000
20,000
25,000
30,000
Total Female Male
Source: CDC Wonder
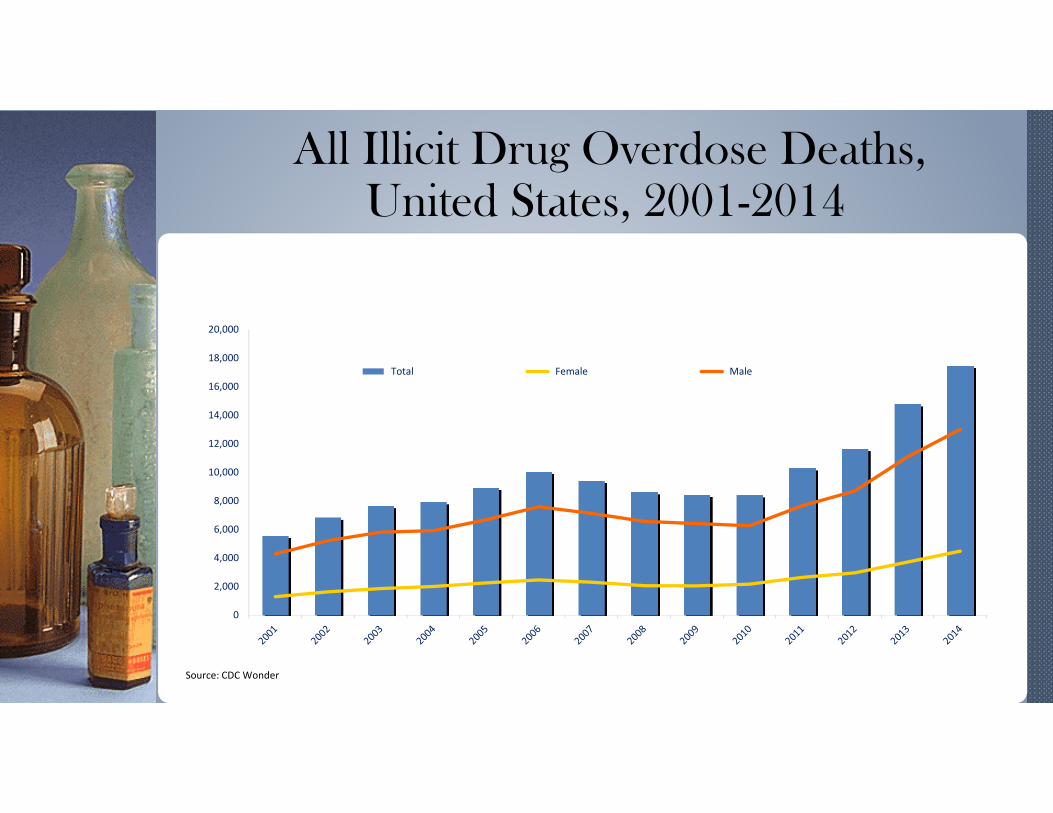
All Illicit Drug Overdose Deaths, United States, 2001-2014
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000
Total Female Male
Source: CDC Wonder

Cocaine Overdose Deaths, United States, 2001-2014
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
Total Female Male

Benzodiazepine Overdose Deaths, United States, 2001-2014
0
1,000
2,000
3,000
4,000
5,000
6,000
7,000
8,000
9,000 Total Female Male

Prescription Opioid Overdose Deaths,United States, 2001-2014
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
20,000 Total Female Male
Source: CDC Wonder

Drug Overdose Deaths Involving Opioids, byType of Opioid, United States, 2000-2014

Opioid Overdose Death Rates by AgeGroup United States 1999-2011

Rates of Opioid Overdose Death Rates, Sales, AndTreatment Admissions, United States, 1999-2010
0
1
2
3
4
5
6
7
8
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Rat
e
Year
Opioid Sales KG/10,000 Opioid Deaths/100,000 Opioid Treatment Admissions/10,000

Unintentional Overdose Deaths Involving Opioid Analgesics Parallel Per Capita Sales of Opioid
Analgesics in Morphine Equivalents by Year, U.S1997-2007
0100200300400500600700800
0
2000
4000
6000
8000
10000
12000
14000
'97 '98 '99 '00 '01 '02 '03 '04 '05 '06 '07
Source: National Vital Statistics System, multiple cause of death dataset, and DEA ARCOS
* 2007 opioid sales figure is preliminary.
Number of Deaths
Opioid sales (mg/person)

