Embed Size (px)
Citation preview
5/2/2017
1
This project was made
possible with funding from:
1
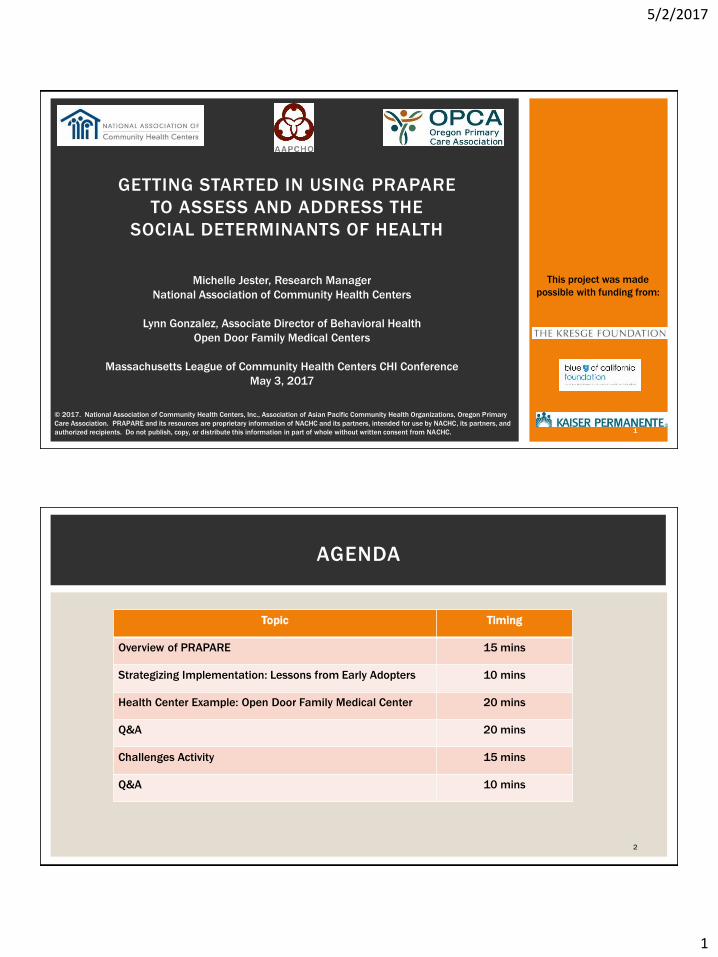
GETTING STARTED IN USING PRAPARE
TO ASSESS AND ADDRESS THE
SOCIAL DETERMINANTS OF HEALTH
© 2017. National Association of Community Health Centers, Inc., Association of Asian Pacific Community Health Organizations, Oregon Primary
Care Association. PRAPARE and its resources are proprietary information of NACHC and its partners, intended for use by NACHC, its partners, and
authorized recipients. Do not publish, copy, or distribute this information in part of whole without written consent from NACHC.
Michelle Jester, Research Manager
National Association of Community Health Centers
Lynn Gonzalez, Associate Director of Behavioral Health
Open Door Family Medical Centers
Massachusetts League of Community Health Centers CHI Conference
May 3, 2017
2
AGENDA
Topic Timing
Overview of PRAPARE 15 mins
Strategizing Implementation: Lessons from Early Adopters 10 mins
Health Center Example: Open Door Family Medical Center 20 mins
Q&A 20 mins
Challenges Activity 15 mins
Q&A 10 mins
5/2/2017
2
Protocol for Responding to & Assessing Patients’ Assets, Risks & Experiences:
A national standardized patient risk assessment protocol designed to engage patients in assessing & addressing social determinants of health (SDH).
PRAPARE = SDH screening tool + implementation/action process
WHAT IS PRAPARE?
3
Customizable Implementation and Action Approach
Assess Needs Respond to NeedsAt the Patient and Population Level
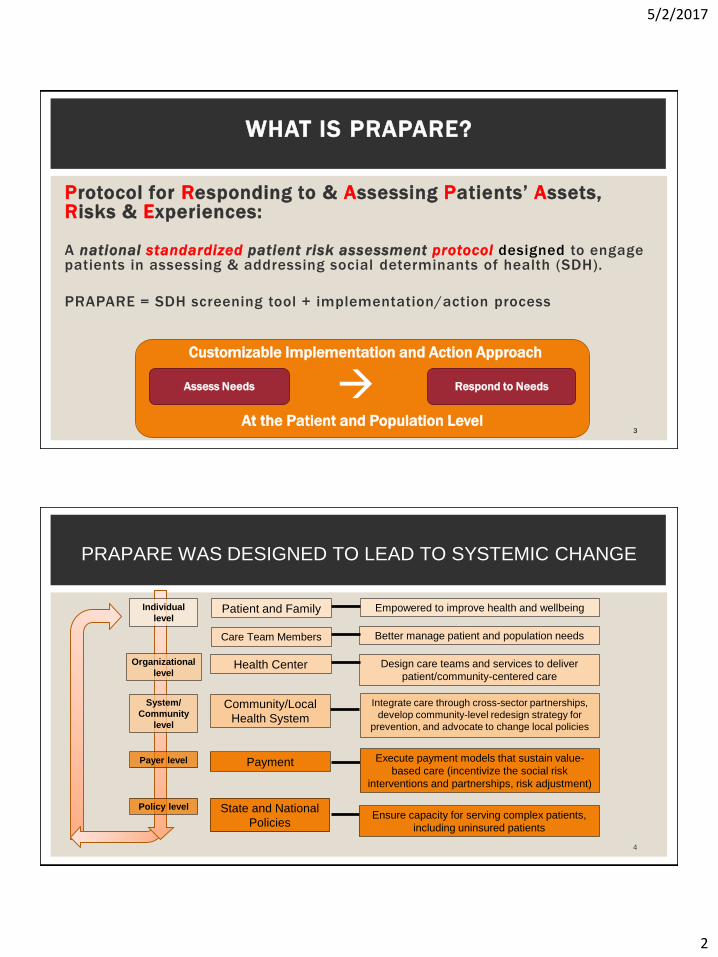
PRAPARE WAS DESIGNED TO LEAD TO SYSTEMIC CHANGE
Patient and Family
Care Team Members
Health Center
Community/Local
Health System
State and National
Policies
Individual
level
Organizational
level
Payer level
Empowered to improve health and wellbeing
Better manage patient and population needs
