-
8/11/2019 Aggressive Central Giant Cell
1/8
CLINICOTHERAPEUTIC CONFERENCE
J Oral Maxillofac Surg68:2537-2544, 2010
Aggressive Central Giant Cell
Granuloma of the MandiblePetr Schtz, MD,*
Khalid H. El-Bassuoni, BDS, HDD, FDSRCS Ed,
Joneja Munish, MSc, FRCPath,
Hussein H. Hamed, BDS, HDD, MSc, PhD, and
Bonnie L. Padwa, DMD, MD
Case Presentation
An 11-year-old Egyptian boy presented with mild pain in hisleft
lower jaw accompanied by swelling. Clinical examination
showed a hard, tender mandibular enlargement extendingfrom the
chin to the left molar area. The orthopantomogram(OPG) showed
poorly defined multilocular radiolucency in-
volving the mandibular body from the right lateral incisor tothe
left first molar (Fig 1A). There were discrete signs ofresorption
of root apices of the adjacent teeth. Computedtomography
examination disclosed a large expansive osteo-lytic lesion with a
soap bubble appearance and erosion of both
vestibular and lingual mandibular cortices (Fig 1B).Incisional
biopsy was performed under local anesthesia.
Sections contained spindle cells within fibrous stroma
andirregularly distributed multinucleated giant cells
clusteringaround areas of hemorrhage. Periphery of the lesionshowed
reactive osteoid tissue formation (Fig 1C).
The overall clinical, radiologic, and histopathologic picturewas
consistent with central giant cell granuloma.
Laboratoryinvestigations including complete blood count, alkaline
phos-phatase, calcium, and parathormone levels were within nor-mal
limits, while phosphorus level was slightly elevated.
Treatment Recommendations
Bonnie L. Padwa, DMD, MD
Giant cell lesions (GCLs) of the jaws are found in
the mandible more commonly than the maxilla, andin females more
often than in males. These benignlesions occur before the age of 30
years.1 GCLs areusually unifocal. Multifocal lesions should alert
theclinician to the possibility of hyperparathyroidismor, if
bilateral, cherubism or Noonan syndrome.1,2
GCLs are osteoclast-rich tumors that are histopatho-logically
indistinguishable from those seen incherubism and Noonan syndrome.
Nevertheless, pa-tients with isolated GCLs do not have the
cherubism-related germline SH3BP2 mutation, andthe lesions donot
contain somatic SH3BP2 mutations.3 This findingsuggests that even
though all GCLs might appear thesame histologically, they likely
have a different etio-pathogenesis.
The first description of GCLs was by Jaffe4 in 1953.However,
confusion remains about the nature of thelesion
(reactive/inflammatory, neoplastic), the cell oforigin, and the
variability in clinical behavior. Thus,an assortment of treatment
modalities, with differentmechanisms of action, have been tried in
patients
with a variety of lesions with inconsistent outcomes;all of
which has made deciphering the best treatmentoption difficult for
the practitioner.
The histopathologic features of GCLs are a large
number of multinucleated giant cells and mononu-clear cells
within a fibrous stroma. The giant cells inGCL may be reactive or
secondary, not the cell oforigin. Macrophages, mesenchymal cells,
and fibro-blasts have all been proposed as being responsible forthe
lesion.5
There is variability in the clinical behavior of GCLs.Rapidly
growing expansile lesions with an aggressiveappearance (eg, pain,
paresthesia, root resorption)are at one end of the spectrum and
small asymptom-atic slow-growing lesions are at the other
end.Chuong et al6 categorized the clinical and radio-
*Consultant, Head of Oral, Maxillofacial Surgery Unit,
Al-Adan
Dental Center, Ministry of Health, Kuwait City, Kuwait.
Senior Registrar, Oral and Maxillofacial Surgery Unit,
Al-Adan
Dental Center, Ministry of Health, Kuwait City, Kuwait.
Head of Histopathology Unit, Radiology, Nuclear Medicine and
Laboratory Center (YIACO Medical Co), Al-Adan Hospital,
Kuwait
City, Kuwait.
Senior Registrar, Oral and Maxillofacial Surgery Unit,
Al-Adan
Dental Center, Ministry of Health, Kuwait City, Kuwait.
Associate Professor of Oral and Maxillofacial Surgery,
Harvard
School of Dental Medicine, and Oral Surgeon-in-Chief,
Department
of Plastic and Oral Surgery, Childrens Hospital, Boston, MA.
Address correspondence and reprint requests to Dr Schtz: Box
3021, 22031 Salmiya, State of Kuwait; e-mail:
petrschutz@yahoo.
com
2010 American Association of Oral and Maxillofacial Surgeons
0278-2391/10/6810-0024$36.00/0
doi:10.1016/j.joms.2009.06.042
2537
mailto:[email protected]:[email protected]:[email protected]:[email protected]
-
8/11/2019 Aggressive Central Giant Cell
2/8
graphic features of aggressive GCLs: 1) size greaterthan 5 cm,
2) rapid growth, 3) recurrence after cu-rettage,4) cortical bone
thinning and/or perforation,and 5) tooth displacement and/or
resorption.
