Embed Size (px)
Citation preview

AIR POLLUTION AND BIRTH WEIGHT IN NORTHERN NEVADA, 1991–1999
Lei Chen
Department of Nutrition and Environmental Sciences and HealthGraduate Program, University of Nevada, Reno, Nevada, USA
Wei Yang
Bureau of Health Planning and Statistics, Nevada State HealthDivision, Carson City, Nevada, USA
Brian L. Jennison
Lane Regional Air Pollution Authority, Springfield, Oregon, USA
Andy Goodrich
Air Quality Management Division, Washoe County District HealthDepartment, Reno, Nevada, USA
Stanley T. Omaye
Department of Nutrition and Environmental Sciences and HealthGraduate Program, University of Nevada, Reno, Nevada, USA
This study examined the association between particulate matter £ 10 µm in aerodynamicsize ( PM10) , carbon monoxide (CO) , and ozone (O3) , and birth weight in WashoeCounty, NV, from 1991 through 1999. In total, 39,338 single births were included in thisstudy. The mean birth weight was 3383 ± 460 g and prevalence of low birth weight(LBW) was 2.46% for single births with a gestational age of 37–44 wk. After controllingfor cofactors including infant sex, maternal residential city, education, medical risk fac-tors, active tobacco use, drug use, alcohol use, prenatal care, mother’s age, race andethnicity of mothers, and weight gain of mothers, we found PM10 exposure in the thirdtrimester of pregnancy to be a significant predictor of birth weight of newborns. A 10-µg/m3 increase in the 24-h PM10 level in the third trimester of pregnancy can be associatedwith a birth-weight reduction of 11 g ( 95% CI: 2.3–19.8 g) using multiple linear re-gression; however, PM10 was not found to be related with the risk of LBW from logisticregression. CO and O3 were not found to be associated with birth weight or risk of LBWof newborns by the same modeling procedure. The results suggest PM10 could be a riskfactor associated with birth-weight reduction of newborns in urban northern Nevada;however, the current level of PM10 is not a risk factor to increase the chance ofLBW newborns.
141
Inhalation Toxicology, 14:141–157, 2002Copyright © 2002 Taylor & Francis0895–8378/02 $12.00 + .00
Received 13 June 2001; sent for revision 8 July 2001; revision received 3 September 2001;accepted 5 September 2001.
Address correspondence to Stanley T. Omaye, PhD, Department of Nutrition, Mail Stop 142,University of Nevada, Reno, NV 89557-0132, USA. E-mail: [email protected]
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

Birth weight is an important variable in relationship to perinatal out-come (Falkner, 1986). It represents an endpoint of intrauterine growth,which depends on maternal, placental, and fetal factors as well as on asequence of constitutional and environmental influences. Low birth weight(LBW) is a weight of less than 2500 g at birth. In both developed and devel-oping countries, LBW is the most important predictor for neonatal mortalityand is a significant determinant of postneonatal mortality and morbidity(McCormick, 1985; Falkner, 1986).
Until recently (Wang et al., 1997; Bobak & Leon, 1999; Bobak, 2000;Ritz & Yu, 1999; Dejmek et al., 1999; Rogers et al., 2000; Dolk et al.,2000), very few epidemiological studies regarding the association be-tween air pollution and LBW were found in the literature. A significantexposure-response relationship between maternal exposures to sulfur di-oxide (SO2) and total suspended particles (TSP) during the third trimesterof pregnancy and infant birth weight was found. TSP and SO2, or a morecomplex pollution mixture associated with these pollutants, may contributeto an excess risk of low birth weight in the Beijing population (Wang etal., 1997). In the Czech Republic, TSP, SO2, and oxides of nitrogen (NOx)were associated with LBW of newborns separately (Bobak, 1999). Exposureto higher levels of ambient CO (>5.5 ppm for 3-mo average) during thelast trimester was associated with a significantly increased risk for LBWafter adjustment for potential confounders in the Los Angeles area (Ritz &Yu, 1999).
Washoe County is located in northwestern Nevada at approximately4400 ft above mean sea level. The county is bordered by California on thewest and Oregon to the north, encompasses a land area of 6608 squaremiles, and in 1999 had a population of 323, 670, most of whom live inthe Reno–Sparks urban area. The community is located in a broad valleysurrounded by mountains, which restrict the dispersion of locally pro-duced pollutant emissions, especially during frequent wintertime atmos-pheric inversions. Currently, Washoe County is classified as a moderatenonattainment area for particulate matter 10 µm and smaller in aero-dynamic diameter (PM10) and for carbon monoxide (CO). Although theCounty is in attainment of the federal ozone (O3) standard, O3 levels arefrequently elevated in the warmer months. Positive associations between1-h maximum ozone concentration and emergency room (ER) visits forasthma as well as between ambient carbon monoxide levels and cardio-vascular disease hospitalization have been reported (Yang et al., 1997,1998). In recent studies, ambient PM10 was found to be a statisticall ysignificant predictor for daily hospital admissions for chronic obstructivepulmonary disease (COPD) (Chen et al., 2000a, 2001), and O3 and COwere found to be the statistically significant predictors for daily elemen-tary school absenteeism (Chen et al., 2000b). The objective of this studywas to examine whether maternal exposure to air pollution during preg-nancy would be associated with the risk of LBW of the newborn after con-
142 L. CHEN ET AL.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

