Embed Size (px)
DESCRIPTION
New Approaches In Medication Management and Care Transition e-Prescribing and Remote Dispensing in Long Term Care. AHRQ Annual Conference September 27, 2007 Presenter – Michael Bordelon. Long Term Care Background. Reimbursement Model: Roughly 15% capitated Part A 58% Medicaid/Part D - PowerPoint PPT Presentation
Citation preview

New Approaches In Medication Management and Care Transition
e-Prescribing and Remote Dispensingin Long Term Care
AHRQ Annual ConferenceSeptember 27, 2007
Presenter – Michael Bordelon

Long Term Care Background Reimbursement Model:
Roughly 15% capitated Part A 58% Medicaid/Part D 27% Private Pay and Commercial Insurance
Typical Number of Beds: 90-120 Pharmacies are almost never co-located with LTC facilities Physicians per facility: 10-40 Nurse Practitioners per facility: 1-2 Nurses per facility: 50-80 Med passes per day: 4-7 Pharmacy trips to the facility: 2-3 Admissions per week: 1-10 Many facilities already manage their own orders in electronic
systems

Pharmacy
ConsultantPharmacist
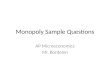
The Infamous LTC Prescribing Slide
Nursing
PhysicianDecide on
patient orderDecide on
patient order
Evaluate order, clarify if needed and file in Patient Record
Evaluate order, clarify if needed and file in Patient Record
Faxed order
Physician signs copy of the orderPhysician signs
copy of the order
Receive new orderReceive
new order
Check patient choice for pharmacy
Check patient choice for pharmacy
Process order and dispense[includes payor verification and formulary compliance]
Process order and dispense[includes payor verification and formulary compliance]
Resolve issues with order (clinical, payor, etc.)
Resolve issues with order (clinical, payor, etc.)
Clarify and update order with nursingClarify and update order with nursing
Clarify and update order with physicianClarify and update
order with physician
Med
Order Question(phone or fax)
Verbal orderSigned copy
of order
Patient MAR
Patient Allergies
Order Sheet
Order Update(Phone or fax)
Order Update(Phone or fax)
Receive updated order
Receive updated order
Patient MAR
Patient Allergies
Patient Orders
Patient Allergies
Patient Orders
MAR Update(optional)
Start
Physician writes order on Order Sheet
Physician writes order on Order Sheet
Written order
Update the MAR
Update the MAR
File Signed copy in Pt. Record
File Signed copy in Pt. Record
Notice updated Order Sheet, evaluate order and clarify if needed
Notice updated Order Sheet, evaluate order and clarify if needed
Patient RecordUpdated Order Sheet
Copy of order (mail, on-site)
Order Exception
Evaluate order, clarify if neededEvaluate order, clarify if needed
Receive and check medication (patient,
med, doc)
Receive and check medication (patient,
med, doc)
Write order on Physician Order Sheet
Write order on Physician Order Sheet
Write order on Physician Order Sheet and send
copy to physician
Write order on Physician Order Sheet and send
copy to physician
Administer and Chart
Administer and Chart
Manage on-hand medications
(Pt Meds, Stock and Emergency Kit)
Manage on-hand medications
(Pt Meds, Stock and Emergency Kit)
Med
Med
Resolve Discrepancy
Resolve Discrepancy
Drug Regimen Review or other Patient Status
Review
Drug Regimen Review or other Patient Status
Review
Resident Change in Condition;
New admission
Resident Change in Condition;
New admissionStart
Order (phone, fax, pickup by driver, auto-fax from SNF order
management application)
Follow pharmacy-specific procedure including after hours rules
Follow pharmacy-specific procedure including after hours rules
Resident Status(phone call, fax, on-site)

LTC Prescribing Nuances Three way communication between
Prescriber – Nurse – Pharmacy Most orders have no end date or
quantity Refill requests represent 80% of orders No concept of Renewals Need unique formulary and benefit
information Part A, Part D and Medicaid

e-Prescribing in Long Term Care
e-Prescribing is new to LTC
2006 CMS Pilot Study was first official standards based e-prescribing study in Long Term Care
There are less than 5 standards based e-Prescribing installations today

LTC e-Rx Pilot Study Abstract 2006 study focused on e-Rx standards most relevant to LTC
SCRIPT Formulary Benefits Electronic Prior Authorization
Other Capabilities Studied Facility Managed Electronic Orders Patient Safety Checks (DUR) Electronic Signature Automated Refill Requests
The study included two geographically diverse treatments facilities and two comparison facilities

