Embed Size (px)
Citation preview
PERCEPTIONS OF RECENT WITS PHYSIOTHERAPY GRADUATES REGARDING THE ORTHOPAEDIC
MANIPULATIVE THERAPY (OMT) UNDERGRADUATE CURRICULUM CONTENT
ANITA .S. GOUNDEN
A research report submitted to the Faculty of Health Sciences, University of the
Witwatersrand, in partial fulfillment for the requirements for the degree of Master
of Science in Physiotherapy
Johannesburg, 2005
DECLARATION
I, Anita S. Gounden declare that this research report is my own work. It is being
submitted for the degree of Master of Science in Physiotherapy at the University
of the Witwatersrand, Johannesburg. It has not been submitted before for any
degree or examination at this or any other University.
__________________
A. S. Gounden
____________day of ________________2005
ABSTRACT
Orthopaedic manipulative therapy (OMT) like other areas of physiotherapy, is a
rapidly advancing field. To keep abreast of changes, curricula need regular
evaluation and updating. The curriculum consists of many components that may
vary from content to timetabling.
The aim of this study was to determine how past graduates from the University of
the Witwatersrand perceived the OMT curriculum with regards to content,
teaching methods and clinical learning. This information will contribute to an
overall evaluation of the present OMT curriculum.
The sample consisted of graduates from 1997-1999. Questionnaires and
interviews were used to gather the information. Some interviews were carried out
following analysis of answers to the questionnaire to clarify issues or gain
additional information.
Results indicated that eighty one percent of the sample found the content
relevant to clinical practice, but forty two percent found certain aspects of the
content inadequate. The following areas of content were deficient: sixty percent
found information on patient education, advice and counseling related to OMT
inadequate. Fifty five percent would have liked to be more exposed to research in
this area. Sixty seven percent felt that teaching of clinical reasoning skills was
lacking. Ninety four percent would have liked information on other joint
mobilization concepts.
It was perceived that active learning methods were more effective than passive
learning methods. Fifty eight percent found tutorials, sixty eight percent found
practical sessions, and fifty eight percent found workshops very effective.
With regards to clinical learning, seventy seven percent found supervision very
helpful in clinical placements. Eighty one percent found patient presentations
helpful, and seventy one percent found discussion of patients with lecturers very
helpful.
Most responses indicated that the OMT curriculum was relevant to current
practice in South Africa but inadequate in certain specific areas.
ACKNOWLEDGEMENTS Jill Giraud (supervisor)
Aimee Stewart (supervisor)
Eugene Senewana
Piet Bekker
Judy Hahn
Marge Steffan
Past graduates who responded to the questionnaire
LIST OF ABBREVIATIONS AND DEFINITIONS Wits University of the Witwatersrand
OMT Orthopaedic manipulative therapy: Refers to a specialist area in
physiotherapy that deals with the management of
neuromusculoskeletal conditions.
Other titles for this area of speciality:
NMS Neuromusculoskeletal therapy
MT Manual therapy
SMT Spinal manipulative therapy
HPCSA Health Professions Council of South Africa
SAQA South African Qualifications Authority
NQF National Qualifications Framework
SGB Standards Generating Body
ETQA Education training Quality Assurance Body
CAM Complementary and alternative therapies
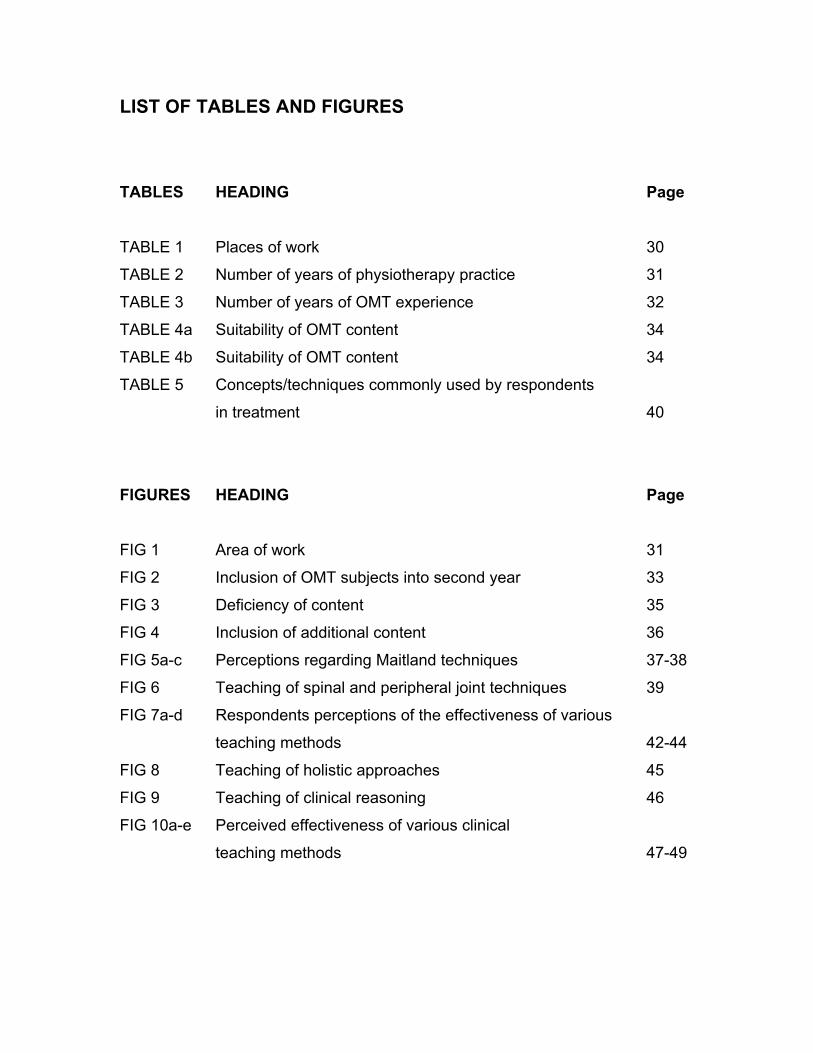
LIST OF TABLES AND FIGURES TABLES HEADING Page TABLE 1 Places of work 30
TABLE 2 Number of years of physiotherapy practice 31
TABLE 3 Number of years of OMT experience 32
TABLE 4a Suitability of OMT content 34
TABLE 4b Suitability of OMT content 34
TABLE 5 Concepts/techniques commonly used by respondents
in treatment 40
FIGURES HEADING Page
FIG 1 Area of work 31
FIG 2 Inclusion of OMT subjects into second year 33
FIG 3 Deficiency of content 35
FIG 4 Inclusion of additional content 36
FIG 5a-c Perceptions regarding Maitland techniques 37-38
FIG 6 Teaching of spinal and peripheral joint techniques 39
FIG 7a-d Respondents perceptions of the effectiveness of various
teaching methods 42-44
FIG 8 Teaching of holistic approaches 45
FIG 9 Teaching of clinical reasoning 46
FIG 10a-e Perceived effectiveness of various clinical
teaching methods 47-49
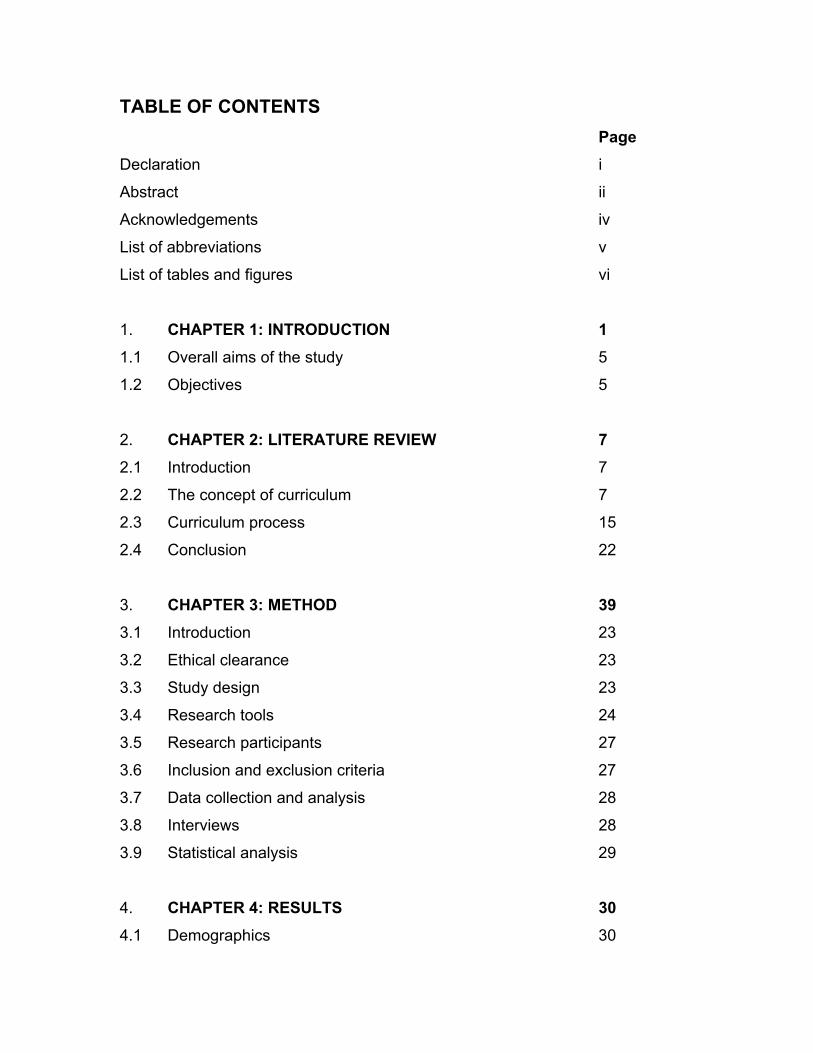
TABLE OF CONTENTS Page Declaration i
Abstract ii
Acknowledgements iv
List of abbreviations v
List of tables and figures vi
1. CHAPTER 1: INTRODUCTION 1 1.1 Overall aims of the study 5
1.2 Objectives 5
2. CHAPTER 2: LITERATURE REVIEW 7 2.1 Introduction 7
2.2 The concept of curriculum 7
2.3 Curriculum process 15
2.4 Conclusion 22
3. CHAPTER 3: METHOD 39 3.1 Introduction 23
3.2 Ethical clearance 23
3.3 Study design 23
3.4 Research tools 24
3.5 Research participants 27
3.6 Inclusion and exclusion criteria 27
3.7 Data collection and analysis 28
3.8 Interviews 28
3.9 Statistical analysis 29
4. CHAPTER 4: RESULTS 30 4.1 Demographics 30
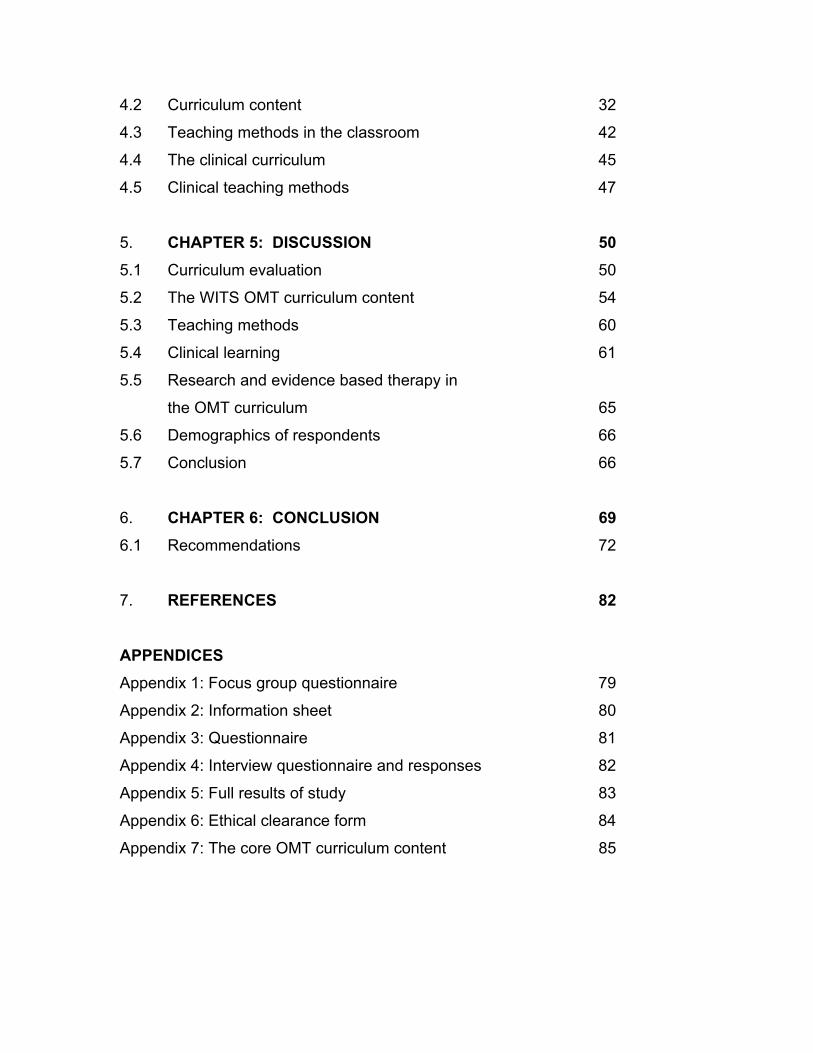
4.2 Curriculum content 32
4.3 Teaching methods in the classroom 42
4.4 The clinical curriculum 45
4.5 Clinical teaching methods 47
5. CHAPTER 5: DISCUSSION 50 5.1 Curriculum evaluation 50
5.2 The WITS OMT curriculum content 54
5.3 Teaching methods 60
5.4 Clinical learning 61
5.5 Research and evidence based therapy in
the OMT curriculum 65
5.6 Demographics of respondents 66
5.7 Conclusion 66
6. CHAPTER 6: CONCLUSION 69 6.1 Recommendations 72
7. REFERENCES 82
APPENDICES Appendix 1: Focus group questionnaire 79
Appendix 2: Information sheet 80
Appendix 3: Questionnaire 81
Appendix 4: Interview questionnaire and responses 82
Appendix 5: Full results of study 83
Appendix 6: Ethical clearance form 84
Appendix 7: The core OMT curriculum content 85
CHAPTER ONE INTRODUCTION
The management of neuromusculoskeletal disorders is a dynamic and exciting
area of physiotherapy. This diverse and extensive field encompasses many
different assessment and treatment techniques.
In the present day context, these disorders may result from various causes e.g. a
sedentary posture at the computer, a muscle strain from a sporting activity, or a
traumatic injury from a motor vehicle accident. Physiotherapists, to manage
these patients, use orthopaedic manipulative therapy (OMT) assessment and
treatment concepts extensively. Significant developments were made in this field
during the late 1900’s.
OMT is taught to undergraduate physiotherapy students at all South African
physiotherapy training centres. The subject has evolved over time in accordance
with advancements in the field. It is important that curriculum content in this area
is evaluated and updated regularly. It may well be that course content may help
to determine the clinical competency of a graduate.
According to Sanson Fisher and Rolfe (2000), curriculum content determines
how well health-care professionals are prepared for their roles. It also impacts on
their levels of clinical competence and beliefs about which aspects are important
for good clinical care. Domination by particular content, for example, is likely to
be perceived by students as more important than other aspects, while
deficiencies in content deprive students of exposure to certain information.
The practice of OMT in the present day context is diverse with respect to
assessment and treatment skills. Treatment may involve joint, neural and soft
tissue mobilization, and exercise therapy. In addition, postural, functional and
ergonomic analysis may indicate further OMT management.
The treatment approach may vary from one therapist to another depending on
their exposure to various OMT concepts and recent OMT trends.
Undergraduate curricula in South African universities originally incorporated the
Maitland concept into the OMT curriculum. They used this concept as a basis for
OMT training. While this was appropriate, it is important that the present
curriculum also include other aspects related to OMT to make it suitable for
present day knowledge and practice. Besides including information on other
concepts, essential knowledge of movement and functional analysis for
neuromusculoskeletal conditions plays a vital role in management and should be
included. Important skills like psychosocial understanding, interpersonal
communication and relationships cannot be ignored. Also, the application of
theoretical knowledge to clinical practice and clinical reasoning skills are
immensely important in the practice of the profession.
Since 1994, physiotherapists became first line practitioners (Professional Board
for Physiotherapy, Podiatry and Biokinetics, HPCSA). Patients may therefore
seek treatment from a physiotherapist without doctors’ referrals. This privilege
comes with responsibility. Good basic diagnostic and treatment skills based on a
sound knowledge of anatomy, physiology, biomechanics and pathology are
crucial. The ability of physiotherapists to successfully and efficiently apply these
skills is often a reflection of their undergraduate training. This forms the basis of
their practice while additional learning (e.g. from postgraduate courses) and
clinical experience, will with time, develop knowledge and clinical reasoning.
Since 2003, new graduates do a year of community service. Supervision and
advice from more experienced colleagues may not always be available. The new
graduate therefore needs to rely on knowledge that was acquired at an
undergraduate level. In the light of this new responsibility, undergraduate training
needs to be of an appropriate standard. This standard should be compliant with
that which has been set by the Standards Generating Body (SGB) for
physiotherapy, which falls under the National Qualifications Framework (NQF).
The South African Qualifications Authority (SAQA) implements the NQF (SAQA
information booklet, 2000).
One way of assessing the standard of undergraduate education is to evaluate the
curriculum. It is then possible to check whether it is relevant and appropriate, and
adequately equips the student for the workplace.
Curriculum evaluation studies involve various classes of information, one being
‘supplemental information’. This includes opinions and views of people
concerning the curriculum. The stakeholders, who could participate in this type
of assessment, may be heads of departments, lecturers, senior clinicians, recent
graduates, students and patients. Students would be the most appropriate due to
their current involvement in the course. However, they lack clinical experience.
Therefore recent graduates could be an alternative given their recent experience
of the undergraduate curriculum and their current clinical role (Sanson-Fisher
and Rolfe, 2000).
Supplemental information is very useful in the evaluation process. One is able to
determine whether a discrepancy exists between what lecturers perceive to be
taking place and what is actually taking place. One may then be able to find out
what additional information is needed to see why students are holding these
views (Wolf, 1984). More importantly, responses of students with regards to
relevance of content can be assessed (Coles and Grant, 1985). This may help to
direct change so that the content included is appropriate for clinical practice in
South African communities. It will also contribute to updating the curriculum
taught in the physiotherapy department at the University of the Witwatersrand
making it relevant to the present context.
The OMT curriculum at the University of the Witwatersrand
The OMT curriculum presently taught at the University of the Witwatersrand
includes assessment of neuromusculoskeletal disorders, and treatment of these.
Treatment techniques that are taught include soft tissue techniques, joint
mobilisation according to the Maitland concept, neural mobilisation, and exercise
therapy.
Soft tissue techniques include myofascial release techniques, trigger point
therapy, deep transverse frictions, and massage. These are taught in the second
year of study and applied in clinical work in the third and fourth year of study.
Neurodynamic tests and treatment techniques are taught in third and fourth year.
Rehabilitation techniques, posture assessment and correction, movement
analysis and exercise therapy are taught in the second, third and fourth year
curriculum. All of the above are related to common pathologies encountered in
the clinical setting in South Africa.
Clinical work starts in the third and fourth years of study and eight weeks are
allocated for this. The students work under supervision provided by hospital
clinicians and university lecturers. Teaching methods used in the OMT course
include lectures, practical sessions, workshops, patient presentations and
discussions.
Following from this description, it would be important to assess whether the OMT
curriculum taught in the physiotherapy department at the University of the
Witwatersrand is up to date and includes sufficient and relevant information for
the undergraduate, on subjects like mobilisation techniques, analysis of posture,
movement and function. Besides actual OMT theory, the curriculum should also
address influencing factors on OMT management e.g. psychosocial and
communication skills. If appropriately designed, this curriculum will prepare
graduates, to an extent, to cater for the basic need (relating to OMT) of the South
African community. This will give them added confidence especially during the
year of community service. Acquiring past graduates’ views is an important part
of the evaluation process and will help answer the question as to whether the
OMT curriculum taught at the above department is suitable.
At the time of the research, the Maitland concept was briefly introduced in
second year. Soft tissue therapy was taught in 38 lectures and practical
sessions. The Maitland concept and peripheral joint mobilisation was taught in
detail in third year, together with neurodynamic testing and treatment in 34
lectures and practical sessions. Six small group tutorials on peripheral nerve
injuries, osteoarthritis and rheumatoid arthritis, the shoulder, posture, gait and
hand injuries were given.
In fourth year, the students were taught spinal assessments and treatments
including mobilization in eighteen lectures and practical sessions. Eleven
workshops and two practical sessions were held on various topics involving the
lumbar, thoracic and cervical spine, traction and back class. Six small group
tutorial topics included the shoulder, overuse injuries, headaches and the spine.
Clinical learning was done in the two OMT blocks in third and fourth year (four
weeks each year). The hospitals used were Johannesburg General Hospital,
Southrand Hospital, Tambo Memorial Hospital, and Helen Joseph Hospital for
third and fourth year. There were approximately six to seven students in each
block and therefore two at each clinical setting. They were supervised two to
three times in the block (Wits Physiotherapy Curriculum Books 2001 and 2002).
1.1 AIM OF THE STUDY
To determine whether Bachelor of Science physiotherapy graduates from the
University of the Witwatersrand consider the OMT undergraduate curriculum
content, teaching methods and clinical learning, adequate and relevant to clinical
practice.
1.2. OBJECTIVES
1. To determine the adequacy of curriculum content
2. To determine the relevance of teaching methods
3. To determine the adequacy of clinical learning
CHAPTER 2 LITERATURE REVIEW 2.1 INTRODUCTION The concepts of curriculum, curriculum evaluation and the general content of the
OMT curriculum are discussed. The concept of curriculum is a broad subject and
much has been written defining and explaining its many components. A general
outline of the concept is given. Information included pertains to the content and
teaching of the undergraduate OMT curriculum in the physiotherapy department
at the University of the Witwatersrand.
2.2 THE CONCEPT OF CURRICULUM
2.2.1. Introduction Education revolves around the curriculum. The curriculum is used to transmit
messages and meanings and teach values (Hawes, 1982). Defining the
curriculum is difficult since people reflect their own perspectives in their
definitions. The curriculum has been described as the content of a subject, or
area of study, or the total programme of an educational institution. However, a
curriculum is not just a syllabus. It is influenced by the way the lecturer interprets
it and by the context in which he/she finds him/herself. Various factors influence it
e.g. the teaching environment, the timetable, relationships and the social context
(Squires, 1987).
The modern curriculum includes objectives and goals besides the content. In the
past, no statements were made about the goals to be achieved in the educational
process. Specifying objectives has caused lecturers to think their courses

through better, and has made it easier for students to know what is expected of
them (Squires, 1987).
The concept of curriculum includes content and process. Students process
content in various ways from the simple learning of facts to the more complex
activity of analysis and problem solving (Lowry, 1993). An example of the
process may be learning the anatomy and biomechanics of a joint, then
understanding how a specific pathology may affect joint structure and motion to
cause pain, and eventually understanding how to treat the cause and reduce
pain (Squires, 1987).
The obvious assumption is that all of these theoretical components in the
physiotherapy curriculum prepare the graduate for practice. However other
factors e.g. professional accreditation groups and regulatory bodies, clinicians,
students and lecturers, also influence the design of this particular curriculum
(Shepard and Jensen, 2002). This helps to make it relevant to the present
standards of practice and a country’s health care needs.
The curriculum should be of an acceptable standard i.e. that set by the
professional regulatory bodies in the country. The controlling regulatory body for
physiotherapy in South Africa is the Health Professions Council of South Africa
(HPCSA). The Standards Generating Body (SGB) is part of the HPCSA and sets
the standards for physiotherapy. The education and training quality assurance
body (ETQA) assures the quality of the training.
2.2.2. Goals and objectives of the curriculum
Goals A micro and macro environment influences goals of the physiotherapy
curriculum. The macro environment includes society, the health care
environment, the higher education system, and physiotherapy related knowledge.
Therefore an epidemic, for example, may need to be addressed by the
physiotherapy curriculum. In this country, we need to address the HIV epidemic.
Due to the impact of the disease on the population of the country, our curriculum
should be modified so that students are made sensitive and aware of the
resulting impact on society and their role in meeting the arising need. The
physiotherapy graduate should be sensitive and responsive to this need in
society.
The micro environment refers to the educational institution and clinical practice
settings. This environment also affects learning. Finally goals should always be
realistic, feasible and desirable (Shepard and Jensen, 2002).
Objectives The main objective of the design and operation of the curriculum is the teaching
of others. Objectives are expectations that should relate directly to the curriculum
goals. If a goal were to develop critical reasoning skills, then the objective would
be to create learning experiences that cause students to reflect and clinically
analyse. They are created to guide the coursework and prepare the students for
practice (Shepard and Jensen, 2002).
Different objectives may denote three kinds of behaviour viz. those concerned
with thinking (cognitive), feelings (affective) and physical actions
(motor/psychomotor) (Matthews, 1989). Objectives should be selected if there is
evidence that they will be of value to the learner, that they is attainable, and that
they will not be achieved unless it is taught (McNeil, 1996).
In physiotherapy, one may describe behavioral, problem solving, or outcome
objectives. Behavioural objectives are identified under the cognitive, affective and
psychomotor domains. The problem-solving objectives relate to a ‘problem’ given
to the student to solve e.g. working out an appropriate exercise programme for a
patient with a lumbar disc herniation. In this case, the student goes beyond
specific behaviours and will need to analyse and think through the problem,
coming up with a solution from the information they have acquired or the
materials they have been given. Outcome objectives are more broad-based and
involve expectations of students practice (Shepard and Jensen, 2002).
2.2.3. Curriculum content Content should include essential knowledge for practice and diverse knowledge.
“Core content should not be static, absolute or permanent”, but should be revised
intermittently to reflect global trends in healthcare and in education for
healthcare” (Bandaranayake, 2000).
a) General classifications of curriculum content There have been many recent classifications of content (Matthews, 1989).
Content may be summarized as:
1) Knowledge based: this may include actual subjects e.g. OMT.
2) Culture based: content should be related to the culture of the community it
serves. It should be sufficiently acceptable to all ethnic groups of that
community.
3) Employment based: content may be relevant to a specific profession for
example, to prepare the individual for the required tasks.
Content may be biased to one of the above types and curricula may stay this way
since staff may be trained and schools accustomed to teach this particular
content (Matthews, 1989). The OMT curriculum content includes all the above
types of content.
b) Breadth and Depth of content

The issue of the appropriate breadth and depth of undergraduate education is a
complex one. Students preferences of broader / narrower courses can only be
determined by surveys. In most professional courses, the scope is determined by
professional ‘needs’. Undergraduate students are developed to a certain level
only, after which they have the choice of specializing (Squires 1987).
c) Determination of curriculum content One way of determining curriculum content would be through job analysis. This is
observation of the actual utilization of concepts and techniques by various
practitioners in the field. Another way would be to ask qualified persons to
indicate what they would consider to be the minimum abilities needed for
practice. A third way would be surveying the needs of the population with respect
to the specialty, and then designing a course to meet those needs (McNeil,
1996).
Determining content again relates to the philosophy and goals of the
physiotherapy department concerned. If the philosophy were to educate
graduates to practice ethically in a diverse society, then the content would
include teaching of ethical behaviour paying attention to social and cultural
differences (Shepard and Jensen, 2002).
In addition to the techniques above, there are various models that may be used
to decide on content (McNeil, 1996). A needs assessment may be performed to
decide what is critically needed by society, therefore making content relevant to
society’s requirements. Resources are therefore being used in the most efficient
manner and society benefits most greatly. This model relates to the macro
environment and its influences on the curriculum as explained earlier. The
futuristic model anticipates future needs and structures the curriculum so that
students are trained to suit those needs. The rational model gives attention to the
learner, society, and fields of knowledge. It involves formulating educational

purposes, selecting and organizing educational experiences, and determines the
extent to which purposes are being attained (McNeil, 1996).
d) Inclusion of evidence based knowledge and research principles into curriculum content
Curriculum content should also be based on evidence from research done on
physiotherapy techniques and modalities. In this way, the knowledge included is
objective (distinguishing it from belief and opinion) (Kelly, 1987). Evidence-based
practice should best serve the needs of patients. Members of the profession
need to perform research to determine whether interventions work. It is therefore
important to help undergraduate students develop research skills (Connolly et al,
2001).
A longitudinal study done by Connolly et al (2001) examined the perception of
knowledge and behaviour of students with respect to research. There was a
change in a positive direction as students were exposed to research
experiences. They also showed confidence in their ability to critically review the
literature and accepted the responsibility of keeping updated on the most recent
information.
e) Intention and reality Finally, there is the concept of ’intention and reality’. There may be various
aspects one may like to include in the curriculum, but this is only possible in
theory. There may not be the time or staff or facilities available to teach them.
Therefore, putting it into practice becomes difficult (Kelly, 1987). For example, it
may be interesting for the student if many different concepts of joint mobilization
were presented in the curriculum to allow them more options for treatment.
However, there is not enough time to teach all these concepts. The student may
be exposed to a variety of interesting and relevant information in the clinical
setting, while in academic settings the emphasis is on theory and critical
analysis. Both perspectives are important in physiotherapy, but may not be
covered in-depth due to time constraints. Students should therefore be taught
how to constantly reflect on their clinical performance and identify their learning
needs so that they are able to continue their education following graduation.
To conclude this topic, another way of deciding on content is to determine current
skills demanded in clinical practice. Ultimately, the basic building blocks of
physiotherapy practice must be provided. These may include not just an array of
treatment techniques but information on teaching the patient and family how to
manage their own health care needs, information on effective teamwork, and
physiotherapy assistant roles (Shepard and Jensen, 2002). Skills that may be
attained later e.g. alternative joint mobilization concepts can be excluded. What
lecturers need to ensure is that graduates are able to work in the present health
care environment, and that the qualification meets the requirements of the
Professional Board for Physiotherapy, Podiatry and Biokinetics.
f) The explicit, implicit and null curriculum The explicit curriculum is that which is found in the university’s curriculum books.
It is publicly stated, is reviewed in curriculum planning meetings, and is
intentionally planned. It also refers to the courses, clinical education settings,
length of time to complete the course, and the degree awarded. When curricula
are evaluated, it is usually this component that is scrutinised.
However, some information is not taught but passed on indirectly. Attitudes and
behaviours in the clinical setting, for example, may not be taught, but ‘acquired’
from watching lecturers or clinicians role model them. This is the ‘implicit’
curriculum. It includes values and beliefs that are passed down from lecturers to
their students. The students, who then receive these messages, interpret them
as significant (Shepard and Jensen, 2002).
Students absorb various attitudes, behaviours and values from clinical and
academic teaching staff concerning lifelong learning, participation in professional
organizations, care of patients, and respect of other staff members. These
implicit messages may also concern the relative importance of certain types of
knowledge, the types of patients who are challenging, specific approaches to
treatment, and what personal and professional behaviours are acceptable. The
‘implicit’ aspect is often disregarded although it has just as much value as the
explicit curriculum.
Every aspect of the explicit curriculum contains an implicit message. For
example, learning OMT techniques in the laboratory may include an emphasis on
professional behaviours. The student should perform the technique the same
way they would on a patient, e.g. comfortably positioning the student who is
modeling as the patient, or asking for feedback about the comfort of their hand
position as they practice (Shepard and Jensen, 2002).
Intuitive skills e.g. clinical reasoning, communication skills, interpersonal skills
and having the right attitude (part of the implicit curriculum) are not
straightforward to teach. Students should be allowed to play out their future roles.
Opportunities that allow reflection and rehearsing of appropriate skills are needed
(Howe, 2002).
The null curriculum includes those elements that are missing from the curriculum
e.g. information on complementary and alternative therapies. Decisions on what
to exclude and include are difficult to make. Sometimes it is purely the extent of
available teaching time for the course that dictates this. Time is also needed for
students to consolidate concepts or reflect on ideas already taught. This also
relates to the concept of intention and reality discussed earlier where it may be
necessary to leave out certain subjects (Shepard and Jensen, 2002).
2.3 CURRICULUM PROCESS
2.3.1 Theory and Practice
In physiotherapy, one of the goals of clinical practice is to bridge the gap
between theory and practice. This can only take place once the student starts
practicing in the clinical placement. It involves a shift from the controlled
classroom environment to a de-controlled one. Practice also includes acting
without being always able to explain how treatment is working. In time, students
develop strategies and routines that may eventually lead to automatic behaviour
(Squires, 1987).
Reflection assists in this process. The students learn to refer back and forth
between the literature and their clinical experiences. Students have to develop
and refine skills like palpation, teaching core stabilization exercises and
facilitation of normal movement. Besides technical skills, they also have to learn
to motivate and teach patients (Shepard and Jensen, 2002).
Clinical environments in which students practice, however, are designed for
patient care and not teaching. Also students’ supervisors are in most cases
clinicians and not teachers i.e. they may not have formal teaching qualifications.
Despite this, clinical rotations provide a good learning experience for students.
Students are given the opportunity to apply and integrate knowledge. The
effectiveness of this exercise, however, depends on many factors such as
feedback to students, staff-student relationships, and organization of teaching.
Supervision of students involves constructive supportive feedback that redirects
their learning toward areas of deficiency. The process of curriculum evaluation
should aim to look at the various factors affecting clinical education e.g. if
adequate feedback is given by the supervisor to the student to assist their
learning, or if reflection by the students is being facilitated. These techniques can
be adopted or improved on if they have been found to be deficient or lacking in
the curriculum.
2.3.2 Organisation of the curriculum Following from this discussion, the next challenge would be to organize the
curriculum appropriately so that its objectives are achieved e.g. it should link
theory to practice. This is a challenge in physiotherapy. The graduates should be
sufficiently competent in applying and integrating their knowledge sufficiently in
clinical practice.
Organization involves continuity, sequence and integration. Continuity refers to
giving students the opportunity to practice and develop the cognitive, affective
and psychomotor skills they’ve learnt. For example, teaching of joint mobilization
techniques is followed by reinforcement of these skills in further laboratory
practical sessions. Sequence refers to the process of building one experience on
another, so that knowledge is broadened and deepened with each experience.
An example would be the task of assuming greater responsibility for patients
through each successive clinical placement. Finally integration refers to the
complementary relationship of courses e.g. two courses may be run concurrently
so that one complements the other reinforcing and clarifying knowledge in each
subject (Shepard and Jensen, 2002).
At Wits, the basic Maitland concept is taught first. The theory is then applied by
means of problem-solving exercises (in lecture and practical sessions), patient
assessments and treatments, and finally case discussions.
2.3.4 Clinical education a) Clinical reasoning and creativity Clinical competence is determined by three important skills. These are patient
consultation, knowledge, and problem solving ability. One needs to be proficient
in clinical reasoning to problem solve. Clinical reasoning is the cognitive process
by which the information contained in a clinical case is synthesized, integrated

with knowledge and experience, and used to diagnose the problem. It is the
thinking underlying clinical practice (Groves et al, 2002).
Creativity in clinical reasoning is also required. Instead of focusing on the
anatomy and pathomechanics alone, one needs to be sensitive to the individual
context of each patient’s presentation. The patient’s interpretation of their pain
goes beyond the anatomical structures to the impact of their problem on their
lives. It influences emotion, expectations and motivation of the patient. Attention
should be paid to psychosocial factors as well. As mentioned in the discussion of
the biopsychosocial model, when developing curricula, these aspects should be
considered (Jones, 1995).
Lippell (2002) suggests that a good student should be a creative, imaginative,
lateral thinker. Although creativity is being more and more valued in higher
education, medical curricula tend to discourage it (Lippell, 2002). The author
suggests that problem-based education may be helpful to change this. Problem
based learning stimulates creativity in the students’ approach to a patient.
Development of creativity can also be achieved by uncovering hidden talents and
by respecting the originality and individuality of students.
Although creativity should be encouraged, this should occur at the correct time.
The student should be exposed to specific learning problems that enable them to
learn routines and standards first. This will reinforce procedural reasoning and
technical skills. They may then be able to develop creative alternatives. The
student will not be able to cope with complex, ambiguous or challenging
situations initially. Once the pattern of learning is developed, the student can then
be challenged with more difficult clinical experiences e.g. encouraged to
problem–solve a diagnosis they have not encountered before (Shepard and
Jensen, 2002).

