Embed Size (px)
Citation preview

AGGRESSIVE PERIODONTITIS

“Infectious, inflammatory disease of thePeridontium with rapid attachment loss and
bone loss in otherwise healthyadolescent with familial aggregation of
diseased individuals.”
DEFINITION OF AGGRESSIVE PERIODONTITIS

CLASSIFICATION

Age of onsetRapid rate of disease progressionThe nature and composition of associated
sub-gingival microflora Alterations in the host’s immune responseFamilial aggregation of diseased individuals
DIFFERENCE BETWEEN AGGRESSIVE AND CHRONIC PERIODONTITIS
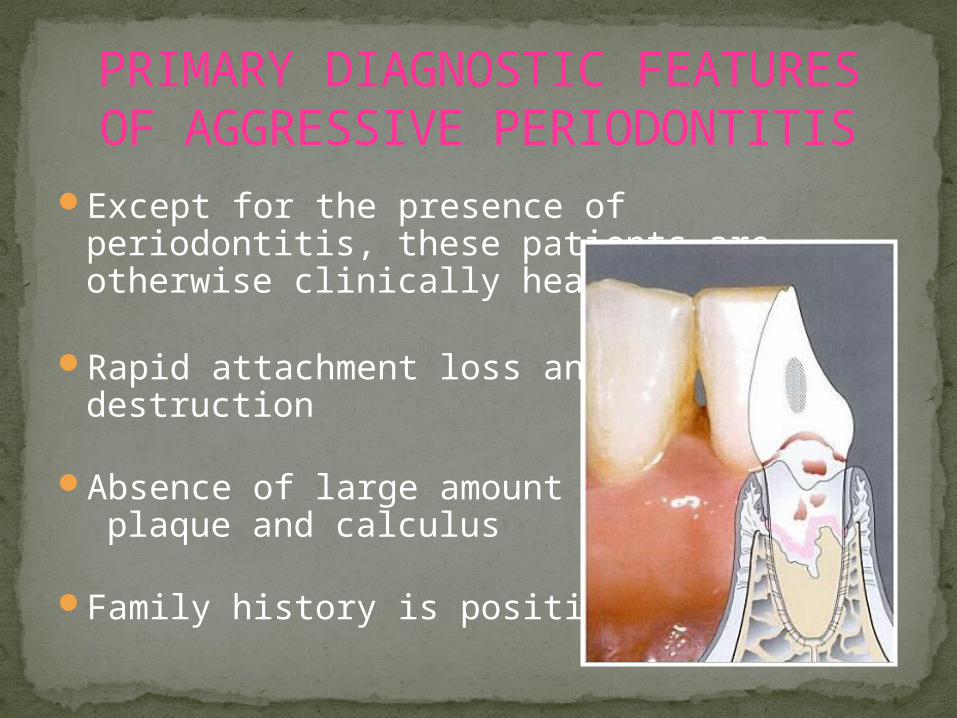
Except for the presence of periodontitis, these patients are otherwise clinically healthy
Rapid attachment loss and bone destruction
Absence of large amount of plaque and calculus
Family history is positive
PRIMARY DIAGNOSTIC FEATURES OF AGGRESSIVE PERIODONTITIS
Elevated levels of Actinobacillus actinomycetem-comitans and, in some cases, Porphyromonas gingivalis
Abnormal phagocytes and hyper-responding macrophages
The progression of bone loss may be self-arresting
Disease is more prevalent among the African Americans
SECONDARY FEATURES OF AGGRESSIVE PERIODONTITIS

“LOCALIZED AGGRESSIVE
PERIODONTITIS’’

Clinical features:1. Age of onset at about puberty.2. Affects both the sexes3. Main characteristic
feature affects mainly the
4. Lack of clinical inflammation despite the presence of deep periodontal pockets.
LOCALIZED AGGRESSIVE PERIODONTITIS
11 mm
9 mm
FIRST MOLARS and INCISORS

