Embed Size (px)
Citation preview

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 1/12
Review and Special Articles
The Rising Prevalence of Severe Poverty in America A Growing Threat to Public HealthSteven H. Woolf, MD, MPH, Robert E. Johnson, PhD, H. Jack Geiger, MD, MS
Background: The U.S. poverty rate has increased since 2000, but the depth of poverty experienced by Americans has been inadequately studied. Of particular concern is whether severe poverty is increasing, a trend that would carry important public health implications.
Methods: Income-to-poverty (I/P) ratios and income deficits/surpluses were examined for the1990–2004 period. The severely poor, moderately poor, and near-poor were classified asthose with I/P ratios of less than 0.5, 0.5 to 1.0, or 1.0 to 2.0, respectively. Incomedeficits/surpluses were classified relative to the poverty threshold as Tier I (deficit $8000or more), Tier II (deficit or surplus less than $8000), or Tier III (surplus more than $8000).Odds ratios for severe poverty and Tier I were also calculated.
Results: Severe poverty increased between 2000 and 2004—those with I/P ratios of less than 0.5grew by 20%, and Tier I grew by 45% to 55%—while the prevalence of higher levels of income diminished. The population in severe poverty was over-represented by children
(odds ratio [OR]ϭ1.69, confidence interval [CI]ϭ1.63–1.75), African Americans(OR ϭ2.84, CIϭ2.74–2.95), and Hispanics (OR ϭ1.64, CIϭ1.58–1.71).
Conclusions: From 2000 to 2004, the prevalence of severe poverty increased sharply while the proportionof Americans in higher income tiers diminished. These trends have broad societalimplications. Likely health consequences include a higher prevalence of chronic illnesses,more frequent and severe disease complications, and increased demands and costs forhealthcare services. Adverse effects on children warrant special concern. The growth in thenumber of Americans living in poverty calls for the re-examination of policies enacted inrecent years to foster economic progress.(Am J Prev Med 2006;xx(x):xxx) © 2006 American Journal of Preventive Medicine
Introduction
Poverty is of great concern to the public healthcommunity because of its influence on healthstatus and access to care.1 The poor account for
a growing proportion of Americans. Although thenation’s poverty rate declined in the 1990s, since 2000the United States Census Bureau (USCB) has reporteda steady rise in the poverty rate, from 11.3% in 2000 to12.7% in 2004.2 Children experienced the sharpest increase; the proportion living in poverty rose by 13.4%, from a rate of 15.7% (11.1 million) in 2000 to17.8% (13.0 million) in 2004.2,3
Other economic trends paint a more positive picture,suggesting that economic growth is bringing greater
affluence to the population. In recent years, the Bushadministration has reported falling unemployment rates and increases in after-tax income, retail, manufac-turing, and overall productivity.4 This good economicnews is tempered by signs of growing income inequal-ity. The Gini index,5 a key measure of inequality, hasincreased by 3.6% from its most recent low of 0.450 in1995 to 0.466 in 2004.2 Over the same time period,increases have also been noted consistently in othermeasures of income inequality, such as the ratio be-tween the highest and lowest quintiles of householdincome, the Theil and Atkinson indexes, and the mean
logarithmic deviation of income.2,5
Although the evidence is clear that more Ameri-cans are poor, how deeply they have sunk intopoverty is less certain. We found no current reportson the topic. Our null hypothesis, supported by reports of low unemployment and higher incomes,
was that most of the poor are concentrated just below the poverty threshold and that a diminishing propor-tion of Americans suffer from severe, abject poverty.The alternative—that the poor are slipping moredeeply into poverty—would have ominous implica-tions for individuals and families and for the vibrancy
From the Departments of Family Medicine (Woolf, Johnson), Epide-miology and Community Health (Woolf), and Biostatistics (John-son), Virginia Commonwealth University, Richmond, Virginia; De-partment of Community Health and Social Medicine (Geiger), City University of New York Medical School, New York, New York
Address correspondence and reprint requests to: Steven H. Woolf,MD, MPH, Department of Family Medicine, Virginia CommonwealthUniversity, 1200 East Broad Street, P.O. Box 980251, MCV Station,Richmond VA 23298-0251. E-mail: [email protected].
The full text of this article is available via AJPM Online at www.ajpm-online.net .
1 Am J Prev Med 2006;xx(x) 0749-3797/06/$–see front matter© 2006 American Journal of Preventive Medicine • Published by Elsevier Inc. doi:10.1016/j.amepre.2006.06.022