b) Techniques used for teaching students in clinical settings Physiotherapy students are faced with many challenges during their clinical
education. Clinical education for physiotherapy students is ‘hands-on’ as soon as
the student enters a placement. They need to know how to examine and treat
patients - skills that were learnt in the classroom and laboratory. The student
needs to adapt quickly to performing these skills in a very different setting from
the laboratory (that is controlled and predictable).
In the past, students were sent to hospital settings only. Now, students may be
sent to various other placements e.g. schools, outpatient health care facilities,
community-based centres, and health promotion centres. They will therefore
have access to patients in the ward, outpatient department, and in the
community. They are being exposed to different perspectives and need to look at
social and occupational factors (Shepard and Jensen, 2002). Certain techniques
discussed below may be adapted to facilitate learning.
The student
All of the above factors affect the student’s clinical experience. He/she needs to
be responsible to make sure that certain goals are achieved at the end of the
block. A way of doing this is for the student to be well aware of the objectives of
the clinical block. At the Wits physiotherapy department, students are each given
a clinical workbook in which the objectives for each block are listed clearly.
Besides setting objectives for the block, students can prepare their own personal
goals and objectives for that placement. This will help develop life-long learning
habits. As students progress through their clinical learning experiences, and
assume more responsibility for their learning, they should also be taught how to
self-assess their performance.
Keeping a journal or presenting a case report is a useful clinical requirement
since these activities encourage students to think about and question their
actions. However, this ends with the placement. Another tool that may be used to
keep this process ongoing is a portfolio. This gives students the opportunity to
reflect on their learning and professional development. They are then able to
assess their own development as a professional. The clinical teacher or the
physiotherapy department should help with structuring of the portfolio to guide
They should be asked to set their own goals as well as learn how to do self-
assessments. At present, students do portfolios for the public health clinical block
only.
The clinical teacher
Clinical teachers play an important role in clinical learning and should be given
information concerning the department’s mission, goals and objectives. These
help to define the context in which the curriculum is presented. Course
descriptions will show them the information the student has been exposed to so
that they can assess readiness of the group for that particular block. The clinical
teacher will also have the added advantage of assessing preparedness and
improvement for clinical practice (Shepard and Jensen, 2002). At the
physiotherapy department at Wits, the clinical supervisors of a particular block
have meetings each year with the lecturer who is the block coordinator. The
clinical supervisors are made aware of the curriculum content and the goals and
objectives of the block. They are also given a general talk regarding the mission,
and goals of the Wits physiotherapy department. They are given the opportunity
to contribute to making decisions regarding the organization of the blocks in
which they are involved.
c) Factors affecting clinical education Clinical hours An investigation was carried out by Dolmans et al (2001) to examine clinical
rotations of medical students. Results showed that some time in the blocks were
spent on non-instructive activities. Students perceived this as wasted time. (It
was difficult to define non-instructive activity since it varied from one block to the
other). They felt that time spent on reflection on experiences and supervision
improved effectiveness of the block. These findings support the earlier discussion
about the importance of supervision.
Although the study focused on medical students and the blocks they cover, it
clarified that a high number of hours in a clinical block does not mean that
students find the time effective. Lecturing staff should focus on kinds of activities
that facilitate learning. There is a need for careful structuring of clinical time.
The Wits students do eight weeks of clinical work in the OMT block in the third
and fourth years of study. A total of 224 hours are spent in this block.
2.3.5 Relevance of the OMT curriculum to the South African situation
It is important for our curriculum to address the needs of the South African
community. Community service requirements put further pressure on academic
institutions to deliver the kind of training that will adequately equip the new
graduate to handle patients and situations in the community. This is because
there is sometimes inadequate supervision and mentoring available for the new
graduate.
Following the elections in 1994, a decision was made to develop a
comprehensive health care system to address the needs of the entire population
(Van Rooijen and Van der Spuy, 2000). Government adopted primary health care
(which involves health promotion, prevention of disease, and supply of care and
effective rehabilitation programmes) as a health care policy. This change
obviously impacts on the training of physiotherapy students. They need more
training at a primary healthcare level, in communication and interpersonal skills,
community based training and professional and management skills. They should

be exposed to the biopsychosocial model with interactive teaching methods (Van
Rooijen and Van der Spuy, 2000).
Bradshaw et al (2003) showed that premature mortality in South Africa
(especially among males) is largely due to violence and road traffic accidents.
HIV/AIDS also accounts for early loss of life in males and females in South
Africa. Physiotherapists treating neuromusculoskeletal problems resulting from
HIV/AIDS or trauma must have the necessary skills required for the treatment of
these patients. The OMT curriculum should equip students with this knowledge.
Clinical placements should also be relevant to the situation in which we find
ourselves as health care providers. A great deal of healthcare is now provided in
the community. In-patient stays are becoming less common and much shorter
than before and therefore hospitals may not be able to provide the experiences
undergraduates need. Therefore, community placements may be more relevant
and give students more opportunity for clinical training (Van Rooijen and Van der
Spuy, 2000). At Wits, the students do a block in the community in third and fourth
year. They are therefore given the opportunity to apply their OMT knowledge
when involved in public health programmes on health promotion, prevention of
disease, and rehabilitation in the community.
A functional approach to treatment has been shown to be of great value (Concha
et al, 1995). Physiotherapy students need to be trained to address function when
assessing and treating since this is more meaningful to patients especially in the
community. The OMT curriculum should therefore place adequate emphasis on
the reeducation of functional activities.
Curriculum process and the application of theory to practice are challenging.
They may be influenced by the clinical environment and organization of the
curriculum. However, the techniques and teaching methods discussed above
may be of great value in achieving these goals. Finally, it is important that all of

these teaching techniques are applied within the context of our society. This will
enable our students to make a meaningful contribution in their clinical
placements.
2.4 CONCLUSION
The concept of curriculum is very broad and encompasses the implicit and
explicit curriculum, content and process, all of which contribute greatly to
students’ growth. Due to the impact of the curriculum on the competency of the
student, there needs to be regular evaluation. The evaluation process consists of
various classes of information. Supplemental information may give clues
regarding the relevance of the curriculum to society, and whether the perceived
intentions of the curriculum are actually being achieved.
With regards to OMT, the curriculum should achieve acquiring of basic
theoretical knowledge of the assessment and treatment of joint and soft tissue
structures, the necessary practical skills and the ability to apply these effectively
in the clinical setting. Clinical education (actual practical work in the clinical
blocks) appears to have a significant influence on the students produced from a
department. Therefore clinical reasoning and application of theory to practice is
important. Active teaching methods seem effective in developing critical thinking.
Relevance of the curriculum to the South African situation is important and
should be considered.
Curriculum evaluation is an extensive process and involves obtaining a great
deal of information. This report focused mainly on gathering and analyzing
supplemental information. This information was obtained from questionnaires
and interviews that are shown to be the most appropriate research tools for this
type of study.
CHAPTER 3 METHOD
3.1 INTRODUCTION This chapter describes the manner in which this study was carried out. Ethical
clearance, the research participants and the research tool are discussed. This is
followed by a description of how data were collected and interpreted.
3.2 ETHICAL CLEARANCE Ethical clearance was obtained from the Committee for Research on Human
Subjects (medical) at the University of the Witwatersrand.
Ethical clearance number: M01-05-38 (See appendix 6)
3.3. STUDY DESIGN This is a descriptive retrospective study. Both questionnaires and interviews were
used. Interviews were carried out to clarify certain information obtained from the
questionnaires.
Use of questionnaires and interviews
Surveys are commonly used in the evaluation process. This research technique
uses questionnaires or interviews as its research tools to collect data from a
large group of people to get an overview of their perceptions. Surveys may be
prospective or retrospective. Prospective studies involve identifying the group of
people you want to study and then accessing them as they use a particular
service. Retrospective studies like this one look at past events. One may look at
the medical records of a clinic and then contact the relevant patients. This is an
easier way to access participants but the disadvantage is that they may have
forgotten some of the information you require (Hicks, 1999).
Questionnaire design
This involves several important steps. The objectives of the researcher need to
be reflected. The validity and reliability should be established. The questionnaire
should be piloted so that any ambiguities/ unclear questions etc can be modified.
Questions may be open or closed ended. The former allows the respondent more
flexibility and therefore more information can be obtained. However analysis is
less objective and therefore not as sophisticated as closed-ended questions. The
latter have a structured response format and therefore can be objectively
analysed. However, the format may not meet the needs of the respondents
(Hicks, 1999). Questions should be put in a logical sequence. The layout of the
questions should not influence the responses (Cormack, 1991).
Mail questions should have a shorter format since this produces a better
response rate. The advantages of a questionnaire study are that a large number
of people can be accessed since the researcher can simply post the questions to
them. He/she does not have to administer them in person and this therefore
saves time and money on travel. The researcher does not also have the
opportunity to influence the sample (Hicks, 1999).
Interviews
The research interview may be used to supplement other methods of inquiry e.g.
a questionnaire. Additional information may be collected, responses validated
and probed into more deeply, through the interview. The interviewer should set
an agenda for the interview. The aims, objectives, and procedure should be
stated first. The interviewee should be assured of anonymity. One may also ask if
he/she had any questions about the interview before continuing. The interview

