Embed Size (px)
Citation preview

11/1/2019
AUTISM AS A NEUROPSYCHIATRIC
DISORDER Ahmad Almai, MD
Child & Adolescent PsychiatryAramco Johns Hopkins Health Center
Dhahran, KSA
OBJECTIVES
Appreciate a developmental perspective of mental illness.
Expand a paradigm for thinking about pediatric brain development and subsequent psychopathology.
Agenda
Neuropsychiatric paradigm Normal brain development
Critical periods/ sensitive periods Experience expectant/dependent
Key Brain Regions pertinent for pediatric neuropsychiatry Basal ganglia Prefrontal Cortex Medial Temporal Lobe
Brain pathophysiology in selected psychiatric conditions Stress Depression Impulsivity
Challenges of Pediatric Psychiatry
Lack of a medical model archetype Historically difficult to do imaging studies in children DSM insufficient to comprehensively describe pediatric mental
illness Children are a moving target
Psychiatric illness is not static Maturation of the brain is key
General Principles of Brain Development
Brain development is activity dependent. Neurons grow first, and connect (synapse) later.
The brain is organized into primary cortex and association cortices—secondary, tertiary, etc. electrical activity at each step—sensory, motor, emotional,
cognitive—shapes the way that circuit consolidates. Sensory input “coded” and connected to other neurons that
add context, and allow higher order processing.
“Cells that fire together, wire together.” Unused synapses and circuits fade away, but the ones that
remain become more efficient.
Two types of brain growth
-Progressive Vast increases in synaptic density
Visual cortex up to 8 months of age Frontal cortex up to 12 months of age
Gray Matter Plateaus or Decreases neurons “multitask” and “cross-reference”, don’t
necessarily need “extra” neurons. White matter increases
Myelination allows more reliable and efficient conduction of electrical messages
-“Bursts” Development does not occur in a straight line. “3
steps forward, 2 steps back” Periods of “remodeling” with peaks at ages 3, 7,
11-12, and 15
١ ٢
٣ ٤
٥ ٦

11/1/2019
Brain Development and Maturation
White matter increases, gray matter decreases with age New neurons are created throughout life, especially granule
cells in the hippocampus-dentate gyrus Myelination pattern progresses from:
Inferior to superior Posterior to anterior
Especially in PFC from ages 5-17 Basal ganglia decrease with age.
ADHD and Tourette’s Syndrome early onset. Temporal lobe structures (amygdala and hippocampus)
increase with age. Depression and Schizophrenia later onset
Durston S, Hulsoff Pol H, Casey BJ et al. JAACAP 2001, 40(9):1012-1020.
Sensitive periods/Critical periods
Periods during which an experience (or its absence) has a marked impact on the neural organization underlying a particular skill or competence
Experience-expectant brain development:Certain species-typical experiences are necessary
in brain development. The brain expects to receive a certain kind of sensory input, e.g. light, patterned visual information, language, etc.
Experience-dependent brain development:Certain experiences lead to brain development and
contribute to the brain’s adaptability and enduring “plasticity”
Stress
Acute stressors trigger physiologic activation to ensure the survival of the organism, but to the temporary detriment of systems controlling growth, recuperation.
Chronic stress may inhibit neurogenesis, disruption of neuronal plasticity, and neurotoxicity.
Frequent activation of the stress response tilts the organism toward consuming resources without sufficient recovery, and increases the risk for physical and behavioral problems.
Gunnar M, Quevedo K. The Neurobiology of Stress and Development. Annu. Rev. Psychol. 2007. 58:11.1–11.29
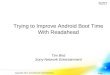
Communication & language
deficit
Social interaction
deficits
Repetitive & stereotyped behaviors
Immuneproblems
Sensorysensitivity
Autism
Neurotransmitters
Alterations in many neurotransmitter systems in autism
-Glutamate
-GABA
-Serotonin
-Catecholamines (norepinephrine, dopamine)
-Neuropeptides
Changes in glutamate and/or GABA could lead to alterations in excitation/inhibition
GABA- major inhibitory neurotransmitter -GAD (glutamic acid decarboxylase) is the rate-limiting enzyme in
GABA biosynthesis -Westerns on postmortem brain tissue (n=4-8 control; n=5 autism)
48 and 50% decrease in 65kDa, parietal lobe and cerebellum 61 and 51% decrease in GAD67 (Fatemi 2002)
-Possible deletions in genes encoding GABA receptors -Fewer GABA binding sites in hippocampus (Blatt 2001)
٧ ٨
٩ ١٠
١١ ١٢