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 2/12
of the American community and economy.6,7 Toclarify which is the case, this analysis grouped thepoor into tiers to quantify the depth of poverty in
America and to examine temporal trends over time.
Methods
The analysis examined the 1990–2004 period to put trends
after 2000 into historical context. The study used two mea-sures of the depth of poverty that adjust for inflation and havebeen tracked consistently by the U.S. Census Bureau (USCB):(1) the income-to-poverty ratio (I/P ratio), and (2) theincome deficit/surplus. Both measures are anchored to thepoverty threshold,8 which the USCB updates annually toaccount for changes in the Consumer Price Index.
The income-to-poverty ratio (I/P ratio) is calculated by dividing individual income by the corresponding poverty threshold. The proportion of Americans with an I/P ratio of Ͻ2.0 is reported annually for seven subgroups: ratios of Ͻ0.5,0.50 to Ͻ0.75, 0.75 to Ͻ1.0, 1.0 to Ͻ1.25, 1.25 to Ͻ1.50, 1.50to Ͻ1.75, and 1.75 to 2.0.9 People were classified as severely
poor, moderately poor, or near-poor if their I/P ratios wereϽ0.5, 0.5 to 1.0, or 1.0 to 2.0, respectively. The analysis alsoexamined the proportion of Americans with an I/P ratio of Ͼ2.0, which was reported by subgroup beginning in 2002.
The income deficit/surplus is the absolute difference indollars between household income and the poverty thresh-old. The study examined USCB reports for 1990 through2004,2,10–23 which present income deficit/surplus data for 20categories: those with an income deficit of Ն$8000 below thepoverty threshold, nine strata for income deficits Ͻ$8000,nine strata for income surpluses of Ͻ$8000, and those with anincome surplus of Ն$8000 above the poverty threshold (seeonline data table at www.ajpm-online.net). These data wereaggregated into four poverty tiers: Tier I (deficit of Ն$8000),Tier IIa (deficit Ͻ$8000), Tier IIb (surplusϽ$8000), and TierIII (surplus of Ն$8000). Because the USCB reports incomedeficit/surplus data separately for families and for “unrelatedindividuals” (people who are not members of families), thisstudy uses the same framework for reporting the results.Income deficit/surplus data for unrelated individuals wereincluded only for 1996 and beyond, because the USCBprovides incomplete source data for 1990 through 1995.
The study examined the demographic characteristics of thepoverty tiers for 2004, the most recent year for which data areavailable. Odds ratios and 95% confidence intervals were
calculated to determine which characteristics were associated with significantly greater risk of experiencing severe poverty.To explore temporal trends, odds ratios for 2004 werecompared with those for 2002 and 2003.
Relying on the official poverty threshold to measure theprevalence of poverty can be criticized. Many householdshave difficulty meeting basic expenses at incomes wellabove the poverty threshold.24 The poverty threshold de-rives from the Orshanksy formula,25 devised in the 1960sbased on the assumption that families spend one third of their income on food, a condition that no longer applies.Other criticisms of the poverty threshold are detailedbelow. This study used the poverty threshold for its calcu-
lations because it is the official government measure of
poverty and the only metric that has been tracked consis-tently over the comparison period.
Results
Income-to-Poverty Ratios
Poverty increased in the United States after 2000, but the most dramatic increases occurred among the se-
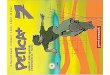
verely poor. Between 2000 and 2004, the proportion of Americans with I/P ratios Ͻ0.5 (an income below 50%of the poverty threshold) increased from 4.5% to 5.4%,a relative increase of 20% (Figure 1, Panel A). Theproportion of Americans in moderate poverty (I/Pratio of 0.5 to 1.0) increased less dramatically, from6.8% to 7.3%, a relative increase of 7.3%. The increasein the near-poor (I/P ratios of 1.0 to 2.0) was modest (an absolute and relative increase of 0.5% and 2.8%,respectively) and erratic (Figure 1, Panel B).
After 2000, the proportion of Americans with thelargest incomes (I/P ratios Ͼ2.0) decreased by 1.9%
(Figure 1, Panel C). In 2002 to 2004, the decline wasconcentrated among those with I/P ratios of 2.0 to 6.0;the proportion of families with I/P ratios Ͼ6.0 re-mained stable.
The size of the middle and upper classes and the risein poverty rates following 2000 represent a reversal intrends observed during the more favorable economicperiod of 1993 to 2000. During that time, the propor-tion of Americans below the poverty threshold declinedby 25%, from 15.1% to 11.3%,2 and the proportion
with the largest incomes (I/P ratios Ͼ2.0) experiencedsteady growth (Figure 1, Panel C). After 2000, the
absolute number of Americans with I/P ratios below 0.5grew by 30% (3.6 million), from 12.1 million people in2000 to 15.6 million in 2004; the number with I/Pratios of 0.5 to 1.0 grew by 12% (2.3 million), from 19.0million in 2000 to 21.3 million in 2004.26,27
Income Deficits and Surpluses
Between 2000 and 2004, the mean income deficit forthe poor grew by 14% among families (from $6820 to$7775) and by 20% among unrelated individuals (from$4388 to $5259), also reflecting an increase in severe
poverty. The only category of Americans to increase insize was that with the greatest income deficit (Tier I,Ն$8000 below the poverty threshold) (Figure 2, Panel
A). The proportion of families in Tier I increased by 45%, from 3.1% in 2000 to 4.5% in 2004, and theproportion of unrelated individuals in Tier I increasedby 55%, from 4.4% to 6.8%. In absolute numbers, TierI grew by 1.2 million families (52%) and 1.3 millionunrelated individuals (63%) between 2000 and 2004.From 1990 to 2004, the proportion of U.S. families inTier I almost doubled (from 2.3% to 4.5% of families).
The proportion of the population in Tiers II and III
decreased after 2000, a trend that began for Tier II
2 American Journal of Preventive Medicine, Volume xx, Number x www.ajpm-online.net

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 3/12
early in the 1990s (Figure 2, Panel B). From 1990 to2004, the proportion of families in Tiers IIa and IIb fellby one third (from 8.4% to 5.7% and from 12.2% to8.1%, respectively). The rate of decline in Tiers IIa andIIb was similar after 1996; these tiers were therefore
treated as a single group (Tier II) in further analyses.
After 2000, the proportion of families in Tier III(income surplus of Ն$8000) began to diminish slightly,from 82.6% to 81.7% (Figure 2, Panel C). The propor-tion of unrelated individuals in Tier III declined from59.5% in 2000 to 57.5% in 2003 and appeared torecover in 2004 (to 58.4%). Although Tier III de-creased in size after 2000, the mean income surplus forTier-III families increased by 9%, from $56,427 to
$61,481 (and by 1% for unrelated individuals).
Demographic Patterns
The population experiencing severe poverty was over-represented by children, African Americans, and His-panics (Tables 1 and 2). As of 2004, the odds of havingan income below 50% of the poverty threshold were69% higher for children aged Ͻ18 years than for adults(aged Ն18), and were doubled for children aged Ͻ5
years (Table 1). Families with children were 4 timesmore likely to have Tier-I incomes than were otherfamilies (Table 2). Older adults (aged Ն65) were lesslikely than younger persons to experience severe pov-erty. Compared with other races, African Americans in2004 were almost three times as likely to have an I/Pratio of Ͻ0.5 (Table 1); African-American household-ers were more than three times as likely to have Tier-Iincomes (Table 2). The odds of having an I/P ratiobelow 0.5 were 64% greater for Hispanics than forothers (Table 1), and Hispanic householders weremore than twice as likely to have incomes in Tier I(Table 2). Whites and Asians were less likely to experi-
ence severe poverty. Data from the 2002–2004 periodsuggest that odds ratios for children and minoritiesdiminished during this period.
Fragmented family units face a heightened risk of severe poverty. Compared to other families, the odds of having a Tier-I income in 2004 were almost seven timeshigher among families led by a female householder
with no spouse (Table 2). Unrelated individuals—people not in families—were twice as likely to have anI/P ratio Ͻ0.5 (Table 1).
Discussion and Conclusions
A rise in poverty rates is important because of theenormous difficulties faced by the poor in meeting themost basic human needs (e.g., food security, clothing,housing, health) and in obtaining the means to escapetheir conditions (e.g., education, jobs, higher earn-ings). This suffering alone is sufficient cause for con-cern among those who advocate social justice, but rising poverty rates are also relevant to those who reject a moral duty to help the poor. The global competitive-ness of the U.S. economy suffers if workers are too poorto obtain an education and modern job skills, the
government loses tax revenue and spends more on
Middle and upper class: > 2.0 times the
poverty threshold
(Panel C)
>2.0
62
64
66
68
70
72
1 9 9 0
1 9 9 1
1 9 9 2
1 9 9 3
1 9 9 4
1 9 9 5
1 9 9 6
1 9 9 7
1 9 9 8
1 9 9 9
2 0 0 0
2 0 0 1
2 0 0 2
2 0 0 3
2 0 0 4
Year
People below (<1.0) poverty threshold
(Panel A)
< 0.5
0.5–1.0
4
5
6
7
8
9
10
The near-poor: 1.0–2.0 times the
poverty threshold
(Panel B)
1.0–2.0
17
18
19
20
21
P r o p o r t i o n o f A m e r i c a n s ( % )
Figure 1. Proportion of Americans below or near the poverty threshold, 1990–2004. Data are derived from U.S. CensusBureau9 and analyzed as described in the text. The poverty threshold is defined by the U.S. Census Bureau based onfamily size (from one person to nine or more people)
cross-classified by presence and number of family membersaged Ͻ18 years (from no children present to eight or morechildren present). Unrelated individuals and two-person fam-ilies are further differentiated by age of reference person(Ͻ65 years and Ն65 years). Poverty thresholds for each yearare available at www.census.gov/hhes/www/poverty/thresh-ld.html.
Month 2006 Am J Prev Med 2006;xx(x) 3