schedule standardizes the interview since the same questions are asked in the
same sequence and manner. The interviewer inviting the respondent to add
further information or clarify his original response may amplify the response
(Cormack, 1991).
3.4 RESEARCH TOOLS 3.4.1 Questionnaire and Interviews (See Appendix 3)
Formulation of Questionnaire Thirty-five questions were formulated. These were based on the researcher’s
background knowledge and on discussions with physiotherapy lecturers
(including some who have specialized in OMT) and lecturers from a variety of
other medical departments. The lecturers were from this university and other
universities viz. University of Kwa-Zulu, and Pretoria. Discussions were also held
with past graduates. The following procedures were undertaken to establish the
validity of the questionnaire.
Possible questions were written down and distributed to some of the above-
mentioned people, to gain their views and suggestions. Focus groups with the
fourth years were held in 2001(See appendix 1 for focus group questionnaire).
This was to determine whether the draft questionnaire addressed issues about
the curriculum that were relevant to them. They had completed most of the OMT
curriculum and had some clinical experience and were therefore in a position to
make appropriate and relevant comments.
Finally, a formal discussion was held with a statistician, two experienced OMT
lecturers, a lecturer from this physiotherapy department, and a faculty member
from the University of the Witwatersrand who had done previous questionnaire
studies on medical curricula. Each question was evaluated individually to see if it
was relevant to the specific objectives, worded correctly, laid out appropriately,
and statistically relevant. All the above processes were carried out to check
wording, accuracy, readability, analysis, and whether each section was
comprehensive and exclusive. This was also done to reduce option bias i.e. to
ensure that the order and position of questions in the layout didn’t affect how
people would respond.
A pilot study was carried out. Physiotherapists from the Johannesburg General
Hospital and lecturers from the University of the Witwatersrand Physiotherapy
Department participated. Ten questionnaires were returned. Not many changes
needed to be made to the draft copy except for several corrections of the wording
of some questions. The questionnaire therefore appeared to be well understood.
This final draft was used in the study. The focus groups and pilot study
contributed to the validity of the questionnaire.
Information sheet (See Appendix 2)
This was used to introduce the researcher and give some background
information about the study to the participant. It also stated that anonymity would
be maintained.
Questions These included a mixture of closed and open-ended questions. There were
various types of closed-ended questions viz. dichotomous, scaled and grid type
questions.
The first section included questions that covered demographic aspects of the
participants i.e. age, area of work, year of qualification, nature of practice and
number of years of OMT practice.
The next section covered aspects of undergraduate study. These covered
technical and reflective content in the second, third and fourth years, relevance of
the Maitland concept, deficient areas in the curriculum, teaching methods, and
the inclusion of an optional course.
The next section covered postgraduate study. This included questions regarding
which postgraduate courses participants may have done to supplement
undergraduate knowledge, and why these courses were useful.
3.5 RESEARCH PARTICIPANTS Physiotherapy graduates who completed their degree in 1997, 1998, and 1999
were selected to be participants in the study.
The names of graduates were acquired from the Physiotherapy Department of
the University of the Witwatersrand records. The Health Professions Council of
South Africa (HPCSA) was contacted and an official letter as required, was sent
requesting contact details i.e. addresses of the relevant registered
physiotherapists. In addition, the South African Society of Physiotherapy (SASP)
was contacted since their records were more recently updated and also included
telephone numbers of graduates who were members.
3.6 INCLUSION CRITERIA The sample included physiotherapists in part-time and full-time employment, in
hospital and outpatient practice, and in government and private institutions. The
sample group consisted of all past graduates from 1997 to 1999.
EXCLUSION CRITERIA None
SAMPLE SIZE The entire population (a total of 121 graduates) was sampled.
3.7 DATA COLLECTION A code was allocated to each questionnaire. An outsider, to maintain anonymity,
did this. They were then posted together with a self-addressed envelope to the
sample group. The researcher then obtained as many telephone numbers as
possible from the SASP records and the telephone directory. The participants
were called three weeks to a month later to establish whether they had received
the questionnaire. Another copy was sent if they had not received the first one.
Data analysis The quantitative data were captured on Microsoft Excel spreadsheets that were
then analysed with the help of a statistician. (See appendix 5 for results of
quantitative data). Responses to open-ended questions were extracted and
summarized. (See appendix 5 for responses). On examination of this data, it was
apparent that some information needed clarification or clearer explanation.
Interviews were subsequently carried out to achieve this.
3.8 INTERVIEWS Interview questionnaire (see appendix 4)
Attempts were made to contact thirty participants in order to obtain a minimum of
six who were willing to be interviewed. Nine participants agreed to being
interviewed. The author then conducted nine telephonic interviews. Anonymity
was assured before each interview commenced. The aim and procedure was
then stated. Six open-ended questions were asked (in the same sequence),
based on information received from the questionnaire. This related to curriculum
content and teaching methods. Respondents were free to add more information
or explain their response in addition to answering the question. The interviewer
asked for clarification if there was any confusion regarding responses to the
questions. The responses were then summarized (see appendix 5 for
responses).
3.9 STATISTICAL ANALYSIS The results in this report are presented both graphically and in table form in
terms of the percentages of the responses to the indicated questions. The overall
results are presented in chapter four. The full results are presented in appendix
five in the same format as in the questionnaire. The data were analysed using
descriptive statistics and are presented in percentages.
CHAPTER 4 RESULTS One hundred and twenty one questionnaires were sent out. Thirty-two
questionnaires were received and nine interviews were conducted.
Results of this study are discussed under demographics, curriculum content, the
clinical curriculum and general teaching methods.
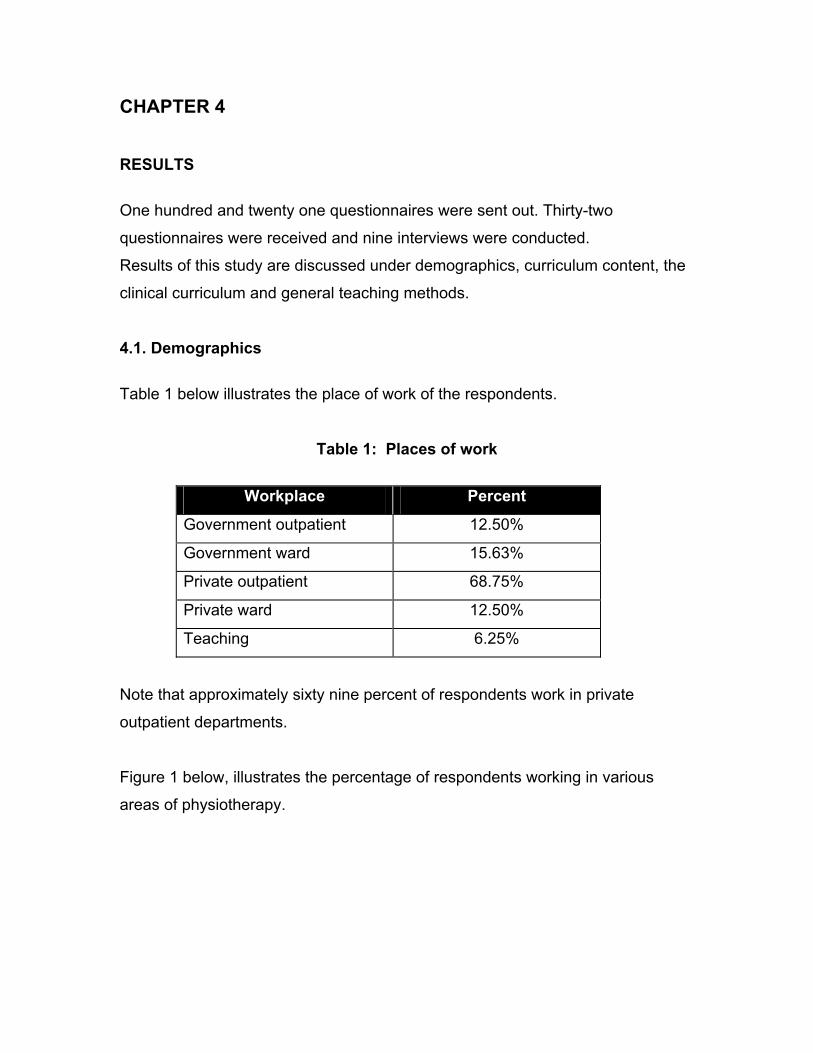
4.1. Demographics Table 1 below illustrates the place of work of the respondents.
Table 1: Places of work
Workplace Percent
Government outpatient 12.50%
Government ward 15.63%
Private outpatient 68.75%
Private ward 12.50%
Teaching 6.25%
Note that approximately sixty nine percent of respondents work in private
outpatient departments.
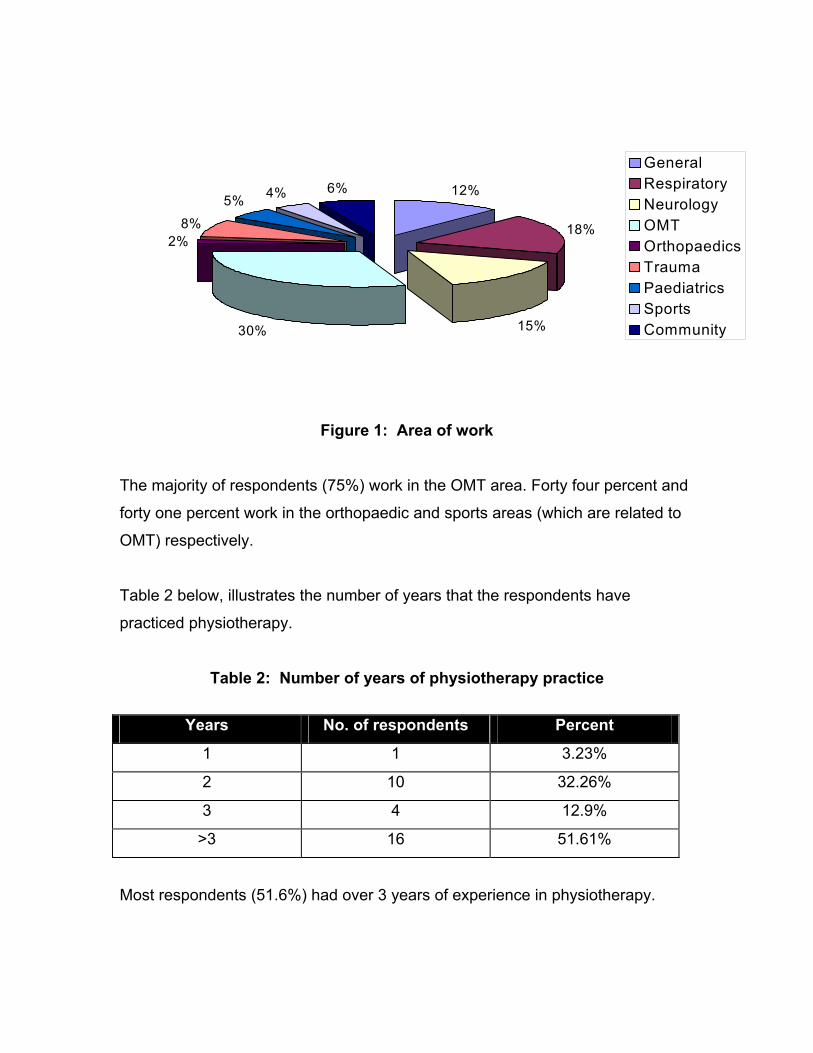
Figure 1 below, illustrates the percentage of respondents working in various
areas of physiotherapy.
12%
18%
15%30%
2%8%
5% 4% 6%
GeneralRespiratoryNeurologyOMTOrthopaedicsTraumaPaediatricsSportsCommunity
Figure 1: Area of work
The majority of respondents (75%) work in the OMT area. Forty four percent and
forty one percent work in the orthopaedic and sports areas (which are related to
OMT) respectively.
Table 2 below, illustrates the number of years that the respondents have
practiced physiotherapy.
Table 2: Number of years of physiotherapy practice
Years No. of respondents Percent
1 1 3.23%
2 10 32.26%
3 4 12.9%
>3 16 51.61%
Most respondents (51.6%) had over 3 years of experience in physiotherapy.
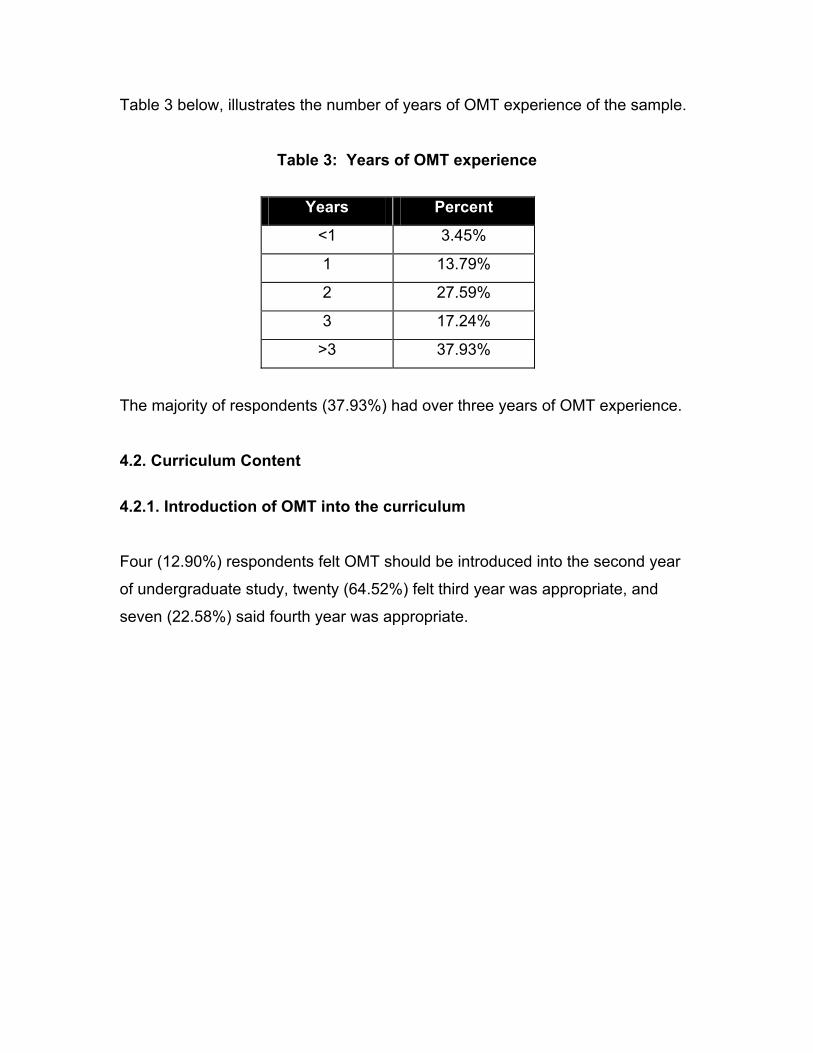
Table 3 below, illustrates the number of years of OMT experience of the sample.
Table 3: Years of OMT experience
Years Percent
<1 3.45%
1 13.79%
2 27.59%
3 17.24%
>3 37.93%
The majority of respondents (37.93%) had over three years of OMT experience.
4.2. Curriculum Content 4.2.1. Introduction of OMT into the curriculum
Four (12.90%) respondents felt OMT should be introduced into the second year
of undergraduate study, twenty (64.52%) felt third year was appropriate, and
seven (22.58%) said fourth year was appropriate.
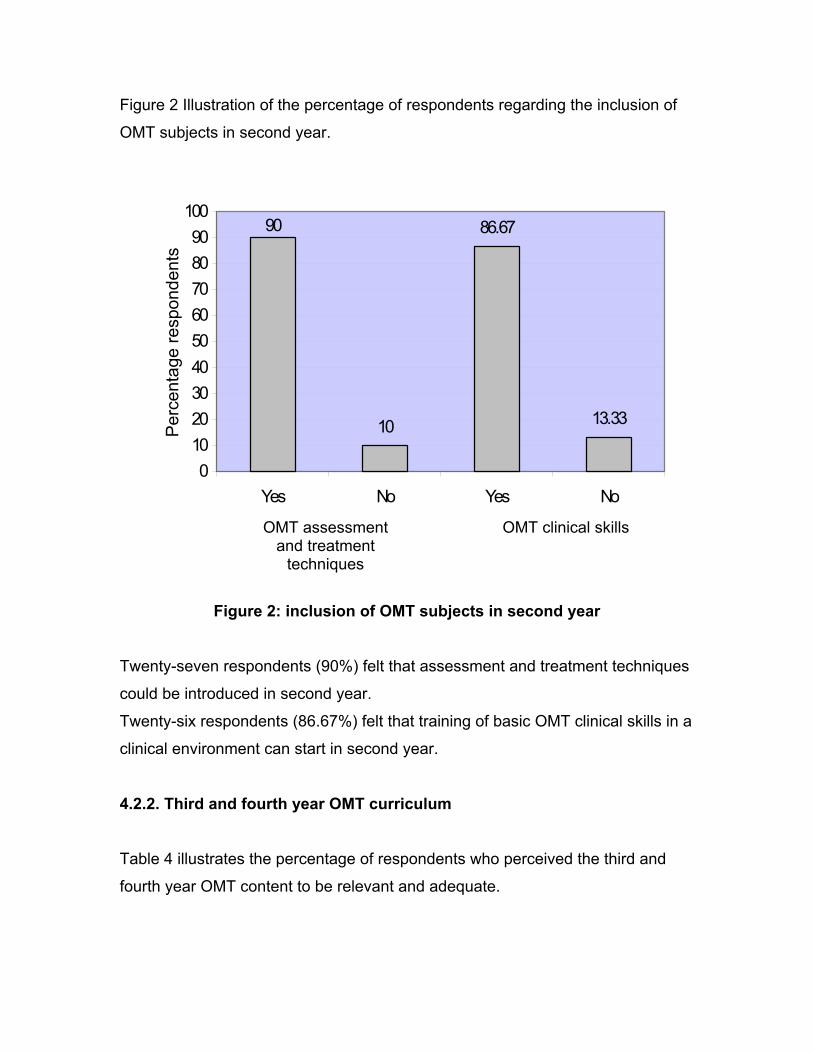
Figure 2 Illustration of the percentage of respondents regarding the inclusion of
OMT subjects in second year.
10
86.67
13.33
90
0102030405060708090
100
Yes No Yes No
Per
cent
age
resp
onde
nts
OMT clinical skills OMT assessment and treatment
techniques
Figure 2: inclusion of OMT subjects in second year
Twenty-seven respondents (90%) felt that assessment and treatment techniques
could be introduced in second year.
Twenty-six respondents (86.67%) felt that training of basic OMT clinical skills in a
clinical environment can start in second year.
4.2.2. Third and fourth year OMT curriculum
Table 4 illustrates the percentage of respondents who perceived the third and
fourth year OMT content to be relevant and adequate.
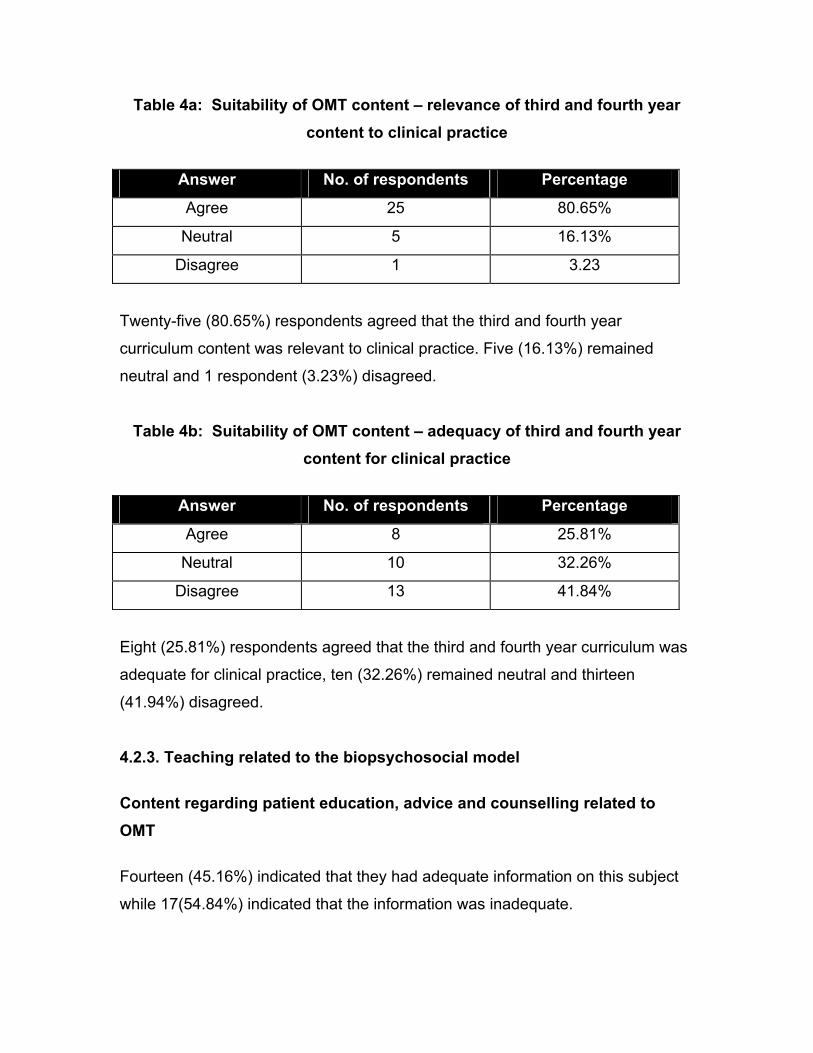
Table 4a: Suitability of OMT content – relevance of third and fourth year content to clinical practice
Answer No. of respondents Percentage
Agree 25 80.65%
Neutral 5 16.13%
Disagree 1 3.23
Twenty-five (80.65%) respondents agreed that the third and fourth year
curriculum content was relevant to clinical practice. Five (16.13%) remained
neutral and 1 respondent (3.23%) disagreed.
Table 4b: Suitability of OMT content – adequacy of third and fourth year content for clinical practice
Answer No. of respondents Percentage
Agree 8 25.81%
Neutral 10 32.26%
Disagree 13 41.84%
Eight (25.81%) respondents agreed that the third and fourth year curriculum was
adequate for clinical practice, ten (32.26%) remained neutral and thirteen
(41.94%) disagreed.
4.2.3. Teaching related to the biopsychosocial model Content regarding patient education, advice and counselling related to OMT Fourteen (45.16%) indicated that they had adequate information on this subject
while 17(54.84%) indicated that the information was inadequate.
Content regarding psychosocial aspects, interpersonal skills and community skills Eleven (35.48%) indicated that the above information was adequate while twenty
(60.45%) indicated that it was inadequate.
Twelve (38.71%) said they had adequate instruction in applying these skills while
nineteen (61.29%) said they did not.
4.2.4. Deficiencies in the OMT curriculum Figure 3 illustrates the percentage of respondents who perceived important
aspects to be lacking in the OMT curriculum.
8 0 %
2 0 %
Y e sN o
Figure 3: Deficiency of content
According to 24 (80%) respondents, there were important aspects lacking in the
curriculum. Six (20%) did not think so.
Areas of deficiency as stated by respondents in the follow-up question: These were:
• Application of the OMT concept and actual OMT techniques in the clinical
setting. Explanation of how the techniques work.
• Biomechanics and functional anatomy.
• Information on the sacroiliac joint and temperomandibular joint.
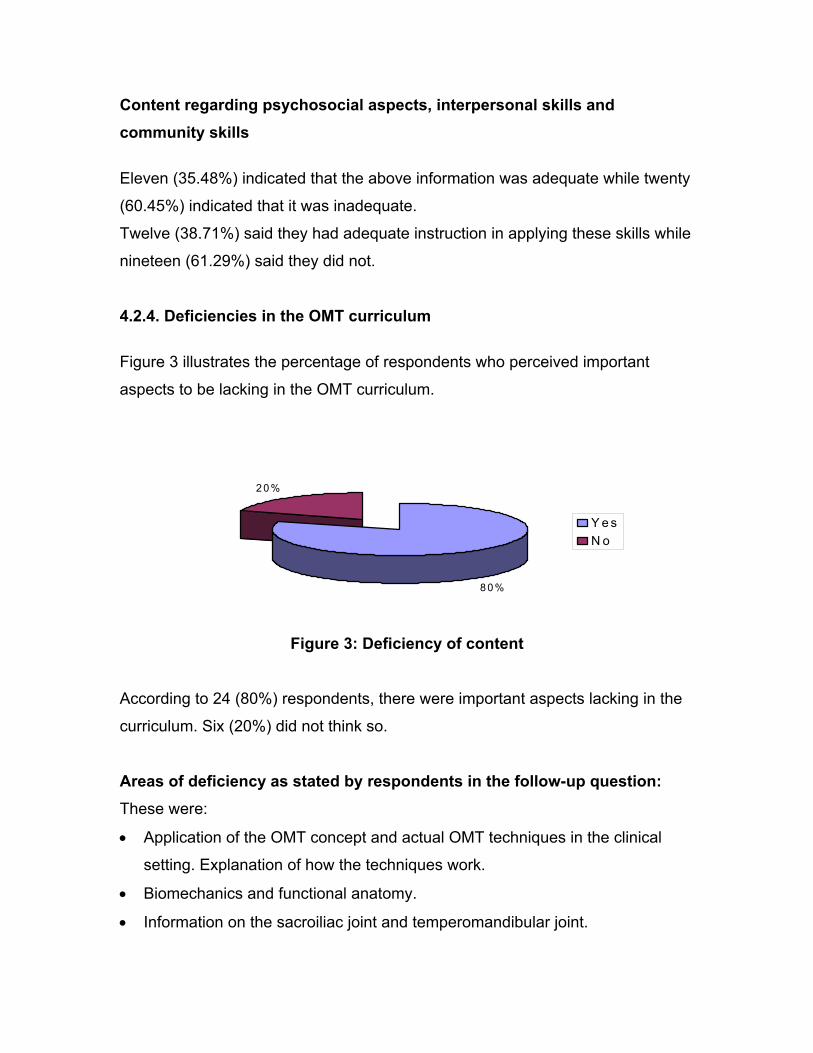
4.2.5. Additions to the OMT curriculum Figure 4 illustrates the percentage of respondents who felt that some important
additional aspects should be included in the OMT curriculum.
6%
94%
Yes No
Figure 4: Inclusion of additional content
Twenty-nine respondents (93.55%) said that more information should be
included into the OMT curriculum while two (6.45%) did not feel this way.
The respondents stated that more information should be included on the
following topics:
• Posture and ergonomics
• Information on psychosocial aspects and counselling.
• Other OMT concepts and alternative therapies.
• More clinical teaching and application of OMT techniques
4.2.6. Alternative and complementary therapies All respondents would have liked more information about OMT related alternative
and complementary therapies.
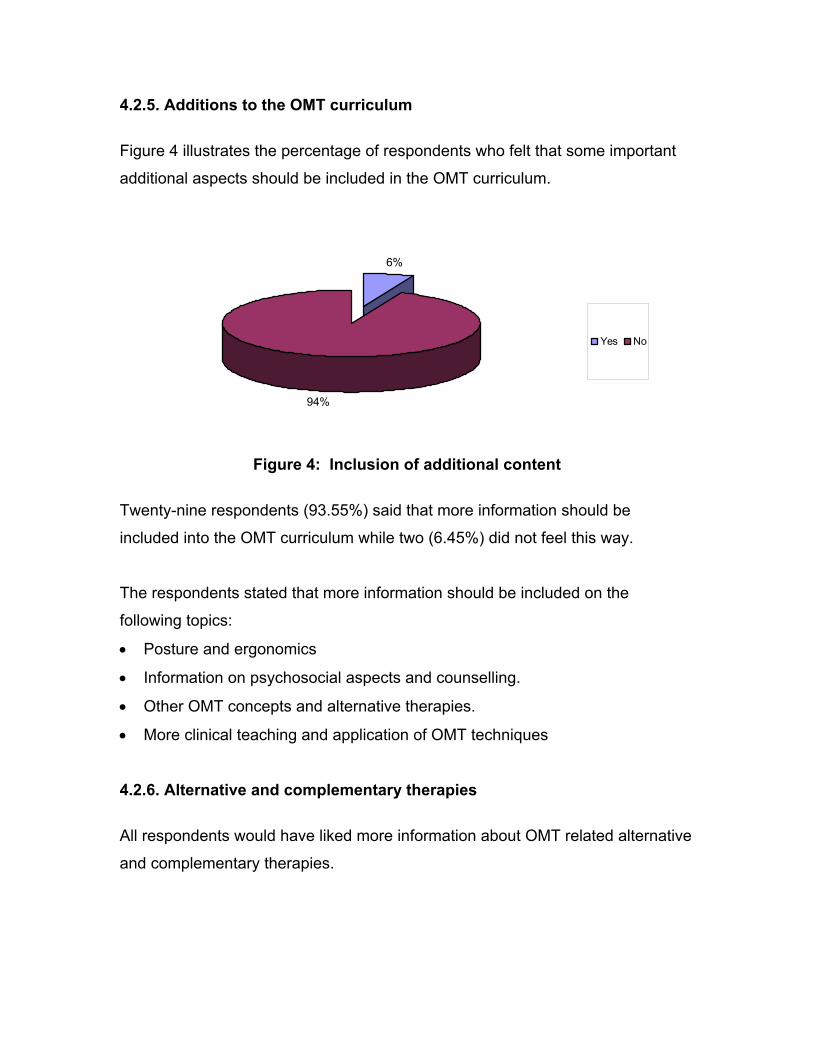
4.2.7. Maitland techniques Figure 5a, b and c illustrate the respondents’ perceptions concerning Maitland
techniques.
47%
53%
Relevant
Sometimesrelevant
Fig 5a Perceptions regarding relevance of the Maitland concept in clinical practice
21%
69%
10%
Adequate
SometimesadequateInadeqate
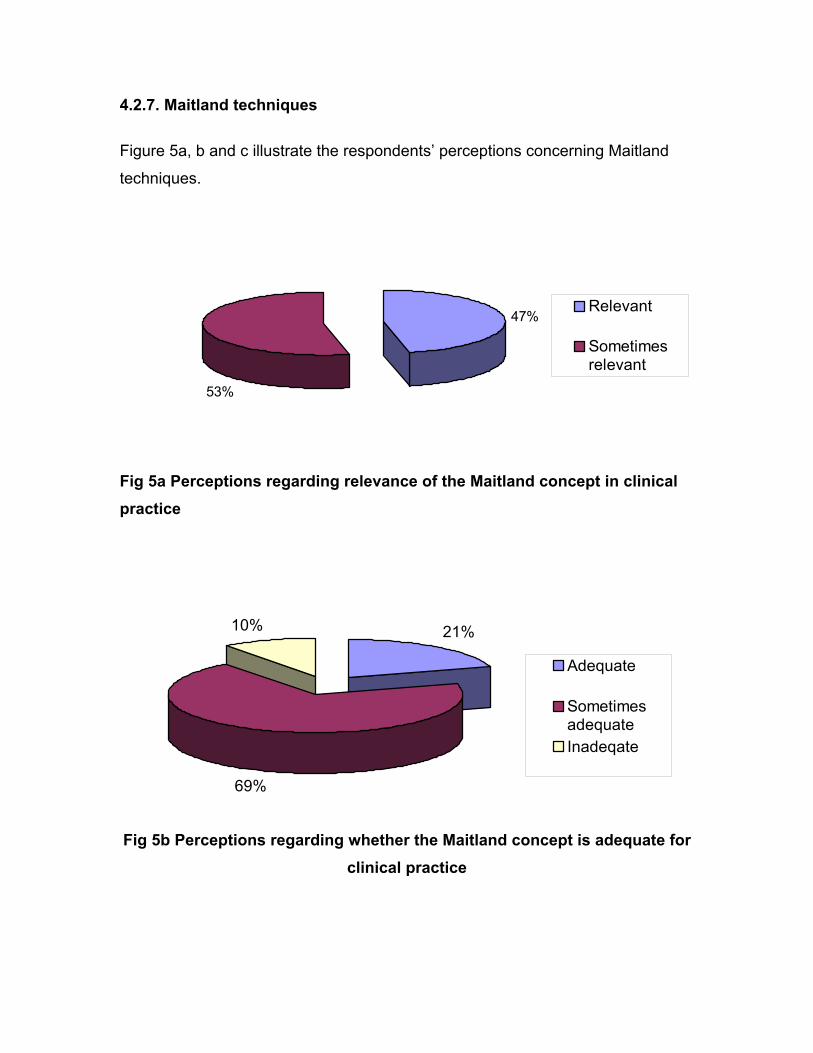
Fig 5b Perceptions regarding whether the Maitland concept is adequate for clinical practice
6%
94%
Always effectiveSometimes effective
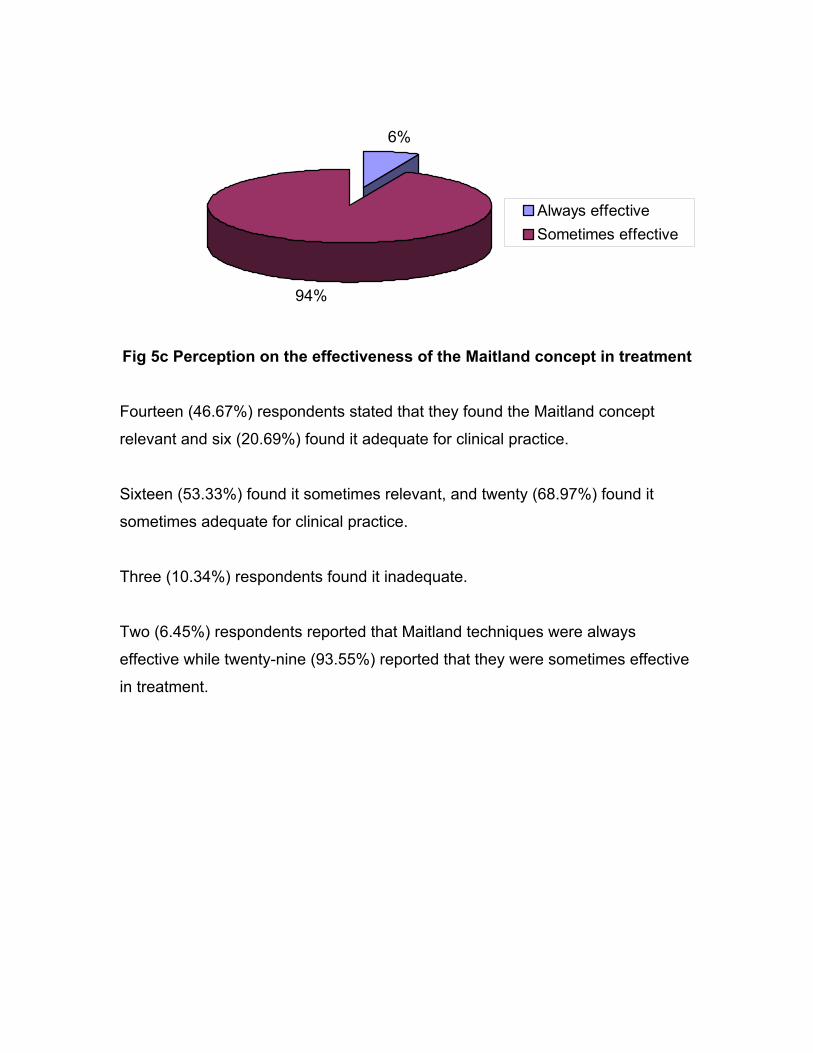
Fig 5c Perception on the effectiveness of the Maitland concept in treatment
Fourteen (46.67%) respondents stated that they found the Maitland concept
relevant and six (20.69%) found it adequate for clinical practice.
Sixteen (53.33%) found it sometimes relevant, and twenty (68.97%) found it
sometimes adequate for clinical practice.
Three (10.34%) respondents found it inadequate.
Two (6.45%) respondents reported that Maitland techniques were always
effective while twenty-nine (93.55%) reported that they were sometimes effective
in treatment.
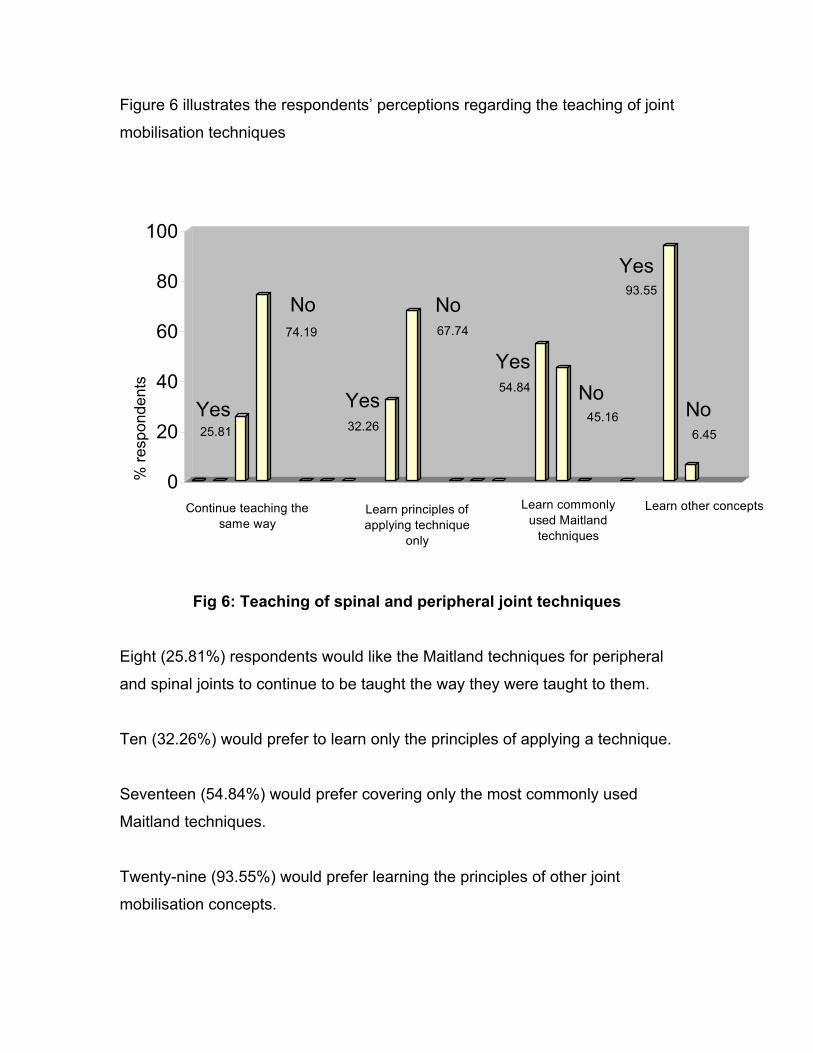
Figure 6 illustrates the respondents’ perceptions regarding the teaching of joint
mobilisation techniques
25.81
74.19
32.26
67.74
54.84
45.16
93.55
6.45
0
20
40
60
80
100
Yes
No
YesNoYes
No
Yes
No
Continue teaching the same way
Learn principles of applying technique
only
Learn commonly used Maitland
techniques
Learn other concepts
% re
spon
dent
s
Fig 6: Teaching of spinal and peripheral joint techniques
Eight (25.81%) respondents would like the Maitland techniques for peripheral
and spinal joints to continue to be taught the way they were taught to them.
Ten (32.26%) would prefer to learn only the principles of applying a technique.
Seventeen (54.84%) would prefer covering only the most commonly used
Maitland techniques.
Twenty-nine (93.55%) would prefer learning the principles of other joint
mobilisation concepts.
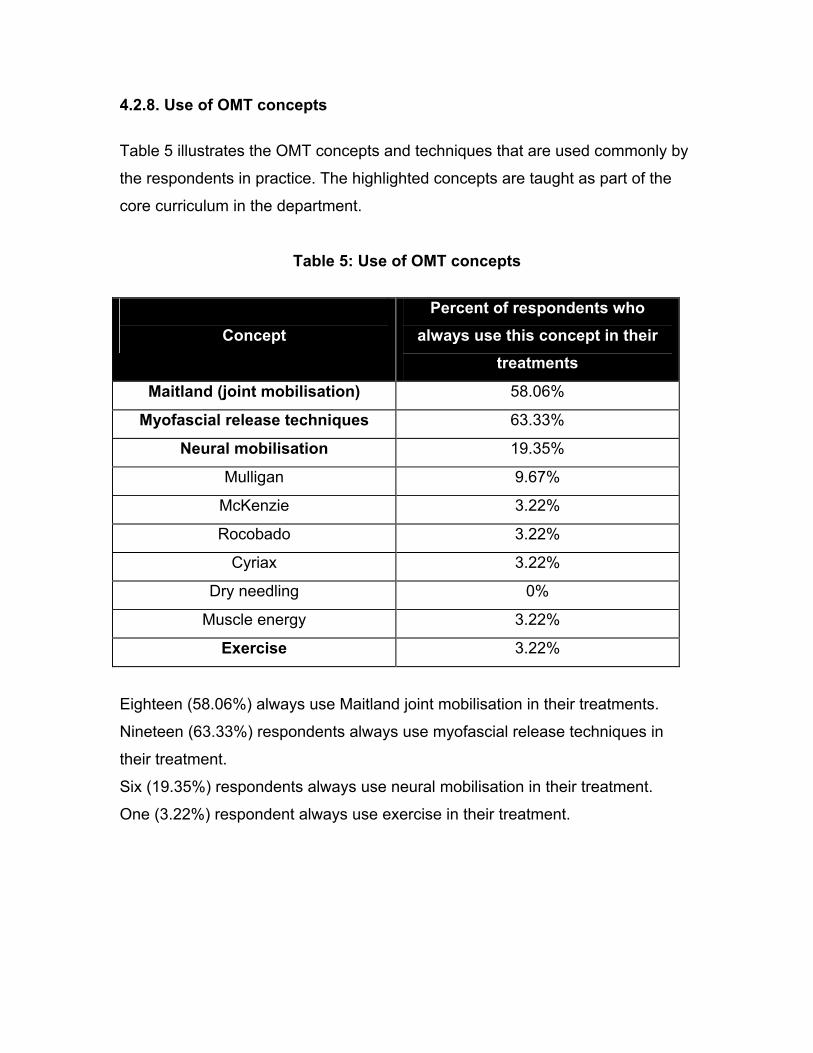
4.2.8. Use of OMT concepts Table 5 illustrates the OMT concepts and techniques that are used commonly by
the respondents in practice. The highlighted concepts are taught as part of the
core curriculum in the department.
Table 5: Use of OMT concepts
Concept
Percent of respondents who always use this concept in their
treatments
Maitland (joint mobilisation) 58.06%
Myofascial release techniques 63.33%
Neural mobilisation 19.35%
Mulligan 9.67%
McKenzie 3.22%
Rocobado 3.22%
Cyriax 3.22%
Dry needling 0%
Muscle energy 3.22%
Exercise 3.22%
Eighteen (58.06%) always use Maitland joint mobilisation in their treatments.
Nineteen (63.33%) respondents always use myofascial release techniques in
their treatment.
Six (19.35%) respondents always use neural mobilisation in their treatment.
One (3.22%) respondent always use exercise in their treatment.
4.2.9. Creativity Ten (32.26%) found that the prescribed curriculum allowed for innovation and
their own creative ideas. Thirteen (41.94%) seldom found this and eight (25.81%)
never found this.
Summary of responses regarding reasons for lack of creativity:
• There was a regimental approach to teaching especially regarding the use
of techniques (techniques had to be performed and used in specific ways).
• The curriculum was too ‘textbook orientated’ and did not allow flexibility.
4.2.10. Perceptions regarding exposure to current research in OMT Twelve respondents (38.71%) felt they were often exposed to current research in
OMT through actual teaching/research articles in reading packs. Seventeen
(54.84%) felt they were seldom exposed to this while two (6.45%) felt that they
were never exposed to this.
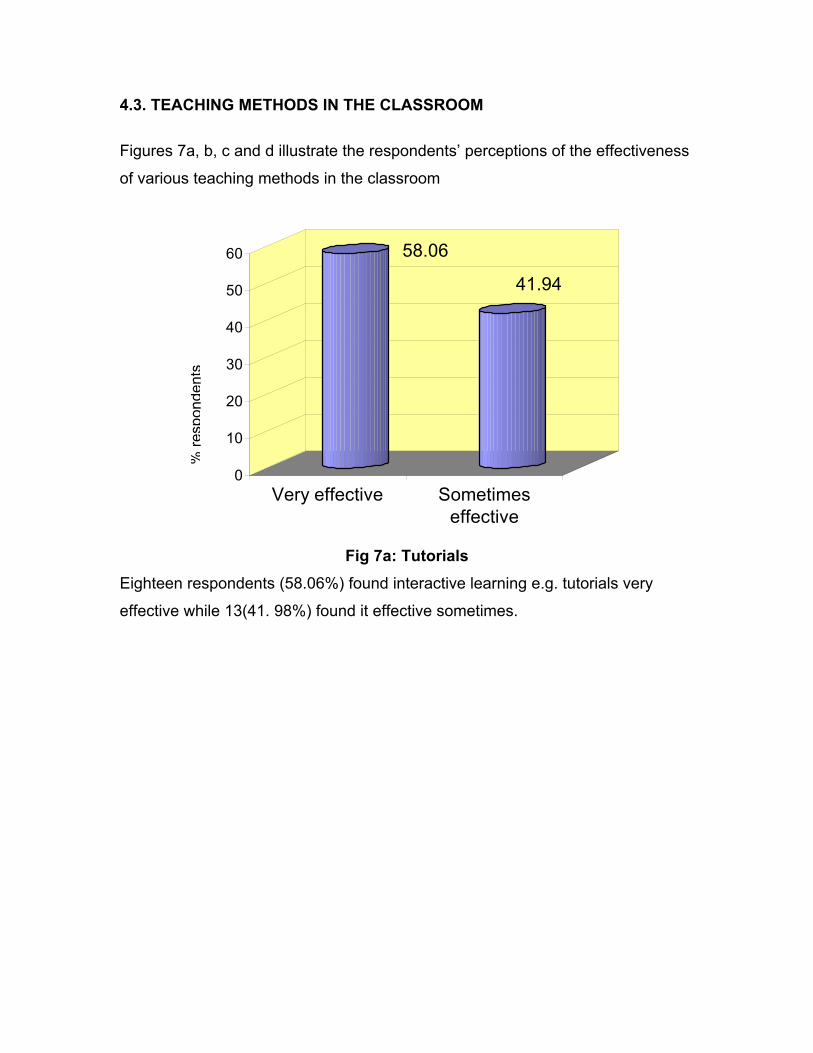
4.3. TEACHING METHODS IN THE CLASSROOM Figures 7a, b, c and d illustrate the respondents’ perceptions of the effectiveness
of various teaching methods in the classroom
58.06
41.94
0
10
20
30
40
50
60
Very effective Sometimeseffective
% re
spon
dent
s
Fig 7a: Tutorials
Eighteen respondents (58.06%) found interactive learning e.g. tutorials very
effective while 13(41. 98%) found it effective sometimes.

