-
8/10/2019 AHIP Issue (Updated 6-4-14)
1/7
Introduction
Spending on specialty drugs represents an increasing share of
U.S. prescription drugspending and is growing at a rapid and
unsustainable rate. Addressing these cost-trendsis critically
important to ensuring a sustainable health care system and
achievingaffordability for businesses and consumers. In 2012, U.S.
spending on prescriptiondrugs totaled $263.3 billion25% of which
was spent on specialty drugs.1
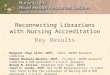
Figure 1: U.S. Spending on Prescription Drugs, 2012
Specialty drugswhich are generally understood to be drugs that
are structurallycomplex and often require special handling or
delivery mechanismsare pricedmuch higher than traditional drugs.
While these drugs have been ground breakingin the treatment of
cancer, rheumatoid arthritis, multiple sclerosis, and other
chronic
conditions, the cost of treating a patient with specialty drugs
can exceed tens ofthousands of dollars a year. Te treatment regimen
for some of the most expensivespecialty drugs can cost $750,000 per
year.2
While these drugs offer tremendous promise when medically
necessary, their highcosts and extended use has put a strain on our
health care system. Health plans,employers, and other stakeholders
are searching for new ways to restrain cost growthwhile
simultaneously maintaining access to safe and effective drugs for
patients.
Tis issue brief explores recent trends in the specialty drug
market, highlights some ofthe innovative strategies health plans
are adopting to control costs, and recommendsadditional policy
solutions to further promote high-value, high-quality care.
Americas Health
Insurance Plans
Issue
Brief
601 Pennsylvania A
South Building
Suite Five Hundred
Washington, D.C. 2
202.778.3200
www.ahip.org
Specialty DrugsIssues and ChallengesAdvancing Effective
Strategies to Address Soaring Drug Costs While
Assuring Access to Effective Treatments and Promoting
Continued
Medical Innovation
Issue Brief
Prescriptions Written in 2012 Prescription Drug Spending in
2012
1%
99%75%
25%
nTraditional Drugs nSpecialty Drugs
Source: Specialty Terapy Class Forecast, 2012. Express Scripts
Drug rend Report.
-
8/10/2019 AHIP Issue (Updated 6-4-14)
2/7
Unlike their traditional counterparts, spendingon specialty
drugs has shown no signs ofmoderation; an increase of 63 percent is
forecastover the 2014-2016 period. By some estimates,
spending on specialty drugs alone will total morethan $400
billion by 2020, and will comprisealmost half of all prescription
drug spending and9.1% of national health spending.6
Figure 3: Components of Commercial Trend,
2013(January-December 2013 compared tosame period in 2012)
Source: Te 2013 Drug rend Report. Express Scripts, April 2014.
Available at:http://lab.express-scripts.com/drug-trend-report/
Te increasing presence of specialty drugs in the
pharmaceutical market further explains theirposition as the
driver of drug spending. In 2010,specialty drug approvals by the
Food and DrugAdministration (FDA) exceeded traditional
drugapprovals for the first time (Figure 4), a trend thathas
continued each year since. And in 2013, 19of the 28 drugs approved
by the FDA70%were specialty drugs.7A recent report by healthcare
accrediting agency URAC noted that themarked increase of chronic
illnesses in Americans(such as cancer, obesity, diabetes) coupled
with
the increasing complexity of the pharmaceuticalindustry has
positioned the specialty drug marketfor continued growth.8
Prescription Drug Cost Trends
National spending on all pharmaceuticals hasmoderated in recent
years following similartrends in overall health care spending.
Te
Centers for Medicare & Medicaid Services(CMS) estimates that
prescription drug spendingwas approximately 9.4 percent ($263.3
billion) ofall health care spending in 2012, growing only0.4
percent from 2011.3While CMS attributesthis decline to greater
adoption of generic drugsand several blockbuster drugs losing
patentexclusivity, it projects sustained increases in drugspending
from 2015-2022 of six percent or moreannually as both drug prices
and utilizationincrease.4
Specialty drugs account for a disproportionateshare of overall
drug spending because of theirextremely high cost. Te average
annual retailcost for a specialty medication to treat a
chroniccondition was almost $29,000 in 20095, withsome drugs
costing as much as $750,000 (Figure 2).