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 4/12
public assistance because of poverty, and communitiesfall victim to urban decay, crime, and unrest.6,7
This study found that the recent increase in poverty rates is explained largely by a dramatic upsurge insevere poverty, refuting our null hypothesis. The rise insevere poverty after 2000 was substantial. In relativeterms, the proportion of Americans with I/P ratios lessthan 0.5 grew by 20%, and Tier I grew by 45% and 55%
among families and unrelated individuals, respectively.In absolute terms, the number of Americans with I/Pratios less than 0.5 grew by 30%, and the number of families and unrelated individuals in Tier I grew by 52% and 63%, respectively.
In contrast, increases in moderate poverty were lessstriking. Indeed, Tier II has been shrinking since theearly 1990s. The fall in the proportion of families andunrelated individuals with incomes within $8000 of thepoverty threshold displayed a similar pattern for thoseabove (Tier IIb) and below (Tier IIa) the poverty threshold (Figure 2, Panel B). The 18 income strata
within Tier II (see Methods) exhibited similar trendsand rates of decline, which were collectively distinct from the temporal patterns observed for Tiers I and III(Figure 2, Panels A and C). The population with anincome deficit of at least $8000 below the poverty threshold therefore appears to be vulnerable to adifferent experience than those with incomes closer tothe poverty threshold. Therefore, analyses that focusonly on the population below the poverty line, mixingTier I with members of Tier II, may lose sight of suchtrends.
The growth in Tier I, set against reductions in Tiers
II and III, suggests that severe poverty may be produc-ing a “sinkhole” effect on income. Just as a sinkholecauses everything above it to collapse downward, fami-lies and individuals in the middle and upper classesappear to be migrating to lower income tiers that bringthem closer to the poverty threshold. Relative to 2000,by 2004 Tiers II and III had experienced net losses of 0.5% and 0.9% of American families, respectively,
whereas Tier I had experienced a net growth of 1.4% of families. The 2.4% absolute increase between 2000 and2004 in the proportion of unrelated individuals in TierI was explained by a 1.3% reduction in Tier II and a
1.1% reduction in Tier III.One would expect this sinkhole effect to be accom-
panied by an overall decrease in median income in the
Tier I: $8000 income deficit
(Panel A)
0
2
4
6
8
Tier I: families Tier I: unrelated individuals
Tier II: < $8000 income deficit/surplus
(Panel B)
0
10
20
30
Tier IIa: families Tier IIa: unrelated individualsTier IIb: families Tier IIb: unrelated individuals
P r o p o r t i o n o f f a m i l i e s a n d i n d i v i d u a l s * ( % )
Tier III: $8000 income surplus
(Panel C)
45
55
65
75
85
1 9 9 0
1 9 9 1
1 9 9 2
1 9 9 3
1 9 9 4
1 9 9 5
1 9 9 6
1 9 9 7
1 9 9 8
1 9 9 9
2 0 0 0
2 0 0 1
2 0 0 2
2 0 0 3
2 0 0 4
Year
Tier III: families Tier III: unrelated individuals
Figure 2. Proportion of families and unrelated individuals inincome deficit/surplus Tiers I, II, and III, 1990 to 2004. Data areaggregated from the table posted online (abstracted from U.S.Census Bureau data2,10–23) and analyzed as described in thetext. Unrelated individuals are persons who are not members of families. The U.S. Census Bureau does not provide completedata for unrelated individuals from before 1996. Tier I, incomedeficit Ն$8000; Tier IIa, income deficit Ͻ$8000; Tier IIb,
income surplus Ͻ$8000; Tier III, income surplus Ն$8000.
4 American Journal of Preventive Medicine, Volume xx, Number x www.ajpm-online.net

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 5/12
United States, which was indeed the case. The USCBreports that U.S. household income, adjusted for infla-tion, declined by 3.6% between 2000 and 2004, from amedian of $46,058 to $44,389.2
Our findings have not, to our knowledge, beenpublished previously. Using the search terms “severepoverty” and “deep poverty,” we searched Social Sci-
ences Citation Index and PubMed from 2001 forwardand found no articles on the topic. A Google searchretrieved information about severe poverty globally but only USCB reports and statements by advocacy organi-
zations provided information that relate to the UnitedStates.
The USCB does announce year-to-year increases inthe poverty rate at annual press briefings, and newsreports have noted the steady rise in rates after 2000—but the media have not emphasized the trend. Between2002 and 2005, the Washington Post and New York Times
ran eight news articles about the census statistics,ranging from 400 to 1410 words in length, but thearticles devoted a median of two sentences to thetemporal increase in the overall poverty rate.28–35
Table 1. Demographic characteristics of U.S. population, by I/P ratio, 2004 (n ϭthousands)
I/P ratio
Odds ratio(95% CI) forsevere poverty a
Severely poor<0.5(n 15,637) (%)
Moderately poor0.5–1.00(n 21,360) (%)
Near poor1.00–2.00(n 53,816) (%)
2.0–6.0(n 144,885) (%)
>6.0(n 54,907)(%)
Age (years)Ͻ5 12 10 8 6 4 1.94 (1.85–2.04)Ͻ
18 36 35 29 24 17 1.69 (1.63–1.75)18–64 58 53 52 64 74 0.83 (0.80–0.86)Ն65 6 12 18 12 9 0.44 (0.42–0.48)
Female 56 56 54 50 48 1.23 (1.19–1.27)Race/ethnicity
Whiteb 65 71 77 82 87 0.43 (0.42–0.45) African Americanb 27 22 16 11 5 2.84 (2.74–2.95) Asianb 3 3 4 4 6 0.81 (0.74–0.88)Hispanic (of any
race/ethnicity)21 27 23 12 5 1.64 (1.58–1.71)
Householder 36 40 40 38 40 0.88 (0.85–0.91)Unrelated individualsc 30 24 22 15 10 2.30 (2.22–2.39)aOdds ratio for having an I/P ratio Ͻ0.5; referent populationϭI/P ratio Ͼ0.5.bIndividuals who reported this race/ethnicity and no other additional category. African Americans classify themselves as “black” in U.S. CensusBureau surveys.cIndividuals who are not in primary families (the householder’s family) or unrelated subfamilies.Source: U.S. Census Bureau.14
CI, confidence interval; I/P, income to poverty.
Table 2. Demographic characteristics of U.S. families,a by income tier, 2004 (n ϭ thousands)
Tier IIncome >$8000 below poverty, threshold(n 3444) (%)
Tier IIIncome $0–$7999below/above poverty threshold (n 10,657)(%)
Tier IIIIncome >$8000 above poverty threshold(n 62,917) (%)
Odds ratio for TierI (95% CI)b
Families with children 81 60 48 4.31 (3.95–4.70)Race/ethnicity of
householder Whitec 64 74 84 0.36 (0.34–0.39) African Americanc 30 19 9 3.54 (3.28–3.82) Asianc 3 3 4 0.69 (0.56–0.84)Hispanic (of any race/
ethnicity)24 24 10 2.35 (2.17–2.55)
Families with femalehouseholder and nospouse
57 38 13 6.76 (6.30–7.25)
aThe U.S. Census Bureau does not publish demographic data for unrelated individuals by income deficit/surplus categories.bOdds ratio for having Tier I income; referent population: Tiers II and III combined.cIndividuals who reported this race and no other additional category. African Americans classify themselves as “black” in US Census Bureau
surveys.
Month 2006 Am J Prev Med 2006;xx(x) 5

