Embed Size (px)
DESCRIPTION
Define RespirationThe exchange of gases between a living organism and the environmentDefine VentilationMechanical Process that moves air in and out of the lungs
Citation preview

AIRWAYS MANAGEMENT

Respiratory Anatomy & Physiology

Airway Anatomy
• Upper Airway– Nose– Pharynx– Epiglottis– Glottis– Vocal cords– Larynx
• Lower Airway– Trachea– Bronchi– Alveoli– Lung tissue, consisting of lobes and lobules (3 on
the right and 2 on the left)– Pleura

www.drsarma.in 4
Anatomy of Respiratory Tree

Functions of the Upper Airway
• Passageway for air• Warm• Filter• Humidify• Protection
– Gag Reflex– Cough
• Speech

Physiology of Respiration
• Define Respiration– The exchange of gases between a living organism
and the environment• Define Ventilation– Mechanical Process that moves air in and out of
the lungs

Basics of the Respiratory SystemRespiration
• What is respiration?– Respiration = the series of exchanges that leads to the
uptake of oxygen by the cells, and the release of carbon dioxide to the lungs
Step 1 = ventilation– Inspiration & expiration
Step 2 = exchange between alveoli (lungs) and pulmonary capillaries (blood)– Referred to as External Respiration
Step 3 = transport of gases in bloodStep 4 = exchange between blood and cells
– Referred to as Internal Respiration– Cellular respiration = use of oxygen in ATP synthesis

External Respiration
Internal Respiration
Schematic View of Respiration

Mechanics of breathing
• Compliance:
– This the ability of the lungs to stretch during inspiration
– lungs can stretch when under tension.• Elasticity:
– It is the ability of the lungs to recoil to their original collapsed shape during expiration
– Elastin in the lungs helps recoil

Inspiration
• Inspiration – Active process• Diaphragm contracts -> increased thoracic
volume vertically.• Intercostals contract, expanding rib cage ->
increased thoracic volume laterally.• More volume -> lowered pressure -> air in.• Negative pressure breathing

Expiration
• Expiration – Passive– Due to recoil of elastic lungs.– Less volume -> pressure within alveoli is just above
atmospheric pressure -> air leaves lungs.– Note: Residual volume of air is always left behind,
so alveoli do not collapse.

Lung Volumes
• Tidal volume (TV): in/out with quiet breath (500 ml)
• Total minute volume: tidal x breaths/min– 500 x 12 = 6 L/min

Lung Volumes
• Inspiratory reserve volume (IRV): extra (beyond TV) in with forced inspiration.
• Expiratory reserve volume (ERV): extra (beyond TV) out with forced expiration.
• Residual volume: always left in lungs, even with forced expiration.– Not measured with spirometer

Lung Capacities
• Vital capacity (VC): the most you can actually ever expire, with forced inspiration and expiration.
VC= IRV + TV + ERV
• Total lung capacity: VC plus residual volume

Pulmonary Function
Insert fig. 16.16

Muscles of Breathing
• Intercostal Muscles• Diaphragm

Regulation of Respiration
Where is the Respiratory Center Controlled?• Brainstem
– Medulla – Apeustic Center (pons)– Pneumotaxic center (pons)
• Stretch receptors– Hering-Breuer reflex
• Chemoreceptors

Oxyhemoglobin Dissociation Curve
Insert fig.16.34

AIRWAYS MANAGEMENT

ABC of Resuscitation• Airway: open the airway
• Breathing: provide positive-pressure ventilations
• Circulation: give chest compressions
• Defibrillation: shock VF/pulseless VT

Secondary Survey: ABCD
• Airway : provide advanced airway management
• Breathing : confirm tube placementcheck for adequate oxygenation and ventilation
• Circulation : obtain IV accessdetermine rhythmgive medications
• Differential Diagnosis : search for, find and treat reversible causes

Opening AirwayHead Tilt and Chin Lift Jaw Thrust
• One hand applies downward pressure to forehead and index and middle finger of the second hand lift at chin.
• Lifts tongue from posterior pharynx
• For unstable cervical spine• Place heels of hands on parieto-occipital area • Grasp angles of mandible with fingers, and displace jaw anteriorly.

