Embed Size (px)
Citation preview
Aging and Care: A Partnership
Dr. Douglas FaulderMedical Director, Continuing Care, Edmonton Zone
Charlene Knudsen BScN, MEd, RNPractice Lead, Dementia Strategy
Shawna Reid RN, MN (student), GNC(C)Practice Lead, Dementia Advice through Health Link
Supported by the Seniors Health Strategic Clinical Network (SHSCN)
2
Aging – How are healthcare and community support systems going to support us as we grow older?
In this presentation we will:
1. Discuss key concepts to support aging Albertans
– Aging – In – Place
– Destination Home
– Person-Centred Care
– Transitions of care
2. Outline why care as we age is a partnership
3. Highlight several current initiatives that will support us to age-in-place
3
Outline
Presenter Topic to be Discussed
Shawna Aging-in-place
Current numbers and projections
Charlene Primary Health Care
Accessing Continuing Care
Home Care
Continuing Care Options
Doug Transitions – multimorbidity, frailty
Advanced Care Planning and Goals of Care Designation
Shawna Initiatives
4
Definition of Aging-in-Place• To include
o A specified location
o Acknowledgement of needs changing over time
• “Aging in place is the ability to live in one’s own home or community safely, independently, and comfortably, regardless of age, income, or ability level.” (CDC, 2010)
5
Wanting to stay in their homes
• Nearly 90% over those over 65 want to stay in their home (Keenan, 2010)
• 80% believe the will always live in their current residence (Keenan, 2010)
• Push factors: home maintenance, safety (e.g. stairs in home), ill health, transportation challenges
• Pull factors: access to health care, meal preparation, social activities

6
Recommendations for Aging-in-Place
• Multi-disciplinary involvement
• Flexibility
• Tempered enthusiasm
(Reid, 2015)
7
Demographics and Projections
• Population growth will be the highest in Canada
• By 2038, Alberta’s population will be 50% larger
• Proportion of our population 65 years and older…
o 2013 = 11.2%
o 2038 = 16.9% to 19.6%
• Median age…
o 2013 = 36 years
o 2038 = 38-41 years » Source: Statistics Canada. (2015)