12.9
77.42
9.68
0
10
20
30
40
50
60
70
80
Very effective Sometimeseffective
Ineffective
% re
spon
dent
s
Fig 7b: Practical sessions Twenty-one respondents (67.74%) found practical sessions very effective,
7(22.58%) sometimes found them effective, and 3(9.68%) found them ineffective.
58.06
41.94
0
10
20
30
40
50
60
Very effective Sometimes effective
% re
spon
dent
s
Fig 7c: Workshops
Eighteen respondents (58.06%) found workshops very effective while
13(41.94%) found them effective sometimes.
12.9
77.42
9.68
0
10
20
30
40
50
60
70
80
Very effective Sometimeseffective
Ineffective
% re
spon
dent
s
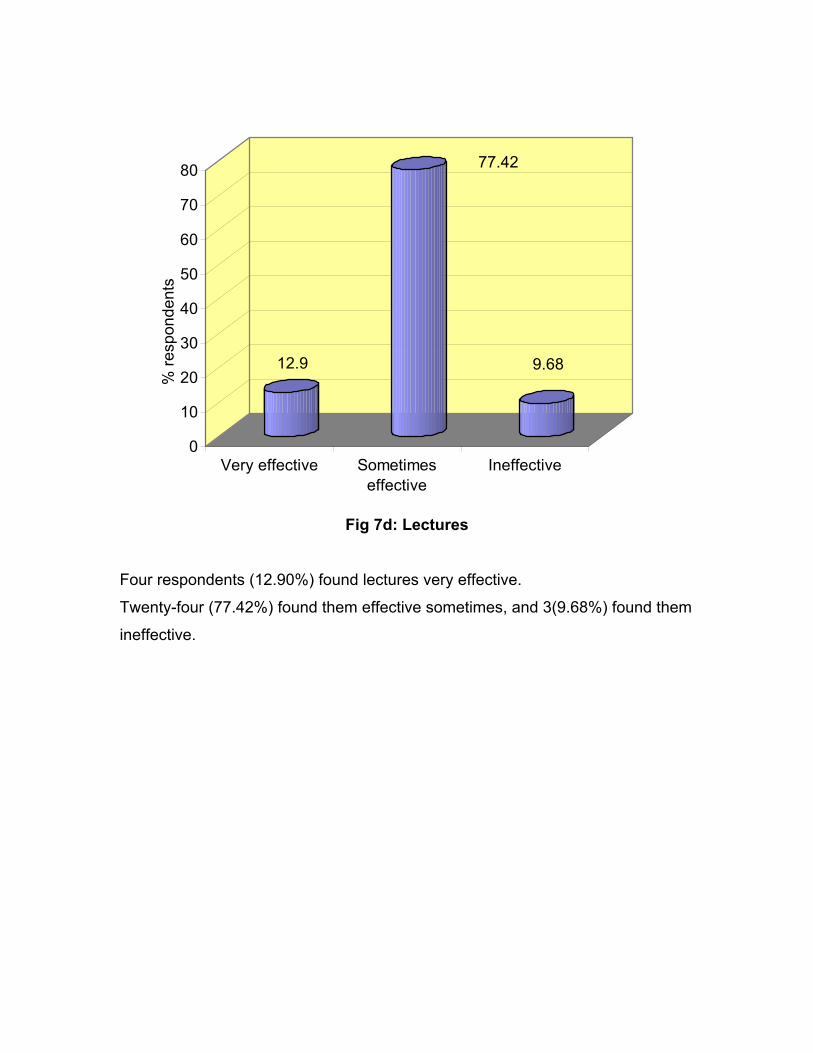
Fig 7d: Lectures
Four respondents (12.90%) found lectures very effective.
Twenty-four (77.42%) found them effective sometimes, and 3(9.68%) found them
ineffective.
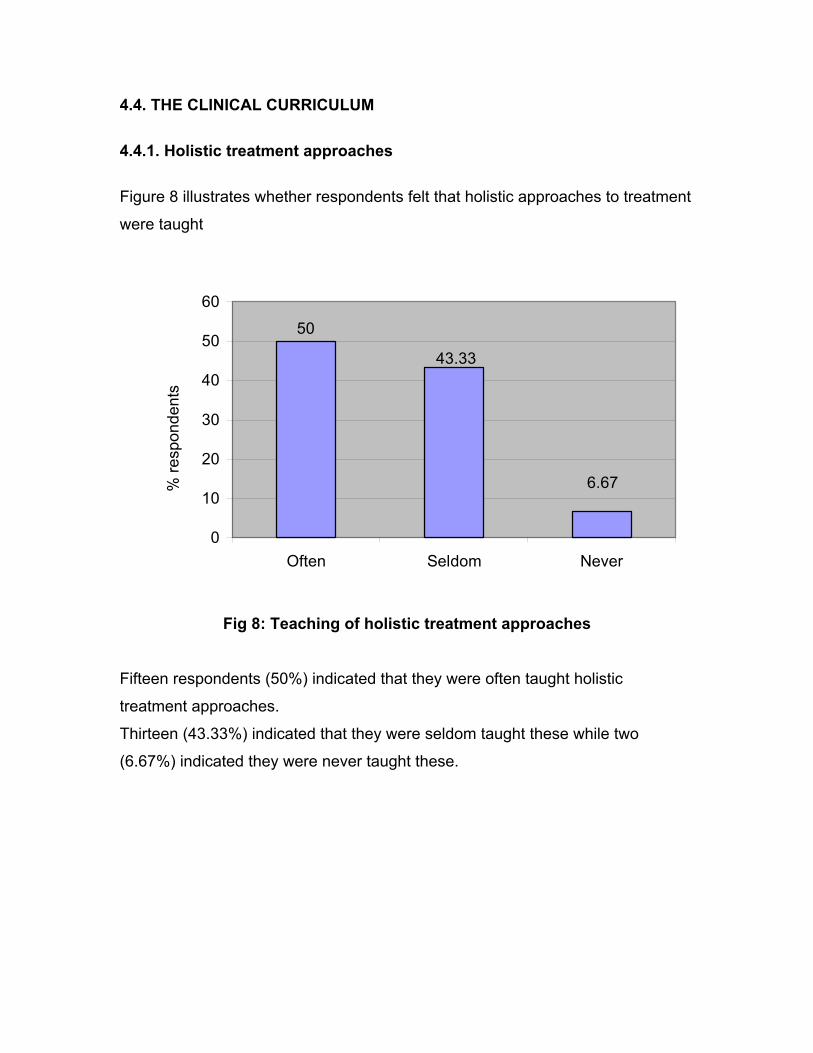
4.4. THE CLINICAL CURRICULUM 4.4.1. Holistic treatment approaches Figure 8 illustrates whether respondents felt that holistic approaches to treatment
were taught
50
43.33
6.67
0
10
20
30
40
50
60
Often Seldom Never
% re
spon
dent
s
Fig 8: Teaching of holistic treatment approaches
Fifteen respondents (50%) indicated that they were often taught holistic
treatment approaches.
Thirteen (43.33%) indicated that they were seldom taught these while two
(6.67%) indicated they were never taught these.
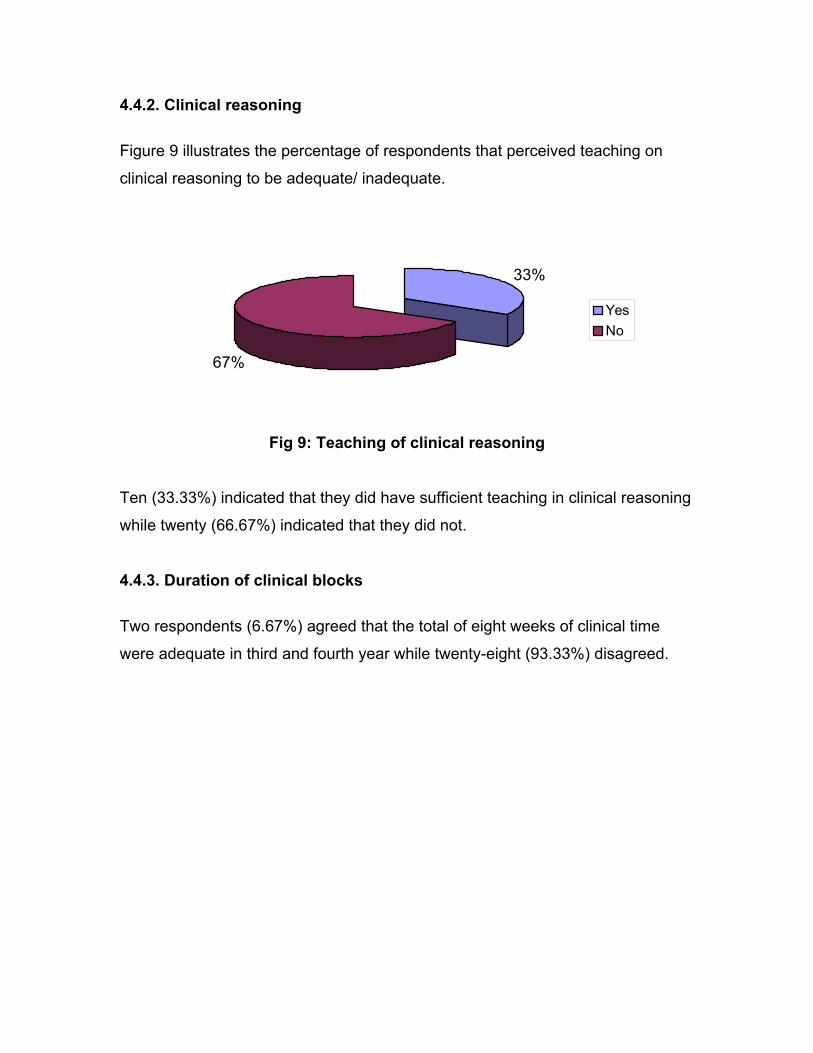
4.4.2. Clinical reasoning Figure 9 illustrates the percentage of respondents that perceived teaching on
clinical reasoning to be adequate/ inadequate.
67%
33%
YesNo
Fig 9: Teaching of clinical reasoning
Ten (33.33%) indicated that they did have sufficient teaching in clinical reasoning
while twenty (66.67%) indicated that they did not.
4.4.3. Duration of clinical blocks Two respondents (6.67%) agreed that the total of eight weeks of clinical time
were adequate in third and fourth year while twenty-eight (93.33%) disagreed.
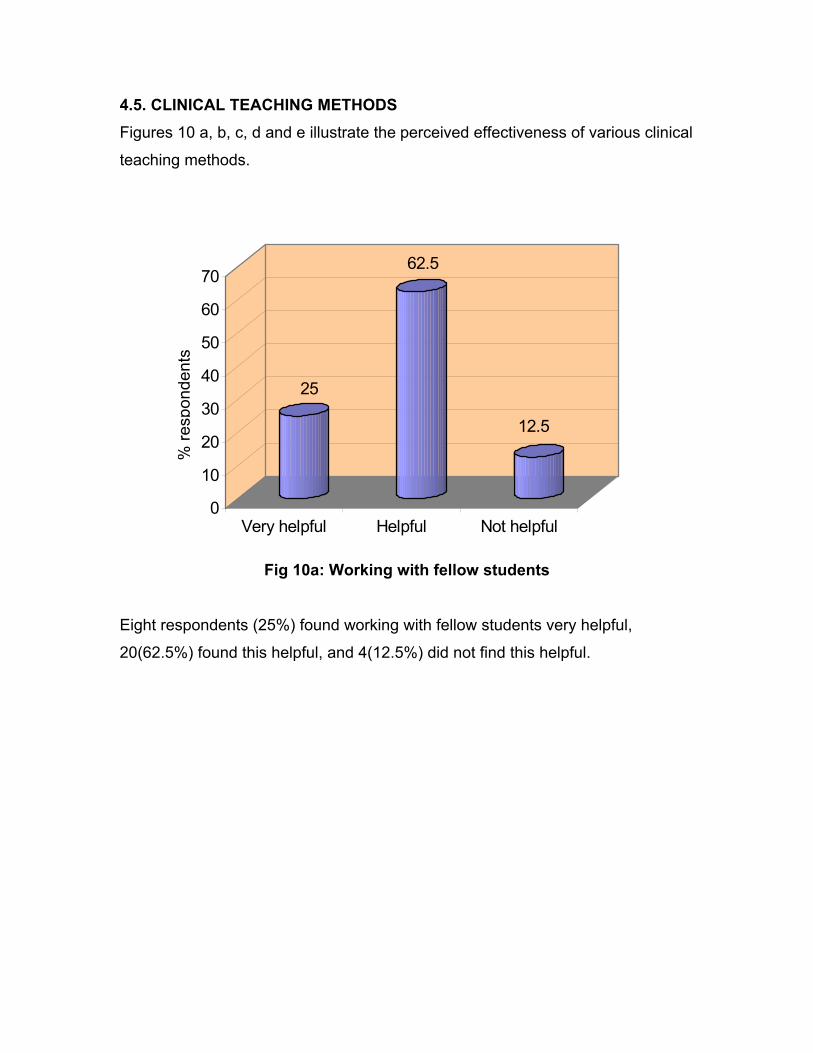
4.5. CLINICAL TEACHING METHODS Figures 10 a, b, c, d and e illustrate the perceived effectiveness of various clinical
teaching methods.
25
62.5
12.5
0
10
20
30
40
50
60
70
Very helpful Helpful Not helpful
% re
spon
dent
s
Fig 10a: Working with fellow students
Eight respondents (25%) found working with fellow students very helpful,
20(62.5%) found this helpful, and 4(12.5%) did not find this helpful.
76.67
20
3.33
0
10
20
30
40
50
60
70
80
Very helpful Helpful Not helpful
% re
spon
dent
s
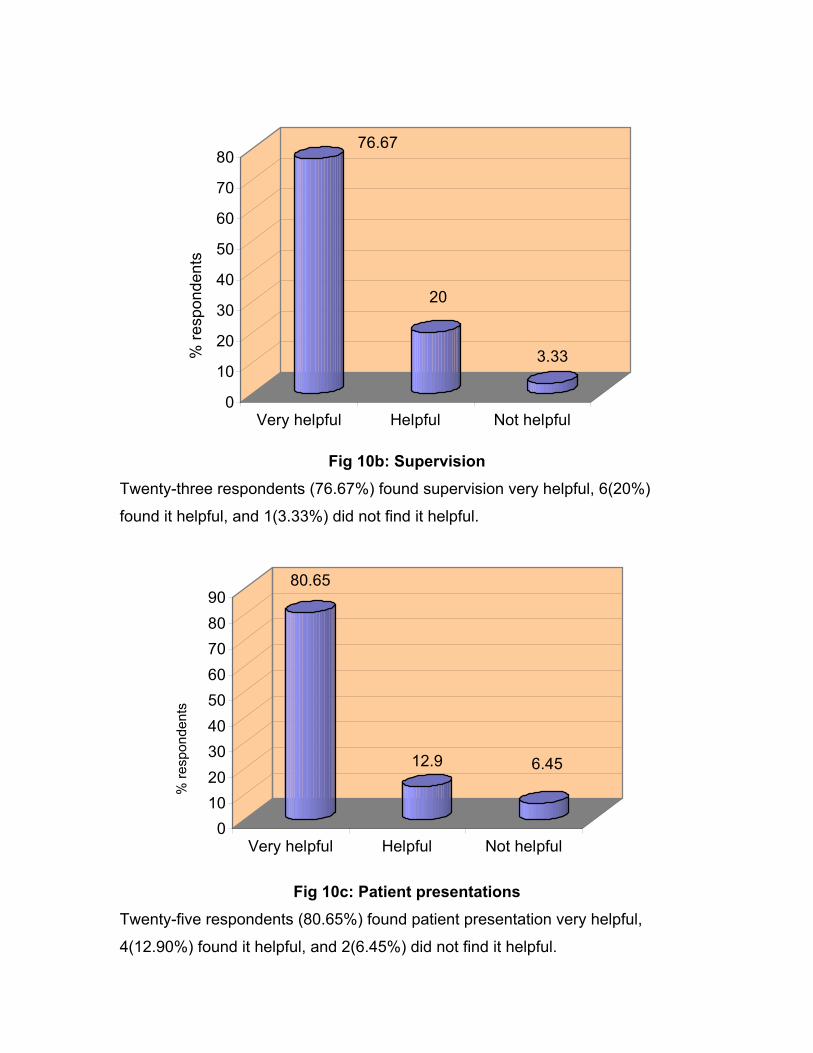
Fig 10b: Supervision
Twenty-three respondents (76.67%) found supervision very helpful, 6(20%)
found it helpful, and 1(3.33%) did not find it helpful.
80.65
12.9 6.45
0102030405060708090
Very helpful Helpful Not helpful
% re
spon
dent
s
Fig 10c: Patient presentations
Twenty-five respondents (80.65%) found patient presentation very helpful,
4(12.90%) found it helpful, and 2(6.45%) did not find it helpful.
48.28 44.83
6.9
05
101520253035404550
% re
spon
dent
s
Very helpful Helpful Not helpful
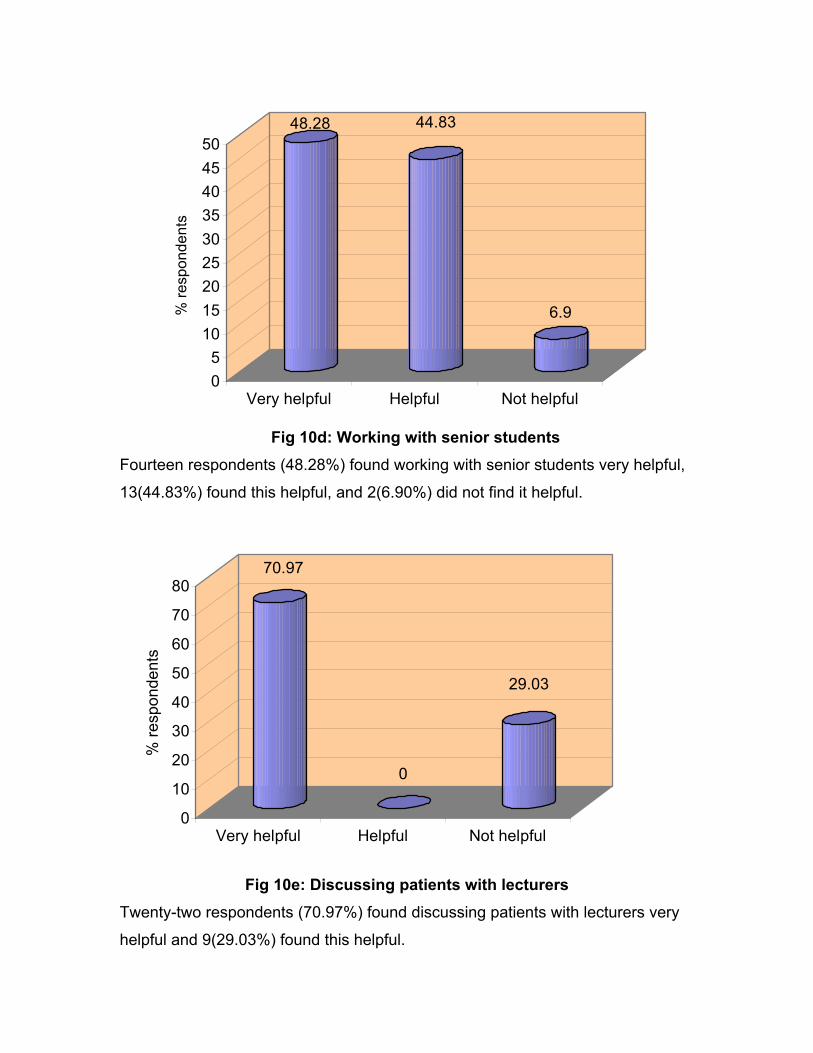
Fig 10d: Working with senior students Fourteen respondents (48.28%) found working with senior students very helpful,
13(44.83%) found this helpful, and 2(6.90%) did not find it helpful.
70.97
0
29.03
0
10
20
30
40
50
60
70
80
% re
spon
dent
s
Very helpful Helpful Not helpful
Fig 10e: Discussing patients with lecturers Twenty-two respondents (70.97%) found discussing patients with lecturers very
helpful and 9(29.03%) found this helpful.
CHAPTER 5 DISCUSSION Curriculum evaluation is an intensive and lengthy process. The purpose of this
research report was to obtain supplemental information with the aim of
determining whether past physiotherapy graduates from the University of the
Witwatersrand, considered the OMT undergraduate curriculum content, teaching
methods and clinical learning adequate and relevant to clinical practice.
Curriculum is discussed in general. Perceptions of the graduates regarding OMT
curriculum content, teaching methods adopted in OMT teaching, and clinical
learning are discussed together with the demographic details of the sample.
5.1. CURRICULUM EVALUATION
a) Definition of curriculum evaluation The definition of curriculum evaluation is to systematically collect relevant
information about the course. The information is interpreted and then used to
judge how well a course is meeting its goals. Finally, action is taken to make
improvements (Wolf, 1984; Coles and Grant, 1985).
When evaluating courses, we assess the values we need to develop in students.
The best way to do this is to evaluate students in clinical practice (Wolf, 1984).
One may also evaluate students by surveys, interviews, or focus groups. These
will assist lecturers in determining if the course achieved its stated goals.
Examining the goals, objectives and content regularly and systematically may
also facilitate curriculum development (Shepard and Jensen, 2002).

b) Reasons for curriculum evaluation
Evaluation should be an ongoing process in our planning that results in regular
modifications of the curriculum. Terminal evaluation is carried out to assess the
final product to establish whether it achieves what it sets out to do, and whether it
does it better than other possible approaches (Wolf, 1984). Problems concerning
the way the curriculum is run and reasons for these problems are also
determined by this information (Coles and Grant, 1985).
c) Factors to consider in curriculum evaluation
Curriculum evaluation may involve assessing various factors viz. methods of
teaching, timetabling, allocation of staff and resources, the effectiveness of
laboratory work, the attitudes and values of staff and students, and the
relationships between learning experiences and examination success.
Anyone associated with an educational event may be involved in its evaluation
i.e. lecturers or students. Students should be the beneficiaries of this undertaking
and should be involved in the process (Coles and Grant, 1985).
d) Classes of information obtained in curriculum evaluation:
Supplemental information
Classes of information obtained in the evaluation process may include
information on the learners’ development, execution of the programme,
comparing the intended and achieved programme and cost of the programme.
One of these classes of information is supplemental information. This aspect is
expanded on since it relates directly to this research report. Supplemental
information includes opinions and views of students, lecturers, administrators,
community members and others. This information can play an important role in
evaluating the overall worth of a programme. One is able to determine:
1) how the programme is perceived by different groups,
2) whether there is a discrepancy between what is perceived to be taking place,
and what is actually taking place,
3) what additional information is needed to help one see why people are holding
these views (Wolf, 1984).
This information is important since it gives feedback on how the students
(consumers of the course) envisaged the curriculum since the curriculum on
paper may not be what actually occurs. The intentions of the planners may not
be carried out. The students’ experience may be quite different from what it was
envisaged to be. Their observations or comments should therefore be
considered. The task of the evaluator is to look at their responses in relation to
relevance of the content. Content analysis has therefore been found to be of use.
As mentioned earlier, lecturing staff may not be aware of deficiencies of content,
less effective teaching methods, course layout/ organization etc. The students,
who have experienced the curriculum and been direct recipients of the
information, will be in a better position to judge its effectiveness (Coles and
Grant, 1985).
There should not be too much emphasis placed on supplemental information
alone. Evaluation studies should consider this information together with the other
classes of information listed above.
Supplemental information can be gathered through questionnaires and interview
techniques. Results of these studies show that extreme views concerning
courses are rare. Reactions are usually mild and new courses are generally
accepted if they are well thought out and presented. However, one is never sure
what views and reactions may be so one needs to find them out. A subclass of
supplemental information involves finding out how well national needs have been
met (Wolf, 1984).
Another subclass of this information is the ‘side-effects’ or unintended effects of
educational programmes, courses and curricula. The unintended effects of
programmes may be positive or negative. A positive unintended effect may be
that students’ interests have been stimulated and their attitudes developed. The
reverse may also occur. A way of determining ‘side-effects’ is through the use of
follow up procedures. Following learners into the first few years of employment
can furnish one with this information. The detection of ‘side-effects’ is thought to
be easier when conducting studies using unstructured interviews and open-
ended questionnaires (Wolf, 1984).
It is necessary to establish if an unintended effect occurring with one group of
learners occurred with another group. If not, it may not be the course or
curriculum that has caused the particular ‘side-effect’. It is therefore desirable
that one assesses more than one group of students or graduates. Effects that are
found in one group can be compared to another. These effects would be useful
to ascertain since negative ‘side-effects’ that are detrimental to learning can be
identified and eliminated while positive ‘side-effects’ can be maintained (Wolf,
1984).
Gathering supplemental information
In obtaining the information, conflicting results may be found but generally one
finds a great deal of agreement amongst members of the specific group studied.
Protection should be given to those who are participating. Anonymity assurance
is sufficient for the participants to be open and candid (Wolf, 1984).
e) Sampling considerations in curriculum evaluation studies
A probability sample is one in which every member of the population has a
known and non-zero chance of being included in the sample. Sampling is widely
used in research. It is accepted since it is often impossible to obtain information
from every member of the population. In evaluation studies, the situation is often
different. A course or curriculum has been developed for a particular group who
are usually very accessible. Also, one is focusing on a particular group that was
exposed to a specific curriculum. Therefore, the whole group should be sampled
(Hicks, 1999) as in this study. This sample of learners that are being studied may
be regarded as representative of all learners i.e. current and future who are to be
exposed to the programme. This group can be used as a basis for inference as
long as the population of learners in the future does not change drastically every
year (Wolf, 1984).
Analysis and interpreting supplemental information in evaluation studies
This depends on the form of the data. Information gained from interviews and
reports from discussions need to be summarized in narrative form and
qualitatively analysed. However, attitude and opinion measures from
questionnaires i.e. closed- ended questions can be quantified (Wolf, 1984).
When looking at opinions, views and reactions, one should pay attention to
extreme results e.g. strong reactions. The majority of the group may feel that it
was ineffective or very effective. This is significant and may be compared to other
areas of evaluation (Wolf, 1984).
5.2. THE WITS OMT CURRICULUM CONTENT In 1997-1999, all OMT teaching was covered in third and fourth year at Wits.
When asked about the third and fourth year curriculum content, most
respondents (87%) agreed that the curriculum was relevant to clinical practice.
Forty two percent, however, found the content inadequate. Some reasons why
they thought it was inadequate, were given in the interview while others were
given in response to certain questions in the questionnaire.
The following paragraph outlines the perceived inadequacies of the curriculum.
Information regarding the following aspects were perceived to be insufficient:
a) Patient education, advice and counseling relating to OMT.
b) Psychosocial aspects, interpersonal skills, and communication skills
required for the management of patients with neuromusculoskeletal
conditions.
c) Instruction in applying the above skills.
d) Clinical reasoning skills.
e) Clinical time.
f) Joint, soft tissue, neural mobilization concepts, psychosocial aspects, and
specific conditions.
The above topics will be discussed now except for clinical reasoning skills and
clinical time that will be discussed under clinical learning. There are many OMT
concepts that may be taught to students at an undergraduate level. However,
each OMT concept is unique and has to be understood well in order for the
student to practice it. They also need to learn the technical skills that go with
each concept. This can take much time to learn since they have to be applied
very precisely to get the desired effect. The lecturer may therefore make
reference to these concepts, so that the students hear about them. He/ she may
not be able to actually teach them in detail due to inadequate time, staff and
facilities (Kelly, 1987; Shepard and Jensen, 2002). However, the present content
should be examined. Certain topics may be less important and can be replaced
with more relevant information on other OMT concepts and specific conditions as
indicated by the respondents.
The respondents indicated that there was perhaps inadequate emphasis or
information relating to psychosocial issues and communication. This part of the
curriculum should be improved on since much of OMT learning is now based on
the biopsychosocial model. The physiotherapist should address psychological
factors in combination with passive treatments like mobilization. This is because
cognitive- behavioural strategies can be effective in dealing with pain and
improving functional outcomes (Shacklock, 1999). Education of the patient can
be integrated with OMT. When treating pain, for example, physiotherapists often
need to discern if physiological, psychological, environmental or behavioural
factors have a contributory role. In recent years, researchers have discovered
that physiotherapists have to address the above factors and may therefore adopt
a combination of interventions to reduce pain. This multi-faceted approach to
back pain is necessary in order to be effective (Li and Bombardier, 2001;
Pinnington, 2001). The curriculum has to address all factors that have a bearing
on the patient’s problem. It should include the necessary information that
physiotherapists will require to identify and deal with the above issues
adequately. This will prepare students to holistically manage their patients.
In conjunction with acquiring the above knowledge, students should learn how to
communicate appropriately with patients in order to obtain relevant information
related to psychosocial aspects e.g. illness behaviour. They need to be able to
deal with these factors to an extent, and know how and when to make referrals to
other health professionals.
Respondents also indicated their use of various OMT related therapies. Almost
100% of the sample always or sometimes uses Maitland, myofascial release,
neural, Mulligan, and McKenzie techniques. These techniques are popular and
this finding probably compares well to OMT practice in South Africa. Rocabado
and Cyriax’ concepts, muscle energy techniques and exercise were used less
often. Although the first three concepts are more rarely practiced, it is quite
alarming that exercise is hardly used in treatment by this sample. While passive
therapies e.g. joint, soft tissue, neural mobilization, and posture correction are
important, and are often indicated in treatment, modern day practice tends to
lean towards the use of active therapies like exercise. Exercise empowers the
patient to participate and continue in treatment even after their physiotherapy
management is over. Twomey (1992) and Goldby (1997), advocate the use of
exercise indicating the physiological benefits like the maintenance of muscle bulk
and bone mass.
Previously, it was common practice for the physiotherapist to simply administer
treatments such as joint mobilization and an electrotherapy treatment for
neuromusculoskeletal conditions. However, the benefits of empowering patients
so that they take responsibility for their health have been realized. A way in which
this can be achieved is to educate the patient on their condition and how to treat
and prevent further problems. Exercise prescription is usually appropriate to treat
and prevent further damage to the body.
The present curriculum does place more emphasis on exercise. The opinion of
physiotherapy lecturers in the department now, is that present physiotherapy
students use more exercise in their treatments than those in the past.
The respondents indicated that they were using much of what was covered in the
university curriculum taught to them. Studies have found that the choice of
treatment may be influenced by the physiotherapists’ academic degree. In
addition physiotherapists’ own perceptions of effectiveness influences what they
use (Li and Bombardier, 2001).
When asked specifically about the use of the Maitland concept, the majority of
the sample found it sometimes relevant and adequate, and sometimes effective
in treatment. According to surveys done to assess which modalities and
techniques physiotherapists use in practice, it was found that a multi-dimensional
approach is adopted. Many of these include passive treatment like manual
therapy e.g. Maitland (Jackson, 2001). The Maitland concept has been taught as
a basic joint mobilization concept in all South African university physiotherapy
departments. Initially much emphasis was placed on this topic since the general
treatment approach was more passive (as discussed above). Recently however,
the trend in OMT has been to rehabilitate the patient. An active therapy such as
exercise to mobilize joints and soft tissue and strengthen muscles has more long-
term benefits. Therefore, although Maitland should be included in the curriculum,
the lecturer should also teach other treatment modalities found to be effective in
managing neuromusculoskeletal conditions. When considering which joint
mobilization concepts to teach, South African physiotherapy schools have
chosen to keep the Maitland concept in the curriculum. The Maitland assessment
is especially good to teach since it is well understood in OMT practice. Reference
is often made to the Maitland assessment and certain treatment techniques at
postgraduate level and in international clinical settings. It provides a good
foundation for students. They can easily build on it and add to this knowledge in
later years. While other joint mobilization concepts are also popular, they cannot
be taught in the short space of time allowed in the curriculum. However, it may
be useful for students to know that these concepts exist, so that they can study
them further if they choose to.
The respondents also wanted to spend more time learning fewer Maitland
techniques (those commonly used in practice), and have more assistance in the
practical sessions. The present OMT curriculum teaches the commonly used
techniques for each peripheral joint and for the spine. This gives the student
adequate time to learn the each technique well. More assistants are now
allocated to the practical sessions wherever possible so that students have
enough help. For several years, the class sizes were larger and this made
teaching of practical skills harder. The present first year class, however, has
fewer students so teaching in these sessions should be more manageable in the
future.
Ninety four percent of the sample would like to learn the principles of other joint
mobilization concepts. However, as discussed earlier, these should be
mentioned but cannot be taught in detail.
Perceptions on alternative and complementary therapies (CAM) were obtained. A
hundred percent of the sample would have liked more information on this subject.
Although this may be beneficial to include, the time allocated may be just enough
for core content only. Secondly, there may be insufficient evidence to support the
theories these therapies are based on. A study by Murdoch-Eaton and Crombie
(2002) showed no statistical differences between one group of students who had
knowledge on CAM, and another (which did not have knowledge on CAM)
regarding their ability to evaluate CAM therapies or advise patients.
While this information may be interesting, it may not be what students have to
know before graduating (Kelly, 1987; Shepard and Jensen, 2002). Perhaps, one
could give a very brief idea of CAM therapies so that students are aware of what
treatment options are available to a patient. It may also help them understand the
kind of treatment a patient may have had if they came for physiotherapy after, or
whilst having CAM.
When asked about introduction of OMT into the curriculum, most respondents felt
that it should be introduced in the third year of study. Also, according to
responses to other questions, the majority felt that more information be added to
the curriculum. If OMT started in third year only, and we added more information
into the curriculum, it would increase the already large volume in third and fourth
year. It may not be possible to teach all of this in just two years of study. The
respondents may not realize this due to lack of teaching experience.
The interview responses were different. Most of those who were interviewed
prefer OMT to be introduced into second year. However, they thought that others
thought third year was appropriate since clinical work starts in this year of study
and students are therefore able to apply their knowledge better at this stage.
Although the sample felt third year was a good starting point, they (90%) also felt
that second year students were ready to be taught assessment and treatment
techniques. About 87% also felt that training of basic clinical skills could start in
second year in a clinical environment.
This discrepancy may be due to the fact that the physiotherapy curriculum at the
University of the Witwatersrand starts in second year. Second year is loaded with
basic physiotherapy subjects. The added OMT volume may crowd the
curriculum. If changes are made to the entire physiotherapy curriculum so that
courses are brought forward to first year, it may be possible to include more OMT
information in second year. Also, if the second year curriculum had a clinical
component e.g. visits to the outpatient department, OMT topics would be suitable
to include. Therefore, the appropriate decision would be re-arrangement of the
entire physiotherapy curriculum so that OMT subjects are covered in a space of
three to four years instead of two years.
5.3. TEACHING METHODS The results from this study indicate that active learning methods were preferred
by this sample of graduates. Interactive learning or active learning methods have
been found to be more effective than passive methods e.g. lecturing (Matthews,
1989). The problem-based approach is a more in-depth approach to learning
because students analyse and integrate information, as opposed to the passive
absorbing of information (Lowry, 1983). In a study by Lake (2001), additional
reading and discussions in class facilitated learning. Students’ marks in this class
were higher than those in the group that were being lectured to. The students in
our department are given additional reading for the block. They should perhaps
be asked to set aside time during the OMT block to discuss some of these topics.
Active learning may help them to apply the information better.
The respondents found tutorials, practical sessions and workshops to be more
effective than lectures. Fifty eight percent found tutorials very effective, sixty eight
percent found practical sessions very effective, and fifty eight percent found
workshops very effective. Only thirteen percent found lectures a very effective
teaching method. While lectures are useful to initially teach/ give large amounts
of basic information (Shepard and Jensen, 2002; Matthews, 1989), tutorials,
workshops/seminars and practical sessions that allow discussion and facilitate
problem solving are effective in getting students to consolidate their knowledge

(Matthews, 1989; Lowry, 1993; Lake, 2001). During some practical sessions,
discussion with other students and the facilitator help students to clarify facts and
resolve problems. The clinical blocks run by the physiotherapy department also
includes tutorial sessions. Lecturers and clinical teachers present patients or
allow students to present patients to the group of students allocated to the
placement. This helps to facilitate discussion around various OMT topics. At the
end of the rotation, case presentations are made by groups of students. A
discussion follows each presentation so that the audience can ask questions or
add information.
If the department chose to have more active learning, it should be introduced
gradually. Students may perceive that the course or the lecturer is not effective
since they are not being given all the information (Lake, 2001). Students prefer
passively absorbing information from the lecturer rather than sourcing it
themselves probably because this is easier to do.
Most respondents (74%) would not like Maitland techniques to be taught the way
they were taught to them. According to the interview results, they would have
preferred to cover application of the techniques to various conditions. This has
been addressed subsequent to 1999. The present curriculum encourages
problem solving in some of the OMT practical sessions. Once techniques are
taught, case scenarios are given to the students so that they can apply what they
have learnt when treating a particular condition. In some sessions, they are
exposed to patients in the outpatient department. After spending time assessing
and treating the patient, they present their findings to the class. A discussion
follows each presentation. More patient presentations to the class by lecturers
may be of great value. This will have to be incorporated into the curriculum.
5.4. CLINICAL LEARNING Most respondents (67%) indicated that there was insufficient teaching in clinical
reasoning. In the interview, the participants suggested that clinical reasoning be
facilitated by problem solving exercises and bedside teaching. Literature
supports the fact that feedback from supervisors and lecturers is useful (Groves
et al, 2002; Jones, 1995). Clinical reasoning is a cognitive process that needs to
be developed by the methods mentioned above together with exposure to expert
clinicians. The patient presentations, case presentations and problem-solving
practical sessions mentioned earlier are a good means of teaching clinical
reasoning skills. However, additional time is needed in the curriculum to include
more patient presentations and problem solving practical sessions. Students do
get feedback from lecturers and clinical teachers on some of their management
of patients which helps to teach clinical reasoning. Documentation by the student
is also assessed and it is quite clear to follow their thinking processes when
looking at the patient files. One can then correct or improve this.
Ninety seven percent thought that undergraduate students would benefit from
interaction with lecturers who lecture in postgraduate courses. Postgraduate
lecturers are often regarded as being expert clinicians. They will therefore
facilitate or further develop clinical reasoning skills. Whenever possible, specialist
OMT lecturers are now asked to do a workshop or give a lecture to students.
Their input in the clinical blocks would also be of great value.
According to the literature, creativity is stifled in medical curricula (Lippell, 2002).
Only 32% of the respondents felt that the OMT curriculum allowed for innovation
and their own creative ideas. The rest felt that that the curriculum never or
seldom offered this opportunity. When asked about how creativity could be
encouraged in the curriculum, participants responded that exposure to more
approaches or methods of treatment would allow creativity. They also felt that if
given the freedom to modify techniques, they would be more creative. One may
assume a rigid and strict approach when teaching OMT treatment techniques
since they are described very specifically in the textbook.
In clinical practice, one cannot adopt a very rigid approach due to the varying
situations in which patients present. Creativity may be stimulated by good
supervision, mentoring and developing a problem-based approach to teaching
(Lippell, 2002). This is also related to understanding that a patient’s problem may
be multi-faceted and addressing issues like the patient’s emotions, expectations,
and other psychosocial factors. Creativity in clinical reasoning may be
encouraged by getting the student to be aware of not only the patient’s condition,
but also the context of their presentation e.g. the patient’s interpretation of their
pain and how it affects their work and personal life.
Creativity in the present curriculum is expected of students at certain times and
not others. It is expected in most cases when students are planning treatments.
They are not given a specific selection of techniques or modalities to use for
each condition. They can choose any combination of treatments as long as they
are able to justify their choices. However, certain treatment techniques or
modalities may be recommended by the lecturers for specific conditions in some
teaching sessions e.g. case presentations or practical sessions. Students are
expected to know and use these. Once students have a good understanding of
the basic knowledge, have more clinical experience, and have acquired more
knowledge, they will be better able to judge how and when to change these
recommended treatment approaches. This may only be possible at a later stage
e.g. end of fourth year or post-qualification in most cases.
The literature shows that the effectiveness of a clinical placement depends on
other factors as well (Dolmans, et al 2001; 2002). A high ‘patient mix’ i.e. seeing
patients with a variety of conditions, and a high level of supervision is necessary
to make the placement effective. Time wasted on ‘non-instructive’ activities (not
defined in the literature) did not contribute to learning. The response to one of the
questions illustrated the value of supervision. Seventy seven percent found
supervision very beneficial in helping students to apply theory to practice. In
recent years, the role of the clinical teacher in the department has been well
defined. Clinical teachers from all the placements are invited to the department to
be made familiar with the department’s mission, goal and objectives, course
content and the process in which the block is run. The importance of their role in
the students’ learning is emphasized. This has helped clinical staff to participate
more in teaching in clinical blocks. Lecturers are required to visit placements
once a week as well, to increase student contact time.
Clinical teaching in the department involves many tasks for example, observing
students assess and treat patients or presenting patients to the student group.
Asking questions is also an effective way of facilitating recollection of facts or
principles (Shepard and Jensen, 2002). Questions may be of different standards
e.g. certain questions may require students to simply recall a fact, while others
need analysis and evaluation of information. Supervisors should also encourage
students to self assess their performance (Shepard and Jensen, 2002). Keeping
a reflective journal could be introduced to enable students to think about their
practice. Dolmans et al (2001) showed that time spent on reflection on
experiences and supervision improved effectiveness of the block.
Respondents found patient presentations, discussing patients with lecturers and
working with senior students very helpful. Perhaps these will also assist in clinical
learning. As discussed earlier, patient presentations are done on a regular basis.
Senior students should be recruited to help to assist wherever possible. This will
have to be well structured into the timetable.
Ninety three percent felt that eight weeks of clinical time spent in the outpatient
department practicing OMT was inadequate. Although more time may be
beneficial to the student, the curriculum may not allow for additional time to be
spent in the blocks. However, a ‘mixed’ orthopaedics and OMT block (16 weeks)
may be the answer to acquiring more clinical experience. The future
neuromusculoskeletal blocks may be arranged this way. Research has shown
that a learner’s level of attainment is directly related to the length of time actively
spent in learning. Learning also depends on whether the time allocated is
properly used (Matthews, 1989). Therefore, although clinical time may be
increased, the individual student is still responsible to make sure that they benefit
from this by spending their time wisely.
5.5. RESEARCH AND EVIDENCE BASED THERAPY IN THE OMT CURRICULUM
Thirty nine percent felt that they were often exposed to current OMT research
while 55% felt that they were seldom exposed. It has been shown in the literature
that if students are expected to do research as part of their course, they show
confidence in their ability to critically review the literature and accept the
responsibility of keeping updated (Connolly et al, 2001). The fourth year
curriculum now includes a specific research course. This may create interest in
this area and encourage students to do post-graduate research and add to the
body of information we already have. In addition to this, students can perhaps be
encouraged to do minor research projects in their clinical blocks e.g. measure
and report on the outcomes of specific treatments. This may stimulate interest in
research and develop critical thinking.
Evidence-based therapy is becoming increasingly important. It is therefore
necessary for students to be exposed to the practice of sourcing and reading the
latest literature relating to the subject and be aware of evidence-based practice.
They should be encouraged to adopt an evidence-based approach to
management of patients (Kelly, 1987). The present curriculum facilitates this
approach since students are required to do a verbal presentation of a case study
at the end of each clinical block. They have to make reference to published
literature to support their management of the patient. They are also required to
submit portfolios at the end of the elective block. The portfolio consists of three
case studies and a reflective journal. Each case study has to be accompanied by
a critique of a journal article on the subject and the clinical reasoning behind their
assessment and treatment of the patient. A reflective journal is also included and
this helps students to consider their management of patients and assess their
own thinking processes to see if their decisions were correct.
The methods mentioned above have been adopted to encourage critical thinking
that will hopefully help to raise the standard of OMT practice. University
departments have a responsibility to take the lead in finding and passing on
updated information to the rest of the profession. This will make an impact that
will help change traditional ways of thinking.
5.6. DEMOGRAPHICS OF RESPONDENTS
The majority of respondents work in an outpatient setting. Most spend time
practicing OMT. Therefore their opinions are relevant to the area of study. They
are well informed and perhaps able to judge the content better than those who
spend more time practicing in other specialist areas. However, their expectations
of the curriculum may also be higher compared to physiotherapists in general
practice and other specialist areas, since this is their area of interest. The results
indicate that some physiotherapists work in two or more workplaces listed in the
questionnaire. They did not indicate one area in which they work the most
although the question asked for this specifically.
The majority of respondents had completed over three years of practice and
therefore had a fair amount of experience in the practice of physiotherapy. Thirty
eight percent of the sample had over three years of OMT experience. These
figures indicate that the respondents were able to make reasonable judgements,
and had knowledge of the information and skills needed for effective practice.
Graduates are appropriate for this study given their recent experience of the
undergraduate curriculum and their current clinical role (Sanson-Fisher and
Rolfe, 2000).
5.7. CONCLUSION
In summary, most past graduates were practicing OMT and had a fair amount of
clinical experience. They stated that the curriculum was lacking in areas
pertaining to other OMT concepts, patient counseling and psychosocial aspects
and research. They would also like information on alternative therapies.
Wherever possible, appropriate information may be added to the curriculum.
However, not all subjects can be covered in detail in the available teaching time.
The respondents appear to be using much of what they were taught at university
in clinical practice. This shows how influential the undergraduate curriculum can
be, and emphasizes the need for regular evaluation and updating.
The respondents indicated that OMT be introduced in third year, although they
felt that second year students are ready to start some of the OMT subjects taught
in third year. This discrepancy may be due to the fact that the physiotherapy
curriculum at the University of the Witwatersrand begins in second year. They
may have therefore felt that the second year curriculum is too full or that OMT is
not appropriate at this stage since the students are not doing clinical work. A
possible change is anticipated in the future first year curriculum. Physiotherapy
teaching may start in the first year and this will make it possible for second years
to be taught OMT and to start practicing it.
The respondents preferred active learning methods. They would also prefer
Maitland techniques to be applied to the clinical situation. Case scenarios in the
present curriculum help students to learn how to apply the techniques they learn.
Perhaps more patient presentations by lecturers will also achieve this. Patient
presentations will also teach application of other OMT treatments, how to
measure outcomes and educate patients. With regards to clinical learning,
respondents preferred that clinical reasoning skills be developed to a greater
extent. They suggested that bedside teaching, problem solving exercises, and
exposure to expert clinicians would facilitate this. This is also supported by the
literature. The practical sessions in the department include problem-solving
exercises and expert clinicians are invited to give some lectures or conduct
practical sessions. Unfortunately a lack of funding does not always permit outside
lecturers to participate in teaching.
The respondents also felt that more clinical time was needed and that
supervision was very valuable in contributing to clinical learning. Clinical
supervision is considered very important in the department and clinical teachers
and lecturers have been allocated to all placements. Students and staff also give
patient presentations. Clinical time for this block may be increased in the future.
A limitation of the study is that the researcher carried out the interviews. This
could have introduced an element of bias although it appears from the above
discussion that graduates were honest in their opinion. Also, a specific format
was followed when the interviews were carried out. This would reduce bias.