11/1/2019
Serotonin
-Released by some populations of midbrain neurons
Project widely to other brain regions
-Involved in the regulation many processes Sleep, mood, body temperature, appetite
-Also implicated in early CNS development Cell proliferation Migration Differentiation of neural progenitors
-Genetic changes in serotonin transporters and biosynthetic enzymes have been shown (Nabi 2004)
-Increased serotonin in the blood platelets in autism (1961) -Altered brain synthesis of serotonin (Chugani 1997)
Serotonin- Developmental changes
Cortical decreases of AMT uptake (red areas) In three autistic children in (1B) the frontal cortex(left hemisphere), (1C) frontal and temporal cortices (left hemisphere), and (1D) frontal, parietal and temporal cortices (right hemisphere) are shown.
Neuropathology summary
-Increased in head size
-Increased brain volume
-Increased volume of specific brain regions (hippocampus)
-Increased packing densities in some regions
-Decreased dendritic complexity
-Decreased cell neuron numbers in cerebellum
-Altered laminar patterns in cortex
-Possible changes in white matter or myelination
Conclusion: Wide-ranging change that can be pretty subtle
Case Khaled is a 19-year-old young man with autism spectrum disorder Autism
spectrum disorder who first presented for evaluation and psychiatric management at age 12. His history of ASD is complicated by multi-domain developmental delays, ADHD, epilepsy, aggression, and self-injurious behaviors. He had been seen by previous practitioners following a number of medication trial failures.
At the time of presentation, Khaled was attending a full-time, specialized school for autistic children where he received a variety of services including speech therapy, occupational therapy, and behavioral therapy as well as developmentally appropriate academic services and art classes. He was being treated with escitalopram 15 mg daily, naltrexone 25 mg twice a day, and olanzapine 5 mg daily but continued to experience significant symptom breakthrough that put his and others’ safety at risk.
Neuropsychiatric Re-evaluation The data on self-injury in ASD is small; studies in SIB and ASD are often
limited by study design, sample size, and methodology. Self-injurious behavior (SIB) and aggression are two serious concerns in
autism that result in care-level escalation and hospitalization. Estimated rates of SIB in ASD range from 15% to 50% with one report as high as 74% reported in cohort of hospitalized individuals [1011].
Aggression can be seen in up to two-thirds of individuals with ASD.
Behavioral management for SIB in intellectually disabled individuals with ASD can take a number of forms. Commonly, behavioral management techniques follow Skinner’s operant conditioning model, where behavior is constituted of the physical behavior itself, environmental events preceding it, and then the subsequent outcomes [14].
A number of steps are involved in behavioral management namely, use of intervention strategies targeting antecedents, reinforcements, and extinction.
Preemptive management of antecedent factors can involve environmental enrichment, provision of alternative sensory experiences that are less dangerous or inappropriate, use of visual schedules and other techniques to facilitate ease of transitions, and careful management of demands to minimize escape-avoidance function of SIB.
Much can be said about reinforcing behaviors; but, in the case of Khaled, of particular importance is the reinforcing role of parental attention as well as the way SIB provided a form of control over his environment and possible escape from unwanted activities.
Non-contingent reinforcement, such as parental attention given frequently and not in response to SIB, can decrease the need to engage in SIB.].
١٣ ١٤
١٥ ١٦
١٧ ١٨