Figure 2: Selected Conditions, Top Medical
Conditions and Specialty Drugs, 2010
Source: Limited Options to Manage Specialty Drug Spending.
Center forStudying Health System Change Research Brief. April
2012.
Because of the comparatively high cost of thesedrugs, the
commercial trend for pharmaceuticalspending in 2013 was driven in
large part byincreases in the unit cost of specialty drugs(Figure
3).
2
Issue Brief June 2014 Americas Health Insurance Plans
Health Condition
Average Cost Per
Treated MemberPer Year
Inflammation Conditions(Embrel, Humira, Remicade)
$14,455
Multiple Sclerosis (Copazone,Avonex, Rebif, Tysabri,
Avastin,Provenge)
$24,118
Cancer (Revlimid, Gleevec,Tarceva, Avastin, Provenge)
$11,089
Pulmonary Hypertension(Tracleer, Revatio, Letairis)
$32,570
Respiratory Conditions (Xolair,
Prolastin)
$18,550
0%
3%
6%
9%
12%
15%
nTraditional
nSpecialty
nAll Drugs
.Utilization Unit Costmn Total
0.5%
2.5%1.9%
2.4%2.4%
11.6%
14.1%
4.9% 5.4%
-
8/10/2019 AHIP Issue (Updated 6-4-14)
3/7
3
Issue Brief June 2014 Americas Health Insurance Plans
The Prescription Drug Market
Unsustainable growth of specialty drug spendingis due to many
complex factors but can beexplained, in part, by the legal and
regulatorytreatment of these therapies in the prescriptiondrug
market. Under current law, brand namebiologic drugs are given a 12
year exclusivityperiod upon approval from the FDAin effecta
government-approved monopoly. Tis period
of exclusivity is typically longer than the patentprotection
remaining for traditional drugs bythe time they are brought to
market. Althoughthese exclusivity periods give
pharmaceuticalmanufacturers the incentive to take on therisk of
developing groundbreaking drugs, theyalso precipitate a number of
negative policyconsequences.
Granting exclusivity to specialty drugs removesthe economic
benefits of price competition,resulting in higher prices relative
to what theywould be in a perfectly competitive market. Tistrend
can be seen in Medicare spending for PartB drugs, which are most
often specialty drugssince they are covered through the
medical,rather than pharmacy benefit. Te GovernmentAccountability
Office released a report examiningtrends in Part B spending and
found that in2010, not only did 10 drugs account for 44percent of
all Part B spending, but none of these
drugs had a generic version also approved bythe FDA.9Te lack of
adequate substitutes forthese drugs constrains payers (health
plans, thegovernment, or employers) efforts to implement
effective cost-containment policies. Healthplans have developed
expertise in using value-based purchasing or cost-sharing designs
thatsteer individuals toward high-quality/high-value treatments and
care. But when generic ortherapeutic alternatives do not exist, the
optionsavailable for encouraging high-value and cost-effective care
are limited.
Even when effective, less-costly substitutes doexist, payment
incentives are not necessarily
aligned to encourage their use. Recently releaseddata from CMS
on Part B expenditures highlightthis problem in the way two
biologicsAvastinand Lucentisare used to treat certain diseasesof
the eye. Although the two drugs have beenfound to be similarly
effective at treating age-related macular degeneration, Lucentis
costs morethan $2,000 per dose, while Avastin costs just$55. An
analysis of Part B expenditures for thesetwo drugs found that if
providers only prescribedAvastin instead of Lucentis over the next
decade,
it would result in nearly $29 billion in savings tothe health
care system.10
As a result of this confluence of factorsincreased FDA approvals
for specialty drugs,near-monopoly pricing, and the growing needfor
effective treatmentsexperts project thatspending on specialty drugs
is expected toskyrocket over the next decade and
beyond...intensifying the cost and access trade-offs thatpayers and
purchasers already face.11
Health Plan Efforts to ManageSpecialty Drug Spending
WhileEnsuring Access to High Quality Care
Health plans have developed a number ofstrategies in response to
sustained cost increasesthat ensure access to critically important
drugswhile also holding down costs.