73
Motor Vehicle Traffic, Poisoning, and DrugPoisoning (Overdose) Death Rates
United States, 1980–2010
NCHS Data Brief, December, 2011. Updated with 2009 and 2010 mortality data.
0
5
10
15
20
25
1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010
Dea
ths
per
10
0,0
00
po
pu
lati
on
Year
Motor Vehicle Traffic Poisoning Drug Poisoning (Overdose)

Morbidity and Mortality with PrescriptionPain Medication Abuse
2004-2011: Increases in Emergency Department visits related to opioid analgesic misuse:
Men: 159% Women: 146%
2010: Deaths related to opioid analgesic use: 16,651 (313% increase over past decade); most deaths involved opioids + other drugs/alcohol
For every death, there were:o 11 treatment admissionso 33 Emergency department visitso 880 non-medical users
CDC, 2013, SAMHSA TEDS, 2001-11, SAMHSA/DAWN, 2011

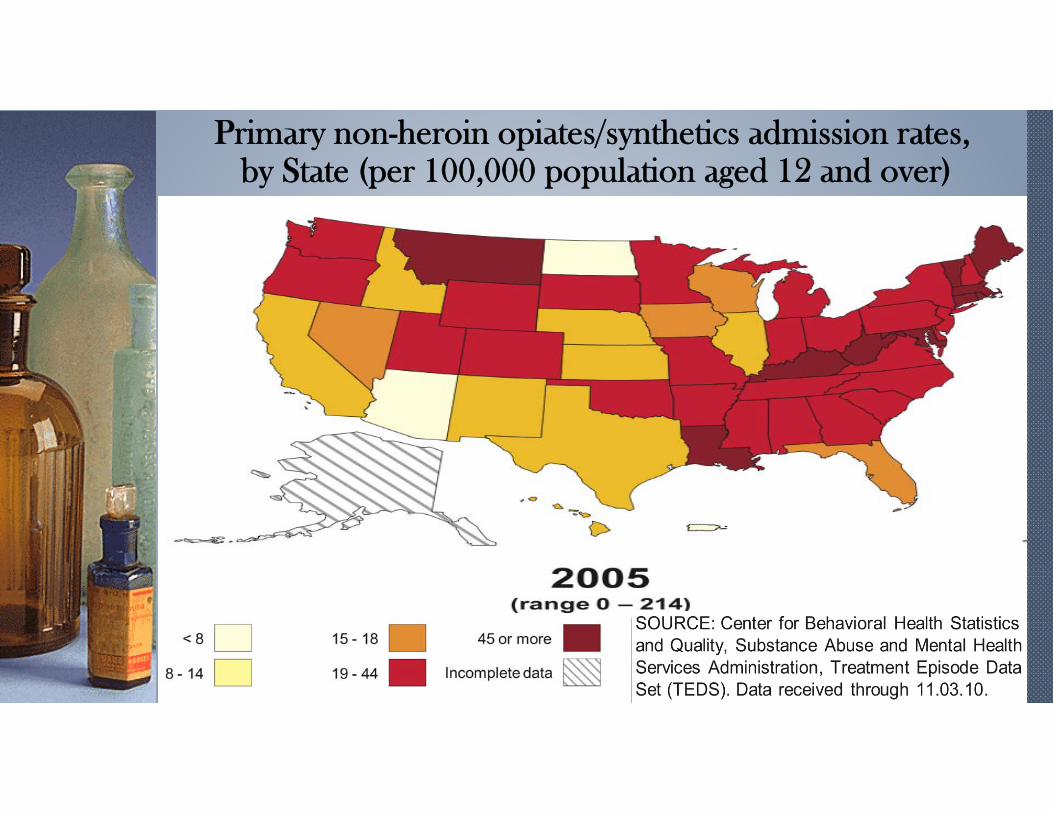
Primary non-heroin opiates/synthetics admission rates, by State (per 100,000 population aged 12 and over)

Primary non-heroin opiates/synthetics admission rates,by State (per 100,000 population aged 12 and over)

Primary non-heroin opiates/synthetics admission rates, by State (per 100,000 population aged 12 and over)
Primary non-heroin opiates/synthetics admission rates, by State (per 100,000 population aged 12 and over)

Primary non-heroin opiates/synthetics admission rates, by State (per 100,000 population aged 12 and over)

Primary non-heroin opiates/synthetics admission rates, by State (per 100,000 population aged 12 and over)