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 6/12
The USCB press briefings have largely omitted dis-cussion of severe poverty. The only briefing to com-ment on severe poverty after 2000 occurred on Septem-ber 26, 2003, when 2002 data were released. By that time, the proportion of individuals with I/P ratios lessthan 0.5 had grown from 4.5% in 2000 to 4.8% in 2001and to 4.9% in 2002.9 The USCB spokesman said only this: “The 14.1 million people with incomes less than
half their thresholds represent 4.9% of the population. . . percentages not different from 2001.”36 Nothingfurther was said about severe poverty, and the topic wasomitted entirely from press briefings in 2004 and 2005(although the proportion had risen to 5.3% by 2003and 5.4% in 2004).37,38 The press briefings were re-cently investigated by the U.S. Government Account-ability Office.39
Reflecting what they hear at press briefings, journal-ists covering the census reports have also reported littleabout severe poverty. A New York Times editorial on
August 31, 2004 did say: “[T]he positive news on the
number of people in poverty masks an alarming trend.The number of people in extreme poverty—that is,subsisting on less than half the income defined as thepoverty line—stands at 15.3 million, higher than at any time since the Census Bureau began collecting data 28
years ago.”40 A year later it had reached 15.6 million.2
Images from New Orleans in late 2005 following Hur-ricane Katrina brought temporary attention to theplight of the severely poor, but even these reports saidlittle about the growth of the problem throughout thecountry.
This study’s findings are consistent with a recent
Federal Reserve Board analysis of the net worth of U.S.families, which it conducts every 3 years. Net worth isthe difference between family assets and liabilities. Forthe 2001–2004 period, the Federal Reserve reportedthat median net worth rose by 1.5%, considerably lessthan in 1998 –2001 (10.3%). Although median net
worth increased by 4% for families above the 90thpercentile for income (from $887,900 to $924,100),median net worth declined by 11% (from $8400 to$7500) among families below the 20th percentile andby 13% (from $39,600 to $34,300) among familiesbetween the 20th and 40th percentiles. The Federal
Reserve reported that mean income for all U.S. house-holds, adjusted for inflation, decreased by 2.3%, from$72,400 to $70,700, consistent with the sinkhole effect that we observed.41 Similarly, an analysis for the Brook-ings Institution found that only the top 10% of theincome distribution has experienced growth in real
wages and salaries equal to or greater than the rate of growth in the economy.42
Several methodologic considerations pertain to our work. First, the increase in poverty rate observed in thisstudy may be temporary; data beyond 2004 could not beassessed. A recession occurred in 2001, and poverty
rates climbed and then stabilized following recessions
in 1969, 1973, 1981, and 1990.2,43 Second, the study relied entirely on USCB data to measure incometrends; such data are the nation’s only primary bench-mark for tracking poverty rates. Third, census data aresubject to sources of error documented by the USCB.44
Fourth, although the poverty threshold is adjusted forinflation, an income deficit of $8000 means less overtime.
Fifth, the highest income categories (I/P ratios above2.0, and an income surplus of at least $8000) are broadand encompass the middle and upper class. Sufficient data were lacking to stratify incomes within this largegroup. Although as a whole this group decreased as aproportion after 2000 (Figures 1 and 2), a highly affluent subgroup may have increased in size. TheUSCB reports that the proportion of households withincomes of at least $250,000 increased from 1.2% in200045 to 1.5% in 2004,46 and the ratio between theincome of households at the 90th and 10th percentilesincreased from 10.58 to 11.07.2 This concentration of
wealth might explain the aforementioned increase inindices of income inequality (e.g., Gini coefficient) andthe observation that Tier-III families decreased as aproportion but experienced a 9% increase in theiraverage income surplus.
Fifth, this study did not explore the causes of theobserved trends or potential remedies. Lower wagesand investment earnings and changes in social pro-grams may account for lower income-adjusted incomes.Like its predecessors, the recession of 2001 would havebeen expected to fuel poverty by causing higher unem-ployment, a reduction in work hours, and stagnation of
family income.47 The economic recovery that oftenfollows a recession can mitigate these conditions, al-though some contend that changes in public policies(e.g., reduced welfare assistance and a weaker socialsafety net) and unfavorable job opportunities may account for the continued growth in poverty after 3
years of economic recovery.48
The increase in severe poverty and the overrepresen-tation of children that were observed in this study may also relate to demographic characteristics among immi-grants, who accounted for 42% of U.S. populationgrowth in the 2000–2005 period.49 Other possibilities
for increased poverty include decreased earnings by parents, diminished real value of income-transfer pro-grams (welfare, or temporary aid to needy families),and increases in female single-parent households.50
The study did not explore potential solutions to pov-erty, such as education; we recently demonstrated that almost 200,000 U.S. deaths could be averted each yearif all adults had the life expectancy of those whoattended college.51
Finally, these analyses are anchored to the poverty threshold, a metric with known limitations. As notedearlier, the Orshansky formula incorporates outdated
assumptions about living expenses. Food now accounts
6 American Journal of Preventive Medicine, Volume xx, Number x www.ajpm-online.net