Because the cell of origin is unknown and histolog-ically
aggressive and nonaggressive GCLs appear thesame through the
microscope, many groups have
considered biomarkers as a means of identifying ag-gressive
versus nonaggressive lesions and correlatingthese with the clinical
behavior and treatment out-come. A wide variety of parameters,
including thenumber and size of the giant cells, the mean numberof
nuclei per giant cell, the fractional surface areaoccupied by giant
cells, the DNA content, mitoticactivity, and the immunohisotologic
features havebeen studied in an attempt to distinguish
aggressiveand nonaggressive subtypesandto predict prognosisand
response to treatment.6-10 Aggressive/recurringlesions have been
found to have a higher number and
relative size index of giant cells and a greater frac-tional
surface area occupied by giant cells.6,8 Addi-tionally, aggressive
subtypes have been shown to ex-press a greater count of nucleolar
organizationregions.9
The angiogenic activity of GCLs was proposed as adeterminant of
the aggressive nature of GCLs. Veredet al11were unable to find
elevated vascular endothe-lial growth factor and fibroblast growth
factor in thesetumors and concluded that GCLs have low
angiogenicactivity. Dewsnup et al12 studied the expression ofCD34,
a cellcell adhesion factor and cell-surface gly-
coprotein found in hematopoietic precursor and cap-illary
endothelial cells. They determined that clinicallyaggressive giant
cell tumors have an increased vascu-lar density compared with
nonaggressive lesionsbased on CD34 staining. Furthermore, they
suggestedthat CD34 evaluation can identify aggressive
lesionsamenabletoantiangiogenic therapy, even at the timeof
biopsy.12 This same group subsequently showedthat CD34 staining
density levels of more than 2.5%
were associated with aggressive GCLs.13 These find-ings strongly
suggest that the CD34 staining densitylevel has a high positive
predictive value for biologicbehavior and might help in planning
treatment and
predicting outcome.One treatment of GCLs is enucleation and
curet-
tage, with or without adjunctive therapy, such asperipheral
ostectomy1 and liquid nitrogen cryothera-py.14 Although
nonaggressive lesions of the jaw aresuccessfully managed with
curettage and have a lowrecurrencerate, aggressive lesions have a
recurrencerate of 70%.15
The gold standard forthetreatment of aggressiveGCL is en bloc
resection.16 Given that these lesionsfrequently occur in children
and resection of vitalstructures for treatment of a benign lesion
can result
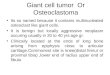
FIGURE 1. A, OPG at the time of presentation. B, Axial
computedtomography scan shows multilocular appearance of the lesion
witherosion of both lingual and vestibular cortices. C,
Photomicrographshowing mass of granulationlike tissue containing
numerous oste-oclastlike giant cells with scattered inflammatory
and hemosiderinladen macrophages. Areas of hemorrhage are present.
Inset: Oc-casional bone formation is evident with above features
(H&E stain-ing; 100).
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
2538 AGGRESSIVE CENTRAL GIANT CELL GRANULOMA OF THE MANDIBLE
-
8/11/2019 Aggressive Central Giant Cell
3/8
in functional, esthetic, and psychological problems,alternatives
to resection have been attempted.17
These have included intralesional steroids, systemiccalcitonin,
and systemic interferon alpha-2a com-bined with curettage.18-20
Vered et al17 immunohistochemically stainedmononuclear and giant
cells for glucocorticoid and
calcitonin receptors in an attempt to provide a reli-able and
practical tool for selecting an appropriatetherapeutic agent to
treat GCLs. They found that themononuclear and giant cells of GCLs
stained for bothglucocorticoid and calcitonin receptors. Flanagan
etal21 proposed intralesional corticosteroid for GCLs.Their
reasoning was that multinucleated giant cellsare osteoclasts and
dexamethasone has been shownto inhibit osteoclast-like cells in
marrow cultures.22
Jacoway et al23 noted the microscopic similaritiesbetween
sarcoidosis and GCLs and also suggestedtreatment with
corticosteroids. A few successful case
reports have been published of GCLs treated byweekly
intralesional injection with corticoste-roids.18,24-26 However, it
is unclear from these reports
whether the lesions treated with corticosteroids
werenonaggressive or aggressive subtypes. The smatteringof case
reports does not allow surgeons to evaluatethe clinical
effectiveness of this therapy. A large seriesor a randomized trial
with reported success rates in alltypes of lesions is necessary to
adequately evaluatethis treatment.