CHAPTER 6 CONCLUSION
In this study, it was found that 25.81% of respondents found the third and fourth
year OMT content adequate while 41.94% found it inadequate. Eighty one
percent found the OMT curriculum relevant.
Ninety four percent of respondents would like information on other OMT
concepts. Fifty five percent indicated that they found information on patient
education and advice lacking. Sixty six percent would like more teaching on
aspects related to the biopsychosocial model. Other areas of inadequacy
included biomechanics, functional anatomy, posture and ergonomics, alternative
therapies and pathology. Content is being revised and when complete, will
include more relevant information e.g. psychosocial aspects relating to back pain.
The respondents felt that the curriculum may be made more relevant if there was
more emphasis on clinical reasoning and application of treatment modalities to
the clinical situation. Exposure to research would also make the practice of OMT
relevant in the clinical setting. Only 38.71% felt that they were often exposed to
current research in OMT.
Active teaching methods were preferred instead of passive learning. Only 13% of
the sample found lectures effective while graduates preferred tutorials, practical
sessions and workshops.
With regards to clinical learning, respondents felt that the development of clinical
reasoning skills was needed. Sixty seven percent indicated that they had
insufficient teaching in this area. Supervision, patient presentations and
discussion of cases with lecturers were found to be very helpful.
The current curriculum is being revised. More information has been included on
posture, ergonomics, biomechanics, pathology, and patient advice and
education. In the pre-clinical teaching in 2006, there will be time available to
relate more information to the biopsychosocial model and other OMT concepts.
There will be time to briefly inform the students on the role of alternative
therapies.
The 2005 first year undergraduate physiotherapy students are for the first time
covering some physiotherapy topics. This makes it easier to teach the OMT
content over the four years of study (and not three years as previously). All of the
content with the exception of a few topics will be taught by the end of the 3rd year
of study, allowing for consolidation of knowledge in 4th year. The new curricular
arrangement gives the lecturer more time with the students making it possible to
use more active learning methods e.g. problem solving exercises. This should
improve clinical reasoning skills.
Supervision in the clinical placements has increased. A university supervisor
attends the placement every week. Clinical supervisors are aware of their role
and have meetings with the block coordinator (at least twice a year) besides the
informal meetings at the clinical placements. Supervision involves patient
presentations, bedside teaching and discussion of patients’ conditions,
assessments and treatment plans. This helps to develop the students’ clinical
reasoning skills.
The students are more exposed to research. They are given research articles to
read in their clinical block. They do a research course in third and fourth year in
which they learn research skills. They are also required to do a literature review
for their case presentations at the end of each block.

Changes to the curriculum have therefore started and will continue to be made
until it includes all the relevant content.
6.1 RECOMMENDATIONS
The results of this study indicate that the OMT curriculum content taught at the
University of the Witwatersrand be inclusive of more topics which are relevant to
practice today. Wherever possible, students should be taught how to apply their
knowledge in clinical practice. More clinical time (extended blocks) and teaching
is also recommended.
A plan for future fourth years would be to include some of the present fourth year
curriculum (spinal mobilization) into third year. The present third year curriculum
has several free lecture periods in the second half of the year. Perhaps the
foundation for treating spinal patients should be laid down at the end of third year
to allow for more application and problem solving in the fourth year pre-clinical
block. The entire OMT curriculum (second year to fourth year) should be
organized in such a way that there is continuity and sequence (Shepard and
Jensen, 2002). Continuity refers, for example, to getting the students to practice
and develop manual techniques. This involves learning and revising in several
practical sessions. Sequence is the process of building one experience on
another. Therefore, after the techniques are learnt, one can introduce case
scenarios to teach students how to select the correct techniques and apply them.
More difficult scenarios where selection of correct techniques is not so obvious,
and where students have to modify them before they are applied, may follow this.
Ninety three percent felt that eight weeks of clinical time spent in the outpatient
department practicing OMT was inadequate. Perhaps a mixed orthopaedics and
OMT block would allow students to have more exposure to patients requiring
OMT assessments and treatments.
Future research in this area may be done to compare OMT curricula taught at
other physiotherapy departments in the country. This may give more clues as to
which topics are relevant for undergraduate OMT study.

A similar study to this should be carried out after changes are made to the OMT
curriculum to see if there has been an overall improvement.
There should be ongoing evaluation of the OMT curriculum so that it is always
relevant to the current situation in South Africa, and of a sufficiently acceptable
standard comparable to OMT practice around the world.
REFERENCES
Bandaranayake R 2000 The concept and practicability of a core curriculum in
basic medical education. Medical Teacher 22(6): 560-564
Ben-Sorek S, Davis CM 1988 Joint Mobilization Education and Clinical Use in the
United States. Physical Therapy 68(6): 1000-1004
Bradshaw D, Groenewald P, Laubsher R, Nannan N, Nojilana B, Norman R,
Pieterse D, Schneider M 2003 Initial estimates from the South African Burden of
Disease Study. MRC Policy Brief (1)
Coles CR, Grant JG 1985 Curriculum evaluation in medical and health care
education. Medical Education 19: 405-422
Concha ME, Nyathi E, Dolan C 1995 Community rehabilitation workers:do they
offer hope to disabled people in South Africa’s rural areas? International Journal
of Rehabilitation Research 18(3): 187-200
Connolly BH, Lupinnaci NS, Bush AJ 2001 Changes in attitudes and perceptions
about research in physical therapy among professional physical therapist
students and new graduates. Physical Therapy 81(5): 1127-1134
Cormack DFS 1991 The Research Process in Nursing, 2nd edition Chap 20 –23.
Blackwell Science Ltd, Oxford
Dolmans DHJM, Wolfhagen IHAP, Essed GGM, Scherpbier AJJA, van der
Vleuten CPM 2001 Students’ perceptions of time spent during clinical rotations.
Medical Teacher 23(5): 471-475
Dolmans DHJM, Wolfhagen IHAP, Essed GGM, Scherpbier AJJA, van der
Vleuten CPM 2002 The impact of supervision, patient mix, and numbers of
students on the effectiveness of clinical rotations. Academic Medicine 77(4): 332-
335
Goldby LJ 1997 Low back pain: The evidence for physiotherapy. Physical
Therapy Review 2:7-11
Groves M, Scott I, Alexander H 2002 Assessing clinical reasoning: a method to
monitor its development in a PBL curriculum. Medical Teacher 24(5): 507-515
Hawes H 1982 Curriculum and Reality in African Primary Schools, 1st edition
Chap 2. Longman Group publishers, Singapore
Hicks CM 1999 Research methods for clinical therapists. Applied project design
and analysis, 3rd edition Chap 3. Churchill Livingstone, Edinburgh
Howe A 2002 Professional development in undergraduate medical curricula.
Medical Education 36(4): 353-359
Jackson DA 2001 How is low back pain managed? Physiotherapy 87(11): 573-
581
Jones M 1995 Clinical reasoning and pain. Manual Therapy 1:17-24
Katavich L 1998 Differential effects of spinal manipulative therapy on acute and
chronic muscle spasm: A proposal for mechanisms and efficacy. Manual therapy
3(3): 132-139
Kelly AV 1987 The curriculum. Theory and practice, 1st edition chapter1 and 3.
Harper and Row, London

Lake DA 2001 Student performance and perceptions of a lecture-based course
compared with the same course utilizing group discussion. Physical Therapy
81(3): 896-902
Li LC Bombardier C 2001 Physical therapy management of low back pain: An
exploratory survey of therapist approaches 81(4): 1018-1027
Lippell S 2002 Creativity and medical education. Medical Education 36(6): 519-
521
Lowry S 1993 Medical education, 1st edition Pg 27. BMJ publishing group,
London
Matthews J 1989 Curriculum exposed, 1st edition chap 1-10. David Fulton
Publishers, London
McNeil J 1996 Curriculum: a comprehensive introduction, 5th edition chap 4.
Harper Collins College publishers, New York
Murdoch-Eaton D, Crombie H 2002 Complementary and alternative medicine in
the undergraduate curriculum. Medical Teacher 24(1): 100-102
Petty NJ, Moore AP 2001 Neuromusculoskeletal examination and assessment. A
handbook for therapists, 2nd edition Pgs1-3. Churchill Livingstone, London
Pinnington MA 2001 Why are we finding it so hard to change our approach to low
back pain? Physiotherapy 87(2): 58-59
Professional Board for Physiotherapy, Podiatry and Biokinetics, HPCSA
Rabey M 2001 Interaction between pain physiology and movement-based
therapy. Physiotherapy 87(7): 338-339
Richardson CA, Jull GA 1995 Muscle control-Pain control. What exercises do
you prescribe? Manual Therapy 1:2-10
Richardson C, Jull G, Hodges P, Hides J 1999 Therapeutic exercise for spinal
segmental stabilization in low back pain. Scientific basis and clinical approach, 1st
edition Chap 2-11. Churchill Livingstone, Edinburgh
SAQA information booklet –The National Qualifications Framework and the
Standards Setting 2000
Sanson-Fisher R, Rolfe I 2000 The content of undergraduate health professional
courses: a topic largely ignored? Medical Teacher 22(6): 564-567
Shacklock M 1995 Neurodynamics. Physiotherapy 81(1): 9-14
Shacklock MO 1999 The clinical application of central pain mechanisms in
manual therapy. Australian Journal of Physiotherapy 45: 215-221
Shepard KF, Jensen GM 2002 Handbook for teaching for physical therapists, 2nd
edition Chap 1-8. Butterworth-Heinemann, USA
Squires G 1987 The curriculum beyond school, 1st edition chap 1.
Hodder and Stoughton, London
Steffan M 1996 Myofascial trigger points and body pain. Continuing Medical
Education 14(3): 275-284
Twomey LT 1992 A rationale for the treatment of back pain and joint pain by
Manual therapy. Physical Therapy 72(12): 885-891
University of the Witwatersrand Physiotherapy Department BSc Physiotherapy
curriculum. 6th and 7th editions 2001 and 2002
Van Rooijen AJ, Van der Spuy AA 2000 The role of Physiotherapy in a changing
healthcare system. South African Journal of Physiotherapy 56(2): 3-5
Wolf RM 1984 Evaluation in education. Foundations of competency, assessment
and program review, 2nd edition. Praeger, USA

APPENDICES
APPENDIX 1 FOCUS GROUP QUESTIONNAIRE
1. What do you like about the OMT course content?
2. What do you think needs improvement concerning course content?
3. What specific suggestions do you have for changing the course/ course content?
APPENDIX 2 INFORMATION SHEET
THE PERCEPTIONS OF RECENT WITS GRADUATES CONCERNING THE
ORTHOPAEDIC MANIPULATIVE THERAPY (OMT) CURRICULUM CONTENT
My name is Anita Gounden. Thank you for taking time to read and answer this
questionnaire.
At present I am teaching the OMT undergraduate curriculum to the 2nd, 3rd and
4th year physiotherapy students at Wits. My teaching role has prompted me to
research the curriculum content to assess whether it is adequate and relevant to
clinical practice today.
OMT is a rapidly advancing field. We hear of developments in assessment and
management all the time. It is therefore important that the curriculum be regularly
evaluated and updated accordingly.
Your response to this questionnaire will play a vital role in the evaluation process.
The results will also be useful to the Professional Development committee who
are currently involved in evaluating and standardising OMT curricula around the
country.
Be reassured that your anonymity as a participant will be maintained. A number
will be allocated to the questionnaire for reference.
As a participant, you will be informed of the results of the study. Your contribution
is valuable and I urge you to please help us in this important assessment
process.
I appreciate your effort and time.
Thank you
Anita Gounden
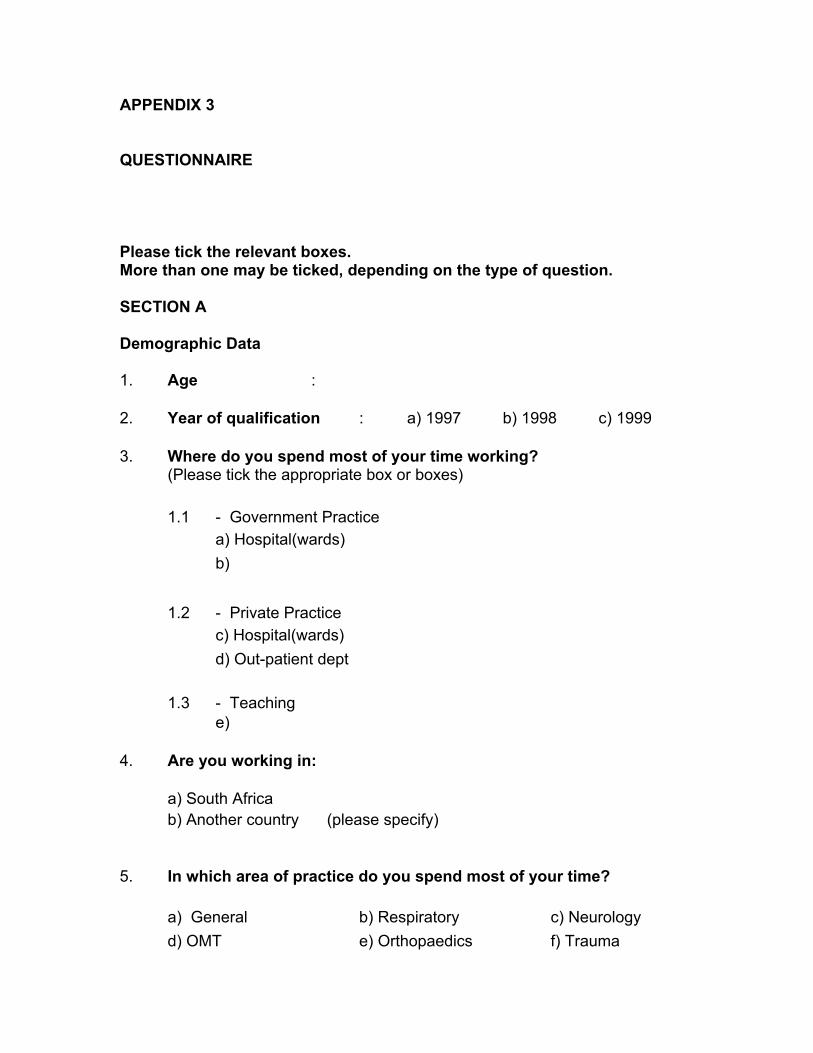
APPENDIX 3 QUESTIONNAIRE Please tick the relevant boxes. More than one may be ticked, depending on the type of question. SECTION A Demographic Data 1. Age : 2. Year of qualification : a) 1997 � b) 1998 � c) 1999 � 3. Where do you spend most of your time working? (Please tick the appropriate box or boxes)
1.1 - Government Practice a) Hospital(wards) � b) � 1.2 - Private Practice c) Hospital(wards) � d) Out-patient dept � 1.3 - Teaching e) �
4. Are you working in:
a) South Africa � b) Another country � (please specify)
5. In which area of practice do you spend most of your time?
a) General � b) Respiratory � c) Neurology � d) OMT � e) Orthopaedics � f) Trauma �
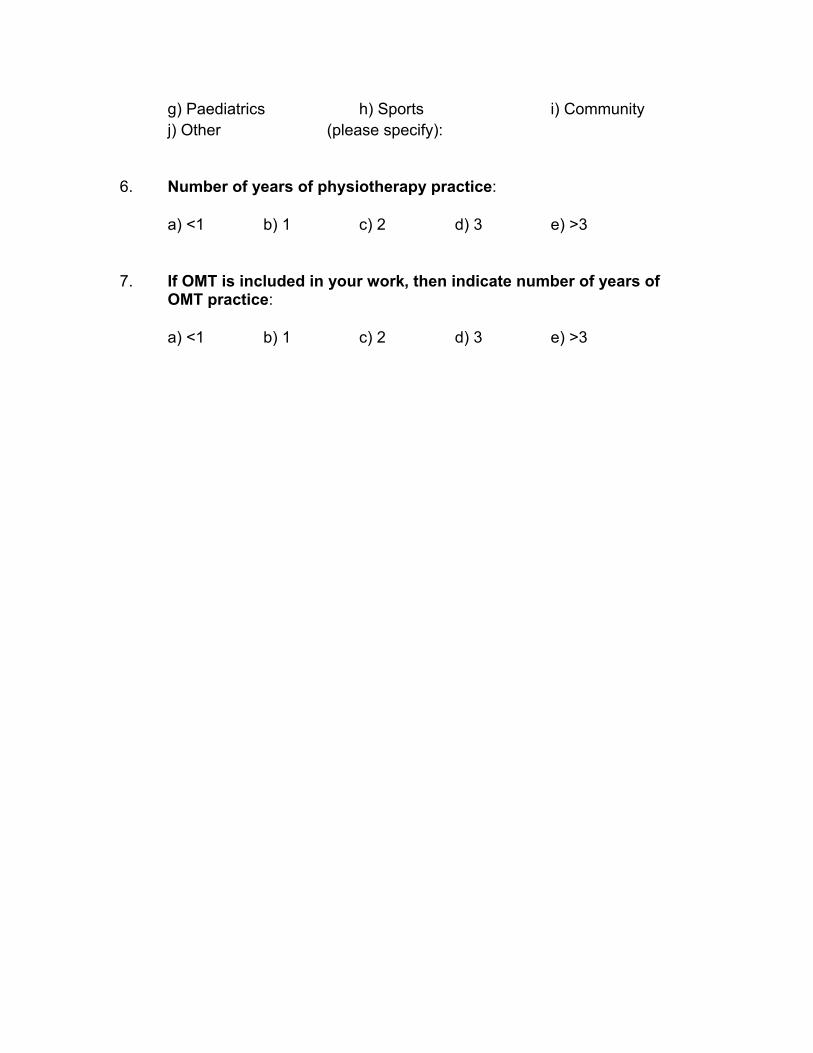
g) Paediatrics � h) Sports � i) Community � j) Other � (please specify):
6. Number of years of physiotherapy practice:
a) <1 � b) 1 � c) 2 � d) 3 � e) >3 �
7. If OMT is included in your work, then indicate number of years of
OMT practice:
a) <1 � b) 1 � c) 2 � d) 3 � e) >3 �

SECTION B Undergraduate Information 1.1 When should OMT be introduced into the undergraduate curriculum?
a) 1st Year � b) 2nd Year � c) 3rd Year � d) 4th Year � 1.2 Would you have preferred the second year syllabus to have
incorporated some third year OMT subjects: (Please tick the appropriate box)
Yes No
a) Assessment and treatment techniques of Peripheral joints 1) 2)
b) Training of Basic OMT Clinical Skills in a Clinical Environment eg: Assessment and treatment techniques of Peripheral joints, exercise programs, application of myofascial release techniques.
1)
2)
1.3 What are your opinions concerning the curriculum content in third
and fourth year? (Please tick the appropriate box)
1.3.1 Third and fourth year curriculum content was relevant to clinical
practice:
a) Agree � b) Neutral � c) Disagree � 1.3.2 Was adequate for clinical practice:
a) Agree � b) Neutral � c) Disagree � 1.4 In your third and fourth year you were taught the Maitland concept of
assessment and treatment techniques for peripheral and spinal joints.
Have you found this concept: (please tick the appropriate box in 1.4.1.1 and 1.4.1.2)
1.4.1.1 a) Relevant � b) Sometimes relevant � c) Irrelevant � for clinical practice
1.4.1.2 a) Adequate � b) Sometimes adequate � c) Inadequate �
for clinical practice
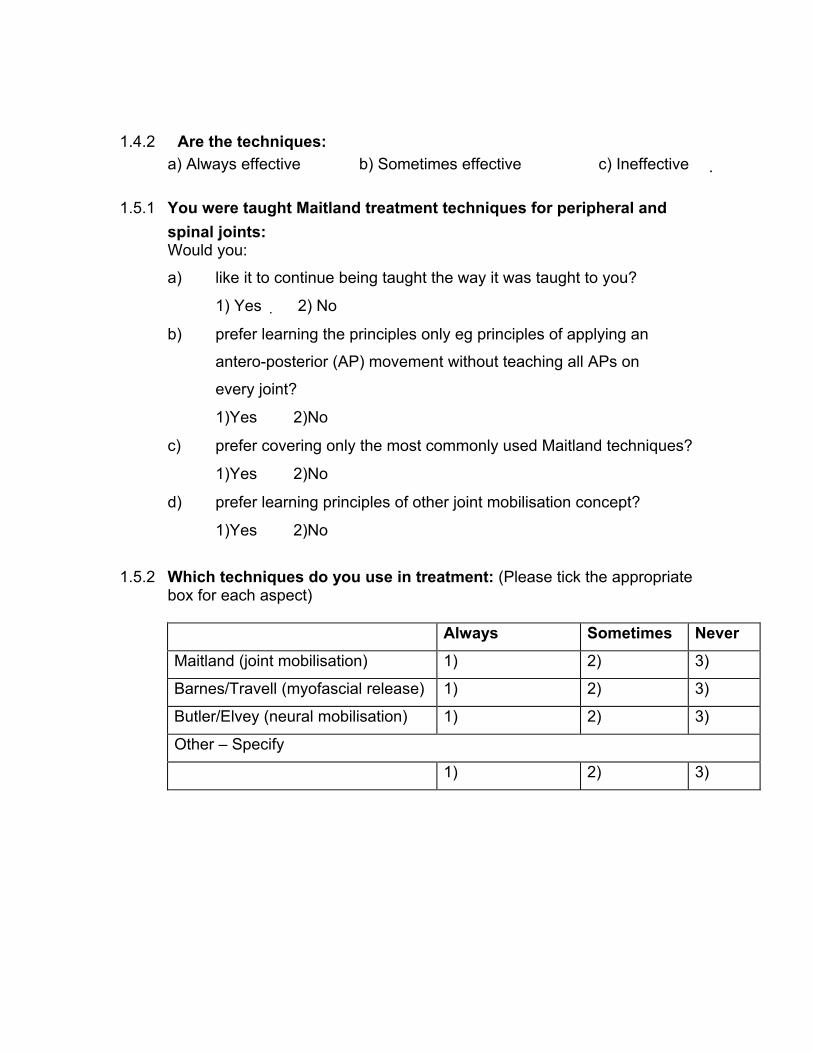
1.4.2 Are the techniques:
a) Always effective � b) Sometimes effective � c) Ineffective � 1.5.1 You were taught Maitland treatment techniques for peripheral and
spinal joints: Would you:
a) like it to continue being taught the way it was taught to you?
1) Yes 2) No �
b) prefer learning the principles only eg principles of applying an
antero-posterior (AP) movement without teaching all APs on
every joint?
1)Yes � 2)No �
c) prefer covering only the most commonly used Maitland techniques?
1)Yes � 2)No �
d) prefer learning principles of other joint mobilisation concept?
1)Yes � 2)No �
1.5.2 Which techniques do you use in treatment: (Please tick the appropriate
box for each aspect)
Always Sometimes Never
Maitland (joint mobilisation) 1) 2) 3)
Barnes/Travell (myofascial release) 1) 2) 3)
Butler/Elvey (neural mobilisation) 1) 2) 3)
Other – Specify
1) 2) 3)
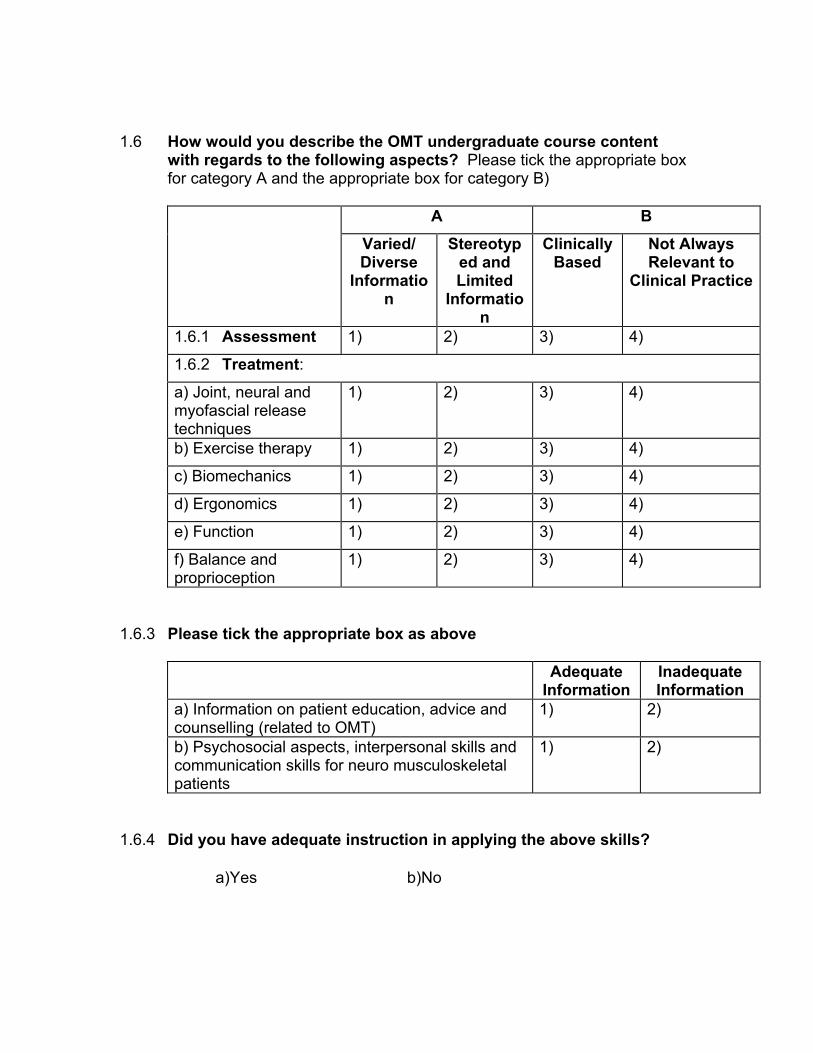
1.6 How would you describe the OMT undergraduate course content
with regards to the following aspects? Please tick the appropriate box for category A and the appropriate box for category B)
A B
Varied/ Diverse
Information
Stereotyped and Limited
Information
Clinically Based
Not Always Relevant to
Clinical Practice
1.6.1 Assessment 1) 2) 3) 4)
1.6.2 Treatment:
a) Joint, neural and myofascial release techniques
1) 2) 3) 4)
b) Exercise therapy 1) 2) 3) 4)
c) Biomechanics 1) 2) 3) 4)
d) Ergonomics 1) 2) 3) 4)
e) Function 1) 2) 3) 4)
f) Balance and proprioception
1) 2) 3) 4)
1.6.3 Please tick the appropriate box as above
Adequate
Information Inadequate Information
a) Information on patient education, advice and counselling (related to OMT)
1) 2)
b) Psychosocial aspects, interpersonal skills and communication skills for neuro musculoskeletal patients
1) 2)
1.6.4 Did you have adequate instruction in applying the above skills?
a)Yes � b)No �

