Embed Size (px)
Citation preview

AL amyloidosis – ASCT yes or no?Yes, but … rarely, and very rarely upfront
Giovanni Palladini
Amyloidosis Research and Treatment CenterFondazione IRCCS Policlinico San Matteoand Department of Molecular Medicine
University of PaviaPavia, Italy

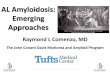
The plasma cell clone is different in multiple myeloma and AL amyloidosis
• AL amyloidosis is caused by a dangerous small PC clone (median BMPC infiltrate 10%)
Merlini & Stone. Blood 2006Paiva, et al. Blood 2016da Silva Filho, et al. Leukemia 2017
Sidiqi, et al. Haematologica 2018Sidana, et al. Leukemia 2018
AL Chromosomal aberration MM
19% gain of 1q21 53%
3% t(4;14) 26%
47% t(11;14) 26%
• Clonal PCs in AL have similar phenotypic and CNA profiles as those in MM, but their GEP is similar to that of normal PCs
• Clonal PCs from AL show almost normal transcriptome• Cyclin D1 is a more prominent driver in AL amyloidosis than in MM• Elevated proliferative index is rare in AL-PC unless there is coexistent MM• Circulating plasma cells are rare in AL amyloidosis unless there is coexistent MM

Dispenzieri, et al. BMT 2013
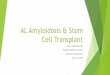
The disease course is different in AL amyloidosis and multiple myeloma


ASCT in AL amyloidosis
Sidiqi, et al. JCO 2018Seldin, et al. Blood 2015
D’Souza, et al. JCO 2015Gertz, et al. BMT 2013

Transplant-related mortality in AL amyloidosis
Time period Pts
(No.)
TRM
Mollee 2004 1996-2001 20 35%
Perfetti 2006 1995-2002 22 14%Kim 2013 2007-2012 24 0%
Landau 2013 2007-2011 40 10%Dispenzieri 2013 1996-2011 454 9%
Sanchorawala 2015 1994-2014 629 7.5%Bochtler 2016 2003-2014 123 <1%
Time period Pts
(No.)
TRM
Moreau 1998 1993-1997 21 43%Gertz 2004 1998-2000 28 14%
Goodman 2006 1994-2004 92 23%Vesole 2006 1995-2001 114 18%Jaccard 2007 2000-2005 50 24%D’Souza 2015 1995-2012 1536 5-20%
Hazenberg 2015 2000-2006 69 4%Rosengren 2016 1994-2009 72 12.5%
Single center studies Multicenter studies

Early mortality can be associated with stem cell harvest
Yeh, et al. Biol BMT 2018
101 patients

Why choosing ASCT as upfront therapy?
• Better response rate?
• Better PFS?
• Better OS?

Regimen HR (CR) OR Common SAEs100-day
mortalityPFS / OS (y)
MDex
vs.
ASCT
68% (32%)
67% (41%)
39%
45%
Overall 16%
Hemodialysis 22%
2%
24%
2.7 / 4.7
2.7 / 1.8
Jaccard et al, N Engl J Med 2007
MDex vs. ASCT a randomized trial

Courtesy of Prof. Arnaud Jaccard
MDex vs. ASCT 10 years later
Landmark analysis, April 2016
MDex
ASCT
MDex
ASCT
OSPFS
ASCT
MDex

sept 2015

Regimen Time period Patients number and staging HR OR Survival
MDexPalladini 2014
2004-2009119 intermediate-risk (IIIa 13%)
140 high-risk (IIIa 24%, IIIb 36%)
76%
(CR 31%, VGPR 29%)
51%
(CR 17%, VGPR 28%)
H 37%, K 24%
H 20%, K 17%
median 88 months
median 20 months
LMDexHegenbart 2017
2009-2012 50 (IIIa 24%, IIIb 12%)68%
(CR 18%, VGPR 32%)H 22%, K 22% median 68 months
BMDexPalladini 2014
2007-201223 intermediate-risk
64 high-risk (IIIb 30%)
74%
(CR 48%, VGPR 17%)
67%
(CR 41%, VGPR 11%)
H 16%, K 16% 66% at 12 months
BMDexKastritis in
preparation
2011-2016 53 stage I-IIIa81%
(CR 23%, VGPR 42%)H 38%, K 44% 70% @ 5 years
CTDVenner 2014
2008-2012 69 (IIIa 36%, IIIb 22%)80%
(CR 25%, VGPR 20%)H 15%, K 39% 67% at 12 months
CLDCibeira 2015
2010-2012 28 (III 50%)46%
(CR 25%, VGPR 18%)H 26%, K 43% 64% at 12 months
CyBorDPalladini 2015
2006-2013158 low/intermediate-risk (IIIa 39%)
43 high-risk (IIIb 100%)
68%
(CR 23%, VGPR 26%)
42%
(CR 14%, VGPR 9%)
H 22%, K25%
H 4%
Stage I, 100% at 3 y
Stage II, 52% at 3 y
Stage IIIa, 55% at 3 y
Stage IIIb, 19% at 3 y
Non-transplant upfront therapy in AL amyloidosis