trolling for other risk factors. This study was conducted in an area with ahigh altitude, dry and cold winters, and low levels of SO2 and NO2.
MATERIALS AND METHODS
Birth Data
The birth data were collected from the Bureau of Health Planning andVital Statistics, Nevada State Health Division. All pregnant women whoresided in Washoe County and delivered a single live birth in WashoeCounty from 1991 through 1999 were included in this study. In total,39,338 births were included. The database of vital statistics at the NevadaState Health Division recorded characteristic s of all live births and in-cluded maternal and paternal information. The characteristics of all livebirths include the birth date, birthplace, infant sex, birth weight, abnor-mal conditions of newborns, and congenital anomalies of newborns. Therecorded maternal information include the mother’s age, estimated weeksof gestation, weight gain in the pregnancy, race and ethnicity, residentialplace, education, marital status, prenatal care, obstetric procedures, com-plications of labor/delivery, and method of delivery. Risk factors includedtobacco, drug, or alcohol use during pregnancy, and other medical riskfactors such as anemia, chronic diseases, uterine bleeding, etc. Paternalinformation included the father’s age, race and ethnicity, and education.We discarded four cases because of missing birth weight, 2931 casesbecause of a gestation less than 37 wk, and 98 cases because of a gesta-tion greater than 44 wk, which left 36,305 cases total. We also excludedthose cases recorded with “unknown” for those important confoundingfactors such as mother’s age, residential city, education, weight gain dur-ing the pregnancy, prenatal visits, race and ethnicity of mother, activetobacco, drug, or alcohol use, and medical risk factors. Thus, in total,33,859 cases were included in the final statistical analyses.
Air-Monitoring Data
Air-monitoring data from 1990 through 1999 were obtained from theWashoe County District Health Department Air Quality ManagementDivision’s air-monitoring stations in Washoe County (Galletti, LemmonValley, Reno, South Reno, Incline Village, Sun Valley, and Sparks). Con-tinuous hourly values for O3 and CO were available from six sites (Reno,South Reno, Incline Village, Lemmon Valley, Galletti, and Sparks). Similardata for PM10 levels were available from four sites (Reno, Sun Valley,Galletti, and Sparks). All monitoring sites and instruments used in thisstudy are maintained according to U.S. EPA standard methods (40 Codeof Federal Regulations Part 58, Appendix E), and the data are consideredrepresentative of air pollution levels in Washoe County. Different scaleswere utilized for each pollutant; for CO and O3, 8-h values (in ppm for CO
AIR POLLUTION AND BIRTH WEIGHT 143
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

and in ppb for O3) were calculated and used to represent the CO or O3
level of that day. Calculations of the 8-h average for CO and O3 are basedon U.S. EPA standard methods (40 Code of Federal Regulations Part 50,Appendix I). For PM10, the 24-h average concentration (µg/m
3) was used.
Maternal Exposure Estimates
According to the available air-monitoring database, we made anassumption that the ambient air pollution level was reasonably indicativeof personal exposure level. Considering that pregnancy is a long-termprocess, the effects of air pollution may be chronic and cumulative ratherthan acute. Thus, we calculated the average maternal exposure to threepollutants of interest, that is, PM10, CO, and O3, for each trimester, basedon the last recorded menstrual date of the mother and birth date for eachcase.
Statistical Analyses
Before we performed any statistical analyses, we addressed the follow-ing questions:
1. Whether air pollution could be associated with birth weight reduction.2. Whether air pollution could be associated with risk of LBW (<2500 g).3. Which endpoint is more sensitive, birth weight or risk of low birth
weight?4. If air pollution is associated with birth outcomes, which trimester will be
the greatest risk period for maternal exposure to air pollution during thepregnancy to be related with adverse birth outcomes, the first, second orthird?
Besides the three air pollutants of interest for our study, other factorscould impact birth weight and risk of LBW. These factors included infantsex, maternal residential city, education, medical risk factors, tobacco,alcohol, and drug use, prenatal visits, marital status, mother’s age, raceand ethnicity of mother and father, weight gain of mother, maternal occu-pation, and household income. Several steps of analyses were performed:
1. We first calculated the mean birth weight and percentage of LBW basedon each of the listed confounding variables. Considering possible timetrends of birth, we also calculated the mean birth weight and percent-age of LBW for each year and each month in the study period.
2. We assessed the differences of mean birth weight among the differenttreatments for each confounding variable using one-way analysis of vari-ance (ANOVA).
3. We utilized multiple linear regression modeling to build up a back-ground model in which we put those significant confounding variablesin ANOVA and time indicators.
144 L. CHEN ET AL.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

