Embed Size (px)
Citation preview

1
Healthwatch Shropshire
An analysis of the awareness and attitudes towards the complaints procedures in local general practices in
Shrewsbury, from the perception of patients and staff members.
Aisling McCann
Eve Horner
Marianne Pourikkou-James
Word Count : 1947
March 2018

2
Contents
Introduction
Project Aims
Method
Results
Evaluation
Recommendations
Handover and future development
Acknowledgments
References
Appendix 1 Questionnaire for GP Staff
Appendix 2 Questionnaire for Patients
Appendix 3 Focus group questions
Appendix 4 Handover Form
Appendix 5 Record of engagement

3
Introduction:
Healthwatch Shropshire is a local organisation and registered charity that is based in
Shrewsbury. The organisation is part of a network of Local Healthwatches across England that were established by the Health & Social Care Act 2012.
Healthwatch Shropshire helps to ensure everyone gets the best from their health and
social care services, also that those services are as good as they can be and work in
a connected way. They do this by giving the general public the opportunity to voice
their opinion on the health and social care services which affect them and gathering
the experiences of local people to influence commissioning, provision and scrutiny of local health and social care services (2).
Their mission is ‘to be the recognised independent voice of the people of Shropshire
in seeking to improve their experience of Health and Social Care services.’ [1]
Funding for local Healthwatches comes from Department of Health via local councils,
Healthwatch Shropshire is commissioned by Shropshire council. The organisation
prides itself in being the ‘health and social care champion for people and local communities in Shropshire.’ [1]

4
Project Aims:
To explore people’s experiences of providing feedback on and making a complaint
about health and social care services:
• Learn about the local GP complaint processes
• Engage with people to gather experiences
• Identify barriers to people sharing their experiences/making a complaint
• Identify staff knowledge of complaints procedure at practice
• Identify good practice
• Develop recommendations that can be taken forward locally
We first met with Adelle Wilkinson (Community Engagement Officer) to discuss the
potential project themes in December and we unanimously agreed on the topic of
complaints within the NHS. This title seemed to spark the most conversation and
interest within the group. Adelle kindly arranged for us to meet with Lynn Cawley, a
member of the Healthwatch Shropshire team, who is the coordinator for the ‘Independent Health Complaints Advocacy Service’(IHCAS).
In this meeting we learnt a lot about the legalities of making a complaint and the
procedures that need to be followed for a formal complaint. We discussed the
differences between formal and informal complaints and the role of patient advice
and liaison services (PALS) within the hospital. We specifically learnt about the
IHCAS service delivered by Healthwatch Shropshire for patient complaints. They
provide an advocacy service for the general public, but cannot complain for people, their role lies within empowering people to make complaints.
After this meeting, we realised the complexities of the complaints policies and
procedures and the differences within primary and secondary care. We decided to
focus our project on the complaints solely within primary care, specifically in the
practices that we were individually attached for general practice, Claremont Bank

5
Surgery, Beeches Medical Practices and Riverside Medical Practice. We agreed that
the tasks of exploring complaints within primary and secondary care would not have been achievable in the allocated time.
Method:
We used a structured questionnaire for patient and staff responses to gain insight
into knowledge about complaints in a general practice setting. We used a
combination of quantitative and qualitative questions, specifically aimed to use
dichotomous questions for accessibility for all our respondents. We focused on
questions including awareness and knowledge of complaints procedure within staff
and patients, and factors we felt that may influence their knowledge. We included
some open qualitative questions to clarify knowledge of both patients and staff
members.
The questionnaires were drafted and trialled on respondents, so we could refine in
on flaws within our wording or style of the questions. This led to some improvements
within the questions and later were approved by Keele University for use. [Appendix
1 & 2]
We decided on allocating ten of each patient and staff questionnaires in each of our
three GP practices, this gave us a total of thirty respondents for each patient and
staff questionnaires, and an idea of a general trend emerging.
We randomly allocated the patient questionnaires to the patients of all clinicians, not
specifically our own patients attending the surgery to reduce selection bias, and with
staff questionnaires we aimed to get an even spread of clinical and non-clinical staff
members.
Once the questionnaires were completed and handed back to reception staff, we
analysed the responses and were able to compile these results into graph form.
Based on the patient questionnaire feedback we compiled some questions to focus
on areas for improvement and further engagement from a patient perspective at the
Shropshire Patient Group (SPG) [Appendix 3]. Collectively we decided to use the