Design care teams and services to deliver
patient/community-centered care
Integrate care through cross-sector partnerships,
develop community-level redesign strategy for
prevention, and advocate to change local policies
Execute payment models that sustain value-
based care (incentivize the social risk
interventions and partnerships, risk adjustment)
Ensure capacity for serving complex patients,
including uninsured patients
4
System/
Community
level
Payment
Policy level
5/2/2017
3
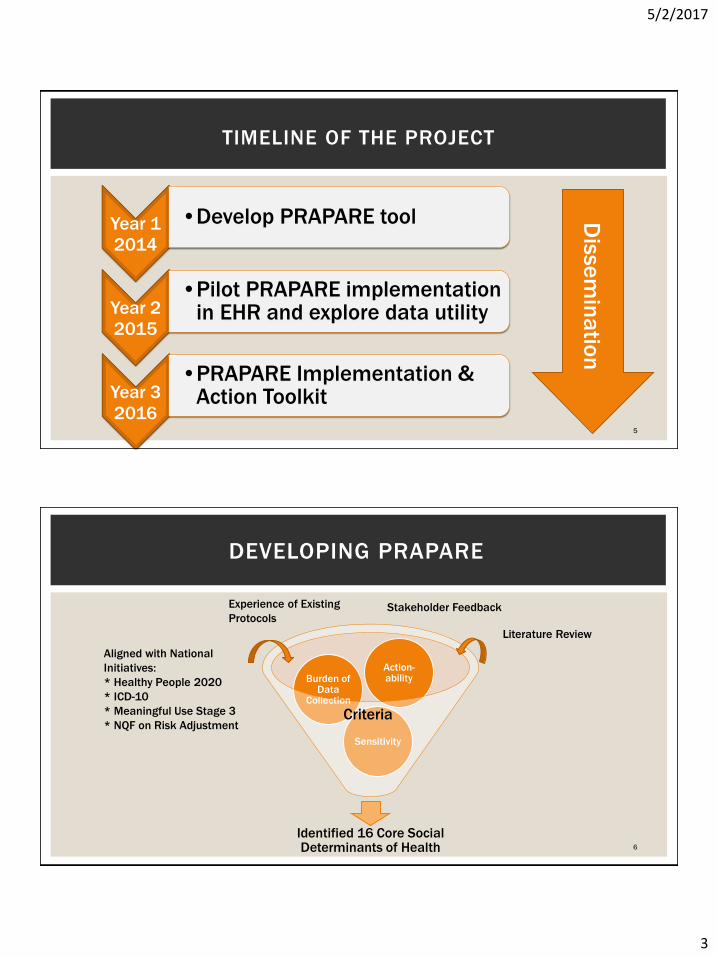
TIMELINE OF THE PROJECT
Year 1
2014
•Develop PRAPARE tool
Year 2
2015
•Pilot PRAPARE implementation in EHR and explore data utility
Year 3
2016
•PRAPARE Implementation & Action Toolkit
5
Dis
se
min
atio
n
DEVELOPING PRAPARE
6
Identified 16 Core Social Determinants of Health
Sensitivity
Burden of Data
Collection
Action-ability
Aligned with National
Initiatives:
* Healthy People 2020
* ICD-10
* Meaningful Use Stage 3
* NQF on Risk Adjustment
Literature Review
Experience of Existing
ProtocolsStakeholder Feedback
Criteria
5/2/2017
4
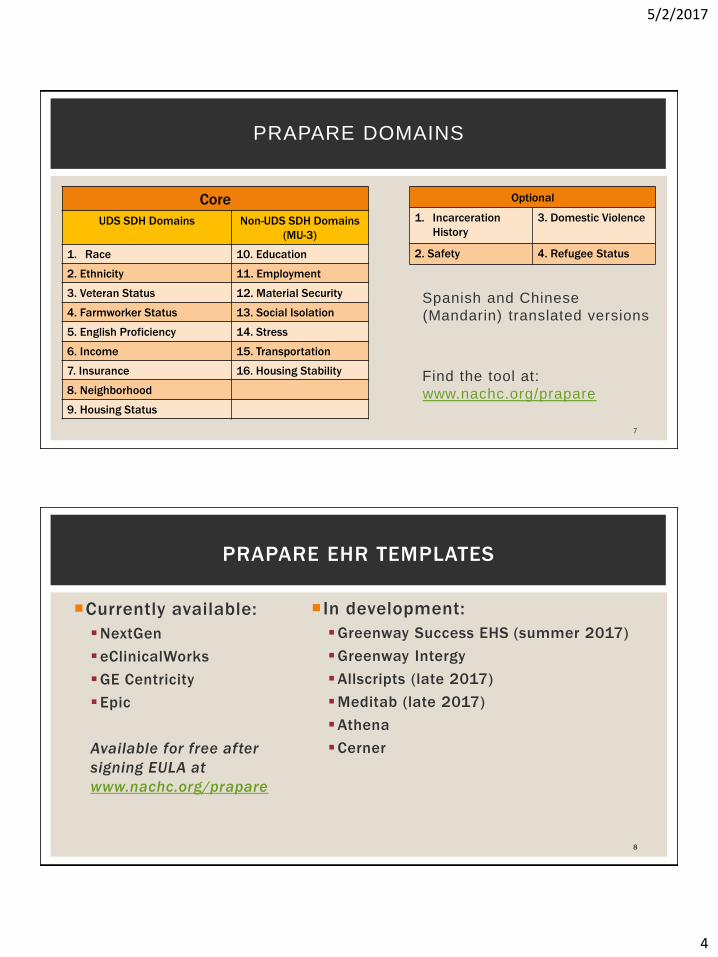
PRAPARE DOMAINS
Spanish and Chinese
(Mandarin) translated versions
Find the tool at:
www.nachc.org/prapare
7
Core
UDS SDH Domains Non-UDS SDH Domains
(MU-3)
1. Race 10. Education
2. Ethnicity 11. Employment
3. Veteran Status 12. Material Security
4. Farmworker Status 13. Social Isolation
5. English Proficiency 14. Stress
6. Income 15. Transportation
7. Insurance 16. Housing Stability
8. Neighborhood
9. Housing Status
Optional
1. Incarceration
History
3. Domestic Violence
2. Safety 4. Refugee Status
Currently available:
NextGen
eClinicalWorks
GE Centricity
Epic
Available for free after
signing EULA at
www.nachc.org/prapare
In development:
Greenway Success EHS (summer 2017)
Greenway Intergy
Allscripts (late 2017)
Meditab (late 2017)