4. After the background model was finalized, we added the air-pollutantvariables separately and jointly into the model to examine the effectsof air pollutants on birth weight quantitatively, and to determine whichtrimester exposure is most sensitive to birth weight changes.
5. We finally created a dichotomous variable for birth weight, assigningnormal birth weight ( ³ 2500 g) as 0 and LBW (<2500 g) as 1.
Multiple logistic regression was used to examine the risk of having LBWnewborns after maternal exposure to elevated air pollution levels duringpregnancy. Multiple logistic regression is a regression model dealing with abinary response variable that has only two qualitative outcomes, for exam-ple, yes versus no, disease versus no disease, etc. In this case, the two out-comes of the response variable are LBW versus normal birth weight. Whenthe response variable is binary, the shape of the response function is curvi-linear rather than linear. The equation to describe the relationship betweenthe response variable and indicator or predictor variables is as follows:
E(Y) = 1/[1 + e –( b 0 + b 1X1 + b 2X2 + b 3X3 + . . . + b nXn)]
where E(Y) represents the probabilities that the response variable is 1, e =2.718, b 0 is a constant, b 1, . . ., b n represent parameter estimates for vari-ables X1, . . ., Xn, and X1 . . ., Xn represent different indicator or predictorvariables. If we assume E(Y) = P, this equation rewritten as the followingequation by logit transformation:
log[P/(1 – P] = b 0 + b 1X1 + b 2X2 + b 3X3 + . . . + b nXn
where P/(1 – P) is called the odds, and the odds ratio (OR) = eestimate . Thevalue of [(OR – 1) × 100%] shows the percentage increase for every one-unit increase in X. The OR can be automatically calculated by many sta-tistical analysis software packages. Details of the logistic regression modelhave been extensively discussed (Hosmer & Lemeshow, 2000).
The marital status of mothers, race and ethnicity of fathers, maternaloccupation, and household income are important variables to be relatedwith birth weight and LBW from the preliminary analyses; however,15,440 cases out of the 33,859 births had missing marital status informa-tion, 6990 cases out of 33,859 births were recorded “unknown” for raceand ethnicity of fathers, and the data on maternal occupation and house-hold income were not available from the current database; therefore, wedidn’t include these variables in the final models. The statistical analyseswere performed by the statistical package SPSS 10.0.
RESULTS
Ambient air pollution levels were generally low throughout the studyperiod from 1991 to 1999 (Table 1). The average 24-h PM10 level was 31.53
AIR POLLUTION AND BIRTH WEIGHT 145
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

µg/m3 (± 22.32 µg/m3), the average 8-h CO level was 0.98 ppm (± 0.55ppm), and the average 8-h O3 level was 27.23 ppb (± 10.62 ppb). Thedistribution for 10th, 25th, 50th, 75th, and 90th percentages is shown inTable 1. The days for which we were missing values of pollutant levelswere 65, 3, and 2 for 24-h PM10, 8-h CO, and 8-h O3, respectively.
Table 2 presents the average of exposure levels of all live births ineach trimester and the whole period of pregnancy. In total, 39,338 birthswere observed during the study period. The average exposure levels for24-h PM10, 8-h CO, and 8-h O3 in each trimester and the entire period ofpregnancy were 31–32 µg/m3, 0.97–1 ppm, and 27–28 ppb, respectively.
A summary of birth weight and percentage of LBW for all single birthswith a gestational age of 37–44 wk for different study variables is given inTable 3. In total, 36,305 cases were included. The differences in mean birthweight and percentage of LBW were tested and observed among study vari-
146 L. CHEN ET AL.
TABLE 1. Summary of daily air pollution levels from 1991 to 1999
PercentilesValid Missing __________________________
Pollutant Mean (range) SD days days 10th 25th 50th 75th 90th
24-h PM10 31.53 (0.97–157.32) 22.32 3500 65 9.95 16.80 26.30 39.35 58.92(µg/m3)
8-h CO 0.98 (0.25–4.87) 0.55 3562 3 0.52 0.62 0.80 1.15 1.69(ppm)
8-h Ozone 27.23 (2.76 – 62.44) 10.62 3563 2 13.07 19.39 28.22 35.81 41.58(ppb)
TABLE 2. Summary of average air pollution levels in each trimester and whole pregnancy for all livesingleton births from 1991 to 1999
ValidPollutant Trimestera Mean SD numbers
24-h PM10 (µg/m3) 1 32.02 10.40 39,338
2 31.88 10.50 39,3383 31.36 10.16 39,338Whole 31.60 5.28 39,338
8-h CO (ppm) 1 1.00 0.34 39,3382 0.99 0.35 39,3383 0.97 0.34 39,338Whole 0.98 0.16 39,338
8-h Ozone (ppb) 1 27.51 7.58 39,3382 27.67 7.77 39,3383 28.07 7.66 39,338Whole 27.75 3.14 39,338
a1, First trimester; 2, second trimester; 3, third trimester; whole, whole pregnancy.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

AIR POLLUTION AND BIRTH WEIGHT 147
TABLE 3. Summary of birth weights for different study variables
Number Number PercentVariables of births Mean SD of LBW of LBW
Total 36,305 3383 460 893 2.46
Infant sexMale 18,465 3440 467 390 2.11Female 17,840 3324 445 503 2.82
Maternal residential cityReno 22,616 3371 459 605 2.68Sparks 8196 3398 465 178 2.17Others 5493 3409 452 110 2.00
Maternal education£ 6 yr 2233 3366 458 52 2.33>6–12 yr 20,497 3356 459 548 2.67>12–<16 yr 7020 3424 464 162 2.31³ 16 yr 6247 3433 448 116 1.86
Maternal medical risk factorsYes 10,601 3370 482 330 3.11No 24,117 3389 450 534 2.21
Maternal drug use during pregnancyYes 9352 3374 462 239 2.56No 26,673 3387 458 643 2.41
Maternal active tobacco use during pregnancyYes 5505 3232 460 275 5.00No 30,577 3410 454 609 1.99
Maternal alcohol use during pregnancyYes 715 3264 469 32 4.48No 35,285 3386 459 847 2.40
The trimester begins prenatal visit1 30,414 3393 458 709 2.33>1 5313 3335 465 160 3.01
Marital statusYes 14,296 3405 461 319 2.23No 6544 3331 457 208 3.18
Total prenatal visits£ 8 4806 3292 464 187 3.89>8–16 26,674 3397 454 571 2.14>16 4216 3407 475 118 2.80
Mother’s age group (yr)<20 4270 3303 440 128 3.0020–24 9418 3359 445 222 2.3625–29 10,488 3398 457 244 2.3330–34 7949 3421 468 184 2.3135–39 3465 3420 486 94 2.71³ 40 715 3358 497 21 2.94
Race and ethnicity of motherWhite 23,672 3405 461 547 2.31Black 804 3244 475 41 5.10
(Table continues on next page)
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