Flow of Information
CPOE/EHR System(Achieve Matrix)
RxHUBSCRIPTSwitch
CPOE Client
Nursing Station
Browser HTTPS
PDPMed History
Formulary BenefitEligibility
Prior AuthorizationBrowser HTTPS
AchieveHostingServcies
RxHubHostingServices
FACILITYSYSTEMS
(BHS)
Pharmacy Billiing
Pharmacist DUR
PHARMACY TOOLS(Preferred Choice)
Browser HTTPS/ Citrix
Browser HTTPS/ Citrix
Dispensing System (RNA)
RxHUBFormularyBenefitsSwitch
PAYER COVERAGE
DATA
SCRIPT Web Service
Pharmacy Dispensing
System
X12 EDI
SCRIPT Web Service
NCPDP 5.1 E1/B1
PHYSICIAN TOOLS
RNA Refill Barcode Scanner
FTP
RNA eRxRequest Refill Scanner

e-Rx Findings - Facility Impacts Benefits
Facilities currently using electronic Physicians Orders will see modest change or disruption to current workflow
Ability to transmit orders directly to the pharmacy yielded benefits in reduced rework and callbacks
Management of Orders at the facility streamlines reconciliation processes
New Challenges Prescriber adoption is vital Integration with clinical systems (EHR) is critical Nurses do not effectively use patient safety (DUR) tools Even with Formulary Benefits data, managing complex Part D
health plans is an ongoing challenge Nursing staff now has to enter and manage data that the
pharmacy once managed Data entry errors can still happen

e-Rx Findings - Pharmacy Impacts Benefits
Demographics pre-populated on new admissions Straightforward new order processing Discontinued orders Readmissions streamlined Do not have to manage MARs and Order Sheets Refill requests streamlined
New challenges Combination & Tapered Orders – Need codified SIG
standard Transcription accuracy Timely transmission on admission orders Fax mode for controlled substances leads to process
inconsistencies

Standards Findings NCPDP SCRIPT Standard works with new
changes in Version 10.1 NCPDP Formulary Benefits V1.0 technically
works, but is dependent on greater prescriber adoption
Electronic Prior Authorization Technically works, but will require greater prescriber adoption
A Refill messaging standard is needed in LTC An Admission, Discharge, Transfer (ADT)
messaging standard is needed

What is Remote Dispensing?
Automated oral solid dispensing in healthcare settings, such as nursing homes and correctional facilities, that
have no onsite pharmacist
Remote dispensing can work hand in hand with e-Prescribing

Oral Solid Packaging
Remote Dispensing Packager
Medication Canister

Process Overview

Process – Dispense Data From Central Pharmacy System

On Site Strip Packaging

On Site Strip Packaging
•Daily Dispense•Med Pass/Resident Sort•Multi Dose Packing•PRN, New, Re-dispense

Process – Data Feedback Loop

Process – Inventory Monitoring

Process – Canister Fill at Pharmacy

Process – Canister Delivery

Value Proposition
Virtually eliminates drug waste
Significantly reduces delivery costs
Eliminates delay of first dose
Decreases administration time
Reduces medication errors
Eliminates the need for a refill process

Experience in early commercial pilots
High Adoption Rate with nursing staff On demand PRNs and quick access to meds for
new admissions are big wins Will save a typical nursing facility more than
$25K per year in Part A drug waste May save $150K per year per facility for Part D
drug waste savings Robust canister logistics is the key to success

Medication Reconciliationin
Long Term Care
AHRQ Annual ConferenceSeptember 27, 2007
Presenter – Michael Bordelon

Long Term Care Background Reimbursement Model:
Roughly 15% capitated Part A 58% Medicaid/Part D 27% Private Pay and Commercial Insurance
Typical Number of Beds: 90-120 Pharmacies are almost never co-located with LTC facilities Physicians per facility: 10-40 Nurse Practitioners per facility: 1-2 Nurses per facility: 50-80 Med passes per day: 4-7 Pharmacy trips to the facility: 2-3 Admissions per week: 1-10 Many facilities already manage their own orders in electronic
systems