Athena
Cerner
8
PRAPARE EHR TEMPLATES
5/2/2017
5
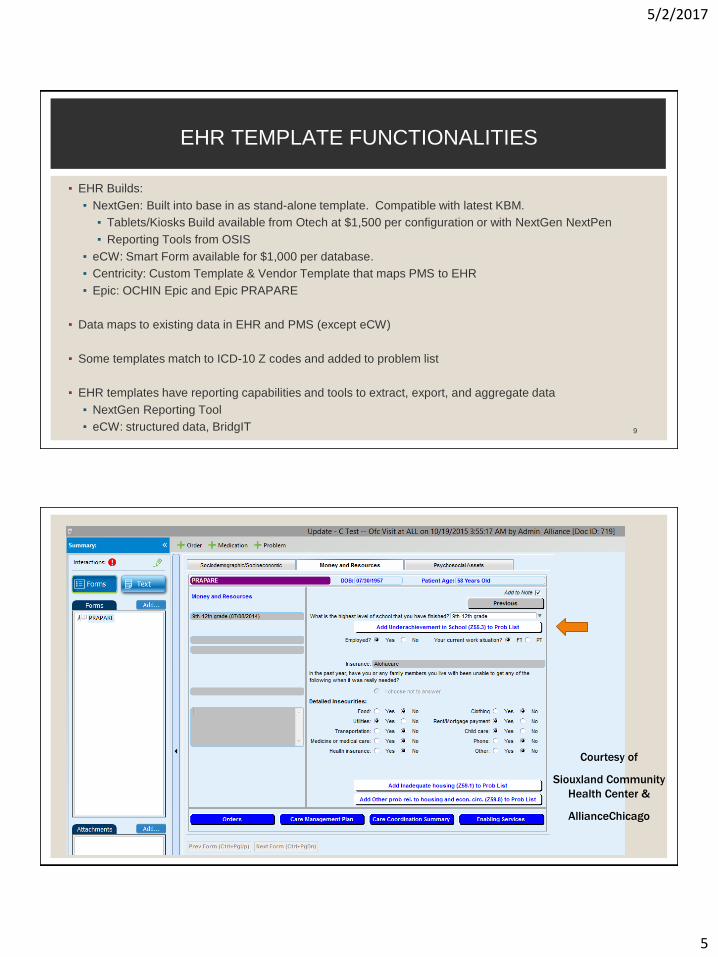
▪ EHR Builds:
▪ NextGen: Built into base in as stand-alone template. Compatible with latest KBM.
▪ Tablets/Kiosks Build available from Otech at $1,500 per configuration or with NextGen NextPen
▪ Reporting Tools from OSIS
▪ eCW: Smart Form available for $1,000 per database.
▪ Centricity: Custom Template & Vendor Template that maps PMS to EHR
▪ Epic: OCHIN Epic and Epic PRAPARE
▪ Data maps to existing data in EHR and PMS (except eCW)
▪ Some templates match to ICD-10 Z codes and added to problem list
▪ EHR templates have reporting capabilities and tools to extract, export, and aggregate data
▪ NextGen Reporting Tool
▪ eCW: structured data, BridgIT 9
EHR TEMPLATE FUNCTIONALITIES
Courtesy of
Siouxland Community
Health Center &
AllianceChicago
5/2/2017
6
16 core domains that have been standardized
All align with national initiatives (HP2020, UDS, IOM, MU, NQF, etc)
Design
Vetted and stakeholder engaged development process
In the EHR to facilitate assessment & interventions (free templates)
Conversation starter and patient-centered
Common core yet flexible:
Able to make more granular and/or add questions
Focus on standardizing the need, not question
Can be used in combination with other tools/data
11
WHAT MAKES PRAPARE UNIQUE AND FEASIBLE?
Health Centers in 44 states are already using PRAPARE EHR
templates
Interest from CHCs in every state
Most PCAs and HCCNs
Some hospitals and health systems
12
PRAPARE IS A NATIONAL MOVEMENT!
5/2/2017
7
13
What We Learned
www.nachc.org/prapare
14
PILOT RESULTS
Easy to administer
Builds patient-provider relationship
Identifies new needs
Many patients face between 4 – 7 social determinants of health
Positive correlation between number of social determinants and
likelihood of having hypertension
5/2/2017
8