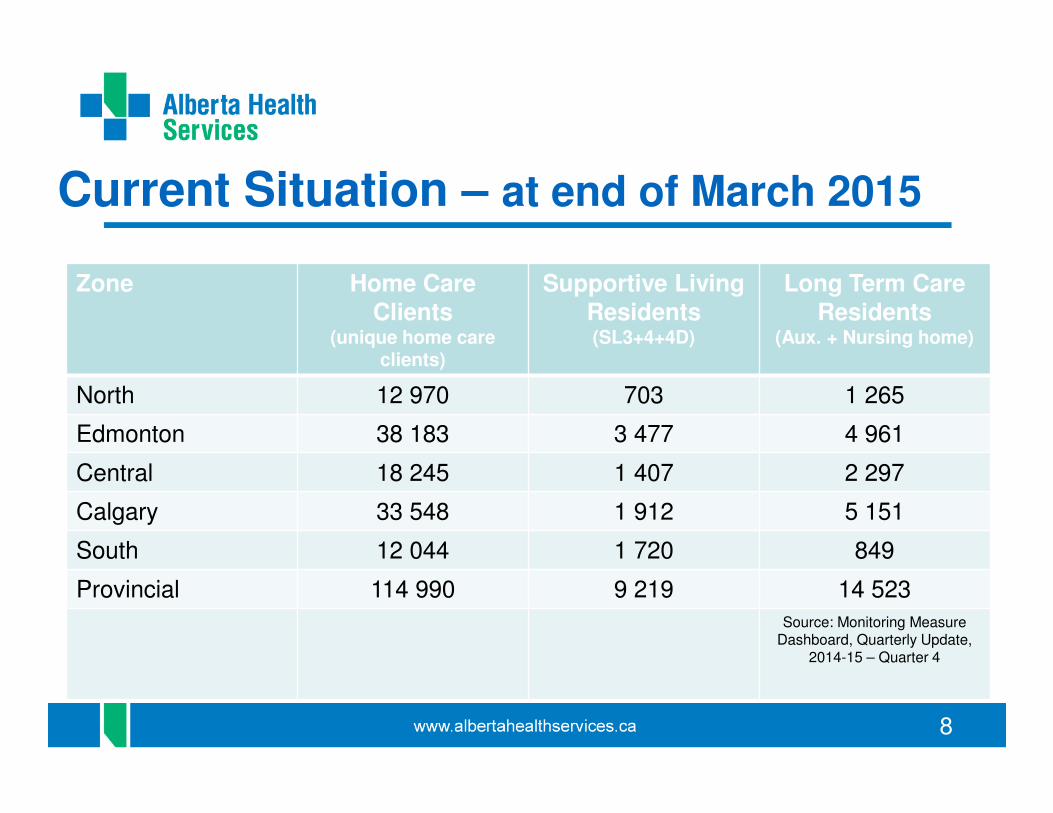
8
Current Situation – at end of March 2015
Zone Home Care Clients
(unique home care clients)
Supportive LivingResidents (SL3+4+4D)
Long Term Care Residents
(Aux. + Nursing home)
North 12 970 703 1 265
Edmonton 38 183 3 477 4 961
Central 18 245 1 407 2 297
Calgary 33 548 1 912 5 151
South 12 044 1 720 849
Provincial 114 990 9 219 14 523
Source: Monitoring Measure Dashboard, Quarterly Update,
2014-15 – Quarter 4
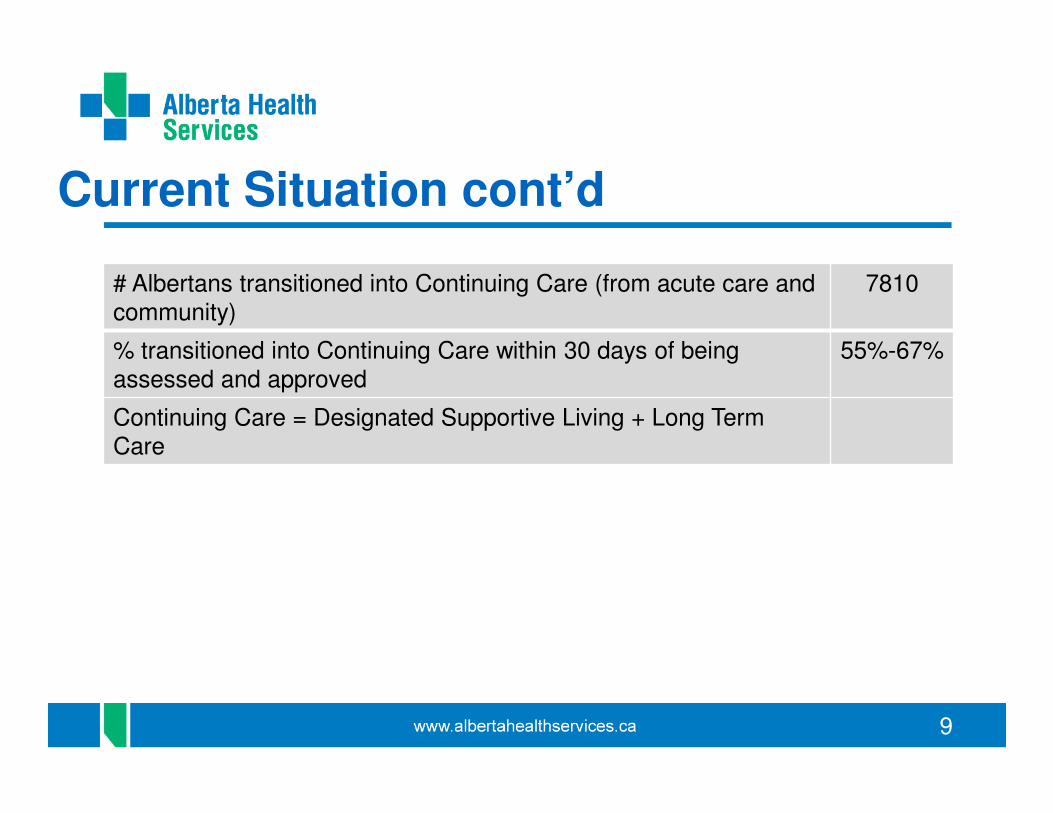
9
Current Situation cont’d
# Albertans transitioned into Continuing Care (from acute care and community)
7810
% transitioned into Continuing Care within 30 days of being assessed and approved
55%-67%
Continuing Care = Designated Supportive Living + Long Term Care
10
Future Situation in Alberta
• About 1900 more community-based spaces will come on stream in the next 2 years
• Streams and locations yet to be determined
• That will result in approximately 25 000 community-based spaces by the end of March 2016.
11
Primary Health Care
• Primary health care is the first place people go for health care or wellness advice or to diagnose or manage physical and mental health conditions. In Alberta, primary health care includes a wide range of services delivered by teams of providers that can include physicians, nurses, psychologists, pharmacists, dietitians, counselors, rehabilitation therapists, and social workers, among others, depending on the needs of the people with whom they are working.

12
Primary Care Networks
• a team of health professionals led by family doctors that delivers and co-ordinates health services
• a network can be one clinic with many family doctors and other health professionals or many family doctors and other health professionals in several clinics in a geographic area
13
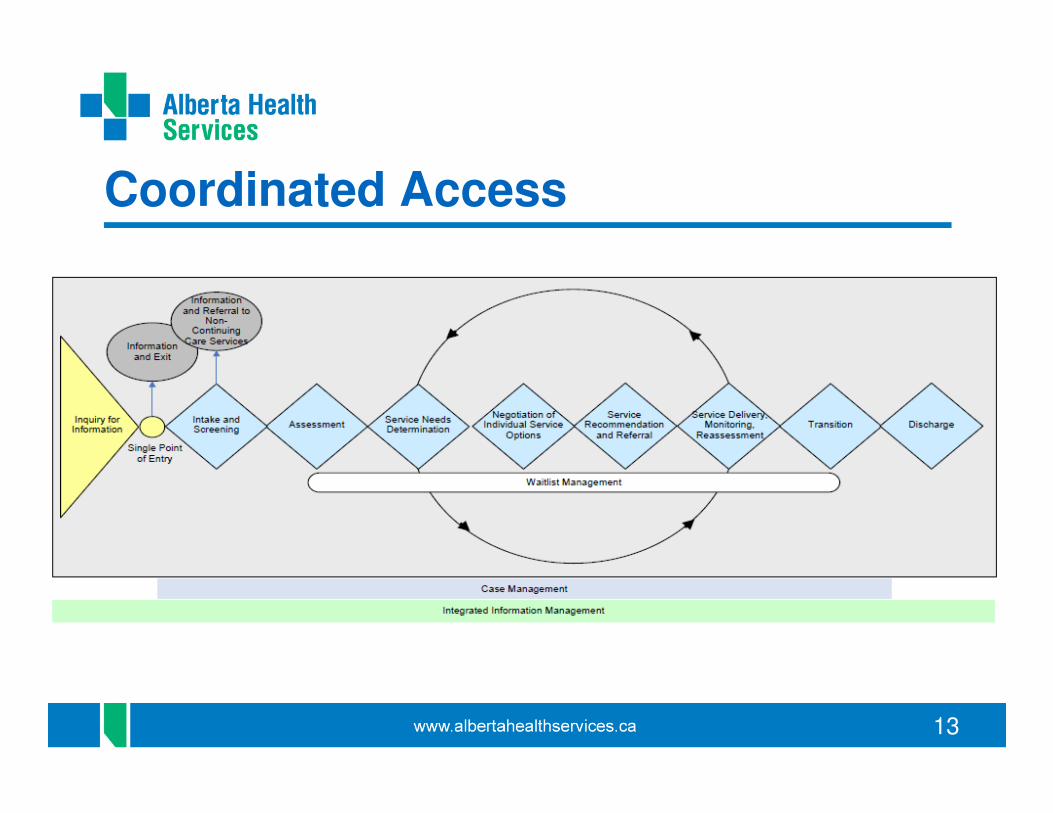
Coordinated Access
14
Supporting People
in their Home and Community
Home Care
• Publicly-funded health care and support services provided to eligible clients as governed by the Alberta Home Care Program Regulations of the Public Health Act.