1.7 Did you have sufficient teaching in clinical reasoning i.e.were you able to diagnose the structure at fault/the biomechanical basis for pain or abnormal movement?
a)Yes � b)No �
1.8 Your course content together with readings helped you to
adequately manage:
a) all patients encountered � b) most patients encountered � c) some patients encountered � d) none of the patients encountered �
1.9 In your opinion, were there any important aspects: 1.9.1 lacking in your OMT training?
a) Yes � b) No � If yes, please specify:
…………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………..
1.9.2 you think should be included into the OMT curriculum?
a) Yes b) No
If yes, please specify: ………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………………
………………………………………………………………………………….
1.9.3 you think should be excluded from the OMT curriculum? a) Yes b) No If yes, please specify:
……………………………………………………………..………………………
…………………..…………………………………………………………….……
………………………………………………………………………………………
………………………………………………………………………………………
……………………….
1.10 Did you find that the prescribed curriculum allowed for innovation
and your own creative ideas?
a) Often � b) Seldom � c) Never � If ‘seldom’, or ‘never’ was ticked, substantiate: …………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………….
1.11 Were you adequately exposed to current research in OMT ie through
actual teaching or research articles within the reading files?
a) Often � b) Seldom � c) Never � 1.12 Were you taught holistic treatment approaches?
a) Often � b) Seldom � c) Never �
1.13 Would you have liked more information about OMT related
alternative and complementary therapies eg. Chiropractic, osteopathy, biokinetics, podiatry? (Please tick the appropriate box for each)
a) Yes b) No
1.14 Were the total of eight weeks of clinical time adequate in third and fourth year?
a) Yes � b) No �
1.15 What helps teaching application of theory to practice? (Please tick the
relevant box for each)
Clinical Learning Very Helpful Helpful Not Helpful
a) Working with fellow students 1) 2) 3)
b) Supervision 1) 2) 3)
c) Patient presentation 1) 2) 3)
d) Working with senior students 1) 2) 3)
e) Discussing patients with lecturers
1) 2) 3)
1.16 How effective are the following?:
Theoretical Learning Very
Effective Sometimes
Effective Ineffective
a) Interactive learning eg tutorial groups 1) 2) 3)
b) Practicals 1) 2) 3)
c) Workshops 1) 2) 3)
d) Lectures 1) 2) 3)
1.17 Core and Optional Curricula
The Core curriculum is that part of the curriculum which is a baseline standard or essential component to a curriculum. Core competencies are the requirements to be satisfied before a new graduate assumes the responsibilities of a qualified practitioner.
The optional curriculum is a special study module for those interested in doing additional OMT training within the undergraduate curriculum. They may be interested in specializing in OMT at a post-graduate level. Institutions overseas have incorporated such “specialist” courses for undergraduates to allow them to pursue their area of interest to an extent before qualification.
1.17.1 Should an optional course be offered?
a) Yes � b) Unsure � c) No �
1.17.2 If an optional course was offered, what information do you think should be included in it?
……………………………………………………………..………………
…………………………………………………..…………………………
………………………………….…………………………………………
…………………………………………………………………………….
1.18 Do you think that undergraduate student interaction with post-
graduate program lecturers be beneficial: a) Yes b) No
POST-GRADUATE 2.1 Please give information about OMT courses you have attended since
you qualified.
Year in which course was done
Name of Course Duration of course eg week-end
2.2 Which courses listed above best supplemented your undergraduate
knowledge and why? ……………………………………………………………..……………………………….
……………………………………..………………………………………………………
…….………………………………………………………………………………………..
………………………………………………………………………………………………
…………………….
GOUNDEN/QUESTIONNAIRE.2001
APPENDIX 4
INTERVIEW QUESTIONNAIRE (WITH RESPONSES)
• Question 1 (regarding Section B question 1.1 from previous questionnaire)
Most respondents (64.52%) stated that OMT should be introduced in the 3rd year
of study. Why do you think this was so? Indicate if ‘unsure’ or ‘don’t know’.
• Question 2 (regarding Section B question 1.3.1 and 1.3.2 from previous questionnaire)
When asked about 3rd and 4th year curriculum content, most (80.65%) agreed
that the content was relevant to clinical practice but 42% stated that the content
was inadequate. Why do you think the 3rd and 4th year curriculum content was
inadequate?
• Question 3 (regarding Section B question 1.5.1)
94% of the respondents would like to learn the principles of other joint
mobilization concepts. Are there any specific OMT concepts you would like to
see included in the curriculum?
• Question 4
How do you think OMT techniques should be taught?
• Question 5 (regarding question Section B question 1.7 from the previous questionnaire)
Most respondents (67%) said that they did not have sufficient teaching in clinical
reasoning while 33% said it was adequate. How would you like to see clinical
reasoning skills being taught or stimulated in the curriculum (clinical and
theoretical curriculum)?
• Question 6 (regarding Section B question 1.10 from the previous questionnaire).
Only 32% of the respondents felt that the curriculum allowed for innovation and
their own creative ideas. The rest felt that the curriculum seldom or never offered
this opportunity. What methods may be used to allow the student to be creative
and innovative in OMT?
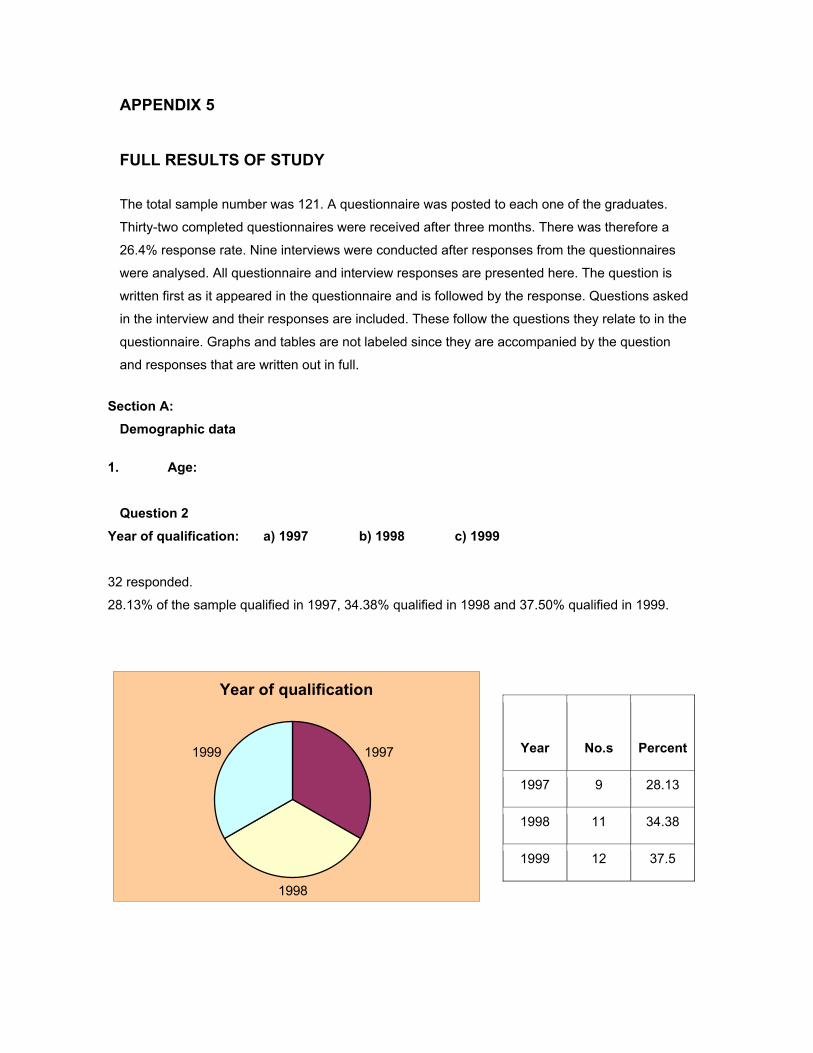
APPENDIX 5 FULL RESULTS OF STUDY The total sample number was 121. A questionnaire was posted to each one of the graduates.
Thirty-two completed questionnaires were received after three months. There was therefore a
26.4% response rate. Nine interviews were conducted after responses from the questionnaires
were analysed. All questionnaire and interview responses are presented here. The question is
written first as it appeared in the questionnaire and is followed by the response. Questions asked
in the interview and their responses are included. These follow the questions they relate to in the
questionnaire. Graphs and tables are not labeled since they are accompanied by the question
and responses that are written out in full.
Section A:
Demographic data 1. Age:
Question 2
Year of qualification: a) 1997 � b) 1998 � c) 1999 �
32 responded.
28.13% of the sample qualified in 1997, 34.38% qualified in 1998 and 37.50% qualified in 1999.
Year of qualification
1997
1998
1999
Year No.s Percent
1997 9 28.13
1998 11 34.38
1999 12 37.5
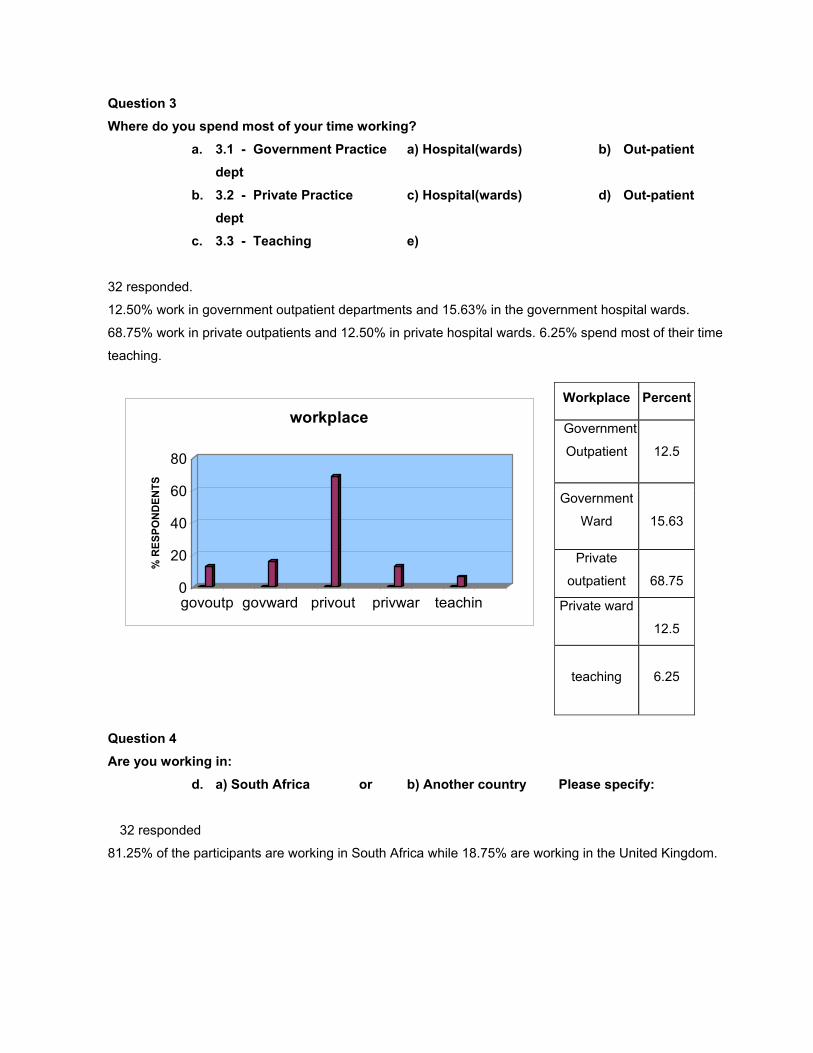
Question 3 Where do you spend most of your time working?
a. 3.1 - Government Practice a) Hospital(wards) � b) Out-patient dept �
b. 3.2 - Private Practice c) Hospital(wards) � d) Out-patient dept �
c. 3.3 - Teaching e) �
32 responded.
12.50% work in government outpatient departments and 15.63% in the government hospital wards.
68.75% work in private outpatients and 12.50% in private hospital wards. 6.25% spend most of their time
teaching.
Workplace Percent
Government
Outpatient
12.5
Government
Ward
15.63
Private
outpatient
68.75
Private ward
12.5
teaching
6.25
0
20
40
60
80
% R
ESPO
ND
ENTS
govoutp govward privout privwar teachin
workplace
Question 4 Are you working in:
d. a) South Africa � or b) Another country � Please specify:
32 responded
81.25% of the participants are working in South Africa while 18.75% are working in the United Kingdom.
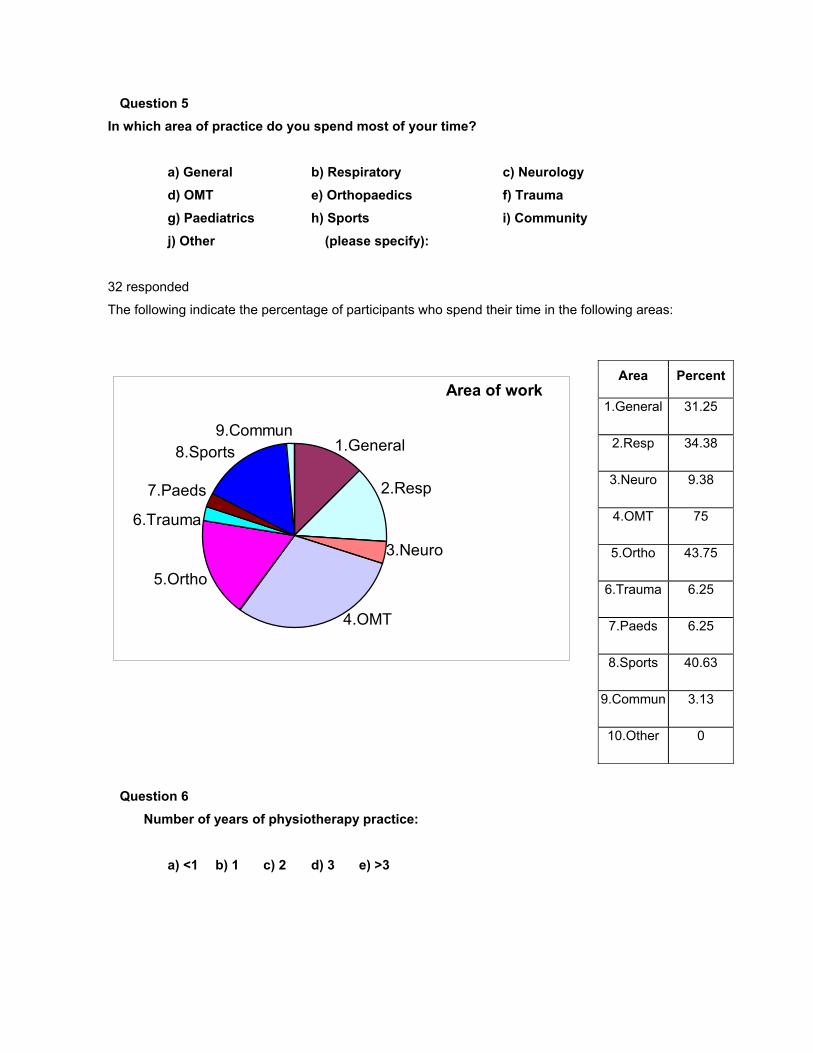
Question 5 In which area of practice do you spend most of your time?
a) General � b) Respiratory � c) Neurology � d) OMT � e) Orthopaedics � f) Trauma � g) Paediatrics � h) Sports � i) Community � j) Other � (please specify):
32 responded
The following indicate the percentage of participants who spend their time in the following areas:
Area Percent
1.General 31.25
2.Resp 34.38
3.Neuro 9.38
4.OMT 75
5.Ortho 43.75
6.Trauma 6.25
7.Paeds 6.25
8.Sports 40.63
9.Commun 3.13
10.Other 0
Area of work
8.Sports
5.Ortho
4.OMT
3.Neuro
2.Resp
1.General9.Commun
7.Paeds
6.Trauma
Question 6 Number of years of physiotherapy practice:
a) <1 � b) 1 � c) 2 � d) 3 � e) >3 �
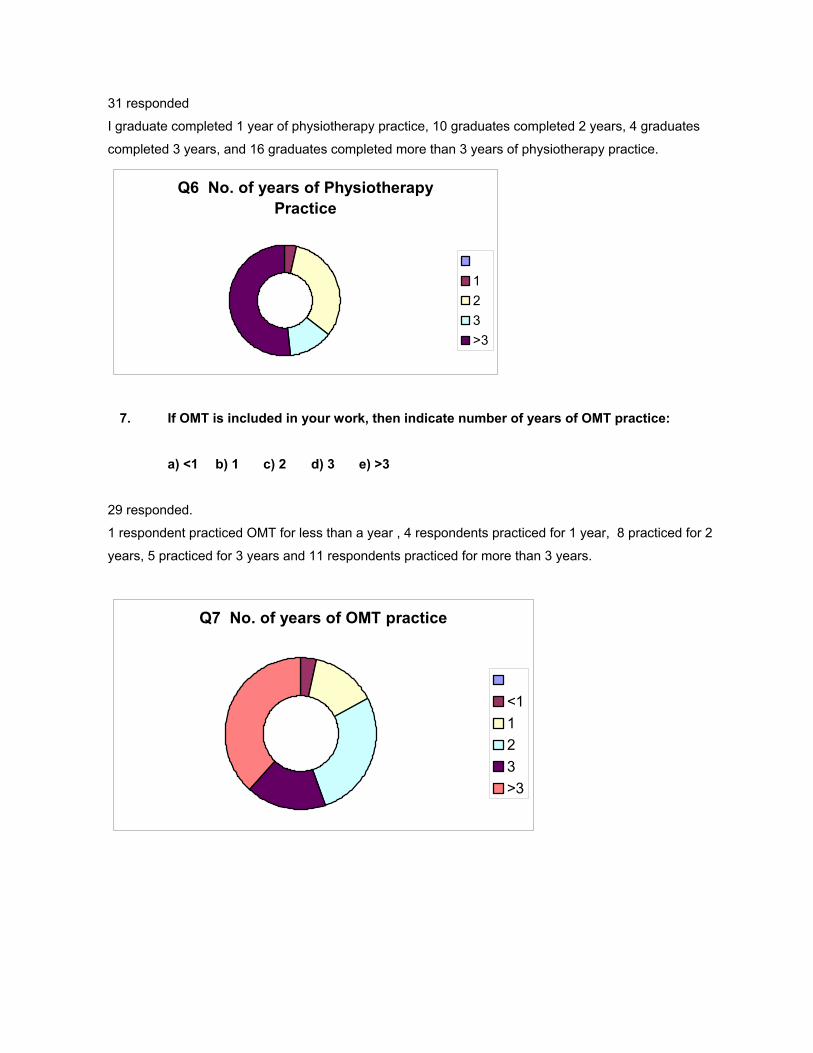
31 responded
I graduate completed 1 year of physiotherapy practice, 10 graduates completed 2 years, 4 graduates
completed 3 years, and 16 graduates completed more than 3 years of physiotherapy practice.
Q6 No. of years of Physiotherapy Practice
123>3
7. If OMT is included in your work, then indicate number of years of OMT practice:
a) <1 � b) 1 � c) 2 � d) 3 � e) >3 �
29 responded.
1 respondent practiced OMT for less than a year , 4 respondents practiced for 1 year, 8 practiced for 2
years, 5 practiced for 3 years and 11 respondents practiced for more than 3 years.
Q7 No. of years of OMT practice
<1123>3
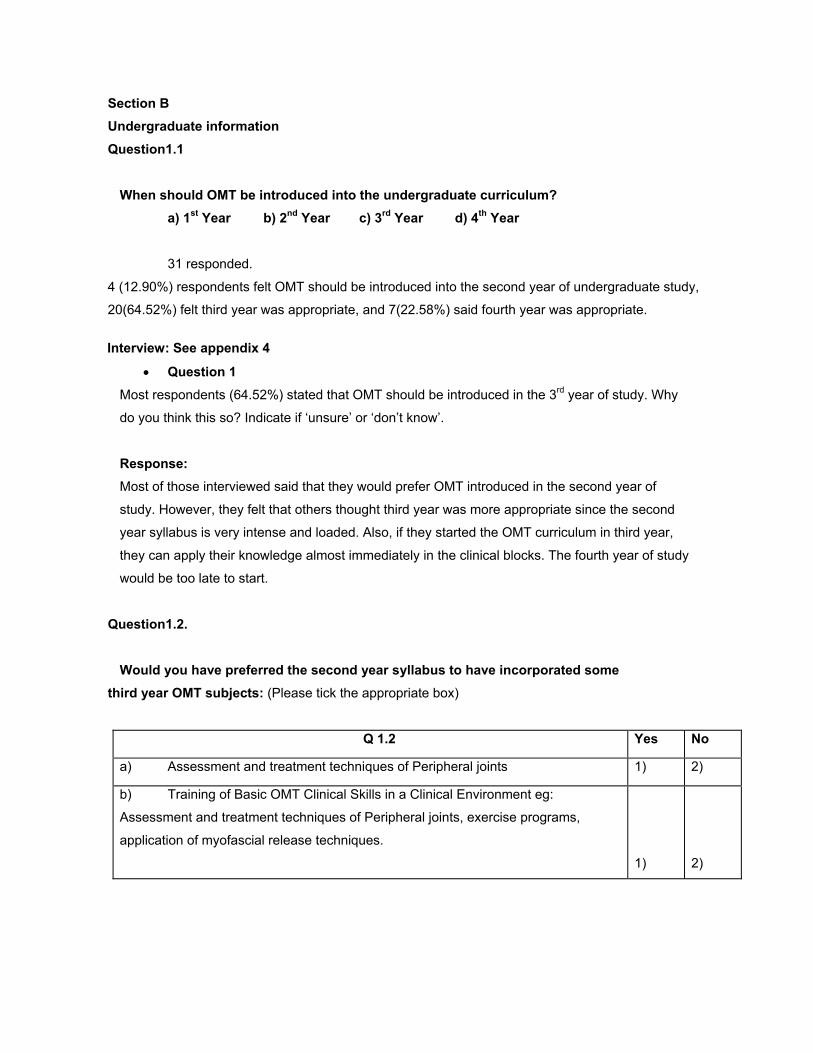
Section B Undergraduate information Question1.1
When should OMT be introduced into the undergraduate curriculum? a) 1st Year � b) 2nd Year � c) 3rd Year � d) 4th Year �
31 responded.
4 (12.90%) respondents felt OMT should be introduced into the second year of undergraduate study,
20(64.52%) felt third year was appropriate, and 7(22.58%) said fourth year was appropriate.
Interview: See appendix 4
• Question 1 Most respondents (64.52%) stated that OMT should be introduced in the 3rd year of study. Why
do you think this so? Indicate if ‘unsure’ or ‘don’t know’.
Response: Most of those interviewed said that they would prefer OMT introduced in the second year of
study. However, they felt that others thought third year was more appropriate since the second
year syllabus is very intense and loaded. Also, if they started the OMT curriculum in third year,
they can apply their knowledge almost immediately in the clinical blocks. The fourth year of study
would be too late to start.
Question1.2.
Would you have preferred the second year syllabus to have incorporated some third year OMT subjects: (Please tick the appropriate box)
Q 1.2 Yes No
a) Assessment and treatment techniques of Peripheral joints 1) 2)
b) Training of Basic OMT Clinical Skills in a Clinical Environment eg:
Assessment and treatment techniques of Peripheral joints, exercise programs,
application of myofascial release techniques.
1)
2)
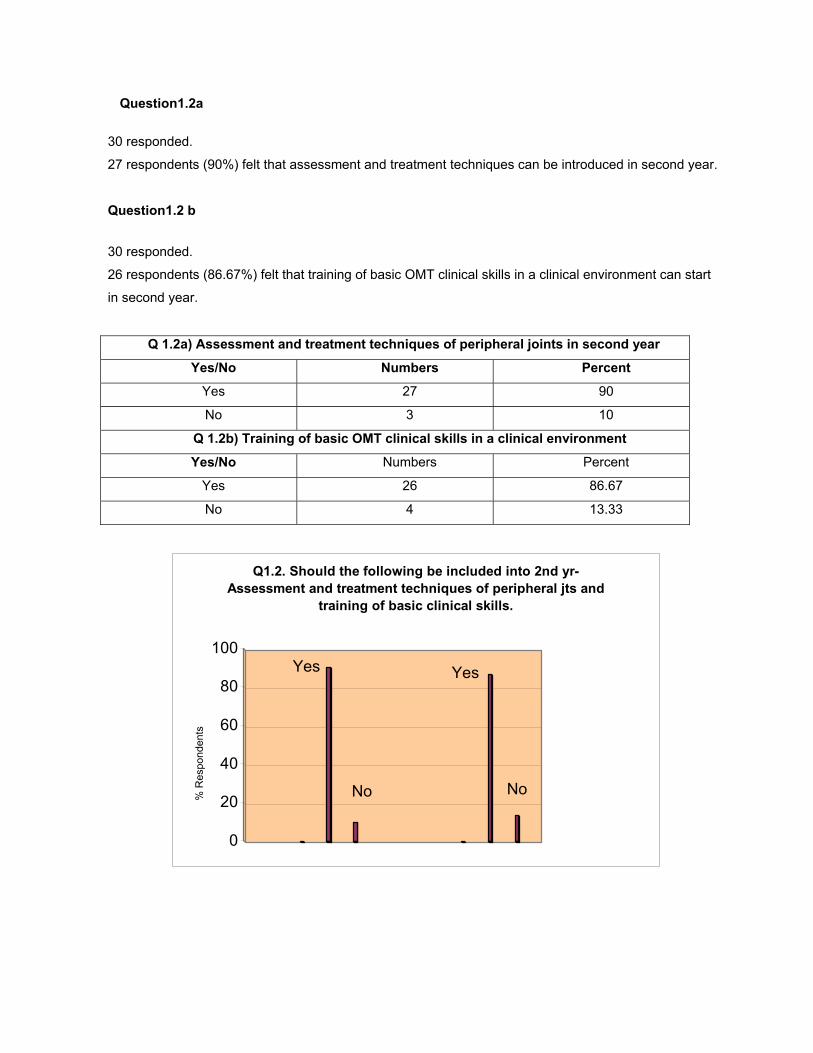
Question1.2a
30 responded.
27 respondents (90%) felt that assessment and treatment techniques can be introduced in second year.
Question1.2 b
30 responded.
26 respondents (86.67%) felt that training of basic OMT clinical skills in a clinical environment can start
in second year.
Q 1.2a) Assessment and treatment techniques of peripheral joints in second year
Yes/No Numbers Percent
Yes 27 90
No 3 10
Q 1.2b) Training of basic OMT clinical skills in a clinical environment
Yes/No Numbers Percent
Yes 26 86.67
No 4 13.33
Yes
No
Yes
No
0
20
40
60
80
100
Q1.2. Should the following be included into 2nd yr-Assessment and treatment techniques of peripheral jts and
training of basic clinical skills.
% R
espo
nden
ts
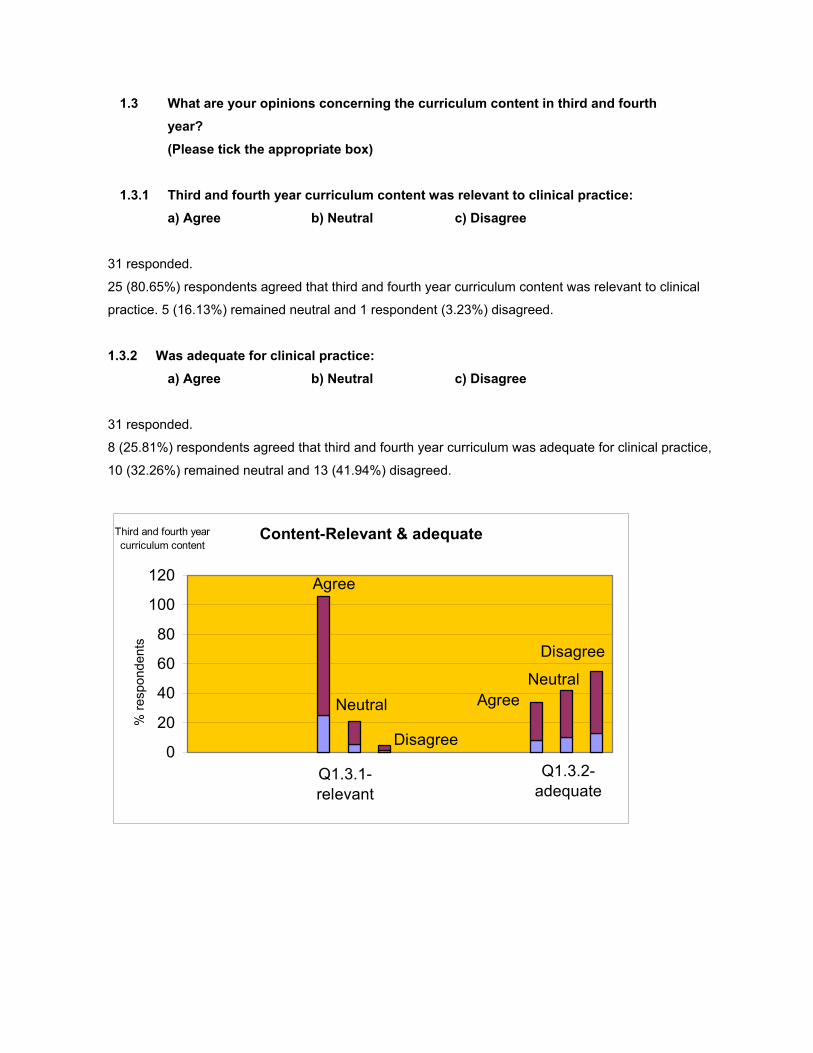
1.3 What are your opinions concerning the curriculum content in third and fourth year? (Please tick the appropriate box)
1.3.1 Third and fourth year curriculum content was relevant to clinical practice:
a) Agree � b) Neutral � c) Disagree �
31 responded.
25 (80.65%) respondents agreed that third and fourth year curriculum content was relevant to clinical
practice. 5 (16.13%) remained neutral and 1 respondent (3.23%) disagreed.
1.3.2 Was adequate for clinical practice:
a) Agree � b) Neutral � c) Disagree �
31 responded.
8 (25.81%) respondents agreed that third and fourth year curriculum was adequate for clinical practice,
10 (32.26%) remained neutral and 13 (41.94%) disagreed.
Content-Relevant & adequateThird and fourth year curriculum content
Q1.3.2-adequate
Disagree
Neutral
Agree
Q1.3.1-relevant
Disagree
AgreeNeutral
0
20
40
60
80
100
120
% re
spon
dent
s
Interview: See appendix 4
• Question 2 (regarding Section B question 1.3.1 and 1.3.2 from previous
questionnaire) When asked about 3rd and 4th yr curriculum content, most (80.65%) agreed that the content was
relevant to clinical practice but 42% stated that the content was inadequate. Why do you think the
3rd and 4th year curriculum content was inadequate?
Response: The interview revealed that the respondents would have liked the concepts taught to be applied a
lot more to the clinical situation. They would also liked to have spent more time in the clinical
blocks applying what they have learnt. They wanted to be informed that other concepts beside
Maitland are used and would have also liked more information on specific topics e.g. the
sacroiliac joint.
Question 1.4
In your third and fourth year you were taught the Maitland concept of assessment
and treatment techniques for peripheral and spinal joints. Have you found this concept: (please tick the appropriate box in 1.4.1.1 and 1.4.1.2)
1.4.1.1 a) Relevant � b) Sometimes relevant � c) Irrelevant � to clinical
practice
1.4.1.2 a) Adequate � b) Sometimes adequate � c) Inadequate � for clinical practice
30 responded
14 (46.67%) respondents stated that they found the Maitland concept relevant and 6 (20.69%) found it
adequate for clinical practice. 16 (53.33%) found it sometimes relevant, and 20 (68.97%) found it
sometimes adequate for clinical practice.
3 (10.34%) respondents found it inadequate.
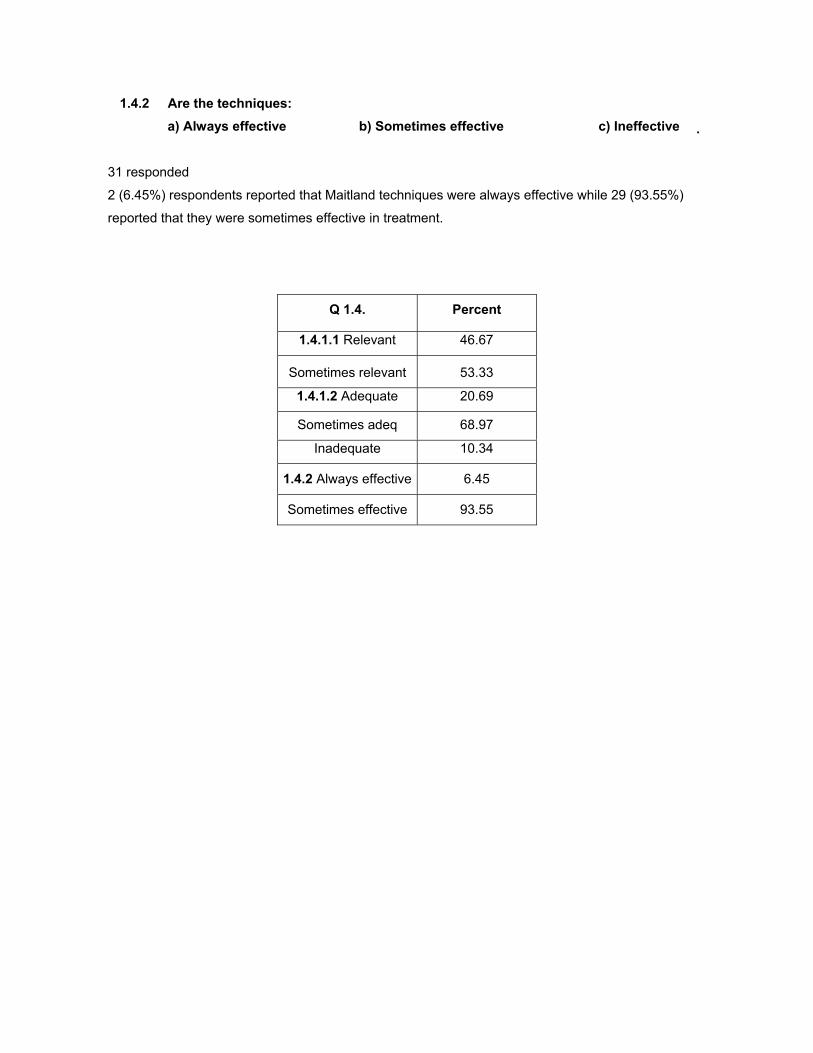
1.4.2 Are the techniques: a) Always effective � b) Sometimes effective � c) Ineffective �
31 responded
2 (6.45%) respondents reported that Maitland techniques were always effective while 29 (93.55%)
reported that they were sometimes effective in treatment.
Q 1.4. Percent
1.4.1.1 Relevant 46.67
Sometimes relevant 53.33
1.4.1.2 Adequate 20.69
Sometimes adeq 68.97
Inadequate 10.34
1.4.2 Always effective 6.45
Sometimes effective 93.55
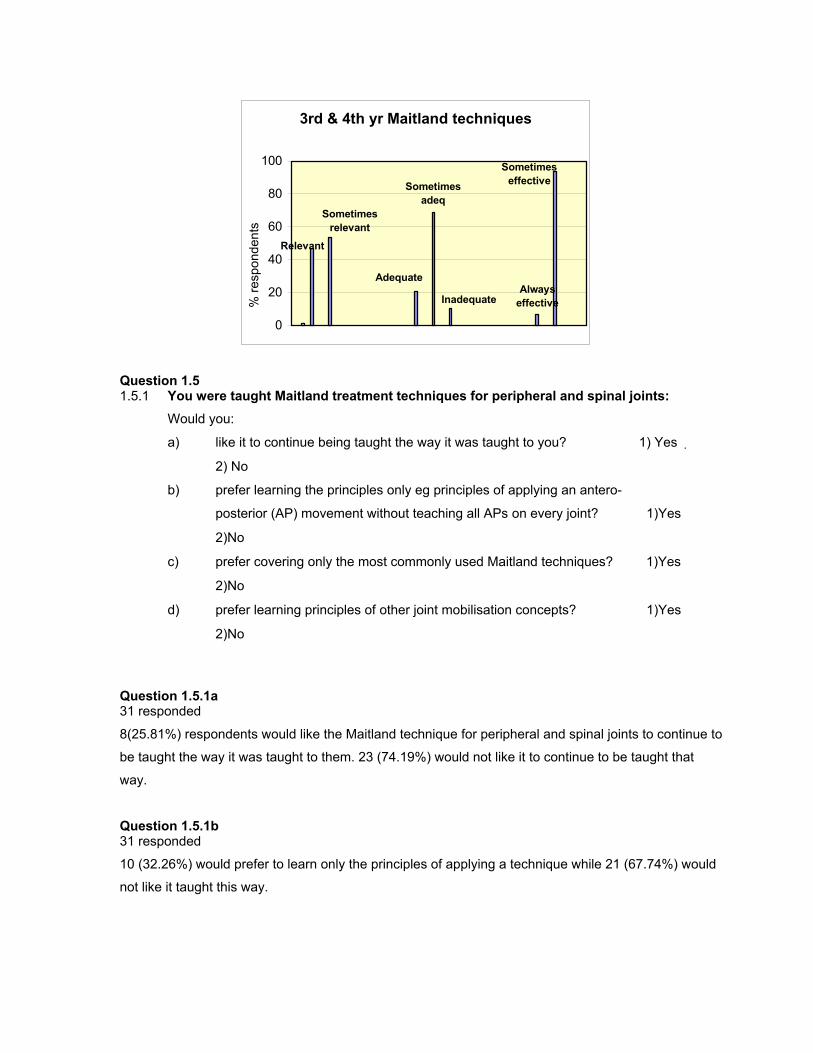
3rd & 4th yr Maitland techniques
Inadequate
Adequate
Relevant
Sometimes relevant
Sometimes adeq
Sometimes effective
Always effective
0
20
40
60
80
100
% re
spon
dent
s
Question 1.5 1.5.1 You were taught Maitland treatment techniques for peripheral and spinal joints:
Would you:
a) like it to continue being taught the way it was taught to you? 1) Yes
2) No �
b) prefer learning the principles only eg principles of applying an antero-
posterior (AP) movement without teaching all APs on every joint? 1)Yes �
2)No �
c) prefer covering only the most commonly used Maitland techniques? 1)Yes �
2)No �
d) prefer learning principles of other joint mobilisation concepts? 1)Yes �
2)No �
Question 1.5.1a 31 responded
8(25.81%) respondents would like the Maitland technique for peripheral and spinal joints to continue to
be taught the way it was taught to them. 23 (74.19%) would not like it to continue to be taught that
way.
Question 1.5.1b 31 responded
10 (32.26%) would prefer to learn only the principles of applying a technique while 21 (67.74%) would
not like it taught this way.
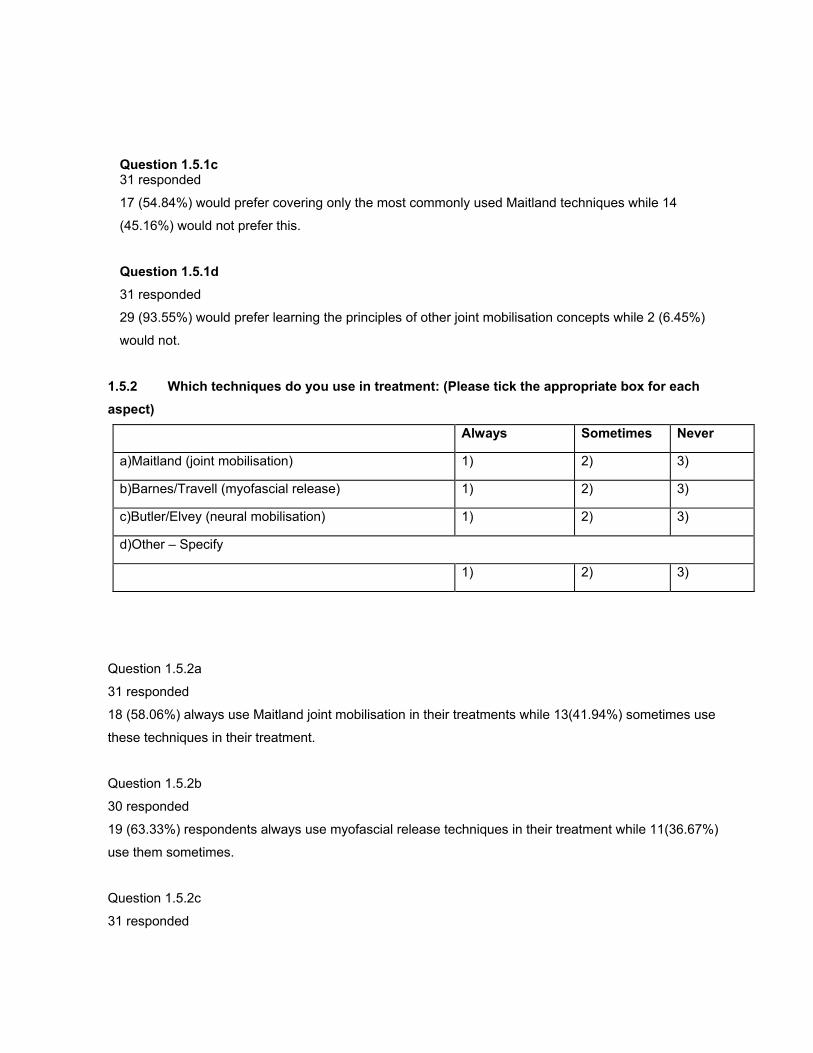
Question 1.5.1c 31 responded
17 (54.84%) would prefer covering only the most commonly used Maitland techniques while 14
(45.16%) would not prefer this.
Question 1.5.1d 31 responded
29 (93.55%) would prefer learning the principles of other joint mobilisation concepts while 2 (6.45%)
would not.