148 L. CHEN ET AL.
TABLE 3. Summary of birth weights for different study variables (continued)
Number Number PercentVariables of births Mean SD of LBW of LBW
Race and ethnicity of mother (continued)Native 748 3466 483 15 2.01Asian 1973 3272 458 78 3.95Hispanic 8984 3355 445 208 2.32
Race and ethnicity of fatherWhite 19,386 3426 455 367 1.89Black 755 3294 504 31 4.11Native 433 3468 479 8 1.85Asian 1522 3259 460 63 4.14Hispanic 7178 3363 451 168 2.34
Weight gain of mothers (lb)£ 25 9674 3281 450 356 3.68>25–32 8171 3360 435 194 2.37>32–40 8176 3437 453 141 1.72>40 7838 3486 474 136 1.74
Year of birth1991 3889 3387 462 95 2.441992 3842 3389 461 93 2.421993 3828 3374 450 92 2.401994 3934 3388 457 86 2.191995 4145 3389 469 105 2.531996 4195 3385 458 108 2.571997 4162 3383 464 101 2.431998 4190 3365 461 126 3.011999 4120 3386 454 87 2.11
Month of birthJanuary 2786 3368 462 68 2.44February 2752 3392 449 67 2.43March 3095 3383 462 63 2.04April 3022 3377 471 93 3.08May 3166 3399 459 67 2.12June 3151 3389 454 66 2.09July 3252 3381 466 76 2.34August 3116 3378 455 77 2.47September 3064 3374 465 91 2.97October 2941 3376 459 77 2.62November 2931 3381 451 69 2.35December 3029 3396 459 79 2.61
Exposure to PM10 at the third trimester (µg/m3)<19.72 3629 3390 466 82 2.2619.72–44.74 29,045 3382 459 729 2.51>44.74 3631 3379 455 80 2.21
Exposure to CO at the third trimester (ppm)<0.62 3622 3377 452 80 2.210.62–1.42 29,059 3384 462 733 2.52>1.42 3624 3381 450 80 2.21
Exposure to ozone at the third trimester (ppb)<17.93 3623 3375 452 86 2.2117.93–37.65 29,052 3384 461 733 2.52>37.65 3630 3381 453 74 2.04
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

ables including infant sex, maternal residential city, maternal education,maternal medical risk factors, maternal active tobacco, drug, and/or alco-hol use during pregnancy, the trimester during which prenatal visit begins,marital status, total prenatal visits, mother’s age group, race and ethnicity ofmothers and fathers, and weight gain of mothers in pregnancy. The differ-ences in birth weight and percentage of LBW for the variables year of birth,month of birth, and different exposure-level groups were tested and no dif-ferences were found.
Multiple linear regression analysis of birth weight for a single-pollutantmodel, two-pollutant model, and three-pollutant model are presented inTable 4 and Table 5. In Table 4, continuous air-pollutant variables were usedin the model. The estimated coefficients and standard errors from a crudemodel (a model with air-pollutant variables and gestational age only) and anadjusted model (a model with air-pollutant variables and other cofactors) fordifferent model specification and for different trimesters are shown in Table4. Significant terms are indicated in this table. Exposure to PM10 in the thirdtrimester of pregnancy was found to be a significant predictor of birthweight. This association remains consistent in different model specifications .Based on the estimated coefficient and standard error from the three-pollu-tant model, birth weight will be reduced 11 g (95% CI: 2.3–19.8 g) for every10-µg/m3 increase of 24-h PM10 in the third trimester of pregnancy. CO andO3 were found not to be related to birth weight. When we used categoricalpollutant variables in the multiple linear regression model (Table 5), PM10
remained statistically significant in the one-pollutant and two-pollutantmodels, and the p value for PM10 was less than the borderline (.1) of statisti -cal significance in the three-pollutant model. In the mean time, CO and O3
showed no statistically significant correlation with birth weight.To examine whether air pollution was associated with risk of LBW in the
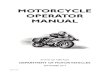
newborns, multiple logistic regression was performed, and the results arepresented in Table 6 and Figure 1. The confounding factors of sex of infant,maternal tobacco use in pregnancy, mother’s residential city, maternal med-ical risk factors, mother’s age group, race and ethnicity of mother, mother’seducation, gestational age, and weight gain of mother were found to bethe significant risk factors of LBW. PM10, CO, and O3, were not found to beassociated with risk of LBW.
DISCUSSION
The present study examined the association between three air pollutants,PM10, CO, and O3, and birth weight and LBW of newborns in WashoeCounty, NV, from 1991 through 1999. In total, 39,338 births were includedin this study. We found that infant sex, maternal residential city, education,medical risk factors, active tobacco smoking, drug, and alcohol use, the tri-mester during which prenatal visits began, total prenatal visits, mother’s age,race and ethnicity of mother, and weight gain of mother were significant fac-tors associated with birth weight and risk of LBW. After controlling for thesecofactors, we found PM10 exposure in the third trimester of pregnancy to be
AIR POLLUTION AND BIRTH WEIGHT 149
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