11/1/2019
Clinical Pearls
No medications are specifically approved for treatment of self-injurious behaviors in autism, and there are no treatments for the core symptoms of autism. At present, only two psychotropic medications have regulatory indications for the treatment of irritability associated with ASD, Risperidone and Aripiprazole. Significant efficacy and overall tolerability have been demonstrated in risperidone and aripiprazole for serious behavioral problems in ASD [16171819].
S.E : Tardive dyskinesia and metabolic, hormonal, cardiovascular. First-generation antipsychotics have a long history in the treatment of
hospitalized individuals with ASD or ID and SIB [20].
Haloperidol, Chlorpromazine, and Thioridazine: A small number of trials exist which show equivocal and inconsistent findings with [6]. Used less frequently extrapyramidal and tardive dyskinesia risks [21]. Better benefit has been reported in second-generation neuroleptics including small trials of clozapine and olanzapine [22,23,24,25].
One of two studies on risperidone showed separation from placebo for SIB in ASD [2627]. Aripiprazole has been explored for agitation and a range of behavioral disturbances in autism, but not SIB specifically [6]. Ziprasidone has also been explored with some benefit in a few, small trials for severe disruptive behavior in ASD [28].
Alpha-2 agonists shown some efficacy in irritability, attentional symptoms, sleep, impulsivity, hyperactivity, and overall severity of symptomatology in ASD [29].
Beta blockers, such as propranolol, have also been explored for disruptive behaviors including hypersexuality, self-injury, and aggression, and results appear promising, but data is limited [30].
Selective serotonin reuptake inhibitors(SSRI’s) are often used in the setting of self-injury and underlying psychiatric conditions, though data in ASD are mixed [6].
Data is limited, benefit in compulsive skin picking, and a trial in self-injury in Prader-Willi syndrome all showed benefits [63,23,33,43,45]. Paroxetine and fluvoxamine have also showed benefit in small trials [3637].
Clomipramine: One open trial and one small double-blinded placebo-controlled trial demonstrated benefit for SIB. use is limited by side effect burden [3839].
Buspirone : showed benefit in anxiety and irritability in ASD. Other trial; benefit for restrictive and repetitive behaviors as an adjunctive therapy [4041].
SIB; individual case reports [6].
Mood stabilizers and Antiepileptics: variable results for aggression, irritability, and self-injury in ASD.
Valproate: mixed results for management of these symptoms[3142]. Lamotrigine: No clear benefit. [43].
Oxcarbazepine, carbamazepine, gabapentin, and Topiramate:limited data, though positive case series[31].
Lithium: limited literature. Benefit in Phelan-McDermid disorder. ASD and co-morbid manic sx [4445].
Naltrexone: self-injurious behaviors in the setting of autism and other neurodevelopmental disabilities, possibly due to its impact on the endogenous opioid system. Studies show mixed efficacy [4647].
Memantine: Anti-glutamatergic NMDA receptor antagonist , some possible potential benefit [48].
N-acetylcysteine (NAC) N-acetylcysteine (NAC) , a glutamatergic modulator. Showed benefit in irritability. Other studies show equivocal effects (49, 50,51].
Baclofen: enantiomer, R-baclofen, a selective GABA-B
agonist, open-label study [52].
Electroconvulsive therapy(ECT): Effecive in severe, treatment-
refractory SIB in ASD developmental conditions, particularly
catatonic features [535455].
Clinical Pearls:
1.Psychotherapeutic behavioral management is a crucial component in the treatment of self-injurious behavior and aggression in autism spectrum disorder and intellectual disability.
2.There are no psychotropic medications that are formally approved in the treatment of core symptoms of ASD; however, aripiprazole and risperidone are indicated for the treatment of agitation and dysregulation. Many other medications are often considered for off-label use when behaviors are dangerous or severe but should be used judiciously in light of limited data and side effect profiles in individuals with ASD.
١٩ ٢٠
٢١ ٢٢
٢٣ ٢٤

11/1/2019
3. Behavioral challenges in ASD and ID can wax and wane based on medical events, life circumstances, or even without an externally obvious, causal trigger. Close clinical attention and hand-in-hand collaboration among family, other caregivers, teachers, and the treatment team as well as the patients themselves are crucial to providing ongoing, carefully tailored management of symptoms.
Summary
Mental illness in adults may have roots that are placed long before age 18.
Sensitive periods of brain development may predict mental illness: Disruption in early maturing structures (striatum) may
lead to externalizing disorders. Disruption in late maturing structures (PFC) may lead
to internalizing disorders. A developmental approach to mental illness is
critical for comprehensive understanding of pathophysiology.
www.amazon.com
References
Als H, Duffy FH, McAnulty GB et al. Early Experience Alters Brain Function and Structure. Pediatrics 2004; 113; 846-857
Carmeliat P, Tessier-Levigne M; “Common Mechanisms of Nerve and Blood Vessel Wiring”, Nature 14July 2005, Vol. 436:193-200.
The Developing Brain, Chapter 8, From Neurons to Neighborhoods. Durston S, Hulsoff Pol H, Casey BJ et al. Anatomical MRI of the
Developing Human Brain: What Have We Learned. JAACAP 2001, 40(9):1012-1020.
Gogtay N, Giedd J, Rapoport JL. Brain Development in Healthy, Hyperactive, and Psychotic Children. Arch Neurol 2002,
Vol 59:1244-1248. Gunnar M, Quevedo K. The Neurobiology of Stress and
Development. Annu. Rev. Psychol. 2007. 58:11.1–11.29
٢٥ ٢٦
٢٧ ٢٨
٢٩ ٣٠

11/1/2019
Introduction/Course Description
Introduction Introductory notes
Introductory notes
Introductory notes
Objectives and Results
Objectives Course objective 1 Course objective 2 Course objective 3
Results Expected results
Skills developed Skill 1 Skill 2
Schedule
Class/Week Topic Reading Assignment
1 Topic Chapter Task
2 Topic Chapter Task
3 Topic Chapter Task
٣١ ٣٢
٣٣ ٣٤
٣٥ ٣٦

11/1/2019
Procedures/Lecture Slide
Add procedure here Step one Step two
Conclusion
Add your conclusions here.
Questions/Discussions
Question One Discussion Discussion
Question Two Discussion
Questions Three Discussion
٣٧ ٣٨
٣٩ ٤٠
٤١