The amyloidogenic LC is an intrinsic stressor for PC
parental line: non-Ig-producing NS0(mouse plasmocytoma)
Oliva, et al. Blood 2017

CyBorD in AL amyloidosis: a retrospective study of 230 patients
Response category Stage I
(30 patients)
Stage II
(67 patients)
Stage IIIa
(61 patients)
Stage IIIb
(43 patients)
Overall hem. 77% 64% 69% 42%*
CR 33% 18% 23% 14%
VGPR 23% 27% 26% 9%
PR 20% 19% 20% 19%
Cardiac - 29% 17% 4%*
*P<0.05 compared to stages (I), II, and IIIa Palladini, et al. Blood 2015
Early stage patients (stage I) without cardiac involvement, benefit most from CyBorD
CyBorD does not overcome the poor prognosis of patients with very advanced cardiac involvement (stage III with NT-proBNP >8500 ng/L)

Why do so many paper argue for superiority of ASCT?

Why do so many paper argue for superiority of ASCT?
ASCT CT
BNP (ng/L) 192 501

59 pts
41 pts
Low risk : interventricular septal thickness ≤15 mm, cardiac ejection fraction > 55 %, serum creatinine ≤ 2.0 mg/dL, bilirubin ≤ 2.0 mg/dL)
0
.2
.4
.6
.8
1
Sur
viva
l
0 20 40 60 80 100 120
Months
MDex vs. ASCT trial according to disease severity
Courtesy of Prof. Arnaud Jaccard

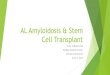
Does ASCT grant better long term survival than non-transplant chemotherapy ?
Survival of 193 patients with AL amyloidosis eligible for ASCT treated with non-transplant
chemotherapy
Median not reached62% alive at 8 years
Median 7.7 years
Survival of 629 patients with AL amyloidosis undergoing ASCT at BU Amyloid Program
Sanchiorawala, et al. Blood 2015 New powerful treatments are coming

in conclusion …
• There is no convincing evidence that ASCT should be preferred over other frontline regimens
• ASCT should be considered as a possible step in the sequential treatment approach of eligible patients

“Induction” and “adjuvant” therapy with ASCT in AL amyloidosisPatients with BMPC>10% benefit from
induction therapy
Turn off the Tap! The Need for Induction Therapy for AL
Amyloidosis Before Transplant
Deferred autologous stem cell transplantation after bortezomib-based therapy
• 22 transplant ineligible patients received bortezomib-based therapy upfront
• All responded, became transplant eligible, and received ASCT for hematologic progression or consolidation
CR almost 60% with “adjuvant” BDex
Hwa, et al. Am J Hematol 2016Manwani, et al. Blood Cancer J 2018Afrough, et al. Biol BMT 2018
Mikhael. Biol BMT 2018Landau, et al. Leukemia 2017

in conclusion …
• There is no convincing evidence that ASCT should be preferred over other frontline regimens
• ASCT should be considered as a possible step in the sequential treatment approach of eligible patients
• So, when should ASCT be recommended?1) Eligible patients with suboptimal response to upfront non-transplant chemotherapy2) Eligible patients with contraindications to bortezomib-based chemotherapy3) Patients with concomitant overt multiple myeloma

Acknowledgements
Giampaolo MerliniLaura Obici Andrea Foli Paolo Milani Mario NuvoloneFrancesca Lavatelli Roberta Mussinelli
Marco BassetStefano PerliniGiuseppina PalladiniMargherita MassaPaola Rognoni Tasaki MasayoshiGiovanni Ferraro
Pasquale Cascino Margherita BozzolaClaudia Cagnoni Simona CasariniJessica RipepiAlice NevoneAnna Carnevale Baraglia
Caludia SforziniElona Luka Eleonora Di BuduoAlberto BoveraArianna Pasi