• These services are provided to individuals living with frailty, disability, acute or chronic illness living at home or in a supportive living setting.
• Source: Alberta Health Services. Continuing Care Definitions.
15
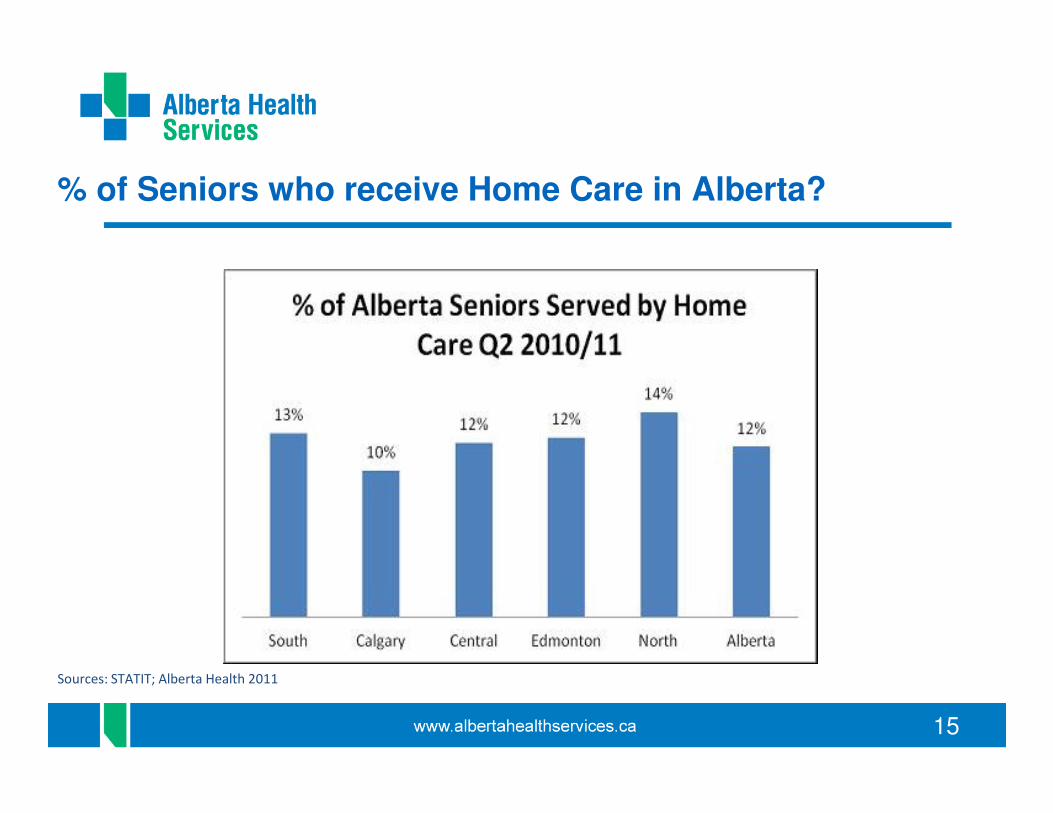
% of Seniors who receive Home Care in Alberta?