6
SPG as our patient population focus group due to time constraints and difficulty
arranging appropriate meeting with each of our practices own PPGs. We collected
this information at the focus group and looked at common themes emerging and
used this information to confirm our initial conclusions and direct improvements that
may be put in place.
Results:
Results from the patient questionnaires [Appendix 2]:
Through the patient questionnaires, the following data has been collected by thirty randomly selected patients, ten from each of the three GP practices.

7

8

9
10
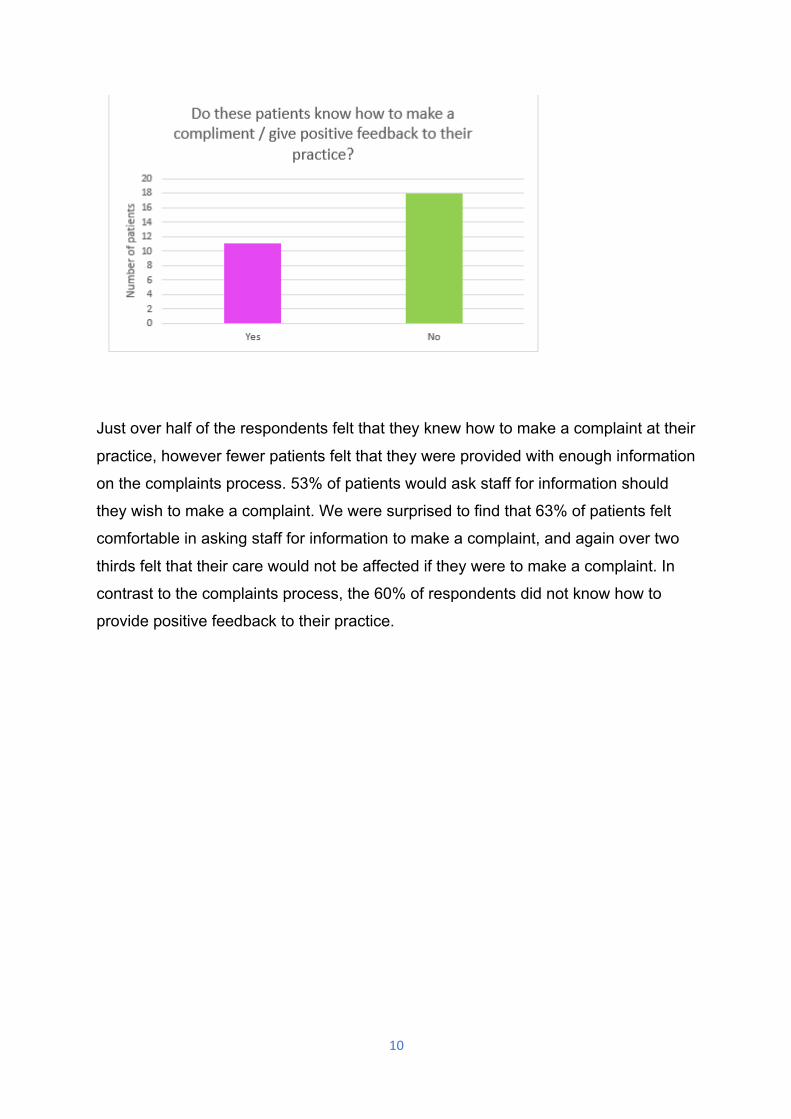
Just over half of the respondents felt that they knew how to make a complaint at their
practice, however fewer patients felt that they were provided with enough information
on the complaints process. 53% of patients would ask staff for information should
they wish to make a complaint. We were surprised to find that 63% of patients felt
comfortable in asking staff for information to make a complaint, and again over two
thirds felt that their care would not be affected if they were to make a complaint. In
contrast to the complaints process, the 60% of respondents did not know how to
provide positive feedback to their practice.