Number of Prescriptions for Opioids Per Person, United States, 2012

Unintentional Drug Overdose DeathsUnited States,1970-2007

Unintentional Drug Overdose DeathsUnited States,1970-2007

Unintentional Drug Overdose DeathsUnited States, 1970-2007

Unintentional Drug Overdose DeathsUnited States,1970-2007

Unintentional Drug Overdose DeathsUnited States,1970-2007



Heroin Overdose Deaths United States 2001-2014
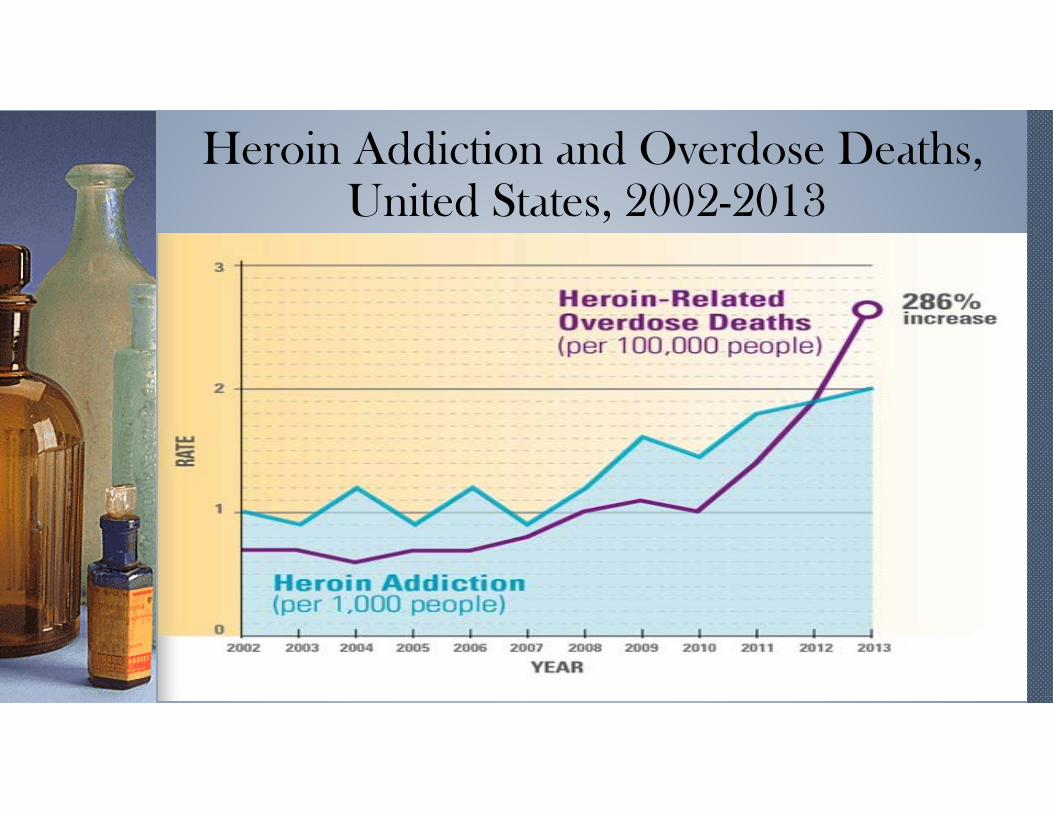
Heroin Addiction and Overdose Deaths,United States, 2002-2013

Rate of Past Year Heroin Use Increasing 2003: 314,000 users
2012: 669,000 (80% increase in 5 years)
2013: 681,000
Trending upward as prescription drugs become less available.
75% of heroin users report previous abuse of opioid pain medication.

Conclusion and Relevance: Our data show that thedemographic composition of heroin users enteringtreatment has shifted over the last 50 years such thatheroin use has changed from an inner-city, minority-centered problem to one that has a more widespreadgeographical distribution, involving primarily white menand women in their late 20s living outside of large urbanareas. JAMA Psych 5/14v

Opioids for CNCP: Quality of Evidence
Patient Selection and Risk Stratification: low quality.
Initiation and titration of chronic opioid therapy: low quality.
Use in high risk patients: low quality.
ALL are based on low quality evidence.
(2009 American Pain Society Guidelines)
Opioids for CNCP: Quality of Evidence
High dose therapy(≥120 morphine equivalents/day):
low quality.
Driving and work safety: low quality.
Treatment of breakthrough pain: low quality.
ALL are based on low quality evidence.
(2009 American Pain Society Guidelines)