Sources: STATIT; Alberta Health 2011
16
17
Home Care Philosophy
• Person-centered care
• Focus on individual strengths & abilities
• Well being & independence
• Home as the First Option
• Care Planning & Systems Thinking
• Foundational: Coordinated Access, Case Management
18
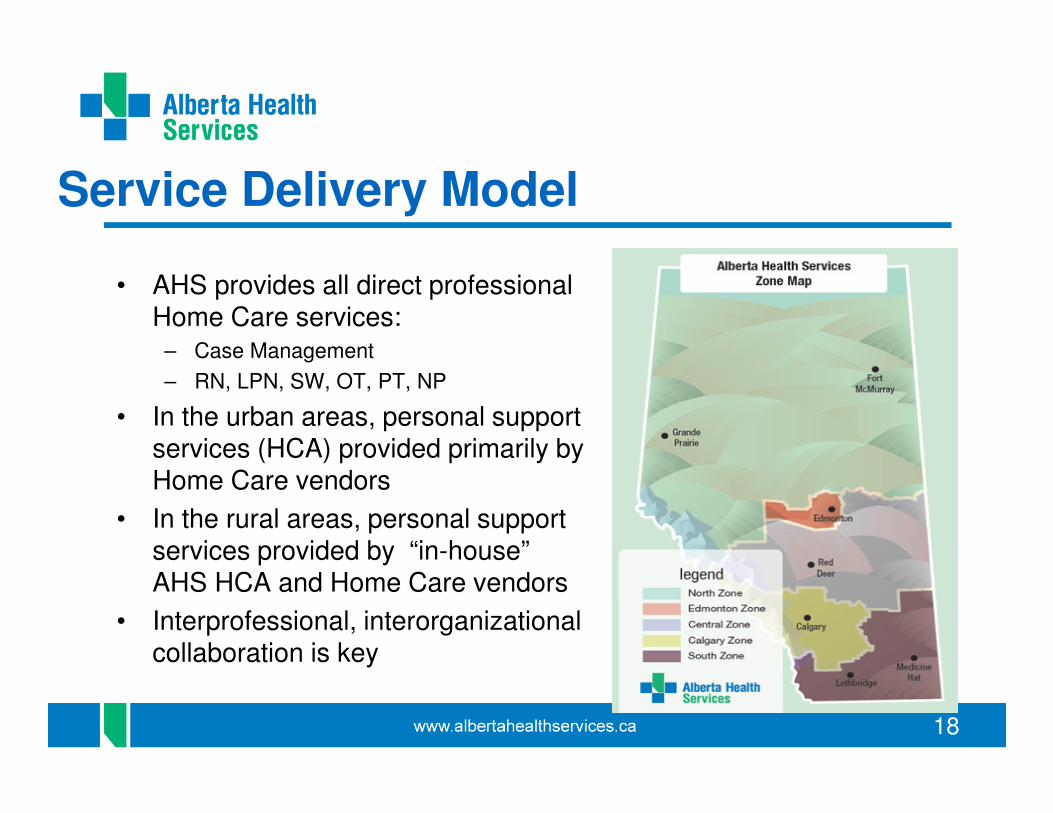
Service Delivery Model
• AHS provides all direct professional Home Care services:
– Case Management
– RN, LPN, SW, OT, PT, NP
• In the urban areas, personal support services (HCA) provided primarily by Home Care vendors
• In the rural areas, personal support services provided by “in-house” AHS HCA and Home Care vendors
• Interprofessional, interorganizationalcollaboration is key
19
Case Management
• collaborative, person-centred strategy for the provision of quality health and supportive services through the effective and efficient use of available resources in order to support the client’s achievement of goals.
20
Case Management Includes
o An initial functional assessment and reassessment in order to determine client needs, wants and service goals.
o The coordination and planning of services required to meet the needs of the client. This includes the location, establishment and maintenance of required services, and the maintenance of communication across various providers, delivery sites, departments, and agencies.
o Ensuring the implementation of care while monitoring and evaluating client outcomes.
o Reassessing the client as required and documenting subsequent revisions to the care plan.
o The coordination and planning of discharge activities.
21
Person referred to Home Care
• Mrs. Tippy, 82 yrs old
• Problem: falls – 2 times in past year
• Goal – prevent falls & planning for future
• Strong Family and Community Support
• Need: Equipment and Strengthening Exercises & Information
22
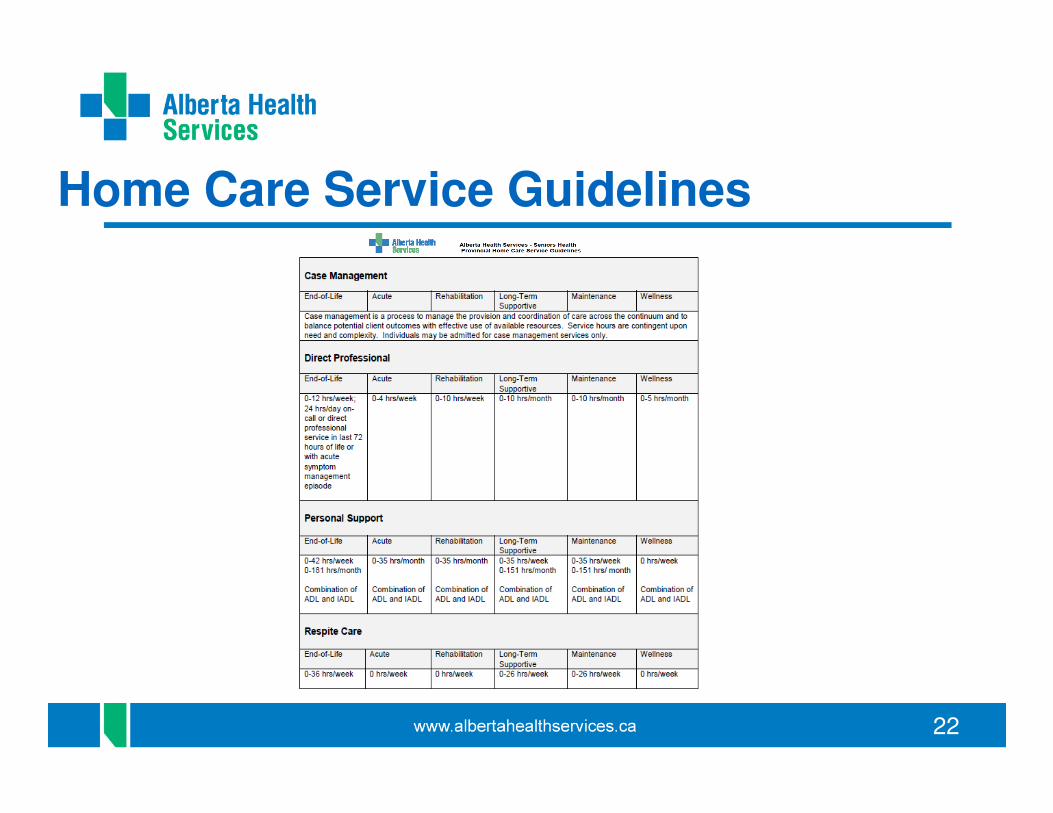
Home Care Service Guidelines
23
Person referred to Home Care
• Mrs. Tippy - 84 years old
• Problem(s) – increase in
frailty and dependence, cognitive decline
• Goal: maintain in home setting &
support caregivers
• Needs: in-home personal
HCA support, linkages to
community supports, care
coordination, collaboration and
communication with primary health care team.
