Embed Size (px)
Citation preview
Ageing as a cross-cutting themeDr Miles D Witham
Clinical Reader in Ageing and Health
Ageing – why bother?
Core business of the NHS Growth area… Current healthcare systems not
equipped to deal with ageing populations and their attendant issues
Underdeveloped evidence base Lot of ill-conceived ‘innovation’ Very little evaluation
Healthy ageing – why bother?
Dramatic increases in longevity over last century
Debatable as to whether this is accompanied by increase in healthy life expectancy
So plenty of work still to do here!
‘adding life to years’ – common, but still useful adage
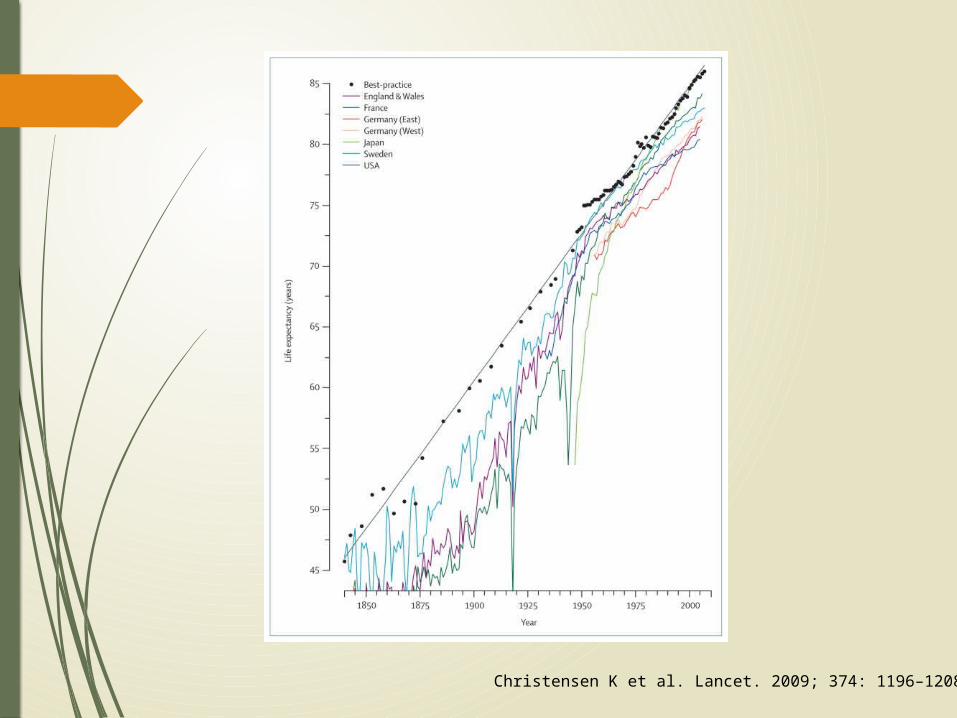
Christensen K et al. Lancet. 2009; 374: 1196–1208
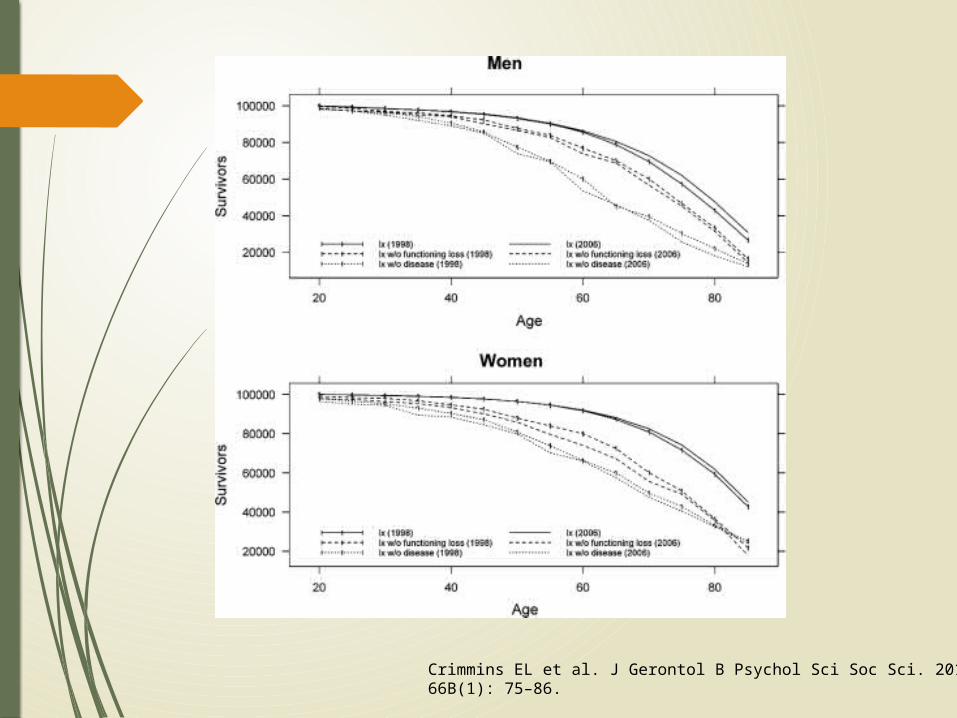
Crimmins EL et al. J Gerontol B Psychol Sci Soc Sci. 2011; 66B(1): 75–86.
Why focus on ageing as a College?
Impact Natural home for collaborative working Some strengths in this area already Historically under-resourced area of
endeavour (but this is changing)
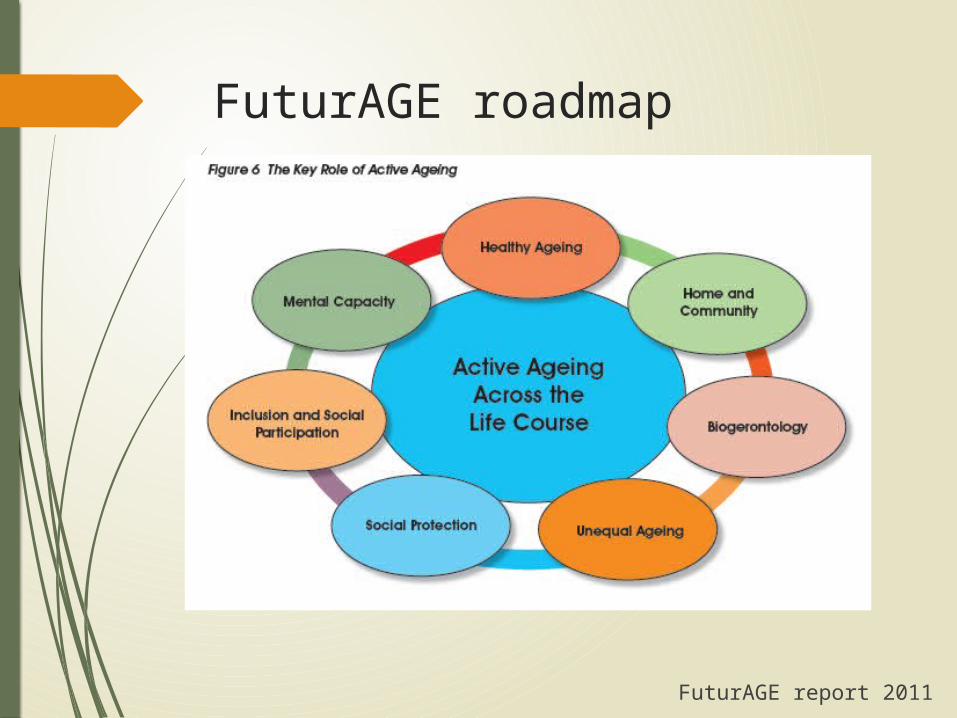
FuturAGE roadmap
FuturAGE report 2011
So what’s wrong with ageing research at the moment?
Basic science in ageing is divorced from clinical practice
Social science (gerontology) is also divorced from clinical practice
Clinical practice lacks an evidence base relevant to older people
Clinical research is often small-scale, single centre, lacking critical mass and lacking the right multidisciplinary ingredients
Lack of ‘follow through’ from discovery, intervention development, testing to implementation and dissemination
The evidence mismatch
Most clinical studies look at young people with single diseases
Older people typically have multiple diseases, and are taking multiple drugs
They lack homeostatic reserve, are highly prone to decompensation, and have multiple functional impairments (the state of frailty)
Older people are highly heterogeneous
So evidence accumulated in younger people may not apply to older people
This leads either to:
- Inappropriate use of interventions in older people that may be either useless or harmful
- Ignoring potentially efficacious interventions in older people because practitioners don’t think the evidence applies to their patient
Health care systems
All this is delivered in healthcare systems set up for:
Single diseases Episodic care And increasingly…Mobile, articulate, IT-
savvy people
Which is not very useful for older people!
So how do we change this?
We need more of:
a) Interventions that target underlying pathological processes common to multiple disorders
b) Studies that deliver evidence that is relevant to older, frail people with multimorbidity
c) Healthcare delivery systems designed for (and by!) older people, which are flexible enough to deal with the heterogeneity of age
We need less of:
Single organ studies Highly selected populations
And also less of: Small pieces of disjointed work Small, isolated teams