11
Results from GP staff questionnaires [Appendix 1]:
We randomly selected ten patients from each of the three GP practices to complete these questionnaires.

12

13
All respondents from the staff questionnaires interacted with patients, with just over
half of them in an administrative job role at their practice. All but one staff member
was aware of the complaints procedure at their practice, however five staff members were not aware of the complaints policy.

14
0
2
4
6
8
10
12
14
Intranet GPteamnet
ProcedureandPolicyfolder
GPportalnet
Docman Practicemanager
Sharednetworkdrive
Num
bero
fstaff
Wherewouldthesestaffmemberslooktofindthecomplaintsprocedureattheirpractice?
13
13.5
14
14.5
15
15.5
16
16.5
Yes No Don’tknow
numbe
rofstaff
Arestaffmembersawareofanyinformationpresentinthewaitingareaoftheirpracticeadvisingpatientsonhowtocomplain?

15
Majority of staff members said that they would advise patients to approach the practice manager, submit a written complaint, or fill in a complaint form should they wish to make a complaint at their practice. Most of the staff members stated that they were aware of where to find the complaints procedure at their practice, mainly through the intranet or discussion with their practice manager. Just over half of staff members questioned were unsure about information available in the waiting area, this is likely due to the mixture of administrative and clinical staff.

16
In addition, most felt that they would feel comfortable signposting patients to make a
complaint and would know what to do if a formal complaint was handed to them.
However, six of the respondents highlighted that they felt they have not received adequate training in the complaints process.

17
Findings from the SPG Meeting: [Appendix 3]
When asked about barriers that would prevent patients from making complaints,
many agreed there was a ‘hierarchy’ within a medical practice, with doctors at the
top and patients at the bottom. Because of this, they felt that the GPs had most of
power and therefore if they were to make a complaint, the members of the SPG felt
that their care would be affected. They also identified that a paternalistic relationship
existed between older patients and GPs which again prevented these patients from
making complaints as they would not want to upset the balance of their relationship
or be labelled as a trouble maker.
We then asked if they felt that their care would be affected if they were to make a
complaint. The majority of the SPG agreed that their care was likely to be affected,
and therefore this would prevent them from making a complaint. During this
discussion, the words ‘intimidation’ and ‘hierarchy’ were repeatedly used as with the
previous question. In addition, one member of the SPG highlighted the fact that
disadvantaged patients were allocated an advocate (for example, from Healthwatch),
however patients who did not fit within this category were not offered such services.
They explained that they felt an advocate for all patients would be supportive and
remove this barrier to complaining.
We also felt it was important to ask the SPG what they thought could be done to
improve the complaints procedure, or at least make it easier for patients to complain.
Many agreed that anonymising complaints would be difficult, or not appropriate, as
some complaints would need to be escalated and the nature of other complaints
would make patients identifiable. Nonetheless, they did have some suggestions
regarding how to avoid some of the barriers previously identified. For example, the
use of an advocate to direct complaints to, someone who did not work at that GP
practice. They also felt that more information needs to be given to patients regarding
complaining, and that posters or leaflets informing patients on the complaints
process should be friendlier and encourage the use of constructive criticism to
improve services and education of staff.
Regarding positive feedback, the SPG felt that patients were quick to complain but
not so to make compliments. They felt that positive feedback was just as important