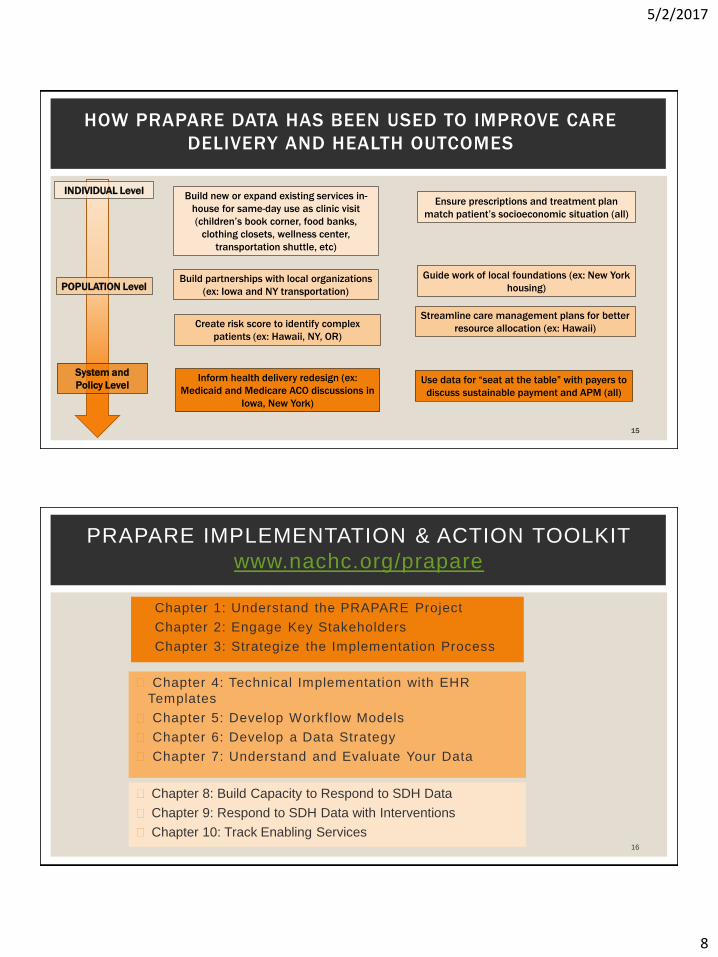
HOW PRAPARE DATA HAS BEEN USED TO IMPROVE CARE
DELIVERY AND HEALTH OUTCOMES
Ensure prescriptions and treatment plan
match patient’s socioeconomic situation (all)
Build new or expand existing services in-
house for same-day use as clinic visit
(children’s book corner, food banks,
clothing closets, wellness center,
transportation shuttle, etc)
Build partnerships with local organizations
(ex: Iowa and NY transportation)
Create risk score to identify complex
patients (ex: Hawaii, NY, OR)
Inform health delivery redesign (ex:
Medicaid and Medicare ACO discussions in
Iowa, New York)
INDIVIDUAL Level
POPULATION Level
System and
Policy Level
Streamline care management plans for better
resource allocation (ex: Hawaii)
Use data for “seat at the table” with payers to
discuss sustainable payment and APM (all)
15
Guide work of local foundations (ex: New York
housing)
◼ Chapter 1: Understand the PRAPARE Project
◼ Chapter 2: Engage Key Stakeholders
◼ Chapter 3: Strategize the Implementation Process
◼ Chapter 4: Technical Implementation with EHR
Templates
◼ Chapter 5: Develop Workflow Models
◼ Chapter 6: Develop a Data Strategy
◼ Chapter 7: Understand and Evaluate Your Data
16
PRAPARE IMPLEMENTATION & ACTION TOOLKIT
www.nachc.org/prapare
◼ Chapter 8: Build Capacity to Respond to SDH Data
◼ Chapter 9: Respond to SDH Data with Interventions
◼ Chapter 10: Track Enabling Services
5/2/2017
9
17
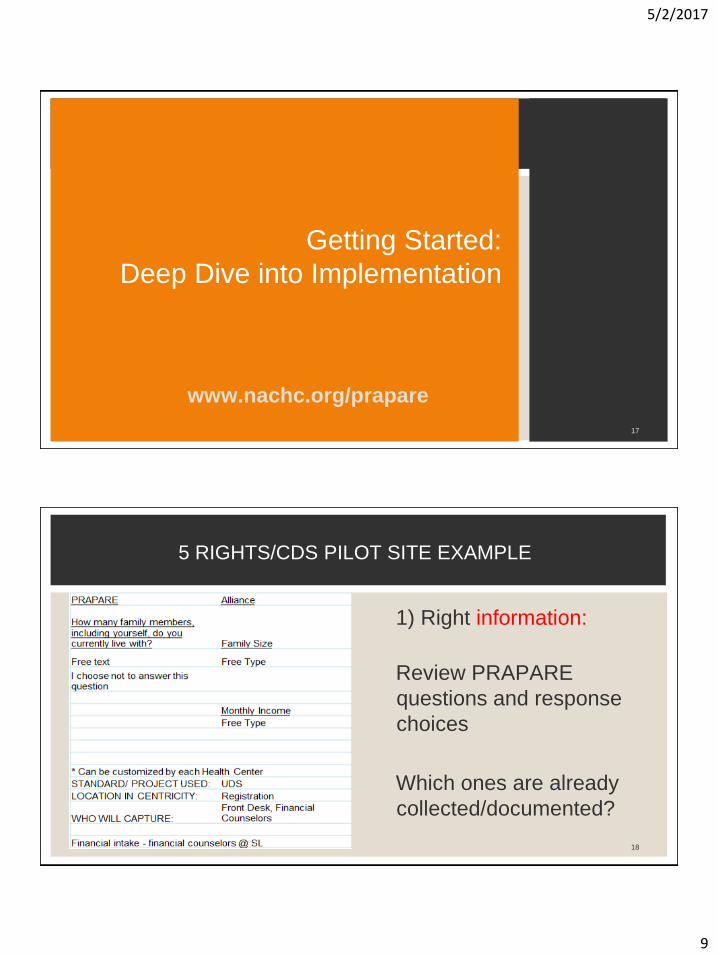
Getting Started:
Deep Dive into Implementation
www.nachc.org/prapare
18
1) Right information:
Review PRAPARE
questions and response
choices
Which ones are already
collected/documented?
5 RIGHTS/CDS PILOT SITE EXAMPLE
5/2/2017
10
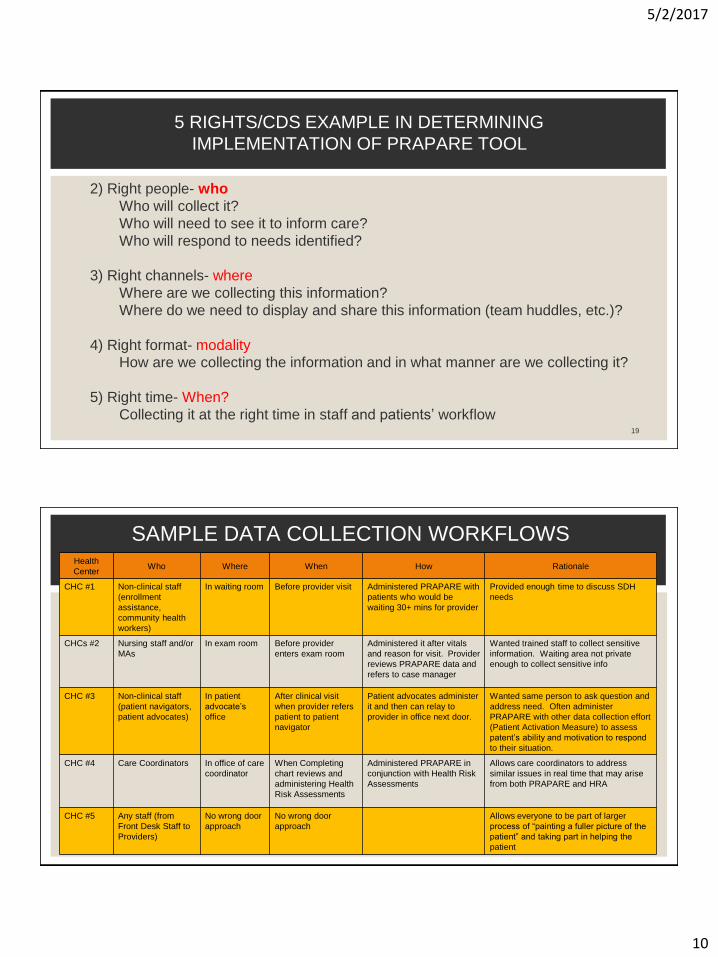
5 RIGHTS/CDS EXAMPLE IN DETERMINING
IMPLEMENTATION OF PRAPARE TOOL
19
2) Right people- who
Who will collect it?