Giant cells in GCLshave also been shown to havecalcitonin
receptors.27 Calcitonin inhibits osteoclast/
giant cell function andhas been suggested as a treat-ment
modality. Harris28 also noted the similaritiesbetween GCLs and the
brown tumor of hyperparathy-roidism and hypothesized that GCLs
might respond tocalcitonin. The results with calcitonin therapy
have
varied; it has had no effect in some patients, andothers have
developed resistance, which occurs be-cause of a loss of
receptors.17,29 Some patients seemto respond, although these case
reports did not ap-pear to include patients with aggressive
lesions.19,30
A randomized double-blind placebo-controlledstudy in 14 patients
treated with calcitonin nasalspray showed a reduction in tumor
volume of 10% or
more in 7 of 14 patients; however, complete remis-sion was not
observed. This group studied the re-sponse in both aggressive and
nonaggressive subtypesand found a reduction/stabilization of tumor
size innonaggressive lesions. However, decrease in tumorsize was
variable in patients with aggressive lesions.They hypothesized that
the lack of predictable results
was related to an insufficient calcitonindosage andthe short
(6-month) follow-up period.31
Kaban et al15 proposed that GCLs are proliferativevascular
lesions that are, in part, angiogenesis-depen-dent. They theorized
that aggressive GCLs would re-
spond to antiangiogenic therapy.15 They reported anindex case
treated with interferon alpha-2a.32 Inter-feron alpha-2a inhibits
angiogenesis and has beenused to treat infantile hemangiomas and
other vascu-lar tumors.33-35 Interferon has also been shown
toinhibit osteoclastic bone resorption and to stimulateosteoblasts
and preosteoblasts in cell culture.15,36,37
Adverse effects include fever, influenza-like symp-toms,
lethargy, postnasal drip, skin rash and hair loss,neutropenia,
thrombocytopenia, elevated livertransaminase,and spastic
diplegia.34,38 In the series ofKaban et al,15 15% of subjects
developed significantside effects that limited interferon
administration andnecessitated alternative therapies.
de Lange et al19 described 2 patients in whomcalcitonin therapy
failed, who were then treated withinterferon alpha-2a without
surgical debulking. Theynoted limited regression (40%) of the
lesion.19 Kabanet al20 proposed combined treatment of
aggressive
GCLs with curettage, maintaining vital structures(teeth and
nerve), and adjuvant therapy with inter-feron alpha-2a beginning 48
to 72 hours postopera-tively. They reported successful tumor
control withdecreased operative morbidity compared with enbloc
resection.20 Of 26 patients, 16 were cured ofdisease, 6 were in
remission, and 4 were in activetreatment.
Based on the clinical and radiographic examination,this patient
has an aggressive GCL of the mandible.CD34 staining of the biopsy
specimen is recom-mended to confirm the aggressive subtype.12
The
lesion should be debulked/enucleated with preserva-tion of vital
structures (nerve and teeth). Per theprotocol developed by Kaban et
al,20 between 48 to72 hours postoperatively, interferon-alpha-2a
(Ro-feron-A, Roche Laboratories, Nutley, NJ) or interferon-alpha-2b
(Intron A, Schering, Kenilworth, NJ) shouldbe started at a dose of
3,000,000 U/m2, administeredonce daily by subcutaneous injection.
The patientshould be monitored for adverse effects, including
FIGURE 2. OPG after 3 months of calcitonin therapy (4
monthsafter presentation): progression of the lesion is obvious in
compar-ison with initial film.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
SCHTZ ET AL 2539
-
8/11/2019 Aggressive Central Giant Cell
4/8
flu-like symptoms, fever, lethargy, postnasal drip, skinrash,
and hair loss. Hematocrit, hemoglobin, whiteblood cell and platelet
counts, and liver function testsshould be obtained every 6
weeks.
Significant side effects, neutropenia (absolute neu-trophil
count 1,000 K/m3), thrombocytopenia, el-evated liver transaminase
values (greater than 5-foldincrease above normal), or the
development of anti-thyroid antibodies are indications to stop
therapy orreduce the interferon dosage. A panoramic radio-graph
should be obtained immediately postopera-tively, at 6 and 12 weeks
postoperatively, and at3-month intervals thereafter until the
defect is filled
with bone. At that time, computed tomography canbe used to
confirm bone regeneration and interferontherapy can be
discontinued. A patient can be con-
sidered cured if no evidence has been found of a GCL2 years
after completion of therapy.20
This case serves to illuminate the challenges clini-cians face
when treating patients with GCL of the jaw.Understanding the
etiopathogenesis of this lesion andidentifying markers for behavior
subtypes that canguide the best treatment of patients are exciting
op-
portunities for additional study.
Subsequent Course
After evaluation of therapeutic options and consultationwith the
patients family, the decision was made to starttreatment with an
intranasal spray of calcitonin. The patientreceived a daily dose of
200 UI Miacalcin (Calcitonin-salmon) Nasal Spray (Novartis, Basel,
Switzerland) and withthis medication he left Kuwait for summer
holidays in hishome country.