Pharmacy
ConsultantPharmacist
The LTC Prescribing Slide
Nursing
PhysicianDecide on
patient orderDecide on
patient order
Evaluate order, clarify if needed and file in Patient Record
Evaluate order, clarify if needed and file in Patient Record
Faxed order
Physician signs copy of the orderPhysician signs
copy of the order
Receive new orderReceive
new order
Check patient choice for pharmacy
Check patient choice for pharmacy
Process order and dispense[includes payor verification and formulary compliance]
Process order and dispense[includes payor verification and formulary compliance]
Resolve issues with order (clinical, payor, etc.)
Resolve issues with order (clinical, payor, etc.)
Clarify and update order with nursingClarify and update order with nursing
Clarify and update order with physicianClarify and update
order with physician
Med
Order Question(phone or fax)
Verbal orderSigned copy
of order
Patient MAR
Patient Allergies
Order Sheet
Order Update(Phone or fax)
Order Update(Phone or fax)
Receive updated order
Receive updated order
Patient MAR
Patient Allergies
Patient Orders
Patient Allergies
Patient Orders
MAR Update(optional)
Start
Physician writes order on Order Sheet
Physician writes order on Order Sheet
Written order
Update the MAR
Update the MAR
File Signed copy in Pt. Record
File Signed copy in Pt. Record
Notice updated Order Sheet, evaluate order and clarify if needed
Notice updated Order Sheet, evaluate order and clarify if needed
Patient RecordUpdated Order Sheet
Copy of order (mail, on-site)
Order Exception
Evaluate order, clarify if neededEvaluate order, clarify if needed
Receive and check medication (patient,
med, doc)
Receive and check medication (patient,
med, doc)
Write order on Physician Order Sheet
Write order on Physician Order Sheet
Write order on Physician Order Sheet and send
copy to physician
Write order on Physician Order Sheet and send
copy to physician
Administer and Chart
Administer and Chart
Manage on-hand medications
(Pt Meds, Stock and Emergency Kit)
Manage on-hand medications
(Pt Meds, Stock and Emergency Kit)
Med
Med
Resolve Discrepancy
Resolve Discrepancy
Drug Regimen Review or other Patient Status
Review
Drug Regimen Review or other Patient Status
Review
Resident Change in Condition;
New admission
Resident Change in Condition;
New admissionStart
Order (phone, fax, pickup by driver, auto-fax from SNF order
management application)
Follow pharmacy-specific procedure including after hours rules
Follow pharmacy-specific procedure including after hours rules
Resident Status(phone call, fax, on-site)

Typical Admission in LTC
Most admissions in LTC are from a hospital setting
Most “residents” begin stay under Medicare Part A
Generally, discharge orders from the hospital are admission orders at the facility

Resident EntersNursing HomeFrom Hospital
with Discharge Orders
PharmacistManually Enters
Orders in PhIS withDUR Check
PharmacyFills Orders and
Delivers Medications
Pharmacy ProvidesPaper Based MARs
andOrder Sheets
Nurse FaxesDischarge Orders
to Pharmacy
Typical Order Management ProcessNew Admission

Resident EntersNursing HomeFrom Hospital
with Discharge Orders
PharmacistManually Enters
Orders in PhIS withDUR Check
PharmacyFills Orders and
Delivers Medications
Pharmacy ProvidesPaper Based MARs
andOrder Sheets
Nurse FaxesDischarge Orders
to Pharmacy
Typical Order Management ProcessNew Admission
RISK:Physicians
often do not review
admission orders in a timely way
RISK:Data entry
errorscan lead to
inconsistencies
RISK:Paper MARs and Order Sheets are
“Stale” almost
immediately

Nursing StaffManually Reviews
and UpdatesOrders on MARs
Physician Reviews,Modifies and Signs
Orders on Order Sheets
Nursing Staff FaxesHandwritten MAR
Updatesto Pharmacy
Pharmacy Sends Revised MAR
to Facility
Nurses PerformSecondary Review
of MAR andHandwrite Corrections
Typical Order Management ProcessDuring last 10 days of the month
Pharmacy DeliversFinal MARs
Before Start ofNew Month

Nursing StaffManually Reviews
and UpdatesOrders on MARs
Physician Reviews,Modifies and Signs
Orders on Order Sheets
Nursing Staff FaxesHandwritten MAR
Updatesto Pharmacy
Pharmacy Sends Revised MAR
to Facility
Nurses PerformSecondary Review
of MAR andHandwrite Corrections
Typical Order Management ProcessDuring last 10 days of the month
RISK:Is the Order
SheetUp to Date with
MAR? RISK:High Potential
for Transcription Error
RISK:New MAR May Be “Stale” due
to NewAdmits and
Order Changes
RISK:Very Time
Consuming and Often not
Performed with Rigor
RISK:Easy to Make
Mistakes WhenHandwriting
Changes to MAR
Pharmacy DeliversFinal MARs
Before Start ofNew Month
RISK:Paper MARs and Order Sheets are
“Stale” almost
immediately