Where could we target?
Multiple points in the lifecourse:
In utero Childhood Young adulthood Healthy ageing Ameliorating disease and decline End of life care
Danger of an embarrassment of riches…
What would an effective research strategy look like?
Multidisciplinary – just like good clinical care
Involve older people in priority setting and design
Spectrum of methodological expertise: Qualitative
Systematic reviews
Basic science
Epidemiology
Complex intervention development
Trials
Implementation science
Focus – no point starting a line of enquiry unless you are going to take it through to definitive trials and implementation

The UK picture
Historically, lack of join up between basic science, gerontology and clinical geriatric medicine
Lack of capacity in clinical geriatric medicine
Multidisciplinary work is common Lot of observational work Few small trials Very few large trials

Lack of critical mass until recently
Some good work, but lacking multicentre / UK-wide approach
Dundee: small trials
Edinburgh: delirium and dementia
Bradford, Notts: Health services research
Southampton, Cambridge: Epidemiology
Newcastle: Basic science, epidemiology

Local expertise
Ageing and Health
Oxidative stress (CVDM)
Trials (TCTU)
Epidemiology (DEBU)
Qualitative expertise (SNM)
Some systematic review expertise (scattered)
Implementation science (SISCC) – early stages
Examples from A+H
Health and Social care data integration:
Team from A+H, Clin Pharm, DEBU, HIC, SCPHRP
Now ESRC / Scottish Govt funded PhD (cosupervised by A+H / SNM / PHS / Napier)
Adherence in older HF patients:
Team from A+H, SNM, Health psychology (from Galway)
CSO-funded PhD
Physical activity in older people
Team from A+H, DEBU (PACS cohort); newer collaborations with SNM (PhD on care home physical activity); Computing and Design (BeSIDE project)
Pharmaceutical interventions to improve physical function in older people
Teams from A+H, Clin Pharm, Imaging, IMAR, Health economics (Aberdeen), trials (TCTU and HSRU Aberdeen)
Multicentre trials (BiCARB, LACE);
Single centre trials (PREFACE, SPIROA, ALFIE)
Pitfalls of cross-cutting themes
1) Getting Ageing and Health to do all the work
2) Tacking the word ‘Ageing’ onto work in a superficial way
3) Chasing grant calls with the word Ageing in them, rather than pursuing a coherent programme of work
4) Keeping the same structures and expecting cross-cutting work to magically happen
Conclusion
Ageing is a natural home for interdisciplinary, cross-cutting research
There is a lot of work that needs to be done The funding and structures nationally are
improving UoD has several inherent strengths in this area A joined-up, focussed approach may be the best
way to develop critical mass in selected areas Local examples of collaboration give a good
basis for future growth




















![50 Years of Witham Hall[1]](https://img.pdfslide.us/doc/110x75/5571fb3a4979599169944a23/50-years-of-witham-hall1.jpg)