On return from holidays 3 months later he presentedwith obvious
progression: his face was distinctly asymmetricand the OPG showed
expansion of osteolytic process thatnow extended from the right
canine to the left second molar(Fig 2). Calcitonin therapy was
discontinued, and the pa-tient received an intralesional injection
of 30 mg triamcin-olone acetonide (Kenacort-A 10; Bristol-Myers
Squibb, New
York, NY) mixed with local anesthetic. This injection
wasrepeated 3 times in 3-week intervals. The fourth application
was already difficult due to increased hardness of the
lesion.Two months after the last triamcinolone injection, the
OPGshoweddistinctive ossification of the lesion but no decreasein
size (Figs 3A,B). It was decided to perform reshaping ofthe
mandible with curettage of accessible portions of thelesion,
followed by antiangiogenic therapy with interferon-alpha.
The surgery was performed 8 months after the first pre-
sentation. Under general anesthesia, the lesion was exposedfrom
marginal paradental incision; the left mental nerve wasidentified
and protected, and the excess of mandibular bone
was resected using burs and chisels. Accessible soft por-tions
of the lesion were curettedtaking care to avoid rootapices and
inferior alveolar nerve (Fig 4). The postoperativehealing was
uneventful and the patient regained normalfacial appearance after
resolution of postoperative edema(Fig 5). The function of the
mental nerve was preserved.The patient was started on daily doses
of 3 MIU interferon-
FIGURE 3. A, OPG after the fourth injection of triamcinolone,
7months after presentation. There are signs of increased
ossification,but no decrease in size. B, Facial appearance of the
patient at thesame time.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
FIGURE 4.OPG taken immediately after surgical reshaping
andcurettage: note persistence of a substantial part of the
lesion.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
2540 AGGRESSIVE CENTRAL GIANT CELL GRANULOMA OF THE MANDIBLE
-
8/11/2019 Aggressive Central Giant Cell
5/8
alpha-2a (Roferon-A) subcutaneously 3 months after theoperation.
This delay was caused by the difficulty the familyfaced in
obtaining funding for this treatment, which is notcovered by health
insurance for non-Kuwaitis.
The treatment was supervised by a pediatric
oncologistexperienced in the administration of interferon.
Baselinecomplete blood cell count and liver function tests
wereobtained and repeated every 6 weeks. Minimal side effects
were recorded and the patient completed a 1-year treat-ment
course without interruption. Clinical examination andOPGs were
repeated at 6 weeks and then at 3-month inter-
vals. There were signs of gradualremodeling and return tonormal
trabecular pattern (Fig 6). One year after discontin-
uation of interferon therapy (3 years after initial
presenta-tion), the patient is without clinical symptoms and the
only
remaining radiologic abnormality is a small hyperostosis ofthe
mandibular margin in the right canine area (Fig 7).
Discussion
Central giant cell granuloma (CGCG) of the jaws isa benign
lesion histologically characterized by thepresence of giant cells
in cellular richly vascularizedstroma of spindle cells. Although
originally termed
giant cell reparative granuloma,4 it is not a granu-loma in the
strict histologic sense, and it is not repar-ative clinically,
often demonstrating neoplastic fea-
tures.
39
CGCG belongs together with giant cell tumor,brown tumor of
hyperparathyroidism, and cherubismto so-called GCLs, which can be
difficult to distinguishsolely by microscopic examination.9 Giant
cell tumorof the long bones is practically identical with CGCGof
the jaws on histopathologic examination, and isconsidered by some
authors as a manifestation of thesame disease, where age and local
factors are respon-sible for different clinical
characteristics.9,40,41
Clinical behavior of CGCG is variable. Some lesionsare
asymptomatic and slow growing and react favor-ably to simple
treatment with curettage; others arefast growing, painful, and lead
to teeth displacement
and root resorption, destruction of cortical bone, andfacial
deformity. This latter variant is termed aggres-sive subtype of
CGCGandhas a high recurrence rateafter simple curettage.9,42 So far
only clinical signsand symptoms and radiologic features have been
themain criteria to differentiate between nonaggressiveand
aggressive lesions.43 Recently, it was reportedthat higher levels
of glycoprotein CD34 are associated
with aggressive lesions and that CD34 staining densitylevel is a
test with a high sensitivity and specificity,and high
positivepredictive value for the biologicalbehavior of
GCLs.12,13
FIGURE 5.Facial appearance of the patient 8 months after
oper-ation, during interferon-alpha therapy.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
FIGURE 6.OPG at the time of discontinuation of interferon
alphatherapy: nearly complete remodeling of the mandible is
obvious.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
FIGURE 7. Follow-up OPG 1 year after discontinuation
oftherapy.
Schtz et al. Aggressive Central Giant Cell Granuloma of
TheMandible. J Oral Maxillofac Surg 2010.