Who will need to see it to inform care?
Who will respond to needs identified?
3) Right channels- where
Where are we collecting this information?
Where do we need to display and share this information (team huddles, etc.)?
4) Right format- modality
How are we collecting the information and in what manner are we collecting it?
5) Right time- When?
Collecting it at the right time in staff and patients’ workflow
SAMPLE DATA COLLECTION WORKFLOWSHealth
CenterWho Where When How Rationale
CHC #1 Non-clinical staff
(enrollment
assistance,
community health
workers)
In waiting room Before provider visit Administered PRAPARE with
patients who would be
waiting 30+ mins for provider
Provided enough time to discuss SDH
needs
CHCs #2 Nursing staff and/or
MAs
In exam room Before provider
enters exam room
Administered it after vitals
and reason for visit. Provider
reviews PRAPARE data and
refers to case manager
Wanted trained staff to collect sensitive
information. Waiting area not private
enough to collect sensitive info
CHC #3 Non-clinical staff
(patient navigators,
patient advocates)
In patient
advocate’s
office
After clinical visit
when provider refers
patient to patient
navigator
Patient advocates administer
it and then can relay to
provider in office next door.
Wanted same person to ask question and
address need. Often administer
PRAPARE with other data collection effort
(Patient Activation Measure) to assess
patent’s ability and motivation to respond
to their situation.
CHC #4 Care Coordinators In office of care
coordinator
When Completing
chart reviews and
administering Health
Risk Assessments
Administered PRAPARE in
conjunction with Health Risk
Assessments
Allows care coordinators to address
similar issues in real time that may arise
from both PRAPARE and HRA
CHC #5 Any staff (from
Front Desk Staff to
Providers)
No wrong door
approach
No wrong door
approach
Allows everyone to be part of larger
process of “painting a fuller picture of the
patient” and taking part in helping the
patient
5/2/2017
11
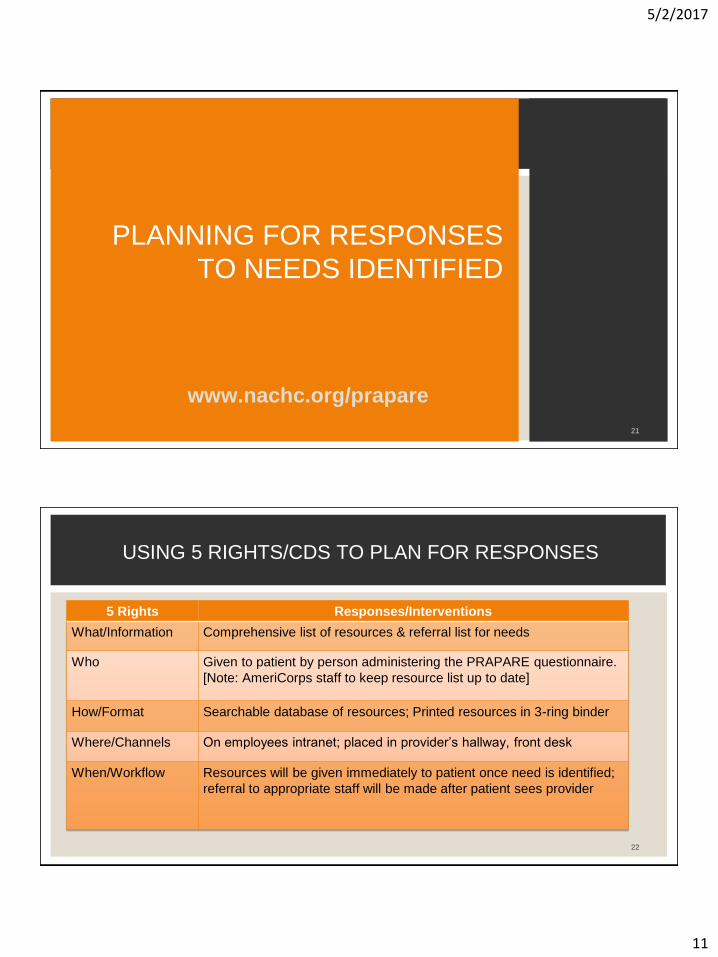
www.nachc.org/prapare
21
PLANNING FOR RESPONSES
TO NEEDS IDENTIFIED
USING 5 RIGHTS/CDS TO PLAN FOR RESPONSES
22
5 Rights Responses/Interventions
What/Information Comprehensive list of resources & referral list for needs
Who Given to patient by person administering the PRAPARE questionnaire.