1.5.2 Which techniques do you use in treatment: (Please tick the appropriate box for each aspect)
Always Sometimes Never
a)Maitland (joint mobilisation) 1) 2) 3)
b)Barnes/Travell (myofascial release) 1) 2) 3)
c)Butler/Elvey (neural mobilisation) 1) 2) 3)
d)Other – Specify
1) 2) 3)
Question 1.5.2a
31 responded
18 (58.06%) always use Maitland joint mobilisation in their treatments while 13(41.94%) sometimes use
these techniques in their treatment.
Question 1.5.2b
30 responded
19 (63.33%) respondents always use myofascial release techniques in their treatment while 11(36.67%)
use them sometimes.
Question 1.5.2c
31 responded
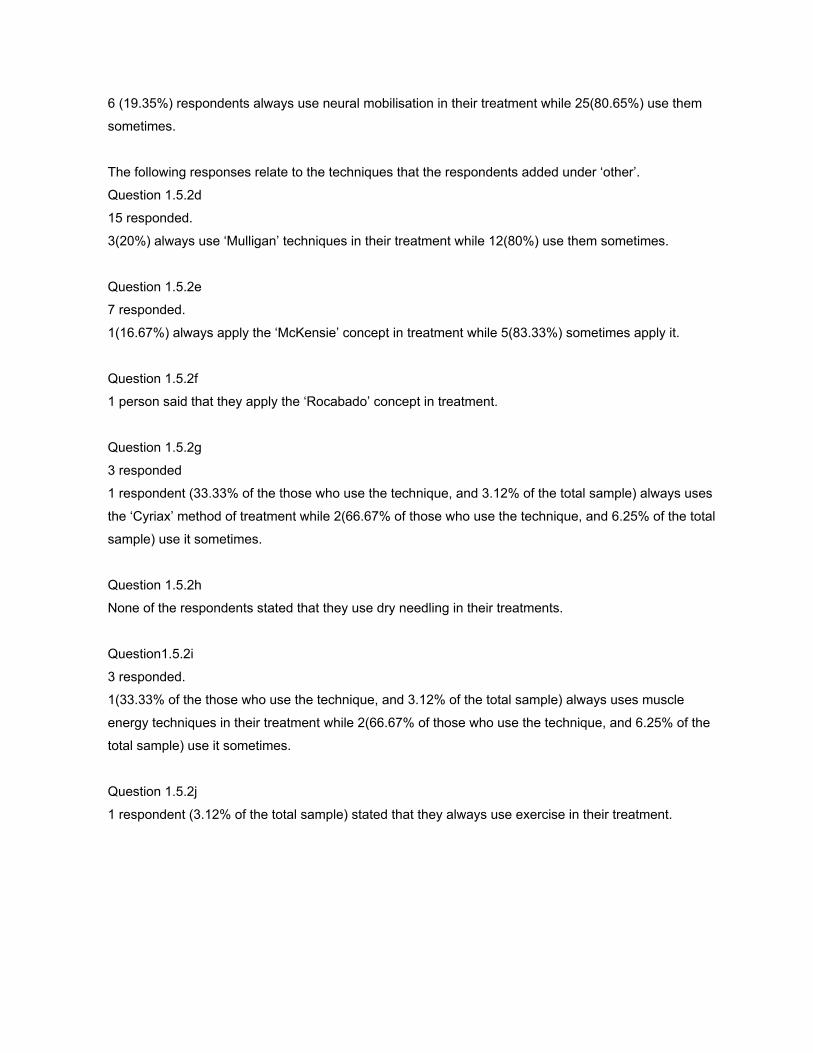
6 (19.35%) respondents always use neural mobilisation in their treatment while 25(80.65%) use them
sometimes.
The following responses relate to the techniques that the respondents added under ‘other’.
Question 1.5.2d
15 responded.
3(20%) always use ‘Mulligan’ techniques in their treatment while 12(80%) use them sometimes.
Question 1.5.2e
7 responded.
1(16.67%) always apply the ‘McKensie’ concept in treatment while 5(83.33%) sometimes apply it.
Question 1.5.2f
1 person said that they apply the ‘Rocabado’ concept in treatment.
Question 1.5.2g
3 responded
1 respondent (33.33% of the those who use the technique, and 3.12% of the total sample) always uses
the ‘Cyriax’ method of treatment while 2(66.67% of those who use the technique, and 6.25% of the total
sample) use it sometimes.
Question 1.5.2h
None of the respondents stated that they use dry needling in their treatments.
Question1.5.2i
3 responded.
1(33.33% of the those who use the technique, and 3.12% of the total sample) always uses muscle
energy techniques in their treatment while 2(66.67% of those who use the technique, and 6.25% of the
total sample) use it sometimes.
Question 1.5.2j
1 respondent (3.12% of the total sample) stated that they always use exercise in their treatment.
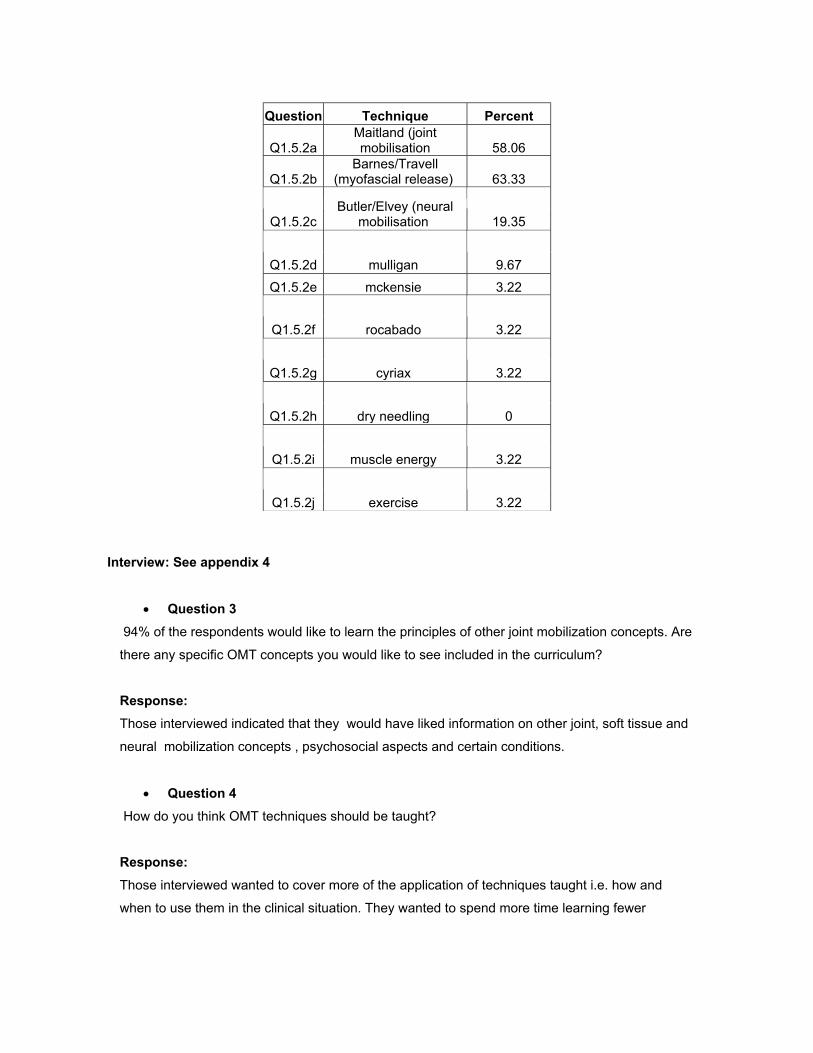
Question Technique Percent
Q1.5.2a Maitland (joint mobilisation 58.06
Q1.5.2b Barnes/Travell
(myofascial release) 63.33
Q1.5.2c Butler/Elvey (neural
mobilisation 19.35
Q1.5.2d mulligan 9.67
Q1.5.2e mckensie 3.22
Q1.5.2f rocabado 3.22
Q1.5.2g cyriax 3.22
Q1.5.2h dry needling 0
Q1.5.2i muscle energy 3.22
Q1.5.2j exercise 3.22
Interview: See appendix 4
• Question 3 94% of the respondents would like to learn the principles of other joint mobilization concepts. Are
there any specific OMT concepts you would like to see included in the curriculum?
Response: Those interviewed indicated that they would have liked information on other joint, soft tissue and
neural mobilization concepts , psychosocial aspects and certain conditions.
• Question 4
How do you think OMT techniques should be taught?
Response: Those interviewed wanted to cover more of the application of techniques taught i.e. how and
when to use them in the clinical situation. They wanted to spend more time learning fewer
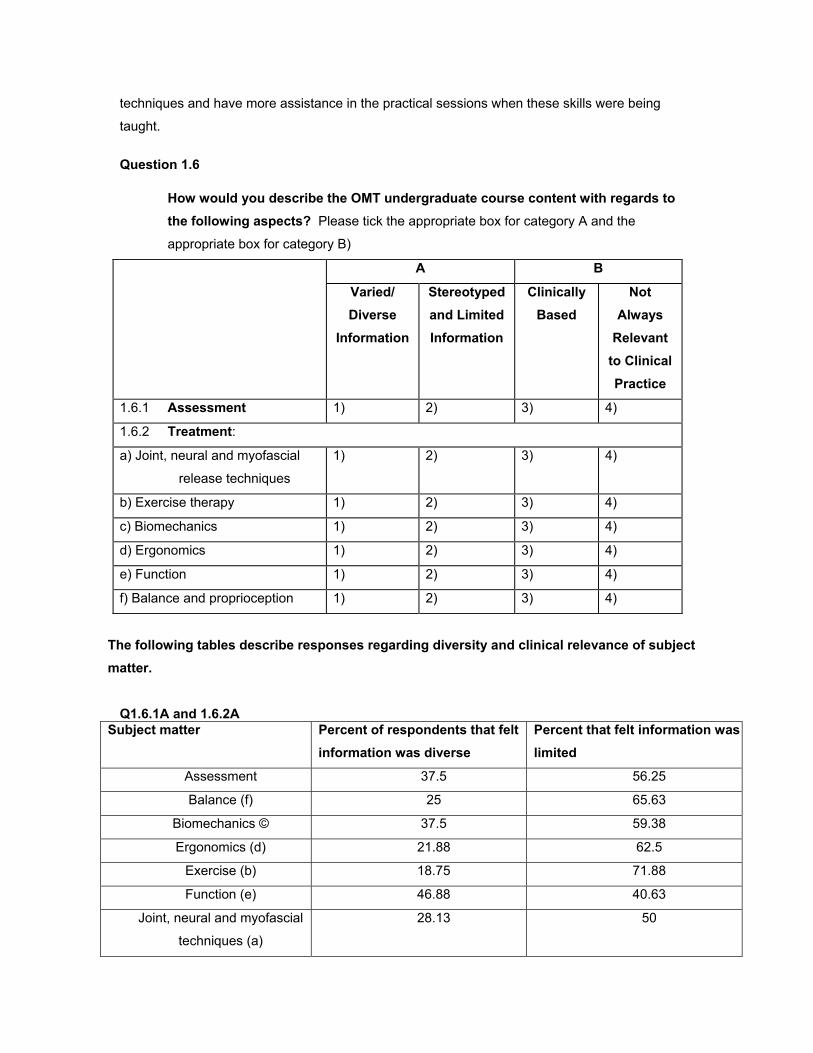
techniques and have more assistance in the practical sessions when these skills were being
taught.
Question 1.6 How would you describe the OMT undergraduate course content with regards to
the following aspects? Please tick the appropriate box for category A and the
appropriate box for category B)
A B
Varied/ Diverse
Information
Stereotyped and Limited Information
Clinically Based
Not Always
Relevant to Clinical Practice
1.6.1 Assessment 1) 2) 3) 4)
1.6.2 Treatment:
a) Joint, neural and myofascial
release techniques
1) 2) 3) 4)
b) Exercise therapy 1) 2) 3) 4)
c) Biomechanics 1) 2) 3) 4)
d) Ergonomics 1) 2) 3) 4)
e) Function 1) 2) 3) 4)
f) Balance and proprioception 1) 2) 3) 4)
The following tables describe responses regarding diversity and clinical relevance of subject matter.
Q1.6.1A and 1.6.2A Subject matter Percent of respondents that felt
information was diverse Percent that felt information was limited
Assessment 37.5 56.25
Balance (f) 25 65.63
Biomechanics © 37.5 59.38
Ergonomics (d) 21.88 62.5
Exercise (b) 18.75 71.88
Function (e) 46.88 40.63
Joint, neural and myofascial
techniques (a)
28.13 50
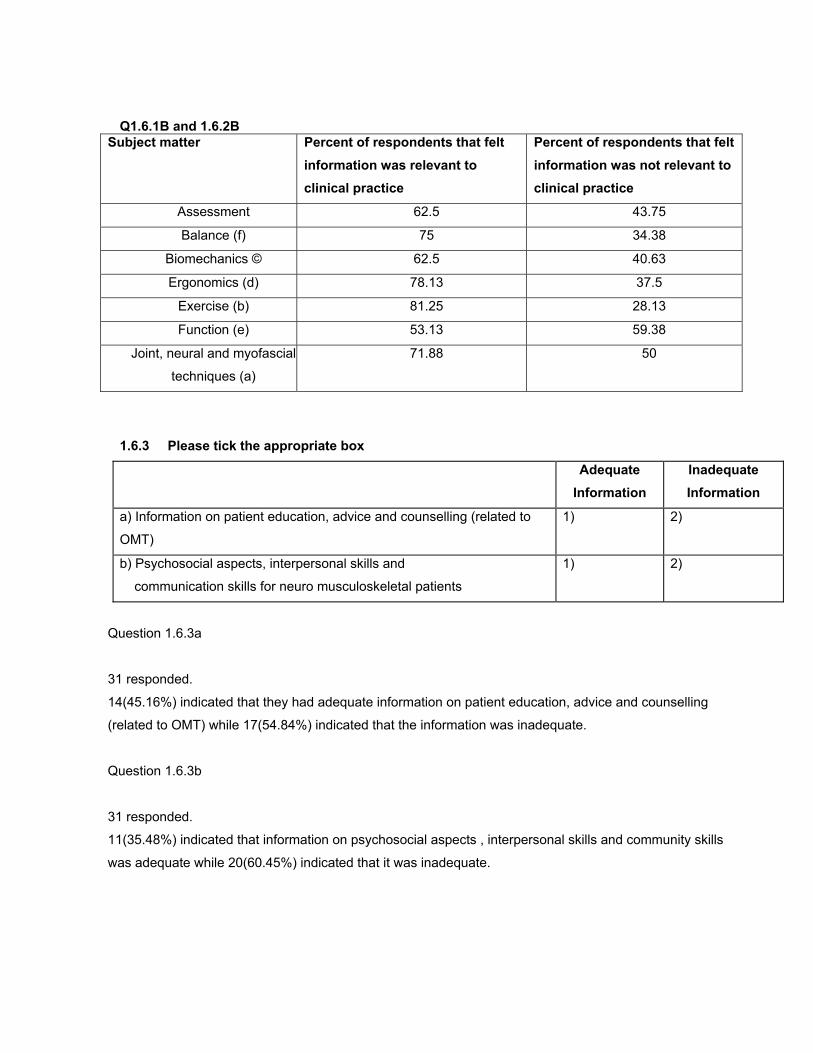
Q1.6.1B and 1.6.2B Subject matter Percent of respondents that felt
information was relevant to clinical practice
Percent of respondents that felt information was not relevant to clinical practice
Assessment 62.5 43.75
Balance (f) 75 34.38
Biomechanics © 62.5 40.63
Ergonomics (d) 78.13 37.5
Exercise (b) 81.25 28.13
Function (e) 53.13 59.38
Joint, neural and myofascial
techniques (a)
71.88 50
1.6.3 Please tick the appropriate box
Adequate Information
Inadequate Information
a) Information on patient education, advice and counselling (related to
OMT)
1) 2)
b) Psychosocial aspects, interpersonal skills and
communication skills for neuro musculoskeletal patients
1) 2)
Question 1.6.3a
31 responded.
14(45.16%) indicated that they had adequate information on patient education, advice and counselling
(related to OMT) while 17(54.84%) indicated that the information was inadequate.
Question 1.6.3b
31 responded.
11(35.48%) indicated that information on psychosocial aspects , interpersonal skills and community skills
was adequate while 20(60.45%) indicated that it was inadequate.
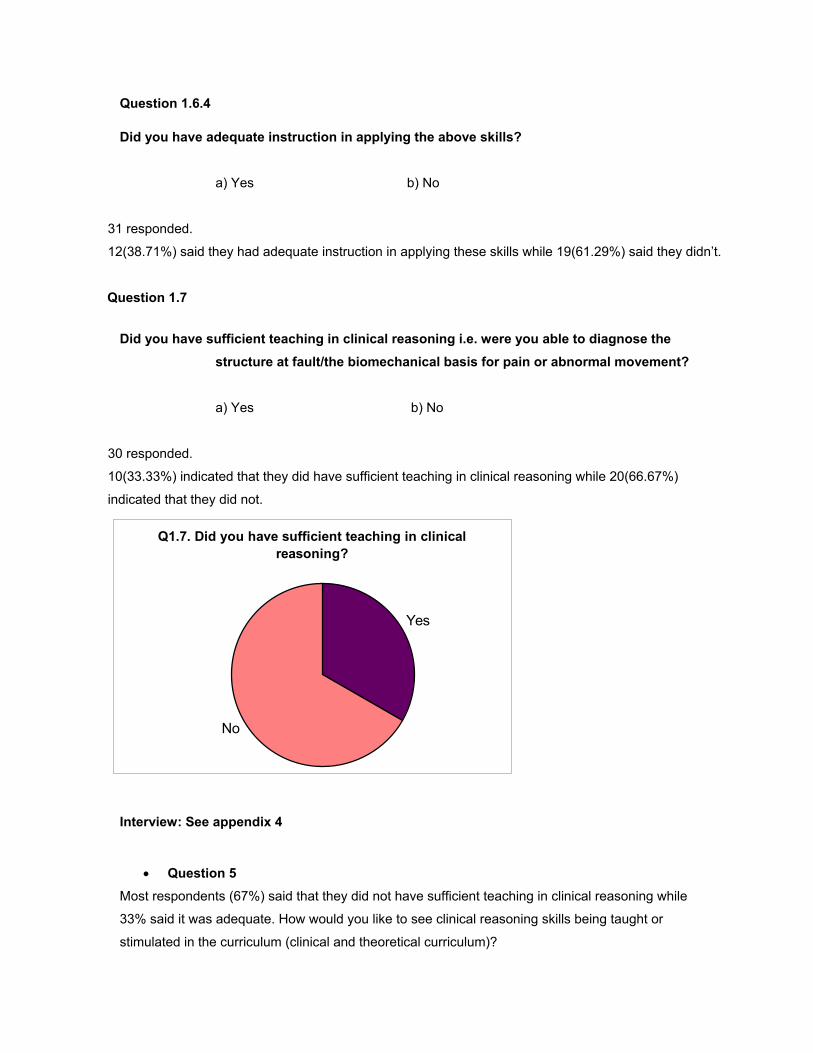
Question 1.6.4 Did you have adequate instruction in applying the above skills?
a) Yes � b) No �
31 responded.
12(38.71%) said they had adequate instruction in applying these skills while 19(61.29%) said they didn’t.
Question 1.7
Did you have sufficient teaching in clinical reasoning i.e. were you able to diagnose the
structure at fault/the biomechanical basis for pain or abnormal movement?
a) Yes � b) No �
30 responded.
10(33.33%) indicated that they did have sufficient teaching in clinical reasoning while 20(66.67%)
indicated that they did not.
Q1.7. Did you have sufficient teaching in clinical reasoning?
Yes
No
Interview: See appendix 4
• Question 5
Most respondents (67%) said that they did not have sufficient teaching in clinical reasoning while
33% said it was adequate. How would you like to see clinical reasoning skills being taught or
stimulated in the curriculum (clinical and theoretical curriculum)?
Response: Clinical reasoning may be facilitated by problem solving exercises and bedside teaching.
Feedback from the lecturers and supervisors are also useful.
Question 1.8 Your course content together with readings helped you to adequately manage:
a) all patients encountered � b) most patients encountered �
c) some patients encountered � d) none of the patients encountered �
31 responded.
22(70.97%) felt that the course content and readings helped them to adequately manage their patients
while 9(29.03%) felt that it helped them manage some patients.
Question 1.9
1.9.1 In your opinion, were there any important aspects: lacking in your OMT training?
a) Yes � b) No �
30 responded.
According to 24 (80%) respondents, there were important aspects lacking in the curriculum. 6(20%) did
not think so.
If yes, please specify:
Summary of responses: Application of the OMT concept and actual OMT techniques in the clinical setting.
Explanation of how the techniques work.
More biomechanics and functional anatomy.
Information on the sacroiliac joint and temperomandibular joint.
1.9.2 In your opinion, were there any important aspects: you think should be included into the OMT curriculum?
a) Yes � b) No �
31 responded.
29(93.55%) said that more information should be included into the OMT curriculum while 2(6.45%) did
not feel this way.
If yes, please specify: Summary of responses: More clinical teaching and application of OMT techniques
Posture and ergonomics
Information on psychosocial aspects and counselling.
Other OMT concepts and alternative therapies.
1.9.3. In your opinion, were there any important aspects: you think should be excluded from the OMT curriculum?
a) Yes � b) No �
31 responded.
9(29.03%) said that certain aspects should be excluded from the OMT curriculum while
22(70.97%) did not feel this way.
If yes, please specify Summary of responses: Certain mobilising techniques
Repetition of basic principles.
Question 1.10
Did you find that the prescribed curriculum allowed for innovation and your own creative ideas?
a) Often � b) Seldom � c) Never �
If ‘seldom’, or ‘never’ was ticked, substantiate:…………………………………………………………………………
31 responded.
10(32.26%) found that the prescribed curriculum allowed for innovation and their own creative ideas.
13(41.94%) seldom found this. 8(25.81%) never found this.
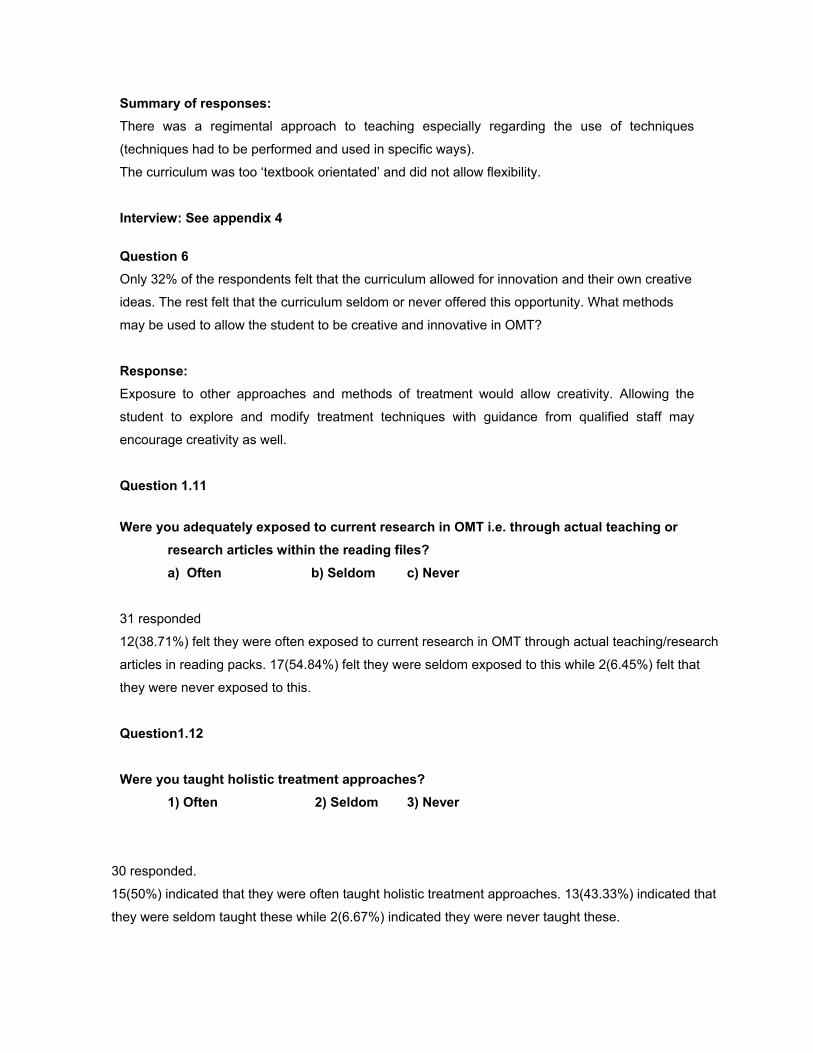
Summary of responses: There was a regimental approach to teaching especially regarding the use of techniques
(techniques had to be performed and used in specific ways).
The curriculum was too ‘textbook orientated’ and did not allow flexibility.
Interview: See appendix 4
Question 6 Only 32% of the respondents felt that the curriculum allowed for innovation and their own creative
ideas. The rest felt that the curriculum seldom or never offered this opportunity. What methods
may be used to allow the student to be creative and innovative in OMT?
Response: Exposure to other approaches and methods of treatment would allow creativity. Allowing the
student to explore and modify treatment techniques with guidance from qualified staff may
encourage creativity as well.
Question 1.11
Were you adequately exposed to current research in OMT i.e. through actual teaching or
research articles within the reading files?
a) Often � b) Seldom � c) Never �
31 responded
12(38.71%) felt they were often exposed to current research in OMT through actual teaching/research
articles in reading packs. 17(54.84%) felt they were seldom exposed to this while 2(6.45%) felt that
they were never exposed to this.
Question1.12 Were you taught holistic treatment approaches?
1) Often � 2) Seldom � 3) Never �
30 responded.
15(50%) indicated that they were often taught holistic treatment approaches. 13(43.33%) indicated that
they were seldom taught these while 2(6.67%) indicated they were never taught these.
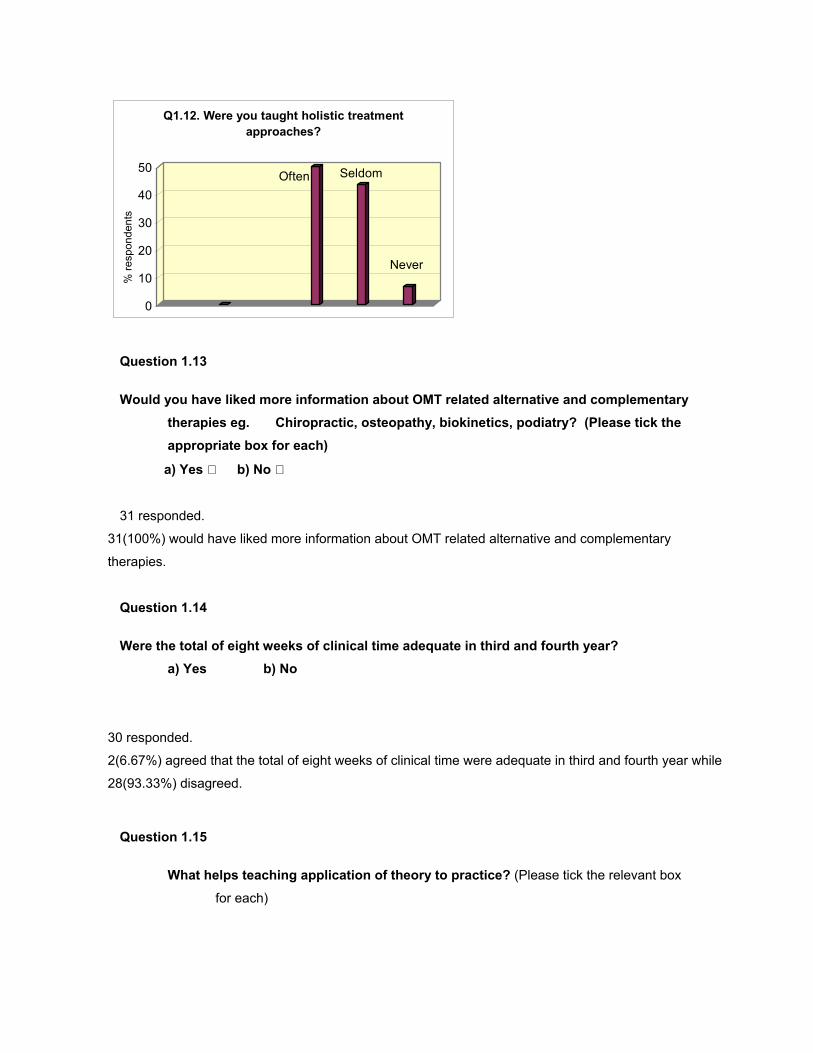
Often Seldom
Never
0
10
20
30
40
50
Q1.12. Were you taught holistic treatment approaches?
% re
spon
dent
s
Question 1.13
Would you have liked more information about OMT related alternative and complementary therapies eg. Chiropractic, osteopathy, biokinetics, podiatry? (Please tick the appropriate box for each)
a) Yes b) No
31 responded.
31(100%) would have liked more information about OMT related alternative and complementary
therapies.
Question 1.14
Were the total of eight weeks of clinical time adequate in third and fourth year?
a) Yes � b) No �
30 responded.
2(6.67%) agreed that the total of eight weeks of clinical time were adequate in third and fourth year while
28(93.33%) disagreed.
Question 1.15
What helps teaching application of theory to practice? (Please tick the relevant box
for each)
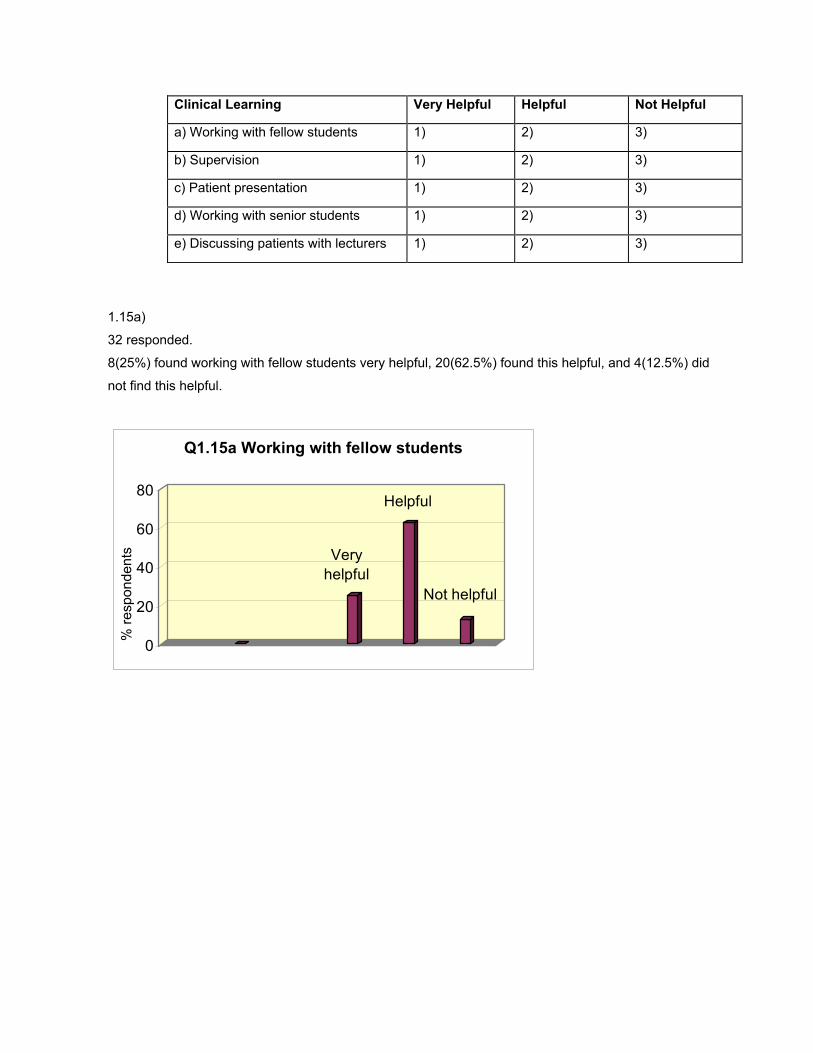
Clinical Learning Very Helpful Helpful Not Helpful
a) Working with fellow students 1) 2) 3)
b) Supervision 1) 2) 3)
c) Patient presentation 1) 2) 3)
d) Working with senior students 1) 2) 3)
e) Discussing patients with lecturers 1) 2) 3)
1.15a)
32 responded.
8(25%) found working with fellow students very helpful, 20(62.5%) found this helpful, and 4(12.5%) did
not find this helpful.
Very helpful
Helpful
Not helpful
0
20
40
60
80
Q1.15a Working with fellow students
% re
spon
dent
s
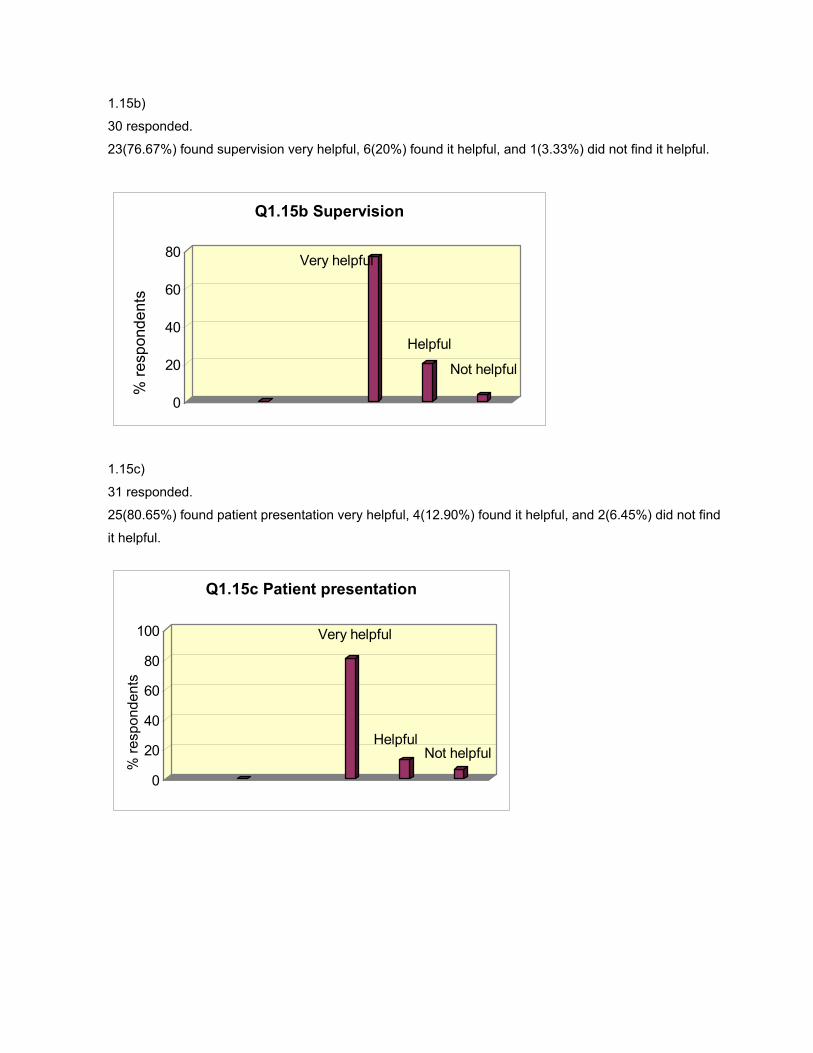
1.15b)
30 responded.
23(76.67%) found supervision very helpful, 6(20%) found it helpful, and 1(3.33%) did not find it helpful.
Very helpful
Helpful
Not helpful
0
20
40
60
80
Q1.15b Supervision
% re
spon
dent
s
1.15c)
31 responded.
25(80.65%) found patient presentation very helpful, 4(12.90%) found it helpful, and 2(6.45%) did not find
it helpful.
Very helpful
HelpfulNot helpful
0
20
40
60
80
100
Q1.15c Patient presentation
% re
spon
dent
s
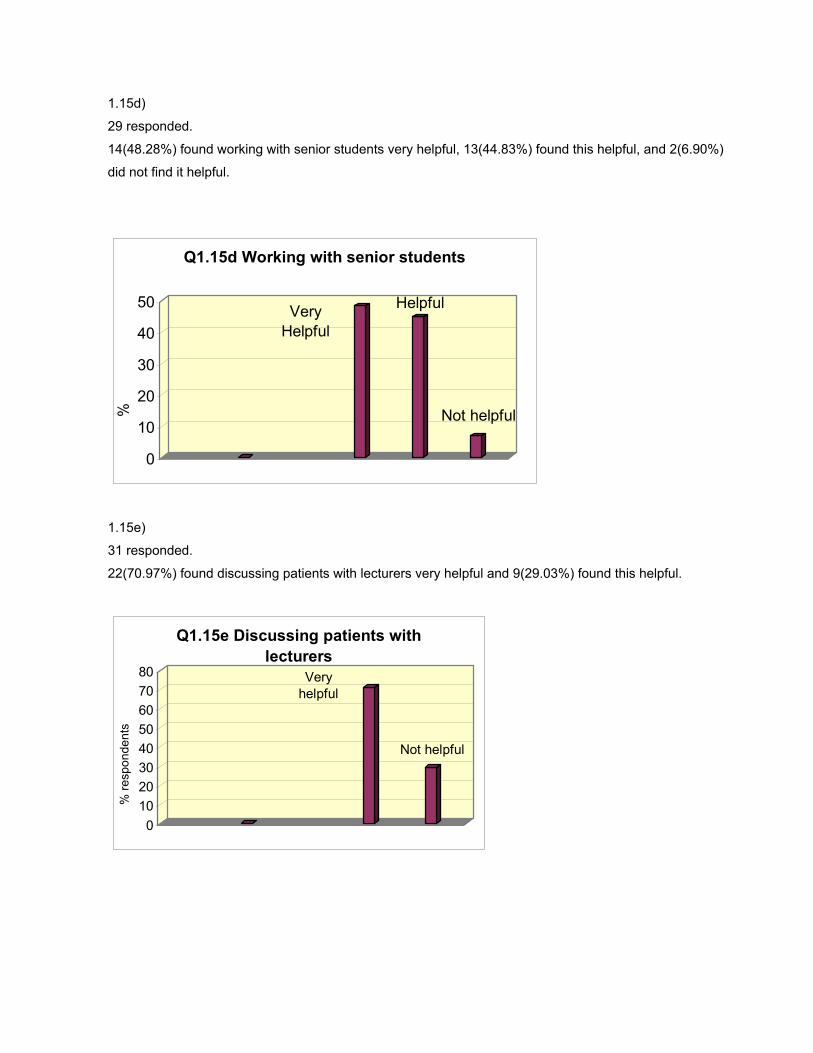
1.15d)
29 responded.
14(48.28%) found working with senior students very helpful, 13(44.83%) found this helpful, and 2(6.90%)
did not find it helpful.
Very Helpful
Helpful
Not helpful
0
10
20
30
40
50
Q1.15d Working with senior students
%
1.15e)
31 responded.
22(70.97%) found discussing patients with lecturers very helpful and 9(29.03%) found this helpful.
Very helpful
Not helpful
01020304050607080
Q1.15e Discussing patients with lecturers
% re
spon
dent
s
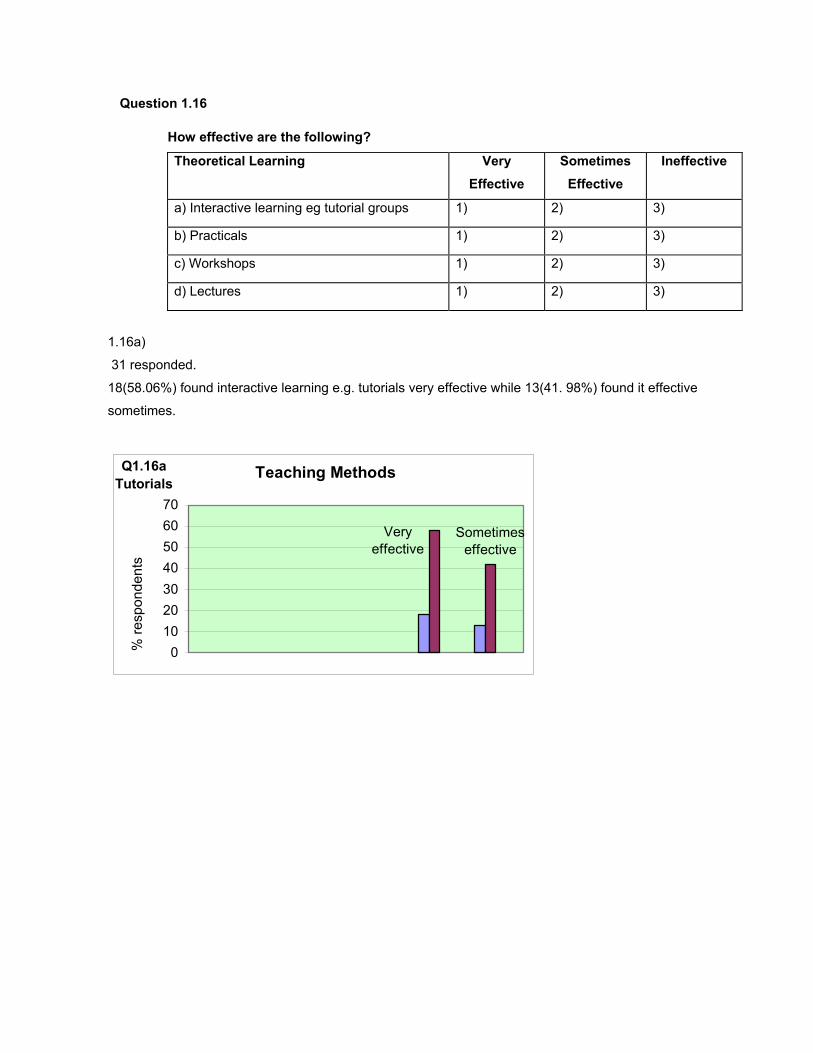
Question 1.16
How effective are the following?
Theoretical Learning Very Effective
Sometimes Effective
Ineffective
a) Interactive learning eg tutorial groups 1) 2) 3)
b) Practicals 1) 2) 3)
c) Workshops 1) 2) 3)
d) Lectures 1) 2) 3)
1.16a)
31 responded.
18(58.06%) found interactive learning e.g. tutorials very effective while 13(41. 98%) found it effective
sometimes.
Teaching Methods
Sometimes effective
Q1.16a Tutorials
Very effective
010203040506070
% re
spon
dent
s
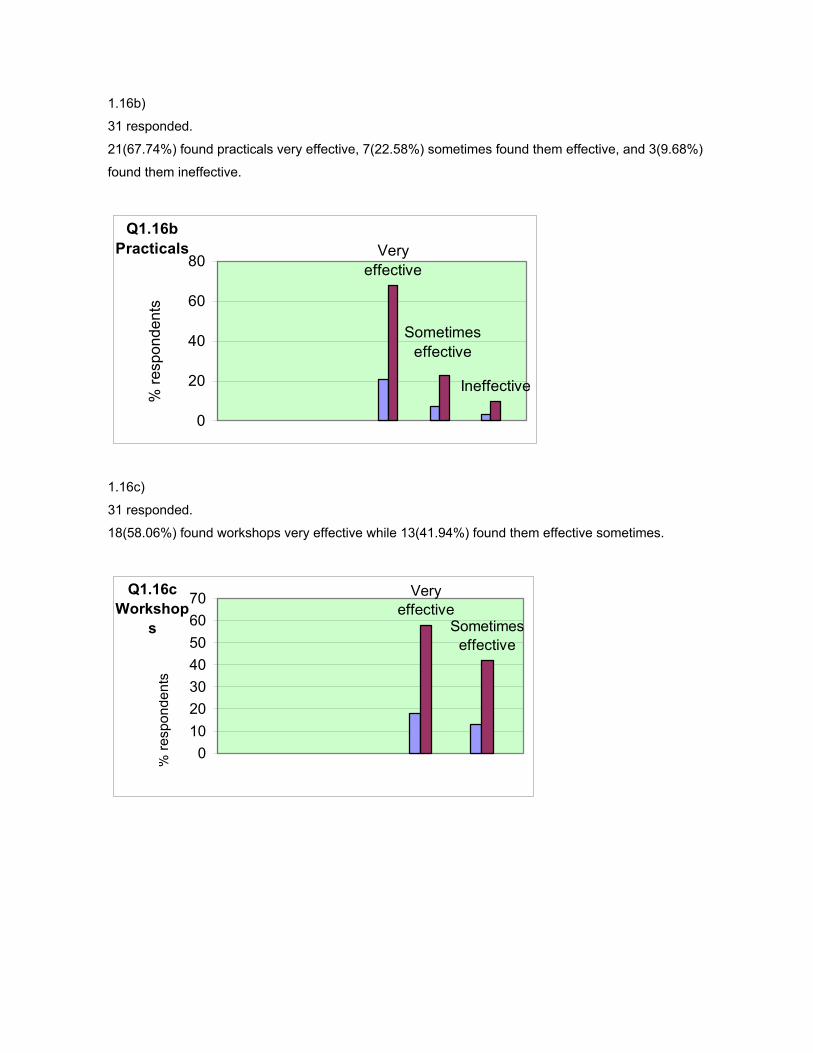
1.16b)
31 responded.
21(67.74%) found practicals very effective, 7(22.58%) sometimes found them effective, and 3(9.68%)
found them ineffective.
Very effective
Ineffective
Sometimes effective
Q1.16b Practicals
0
20
40
60
80
% re
spon
dent
s
1.16c)
31 responded.
18(58.06%) found workshops very effective while 13(41.94%) found them effective sometimes.
Very effective
Sometimes effective
Q1.16c Workshop
s
010203040506070
% re
spon
dent
s
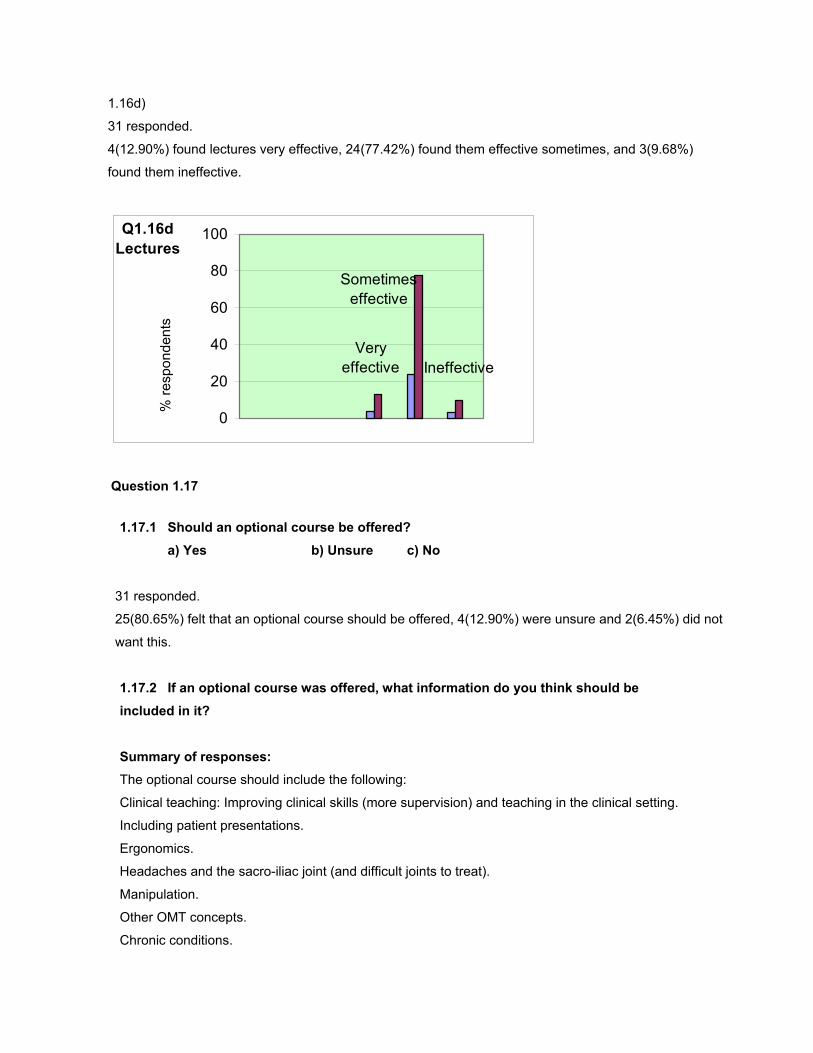
1.16d)
31 responded.
4(12.90%) found lectures very effective, 24(77.42%) found them effective sometimes, and 3(9.68%)
found them ineffective.
Very effective
Q1.16d Lectures
Ineffective
Sometimes effective
0
20
40
60
80
100
% re
spon
dent
s
Question 1.17
1.17.1 Should an optional course be offered?
a) Yes � b) Unsure � c) No �
31 responded.
25(80.65%) felt that an optional course should be offered, 4(12.90%) were unsure and 2(6.45%) did not
want this.
1.17.2 If an optional course was offered, what information do you think should be included in it? Summary of responses: The optional course should include the following:
Clinical teaching: Improving clinical skills (more supervision) and teaching in the clinical setting.
Including patient presentations.
Ergonomics.
Headaches and the sacro-iliac joint (and difficult joints to treat).
Manipulation.
Other OMT concepts.
Chronic conditions.
Exercise therapy.
Biomechanics and functional anatomy.
Exposure to OMT research.
Preventative therapy including exercise programmes and advice and education of patients.
Counselling and communication skills.
More sports physiotherapy
Question 1.18 Do you think that undergraduate student interaction with post-graduate program lecturers is beneficial:
a) Yes b) No
30 responded.
29(96.67%) thought that undergraduate student interaction with postgraduate programme lecturers is
beneficial while 1(3.33%) did not think so.
POST-GRADUATE
2.1 Please give information about OMT courses you have attended since you qualified.
Year in which course was done
Name of Course Duration of course e.g. weekend
2.2 Which courses listed above best supplemented your undergraduate knowledge
and why? Summary of responses for 2.1 and 2.2: OMT1
Alternative therapies.
Dry needling.
Post-surgical spines.
Courses on the neural and myofascial system and treatment of these.
Courses on specific joints/conditions e.g. sacroiliac joint, temperomandibular joint, lumbar spine
and headaches.