150 L. CHEN ET AL.
TABLE 4. Multiple linear regression analysis of birth weight for different pollutant models usingcontinuous pollutant variables
Crude modelc Adjusted modeld
Model ______________ _____________typea Pollutant Trimesterb b SE b SE
One PM10 1 –0.186 0.225 –0.082 0.2212 0.045 0.223 –0.020 0.2213 –0.509 0.231f –0.395 0.227g
Whole –0.823 0.459g –0.726 0.483
One CO 1 –3.702 6.846 –1.020 6.6822 2.686 6.709 –0.072 6.5803 –8.381 6.923 –3.953 6.763Whole –13.792 14.577 –8.280 14.930
One Ozone 1 0.329 0.310 0.234 0.3012 –0.366 0.302 –0.194 0.2943 0.224 0.308 0.077 0.299Whole 0.319 0.749 0.209 0.744
Two CO and PM10 3CO 18.573 13.680 23.624 13.241PM10 –1.044 0.457f –1.078 0.445 f
Two Ozone and PM10 3Ozone –0.876 0.512g –0.938 0.497g
PM10 –1.035 0.385e –0.966 0.378e
Two Ozone and CO 3Ozone –0.705 0.757 –0.503 0.737CO –22.868 17.032 –14.372 16.681
Three PM10 3 –1.070 0.458f –1.102 0.446e
CO 3 2.817 20.269 11.373 19.664Ozone 3 –0.798 0.758 –0.622 0.738
Three PM10 Whole –1.413 0.733f –1.332 0.738g
CO Whole –10.539 29.983 –1.141 29.462Ozone Whole –1.851 1.496 –1.337 1.478
Note. b , Estimated coefficient; SE, estimated standard error.aModel type: one, single-pollutant model; two, two-pollutant model; three, three-pollutant model.bTrimester: 1, first; 2, second; 3, third; whole, whole pregnancy.cCrude model: model with air-pollutant variables controlled with gestational age (wk) only.dAdjusted model: model with air-pollutant variables controlled with confounding variables includ-
ing gestational age, infant sex, maternal residential city, education, medical risk factors, active tobac-co use, drug use, alcohol use, the trimester begins prenatal visits, total prenatal visits, mother’s age,race and ethnicity of mother, and weight gain of mother.
ep £ .01, highly statistically significant.fp £ .05, statistically significant.g.05< p £ .1, the borderline of statistical significance.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

a significant predictor of birth weight of newborns. A 10-µg/m3 increase inthe 24-h PM10 level in the third trimester of pregnancy can be associatedwith a birth-weight reduction of 11 g (95% CI: 2.3–19.8 g) using multiplelinear regression; however, PM10 was not found to be related with the riskof LBW from logistic regression. CO and O3 were not found to be associ-ated with birth weight or risk of LBW of newborns by the same modelingprocedure. Thus, PM10 could be a risk factor associated with birth-weightreduction of newborns in urban northern Nevada; however, PM10 is not arisk factor contributing to LBW.
The assessment of possible association between air pollution and birthweight has been brought to the forefront by recent air pollution epidemio-logical studies, although the literature on this subject is very limited. Thefirst well-defined cohort study was conducted by Wang et al. (1997) in
AIR POLLUTION AND BIRTH WEIGHT 151
TABLE 5. Multiple linear regression analysis of effects of third trimester exposure on birth weight fordifferent pollutant models using categorical pollutant variables
Adjusted modelc
Model ________________________typea Pollutantb b SE
One PM10 –10.243 5.235d
One CO –2.885 5.134
One Ozone 6.466 5.164
Two PM10 –11.883 6.108d
CO 3.120 5.990
Two PM10 –9.144 5.860Ozone 2.413 5.780
Two CO 1.846 6.570Ozone 7.625 6.609
Three PM10 –10.937 6.222e
CO 5.973 6.977Ozone 5.368 6.732
Note. b , estimated coefficient; SE, estimated standard error.aModel type: one, one-pollutant model; two, two-pollutant model; three, three-pollutant model.bPollutant: air pollution levels were categorized into three different levels. Low level: <10th per-
centiles; medium level: 10–90th percentiles; high levels: >90th percentiles. For PM10 (in µg/m3): lowlevel: <19.72; medium level: 19.72–44.74; high level: >44.74. For CO (in ppm): low level: <0.62;medium level: 0.62–1.42; high level: >1.42. For ozone (in ppb): low level: <17.93; medium level:17.93–37.65; high level: >37.65.
cAdjusted model: a model with air pollutant variables controlled with confounding variablesincluding gestational age, infant sex, maternal residential city, education, medical risk factors, activetobacco use, drug use, alcohol use, the trimester begins prenatal visits, total prenatal visits, mother’sage, race and ethnicity of mother, and weight gain of mother.
dp value £ .05, statistically significant.ep value <.1, the borderline of statistical significance.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