SCHTZ ET AL 2541
-
8/11/2019 Aggressive Central Giant Cell
6/8
The etiology of CGCG remains unknown, but theoccurrence of CGCG
in patients with anomalies witha known genetic origin such as
neurofibromatosistype 1 and Noonan syndrome suggests that a
genetic-related etiology might be possible.43 Because only
1instance of familial giant cell granuloma occurrencehas been
reported, DNA aberration probably occursspontaneously in a specific
group of cells, causing thefocal lesions, and is not
hereditary.44
Conventional therapycurettage or resectioncan result in loss of
teeth, facial disfigurement, oreven discontinuity defects of the
jaws in advancedcases.1,14,45,46 Moreover, overall recurrence
ratesrange from 11% to 49% for curettage alone43 and canbe as high
as 72% for aggressive subtype.42
In an effort to avoid deleterious consequences ofradical
surgical treatment, different pharmacologictherapies based on
presumptions regarding origin oflesional cells were arbitrarily
used with different suc-
cess. These included intralesional application of
cor-ticosteroids and systemic treatment with
calcitonin,interferon-alpha, imatinib, or bisphosphonates.
The earliest of these nonsurgical therapeutic strat-egies was
the intralesional application of corticoste-roid proposed in 1988
by Jacoway et al.24,47 Theoriginal rationale stated for this
treatment was his-topathologic resemblance of CGCG to
sarcoid.24
However this resemblance is only superficial andCGCG lesions
lack macrophage granulomas character-istic for sarcoid, as was
shown immunohistochemi-cally.48 A contemporary explanation for the
effect of
corticosteroid therapy on CGCG is the inhibition ofextracellular
production of lysosomal proteases andapoptotic action on
osteoclast-like cells.49 On theother hand, corticosteroids are also
known to en-hance bone resorption; some cases are unresponsiveto
corticosteroid therapy or may even display accel-erated
growth.48
Calcitonin therapy of CGCG was introduced as analternative
treatment of aggressive CGCG by Har-ris28 in 1993. It is based on
the discovery of expres-sion of several osteoclast-specific
characteristics bythe giant cells in CGCG.21 According to
contempo-
rary knowledge, osteoclasts are not the proliferat-ing tumor
cells in CGCG, but they differentiatefrom peripheral blood
mononuclear cells that ex-press its receptor activator of nuclear
factor B(RANK). Expression of RANK is a necessary step inthe origin
of osteoclasts. Differentiation takes placeunder the influence of
proliferating spindle-shapedstroma cells expressing cytokine
RANKL.50 Calcito-nin, peptide hormone produced by the C-cells of
thethyroid gland, inhibits the bone-resorbing activity
ofosteoclasts. The mechanism of action of calcitoninremains
unclear.51
de Lange et al19 successfully treated 4 patients withcalcitonin
and Pogrel48 achieved complete remissionin 8 of 10 patients;
however, de Lange et al52 did notget the same favorable results in
any of their later 14patients. Review21 of previously reported
series fromthe English-language literature with the addition of
5new cases showed that of a total 34 reported casestreated
exclusively with calcitonin, 22 (64.7%) achievedcomplete
resolution. In the other 12 cases, additionalsurgical curettage or
excision was necessary. The calci-tonin administration course in
this group ranged be-tween 6 and 64 months, with a mean of 23.9
months.
Recently, it was reported that the relative percent-age of
immunohistochemically stained mononuclearand giant cells for
calcitonin and/or glucocorticoidreceptors in CGCG can serve as a
tool for selectingeither calcitonin or glucocorticoid
therapy.17
Employment of interferon-alpha in the managementof aggressive
variant of CGCG, which is usually highly
vascularized, was inspired by its earlier success in
thetreatment of infantile hemangiomas.53 Interferon-alpha is a
cytokine with immunomodulatory andantiangiogenic properties.
Interferon-alpha therapylimits proliferation of various neoplastic
lesions bydepriving them of neovascular supply. The mecha-nism of
action of interferon is the inhibition of pro-duction of
angiogenesis stimulators: vascular endothe-lial growth factor and
basic fibroblast growth factor.Recent research suggests that CGCG
is not a trueproliferative vascular lesion, but the
immunoreactiv-ity of the lesional cells for angiogenic factors is
as-
sumed to play an important role in the osteoclasto-genesis
process contributing to the growth of thelesion.11
Interferon-alpha was introduced into clinical appli-cation in
1989 to treat a child with pulmonary heman-giomatosis, and later
the use of interferon alpha-2a
was reported for treating life-threatening hemangio-mas and
other vascular tumors.20 The first knowncase report of treatment of
a CGCG with alpha-2a-interferon was published in 1999 by Kaban et
al.32
This was followed by subsequent reports on success-ful
application of a treatment protocol combining
conservative surgery with postoperative adjuvanttreatment by
interferon-alpha in 26 patients.15,20
Bisphosphonates are used in the treatment of os-teoporosis,
hypercalcemia of malignancy, Pagets dis-ease, multiple myeloma, and
various skeletal metasta-ses. Landesberg et al54 suggested
employment ofbisphosphonates as a primary or adjunctive
treatmentfor GCLs of the jaws, giant cell tumors of the
appen-dicular skeleton, pediatric osteogenesis imperfecta, fi-brous
dysplasia, Gauchers disease, and osteomyelitis.They reported on the
treatment of 3 patients with GCLsof the jaws, the term they prefer
over CGCG. Only 1
2542 AGGRESSIVE CENTRAL GIANT CELL GRANULOMA OF THE MANDIBLE
-
8/11/2019 Aggressive Central Giant Cell
7/8
case managed by a single infusion of zoledronic acid
wascompletely successful.