24
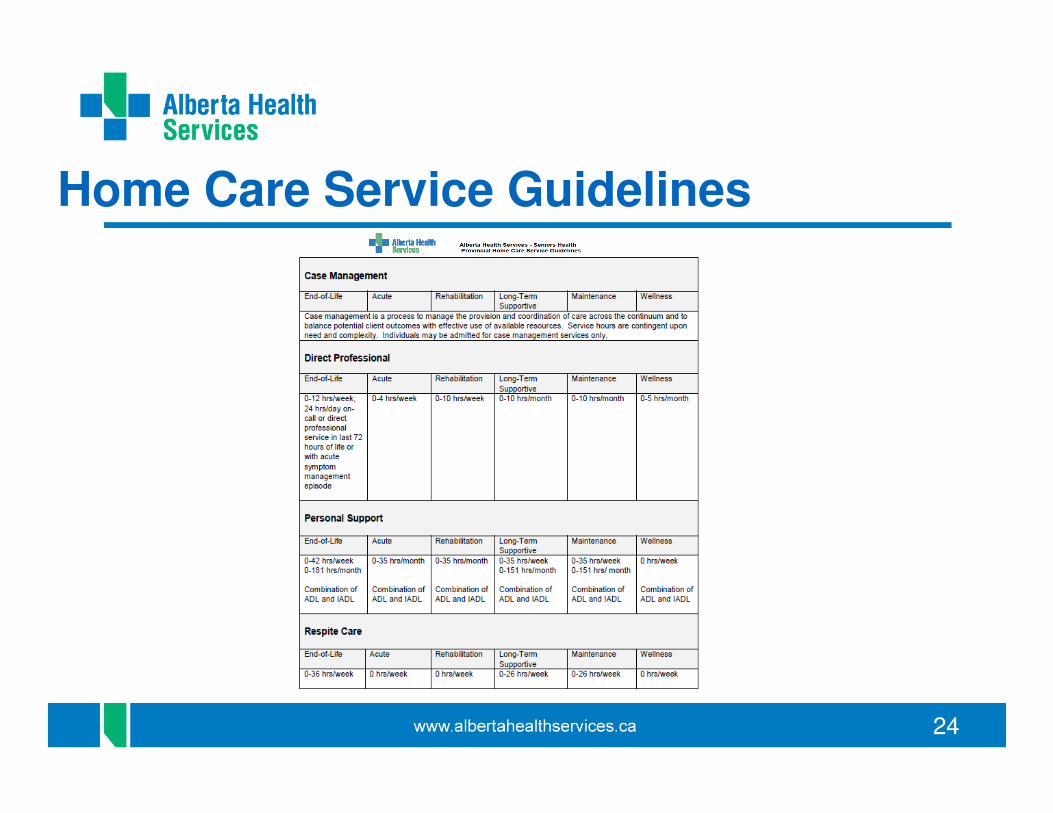
Home Care Service Guidelines
25
Supporting Caregivers & Respite
• Caregivers are key – up to 75% of total care provided in homes in Canada is by caregivers, est. $25 billion per year “hidden costs” (Health Council of Canada, 2012)
• Evidence suggests supporting caregivers can reduce caregiver burden, can result in decreased alternate level of care days and delayed admission to CC Living Option
26
Home Care Current Priorities
• Basket of Services Determination
• Hours of Service – Service Guidelines
• Restorative Care
• Caregiver Support
• Enhanced Case Management
• Spread of Destination Home
27
Continuing Care Options
Supportive Living
• A home-like setting where people can maintain control over their lives while also receiving the support they need.
• Supportive living promotes residents’ independence and aging in place through the provision of services such as 24-hour monitoring, emergency response, security, meals, housekeeping and life-enrichment activities.
• Publicly-funded personal care and health services.
28
Continuing Care Options
Long-Term Care (LTC)
• an environment that provides services for people with complex medical needs requiring 24-hour on site Registered Nurse assessment and/or treatment.
• In addition, professional services may be provided by Licensed Practical Nurses and 24-hour on site unscheduled and scheduled personal care and support will be provided by Health Care Aides.
• Other consultative services such as but not limited to Geriatric/Psychogeriatric Outreach Teams, Palliative Care, etc are provided through Alberta Health Services.
• Long-term care facilities may have secured long-term care, dementia care units. Long-term care facilities include “nursing homes” under the Nursing
Homes Act and “auxiliary hospitals” under the Hospitals Act.