152 L. CHEN ET AL.
TABLE 6. Effects of maternal exposure to air pollution at the third trimester on risk of LBW bymultiple logistic regression
Adjusted modela___________________________________Variables Odds ratio (OR) 95% CI
Exposure to PM10 at the 3rd term (µg/m3) >44.74 1.105 0.714 – 1.709Level <19.72 as a reference 19.72–44.74 1.050 0.811–1.360
Exposure to CO at the 3rd term (ppm) >1.42 0.907 0.564–1.461Level <0.62 as a reference 0.62–1.42 1.026 0.765–1.377
Exposure to ozone at the 3rd term (ppb) >37.65 0.784 0.508–1.209Level <17.93 as a reference 17.93–37.65 1.059 0.773–1.452
Sex of infant Male vs. female 0.672 0.582–0.775b
Drug use Yes vs. no 0.872 0.741–1.028
Tobacco use Yes vs. no 2.661 2.239–3.163b
Alcohol use Yes vs. no 1.398 0.941–2.077
Mother’s residential city Sparks 0.819 0.684–0.979c
Reno as a reference Others 0.748 0.599–0.935c
Medical risk factors of mother No vs. yes 0.823 0.707–0.958c
Prenatal visits begin at the 1st term No vs. yes 1.022 0.834–1.251
Mother’s age group (yr)20–24 as a reference <20 1.275 1.007–1.613c
25–29 0.999 0.820–1.21530–34 0.991 0.800–1.22935–39 1.047 0.802–1.366³ 40 1.194 0.731–1.953
Race and ethnicity of mothers Black 1.856 1.305–2.642b
White as a reference Native 0.998 0.586–1.699Asian 2.065 1.590–2.680b
Hispanic 1.005 0.810–1.247Others 1.851 0.415–8.261
Mother’s education (yr) 0.966 0.936–0.998c
Gestational age (wk) 0.459 0.430–0.489b
Weight gain of mother (lb) 0.989 0.984–0.993b
Total prenatal visits 1.004 0.991–1.018
aAdjusted model: a model with air pollutant categorical variables controlled with confoundingvariables including gestational age, infant sex, maternal residential city, education, medical risk factors,active tobacco use, drug use, alcohol use, the trimester begins prenatal visits, total prenatal visits,mother’s age, race and ethnicity of mother, and weight gain of mother.
bp £ .01, highly statistically significant.cp £ .05, statistical significance.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

four districts of Beijing, the capital of China. They found that the adjustedodds ratio for low birth weight was 1.11 (95% CI, 1.06–1.16) for each 100-µg/m3 increase in SO2, and 1.10 (95% CI, 1.05–1.14) for each 100-µg/m3
increase in total suspended particulates (TSP). The estimated reduction inbirth weight was 7.3 g and 6.9 g for each 100-µg/m3 increase in SO2 andin TSP, respectively. Later studies (Bobak & Leon, 1999; Bobak, 2000) inthe Czech Republic reported that LBW was associated with SO2 and TSP.Their adjusted odds ratios of LBW were 1.20 (95% CI, 1.11–1.30) and1.15 (95% CI, 1.07–1.24) for a 50-µg/m3 increase in SO2 and TSP, respec-tively, in the first trimester. Another study done in the Czech Republic(Dejmek et al., 1999) found that PM10 and PM2.5 had an adverse impacton intrauterine growth retardation (IUGR) risk in a highly polluted area ofnorthern Bohemia (Teplice District). Adjusted odds ratios for IUGR relatedto ambient PM10 levels in the first gestational month increased along theconcentration intervals: medium 1.62 (95% CI, 1.07–2.46), high 2.64 (95%CI, 1.48–4.71). Odds ratios for PM2.5 were 1.26 (95% CI, 0.81–1.95) and2.11 (95% CI, 1.20–3.70), respectively. In Los Angeles, exposure to higherlevels of ambient CO (>5.5 ppm for 3-mo average) during the last trimesterwas associated with a significantly increased risk for LBW (odds ratio =
AIR POLLUTION AND BIRTH WEIGHT 153
FIGURE 1. Adjusted odds ratios of LBW and 95% confidence intervals for categorical air-pollutantexposures at the third trimester from logistic regression models after controlled all confounding fac-tors. Low level, <10th percentiles; medium level, 10–90th percentiles; high levels, >90th percentiles.For PM10 (in µg/m
3): low level, <19.72; medium level, 19.72–44.74; high level, >1.42. For ozone (inppb): low level, <17.93; medium level, 17.93–37.65; high level, >37.65.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