6
7
8
8
10
14
18
22
22
18
23
24
12
17
21
0
5
10
15
20
25
Figure 4: FDA Traditional and Specialty Drug
Approvals, 20052012
nSpecialty Drug Approvals nTraditional Drug Approvals
2005 2006 2007 2008 2009 2010 2011 2012
Source: Medical Cost rend: Behind the Numbers
2014,PricewaterhouseCoopersHealth Research Institute. June 2013.
Figure 6.
6
7
8
8
10
14
18
22
22
22
18
23
24
12
17
21
-
8/10/2019 AHIP Issue (Updated 6-4-14)
4/7
4
Issue Brief June 2014 Americas Health Insurance Plans
Integration of Pharmacy and Medical
Benefits
Because of their complex nature and their deliverymechanism,
specialty drugs are often covered
through the medical, rather than the pharmacybenefit. Tis
distinction has interfered with theincorporation of traditional
cost-sharingmechanisms by obscuring prescribing and
utilizationpatterns across the two benefits causing amismatch
between utilization managementtechniques used for specialty and
traditional drugs.
Health plans have begun developing innovativebenefit designs
that both recognize the uniquenature of specialty drugs but allow
for appropriate
tiers and/or coinsurance rates. More tightlyintegrating the
pharmacy and medical benefitsalso allows plans to better track the
usage ofspecialty drugs across its enrollees and identifyadditional
areas for benefit modernization.
Policies to Maximize Treatment Adherence
Coverage of a specialty drug is ultimately fruitlessif patients
have poor adherence to a dosingregimen, or if they discontinue use
after filling theprescriptionleading to poor outcomes and
highercosts. Health plans are helping to ensure thatpatients are
taking their medications by engagingthem about the disease and the
therapeutic process.Health plans are also helping patients
understandhow to take their medications correctly bycoordinating
with providers and making sure thatpatients understand the
guidelines for using themedication and any potential side
effects.
Growing Role of Specialty Pharmacies
Many health plans now contract with specialtypharmacies that
supply enrollees with thespecialty drugs they need and coordinate
theoften complex delivery and treatment processesassociated with
these drugs. Tese pharmaciesare better suited than traditional
pharmaciesto monitor and track the use of specialty drugsand have
the necessary training and expertise tohandle their distribution.
Specialty pharmaciesalso employ dedicated teams of health care
specialists that can help enrollees understand howto manage
their medication and can help ensurethat these drugs are
administered at the mostappropriate site of care.
Utilization and Pharmacy Management
By covering specialty drugs for their intendeduses and
monitoring the effectiveness and anyside effects that occur during
the therapy session,health plans can help to ensure that
individualsare receiving safe and cost-effective care.
Policy Options to Promote High-Quality,Cost-Effective Drug
Coverage
Although health plan efforts at lowering thegrowth of spending
on specialty drugs haveshown signs of success, substantial reforms
areneeded at the state and federal levels to bettercontrol
specialty drug spending and promotepatient safety in the aggregate
and over the longterm. Policymakers can leverage the experienceof
health plans and other payers to enact policiesthat strike the
appropriate balance between costcontrol and promoting individuals
access toeffective treatments. Tese policy options include:
Encouraging alternative payment andincentive structuressuch as
coverage withevidence developmentfor new drugs andtechnologies.Such
payment strategies canensure access to new drugs while
generatingadditional evidence on the value to patientsof these new
medications. As part of abroader value-based purchasing strategy,
thesealternative arrangementssuch as outcomes-base contracting or
reimbursing providers
a flat fee for obtaining drugs, rather than apercentage of the
drugs total costprovideenhanced financial incentives for
manufacturersof new drugs and medical technologies thatare
contingent on agreed-upon standardsfor quality care, performance,
and healthoutcomes. Greater use and availability ofcomparative
effectiveness data is a key elementin the future growth of these
innovativepayment arrangements.