29
Transitions in Care
• Transitions in Care are a time of stress and risk
– They need to be managed well to avoid poor outcomes to patients, and wastefulness in the health system
– In Alberta over 400 people monthly to LTC, and about 250 monthly to Supportive Living (SL3, SL4)
– http://insite.albertahealthservices.ca/sh/tms-sh-transitions-continuing-care-best-practice.pdf
30
Transitions in Care
• Transitions may involve:
� A change in medical status
� A change in functional status
� A change in care settings
� A change in services
� A change in health care providers
31
Transitions in Care
• Not just more elderly in our population:
– More people with chronic health issues
– More people with multiple chronic health issues (multimorbidity or comorbidities)
– More people with complex care needs
– More people with frailty
32
Transitions in Care
MULTIMORBIDITY� The presence of more than one acute or chronic condition
or disease in one person
� Most elderly with a chronic disease have multimorbidity
� Majority of older people have multimorbidity
• 55% over age 75 years have four or more chronic
conditions
• In LTC an average of 8 conditions
Uijen A, et al. Eur J Gen Pract 2008;1:28
33
Transitions in Care
MULTIMORBIDITY
• Increasing medicalisation of the elderly
• In those older than 85 in the UK between 2004 and 2012:
• ≥ 3 conditions – from 32% to 55%
• ≥ 3 medications – from 44% to 66%
• On no medications – 29% to 13%
Melzer D, et al. Age and Ageing 2015:44:46-53
34
Transitions in Care
FRAILTYDefinition by international consensus:
– An important clinical state of increased vulnerability, such that exposure to a stressor is more likely to result in adverse health outcomes, or dying, or increased dependency.
– A useful concept at all levels of health care.
Morley JE, et al. Frailty Consensus: A Call To Action:
J Am Med Dir Assoc 2013;14:392-397
35
Transitions in Care
FRAILTYThe frail are especially vulnerable at a time of transition.
Frail patients go into hospital with complex care needs, and come out of hospital with even more complex ongoing care needs.
Seniors have difficulty navigating through transitions
36
Transitions in Care
It is critical to find solutions!
• Identify those at risk – Who is frail and vulnerable?
• Improve integration and communication
• Case Management – an overarching collaborative and person-centered approach
• Plan of Care – person-centered based on their goals, values, strengths and resources
• Reducing the number of Transitions

37
Transitions in Care