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 7/12
for approximately one sixth of family budgets,52 andthe formula ignores modern-day expenses such as childcare and higher costs for housing and transportation.The threshold makes no adjustment for geographic
variation in the cost of living. In communities such as Washington DC and San Francisco, the average rentalfor a one-bedroom apartment exceeds the entire pov-erty threshold for an individual or couple.53,54
Although these factors suggest that the federal pov-erty threshold underestimates the prevalence of pov-erty, the exclusion of some income categories in theOrshanksy formula might serve to inflate the poverty rate. For example, the formula excludes cash andnoncash transfers received by the poor, such as publicassistance (e.g., government insurance, food stamps,housing aid, tax credits), tax benefits, and gains fromstock holdings. Experimental alternative poverty mea-sures that have been suggested to correct for thedeficiencies in the Orshansky formula include somethat generate higher prevalence estimates for poverty
(e.g., measures proposed by the National Academy of Sciences) and some that generate lower estimates (e.g.,measures considered by the USCB).55–58 Others advo-cate the use of relative, rather than absolute, measuresof poverty.5,59
These considerations speak to the imprecision of theofficial poverty threshold in quantifying the true pov-erty rate—for 2003, when the official poverty rate was12.5%, the estimated poverty rate from experimentalmeasures ranged from 7.4% to 14.5%57—but this im-precision bears little on the temporal trends reportedhere because the magnitude of the variation has held
constant over time. From 1987 to 2003, alternativemeasures that yield lower estimates for the poverty ratefollowed the same slope as did the official measure.57
The exclusion of cash and noncash assistance from theofficial measure could conceivably act as a confounding
variable in our key finding—that the growth of severepoverty was greater than for moderate poverty—hadthe severely poor received more of such assistance.There is little evidence of such a difference, however.For example, in 2004, the severely poor (I/P ratio of less than 0.5) and the moderately poor (I/P ratio of 0.5to 1.0) differed little in their receipt of cash or noncash
transfers (93% vs 95%, respectively)60 or Medicaid(76% vs 75%, respectively).61 Differences noted forsome forms of aid, such as food stamps (56% vs 47%,respectively),62 were unlikely to account for the dra-matic differences in the growth of moderate and severepoverty observed in this study.
The risk of slipping into severe poverty is not sharedequally across the population. This study found that
African Americans and Hispanics face a greater riskthan do whites or Asians. In 2004, African Americansaccounted for 9% of those with an I/P ratio of greaterthan 2.0,27 but they constituted an increasing propor-
tion of those with progressively lower incomes (16%,
22%, and 27%, respectively, of Americans with an I/Pratio of 1.0 to 2.0, 0.5 to 1.0, and less than 0.5). Theburden of supporting a family in severe poverty fallsdisproportionately on minorities. In 2004, African
Americans led the households of 9% of families in TierIII, but 19% of families in Tier II and 30% of families inTier I. Hispanics led 10% of families in Tier III but 24%of families in Tiers I and II.
The most troubling finding is that the risk of severepoverty is greater among children than among adults.Children aged less than 5 years face the greatest risk(Table 1). In 2004, one of three Americans withincomes less than 50% of the poverty threshold—a totalof 5.6 million people—was a child. The risks areenormous among minority children: Children account for 44% and 45%, respectively, of Hispanic and African
Americans with I/P ratios less than 0.5.27 Families withchildren account for 48% of families in Tier III and81% of families in Tier I (Table 2).
The public health implications of increasing poverty
are profound, given how strongly social class is linked with premature mortality, disease, and mental ill-ness.1,63–67 The poor have greater exposure to riskfactors, such as those caused by homelessness, substan-dard housing, and environmental pollutants.68,69 They experience greater rates of smoking, physical inactivity,and obesity,63,70 in part because impoverished neigh-borhoods are not conducive to healthy lifestyles (e.g.,having built environments for walking71 and supermar-kets that offer healthy food choices72); these commu-nities are also targets for the promotion of cigarettes,alcoholic beverages, and fast foods.73–75
The poor lack jobs that offer health insurance andcannot afford to purchase insurance themselves.76 Fully 31% of those below the poverty threshold are unin-sured, and 23% report no usual source of care.63 Cost remains a barrier even among those eligible for Med-icaid or indigent services, due to greater cost shifting topatients and out-of-pocket expenditures.77–79 Thesebarriers often impel the poor to forego care or to seekit episodically for acute problems, missing opportuni-ties for prevention and allowing disease complicationsto intensify.80 The quality of care that they do receive iscompromised by the fragmented infrastructure in un-
derserved communities, where facilities and cliniciansare often lacking in number, resources, and culturalsensitivity.81,82 For these various reasons, the poor onaverage receive inferior health care, have worse healthstatus, and require greater use of resources.63,83,84
Emergency department visits and the length of hospitalstays among the poor are more than twice those of thegeneral population.63
These health effects result partly from inadequateincome but also reflect other interrelated characteris-tics of the poor, such as education, race, ethnicity, andenvironmental factors. Inadequate education, which
often accompanies poverty, is a barrier to making wise
Month 2006 Am J Prev Med 2006;xx(x) 7

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 8/12
personal health choices and to advancing to suitable jobs that provide higher earnings and health insurance.Health status and health care differ by race and ethnic-ity, even after adjustment for socioeconomic status.85,86
Given that the population in poverty is over-repre-sented by immigrants, some might wonder whether thelink between poverty and health is refuted by the“healthy immigrant” phenomenon, in which new immi-
grants enter the country in comparatively better healththan their native-born counterparts or than immigrants
who have lived in the United States for more than 10 years.87,88 This phenomenon may result in part fromselection factors in the population who choose toemigrate and from conditions that cause deteriorationin health as residents in the United States (e.g., accul-turation, adoption of unhealthy behaviors, poor accessto healthcare services). Exposure to poverty is likely toexacerbate these conditions and to accelerate the pro-cess by which the health of immigrants deteriorates.
The adverse health experienced by those below the
poverty threshold is amplified for severe poverty. Therelationship between income and life expectancy climbssteeply at the extremes of poverty and plateaus at higherincome levels.89 Health outcomes for the severely poorare worse than for those in moderate poverty.90,91 Therising prevalence of severe poverty, which is reportedhere, is therefore cause for concern. As the number of people in severe poverty increases, we would expect growth in the prevalence of chronic illness, more fre-quent and severe complications, and greater demandsand costs for healthcare services. The number of unin-sured will grow, further burdening public programs (e.g.,
Medicaid) and facilities for indigent care. Severe poverty also threatens the economy: The severely poor cannot contribute to a vibrant workforce, and their health needsrequire society to pay higher taxes or insurance premiumsto offset treatment costs.
Perhaps the most lasting consequences are for chil-dren, the age group that we found to be at greatest riskfor severe poverty. Children are especially vulnerable toharm from severe poverty because of its influences onperinatal outcomes, growth, nutrition, parenting,safety, development, emotional health, access to healthcare, adolescent pregnancy, cognition, and educational
success.50,92–94 Children exposed to severe poverty areat greater risk of experiencing unemployment, learningdisabilities, mental illness, physical disease, substanceabuse, and crime as adults.95–103 They are also morelikely to remain in poverty as adults,104 thereby perpet-uating the cycle for their children.105,106 According toone report, only 6% of children who grow up in thelowest quintile of income attain the highest incomequintile as adults (compared to 42% of those who grow up in the highest income quintile).104
In recent years, government policy for fosteringupward mobility among the lower and middle classes
has been to promote vibrant commerce as a vehicle for
job creation and to reduce outlays for social services tofinance tax cuts and other incentives to “grow theeconomy.” The findings reported here suggest that thispolicy has improved incomes for only a small propor-tion of the population—primarily the most affluent class—while poverty rates at the other end of thespectrum have increased. Millions of Americans, over-represented by children and minorities, have entered
conditions of extreme poverty. After 2000, Americanssubsisting under these conditions grew as a class morethan any other segment of the population. Potentialsolutions to poverty are formidable and politically difficult,6,7,107,108 but the first step is to recognize theproblem, which to date has received little exposure,and its implications for public health and society.Policymakers should consider our data in judging
whether policies enacted in recent years have helped orhindered the public.
No financial conflict of interest was reported by the authors of
this paper.
References1. Marmot MG, Wilkinson RG, eds. Social determinants of health. Oxford:
Oxford University Press, 1999.
2. DeNavas-Walt C, Proctor BD, Lee CH. Income, poverty, and health
insurance coverage in the United States: 2004. Current Population
Reports, P60-229. Washington DC: U.S. Census Bureau, 2005. Accessed at:
www.census.gov/prod/2005pubs/p60-229.pdf.
3. Dalaker J. Poverty in the United States: 2000. Current Population Reports,
Series P60-214. Washington DC: U.S. Census Bureau, 2001. Accessed at:
www.census.gov/prod/2001pubs/p60-214.pdf.
4. U.S. White House. Economic growth continues: unemployment rate falls
to 4.7 percent. Washington DC, July 7, 2006. Accessed at: www.whitehouse.gov/infocus/economy/.
5. Kawachi I, Subramanian SV, Almeida-Filho N. A glossary for health
inequalities. J Epidemiol Community Health 2002;56:647–52.
6. Rank MR. One nation, underprivileged: why American poverty affects us
all. Oxford: Oxford University Press, 2004.
7. Iceland J. Poverty in America: a handbook. Berkeley: University of
California Press, 2003.
8. U.S. Census Bureau. How the Census Bureau measures poverty (official
measure). Washington DC: U.S. Census Bureau, 2005. Accessed at:
www.census.gov/hhes/www/poverty/povdef.html.
9. U.S. Census Bureau. Historical poverty tables. Table 5. Percent of people
by ratio of income to poverty level: 1970 to 2004. Washington DC: U.S.
Census Bureau, 2005. Accessed at: www.census.gov/hhes/www/poverty/
histpov/hstpov5.html.
10. U.S. Census Bureau. Poverty in the United States, 1990. Current Popula-
tion Reports, Series P-60, No. 175. Washington DC: U.S. Census Bureau,1991. Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-
175.pdf.
11. U.S. Census Bureau. Poverty in the United States, 1991. Current Popula-
tion Reports, Series P-60, No. 181. Washington DC: U.S. Census Bureau,
1992. Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-
181.pdf.
12. U.S. Census Bureau. Poverty in the United States, 1992. Current Popula-
tion Reports, Series P-60, No. 185. Washington DC: U.S. Census Bureau,
1993. Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-
185.pdf.
13. U.S. Census Bureau. Income, poverty, and valuation of noncash benefits:
1993. Current Population Reports, Series P-60, No. 188. Washington DC:
U.S. Census Bureau, 1995. Accessed at: www.census.gov/hhes/www/
poverty/prevcps/p60-188.pdf.
14. U.S. Census Bureau. Income, poverty, and valuation of noncash benefits:
1994. Current Population Reports, Series P-60, No. 189. Washington DC:
8 American Journal of Preventive Medicine, Volume xx, Number x www.ajpm-online.net