18
as complaints. Many of the GP practices within the SPG has suggestion boxes for
positive feedback and for constructive criticism, which they felt worked well.
However, they all agreed that such boxes are not appropriate for complaints,
especially for the type of complaints that may need to be escalated.
Evaluation:
Analysis of the patient questionnaires displayed a surprising number of patients who
felt comfortable making complaints about their GP practice, and that the majority of
those asked did not feel their care would be affected by making a complaint.
Discussion with the SPG demonstrated a contrast to this. We felt the results of the
questionnaires may have hindered a true reflection of how these patients felt,
because of the setting, and because the questionnaires were being handed back to
reception staff.
In addition, the suggestion of an independent person to oversee internal complaints
has a potential role in the GP complaints process. Aimed at reducing bias or stigma
attached to making a complaint, and hopefully overcome this hierarchical barrier. We
acknowledge that some complaints are very case specific and therefore are easily
identifiable thus, regardless of the independent complaints advocate, the complaint
would be alerted to the staff member involved and therefore patients may still feel
that their care would be affected and ultimately have no impact on the likelihood of
that patient complaining.
Many staff members understood how to make a complaint and knew how to inform
patients on complaining. We identified that the mainstay of training was an online e-
learning module and one respondent highlighted that they felt this was ‘monotonous’
in free text alongside the question. Therefore, we considered whether role play
scenarios within the practice training day would be beneficial and educational.

19
Recommendations:
If we were to repeat this project and improve our methodology, it may be beneficial
to have questionnaires completed by members of the public, independent to the GP
practice and include a larger sample size. Additionally, we could prioritise anonymity
(use of survey monkey) to better our results. This way, respondents may be more
likely to be honest regarding their thoughts about complaining and barriers such as
impact on their care if a complaint were made.
We could also include information given to patients in relation to making complaints
and compliments about the practice and consider improvements to information
available within the patient waiting area.
Education around patient and staff knowledge that not all complaints need to be
formal, possible use of open and informal feedback is valuable to offer constructive
improvements to the practice or service provided.
Handover and Future development
[Appendix 4]

20
Acknowledgements
We would like to thank Adelle Wilkinson and Jane Randall-Smith for all their help
and support throughout the project, and a special thanks to the Shropshire Participation Group for allowing us to attend their group.
References
1. Healthwatch Shropshire website: http://www.healthwatchshropshire.co.uk/content/about-us
2. Healthwatch Shropshire Leaflet: http://www.healthwatchshropshire.co.uk/sites/default/files/hws19126.pdf
21
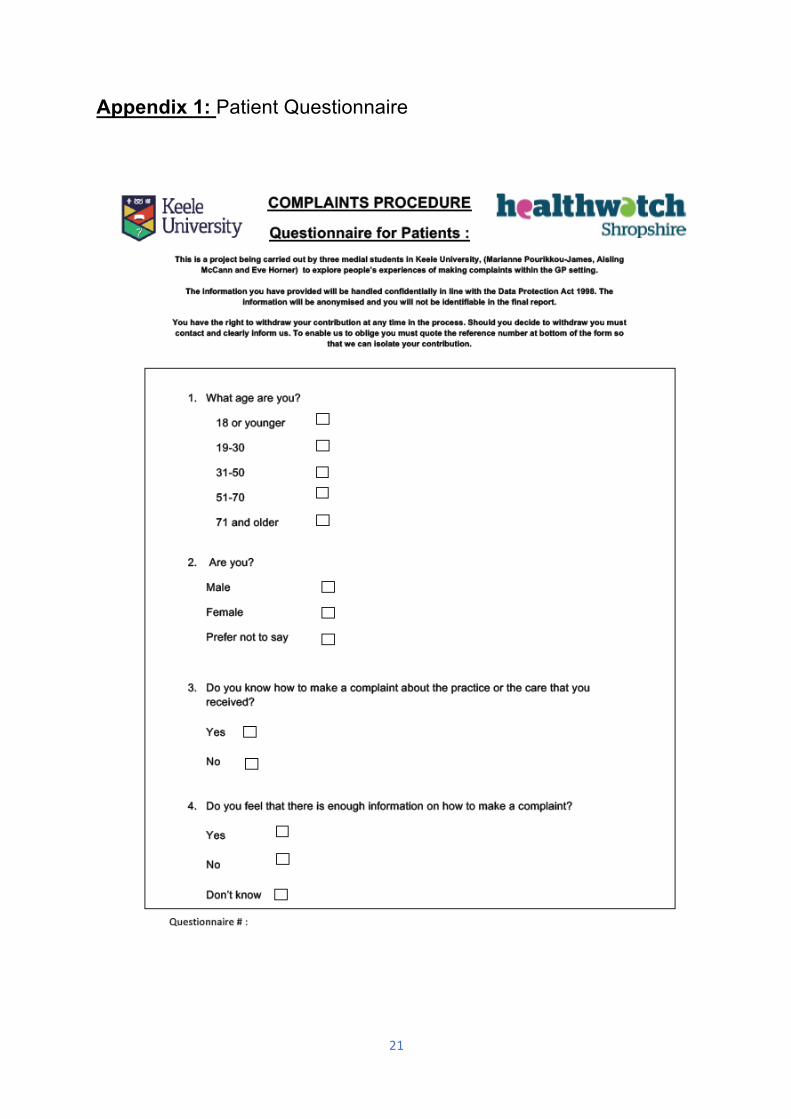
Appendix 1: Patient Questionnaire