Another addition to the arsenal of anti-osteolyticagents is
imatinib. Imatinib is a protein tyrosine kinaseinhibitor that is
used to treat chronic myeloid leukemiaand gastrointestinal stromal
tumors. The effect of ima-tinib on osteoclasts is a dose-dependent
decrease inRANK.55 de Lange et al56 reported on treatment of
apatient with Stickler syndrome and an aggressive CGCGof the
mandible by a combination of interferon-alphaand imatinib after the
failure of initial treatment withintralesional corticosteroid and
systemic calcitonin.
Our patient fulfilled criteria42 for diagnosing aggres-sive
variant of CGCG: lesion larger than 5 cm, teethdisplacement with
root resorption, cortical bone ero-sion documented by computed
tomography examina-tion. The extent of the lesion made
conventionalconservative surgical treatment (curettage)
unfeasibleand the only viable surgical option was segmental
resection with continuity defect reconstruction bytransfer of
microvascular free bone flap, followed byplacement of implants and
prosthetic rehabilitation.Such a procedure would have burdened the
patient
with considerable surgical morbidity, cosmetic con-sequences,
and financial expenses.
From available alternative pharmacological thera-pies, we
decided on intranasal application of salmoncalcitonin as the first
line of treatment. Intranasalspray can be easily self-administered
and is accompa-nied by minimal side effects.19,51,52 No regular
labo-ratory monitoring is necessary. On the other hand
intralesional application of corticosteroid is painfuland
necessitates regular office visits. Interferon-alphaas monotherapy
can stabilize the lesion or lead topartial regression,31 but its
administration can be ac-companied by serious side effects and
therefore re-quires regular laboratory monitoring.15,57
No improvement can be expected in x-ray examina-tion for the
first 4 to 6 months of calcitonin therapy48;however, our patient
displayed obvious progression,clinically and radiologically, 3
months after the initia-tion of treatment, and his parents were
alarmed andnot willing to continue obviously ineffective treat-
ment. This lack of response prompted us to switchtherapy to
intralesional corticosteroids. Triamcino-lone acetonide
administration achieved considerableossification of the lesion,
making it amenable to re-shaping, but no reduction in size, and
intolerablecosmetic deformity persisted. Subsequent conserva-tive
surgical intervention was successful in full cos-metic
rehabilitation of the patient without any dele-terious consequences
like loss of teeth, external scars,or neurosensory deficit. The
following adjuvant ther-apy with interferon-alpha was based on the
latesttherapeutic recommendations available at that time58
and achieved its goal despite the initial delay causedby social
circumstances of the patients family.
The presented case illustrates that perseveranceand employment
of all available therapeutic optionscan optimize the results of
management of aggressiveCGCG and spare the patients mutilating
surgery thatdoes not seem any more justifiable as the first line
oftreatment.
References
1. Eisenbud L, Stern M, Rothberg M, et al: Central giant
cellgranuloma of the jaws: Experiences in the management
ofthirty-seven cases. J Oral Maxillofac Surg 46:376, 1988
2. Cohen MM Jr, Gorlin RJ: Noonan-like/multiple giant cell
lesionsyndrome. Am J Med Genet 40:159, 1991
3. Idowu BD, Thomas G, Frow R, et al: Mutations in SH3BP2,
thecherubism gene, were not detected in central or peripheralgiant
cell tumors of the jaw. Br J Oral Maxillofac Surg 46:229,2008
4. Jaffe HL: Giant-cell reparative granuloma, traumatic bone
cyst,
and fibrous (fibro-osseous) dysplasia of the jawbones. Oral
SurgOral Med Oral 6:159, 1953
5. Liu B, Yu S-F, Li T-J: Multinucleated giant cells in various
formsof giant cell containing lesions of the jaws express features
ofosteoclasts. J Oral Pathol Med 32:367, 2003
6. Chuong R, Kaban LB, Kozakewich H, et al: Central giant
celllesions of the jaws: A clinicopathologic study. J Oral
MaxillofacSurg 44:708, 1986
7. Eckardt A, Pogrel MA, Kaban LB, et al: Central giant cell
gran-ulomas of the jaws: Nuclear DNA analysis using image
cytom-etry. Int J Oral Maxillofac Surg 18:3, 1989
8. Ficarra G, Kaban LB, Hansen LS: Central giant cell lesions of
themandible and maxilla: A clinicopathologic and cytometricstudy.