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 9/12
U.S. Census Bureau, 1996. Accessed at: www.census.gov/hhes/www/
poverty/prevcps/p60-189.pdf.
15. Baugher E, Lamison-White L. Poverty in the United States: 1995. Current
Population Reports, Series P60-194. Washington DC: U.S. Census Bureau,
1996. Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-
194.pdf.
16. Lamison-White L. Poverty in the United States: 1996. Current Population
Reports, Series P60-198. Washington DC: U.S. Census Bureau, 1997.
Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-198.pdf.
17. Dalaker J, Naifeh M. Poverty in the United States: 1997. Current Popula-
tion Reports, Series P60-201. Washington DC: U.S. Census Bureau, 1998.
Accessed at: www.census.gov/hhes/www/poverty/prevcps/p60-201.pdf.18. Dalaker J. Poverty in the United States: 1998. Current Population Reports,
Series P60-207. Washington DC: U.S. Census Bureau, 1999. Accessed at:
www.census.gov/hhes/www/poverty/prevcps/p60-207.pdf.
19. Dalaker J, Proctor BD. Poverty in theUnited States: 1999.Current Population
Reports, Series P60-210. WashingtonDC: U.S. Census Bureau, 2000. Accessed
at: www.census.gov/hhes/www/poverty/prevcps/p60-210.pdf.
20. Dalaker J. Poverty in the United States: 2000. Current Population Reports,
Series P60-214. Washington DC: U.S. Census Bureau, 2001. Accessed at:
www.census.gov/prod/2001pubs/p60-214.pdf.
21. Proctor BD, Dalaker J. Poverty in the United States: 2001. Current
Population Reports, Series P60-219. Washington DC: U.S. Census Bureau,
2002. Accessed at: www.census.gov/prod/2002pubs/p60-219.pdf.
22. Proctor BD, Dalaker J. Poverty in the United States: 2002. Current
Population Reports, Series P60-222. Washington DC: U.S. Census Bureau,
2003. Accessed at: www.census.gov/prod/2003pubs/p60-222.pdf.
23. U.S. Census Bureau. Income deficit or surplus of families and unrelated
individuals by poverty status. Washington DC: U.S. Census Bureau, 2004.
Accessed at: http://pubdb3.census.gov/macro/032004/pov/new28_000.
htm.
24. Shipler DK. The working poor: invisible in America. New York: Knopf,
2004.
25. Fisher GM. The development and history of the poverty thresholds. Social
Security Bull 1992;55:3–14.
26. U.S. Census Bureau. People and families in poverty by selected character-
istics: 1999 and 2000. Washington DC: U.S. Census Bureau, 2000. Ac-
cessed at: www.census.gov/hhes/www/poverty/poverty00/tablea.pdf.
27. U.S. Census Bureau. Age and sex of all people, family members and
unrelated individuals iterated by income-to-poverty ratio and race. Wash-
ington DC: U.S. Census Bureau, 2005. Accessed at: http://
pubdb3.census.gov/macro/032005/pov/new01_000.htm.
28. Pearlstein S. U.S. poverty rate rises, income drops; increase in ranks of poor is first in 8 years. Washington Post, September 25, 2002, p. A3.
29. Kaufman L. City poverty rate shows first rise in 5 years. New York Times,
September 26, 2002, p. B3.
30. Weisman J. U.S. household incomes fell, poverty rose in 2002; Democrats
say Bush policies are to blame; White House points to recent pickup in
economic recovery. Washington Post, September 28, 2003, p. A20.
31. Clemetson L. More Americans in poverty in 2002, Census study says. New
York Times, September 27, 2003, p. A1.
32. Connolly C, Witte G. Poverty rate up 3rd year in a row; more also lack
health coverage. Washington Post, August 27, 2004, p. A1.
33. Polgreen L. New York City’s poverty rate holds steady while nation’s rises.
New York Times, September 15, 2004, p. B7.
34. Weisman J, Connolly C. Poverty rate continues to climb; 2004 census data
show labor market is still struggling. Washington Post, August 31, 2005, p
A3.
35. Leonhardt D. Poverty in U.S. grew in 2004, while income failed to rise for5th straight year. New York Times, August 31, 2005, p. A9.
36. Weinberg DH. Press briefing on 2002 income and poverty estimates.
Washington DC: U.S. Census Bureau, September 26, 2003. Accessed at:
www.census.gov/hhes/www/income/income02/prs03asc.html.
37. Weinberg DH. Press briefing on 2003 income and poverty estimates from
the Current Population Survey. Washington DC: U.S. Census Bureau,
August 26, 2004. Accessed at: www.census.gov/hhes/www/income/
income03/prs04asc.html.
38. Nelson C. News conference on 2004 income, poverty, and health insur-
ance estimates from the Current Population Survey. Washington DC: U.S.
Census Bureau, August 30, 2005. Accessed at: www.census.gov/hhes/
www/income/income04/prs05asc.html.
39. U.S. Government Accountability Office. Data quality: expanded use of key
dissemination practices would further safeguard the integrity of federal
statistical data. Washington DC: U.S. Government Accountability Office,
2006 (GAO-06-607). Accessed at: www.gao.gov/new.items/d06607.pdf.
40. Poverty and health (editorial). New York Times, August 31, 2004, p. A20.
41. Bucks BK, Kennickell AB, Moore KB. Recent changes in U.S. family
finances: evidence from the 2001 and 2004 Survey of Consumer Finances.
Federal Reserve Bull 2006. Accessed at: www.federalreserve.gov/pubs/
bulletin/2006/financesurvey.pdf.
42. Dew-Becker I, Gordon RJ. Where did the productivity growth go? Inflation
dynamics and the distribution of income. Washington DC: Brookings
Institution, 2005. Accessed at: http://brookings.edu/es/commentary/
journals/bpea_macro/forum/200509bpea_gordon.pdf.
43. U.S. Census Bureau. Historical poverty tables—periods of recession.
Washington DC: U.S. Census Bureau, 2005. Accessed at: www. census.gov/
hhes/www/poverty/histpov/recessn.html.44. U.S. Census Bureau. Source and accuracy of estimates for income,
poverty, and health insurance coverage in the United States: 2004.
Washington DC: U.S. Census Bureau. Accessed at: www.census.
gov/hhes/www/income/p60_229sa.pdf.
45. U.S. Census Bureau. Income distribution to $250,000 or more for
households: 2000. Washington DC: U.S. Census Bureau, 2001. Accessed
at: http://pubdb3.census.gov/macro/032001/hhinc/new07_000.htm.
46. U.S. Census Bureau. Income distribution to $250,000 or more for
households: 2004. Washington DC: U.S. Census Bureau, 2005. Accessed
at: http://pubdb3.census.gov/macro/032005/hhinc/new06_000.htm.
47. Iceland J, Kenworthy L, Scopilliti M. Macroeconomic performance and
poverty in the 1980s and 1990s: a state-level analysis. Madison: University
of Wisconsin, Institute for Research on Poverty, 2005. Accessed at:
www.irp.wisc.edu/publications/dps/pdfs/dp129905.pdf.
48. Children’s Defense Fund. The unprotected recession: record numbers of
families have no work and no welfare in 2001. Washington DC: Children’s
Defense Fund, 2003. Accessed at: www.childrensdefense.org/pdf/
noworknowelfare.pdf.
49. U.S. Census Bureau. Cumulative estimates of the components of popula-
tion change for the United States and states: April 1, 2000 to July 1, 2005.
Washington DC: U.S. Census Bureau, 2005. Accessed at: www. census.gov/
popest/states/tables/NST-EST2005-04.xls.
50. Wood D. Effect of child and family poverty on child health in the United
States. Pediatrics 2003;112:707–11.
51. Woolf SH, Johnson RE, Phillips RL Jr, Philipsen M. Giving everyone the
health of the educated: would social change save more lives than medical
advances? Am J Public Health. In press.
52. Willis J. How we measure poverty: a history and brief overview. Silverton:
Oregon Center for Public Policy, 2000. Accessed at: www.ocpp.org/
poverty/how.htm.
53. Harrington DB. Top 10 Out-of-Control Rental Markets. Move, Inc. Accessed at www.move.com/Rentals/Apartment%20Search%20Tips/
Content00026388.aspx?poeϭmove.
54. The State of the Rental Market. RentalGuide.com. Publishing Group, Inc.
Accessed at http://www.rentalguide.com/rentalmarket.html.
55. Citro CF, Michael RT, Measuring poverty: a new approach. panel on
poverty and family assistance: concepts, information needs, and measure-
ment methods. Washington DC: National Academy Press, 1995.
56. Short K. Experimental poverty measures: 1999. Current Population
Reports, Series P60-216. Washington DC: U.S. Census Bureau, 2001.
Accessed at: www.census.gov/prod/2001pubs/p60-216.pdf.
57. U.S. Census Bureau. Alternative poverty estimates in the United States:
2003. Current Population Reports. Washington DC: U.S. Census Bureau,
2005. Accessed at: www.census.gov/prod/2005pubs/p60-227.pdf.
58. U.S. Census Bureau. The effects of government taxes and transfers on
income and poverty: 2004. Washington DC: U.S. Census Bureau, February
2006. Accessed at: www.census.gov/hhes/www/poverty/effect2004/effectofgovtandt2004.pdf.
59. Cassidy J. Relatively deprived. How poor is poor? New Yorker, April 2006.
60. U.S. Census Bureau. People in households that received means-tested
cash or noncash assistance including school lunch, 2004. Washington DC:
U.S. Census Bureau, 2005. Accessed at: http://pubdb3.census.gov/
macro/032005/pov/new25_002_02.htm.
61. U.S. Census Bureau. People in households in which one or more
members were covered by Medicaid, 2004. Washington, DC: U.S. Census
Bureau, 2005. Accessed at: http://pubdb3.census.gov/macro/032005/
pov/new25_005_05.htm.
62. U.S. Census Bureau. People in households that received food stamps,
2004. Washington DC: U.S. Census Bureau, 2005. Accessed at: http://
pubdb3.census.gov/macro/032005/pov/new25_004_04.htm.
63. National Center for Health Statistics. Health, United States, 2005. Hyatts-
ville MD: National Center for Health Statistics, 2005. Accessed at: www.
cdc.gov/nchs/data/hus/hus05.pdf.
Month 2006 Am J Prev Med 2006;xx(x) 9