1.22; 95% CI, 1.03–1.44) after adjustment for potential confounders, in-cluding commuting habits in the monitoring area, sex of the child, levelof prenatal care, and age, ethnicity, and education of the mother (Ritz &Yu, 1999). The most recent related study (Bobak et al., 2001) examinedand analyzed the data from the British 1946 birth cohort. A strong associ-ation was found between birth weight and an air pollution index basedon coal consumption. Babies born in the most polluted areas were onaverage 87 g lighter than those born in the areas with the cleanest air;however, this study didn’t report the relationship between risk of LBW andthe air pollution index.
We found that ambient PM10 concentrations were positively significantlyassociated with a reduction in birth weight, consistent with other studies(Wang et al., 1997; Bobak, 2000; Bobak et al., 2001); however, we did notfind evidence to suggest that the current PM10 level is associated with risk ofLBW, inconsistent with studies in China (Wang et al., 1997) and the CzechRepublic (Bobak, 2000; Dejmek et al., 1999). Ambient CO was not found tobe related to birth weight of newborns in this study area and period, incon-sistent with results from a study from Los Angeles area (Ritz & Yu, 1999).Ambient O3 was not found to be related to birth weight of newborns. Theeffects of SO2 and NOx on birth weight was not examined because the levelsof SO2 and NOx were very low in the Reno area (Chow et al., 1989).
We examined the effects of PM10, CO, and O3, in this study. The re-sults remained consistent among different model specifications (Table 4).To prevent multicollinearity among continuous air pollutant variables inthe multipollutant models, we created categorical variables for all three airpollutants (Table 5), which successfully decreased the values of varianceinflation factors (VIF) of the model. VIF is a value used to judge whethermulticollinearity exists in a regression model. We used the third-trimesterexposure and full-term pregnancy exposure in the multipollutant models(Tables 4 and 5) because the single-pollutant model showed the exposurein the last trimester of gestation was more sensitive to birth weight changes.After we modified air pollutant from continuous variables into categoricalvariables, the significance level was decreased but still remained significantfor the single- and two-pollutant models and marginally significant in thethree-pollutant model (Table 5). The Durbin–Watson statistic is a value usedto check the serial correlation of the residuals from the model. Generallyspeaking, a Durbin–Watson value of <2 suggests serial correlation mightexist in the regression model (Chatterjee et al., 2000). The Durbin–Watsonstatistic from each model was checked and no serial correlation of residualswas found in all models.
Although early animal studies (Kavlock et al., 1980) found that expo-sure to ozone in the late gestation of pregnancy in rats led to some abnor-mal reproductive performances for neonates, as yet no human study hasbeen reported to examine the role of ambient ozone on birth outcomes.Our study is the first report to our knowledge that examines the effect of O3
154 L. CHEN ET AL.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

on birth weight and shows that current ozone level is not associated withbirth weight of newborns in northern Nevada area (Tables 4–6, Figure 1). Itis known that CO crosses the placental barrier and that the hemoglobin infetal blood has 10 times more affinity for binding CO than does adult hemo-globin (Ritz & Yu, 1999); however, our study did not find evidence to sup-port that CO levels are related to either birth weight or a risk factor for LBW(Tables 4–6, Figure 1). PM10 concentrations in the third trimester were re-lated to birth weight (Tables 4 and 5) but not associated with risk of LBW(Table 6, Figure 1). The possible mechanisms include:
1. The association between PM10 and hospital admissions or emer-gency room (ER) visits for respiratory illnesses is well established (Chen &Omaye, 2001b). Maternal illnesses due to respiratory infection are possi-ble, thus resulting in intrauterine infections. One of the known determi-nants of birth outcomes is intrauterine infection (Kramer, 1987).
2. Hematological change could be another possible mechanism. There wasa report (Peters et al., 1997) of increased plasma viscosity during an airpollution episode. The increased plasma viscosity could influence theblood perfusion of the placenta (Knottnerus et al., 1990). Therefore wecould speculate that air pollution may influence placental development.
3. Transplacental exposure to polycyclic aromatic hydrocarbons (PAHs)in PM10 may affect the fetal development. Perera and coauthors (1998)found a significant association of fetal LBW and head circumferenceof newborns with polycyclic aromatic hydrocarbons (PAH)–DNA adductlevels. PAHs are among the components of particulate matter (Dejmeket al., 1999).
4. In Western countries, birth weight is generally determined by factorsimpacting pregnancy after wk 28 of gestation (Kline et al., 1989). Ourstudy assessed all three trimesters, and the results confirmed that thethird trimester appeared to be more sensitive to those factors that canimpact birth weight than other two trimesters for effects of PM10.
The strengths of this study can be summarized as follows:
1. This was a population-based study with no biases due to sampling; thistype of data collection increased the reliability of this study.
2. The study subjects and air-monitoring data spanned from 1990 through1999. This allowed us to understand the health effects of the currentfairly low-level ambient air pollution concentrations in the northernNevada area.
3. This study successfully controlled for most individual confounding fac-tors while examining the effects of air pollutants on birth weight.
4. According to our knowledge, this is the first report to investigate theeffect of ambient O3 on birth weight of newborns, although we didn’tfind any associations between O3 and birth weight in northern Nevada.
AIR POLLUTION AND BIRTH WEIGHT 155
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