Oral Surg Oral Med Oral Pathol 64:44, 1987
9. Whitaker SB, Waldron CA: Central giant cell lesions of the
jaws.Oral Surg Oral Med Oral Pathol 75:199, 1993
10. OMalley M, Pogrel MA, Stewart JC, et al: Central giant
cellgranulomas of the jaws: Phenotype and
proliferation-associatedmarkers. J Oral Pathol Med 26:159, 1997
11. Vered M, Buchner D, Dayan D: Giant cell granulomas of
thejawbonesA proliferative vascular lesion? Immunohistochem-ical
study with vascular endothelial growth factor and basicfibroblast
growth factor. J Oral Pathol Med 35:613, 2006
12. Dewsnup NC, Susarla SM, Abulikemu M, et al:
Immunohisto-chemical evaluation of giant cell tumors of the jaws
using CD34density analysis. J Oral Maxillofac Surg 66:928, 2008
13. Susarla SM, August M, Dewsnup N, et al: CD34 staining
densitypredicts giant cell tumor clinical behavior. J Oral
MaxillofacSurg 67:951, 2009
14. Webb DJ, Brockbank J: Combined curettage and
cryosurgicaltreatment for the aggressive giant cell lesion of the
mandible.Int J Oral Maxillofac Surg 5:780, 1986
15. Kaban LB, Troulis MJ, Wilkinson MJ, et al: Adjuvant
antiangio-genic therapy for giant cell tumors of the jaws. J Oral
Maxillo-fac Surg 65:2018, 2007
16. Tosco P, Tanteri G, Iaquinta D, et al: Surgical treatment
andreconstruction for central giant cell granuloma of the jaws:
Areview of 18 cases. J Craniomaxillofac Surg 37:380, 2009
17. Vered M, Buchner A, Dayan D: Immunohistochemical expres-sion
of glucocorticoid and calcitonin receptors as a tool forselecting
therapeutic approach in central giant cell granulomasof the
jawbones. J Oral Maxillofac Surg 35:756, 2006
18. Kermer C, Millesi W, Watzke IM: Local injection of
corticoste-roids for central giant cell granuloma: A case report.
Int J OralMaxillofac Surg 23:36, 1994
19. de Lange J, Rosenberg AJ, van den Akker HP, et al:
Treatmentof central giant cell granuloma of the jaw with
calcitonin. Int
J Oral Maxillofac Surg 28:372, 1999
SCHTZ ET AL 2543
-
8/11/2019 Aggressive Central Giant Cell
8/8
20. Kaban LB, Troulis MJ, Ebb D, et al: Antiangiogenic therapy
withinterferon alpha for giant cell lesions of the jaws. J Oral
Max-illofac Surg 60:1103, 2002
21. Flanagan AM, Nui B, Tinkler SMB, et al: The multinucleate
cellsin the giant cell granulomas of the jaw are osteoclasts.
Cancer62:1139, 1988
22. Pharoah MJ, Heersche JNM: Dexamethasone inhibits formationof
osteoclast-like cells in bone-marrow cultures. J Dent Res65:1006,
1986
23. Jacoway JR, Howell FV, Terry BC: Central giant cell
granu-lomaAn alternative to surgical therapy. J Oral Surg
5:572,1988
24. Terry BC, Jacoway JR: Management of central giant cell
lesions:An alternative to surgical therapy. Oral Maxillofac Surg
ClinNorth Am 6:579, 1994
25. Rajeevan NS, Soumithran CS: Intralesional corticosteroid
injec-tion for central giant cell granuloma: A case report. Int J
OralMaxillofac Surg 27:303, 1998
26. Comert E, Turanli M, Ulu S: Oral and intralesional
steroidtherapy in giant cell granuloma. Acta Otolaryngol 26:664,
2006
27. Nicholson GC, Horton MA, Sexton PM, et al: Calcitonin
recep-tors of human osteoclastoma. Horm Metab Res 19:585, 1987
28. Harris M: Central giant cell granulomas of the jaws regress
withcalcitonin therapy. Br J Oral Maxillofac Surg 31:89, 1993
29. Pondel M: Calcitonin and calcitonin receptors: Bone and
be-
yond. In J Exp Pathol 81:405, 200030. Pogrel MA, Regezi JA,
Harris ST, et al: Calcitonin treatment for
central giant cell granulomas of the mandible: Report of
twocases. J Oral Maxillofac Surg 57:848, 1999
31. de Lange J, van den Akker HP, van den Berg H, et al:
Limitedregression of central giant cell granulomas by interferon
alphaafter failed calcitonin therapy: A report of 2 cases. J
OralMaxillofac Surg 35:865, 2006
32. Kaban LB, Mulliken JB, Ezekowitz A, et al:
Antiangiogenictherapy of a recurrent giant cell tumor of the
mandible withinterferon alpha-2a. Pediatrics 103:1145, 1999
33. Sidky YA, Borden EC: Inhibition of angiogenesis by
interferons:Effects on tumor and lymphocyte-induced vascular
responses.Cancer Res 47:5155, 1987
34. Ezekowitz RAB, Mulliken JB, Folkman J: Interferon
alpha-2atherapy for life-threatening hemangiomas of infancy. N
Engl
J Med 326:1456, 1992. Erratum 330:300, 199435. Mulliken JB, Boon
LM, Takahashi K, et al: Pharmacologic ther-apy for endangering
hemangiomas. Curr Opin Dermatol 2:109,1995
36. Abukawa H, Kaban, LB, Williams WB, et al: Effect of
interferonalpha-2b on porcine mesenchymal stem cells. J Oral
MaxillofacSurg 64:1214, 2006
37. Takayanagi H, Kim S, Matsuo K, et al: RANKL maintains
bonehomeostasis through c-Fos-dependent induction of
interferon-beta. Nature 416:774, 2002
38. Barlow CF, Priebe CJ, Mulliken JB, et al: Spastic diplegia
as acomplication of interferon alfa-2a treatment of hemangiomas
ofinfancy. J Pediatr 132:527, 1988
39. Batsakis JG: Non-odontogenic tumors: Clinical evaluation
andpathology, in Thawley SE, Panje WR, Batsakis JG, Lindberg
RD(eds): Comprehensive management of head and neck
tumors.Philadelphia, PA, WB Saunders, 1999
40. Auclair PL, Cuenin P, Kratochvil FJ, et al: A clinical and
histo-morphologic comparison of the central giant cell
granuloma
and the giant cell tumor. Oral Surg Oral Med Oral Pathol66:197,
1988
41. Al Sheddi M, Mosadomi H, Al Dayel F: Central giant cell
gran-uloma of the jaws and giant cell tumor of long bones.