-
8/10/2019 AHIP Issue (Updated 6-4-14)
5/7
5
Issue Brief June 2014 Americas Health Insurance Plans
Shortening the exclusivity period forgeneric biologicsto promote
greater pricecompetition and earlier access to lower-costspecialty
drugs or generic biologics.Congress
should shorten the exclusivity period forbiologics to allow for
more competition fromfollow-on or generic biologicssimilar to
thepatent protections afforded to traditional, smallmolecule
prescription drugs. By shorteningthe exclusivity period, this
proposal wouldfacilitate the entry of lower-cost, genericbiologic
drugsreducing costs throughoutthe health care system. While
specialtyand other breakthrough drugs can offerlifesaving
treatments to patients with serious
medical conditions, there are opportunitiesto help reduce costs
and improve efficiencyin delivering high-quality,
cost-effectivetreatments to patients. By shortening theexclusivity
period, policymakers can ensuregreater price competition in the
specialty drugarea and help alleviate cost pressures for payersand
consumers.
Te U.S. Federal rade Commission (FC) hasconcluded that the
current 12-year exclusivityperiod is unnecessary to promote
innovation bypioneer biologic drug manufacturers and mayharm
consumers by directing scarce researchand development dollars
toward developinglow-risk clinical and safety data for drugproducts
with proven mechanisms of actionrather than toward new medical
inventionsto address unmet medical needs.12PresidentObamaas part of
the Administrations mostrecent budget proposal to Congresssupportsa
shorter exclusivity period as a way to strike
an appropriate balance between promotingaffordable access to
medication while at thesame time encouraging innovation to
developneeded therapies.13Te Administrationestimates that reducing
the exclusivity periodwill save $3.3 billion over ten years.14
Remove barriers at the state level thatrestrict the use of
biosimilars.While theAffordable Care Act authorized the FDA to
develop an abbreviated licensure pathwayfor biosimilar drugs, it
has yet to issue finalstandards that will determine when a
biosimilardrugs is truly interchangeable with an already
approved biologic. Ahead of these standards,some states have
already adopted legislationthat may restrict the availability of
biosimilarsbefore they even reach the market. Teseproposals will
limit patient access to drugs thatare not clinically different, yet
cost substantiallyless than their brand-name counterparts.
Expanding agencies authority to considerresearch on treatment
effectiveness.Consumers and providers have a right to know
which treatments and drug regimens workand which are less
effective. In the absenceof a national process for measuring the
cost-effectiveness of procedures and drugs, manyproviders are
attempting to control costs bybasing coverage decisions on the
relative costsof similar treatments. Sloane-Kettering CancerCenter
announced in 2012 that it would notprovide patients with Zaltrapa
drug usedto treat advanced colorectal cancer becauseit cost more
than double the price of Avastin
while offering no clinical advantages.15
Healthcare systems in Europe have also begunpursuing policies
that reimburse only for drugsthat have been clinically proven to
work.
o expand this evidence base in America,Congress should provide
new authorizinglanguage for the Patient-Centered OutcomesResearch
Institute (PCORI ) that explicitlyallows it to consider research on
cost-effectiveness as a valid component of patientoutcomes
research. PCORI and the Agency
for Healthcare Research and Quality(AHRQ ), in their funding of
research on theeffectiveness of treatments and technologiesand
their dissemination of the results of thatresearch, should
prioritize the establishment ofa multi-stakeholder, deliberative
process thatcan use such research to provide
trustworthyrecommendations on high-value and low-valuecare options
to providers, payers, and patients.
-
8/10/2019 AHIP Issue (Updated 6-4-14)
6/7
-
8/10/2019 AHIP Issue (Updated 6-4-14)
7/7
7
Issue Brief June 2014 Americas Health Insurance Plans
Conclusion
Te skyrocketing cost of specialty drugs remainsa critical
concern for policymakers and payersgiven the current trajectory of
pricing trends
in this fast-growing and emerging area. Teserecommendations
represent actionable steps thatcould be implemented to ensure the
efficientand effective use of these high-cost treatmentswhileat the
same timepromoting continuedmedical advances and innovations that
offerpromise and benefit patients and consumers.