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 10/12
64. Marmot MG, Davey Smith G, Stansfeld SA, et al. Health inequalities among
British civil servants: the Whitehall II study. Lancet 199;:337:1387–93.
65. Kennedy BP, Kawachi I, Glass R, Prothrow-Stith D. Income distribution,
socioeconomic status, and self rated health in the United States: multilevel
analysis. BMJ 1998;317:917–21.
66. Martikainen P, Makela P, Koskinen S, Valkonen T. Income differences in
mortality: a register-based follow-up study of three million men and
women. Int J Epidemiol 2001;30:1397–405.
67. Daniels N, Kennedy B, Kawachi I, Cohen J, Rogers J. Is inequality bad for
our health? Boston: Beacon Press, 2000.
68. Hwang SW, Tolomiczenko G, Kouyoumdjian FG, Garner RE. Interven-
tions to improve the health of the homeless: a systematic review. Am J Prev Med 2005;29:311–9.
69. Brulle RJ, Pellow DN. Environmental justice: human health and environ-
mental inequalities. Annu Rev Public Health 2006;27:103–24.
70. Miech RA, Kumanyika SK, Stettler N, Link BG, Phelan JC, Chang VW.
Trends in the association of poverty with overweight among US adoles-
cents, 1971–2004. JAMA 2006;295:2385–93.
71. Humpel N, Owen N, Leslie E. Environmental factors associated with
adults’ participation in physical activity: a review. Am J Prev Med
2002;22:188–99.
72. Moore LV, Diez Roux AV. Associations of neighborhood characteristics
with the location and type of food stores. Am J Public Health
2006;96:325–31.
73. Gardiner PS. The African Americanization of menthol cigarette use in the
United States. Nicotine Tob Res 2004;6(suppl 1):S55–65.
74. Alaniz ML, Wilkes C. Pro-drinking messages and message environments
for young adults: the case of alcohol industry advertising in African American, Latino, and Native American communities. J Public Health
Policy 1998;19:447–72.
75. Block JP, Scribner RA, DeSalvo KB. Fast food, race/ethnicity, and income:
a geographic analysis. Am J Prev Med 2004;27:211–7.
76. Gabel J, Claxton G, Gil I, et al. Health benefits in 2005: premium increases
slow down, coverage continues to erode. The average cost of family
coverage now exceeds the average yearly income of minimum-wage
Americans. Health Aff 2005;24:1273–80.
77. Johnson TJ, Rimsza M, Johnson WG. The effects of cost-shifting in the
State Children’s Heath Insurance Program. Am J Public Health
2006;96:709–15.
78. Galbraith AA, Wong ST, Kim SE, Newacheck PW. Out-of-pocket financial
burden for low-income families with children: socioeconomic disparities
and effects of insurance. Health Serv Res 2005;40:1722–36.
79. Himmelstein DU, Warren E, Thorne D, Woolhandler S. Illness and injury
as contributors to bankruptcy. Health Aff 2005. Supplemental web exclu-sives W5-63-W5-73.
80. Ross JS, Bradley EH, Busch SH. Use of health care services by lower-
income and higher-income uninsured adults. JAMA 2006;295:2027–36.
81. Georges CA, Bolton LB, Bennett C. Quality of care in African-American
communities and the nursing shortage. J Natl Black Nurses Assoc
2003;14:16–24.
82. Sullivan Commission. Missing persons: minorities in the health profes-
sions. A report of the Sullivan Commission on diversity in the healthcare
workforce. Durham, NC: Duke University, 2004.
83. Agency for Healthcare Research and Quality. National healthcare dispar-
ities report, 2005. Rockville MD: Agency for Healthcare Research and
Quality, 2005. Accessed at: www.ahrq.gov/qual/nhdr05/nhdr05.htm.
84. Asch SM, Kerr EA, Keesey J, et al. Who is at greatest risk for receiving
poor-quality health care? N Engl J Med 2006;354:1147–56.
85. Smedley BD, Stith AY, Nelson AR, eds. Unequal treatment: confronting
racial and ethnic disparities in health care. Committee on Understandingand Eliminating Racial and Ethnic Disparities in Health Care, Board on
Health Sciences Policy, Institute of Medicine. Washington DC: National
Academy Press, 2003.
86. Geiger HJ. Race and health care—an American dilemma? N Engl J Med
1996;335:815–6.
87. Stephen EH, Foote K, Hendershot GE, Schoenborn CA. Health of the
foreign-born population: United States, 1989–1990. Adv Data
1994;241:1–12.
88. McDonald JT, Kennedy S. Insights into the ‘healthy immigrant effect’:
health status and health service use of immigrants to Canada. Soc Sci Med
2004;59:1613–27.
89. World Bank. World Development Report 1993: investing in health.
Oxford: Oxford University Press, 1993. Accessed at: www-wds.worldbank.
org/external/default/WDSContentServer/IW3P/IB/1993/06/01/
000009265_3970716142319/Rendered/PDF/multi0page.pdf.90. Pappas G, Queen S, Hadden W, Fisher G. The increasing disparity in
mortality between socioeconomic groups in the United States, 1960 and
1986. N Engl J Med 1993;329:103–9.
91. Seguin L, Xu Q, Potvin L, Zunzunegui MV, Frohlich KL. Effects of low
income on infant health. CMAJ 2003;168:1533–8.
92. Stevens GD, Seid M, Mistry R, Halfon N. Disparities in primary care for
vulnerable children: the influence of multiple risk factors. Health Serv Res
2006;41:507–31.
93. Cawley J, Schroeder M, Simon KI. How did welfare reform affect health
insurance coverage of women and children? Health Serv Res
2006;41:486–506.
94. Zill N, Schoenborn CA. Developmental, learning, and emotional prob-
lems. Health of our nation’s children, United States, 1988. Adv Data
1990;190:1–18.
95. Case A, Fertig A, Paxson C. The lasting impact of childhood health and
circumstance. J Health Econ 2005;24:365–89.96. Graham H, Power C. Childhood disadvantage and health inequalities: a
framework for policy based on lifecourse research. Child Care Health Dev
2004;30:671–8.
97. Wadsworthx ME. Changing social factors and their long-term implications
for health. Br Med Bull 1997;53:198–209.
98. Singh-Manoux A, Richards M, Marmot M. Socioeconomic position across
the lifecourse: how does it relate to cognitive function in mid-life? Ann
Epidemiol 2005;15:572–8.
99. Lawlor DA, Ebrahim S, Davey Smith G. Adverse socioeconomic position
across the lifecourse increases coronary heart disease risk cumulatively:
findings from the British women’s heart and health study. J Epidemiol
Community Health 2005;59:785–93.
100. Feinstein L, Bynner J. The importance of cognitive development in
middle childhood for adulthood socioeconomic status, mental health,
and problem behavior. Child Dev 2004;75:1329–39.
101. Kuh DL, Ben Shlomo Y, eds. A life course approach to chronic diseaseepidemiology. Tracing the origins of ill health from early to adult life.
Oxford: Oxford University Press, 1997.
102. Hertzman C. The biological embedding of early experience and its effects
on health in adulthood. Ann NY Acad Sci 1999;896:85–95.
103. Werner EE, Smith RS. Journeys from childhood to midlife: risk, resilience
and recovery. Ithaca NY: Cornell University Press, 2001.
104. Hertz T. Understanding mobility in America. Washington DC: Center for
American Progress, 2006. Accessed at: www.americanprogress.org/atf/cf/
{E9245FE4-9A2B-43C7-A521-5D6FF2E06E03}/HERTZ_MOBILITY_
ANALYSIS.PDF.
105. Kahn RS, Wilson K, Wise PH. Intergenerational health disparities: socio-
economic status, women’s health conditions, and child behavior prob-
lems. Public Health Rep 2005;120:399– 408.
106. Goldman N. Social inequalities in health disentangling the underlying
mechanisms. Ann NY Acad Sci 2001;954:118–39.
107. Sachs JD. The end of poverty: economic possibilities for our times. New York: Penguin Press, 2005.
108. Phillips K. Wealth and democracy: a political history of the American rich.
New York: Broadway Books, 2002.
10 American Journal of Preventive Medicine, Volume xx, Number x www.ajpm-online.net