Typical MAR Flowsheet
Blank Space To
Handwrite New Orders During The
Month

Medication Reconciliation withe-Prescribing Facility “owns” all orders Orders are managed in facility CPOE system MARs are printed from the CPOE system New orders are transmitted electronically to
pharmacy Discontinued and changed orders are
Transmitted electronically to pharmacyNote:
CPOE = Computerized Physician Order Entry

Resident EntersNursing HomeFrom Hospital
with Discharge Orders
Pharmacy ReceivesOrder Electronically
PharmacyFills Orders and
Delivers Medications
Physician Enters andSigns Orders in
Facility CPOE Systemwith DUR and Formulary
Checks
Facility PrintsMARs and Order Sheets
From CPOE System
Order Management with e-PrescribingNew Admission

Resident EntersNursing HomeFrom Hospital
with Discharge Orders
Pharmacy ReceivesOrder Electronically
PharmacyFills Orders and
Delivers Medications
Physician Enters andSigns Orders in
Facility CPOE Systemwith DUR and Formulary
Checks
Facility PrintsMARs and Order Sheets
From CPOE System
BENFIT:Physician Upfront Review
of Orders ande-Signatures
BENFIT:MARs and
Order Sheets are AlwaysUp to Date BENFIT:
Reduction InData Entry
Errors
Order Management with e-PrescribingNew Admission
BENFIT:Pharmacy Does Not
Manage MARs or Order Sheets

Nursing StaffNotified of Changes
andPrints MAR UpdatesFrom CPOE System
Physician Writes or DC'sOrders In Facility CPOE
System withe-Signature
Nursing Staff canPrint Entire Up to DateMAR and Order Sheet
at Any Time
Pharmacy ReceivesOrder Electronicallyand Resolves DUR
Issues
Order Management with e-PrescribingOngoing Processes

Nursing StaffNotified of Changes
andPrints MAR UpdatesFrom CPOE System
Physician Writes or DC'sOrders In Facility CPOE
System withe-Signature
Nursing Staff canPrint Entire Up to DateMAR and Order Sheet
at Any Time
Pharmacy ReceivesOrder Electronicallyand Resolves DUR
Issues
BENFIT:Reduction InData Entry
Errors
BENFIT:No
Handwritten Updates and MAR Always Up To Date
BENFIT:Pharmacy System
Always Up to Date
BENFIT:Eliminates Monthly ReviewBecause
Orders are Always Up to
Date
Order Management with e-PrescribingOngoing Processes

e-Prescribing in Long Term Care
e-Prescribing is new to LTC
2006 CMS Pilot Study was first official standards based e-prescribing study in Long Term Care
There are less than 5 standards based e-Prescribing installations today

LTC e-Rx Pilot Study Abstract 2006 study focused on e-Rx standards most relevant to LTC
SCRIPT Formulary Benefits Electronic Prior Authorization
Other Capabilities Studied Facility Managed Electronic Orders Patient Safety Checks (DUR) Electronic Signature Automated Refill Requests
The study included two geographically diverse treatments facilities and two comparison facilities

e-Rx Findings - Facility Impacts Benefits
Facilities currently using electronic Physicians Orders will see modest change or disruption to current workflow
Ability to transmit orders directly to the pharmacy yielded benefits in reduced rework and callbacks
Management of Orders at the facility streamlines reconciliation processes
New Challenges Prescriber adoption is vital Integration with clinical systems (EHR) is critical Nurses do not effectively use patient safety (DUR) tools Even with Formulary Benefits data, managing complex Part D
health plans is an ongoing challenge Nursing staff now has to enter and manage data that the
pharmacy once managed Data entry errors can still happen

e-Rx Findings - Pharmacy Impacts Benefits
Demographics pre-populated on new admissions Straightforward new order processing Discontinued orders Readmissions streamlined Do not have to manage MARs and Order Sheets Refill requests streamlined
New challenges Combination & Tapered Orders – Need codified SIG
standard Transcription accuracy Timely transmission on admission orders Fax mode for controlled substances leads to process
inconsistencies

Med Reconciliation Conclusions e-Prescribing forces facilities to take ownership of their
orders Once a facility manages their own orders, they
typically have up to date data for MARs and Order Sheets
e-Prescribing can significantly streamline processes and reduce reconciliation errors during new admissions from hospitals
e-Prescribing can reduce reconciliation errors between the nursing facility and the pharmacy
It is difficult to keep a facility managed CPOE system in sync with a pharmacy system without e-Prescribing