Opioids for CNCP: Quality of Evidence
No prospective study has clearly demonstrated long-term safety or long-term efficacy, in terms of functional improvement.
No prospective study has clearly demonstrated long-term analgesia.
Long-term benefits for chronic pain have not been established.
(2009 American Pain Society Guidelines)

Efficacy of Opioids for Dental Pain AfterWisdom Tooth Extraction?
2013 quantitative systematic review in the Journal of the American Dental Association.
“325 mg of acetaminophen (APAP) taken with 200 mg of ibuprofen provides better pain relief than oral opioids.”
(National Safety Council WHITE PAPER, 2014)

Opioids for Treatment of Back Pain?
2013 journal article in Spine.
Patients “initially” treated with opioids (for lumbar disc herniation) had a higher rate of surgery and a greater chance of being on opioids four years later but no significant change in overall outcome.
(National Safety Council WHITE PAPER, 2014)

Long Term (>16wks.) COT for CNCP“..No high quality evidence on the efficacy of COT
for CNCP.” no RCT lasting >3mos
“Until 2003, opioid addiction associated with the treatment of CNCP was clearly a neglected topic of publication.”
Long-term Opioid Treatment of Chronic Nonmalignant Pain: Unproven Efficacy and Neglected Safety. Kissin, Igor Journal of Pain Research, 2013:6 513-529

Has Pain Gotten Better
“Americans suffered as much disability from back pain in 2010 as they did in 1990 before the escalation in the prescribing of opioids.” (Murray, 2013)
A 2008 JAMA study found that:
“…from 1997 to 2005, there was no improvement in self-assessed health status, functional disability, work limitations, or social functioning among respondents with spine problems.” (Martin et al., 2008, p. 661)

“I think that after 20 years of a failed experiment that there are not many people supporting this except for the die-hards and the pharmaceutical industry.”
Jane C. Ballantyne, MD FRCAProfessor, Univ. of Washington
Source: New York Times, April 9, 2012. “Tightening the Lid on Pain Prescriptions.”


New England Journal of Medicine 1980Jan10;302(2):123.

R & D Costs for New Drugs
Why are prescription medications so expensive???
“Drug companies spend 19 times more on marketing than Research & Development.”
(BMJ 2012; 345:e4348)

Are Drugs Profitable?

2012 US Senate Investigation May 8, 2012
“allegations of a network of national organizations and researchers, (including physicians, pain societies and regulatory agencies) with financial connections to the makers of narcotic painkillers.
…helped create a body of dubious information favoring opioids “that can be found in prescribing guidelines, patient literature, position statements, books and doctor education courses.”

Citizens Petition to FDA: July 2012 1.“To exercise its regulatory responsibility” Strike the term "moderate" from the indication for non-cancer pain.
2. Add a maximum daily dose, equivalent to 100 milligrams of morphine for non-cancer pain.
3. Add a maximum duration of 90-days for continuous (daily) use for non-cancer pain.

FDA ResponseSeptember 10, 2013
“Management of pain severe enough to require daily, around-the-clock, long-term opioid treatment and for which alternative treatment options are inadequate.”
ER/LA Opioids no longer indicated for moderate pain.
Warnings about Neonatal Abstinence Syndrome.

FDA ResponseOctober 24, 2013
FDA to recommend to DEA to reschedule hydrocodone from schedule III to schedule II.
“This determination comes after a thorough and careful analysis of extensive scientific literature, review of hundreds of public comments on the issue, and several public meetings…”
FDA Response:
October 25, 2013
Approves Zohydro ER
Pure hydrocodone in capsule form, with no abuse deterrent.
FDA ignores Advisory Committee recommendation against approval December 7, 2012 which had voted 11-2 against approval.

FDA Approves Zyhydro ER Bob Rappaport, MD director of the FDA's Division of Anesthesia, Analgesia, and Addiction Products:
"Many patients in the U.S. suffer from untreated or poorly treated chronic pain. Further limiting access to potential treatments is not the answer when new treatments are critically needed.”
"I firmly believe that the benefits of this product outweigh its risks."