1 Express Scripts: Drug rend Report, Specialty Terapy Class
Forecast. Availableat:
http://www.drugtrendreport.com/commercial/specialty-forecast-by-therapy-class
2 Brian Schill ing. Purchasing High Performance: Specialty Drugs
Poised toSkyrocket but Many Employers Have Yet o ake Notice. Te
CommonwealthFund; April 2012
3 National Health Spending in 2012: Rate of Health Spending
Growth Remained
Low For the Fourth Consecutive Year. Health Affairs.January
2014. Availableat:
http://content.healthaffairs.org/content/33/1/67.full.pdf
4 National health Expenditure Projections, 2012-2022. Te
Department ofHealth and Human Services, Centers for Medicare &
Medicaid Services.Available at: http://www.cms.gov/Resea
rch-Statist
ics-Data-and-Systems/Statistics-rends-and-Reports/NationalHealthExpendData/Downloads/Proj2012.pdf
5 Rx Price Watch Report: rends In Retail Prices of Specialty
Prescription DrugsWidely Used by Medicare Beneficiaries, 2005 to
2009. AARP Public PolicyInstitute. Available at:
http://www.aarp.org/content/dam/aarp/research/public_policy_institute/health/2011/rx-pricewatch-01-2012.pdf
6 Express Scripts Lab, 2013 Drug rend Report. April 2014.
Available at:http://lab.express-scripts.com/
7 Specialty Drug Approvals in 2013. Express Scripts Insights.
March 26, 2014.Available at: http://lab.express-scripts
.com/insights/drug-options/specialty-d rug-approvals-in-2013
8 CVS Caremark, Specialty rend Management: Where to Go Next,
Insights2013. Available at:
http://info.cvscaremark.com/cvs-insights/insights-specialty-
trend-management9 Medicare: Information on Highest-Expenditure
Part B Drugs. GAO estimony
before the Subcommittee on Health, Committee on Energy and
Commerce,House of Representatives. June 28, 2013. Available at:
http://www.gao.gov/assets/660/655608.pdf
10 David Hutton et. al. Switching o Less Expensive Blindness
Drug Could SaveMedicare Par t B $18 Billion Over A en-Year
Period.Health Affairs, 33 no. 6(2014): 931-939
11 Ha . u and Divya R. Samuel. Limited Options to Manage Specia
lty DrugSpending. Center for Studying Health System Change; April
2012
12 Federal rade Commission Report. Emerging Health Care Issues:
Follow-OnBiologic Drug Competition. June 2009.
13 Obama Administrations FY 2014 Budget Proposal.
14 Fiscal Year 2014 Budget, Page 198. Available at:
http://www.aarp.org/content/dam/aarp/research/public_policy_institute/health/2011/rx-pricewatch-01-2012.pdf
http://www.whitehouse.gov/sites/default/files/omb/budget/fy2014/assets/budget.pdf
15 Peter Bach, Leonard Saltz, and Robert Wittes. In Cancer Care,
Cost Matters.October 14, 2012. Available at :
http://www.nytimes.com/2012/10/15/opinion/a-hospital-says-no-to-an-11000-a-month-cancer-drug.html?_r=1&
16 Washington State: An Integrated Approach to Evidence-Based
DrugPurchasing. Te Commonwealth Fund
http://www.commonwealthfund.org/Newsletters/States-in-Action/2006/Mar/March-2006/Profiles--In-Depth-Looks-at-Initiatives-that-Are-Making-a-Difference/Washington-State--An-Integrated-Approach-to-Evidence-Based-Drug-Purchasing.aspx
17 Ha . u and Divya R. Samuel. Limited Options to Manage Specia
lty DrugSpending. Center for Studying Health System Change; April
2012
18 Least Costly Alternative Policies: Impact on Prostate Cancer
Drugs CoveredUnder Medicare Part B. Department of Health and Human
Services, Officeof the Inspector General. November 2012. Available
at: http://oig.hhs.gov/oei/reports/oei-12-12-00210.pdf
18 Estimates Effects on Direct Spending and Revenues for Health
Care Programsof Proposals in the Presidents 2014 Budget. Available
at:
http://www.cbo.gov/sites/default/files/cbofiles/attachments/44247_APB_HealthCarePrograms.pdf
For additional information or questions about this Issue
Brief,contact our Federal Affairs Department at 202.778.3200 or
[email protected]. Copyright 2014 by AmericasHealth
Insurance Plans. All rights reserved.
Americas Health Insurance Plans
601 Pennsylvania Ave., NW
South Building Suite 500
Washington, DC 20004
202.778.3200 www.ahip.org