It is critical to find solutions!
Post-Acute Care options
Why – avoid the risks of acute care such as iatrogenic disability and C. difficile infections, and avoid premature and unnecessary transitions
What – SubAcute, Restorative Care, Rural Hospitals
38
Transitions in Care
AN EXAMPLE – FRACTURED HIP CARE
• Over 2700 hip fractures in Alberta each year, with increasing average age and increasing co-morbidities
• Almost half of seniors with a hip fracture will still be alive in 5 years.
• Half are out of the surgical hospital in just over 8 days.
• Most recently 71% return home (AHS Goal is 75%), and
76 % get to their original home or new home in 28 days (Goal – 80%).
39
Transitions in Care
AN EXAMPLE – FRACTURED HIP CARE
Through the Bone and Joint Health SCN there has been:
• a standardization of pre-operative care in urban and rural hospitals across the province
• a standardization of postoperative care across the province
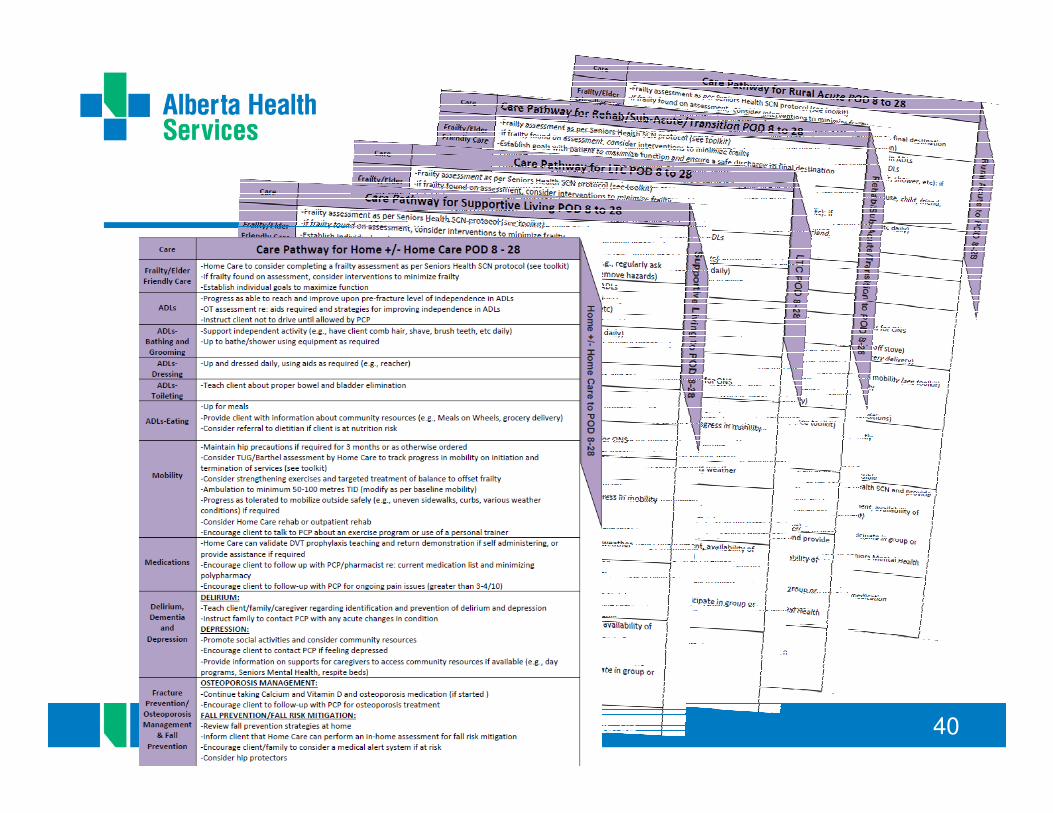
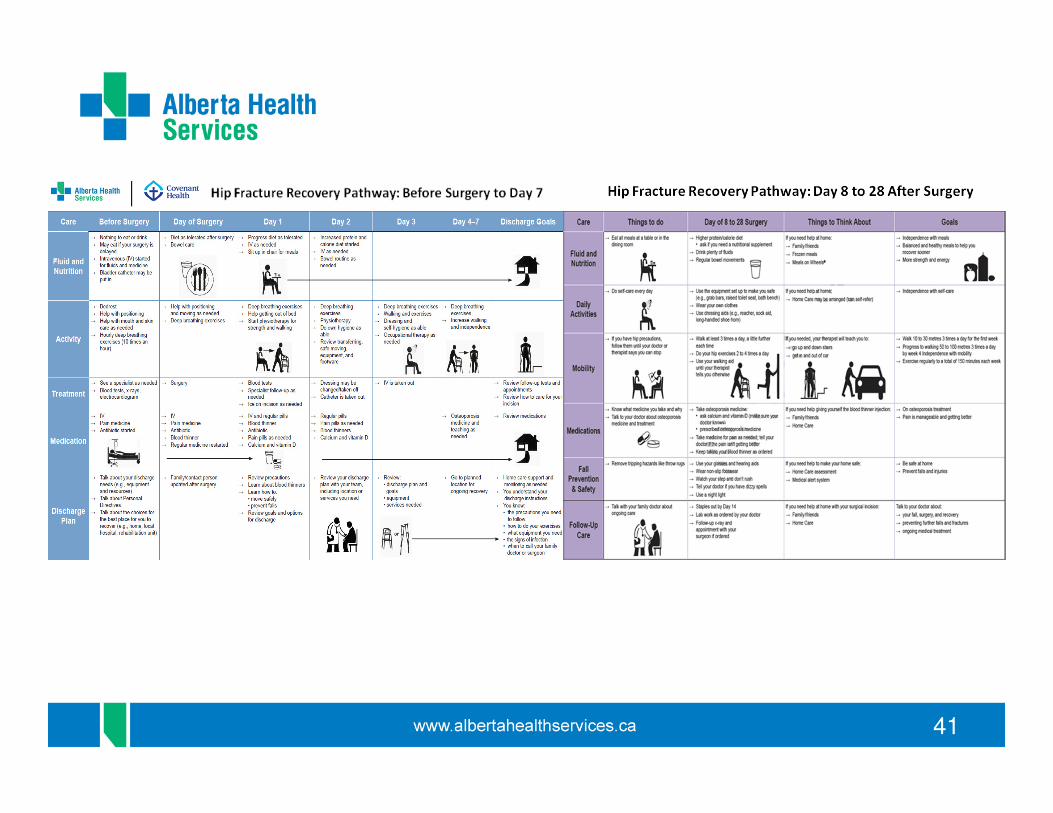
• The development of Fractured Hip Restorative Care Pathways for Surgical and Post-surgical sites
40
41
42
Advanced Care Planning (ACP) and Goals of Care Designation (GCD)
• Standardized processes to help Albertans and their health care teams have conversations (Advanced Care Planning) and then document their goals of care decisions (Goals of Care Designations)
• Different from Personal Directives!
• ACP and GCD forms – Green Sleeve
• Well integrated into acute care, long term care, and supportive living
43
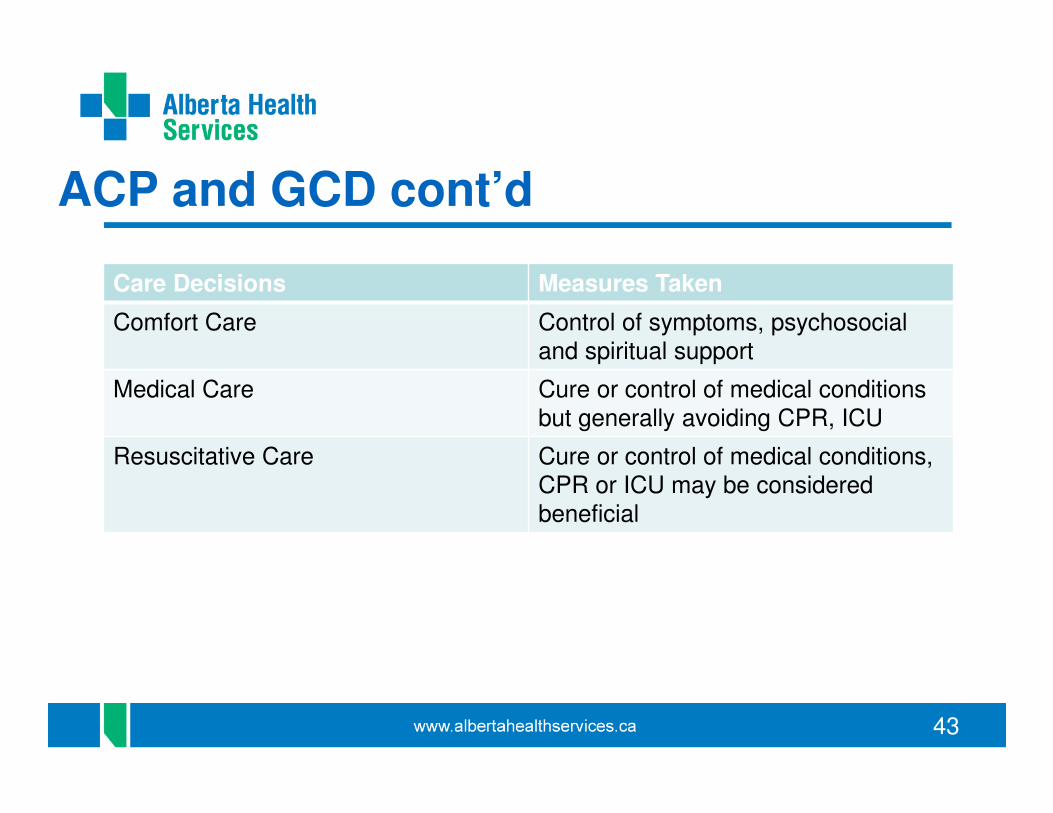
ACP and GCD cont’d
Care Decisions Measures Taken
Comfort Care Control of symptoms, psychosocial and spiritual support
Medical Care Cure or control of medical conditions but generally avoiding CPR, ICU
Resuscitative Care Cure or control of medical conditions, CPR or ICU may be considered beneficial
44
Initiatives: Seniors Health Strategic Clinical Network
• Mission/mandate
o To make improvements to health care services and practices that enable Alberta’s seniors to optimize their health, well being and independence
• Network of health care providers, managers, researchers, policy makers, and caregivers
• Change agent to improve health care based on research and innovation
(Alberta Health Services, 2015)
45
SH SCN cont’d
• Appropriate Use of Antipsychotics
o Has rolled out to 170 long term care sites in Alberta
o Goal of <20% of LTC residents on antipsychotic medication without an appropriate diagnosis
o Success - provincial average 19.8% !!