Latest Evidence… 2014 AmericanAcademy of Neurology Position Paper
Opioids for chronic, noncancer pain
“No substantial evidence for maintenance of pain relief over longer periods of time, or significant evidence for improved physical function.”
(Franklin, 2014)

Latest Evidence… 2014 AmericanAcademy of Neurology Position Paper
“The risks for chronic opioid therapy for some chronic conditions such as headache, fibromyalgia, and chronic low back pain likely outweigh the benefits.”
(Franklin, 2014)

US Opioid Epidemic Fueled by Prescribing Practices
The United States is facing the worst "man-made epidemic"of opioid abuse in the history of modern medicine, and it isthe direct result of poor research and outdated teachingpractices, according to a leading pain expert.
The most important step toward reversing the epidemic ofprescription opioid abuse is to stop prescribing opioids forthe wrong indications.2015, Gary Franklin, MD, MPH, vice president of Physicians forResponsible Opioid Prescribing

“Reality is a crutch for people who can't handle drugs"
George Bernard Shaw(1856 - 1950)

I'll die young, but it's like kissing God"
Lenny Bruce

POST SCRIPT

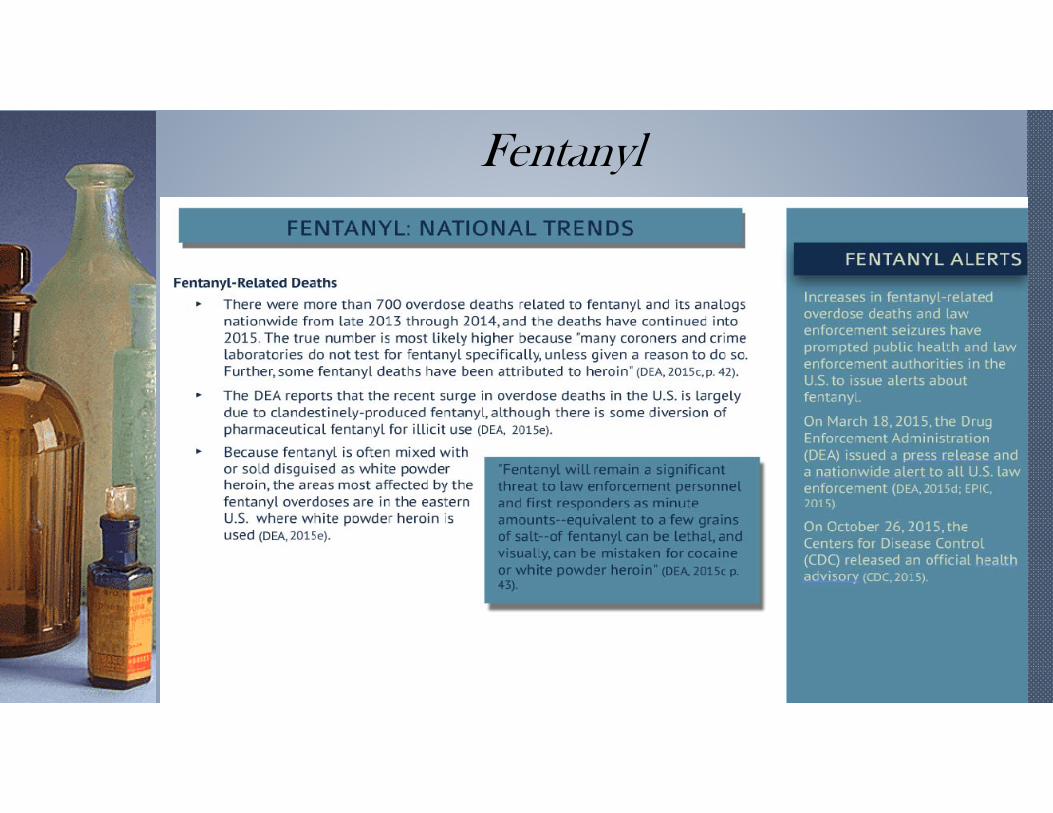
Fentanyl

Kratom› One of the most popular ways to
take the herbal supplement Kratom in social settings is in shots and in drinks. In ancient Southeast Asian cultures people just put the raw leaves in their mouths and chewed them all day long. In today’s world connoisseurs of the MitragynaSpeciosa tree have come up with a more enjoyable and tastier method for taking in the herbal medicine. Kratom drinks and shots are easy to use and offer all the same benefits of other forms of Kratomproducts. Click here to buy Kratomonline.

More than 90% of people who overdosed onprescription painkillers can still get refills, study says.