22

23
Appendix 2: Staff Questionnaire

24

25
Appendix 3 Focus Group Questions “Makingacomplaint:RecommendationswithintheGPsettingfromapatient’sperspective”
Anybarriersthatpreventpatientsfrommakingcomplaints?
Somepatientsfeelthattheircarewouldbeaffectediftheyweretomakeacomplaint–wouldyouagreewiththis?Howcouldthisbeavoided?
Whatdoyouthinkcanbedonetoimprovethecomplaintsprocedure/makeiteasierforpatients?
Positivefeedback/constructivecriticism–doyouthinkthisisasimportantashelpingpatientstomakecomplaints?
Anyadditionalcommentsregardingcomplaints/positivefeedback?

26
Appendix 4: Handover Form
Appendix 5: Activity Log

27
Project: Healthwatch Shropshire: An analysis of the awareness and attitudes
towards the complaints procedures in local general practices in Shrewsbury, from the perception of patients and staff members.
Wk No Day/Date/Time Proposed plan Actual plan
1 Wed 13th Dec
2017 10am
First meeting with Healthwatch Shropshire
Agreed consensus to focus on the complaints
2 Tues 2nd Jan
2018 10am
Meeting with the Lynn the NHS advocacy complaints
coordinator
Decision to focus on complaints in primary care
3 Tues 9th Jan
2018 9:30am
Drafts of questionnaires Drafts of questionnaires for patients and staff
4 Tues 16th Jan 2018
Final versions of questionnaires created
Final changes to questions and questionnaires made.
Questionnaires sent to Keele for approval
5 Tues 23rd Jan 2018
Trials of questionnaires handed to people
Trials of questionnaires handed to people
6 Tues 30th Jan 2018
Focus group preparation
Questions for focus group discussed
Questionnaires started to be handed out to GP staff and
patients
7 Wed 7th Feb 2018
Focus Group with Shropshire Participation Group (SPG) Focus group
9 Tues 13th Feb 2018 Data collection Data collection
10 Wed 21st Feb 2018
Recording of data in excel document for each practice
Recording of data Report plan
11 Tues 6th March 2018
Discuss Results Plan Report
To do individual parts of report and meet to discuss and put
together
12 Tues 13th March 2018
Meet to discuss report and email to Adelle
To finalise report and start presentation
13 Tues 20th March 2018
Meet to discuss report before sending off final report Met in library to finalise report

28
14 Tues 27th March 2018
Practice presentation at Healthwatch, finalise minor
details
14 Thurs 29th March 2018 Presentation Day!