Clinical features (cont.)5. Plaque that is present forms
thin biofilm on the teeth.6. Plaque contains elevated
levels of : Actinobacillus actinomycetem-comitans (Serotype b) Porphyromonas gingivalis (in some pts)
7. Disease progresses rapidly
LOCALIZED AGGRESSIVE PERIODONTITIS

Clinical features (cont.)
8. The rate of bone loss is 3 to 4 times faster than in chronic periodontitis.
LOCALIZED AGGRESSIVE PERIODONTITIS

Other Clinical Findings:
1. Maxillary incisors migrate disto-labially that results in diastema formation.
2. Increasing mobility of the affected teeth
3. Sensitivity of denuded root surfaces to thermal and tactile stimuli
LOCALIZED AGGRESSIVE PERIODONTITIS

4. Deep, dull radiating pain during mastication.5. Periodontal abscess may form.6. Regional lymph node enlargement may occur.
LOCALIZED AGGRESSIVE PERIODONTITIS

Following are the possible reasons for localized distribution of lesions:
1. Strong antibody response to infecting agents:
“BURN-OUT PHENOMENA”
Actinobacillus actinomycetem initially colonizes the 1st permenant teeth to erupt.
The host defenses are evaded.
LOCALIZED AGGRESSIVE PERIODONTITIS

Entry of bacteria into the pocket
Initiation of destruction of periodontal tissues.
In turn, immune defenses are stimulated production of opsonic antibodies enhance clearance of invading bacteria and neutralize leukotoxic activity.
This may prevent colonization at other sites.
LOCALIZED AGGRESSIVE PERIODONTITIS

2. Action of antagonistic bacteria:
Colonization of periodontal tissues.
Inhibit further colonization of Actinobacillus actinomycetem-comitans.
Localized tissue destruction.
LOCALIZED AGGRESSIVE PERIODONTITIS

3. Actinobacillus actinomycetem-comitans loses its ability to produce leukotoxin
Progression of the disease may become arrested.
4. Denuded root surfaces
Defect in cementum formation maybe resposible for localization of the lesions.
Hypoplasic or aplasitic cementum.
LOCALIZED AGGRESSIVE PERIODONTITIS

Radiographic finding:
o Classic diagnostic sign VERTICAL LOSS of alveolar bone around the first molars and incisors.
LOCALIZED AGGRESSIVE PERIODONTITIS

o Other finding “Arc-shaped” loss of alveolar bone extending from the distal surface of 2nd premolar to the mesial surface of the 2nd molar.
o Bone defects are usually wider than usually seen with chronic periodontitis.
LOCALILIZED AGGRESSIVE PERIODONTITIS
Notice the typical angular (vertical) bone loss and its typical location involving the first molars. Calculus is absent and is not an etiologic factor.

GENERALIZED AGGRESSIVE
PERIODONTITIS

Generalized aggressive periodontitis
“Characterized by generalized interproximal attachment loss affecting at least three
permanent teeth other than first molars and incisors”
Generalized juvenile periodontitis Rapidly progressive periodontitis

Etiology
The amount of plaque seems inconsistent with the amount of periodontal destruction.
Bacteria frequently detected are p.gingivalis, a.actinomycetem-comitans and tannerella forsythia

Clinical featuresUsually affects individuals between
puberty and 35 years (may be older).No Gender discriminationPronounced episodic nature of
destruction followed by stages of quiescence that may last weeks to months or years.
almost all or most of the teeth are affected.
Poor serum antibody response to infecting bacteria.

Tissue response
Episodic nature of disease produces Two gingival response.
1. Destructive phase2. Non-destructive phase

Destructive phase:Tissue appears severely inflamed, ulcerated &
fiery red.Bleeding with or without stimulation.Suppuration.Active attachment & bone loss.