[Note: AmeriCorps staff to keep resource list up to date]
How/Format Searchable database of resources; Printed resources in 3-ring binder
Where/Channels On employees intranet; placed in provider’s hallway, front desk
When/Workflow Resources will be given immediately to patient once need is identified;
referral to appropriate staff will be made after patient sees provider
5/2/2017
12
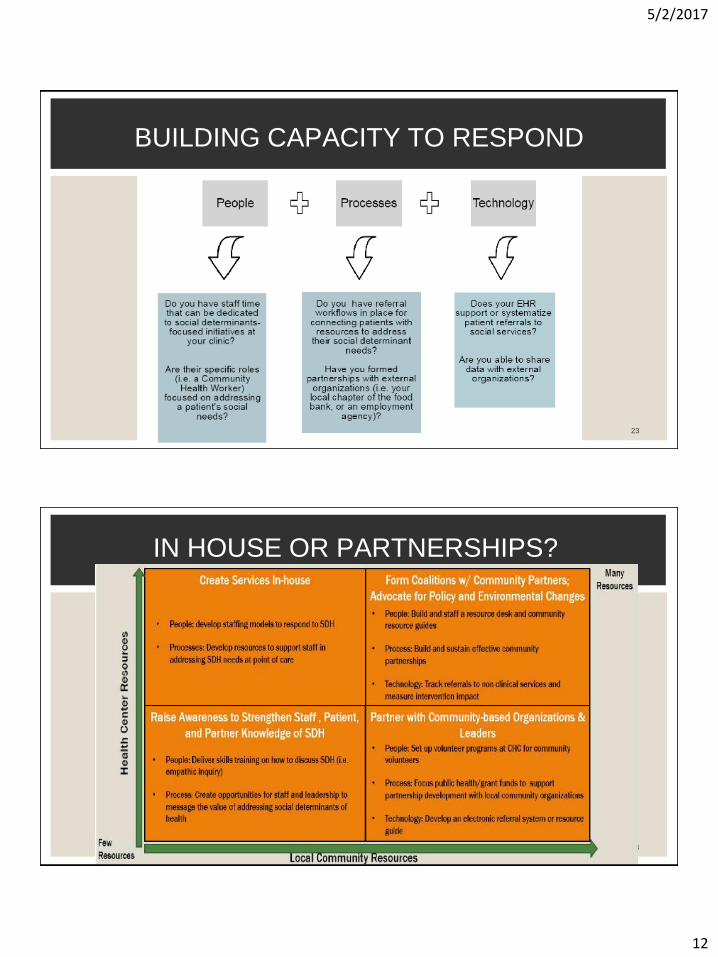
23
BUILDING CAPACITY TO RESPOND
24
IN HOUSE OR PARTNERSHIPS?
5/2/2017
13
25
HEALTH CENTER EXAMPLE:
OPEN DOOR FAMILY MEDICAL CENTER
PRAPARE Implementation -Open Door Family Medical Centers
Objectives:• Open Door Family Medical Centers History
• Patient Population
• Why PRAPARE?
• Data Gathered
• Next Steps
5/2/2017
14
Open Door Family Medical Centers
Founded in the basement of a church in 1972
Originally staffed by volunteer Doctors and Nurses
Gained Federally-Qualified Health Center recognition and Section 330 funding
External Accreditation
Joint Commission & NCQA
JCAHO since 1998
Keen focus on patient safety, staff competency, led to enhanced Quality Improvement
capabilities
NCQA PCMH Level 3 since 2009
Importance of patient access and primary care provider empanelment; focus on
transitions of care and care coordination
DRP NCQA Recognition since 2012
Evidence-based care of patients with diabetes emphasized
5/2/2017
15
Open Door ServicesLicensed under Department of Health
Article 28
• 6 Primary Care Sites in Two Counties
• 7 School-based Health Centers
• Mobile Dental Vans
• Family Medicine Residency program
• Dental Residency program
Open Door Family Medical Centers
At the end of 2016, we had:
• Over 100 Medical, Behavioral Health, and Dental clinicians providing care to…
• 50,000+ patients in…
• 280,000+ visits
5/2/2017
16
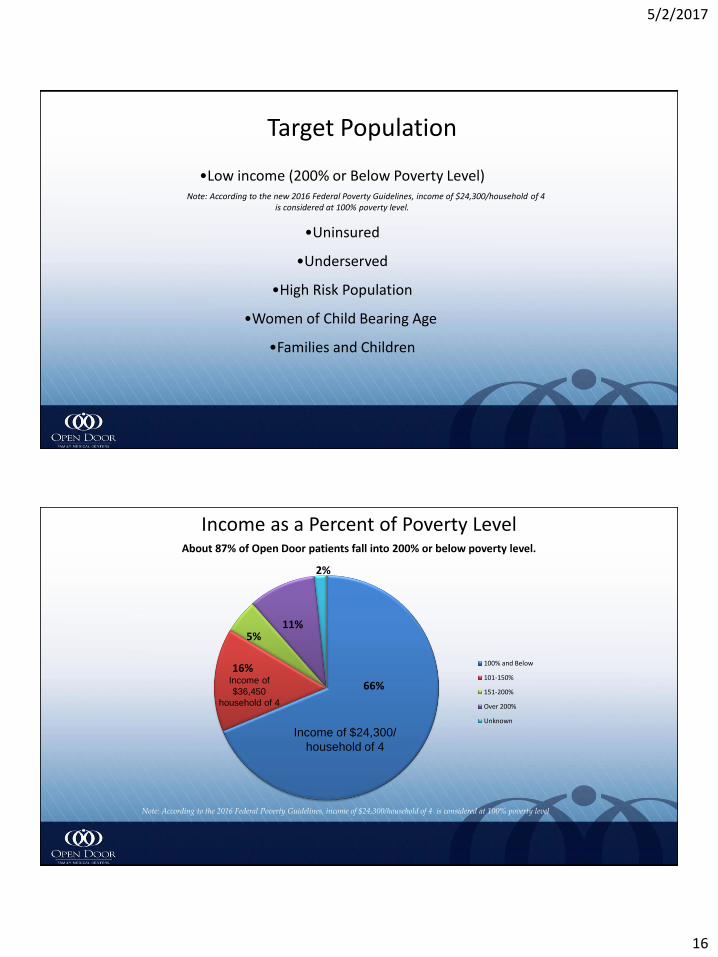
Target Population
•Low income (200% or Below Poverty Level)Note: According to the new 2016 Federal Poverty Guidelines, income of $24,300/household of 4
is considered at 100% poverty level.
•Uninsured
•Underserved
•High Risk Population
•Women of Child Bearing Age
•Families and Children
Income as a Percent of Poverty LevelAbout 87% of Open Door patients fall into 200% or below poverty level.