Physician Convicted of MurderDoctor convicted of murder after three patients overdosed on 'crazy and outrageous' amount of painkillers she prescribed
Dr. Hsiu-Ying 'Lisa' Tseng was convicted of murder after three of her patients overdosed on painkillers she prescribed
The second-degree murder convictions of Dr Tseng were the first against a U.S. doctor for recklessly prescribing drugs
A dozen of Tseng's patients died, though prosecutors only brought three murder charges
Tseng barely kept any records on the three men until she was contacted by the Medical Board of California
Tseng also ignored pleas from family members of patients who demanded she stop prescribing drugs to them
By ASSOCIATED PRESS and DAILY MAIL ONLINE REPORTER
PUBLISHED: 21:13 EST, 30 October 2015 | UPDATED: 18:30 EST, 31 October 2015

'Pill Mill' doctor pleads guilty to moneylaundering and drug distribution
MONTGOMERY, AL (WSFA) -A physician in Montgomery has pleaded guilty to conspiring to distribute oxycodone and money laundering, according to George L. Beck Jr., the United States Attorney for the Middle District of Alabama.According to Attorney Beck, 48-year-old Francisco Huidor-Figureoa pled guilty to one count of conspiring to distribute oxycodone and one count of conspiring to commit money laundering. During the plea hearing, Dr. Huidor-Figureoa admitted to working as a doctor at a "pill mill", which is a medical clinic created to sell pills unlawfully, illegally, and for no medical reason.

Dr. Huidor-Figureoa was the sole physicianemployed by the EMED Medical ManagementCorporation, which operated a "pill mill" in Opelikabetween 2012 and 2013. Officials say while workingat the "pill mill", Dr. Huidor-Figureoa soldoxycodone to pill dealers with fraudulentprescriptions when there was no medical purpose.Dr. Huidor-Figureoa also assisted the "pill mill's" twoowners, Erik Torres and Marc Adam of SouthFlorida, in laundering the money generated fromthe prescriptions.

The United States District Attorney's office for theMiddle District of Alabama says Dr. Hudior-figureoa knew that the recipients of these illegal pillsdid not need the medicine and that the recipientsintended to either abuse the pills or sell the pills toothers who would abuse them.Dr. Huidor-Figueroa faces up to 20 years in prisonfor each count. He also faces a maximum fine of$1,000,000 for conspiring to distribute oxycodone.For the money laundering conspiracy count, themaximum fine he could pay is $500,000 or twice thevalue of the property involved in the transaction,whichever is greater.

Case Presentation66 year old male with the following medical diagnoses:
1. Type II insulin dependent diabetes mellitus
2. Hypertensive vascular disease
3. Hyperlipidemia
4. Peripheral arterial disease
5. Suspect coronary artery disease
6. Carotid artery disease
7. Osteoarthritis
8. Chronic alcoholism

9. Diabetic peripheral neuropathy
10. Bilateral total knee arthroplasties
11. Chronic pain syndrome
12. Moderate opioid use disorder
Prescribed hydrocodone in 2006 to 2008 from seven physicians.
September 2008 prescribed Fentanyl 100 ugm every three days for three months.
Patient continued to drink alcohol.

He was seen in follow up by his physician in March and June 2009
Medications:
1. Clonidine o.4 mg HS
2. Cymbalta 60 mg QD
3. Demadex 20 mg QD
4. Glucovance 5/500 mg BID
5. Zestril 20 mg QD
6. Zocor 40 mg QD
7. Levemir insulin 50 units QD
8. Fentanyl patch 100 ugm Q3days

June 8, 2009 the patient was found dead in his home sitting in a chair.
Personal physician called and notified.
Autopsy and complete forensic drug testing ordered by physician.
Family refused and descendent cremated.
June 2011 plaintiff attorney notified physician for complete copy of medical record.
Law suit filed in county court naming pharmaceutical company and physician as defendants in wrongful death claim.

Case kept in Alabama State Court by naming physician to prevent trial in Federal Court
Late 2012 pharmaceutical company settled with plaintiff for $25,000.00
Case against physician summarily dismissed in March 2013
Cost of defending case against physician $150,000.00

Like Minded Docs
We seek to put more heart and soul back into addiction medicine.
We are all passionate in our belief that psychosocial and spiritual interventions are always important and that medication management alone is not adequate.
We also believe that prescribing medication for opioid addiction without providing and/or prescribing other psychosocial and spiritual interventions falls far short of “best practice” for an addiction medicine specialist.
We are believers in the great benefits of 12 step recovery modalities in facilitating long-term recovery.
www.LikeMindedDocs.com



![[PHYSICIANS - November 1, 1993] THE CORPORATE PRACTICE …archive.healthlawyers.org/google/health_law_archive... · ALABAMA Statutes §34-24-51 (prohibiting unlicensed practice of](https://img.pdfslide.us/doc/110x75/5f0847b57e708231d4213a21/physicians-november-1-1993-the-corporate-practice-alabama-statutes-34-24-51.jpg)