o Next steps - implementation in Supportive Living and set new target goal to further reduce antipsychotic medication usage in SL and LTC.
46
SH SCN cont’d
• Elder-friendly Care (studies)
1.Elder-friendly care (EFC) in Acute Care
o Initiative to promote comfort rounds, delirium detection and least restraint among acute care units
2.Elder-friendly Approaches to Surgical Environment (EASE)
o Promotion of practices before and after surgery, to reduce complications and return to normal routine
• Mobilization of Vulnerable Elders (MOVE)
o Promotion of early mobilization of older in-patients
47
SH SCN cont’d
• Dementia Advice through Health Link
o Telephone advice line providing dementia-related support to caregivers and to PLWD
o Available 7 days per week, 8 hours per day
o Launched September 28 in North, Central, and South Zones
o Later expansions into Edmonton and Calgary Zones, to 10 hours per day, and to clinicians/care providers
48
Current Initiatives: EMS
o Paramedic Response Unit – Medicine Hat
o Pilot project – frequent EMS and ED users – Grande Prairie
o Community paramedic – Calgary zone
o Complex Client Team – Edmonton zone
o Mental Health Crisis Team – Edmonton zone
o Edmonton Continuing Care Urgent Response Team – Edmonton zone
o Community Health and Prehospital Support (CHAPS)
• Provincial
o Palliative and End-of-Life Care, Assess, Treat and Refer Program
• Provincial
49
Current Initiatives: Other
• Continuing Care Resolution Team
• Development of Continuing Care and Dementia Strategies
• Destination Home
• Palliative and End-of-Life Care (PEOLC) Strategy
• Central Zone: home dialysis
• South Zone: NPs in Continuing Care
50
Questions?
51
Acknowledgements
• Jamie Davenport, Director, Home Care Development, AHS
• Niall MacDonald, Strategic Implementation, Capacity Management,
AHS
• Curtis Snider, Lead Capacity Management, AHS
• Dawna Chalifoux, Lead Senior Consultant, Accountability and
Monitoring
• Jody Wilson, Accountability and Monitoring
52
References• Alberta Health and Wellness. (December, 2008). Continuing care strategy: Aging in the right place. Retrieved March 1,
2010 from http://www.health.alberta.ca/documents/ Continuing-Care-Strategy-2008.pdf
• Alberta Health Services. (2015). Annual Report: 2014-2015. Retrieved from http://www.albertahealthservices.ca/assets/about/publications/ahs-pub-2014-2015-annual-report.pdf
• Alberta Health Services. (2010). Case Management Literature Review. Alberta: Author.
• Alberta Health Services. (2013). Continuing Care Service Needs Determination Guide. Alberta: Author.
• Alberta Health Services. (2015). Monitoring Measure Dashboard: Quarterly Update: 2014-2015 – Quarter 4. Retrieved from http://www.albertahealthservices.ca/assets/about/publications/ahs-pub-monitoring-measures-q4-2014-2015.pdf
• Alberta Health Services. (2011c). Progressing the Continuing Care Strategy: Continuing Care Case Management Framework & Guidelines.
• Alberta Health Services. (2015). Provincial Performance Measure Update: Q4 2014-2015. Retrieved from http://www.albertahealthservices.ca/assets/about/publications/ahs-pub-pr-2014-15-q4.pdf
• Alberta Health Services. (2015). Seniors Health Strategic Clinical Network. Seniors Health SCN (Quick Facts). Retrieved from : http://www.albertahealthservices.ca/Strategic%20Clinical%20Networks/ahs-scn-srs-quick-facts.pdf and http://www.albertahealthservices.ca/7702.asp
• Centers for Disease Control and Prevention, Healthy Places Terminology (Washington, D.C.: Centers for Disease Control and Prevention, 2010); http://www.cdc.gov/healthyplaces/terminology.htm).
• Keenan, T. A. (2010). Home and Community Preferences of the 45+ Population (Washington, D.C.: AARP, 2010), 4.
• Reid, S. (2015). Exploring perspectives of aging-in-place: An integrative review.
• Statistics Canada. (2015). Section 3: Results at the provincial and territorial level. 2013 – 2038. Retrieved from http://www.statcan.gc.ca/pub/91-520-x/2014001/section03-eng.htm#a11