PHARYNGEAL AIRWAY
Nasopharyngeal AirwayOropharyngeal Airway

1.Oropharyngeal Airway
• Size is measured from the corner of the mouth to the angle of the jaw
• Sizes range from 0-6• It holds the tongue away from the posterior
pharynx, but does not isolate the trachea

Technique
• Clear the mouth and pharynx
• Place the airway so that it is turned backward as it enters the mouth
• As airway approaches the posterior wall of the pharynx– rotate 180 degrees

2.Nasopharyngeal Airway
• Soft plastic or rubber tube that is designed to pass just inferior to the base of the tongue
• Passed through one of the nares and can be used in patients with an intact gag reflex
• CONTRAINDICATED in cases of suspected or possible basilar skull fracture
• Sizes range from 17-26 cm in length and 6-9 mm internal diameter
• Measured from tip of the nose to the corner of the patients ear

Technique
lubrication

• Airway trauma, particularly epistaxis• Incorrect size or placement will compromise
effectiveness• Exacerbate injury in base of skull fracture, with
NPA potentially displacing into the cranial vault• Can still stimulate a gag reflex in sensitive
patients, precipitating vomiting or aspiration
Complications

Ventilate the Patient
1. Mouth to Mouth / Mouth to Nose2. Mouth-to-Mask3. Bag-Mask

Types of Rescue Devices
• LMA• Combitube• King

Laryngoscopes
Macintosh Blade Miller Blade

Curved vs Straight Blade
Moderate head elevation (5–10 cm above the surgical table) and extension of the atlantooccipital joint place the patient in the desired sniffing position. The lower portion of the cervical spine is flexed by resting the head on a pillow.

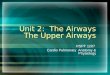
Combitube
E
Distal End
A
C H
G
D BF
Proximal End
A = esophageal obturator; ventilation into trachea through side openings = B C = tracheal tube; ventilation through open end if proximal end inserted in tracheaD = pharyngeal cuff; inflated through catheter = EF = esophageal cuff; inflated through catheter = GH = teeth marker; blindly insert Combitube until marker is at
level of teeth

Combi-tube
• This is a multi-lumen airway that works whether it is inserted into the esophagus or the trachea
• It either blocks the esophagus above and below the glottic opening or by directly ventilating the trachea
• Contraindicated in patients under 5 foot tall or those under 14 years old, in patients who have ingested caustic substances, patients with esophageal trauma or disease, and in patients with an intact gag reflex

Combi-tube continued

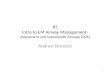
Laryngeal Mask Airway
• Sits over the glottic opening• Available in different sizes• Has a drain tube to aid in
gastric suctioning • With some versions an
endotracheal tube may be passed through to aid in intubation

LMA Positioning

Laryngeal Mask Airway

Laryngeal Mask Airway• Why
– As an alternative to the face mask for achieving and maintaining control of the airway.
– LMA™ airways are indicated for use in:• Known or unexpected difficult airways • Establishing an airway during resuscitation in the profoundly unconscious
patient with absent gag reflex• Known Issues
– Multiple sizes, based on weight, match correct syringe with device to inflate cuff
– Does not prevent aspiration– Improper placement (cuff folded over)– EDD is not recommended as a confirmation device with the LMA– Is NOT a medication route for Endotracheal drugs

King Airway

King Airway• Why
– Unconscious / unresponsive patients without gag reflex– Blind insertion technique– Alternative to E.T.T.
• Known Issues– Obtaining proper seal / placement– Is NOT a medication route for Endotracheal drugs– Multiple sizes, based on height, also multiple cuff volumes– Contraindications
• Responsive patients with an intact gag reflex.• Patients with known esophageal disease.• Patients who have ingested caustic substances.