Limitations of this study were as follows. The father’s race and ethnicityare known to be related to birth weight (Table 3). The average birth weightsof newborns whose fathers are African-American and Asian are 3294 g and3259 g, which are 89 g and 124 g lower than the average birth weight(3383 g), respectively. This phenomenon might result from relatively poorprenatal care, poor access to health care services, and lower householdincome for African-Americans and overall smaller size for Asians (Kline etal., 1989). Unfortunately, 21% of cases were reported “unknown” for raceand ethnicity of the fathers; therefore, we did not include this variable inthe regression model. However, this reasonable exclusion should not affectthe overall results because race and ethnicity of fathers are very signifi-cantly correlated with race and ethnicity of mothers, and the race of ethnic-ity of mothers were included in the analysis. Marital status is another factorrelated to birth weight (Table 3). Single mothers have smaller babies thanmarried mothers (3331 g vs. 3405 g) and have greater prevalence of LBWbabies (3.18% vs. 2.23%); however, 46% of cases had no information formarital status. Therefore, this variable was not included in the model. Also,we made an assumption in this study that personal exposure to air pollu-tants was equal to ambient air pollution levels. The current birth databasewas not able to provide us information such as environmental tobacco ex-posure (ETS) and occupational exposures, although active smoking historywas available.
In conclusion, this study provides additional evidence to suggest thatexposure to elevated ambient PM10 pollution in the last trimester of preg-nancy may be associated with reduction of birth weight of newborns; how-ever, there was not enough evidence to be found that air pollution wasrelated with occurrences of LBW in northern Nevada. This issue deservesfurther investigation in different locations and populations.
REFERENCESBobak, M. 2000. Outdoor air pollution, low birth weight, and prematurity. Environ. Health Perspect.
108(2):173–176.Bobak, M., and Leon, D. A. 1999. Pregnancy outcomes and outdoor air pollution: An ecological
study in districts of the Czech Republic 1986–8. Occup. Environ. Med. 56:539–543.Bobak, M., Richards, M., and Wadsworth, M. 2001. Air pollution and birth weight in Britain in 1946.
Epidemiology 16:358–359.Chatterjee, S., Hadi, A. S., and Price, B. 2000. Regression analysis by example, 3rd ed. New York:
Wiley.Chen, L., and Omaye, S. T. 2001. Air pollution and health effects in northern Nevada. Rev. Environ.
Health 16:133–149.Chen, L., Yang, W., Jennison, B. L., and Omaye, S. T. 2000a. Air particulate pollution and hospital ad-
missions for chronic obstructive pulmonary disease in Reno, Nevada. Inhal. Toxicol. 12:101–118.Chen, L., Jennison, B. L., Yang, W., and Omaye, S. T. 2000b. Elementary school absenteeism and air
pollution. Inhal. Toxicol. 12:997–1016.Chen, L., Yang, W., Jennison, B. L., Goodrich, A., and Omaye, S. T. 2001. Using two different statistical
models to compare the associations between PM10 and hospital admissions for COPD. Toxicol.Methods 11(4):233–246.
156 L. CHEN ET AL.
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.

Chow, J. C., Watson, J. G., Egami, R. T., Frazier, C. A., and Lu, Z. 1989. The State of Nevada Air Pollu-tion Study (SNAPS). DRI Document 8086.5E. Prepared by Desert Research Institute, Reno, NV.
Dejmek, J., Selevan, S. G., Benes, I., Solansky, I., and Sram, R. J. 1999. Fetal growth and maternalexposure to particulate matter during pregnancy. Environ. Health Perspect. 107:475–480.
Dolk, H., Pattenden, S., Vrijheid, M., Thakrar, B., and Armstrong, B. 2000. Perinatal and infant mor-tality and low birth weight among residents near coke-works in Great Britain. Arch. Environ.Health 55:26–30.
Falkner, F. 1986. Volume 1 Developmental biology: Prenatal growth in human growth, 2nd ed. NewYork: Plenum Press.
Hosmer, D. W., and Lemeshow, S. 2000. Applied logistic regression. New York: Wiley.Kavlock, R., Meyer, E., and Grabowski, C. T. 1980. Studies on the developmental toxicity of ozone:
Postnatal effects. Toxicol. Lett. 5:3–9.Kline, J., Stein, Z., and Susser, M. 1989. Conception to birth. Epidemiology of prenatal development.
New York: Oxford University Press.Knottnerus, J. A., Delgado, L. R., Knipschild, P. G., Essed, G. G., and Smits, F. 1990. Haematologic
parameters and pregnancy outcome. A prospective cohort study in the third trimester. J. Clin.Epidemiol. 43:461–466.
Kramer, M. S. 1987. Intrauterine growth and gestational duration determinants. Pediatrics 80:502–511.
McCormick, M. C. 1985. The contribution of low birth weight to infant mortality and childhood mor-bidity. N. Engl. J. Med. 312(2):82–90.
Perera, F. P., Whyatt, R. M., Jedrychowski, W., Rauh, V., Manchester, D., Santella, R. M., andOttman, R. 1998. A study of the environmental polycyclic aromatic hydrocarbons on birth out-comes in Poland. Am. J. Epidemiol. 147:309–314.
Peters, A., Doering, A., Wichmann, H. E., and Koenig, W. 1997. Increased plasma viscosity duringan air pollution episode: A link to mortality? Lancet 349:1582–1587.
Ritz, B., and Yu, F. 1999. The effect of ambient carbon monoxide on low birth weight among chil-dren born in southern California between 1989 and 1993. Environ. Health Perspect. 107:17–25.
Rogers, J. F., Thompson, S. J., Addy, C. L., McKeown, R. E., Cowen, D. J., and Decoufle, P. 2000.Association of very low birth weight with exposures to environmental sulfur dioxide and totalsuspended particulates. Am. J. Epidemiol. 151:602–613.
Wang, X., Ding, H., Ryan, L., and Xu, X. 1997. Association between air pollution and low birthweight: A community-based study. Environ. Health Perspect. 105:514–520.
Yang, W., Jennison, B. J., and Omaye, S. T. 1997. Air pollution and asthma emergency room visits inReno, Nevada. Inhal. Toxicol. 9:15–29.
Yang, W., Jennison, B. J., and Omaye, S. T. 1998. Cardiovascular disease hospitalization and ambi-ent levels of carbon monoxide. J. Toxicol. Environ. Health. A 55:185–196.
AIR POLLUTION AND BIRTH WEIGHT 157
Inha
latio
n T
oxic
olog
y D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y B
row
n U
nive
rsity
on
10/2
9/14
For
pers
onal
use
onl
y.