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 11/12
Table 1. Number of families and unrelated individuals, by income deficit/surplus, 1990 - 2004
(continued)
Am J Prev Med 2006;xx(x) 10.e1

7/27/2019 AJPM_Woolf_Oct06 (1).pdf
http://slidepdf.com/reader/full/ajpmwoolfoct06-1pdf 12/12
Table 1. Continued
10 2 A i l f i di i l b


![science3stprimaryschool[1] (1).pdf](https://img.pdfslide.us/doc/110x75/5695d0681a28ab9b029256b7/science3stprimaryschool1-1pdf.jpg)
![1 habit 1[1].pdf](https://img.pdfslide.us/doc/110x75/55cf92cb550346f57b999be7/1-habit-11pdf.jpg)


![Case_Studies[1] (1).pdf](https://img.pdfslide.us/doc/110x75/55cf8fbc550346703b9f471e/casestudies1-1pdf.jpg)

![PDF-LEctura previa-Bloque1 (1)[1].pdf](https://img.pdfslide.us/doc/110x75/55cf91bc550346f57b903215/pdf-lectura-previa-bloque1-11pdf.jpg)




![Media kit 2010[1].pdf low res..pdf-1](https://img.pdfslide.us/doc/110x75/58f19a9f1a28aba8488b45d9/media-kit-20101pdf-low-respdf-1.jpg)