APPENDIX 6 ETHICAL CLEARANCE FORM

APPENDIX 7 THE CORE OMT CURRICULUM CONTENT
THE CORE OMT CURRICULUM CONTENT
Introduction to the OMT curriculum
Physiotherapists who use OMT are concerned with the prevention and treatment
of joints, soft tissue, and neural pain and dysfunction. This may be achieved
through various physical modalities including exercise, passive joint movement
(including mobilization and manipulation), traction, massage, myofascial release
techniques, neural mobilization, postural and functional rehabilitation and patient
education. These techniques and modalities have been considered as most
important and are commonly used when managing patients. The concepts and
techniques included in the curriculum will be discussed.
Manual physiotherapy concepts
Various therapists have developed different OMT concepts (Petty and Moore,
2001). Many therapists have been involved in expanding and evolving the
examination and treatment of joints, muscles and nervous tissue. Methods of
examination and treatment are continuing to be developed.
Joint mobilization
During the 1950’s, Grieve and Maitland developed and used joint assessments
and treatment techniques. Maitland is widely regarded as one of the most
important original contributors to the assessment and treatment methods used in
the management of neuromusculoskeletal conditions (Petty and Moore, 2001).
The Maitland concept is taught as part of the core curriculum. Other concepts
mentioned below are referred to.
The following manual therapy concepts were described by Petty and Moore
(2001). Cyriax developed techniques for joint and soft tissue diagnosis and
treatment. McConnell has looked at peripheral joints and provided a method of
evaluation of the patellofemoral joint. Kaltenborn provided alternative methods of
joint examination and treatment. McKenzie demonstrated how specific spinal
regions may be examined, and developed a ‘hands-off’ approach to treatment.
Mulligan uses treatment techniques where accessory and physiological
movements are combined. Although all these concepts are useful in practice,
there is not enough time in the undergraduate course to teach all of them in
detail. Reference is made to some of these in teaching.
Spinal manipulative therapy (SMT) has been shown to change range of
movement of muscle, cause alterations to muscle testing responses, and cause
changes to tissue compliance. SMT activates descending pain inhibitory control
systems e.g. the noradrenergic or serotonergic systems (Katavich, 1998).
A study done by Ben-Sorek and Davis (1988) showed that mobilisation
techniques were becoming more widely used by physiotherapists to treat joint
dysfunction. In response to this, curricula have been expanded to prepare
students adequately.
Soft tissue
Treatment of soft tissue structures forms an important part of physiotherapy.
Before treatment, a postural assessment is performed to determine areas of
myofascial tightness. Vision motion analysis of functional positions e.g. standing
is done. This is followed by palpation where factors like tissue texture and skin
mobility is noted (Petty and Moore, 2001). Selective tension tests developed by
Cyriax may be used to determine whether the affected structure is contractile/
non-contractile. Extrinsic, intrinsic and task related factors are also taken into
account.
John Barnes, Francine St George and Travell and Simons have all contributed by
developing different techniques to treat soft tissue (Petty and Moore, 2001;
Steffan, 1996).
Neurodynamics
Examination and treatment of the nervous system may be an important part of
treatment. Neural elements may undergo elongation, sliding, cross sectional
changes, angulation, and compression. These dynamic features occur at many
sites and affect both the central and peripheral nervous systems. If
protective mechanisms fail, symptoms may result. Specific tests are used to
examine the integrity of the system. These tests may then be used as techniques
to treat adhesions and tethering of the neural system (Shacklock, 1995).
Rehabilitation
An important focus of OMT, integral to the practice of the profession, is exercise
therapy, posture assessment and correction, movement analysis and correction
of movement patterns, and functional rehabilitation. Normalisation of movement
will restore function and alleviate pain and therefore physiotherapy is directed at
active movement (Rabey, 2001).
Muscle imbalance
Janda, Jull, Richardson, White and Sahrmann have been instrumental in the
recent development of methods of examination and muscle function (Petty and
Moore, 2001). Muscle imbalance syndromes are commonly diagnosed when a
patient presents with pain from the neuromusculoskeletal system.

Acute pain and impairment of motor control by the central nervous system results
in poor movement patterns that have an adverse effect on joint and muscle
mechanics. Muscle reactions initially affect the local symptomatic region but may
eventually spread through the whole system resulting in changes in posture.
Physiotherapists therefore advocate testing flexibility and strength of muscle and
assessing postural and movement patterns.
Treatment includes correction of muscle length and strength and movement
imbalances. Neurological and biomechanical factors have to be addressed.
Active therapy is encouraged with an emphasis on functional and recreational
activities (Petty and Moore, 2001).
Exercise
Research of the musculoskeletal system has demonstrated the beneficial effects
of movement on all joint tissues. The stress of exercise allows for the
maintenance of muscle bulk and bone mass. Back and joint pain usually
responds favourably to movement. The physiotherapist uses movement and
exercise as the principle tools in the treatment of low back pain and peripheral
joints and there has been abundant research to show the value of movement
(Twomey, 1992; Goldby, 1997).
Exercise therapy is a broad field in OMT and encompasses mobilization
exercise, exercise for treating pain, and increasing muscle strength, postural
correction exercise, and exercise based on motor learning to normalize
movement patterns. Strengthening exercises have traditionally targeted
mobiliser/global muscles. Physiotherapists now pay a great deal of attention to
the stabilizer (local deep postural muscles). Spinal stability is paramount in the
rehabilitation of spinal and postural syndromes (Richardson and Jull, 1995;
Richardson et al, 1999).
Common manual therapy interventions In addition to teaching the various components of OMT in isolation, one needs to
expose students to the multidimensional approach used in practice.
Physiotherapists seldom use one intervention at a time. Combinations of
modalities are used. In OMT, the actual combinations are not standard, but
depend on what the physiotherapist has found to be successful in the
management of a condition. Research shows that a multi-dimensional approach
to the treatment of neuromusculoskeletal conditions is effective.
A study by Li and Bombardier (2001) surveyed physiotherapy approaches to the
management of acute and subacute low back pain. Patient education and
exercise were the most common interventions for acute lumbar impairment. This
was in keeping with another study (Pinnington, 2001) where it was found that
therapeutic exercise was used frequently. In the sub-acute phase, one third of
the physiotherapists said they would use mobilization techniques and increase
physical activity.
A postal survey of one thousand five hundred physiotherapists done in the United
Kingdom showed that Maitland and McKenzie therapies were the most popular
approach. These were followed by exercise therapy. Exercises included
abdominal strengthening, passive stretching and neural tension (Pinnington,
2001).
A study by Jackson (2001) showed that modalities used were passive treatments
in ninety five percent of cases. Manual therapies were used in ninety three
percent and electrotherapy in seventy nine percent of cases. Both of these latter
modalities were used in combination in seventy one percent of cases. In addition
to the combination of physiotherapy modalities, the author comments on
psychological factors in the discussion. These factors may be the predictors of
treatment outcome. Clinicians encourage the use of the biopsychosocial
approach. Cognitive behavioural approaches are now being explored and have
been found to be effective in the management of back pain. The physiotherapist
should therefore also address influencing factors e.g. psychological beliefs about
pain.
Previous studies have found that the choice of treatment may be influenced by
the therapists’ academic degree. In addition, physiotherapists’ own perceptions
of effectiveness influences what they use (Li and Bombardier, 2001).
It can be concluded from the above discussion that the practice of OMT is
becoming increasingly complex. Students should not only be taught individual
techniques or modalities and the application of these, but how and when to
combine various components of OMT therapy. The ability to appropriately
combine therapies for each individual patient may be facilitated by developing
clinical reasoning skills in students. This aspect will be discussed later. Students
cover one join mobilization concept i.e. the Maitland concept and therefore are
not required to choose between various types of joint mobilising techniques. This
skill is developed at a postgraduate level. However students should be
competent in selecting appropriate modalities or techniques taught in the
undergraduate curriculum to formulate treatments.
Additional content related to OMT
Biopsychosocial model Shacklock (1999) advocates education of the patient about pain mechanisms
and the integrative action of the central nervous system. Reference is also made
to the concept of abnormal ‘illness behaviour’ and beliefs. There are several
facets of this concept relevant to OMT. One of these involves the physiotherapist
giving, and the patient expecting a great deal of treatment (which is inappropriate
since the central cause has not been detected by either of them).
The second is ‘somatic focus’ where attention is focused for instance, on body
sensations and proprioception. Here, somatic structures are implicated as the
only source of pain. This can lead to pain avoidance where the patient chooses
not to perform certain activities or movements due to the fear that pain will be
provoked. The physiotherapist can play an important role in appropriate
questioning and observation of sickness and related behaviour. These concepts
should be considered in assessment and become part of treatment. In these
cases, manual techniques should be given less emphasis. In fact, active
movement and educating the patient about their pain would be very beneficial
(Shacklock, 1999; Rabey, 2001).
When dealing with pain where maladaptive beliefs have set in, passive therapy
should be performed only until the patient is able to perform some normal
movement themselves (Shacklock, 1999; Rabey, 2001). The curriculum should
therefore teach students about the social and psychological impact on a patient’s
pain. They need to be aware that this dimension to pain exists and that they will
need to think beyond the anatomy and pathology itself. Teaching these skills is
part of the explicit and implicit curriculum. They can be taught by being given
information on this subject (explicit) and watching clinicians in practice (implicit)
(Rabey, 2001).
Complementary and alternative medicine (CAM)
This is not part of the core curriculum taught in this department but past
graduates were questioned as to whether they felt it should be included. A study
by Murdoch–Eaton and Crombie (2002) was done to see if inclusion of CAM
made a difference to students’ awareness and knowledge of it. Students that had
knowledge of CAM were able to advise family members but did not feel
adequately informed to advise patients. Undergraduate physiotherapy curricula
focus on conventional medical practice. When considering what content to
include in the OMT curriculum, it is the core content that is given priority.
Therefore there may not be enough time allocated to include this subject. Also,
there is not enough scientific evidence to support CAM. This is another reason
why it may not be included in the curriculum.
Finally, the core OMT curriculum should include teaching of the OMT concepts
described above (CAM is not a part of OMT). Combinations of therapy should be
discussed in class and in the clinical setting.