Note: According to the 2016 Federal Poverty Guidelines, income of $24,300/household of 4 is considered at 100% poverty level
100% and Below
101-150%
151-200%
Over 200%
Unknown
Income of $24,300/
household of 4
Income of
$36,450
household of 4
66%
16%
5%11%
2%
5/2/2017
17
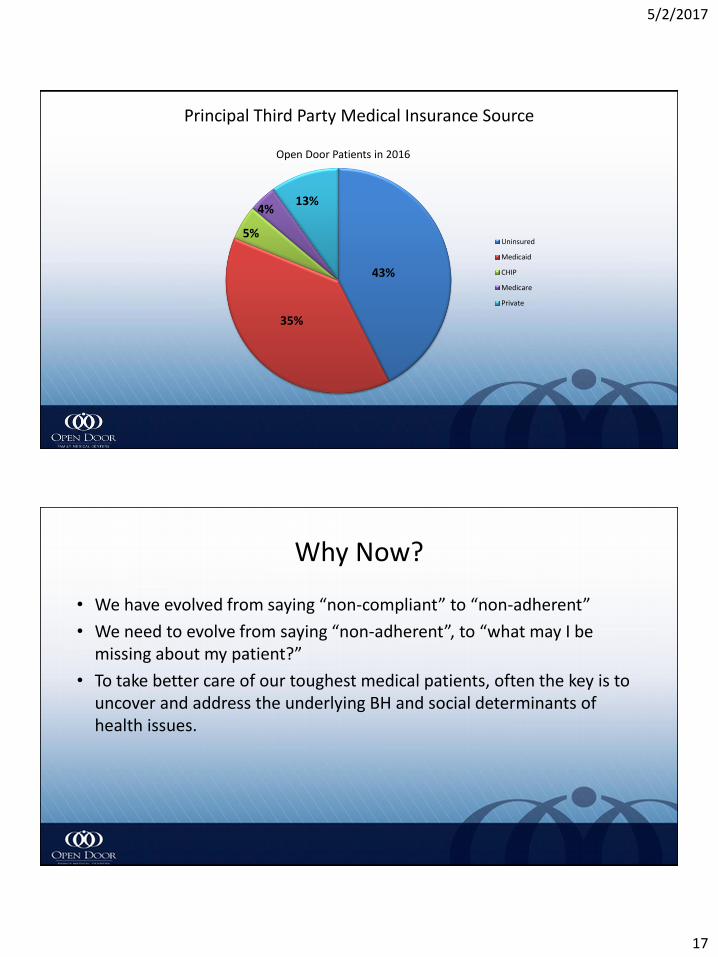
Principal Third Party Medical Insurance Source
39%
Open Door Patients in 2016
Uninsured
Medicaid
CHIP
Medicare
Private
43%
35%
5%
4%13%
Why Now?
• We have evolved from saying “non-compliant” to “non-adherent”
• We need to evolve from saying “non-adherent”, to “what may I be missing about my patient?”
• To take better care of our toughest medical patients, often the key is to uncover and address the underlying BH and social determinants of health issues.
5/2/2017
18
Addressing the Gap
• Consultation model for psychosocial issues on the medical units
– Behavioral Health Integration Specialist (BHIS)
– Licensed Clinician (LMSW)
– Embedded, full-time member of the primary care team
– BHIS patient interactions are not billed (not reimbursable)
5/2/2017
19
Initial Foray into Gathering SDHPilot to Purpose:
• Screening for needs
• Assessing patients Holistically & Ecologically
• Gathering Social History
• Pilot Project in 2015- PRAPARE questions embedded in the EMR (Social History)
• PRAPARE entered into EHR as a SMART form in January, 2017
Who is Doing PRAPARE?
Behavioral Health Integration Specialist (BHIS)
• Clinicians Embedded in the medical units
• LMSW- Licensed Masters Social Worker
• Perform BH assessments and link patients to BH care
• Meet with patients in exam rooms before or after provider enters
• BHIS screens patient because of a previously documented unmet health concern, previous BH involvement, or new patient to Open Door
• Provider identifies a BH concern and calls in BHIS
5/2/2017
20
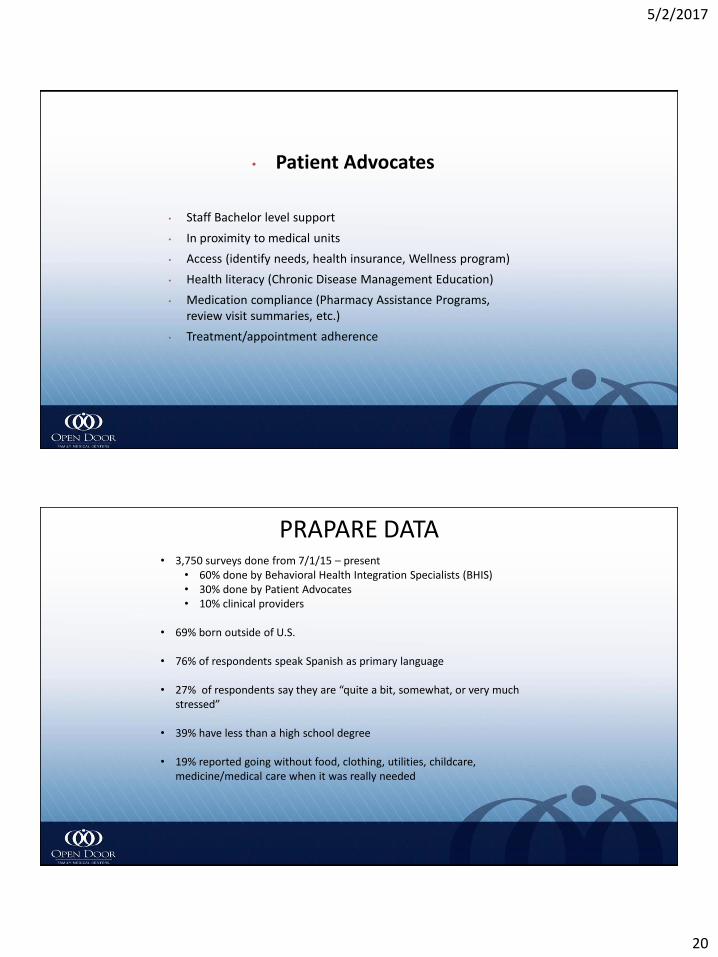
• Patient Advocates
• Staff Bachelor level support
• In proximity to medical units
• Access (identify needs, health insurance, Wellness program)
• Health literacy (Chronic Disease Management Education)
• Medication compliance (Pharmacy Assistance Programs, review visit summaries, etc.)