Non-destructive phase:
Tissues appear pink with some stippling.Lack of inflammation.Probing will reveal deep pockets.Bone & attachment levels relatively stable.
Associated Systemic manifestations
Some patients with GAP may exhibit:Weight lossMental depression, general malaise
Systemic conditions may predispose client to GAP, these include:Chronic neutrophil defects, leukocyte
adherence deficiencyFunctional defects of PMNs, monocytes or
both impaired chemotaxis & phagocytosis

Radiographic evaluation
Radiographic evaluation can range from :
Severe bone loss affecting minimal number of teeth -OR-
Majority of teeth affected by advanced bone loss



Case no.1A 11 year old boy diagnosed as generalized
aggressive periodontitis

Radiographic presentation:

Case no 2.A case of 31 year old female with LAP over
14 years

Radiographic status after full mouth disinfection therapy and surgical
regenrarive procedures.(impressive regenration at the mandibular first
molars)

RISK FACTORS FOR AGGRESSIVE
PERIODONTITIS.

RISK FACTORS:There are mainly four recognized risk factors
for aggressive periodontitis:
Microbiological factorsImmunological factorsGenetic factorsEnvironmental factors
MICROBIOLOGICAL FACTORS:
A. actinomycetemcomitans:These are short, facultative anaerobic gram
negative rods.Virulence factors associated with
A.actinomycetemcomitans: Leukotoxins Endotoxins Collegenase Chemotactic inhibition factors


Studies show… A.actinomycetemcomitans is found in high
frequency with lesions associated with LAP.
Sites with rapid progression show elevated levels of this bacteria.
Patients with cliniclly manifested LAP show elevated levels of A.actinomycetemcomitans.
Treatment shows reduction in sub-ginival load of this bacteria.

Other microbiological factors include:Porphyromonas gingivalisCapnocytophaga sputigenaPrevotella intermediaMycoplasma speciesSpirochetes

IMMUNOLOGICAL FACTORS:Functional defects of PMNs and monocytes Impairment of the chemotactic attraction
of the PMNs to the site of infection Ultimately
leading to reduced phagocytosis.
Functional neutrophil defects may be induced by bacterial infection or it may be genetic in origin.

GENETIC FACTORS:
Familial clustering of the neutrophil abnormalities suggest that defects my be inherited.
Several studies show that response to periodontal pathogens is under genetic control.

ENVIRONMENTAL FACTORS:Amount and duration of Smoking.Smokers with GAP usually have more no. of
teeth affected.

TREATMENT FOR LOCALIZED AGGRESSIVE PERIODONTITIS:
Extraction of involved teeth (depends on severity of tissue loss)
Periodontal therapy:Plaque control
instructionDebridement with or
without flap surgeryIrrigation with CHX,
home rinsing with CHXBone grafts, root
resections, hemisections

Antibiotic therapy:Adjunctive therapy often
required to eliminate A.a. from tissues
Tetracycline (250 mg qid for 2 weeks)
Metronidazole combined with amoxicillin
Doxycycline
The earlier the condition is diagnosed, the sooner treatment can begin – outcome often more predictable

TREATMENT FOR GENERALIZED AGGRESSIVE PERIODONTITIS:
Careful monitoring of younger clients with GAP b/c rate of disease progression is often faster
Maintenance every 3 weeks or less is recommended if disease in active phase
Periodontal therapy:Debridement in combination with antibiotic
therapy, strict plaque control, CHX irrigation & rinsing
Periodontal surgery


Antibiotic therapy:Highly recommended that microbial
diagnostic & susceptibility testing be done
Combination therapies include:Metronidazole/amoxicillinAmoxicillin/doxycyclineClindamycin

PERIODONTAL SURGERY
1. PRE-SURGICAL BONY DEFECT

2. FLAP INCISION ACCESSES BONE

3. IF NECESSARY, BONE IS CONTOURED

4. IN SOME CASES THE BONE WILL BE REBUILT WITH A BONE GRAFT.

5. GUM IS SUTURED.

6. GUM HEALED INTO NEW POSITION.

THANK YOU!!!