Aclinicopathologic, cytometric, and immunohistochemical
com-parative study. Oral Surg Oral Med Oral Pathol Oral RadiolEndod
98:195, 2004
42. Chuong R, Kaban LB, Kozakewich H, et al: Central giant
celllesions of the jaws: A clinicopathologic study. J Oral
Maxillofac
Surg 44:714, 198643. de Lange J, van den Akker HP, van den Berg
H: Central giant
cell granuloma of the jaw: A review of the literature
withemphasis on therapy options. Oral Surg Oral Med Oral PatholOral
Radiol Endod 104:603, 2007
44. de Lange J, van Maarle MC, van den Akker HP, et al:
DNAanalysis of the SH3BP2 gene in patients with aggressive
centralgiant cell granuloma. Br J Oral Maxillofac Surg 45:499,
2007
45. Tallan EM, Olsen KD, McCaffrey TV, et al: Advanced giant
cellgranuloma: A twenty-year study. Otolaryngol Head Neck
Surg110:413, 1994
46. Kruse-Lsler B, Diallo R, Gaertner C, et al: Central giant
cellgranuloma of the jaws: A clinical, radiologic, and
histopatho-logic study of 26 cases. Oral Surg Oral Med Oral Pathol
OralRadiol Endod 101:346, 2006
47. Jacoway JR, Howell FV, Terry BC: Central giant cell
granulomaAnalternative to surgical therapy. Oral Surg Oral Med Oral
Pathol 66:572, 1988
48. Pogrel MA: Calcitonin therapy for central giant cell
granuloma.J Oral Maxillofac Surg 61:649, 2003
49. Carlos R, Sedano HO: Intralesional corticosteroids as an
alter-native treatment for central giant cell granuloma. Oral
SurgOral Med Oral Pathol Oral Radiol Endod 93:161, 2002
50. Itonaga I, Hussein I, Kudo O, et al: Cellular mechanisms
ofosteoclast formation and lacunar resorption in giant cell
gran-uloma of the jaw. J Oral Pathol Med 32:224, 2003
51. Allon DM, Anavi Y, Calderon S: Central giant cell lesion of
thejaw: Nonsurgical treatment with calcitonin nasal spray. OralMed
Oral Pathol Oral Radiol J Endod 107:811, 2009
52. de Lange J, van den Akker HP, Veldhuijzen van Zanten GO, et
al:Calcitonin therapy in central giant cell granuloma of the jaw:
Arandomized double-blind placebo-controlled study. Int J Oral
Max-illofac Surg 35:791, 2006
53. Kaban LB: Biomedical technology revolution: Opportunitiesand
challenges for oral and maxillofacial surgeons. Int J
OralMaxillofac Surg 31:1, 2002
54. Landesberg R, Eisig S, Fennoy I, et al: Alternative
indications forbisphosphonate therapy. J Oral Maxillofac Surg
67(Suppl. 1):27, 2009
55. Dewar AL, Farrugia AN, Condina MR, et al: Imatinib as
apotential antiresorptive therapy for bone disease. Blood 107:4334,
2006
56. de Lange J, van Rijn RR, van den Berg H, et al: Regression
ofcentral giant cell granuloma by a combination of imatiniband
interferon: A case report. Br J Oral Maxillofac Surg47:59, 2009
57. Goldman KE, Marshall MK, Alessandrini E, et al:
Complicationsof alpha-interferon therapy for aggressive central
giant celllesion of the maxilla. Oral Surg Oral Med Oral Pathol
Oral
Radiol Endod 100:285, 200558. Kaban LB, Dodson TB: Management of
giant cell lesions. IntJ Oral Maxillofac Surg 35:1074, 2006
2544 AGGRESSIVE CENTRAL GIANT CELL GRANULOMA OF THE MANDIBLE