• Treatment/appointment adherence
PRAPARE DATA• 3,750 surveys done from 7/1/15 – present
• 60% done by Behavioral Health Integration Specialists (BHIS)• 30% done by Patient Advocates• 10% clinical providers
• 69% born outside of U.S.
• 76% of respondents speak Spanish as primary language
• 27% of respondents say they are “quite a bit, somewhat, or very much stressed”
• 39% have less than a high school degree
• 19% reported going without food, clothing, utilities, childcare, medicine/medical care when it was really needed
5/2/2017
21
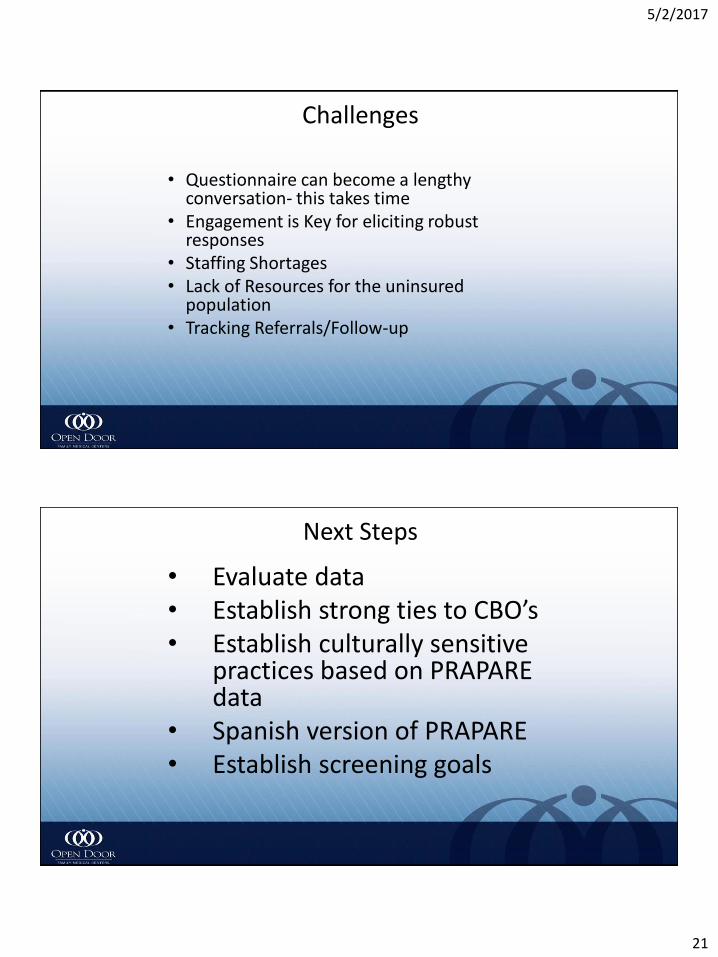
Challenges
• Questionnaire can become a lengthy conversation- this takes time
• Engagement is Key for eliciting robust responses
• Staffing Shortages• Lack of Resources for the uninsured
population• Tracking Referrals/Follow-up
Next Steps
• Evaluate data• Establish strong ties to CBO’s• Establish culturally sensitive
practices based on PRAPARE data
• Spanish version of PRAPARE• Establish screening goals
5/2/2017
22
Thank You!
Lynn Gonzalez, LCSW
Associate Director of
Behavioral Health
(914) 502-1482
44
QUESTIONS AND DISCUSSION
For more information, visit www.nachc.org/prapare
To receive the latest updates on PRAPARE, join our listserv!
Email Michelle Jester at [email protected].
5/2/2017
23
45
GETTING STARTED
Medicaid (2703 Health Homes, etc.)
Private Foundation Grants
Cooperative Agreement
Aligning with other state initiatives (payment reform, delivery system
transformation, quality, etc.)
Just doing it!
46
STATE MODELS FOR IMPLEMENTING PRAPARE
5/2/2017
24
◼We invited clinics to pick a patient population and interview 10
consumers using 3 questions from PRAPARE
◼Afterwards, clinics met face-to-face to share their experiences
How did you and the patient discuss these questions?
What did you observe about the process (your experience, patient’s
reaction)?
Did asking these questions lead to conversations about other topics?
Starting Small: Experimenting with PRAPARE in Oregon
APCM Clinics
47
Visit www.nachc.org/prapare
PRAPARE Tool
PRAPARE Implementation and Action Toolkit
Electronic Health Record PRAPARE Templates
Readiness Assessment
Webinars
PRAPARE Overview
EHR and Workflow-specific
Frequently Asked Questions
Contact: Michelle Jester at [email protected]
Visit http://enablingservices.aapcho.org
AAPCHO’s Enabling Services Accountability
Project
protocol for data collection of non-clinical
enabling services
Enabling Services Data Collection
Implementation Guide and Best Practices
Contact Tuyen Tran at [email protected]
48
RESOURCES AVAILABLE NOW
Upcoming Opportunities:
* Train the Trainer Academy
* CHC Engagement Grants
* Resources from State Pilots
5/2/2017
25
49
CHALLENGES ACTIVITY
◼ Think about what challenges you anticipate facing as you implement PRAPARE
◼ Volunteers will present their challenges to the group
◼ We’ll use the collective brainpower of the group to troubleshoot these challenges
50
Challenges and Overcoming Challenges
5/2/2017
26
51
QUESTIONS AND DISCUSSION
For more information, visit www.nachc.org/prapare
To receive the latest updates on PRAPARE, join our listserv!
Email Michelle Jester at [email protected].
◼ What other activities could PRAPARE leverage and/or add value to? Does this affect or inform the workflow model?
◼ What will the population of focus be? How does that affect the workflow model?
◼ Who will be involved in the implementation of PRAPARE? ▪ Data collection, input data, exporting data, responding to needs identified
◼ Where and when will data be collected and needs responded to?
◼ What modality will be used to collect PRAPARE data and respond to needs identified? ▪ In-person with staff or self-assessment through tablets, kiosks, patient-portal, paper, etc.
◼ What resources are available to respond to needs identified?
◼ Develop plans and process for using the data for enhanced clinical care, complexity analyses, and advocacy for more effective payment.
52
Aspects to Consider When Strategizing Implementation Plans